")
Back to Journals » Cancer Management and Research » Volume 14
CXCL4L1 May Help Differentiate Benign from Malignant Pulmonary Lesions and Predicts Prognosis of Patients with Lung Cancer
Authors Zhang L, Li G, Zhang H, Liu H, Li S, Wang Y, Qi H
Received 2 December 2021
Accepted for publication 24 March 2022
Published 7 June 2022 Volume 2022:14 Pages 1903—1910
DOI https://doi.org/10.2147/CMAR.S352217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Beicheng Sun
Lei Zhang,1,* Guangping Li,2,* Hongxin Zhang,3 Huaqun Liu,4 Songlin Li,1 Yanan Wang,4 Huisheng Qi1
1Department of Respiration, Tangshan Workers’ Hospital, Tangshan, 063000, People’s Republic of China; 2Department of Clinical Laboratory, Tangshan Workers’ Hospital, Tangshan, 063000, People’s Republic of China; 3Department of Cardiology, Tangshan Workers’ Hospital, Tangshan, 063000, People’s Republic of China; 4Department of Oncology, Tangshan Workers’ Hospital, Tangshan, 063000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huisheng Qi, Department of Respiration, Tangshan Workers’ Hospital, No. 27 Wenhua Road, Tangshan, 063000, People’s Republic of China, Email [email protected]
Background: Lung cancer (LC) is the leading type of cancer worldwide, yet it’s challenging to detect early LC. Therefore, it is valuable to explore diagnostic biomarker that can distinguish malignant pulmonary lesions from benign diseases. The potential role of plate factor-4 variant (CXCL4L1) will be investigated in detecting early LC.
Methods: A consecutive of 174 patients with single pulmonary nodule and 50 healthy controls were enrolled. Serum CXCL4L1 expression level was evaluated using ELISA. Survival curves were generated to analyze survival outcomes. Receiver operating characteristic curves were used to calculate diagnostic accuracy.
Results: Serum CXCL4L1 was downregulated in patients with LC when compared with those with lung benign lesions (LBL) or healthy controls. Meanwhile, lower serum CXCL4L1 expression was associated with advanced TNM stage and lymph node metastasis. Furthermore, a low expression of CXCL4L1 resulted in worse survival outcomes in LC patients. Serum CXCL4L1 expression obtained an area under curve (AUC) of 0.81 (95% CI: 0.74– 0.88), a sensitivity of 70.6%, and a specificity of 85.8% for discriminating patients with LC form patients with LBL. In addition, serum CXCL4L1 expression achieved an AUC of 0.82 (95% CI, 0.74– 0.90), a sensitivity of 72.0%, and a specificity of 85.9% for distinguishing patients with LC form healthy controls.
Conclusion: This study suggests that CXCL4L1 may prove to be a potential non-invasive diagnostic and prognostic biomarker for early LC patients.
Keywords: CXCL4L1, lung cancer, cancer detection, lung benign lesion, prognosis
Introduction
Lung cancer (LC) is the leading cause of cancer-related mortality worldwide.1 Especially in China, LC is much more prevalent and life-threatening with a mortality of 28.49 per 100,000 persons in 2014.2 Currently, multidisciplinary therapies based on surgery have achieved considerable prognosis for patients with early-stage LC with a one-year survival rate of 70%.3 Unfortunately, more than 75% of LC patients have been diagnosed at more advanced stages with a poor five-year survival of 15.6% in China.4 Low dose CT (LDCT) screening is currently recommended for high-risk people (55–75 years old, smoking over 30 pack-years) to increase the detection rate and reduce the mortality of LC.5 However, it’s still a challenge to deal with solitary pulmonary nodules (SPNs) detected by LDCT in clinical practice because a lot of SPNs turn out to be benign nodules. As the US National Lung Cancer Screening Test (NLST) study reported, LDCT screening has a false positive rate as high as 96.4%,6 which could result in both wastage of medical care and unnecessary psychological burden. Therefore, it is crucial to explore noninvasive serological biomarkers for the diagnosis of early LC with high sensitivity and specificity, and further to help with prognosis stratification.
