Back to Journals » Advances in Medical Education and Practice » Volume 12
Curriculum Mapping and Alignment of the Neuroscience Block in an Undergraduate Medical Education Program: A Delphi Study
Authors Al Dera H ![]()
Received 28 May 2020
Accepted for publication 21 December 2020
Published 31 May 2021 Volume 2021:12 Pages 567—575
DOI https://doi.org/10.2147/AMEP.S263915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Hussain Al Dera1,2
1Department of Basic Medical Sciences, College of Medicine, King Saud Abdulaziz University for Health Sciences (KSAU-HS), Riyadh, Kingdom of Saudi Arabia; 2King Abdullah International Medical Research Center (KAIMRC), Riyadh, Kingdom of Saudi Arabia
Correspondence: Hussain Al Dera Email [email protected]
Background: Curriculum mapping and alignment are complex processes essential for the improvement of curriculum and serve as guidelines for students, faculty, and college administrators. This project aims to map different components of the curriculum in a comprehensive manner to ensure smooth running of the curriculum for the end users.
Materials and Methods: The project addressed the neuroscience block of the undergraduate medicine program. Eight parameters were investigated: competencies (learning outcomes), curriculum themes, block objectives, weekly problems, and objectives of weekly problems, disciplines, delivery, and assessment. The Delphi method was used by ten experts to assess the importance of these parameters. Focus interviews were then conducted with faculty members.
Results: The panel of ten experts reached consensus by agreeing that the eight parameters are important for aligning and mapping the neuroscience block and can be helpful for smooth operation of the curriculum. Mapping and alignment were performed electronically using eight parameters over 8 weeks. Majority of the faculty members appreciated the use of curriculum mapping.
Conclusion: Curriculum mapping using electronic software helps in identifying gaps and redundancies and facilitating alignment between learning and assessment and learning objectives and competencies (learning outcomes). Training programs for faculty members and encouragement from leaders are suggested.
Keywords: curriculum alignment, curriculum mapping, neuroscience block, electronic mapping, Delphi method
Introduction
The development of all aspects of education has continued worldwide, and with increased demands from professionals in various fields, it is necessary to develop high-quality graduates who would fulfill their respective roles. In relation to the field of medicine, the need for high-quality professionals who successfully complete their undergraduate studies has led to a review of the undergraduate curriculum. This makes curriculum mapping an important process for ensuring that the quality attained is established as per international standards.1 As there is constant progression and innovation in the fields of medicine and healthcare, graduates who complete their studies must remain abreast of the various advances to guarantee that they will be able to address the various issues they may encounter in their professional domains.
The main purpose of conducting curriculum mapping is to identify components and then assess how different elements work together to ensure that individuals are competent and better equipped as professionals when they complete their education.2 Mapping is more focused on components such as teaching methods; content; learning materials and resources; learning set-up and surroundings; teaching techniques; and various methods of assessment. Comprehensive mapping facilitates the smooth delivery of the curriculum and identifies areas that need to be addressed, in addition to enabling various components of the curriculum to function together.3 Moreover, mapping plays an important role in constructing a comprehensive assessment blueprint based on various parameters such as learning objectives and outcomes, ensuring that the material to be used in the curriculum remains relevant. In summary, the mapping process aims toward reviewing the contents, recording the content and skills actually delivered, and identifying the redundancies in the curriculum.4
Curriculum mapping links alignments to benchmarks and standards in higher education, which are achieved through assessments and evaluations.5 A focus on the standards setting in the curriculum is imperative to understand the concept of social accountability in medical institutions. The alignment process combines curriculum, instructional methods, resources, and the assessments with the standards.6
In the past, mapping has not been given much consideration in the curriculum. For instance, at the Association for Medical Education in Europe (AMEE), only three concepts have been presented on curriculum mapping. According to the information provided by different authors concerning curriculum, much work is needed, especially in terms of the vital parameters required to perform a comprehensive mapping and alignment in health science curricula. Among the completed mappings, very few have focused on medical education. The importance of mapping is reflected in its visibility to all the involved parties or stakeholders.7 For instance, connections or links among various parts of the curriculum, such as learning outcomes, learning assessments, and content can be observed when technology is employed in the mapping process.