The plate factor-4 variant (CXCL4L1), the non-allelic variant of CXCL4, was discovered in 1989 by Green et al and cloned shortly thereafter.7,8 CXCL4 has significant antitumoral activity by inhibition of GPCR-mediated endothelial cell chemotaxis.9 One study has shown that downregulation of CXCL4L1 was significantly associated with advanced pathological features and poor prognosis in prostate cancer patients after surgery.10 Moreover, CXCL4L1 could inhibit melanoma and lung carcinoma growth and metastasis in vivo by preventing angiogenesis.11 Given the critical role of CXCL4L1 in the tumorigenesis of LC, we further speculated that CXCL4L1 might be a potential diagnostic or prognostic biomarker for early LC patients.
In this study, we measured CXCL4L1 expression in the serum of early LC patients and patients with lung benign lesion (LBL). We investigated the diagnostic power of CXCL4L1 in differentiating malignant from benign pulmonary nodules. We further analyzed the relationship between CXCL4L1 expression and clinicopathologic features and survival outcomes for LC patients.
Materials and Methods
Patients
This study was approved by the Ethics Committee of Tangshan Workers’ Hospital and conformed to the Declaration of Helsinki. All enrolled individuals have provided signed informed consents. A consecutive of 174 patients with single pulmonary nodule (< 5 cm in diameter) determined by CT/LDCT scan were recruited between January 2017 and January 2021. All included cases underwent surgical resections and were evaluated by postoperative pathology. Patients had an age over 18 and no prior history of malignancy. In addition, a group of 50 age and sex-matched healthy controls (HC) were enrolled. Blood samples were collected one day before surgery for patients with pulmonary nodule and collected from the healthy controls during physical check. The peripheral blood samples were collected from all participants in serum gel separator tubes. Each sample was immediately centrifuged at 3000 g for ten minutes at 4°C to separate serum and then stored at −80°C until tested.
Data Collection
All relevant clinical and pathological data were collected from each patient based on electronic medical records, including age, gender, smoking status, histology, tumor size, TNM stage, and lymph node metastasis. All patients were regularly followed up by telephone and the last follow-up date was June 2021. Survival information included overall survival (OS) and recurrence-free survival (RFS). OS was defined as the interval from the date of surgery to the date of death or endpoint. RFS was defined as the interval from the date of surgery to the date of tumor recurrence or death.
Enzyme-Linked Immunoassay (ELISA) Assay
Serum CXCL4L1 levels were measured using a commercially available ELISA kit (EL017810HU, Cusabio Biotech, Wuhan, China) as previously described. Briefly, 100 µL serum samples were added into the corresponding wells and incubated at 37°C for 2 h with gentle shaking. The waste liquid was then discarded. Biotinylated antibody (100 μL) was added into each well, and the samples were incubated at 37°C for 1 h with gentle shaking. After three washes with washing buffer, 100 μL of streptavidin-horseradish peroxidase (avidin-HRP) was added into each well. Incubation was performed at 37°C for 1 h. The washing process was repeated as described above. Color development was achieved by adding 90 μL per well of 3,3’,5,5’-tetramethylbenzidine (TMB) as a substrate; sulfuric acid (50 μL) was added to stop the reaction. The optical density was measured at 450 nm on the SpectraMax 190 Microplate Reader (Molecular Devices, San Jose, CA, USA). CXCL4L1 expression was calculated with a four-parameter logistic curve and fit to the standard value. All serum specimens were measured in duplicate.
Statistical Analyses
Continuous variables were expressed as mean ± standard deviation or median with interquantile range when appropriate; categorical variables were expressed as frequencies with percentages. Differences between two groups were analyzed using Student’s t-test or Mann–Whitney U-test. Comparisons of multiple groups were analyzed using ANOVA followed by Dunnett’s test. Categorical data were compared using chi-square test or Fisher’s exact test. Kaplan-Meier curves were plotted for OS and RFS, and compared using Log rank test. Factors associated with OS or RFS were assessed by both univariate and multivariate Cox regression analyses with forward step-wise approach. Receiver operating characteristic curves (ROC) were utilized to calculate diagnostic accuracy. Statistical evaluations were performed using SPSS 20.0 (IBM SPSS Inc., Chicago, IL, USA) and GraphPad Prism 8.01 (GraphPad Software lnc.). Differences were considered to be significant when P< 0.05.
Results
Study Population
As shown in Table 1, among all 174 patients with pulmonary nodule who underwent surgery, 106 patients were pathologically confirmed as LC and 68 patients as LBL. The baseline characteristics including age, sex, and smoker status were comparable between LC, LBL, and HC groups (all P > 0.05). Among 106 patients with LC, 55 (51.9%) patients had adenocarcinoma, 28 (26.4%) patients had squamous cell carcinoma, 8 (7.5%) patients had large cell carcinoma, and 15 (14.2%) patients had small cell carcinoma. 56 (52.8%) patients had TNM stage I and 50 (47.2%) had stage II. Among 68 patients with LBL, 23 (33.8%) patients had tuberculosis, 21 (30.9%) patients had hamartoma, 12 (17.6%) patients had fungal infection, 8 (11.8%) patients had inflammation, and 4 (5.9%) patients had granuloma.
 |
Table 1 Patients Clinical Characteristics |
Circulating CXCL4L1 is Downregulated in LC Patients
Circulating CXCL4L1 expression levels in serum samples of patients with LC, LBL, and HC were evaluated using ELISA. Our results showed that CXCL4L1 expression in patients with LC was significantly lower than that in patients with LBL or HC (P< 0.001, Figure 1A). In terms of TNM stage, LC patients with stage II had significant lower CXCL4L1 expression than patients with stage I (P< 0.01, Figure 1B). Additionally, CXCL4L1 expression level was markedly lower in patients with lymph node metastasis than those without lymph node metastasis (P< 0.01, Figure 1C). No significant difference was observed in CXCL4L1 expression level with respect to different histology types (P= 0.75, Figure 1D).
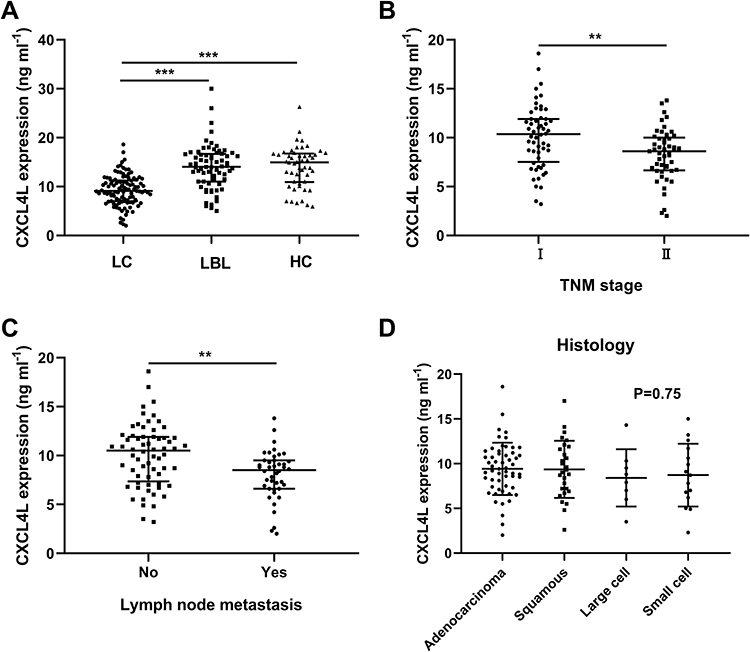 |
Figure 1 Downregulation of serum CXCL4L1 in lung cancer (LC) patients. (A) Serum CXCL4L1 expression in patients with LC, patients with lung benign lesion (LBL), and healthy controls (HC). (B–D) Serum CXCL4L1 expression in LC patients stratified by TNM stage, lymph node metastasis, and histology types. **P< 0.01, ***P< 0.001. |
Correlation of CXCL4L1 Expression Level with Clinicopathological Features
In order to analyze the correlation of CXCL4L1 expression with clinical characteristics, we divided the 106 patients with LC into a low-expression group and a high expression group with the median level of CXCL4L1 (9.5 ng mL−1) as the cutoff value. As shown in Table 2, low expression of CXCL4L1 was significantly associated with advance TNM stage (P = 0.002) and lymph node metastasis (P = 0.017). However, no correlation was observed in CXCL4L1expression with age (P = 0.754), sex (P = 0.204), smoking status (P = 0.229), histology (P = 0.868), and tumor size (P = 0.244).