The College of Medicine (COM) initiated the curriculum alignment project in 2018 to serve as a good example of a quality initiative. In this project, a software was developed to align eight curriculum parameters with each other. These parameters include competencies/program learning outcomes, curriculum delivery, instructional methods, course learning outcomes, specific objectives, weekly problems, and assessments. The aligned parameters are utilized for many purposes, including curriculum mapping and the blue printing assessment. This program identifies gaps and redundancies in the curriculum and ensures proper integration of all program learning outcomes. This way, not only is the coverage of competencies/program learning outcomes identified, but the weight of each outcome in the whole curriculum is precisely ascertained.
Depending on the type of curriculum, different starting points, such as learning outcomes and objectives, can be initiated and designed. This report provides an account of our experience of using a method, which is currently regarded as the most comprehensive mapping comprising of eight parameters. To achieve set deliverables such as assessment blueprints, a program was designed to ensure that the various parts of the curriculum functioned as desired.
The study objective was to assess important parameters for curriculum alignment and the coverage of different competencies and other parameters in the curriculum of the neuroscience block by implementing the actual alignments. The perceptions of the faculty members on effectiveness and associated challenges related to curriculum alignment were assessed.
Methods
The project was conducted in the neuroscience block of the Public Sector COM, Saudi Arabia. The project was conducted by using a hybrid problem-based integrated version of the organ system curriculum. The medicine program was delivering the Sydney curriculum, which was adopted at its inception. A curriculum reform for Phase II was proposed, and the Curriculum Alignment Committee was given the task of aligning the curriculum with delivery and outcomes based on the suggestions given by the faculty members, students, and experts. In the pilot phase, a neuroscience block was chosen as a model block for curriculum mapping and alignment. Curriculum mapping software was designed to align all the parameters and access to keep a record of students’ progress and ensure the quality of the course. The software was shared with all the neuroscience faculty members before the start of the block.
The neuroscience block is an 8-week course offered at the beginning of the second year of phase II (pre-clinical phase). In the pre-clinical phase, eight blocks are offered over two years, with each year having four blocks.
A modified Delphi technique was used to assess the importance of the eight parameters already utilized in the alignment from the curriculum experts: competencies (Saudi medical standards), Canadian medical standards (CAN-Med), domain, learning outcomes, objectives of weekly problems, disciplines, mode of delivery, and assessment types. The eight parameters were chosen from different sources, including the assessment unit, academic affairs, online curriculum website, and Department of Medical Education, and validated by medical education experts. Similar to our study, Smith and Simpson8 also used the Delphi method to develop and validate a framework of teaching competencies in higher education.
The Delphi technique has several advantages that make it useful. First, it is an efficient technique to obtain information from experts and leaders in education to reach a consensus, for after each round, panelists are confronted with their own ratings compared to the mean score and standard deviation of each item. Furthermore, the bias of dominant views within group discussions is avoided, as members can individually consider the competencies of professionalism they find important. Finally, when compared to the other techniques, it can be used to analyze the required competencies. Most importantly, it calls for free expression due to its policy of anonymity.9
Studies used multiple rounds of the Delphi technique to collect the experts’ opinions.9,10 In the first round, the experts responded to open-ended questions. In the second round, the collected data were presented back to the experts for refinement, review, and to ascertain consensus in the later rounds.10,11
This study comprises two phases. The first phase focuses on the Delphi project, and the second phase shares the perception of faculty members on the use of electronic curriculum mapping, effectiveness of parameters in neuroscience blocks, and future use. The Delphi project study was conducted in two rounds, given that participants were busy senior medical educators. In round one, which was a brainstorming round of various stakeholders from different disciplines, specialties, and academic rank, particularly from the COM, the stakeholders were asked for their opinions on the curriculum alignment process, benefits, and associated parameters they considered important in aligning a medical curriculum. As part of this technique, an open-ended questionnaire was administered to a panel of experts comprising of medical educators until a consensus or stability in the panel members’ responses was reached. Experts’ opinions were reviewed and endorsed by two senior medical educationists. A list of parameters of curriculum mapping was then assessed in round 2.