 |
Table 2 The Association Between CXCL4L1 Expression and Clinicopathological Characteristics of LC |
The Prognostic Significance of CXCL4L1 Level in LC Patients
Next, by generating Kaplan-Meier curves, our data showed that LC patients with a low level of CXCL4L1 was associated with worse OS (Figure 2A; P = 0.010) and RFS (Figure 2B; P = 0.015). As shown in Table 3, univariate and multivariate analyses of the factors affecting OS were performed. TNM stage, lymph node metastasis, and higher CXCL4L1 found to be significant in the univariate analysis were included in the multivariate regression analysis. The results revealed that TNM stage (hazard ratio [HR] with 95% confidence interval [CI] = 2.985 [1.524–4.584]; P = 0.013), lymph node metastasis (HR with 95% CI = 2.121 [1.354–3.451]; P = 0.031), and higher CXCL4L1 (HR with 95% CI = 0.764 [0.571–0.936], P = 0.019) remained as significant predictors of OS. In addition, we also found that TNM stage, lymph node metastasis, and higher CXCL4L1 were also associated with RFS on univariate and multivariate analyses (Table 4).
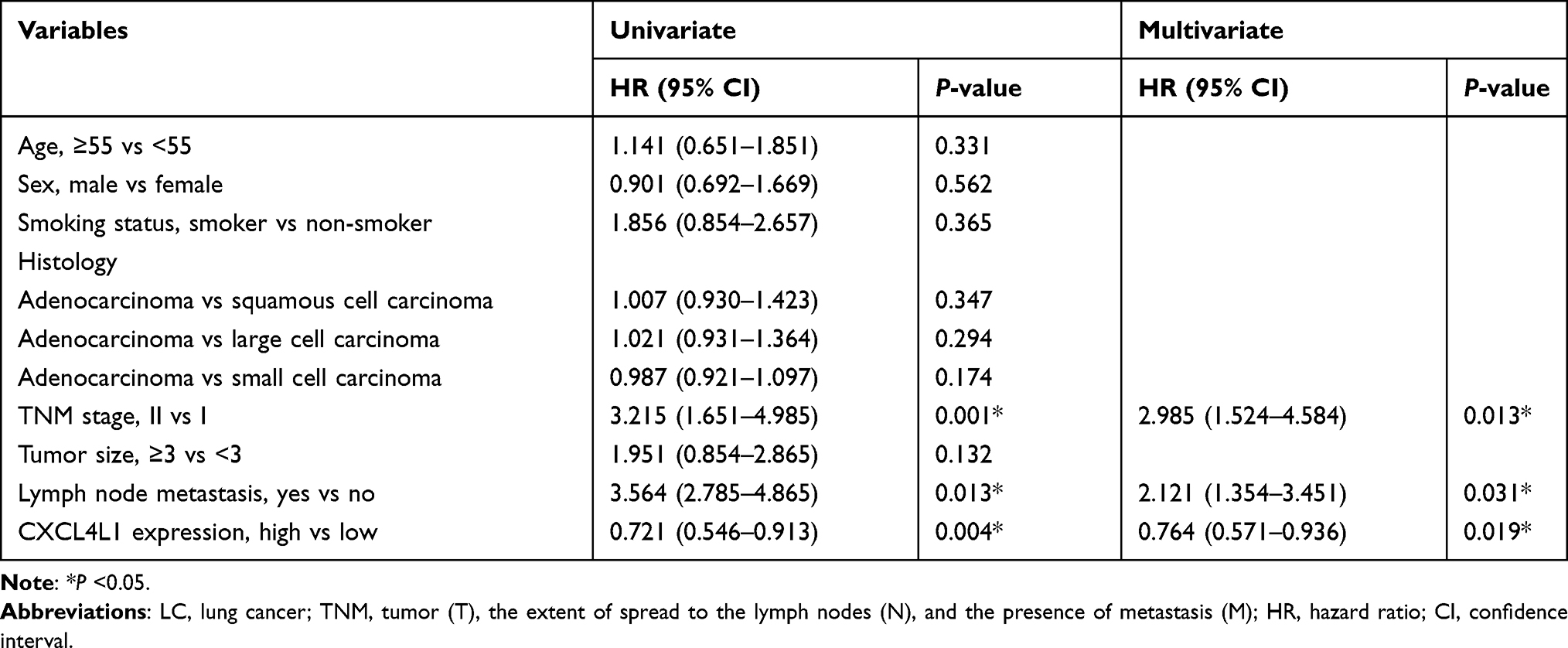 |
Table 3 Univariate and Multivariate Cox Proportional Analyses of Prognostic Factors Associated with Overall Survival in LC Patients |