In the second round, a panel of ten experts who met the inclusion criteria was chosen. The inclusion criteria specified that all experts must be certified in medical education (diploma, masters, or PhD), participate in medical teaching, and be involved in curriculum mapping at some stage of their profession (Figure 1). All selected experts were from the respondent group from the first round. A questionnaire was designed on the parameters of alignment and then sent electronically and anonymously to all ten experts for their feedback. Each expert rated the eight parameters listed in the questionnaire, using a five-point Likert scale, as very important, important, neutral, not important, and not important at all. The responses were used to determine the level of importance of each parameter after consensus and presented as frequency and percentages.
 |
Figure 1 (A) shows phase 1, the three rounds of the Delphi method used to reach expert consensus on the importance of the eight parameters and (B) shows phase 2, the interviews of the faculty members and the thematic analysis. |
Concerning the satisfaction of faculty members with parameters and curriculum mapping of neuroscience blocks and software, each full-time faculty member (five males and three females) involved in the teaching of the neuroscience block were invited to express their perceptions of the construction of courses based on the eight parameters, making them visible in the alignment mapping tool. They were divided into two focus groups. Only those who were involved in neuroscience teaching over the last three years and who had attended training workshops on curriculum mapping—one with local faculty and one conducted by international faculty—were included. Semi-structured interviews were administered, and a purposeful sampling technique was used. The interview process was largely based on the queries that involved an interaction between the interviewer and interviewees. After obtaining permission from the participants, the interviews were recorded and transcribed (verbatim) immediately by the two independent transcribers to avoid any inaccuracies in the transcription. The interviews continued for an approximate fifty minutes to one hour.
This study was approved by the Institutional Review Board of the King Abdullah International Medical Research Center. The ethical approval number is IRB: SP18/441/R. Informed consent was obtained from all participants (including their anonymous responses), and the confidentiality of results was assured.
Results
The members of the panel belonged to COM and had different academic ranks. Among them, two were lecturers, four assistant professors, three associate professors, and one was a professor (Table 1), who had earned certificates in medical education (diploma, masters, or PhD). Most of them (nine) had worked in the medical education department and had experience in undergraduate medical curriculum alignment prior to joining the COM.
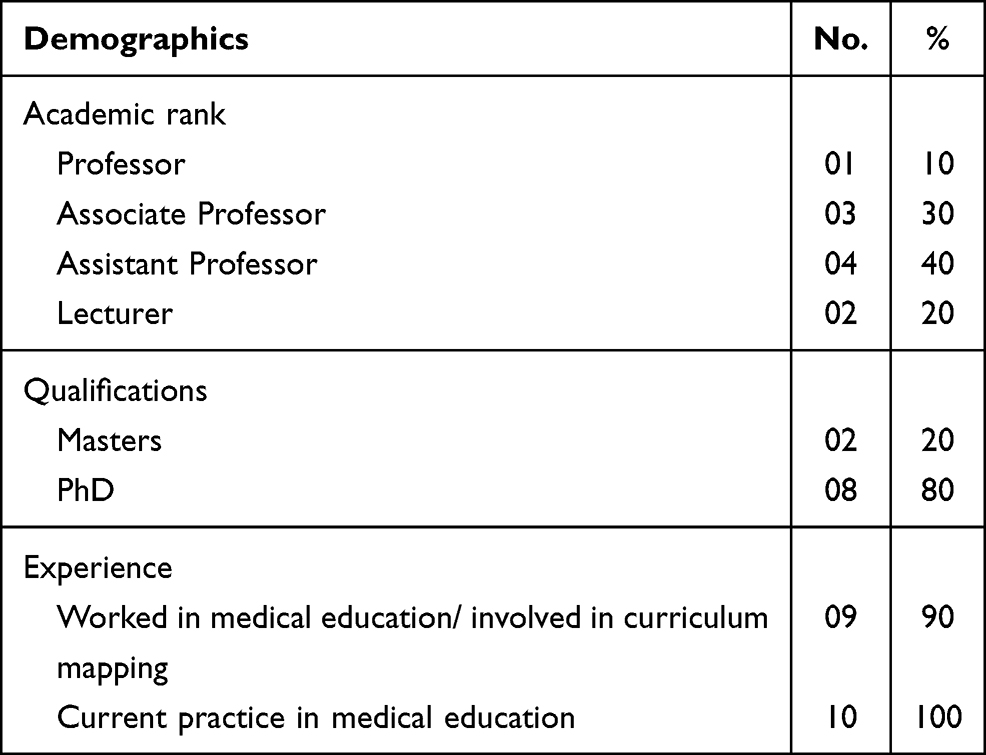 |
Table 1 Important Characteristics of the Panel of Experts Who Participated in the Study |
In the first round, members of the panel of experts reached consensus when rating all eight parameters (competencies, Canadian medical standards, domain, learning outcomes, weekly problems’ objectives, disciplines, mode of delivery, and assessment types) to be utilized in the alignment of the neuroscience block either as important or very important (Table 2). In the second Delphi round, the questionnaire was sent to each member with a request for more parameters when aligning the neuroscience curriculum. However, none of the members suggested any parameters to be added to the list.
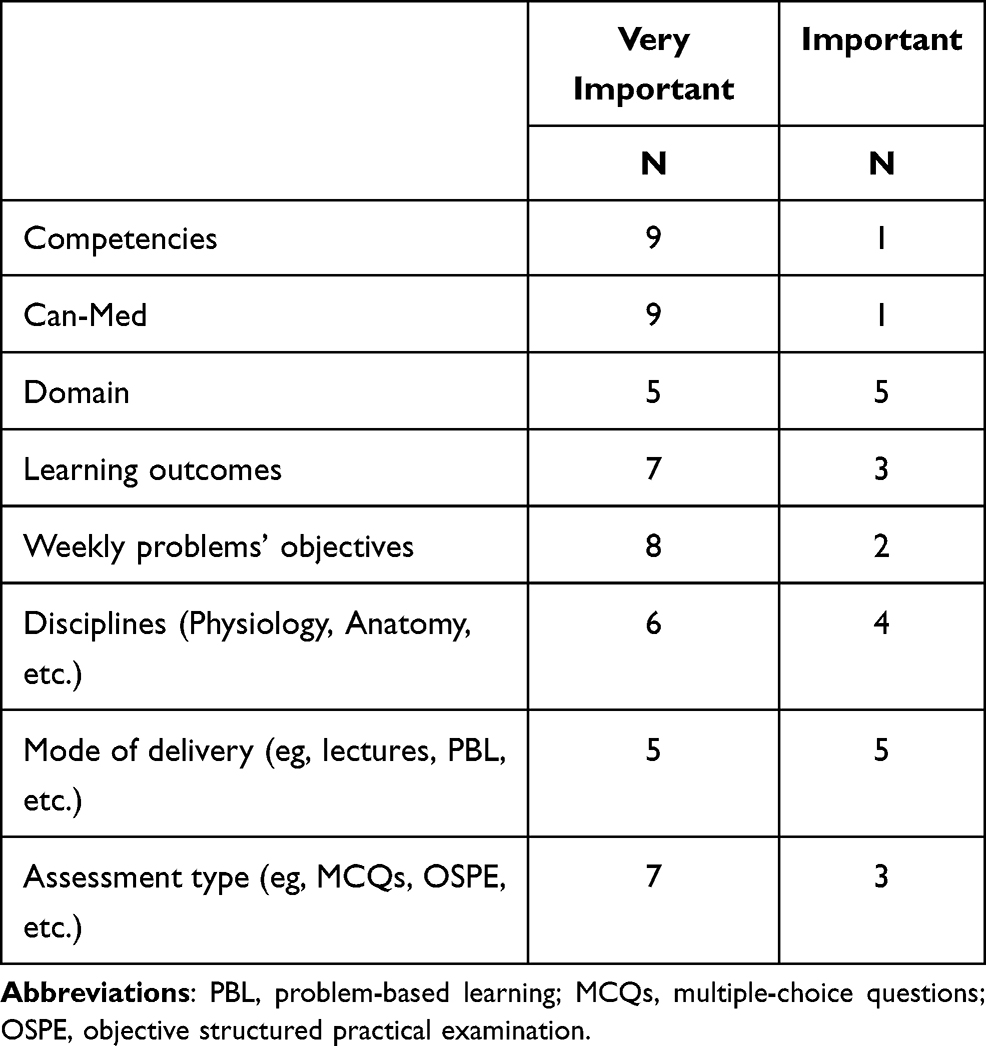 |
Table 2 List of Eight Parameters to Be Used in Neuroscience Curriculum Mapping and Alignment |
Once the panel had arrived at a complete consensus, the alignment process using the above-mentioned list of eight parameters was performed. Hence, all educational activities, including lectures, problem-based learning, and practical and communication skills, were aligned utilizing the eight parameters. The alignment process was performed session by session daily for the whole neuroscience block. Notably, the alignment report and output that illustrates the aligned outcomes for each parameter. For instance, by the end of the block, it should be clear how many learning objectives had been met under each domain and how many weekly objectives had been delivered. It also showed the number of times the domain was represented in the neuroscience block. Furthermore, the type of assessment that served to better achieve these objectives and competencies was reported.