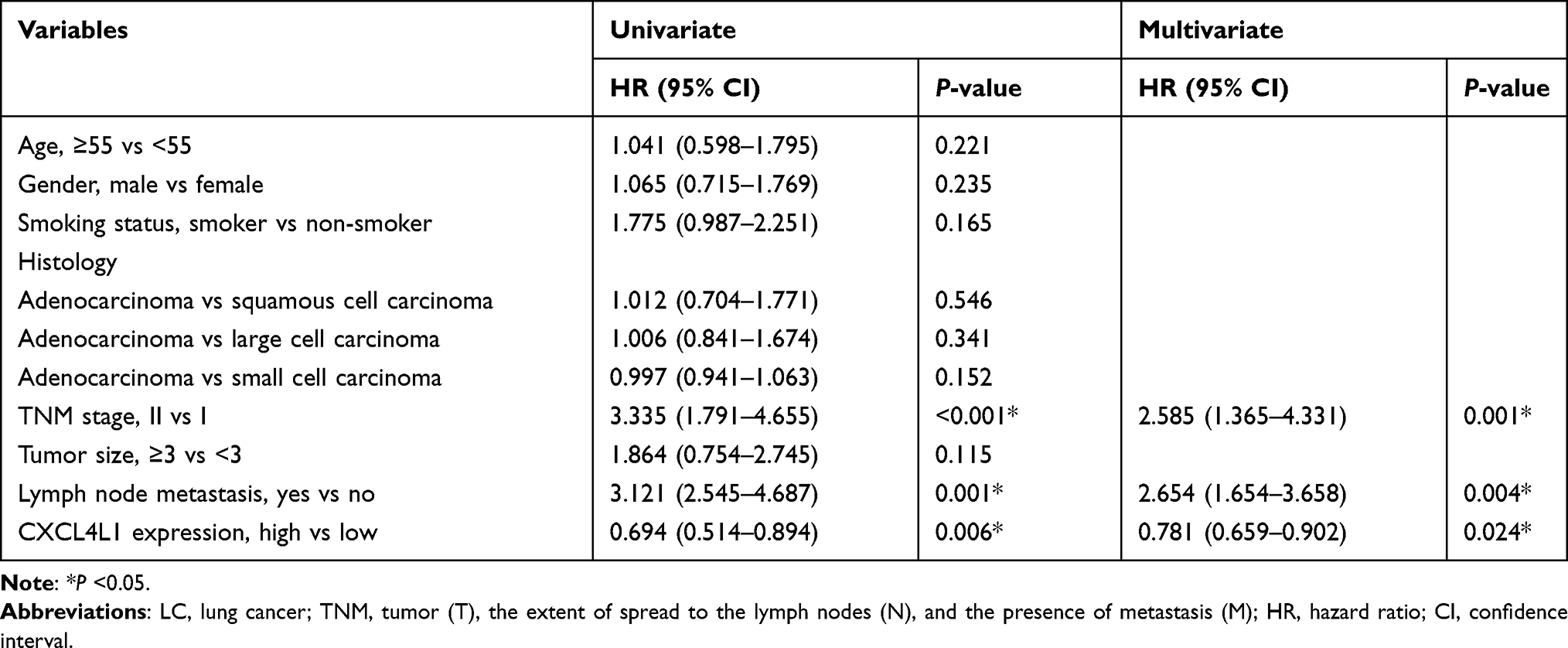 |
Table 4 Univariate and Multivariate Cox Proportional Analyses of Prognostic Factors Associated with Recurrence-Free Survival in LC Patients |
 |
Figure 2 Kaplan-Meier curves of prognosis. Overall survival (A) and recurrence-free survival (B) of patients with lung cancer stratified by serum CXCL4L1 expression. |
The Diagnostic Performance of Serum CXCL4L1 in LC Patients
To evaluate the diagnostic value of CXCL4L1 in LC patients, we analyzed the performance of serum CXCL4L1 in distinguishing LC patients from LBL or healthy control using ROC analysis. Figure 3A demonstrated that serum CXCL4L1 level could be used as a promising biomarker for distinguishing LC patients from LBL, with an area under the curve (AUC) of 0.81 (95% CI: 0.74–0.88), a sensitivity of 70.6% and a specificity of 85.8%, and a cutoff value of CXCL4L1 of 12.15 ng mL−1 (P < 0.001). Moreover, as shown in Figure 3B, serum CXCL4L1 level had significant ability in differentiating LC patients from HC, with an AUC of 0.82 (95% CI, 0.74–0.90), a sensitivity of 72.0% and a specificity of 85.9%, and a cutoff value of CXCL4L1 of 12.25 ng mL−1 (P < 0.001).