In the third round, the faculty members’ evaluations of the neuroscience block post-alignment indicated satisfaction with the block objectives, delivery, and assessment methods (as shown in Table 2). Three themes were derived from the focus group interview pertaining to curriculum mapping: general knowledge, positive impact, and challenges.
Theme 1: General Knowledge of Curriculum Mapping
Most of the faculty members had prior knowledge of curriculum mapping through workshops and seminars conducted in college. Most of the participants observed that the content in the neuroscience curriculum overlapped and that the topics in the course sequence were repetitive.
There is a dire need to align the course content with the objectives and assessment, and we have to review student evaluations to improve the course.
In general, faculty members agreed that mapping the curriculum was urgent, essential, and advantageous in improving curriculum and performance assessment. However, although their perceptions of the effect of mapping on better understanding helped them to determine gaps in the curriculum, improvement in faculty teaching was not significantly approved by most faculty members. The only point they agreed on was the alignment of course objectives with teaching strategies and assessment methods, which would have to be changed or removed if they could not be mapped effectively.
Whatever knowledge and skills we teach in lecture(s) always help students in their clinical phase and with their practice. After mapping the eight parameters, we did not change much, but yes, we stressed when a course did fit in the curriculum map. If not, we recommended that the content be changed by the faculty immediately to avoid any misunderstanding.
Theme 2: Positive Impact of Curriculum Mapping
Most interviewees had positive perceptions of curriculum mapping. According to them, it is an effective tool for eliminating course gaps and repetition, matching courses to the standards laid out by the university and educational bodies, and helping set up instructional goals aligned with industry requirements.
This mapping helped me focus on the material relevant to students’ learning and help them in a way that leads toward their targets.
Curriculum mapping ensured that all students received the same level of education, and helped them master the associated skills. One of the interviewees said,
With mapping, the teacher knows what students read, what they must learn, what mastery level they have achieved, and how this knowledge and mastery of skill was assessed. These eight parameters in the curriculum map made the purpose and methods of teaching this course very clear.
Most of the interviewees agreed that clear curriculum maps of the eight parameters provided guidelines that allowed the faculty to design and develop methods to achieve course objectives and provide information to parents and stakeholders about how goals were achieved. They opined that sharing information improved teamwork.
It helped me in determining the structure and steps suitable for covering the course objectives and gave me an opportunity to discuss my students’ progress with their parents and other colleagues. This discussion enhanced teamwork and collegiality among faculty members in the neuroscience block.
Previously, there was repetition of content, redundancy, and inconsistency in teaching methods. These parameters allowed me to become aware of how and what I should teach that would fit into the curriculum as a whole.
Five of the eight participants reported a positive association between curriculum mapping and students’ academic performance after the curriculum was aligned:
Although there were many challenges with the curriculum maps, they had a positive effect, and the assessment results showed a significant improvement in students’ grade point average. Moreover, their end of block evaluations was more positive with respect to process, the comprehensive nature of the course, and assessment methods.
Theme 3: Challenges of Curriculum Mapping
The participants perceived many challenges in terms of curriculum mapping. The most important aspect was faculty members’ acceptance of curriculum mapping implementation in the block. They discussed that many instructors were not informed about curriculum mapping by the college administration or curriculum committee, so most were unaware of the benefits and relevance of curriculum alignment. This lack of information sharing had a negative effect. The instructors were not part of the curriculum mapping decision-making process, which may have hindered their acceptance of the alignment. One of the interviewees debated:
The chief coordinator simply informed us and did not ask for our opinions regarding the implementation, or our readiness for the curriculum.
A few teachers did not feel the need for curriculum mapping, so to achieve the instructional goals, approval from everyone in the neuroscience block regarding the inclusion of the eight parameters was imperative.
Another stated challenge was the lack of training and how to effectively use mapping in teaching. One participant argued,
Everyone perceives a map differently, so training by experts on the curriculum committee should be offered to teachers on an ongoing basis. The purpose should be to monitor whether all the parameters have been fully addressed and achieved.
Another participant discussed the following:
As the faculty had previously been working individually, and everyone had their own instructional and assessment methods, professional training and ongoing discussions would help with collaboration and alignment, which is important for building a shared goal.
With electronic curriculum mapping, most of the faculty reported,
We, as faculty, were previously unfamiliar with the use of an electronic curriculum, so it was really difficult for us to understand. It should be made more visible, and the software should be easy to use.
Discussion
Curriculum mapping and alignment began as early as 1981. Gjerde 12 described this complex process as an evaluation approach to assess and analyze congruency among objectives, teaching methods, and assessment tools. Mapping is found to be a useful tool in recognizing the alignments of course outcomes and learning outcomes in the program both vertically and horizontally.13 The main benefits of this process include demonstrating the links and alignment of different parts of a curriculum and assisting with faculty development by identifying areas of improvement. Moreover, it ensures structured communication among all teaching staff, serves as an evaluation tool with which to update teaching material in the curriculum and standardize assessment methods.14 For successful implementation, a curriculum should be mapped and aligned in a timely manner prior to teaching students and should be updated periodically. With advances in technology, electronic curriculum mapping and alignment are now widely used.15 The authors produced an electronic mapping program that identified relationships among certain parameters and whether they could ensure the delivery of competencies and learning outcomes to students. This facilitated the generation of a blueprint and a final report of links among all the parameters. This process allows educationists to identify any gaps and present the differences between the intended learning outcomes and the delivered curriculum. As 65% of medical schools use computer-based instruction and 37% use computer-based evaluation, modern technology has been widely used.16
In this study, the consensus of the educational experts proved the significance of several parameters in performing the mapping and alignment of the neuroscience block. The findings of this study are consistent with several reports in the literature. Mazurat and Schönwetter17 confirmed that mapping must be related to competencies. Their study was conducted on the mapping of learning objectives and their correlation with teaching methods in the occupational and environmental medicine curriculum. This was uploaded to a web-based program.17 Additionally, this study fulfilled the recommendations of the National Qualification Framework for higher education in Saudi Arabia,18 since all the assessment types consider the appropriate types of assessments to be used in the learning process in different domains.19 A study conducted by Ketteridge and Marshall20 also aligned related objectives and learning styles to specific disciplines and types of assessments.
A qualitative analysis of the effectiveness and challenges encountered by faculty during teaching showed that most appreciated the curriculum alignment based on the eight parameters. The results were similar to those of a study that reported the positive attitude of the faculty toward curriculum mapping.21
While most of the faculty members agreed that the eight parameters were relevant to better alignment, a few disagreed for a variety of reasons, including a poor understanding of parameter concepts that were new to them, the lack of active participation in the process, and, most importantly, no specific training in the eight parameters. There may be other concerns that this study did not identify, which would be of interest for future studies. Previous studies have identified concerns similar to the present study: multiple factors, including time demands, loss of control over the curriculum, and inconsistent assessment requirements were the cause of resistance to curriculum mapping and assessment processes.22–25
A commonly cited concern of faculty members was their professional development and lack of active participation in the mapping process. This highlights the urgent need for extensive training programs to improve faculty participation in the process and motivate reluctant teachers. Concerning the importance of involvement, it is necessary to involve all active neuroscience faculty members to correct curriculum redundancies and resolve the issues students may face while applying course concepts, which may increase the applicability of the parameters. One study suggested that once reluctant teachers accept the concept of curriculum mapping, they strongly favor the idea.26 Despite these challenges, most faculty appreciated the eight parameters included in the curriculum mapping. The most cited example was that mapping helped faculty significantly with the process of curriculum delivery and evaluation. This advantage is stated in previous literature,27–29 which reflected the transparency and availability of curriculum objectives.