 |
Figure 3 Diagnostic value of serum CXCL4L1 expression. (A) ROC curve for serum CXCL4L1 to distinguish patients with lung cancer (LC) from patients with lung benign lesion (LBL). (B) ROC curve for serum CXCL4L1 to distinguish patients with lung cancer (LC) from healthy controls (HC). Abbreviation: ROC, receiver operating characteristic curve. |
Discussion
Currently, cancer early screening is the most economical and effective method to reduce cancer-specific mortality in clinical practice.12,13 Nevertheless, it has long been a great challenge to detect early LC due to the high false positive rate of LDCT screening and the difficulty to perform diagnostic biopsies.14 Therefore, it will be particularly valuable to explore a non-invasive, convenient, and highly sensitive diagnostic biomarker that can distinguish malignant pulmonary lesions from benign diseases.
Various studies have implicated CXCL4L1 in angiogenesis, anti-angiogenesis, and tumorigenesis. As reported, CXCL4L1 exhibits a strong staining in tumor cells in colorectal cancer, while a weak to negative staining in tumor cells in esophageal cancer.15 Furuya et al determined that CXCL4L1 were significantly lower in endometriosis-associated ovarian cancer tissues than in corresponding endometriosis.16 In contrast, Quemener et al reported a greatly increased CXCL4L1 expression in primary and metastatic pancreatic adenocarcinoma using a tissue microarray analysis.17 Notably, CXCL4L1 exerted antitumoral effects in lung carcinoma growth and metastasis in vivo via inhibition of angiogenesis.11
In this study, we demonstrated that serum CXCL4L1 was significantly downregulated in patients with LC comparing with patients with LBL and healthy controls. Our data showed that lower serum CXCL4L1 expression was associated with advanced TNM stage and lymph node metastasis. Furthermore, we evaluated the correlation between CXCL4L1 expression and LC patients’ prognosis, and found that a low serum CXCL4L1 level was associated with poorer survival in LC patients. The tumor suppressive role of CXCL4L1 in LC patients is consistent with the previous studies mentioned above. Downregulation of CXCL4L1 probably alters the delicate angiostatic balance toward angiogenesis, which may partially explain why CXCL4L1 under-expression results in tumor recurrence and progression of LC.
The value of CXCL4L1 in predicting early LC has not been previously investigated. In our study, we found that serum CXCL4L1 could be utilized as a capable diagnostic biomarker to discriminate malignant from benign lesions with a sensitivity of 70.6% and a specificity of 85.8%. The cutoff value of CXCL4L1 was 12.15 ng mL−1, which could provide a clinical guidance for early LC detection in patients with lung lesions, in complement with LDCT screening. The serum sample could be defined as “positive” when CXCL4L1 expression was lower than 12.15 ng mL−1, and further pathological test should be recommended. Moreover, a regular follow-up with imaging examination could be recommended for patients with negative CXCL4L1 expression, which may reduce the excessive medical burden due to the false-positive of LDCT. In addition, serum CXCL4L1 demonstrated a great ability to differentiate patients with early LC from healthy controls, which could not only predict early LC for patients with lung lesions but also for healthy population conducting physical examination.
Some limitations exist in this study. First, the external validation cohort is lacking, hence a larger number of individuals would be needed to validate the diagnostic and prognostic value of CXCL4L1 in early LC. In addition, despite the strong correlation between CXCL4L1 expression and clinical malignant characteristics, the exact mechanisms of CXCL4L1 in LC progression remain unclear and warrant further investigation.
In conclusion, this study demonstrates that CXCL4L1 was downregulated in early LC, and could be used as a diagnostic and prognostic biomarker for LC patients.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Funding
There is no funding to report.
Disclosure
No conflict of interests was declared in the study.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Cao M, Chen W. Epidemiology of lung cancer in China. Thoracic Cancer. 2019;10(1):3–7. doi:10.1111/1759-7714.12916
3. Low M, Ben-Or S. Thoracic surgery in early-stage small cell lung cancer. Thorac Surg Clin. 2018;28(1):9–14. doi:10.1016/j.thorsurg.2017.08.003
4. Bade BC, Dela Cruz CS. Lung cancer 2020: epidemiology, etiology, and prevention. Clin Chest Med. 2020;41(1):1–24. doi:10.1016/j.ccm.2019.10.001
5. O’Dowd EL, Baldwin DR. Lung cancer screening-low dose CT for lung cancer screening: recent trial results and next steps. Br J Radiol. 2018;91(1090):20170460. doi:10.1259/bjr.20170460
6. Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395–409.
7. Ruytinx P, Proost P, Struyf S. CXCL4 and CXCL4L1 in cancer. Cytokine. 2018;109:65–71. doi:10.1016/j.cyto.2018.02.022
8. Green CJ, Charles RS, Edwards BF, Johnson PH. Identification and characterization of PF4varl, a human gene variant of platelet factor 4. Mol Cell Biol. 1989;9(4):1445–1451. doi:10.1128/mcb.9.4.1445-1451.1989
9. Maione TE, Gray GS, Petro J, et al. Inhibition of angiogenesis by recombinant human platelet factor-4 and related peptides. Science. 1990;247(4938):77–79. doi:10.1126/science.1688470
10. Zhang M, Guan J, Huo YL, Song YS, Chen LZ. Downregulation of serum CXCL4L1 predicts progression and poor prognosis in prostate cancer patients treated by radical prostatectomy. Asian J Androl. 2019;21(4):387–392. doi:10.4103/aja.aja_117_18
11. Struyf S, Burdick MD, Peeters E, et al. Platelet factor-4 variant chemokine CXCL4L1 inhibits melanoma and lung carcinoma growth and metastasis by preventing angiogenesis. Cancer Res. 2007;67(12):5940–5948. doi:10.1158/0008-5472.CAN-06-4682
12. Eggert JA, Palavanzadeh M, Blanton A. Screening and early detection of lung cancer. Semin Oncol Nurs. 2017;33(2):129–140. doi:10.1016/j.soncn.2017.03.001
13. Nanavaty P, Alvarez MS, Alberts WM. Lung cancer screening: advantages, controversies, and applications. Cancer Control. 2014;21(1):9–14. doi:10.1177/107327481402100102
14. Snowsill T, Yang H, Griffin E, et al. Low-dose computed tomography for lung cancer screening in high-risk populations: a systematic review and economic evaluation. Health Technol Assess. 2018;22(69):1–276. doi:10.3310/hta22690
15. Verbeke H, De Hertogh G, Li S, et al. Expression of angiostatic platelet factor-4var/CXCL4L1 counterbalances angiogenic impulses of vascular endothelial growth factor, interleukin-8/CXCL8, and stromal cell-derived factor 1/CXCL12 in esophageal and colorectal cancer. Hum Pathol. 2010;41(7):990–1001. doi:10.1016/j.humpath.2009.09.021
16. Furuya M, Tanaka R, Miyagi E, et al. Impaired CXCL4 expression in tumor-associated macrophages (TAMs) of ovarian cancers arising in endometriosis. Cancer Biol Ther. 2012;13(8):671–680. doi:10.4161/cbt.20084
17. Quemener C, Baud J, Boyé K, et al. Dual roles for CXCL4 chemokines and CXCR3 in angiogenesis and invasion of pancreatic cancer. Cancer Res. 2016;76(22):6507–6519. doi:10.1158/0008-5472.CAN-15-2864
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.