In the future, the results of this study will help medical schools working on curriculum mapping in the development process, collaboration of different stakeholders, and efficacy of mapping by developing curriculum mapping software. It is recommended that leadership should encourage faculty members in their efforts and promote active participation in the mapping process and implementation. Further longitudinal studies on effective methods of implementation and review are needed.
Limitations
There are several limitations to this study. First, the parameters were aligned in one block and responses were collected from neuroscience faculty. Therefore, it is recommended that curriculum mapping is performed for other blocks. Second, the validity issue is associated with the Delphi approach. Although, in order to validate the results, a qualitative method was used in this study to obtain faculty perceptions regarding mapping and alignment, triangulation through the use of another research approach with the Delphi method may improve the validity.
Nevertheless, the current research provides information that may be useful for academic institutions and health professionals working on curriculum mapping and alignment of standards related to teaching and learning.
Conclusion
The Delphi method is an appropriate method to study newly-introduced phenomena in any institution of higher learning. It proved that all eight parameters are important and should be utilized to map and align the neuroscience block. This study provided a clear mapping and alignment of each component of the neuroscience block in terms of instructional activities, weekly learning objectives, domains, competencies, intended learning outcomes, and assessment tools. Furthermore, the mapping and alignment processes employed in this study may help meet the requirements of the National Quality Framework.
Acknowledgments
The author would like to acknowledge Mohi Eldin Magzoub, professor of medical education, former chairman of the Medical Education Department, for his support and advice in completing this work. Special thanks also go to Sajida Agha, associate professor of medical education and coordinator of the Faculty Enhancement Unit, COM, for her role in facilitating the focus group interviews . Hussain Al Dera. BSc (rehab), MCSc, MSc, PhD, is a physiologist and associate professor of clinical physiology. He has another master’s degree in medical education.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Britton M, Letassy N, Medina MS, Er N. A curriculum review and mapping process supported by an electronic database system. Am J Pharm Educ. 2008;72:5. doi:10.5688/aj720599
2. Harden RM. AMEE guide no. 21: curriculum mapping: a tool for transparent and authentic teaching and learning. Med Teach. 2001;23(2):123–137. doi:10.1080/01421590120036547
3. Plaza CM, Draugalis JR, Slack MK, Skrepnek GH, Sauer KA. Curriculum mapping in program assessment and evaluation. Am J Pharm Educ. 2007;71(2):20. doi:10.5688/aj710220
4. Jacobs HH. Mapping the Big Picture: Integrating Curriculum and Assessment K-12. Alexandria, VA: Association for Supervision and Curriculum Development; 1997.
5. English FW. Deciding What to Teach and Test: Developing, Aligning, and Auditing the Curriculum. Thousand Oaks, CA: Corwin Press; 2000.
6. Carr JF, Harris DE. Succeeding with Standards: Linking Curriculum, Assessment, and Action Planning. Alexandria, VA: Association for Supervision and Curriculum Development; 2001.
7. Irby DM, Wilkerson L. Educational innovations in academic medicine and environmental trends. J Gen Intern Med. 2003;18(5):370–376. doi:10.1046/j.1525-1497.2003.21049.x
8. Smith KS, Simpson RD. Validating teaching competencies for faculty members in higher education: a national study using the Delphi method. Innov High Educ. 1995;19(3):223–234. doi:10.1007/BF01191221
9. Powell C. The Delphi technique: myths and realities. J Adv Nurs. 2003;41(4):376–382. doi:10.1046/j.1365-2648.2003.02537.x
10. Hsu C, Sandford B. The Delphi technique: making sense of consensus. Pract Assess Res Eval. 2007;12(10):1–8.
11. Williams PL, Webb C. The Delphi technique: a methodological discussion. J Adv Nurs. 1994;19(1):180–186. doi:10.1111/j.1365-2648.1994.tb01066.x
12. Gjerde CL. “Curriculum mapping”: objectives, instruction, and evaluation. Med Educ. 1981;56(4):316–323.
13. Jacobs HH. Getting Results with Curriculum Mapping. Alexandria, VA: Association for Supervision and Curriculum Development; 2004.
14. Rodríguez-Revelo N. Standardization in the educational curriculum: the tip of the homogenization iceberg. Revi Edu. 2017;12(2):248–258.
15. Wijngaards-de Meij L, Merx S. Improving curriculum alignment and achieving learning goals by making the curriculum visible. Int J Acad Dev. 2018;23(3):219–231. doi:10.1080/1360144X.2018.1462187
16. Tomesko J, Touger-Decker R, Dreker M, Zelig R, Parrott JS. The effectiveness of computer-assisted instruction to teach physical examination to students and trainees in the health sciences professions: a systematic review and meta-analysis. J Med Educ Curric Dev. 2017;4:2382120517720428. doi:10.1177/2382120517720428
17. Mazurat R, Schönwetter DJ. Electronic curriculum mapping: supporting competency-based dental education. J Can Dent Assoc. 2008;74(10):886–889.
18. AlMusallam, Abdullah. Accreditation and quality assurance in higher education in the Kingdom of Saudi Arabia. In: Secretary General, National Commission for Academic Accreditation & Assessment Roundtable meeting of QA. 2009:13–15..
19. Alfauzan AA, Tarchouna N. The role of an aligned curriculum design in the achievement of learning outcomes. J Educ eLearn Res. 2017;4(3):81–91. doi:10.20448/journal.509.2017.43.81.91
20. Marshall S, Fry H, Ketteridge S. A Handbook for Teaching and Learning in Higher Education: Enhancing Academic Practice. Routledge; 2014.
21. Shilling T. Opportunities and challenges of curriculum mapping implementation in one school setting: considerations for school leaders. JoCI. 2013;7(2):20–37. doi:10.3776/joci.2013.v7n2p20-37
22. Oliver B, Ferns S, Whelan B, Lilly L. Mapping the curriculum for quality enhancement: refining a tool and processes for the purpose of curriculum renewal.
23. Rahimi A, Borujeni SAM, Esfahani ARN, Liaghatdar MJ. Curriculum mapping: a strategy for effective participation of faculty members in curriculum development. Procedia Soc Behav Sci. 2010;9:2069–2073. doi:10.1016/j.sbspro.2010.12.448
24. Swanson DJ. Best Practices for Student Learning Assessment in Smaller-Sized Undergraduate Mass Communication Programs. San Fransicso, Calif: Association for Education in Journalism and Mass Communication; 2015.
25. Joyner HS. Curriculum mapping: a before-and-after look at faculty perceptions of their courses and the mapping process. J Food Sci Educ. 2016;15(2):63–69. doi:10.1111/1541-4329.12085
26. Lee MY, Albright SA, Alkasab T, Damassa DA, Wang PJ, Eaton EK. Tufts health sciences database: lessons, issues, and opportunities. Acad Med. 2003;78(3):254–264. doi:10.1097/00001888-200303000-00003
27. Watson EG, Moloney PJ, Toohey SM, et al. Development of eMed: a comprehensive, modular curriculum-management system. Acad Med. 2007;82(4):351–360. doi:10.1097/ACM.0b013e3180334d41
28. Jacobs J, Salas A, Cameron T, Naguwa G, Kasuya R. Implementing an online curriculum management database in a problem-based learning curriculum. Acad Med. 2005;80(9):840–846. doi:10.1097/00001888-200509000-00011
29. Cottrell S, Linger B, Shumway J. Using information contained in the curriculum management information tool (CurrMIT) to capture opportunities for student learning and development. Med Teach. 2004;26(5):423–427. doi:10.1080/0142159042000218650
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.