Back to Journals » Journal of Inflammation Research » Volume 15
Current Perspectives in ABO-Incompatible Kidney Transplant
Authors Maritati F ![]() , Bini C, Cuna V, Tondolo F, Lerario S, Grandinetti V
, Bini C, Cuna V, Tondolo F, Lerario S, Grandinetti V ![]() , Busutti M, Corradetti V, La Manna G
, Busutti M, Corradetti V, La Manna G ![]() , Comai G
, Comai G
Received 29 January 2022
Accepted for publication 17 March 2022
Published 25 May 2022 Volume 2022:15 Pages 3095—3103
DOI https://doi.org/10.2147/JIR.S360460
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam Bachstetter
Federica Maritati, Claudia Bini, Vania Cuna, Francesco Tondolo, Sarah Lerario, Valeria Grandinetti, Marco Busutti, Valeria Corradetti, Gaetano La Manna, Giorgia Comai
Nephrology, Dialysis and Renal Transplant Unit, IRCCS-Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy
Correspondence: Gaetano La Manna, Nephrology, Dialysis and Renal Transplant Unit, IRCCS-Azienda Ospedaliero-Universitaria di Bologna, Via Giuseppe Massarenti, 13, Bologna, 40138, Italy, Tel +39-051-2142584, Fax +39-051-2142509, Email [email protected]
Abstract: For a long time, ABO incompatible living donor kidney transplantation has been considered contraindicated, due to the presence of isohemagglutinins, natural antibodies reacting with non-self ABO antigens. However, as the demand for kidney transplantation is constantly growing, methods to expand the donor pool have become increasingly important. Thus, in the last decades, specific desensitization strategies for ABOi transplantation have been developed. Nowadays, these regimens consist of transient removal of preformed anti-A or anti-B antibodies by using plasmapheresis or immunoadsorption and B-cell immunity modulation by CD20+ cells depletion with rituximab, in association with maintenance immunosuppression including corticosteroids, tacrolimus and mycophenolate mofetil. The outcome in ABOi kidney transplantation have markedly improved over the years. In fact, although randomized trials are still lacking, recent meta analysis has revealed that there is no difference in terms of graft and patient’s survival between ABOi and ABO compatible kidney transplant, even in the long term. However, many concerns still exist, because ABOi kidney transplantation is associated with an increased risk of bleeding and infectious complications, partly related to the effects of extracorporeal treatments and the strong immunosuppression. Thus, a continuous improvement in desensitization strategies, with the aim of minimize the immunosuppressive burden, on the basis of immune pathogenesis, antibodies titers and/or ABO blood group, is warranted. In this review, we discuss the main immune mechanisms involved in ABOi kidney transplantation, the pathogenesis of tolerance and the desensitization regimens, including immunoadsorption and plasmapheresis and the immunosuppressive protocol. Finally, we provide an overview on outcome and future perspectives in ABOi kidney transplant.
Keywords: ABO incompatible kidney transplant, blood group, plasma exchange, rituximab
Introduction
Kidney transplantation provides a considerable survival advantage compared to hemodialysis in patients with end-stage kidney disease. Thus, the organ demand is continuously growing while a considerable gap exists between organ availability and waiting listed patients, although the pool of deceased donors has been successfully expanded with donation after circulatory death or kidneys from extended criteria donors.1,2 In fact, in 2020 in Italy, of the 8310 patients listed in the deceased-donor waiting list, only 1623 underwent kidney transplant, with a mean waiting time of 40 months.3
Kidney transplant from living donor offers a superior survival of both patient and graft than transplant from deceased donation and is the most effective way to expand the donor pool.4 However, immunologic barriers frequently pose limitations to this transplant. These barriers are mainly represented by preformed anti-human leukocyte antigen (HLA) antibodies and ABO system antibodies, which can cause hyperacute rejection.5,6
For a long time, ABO incompatible (ABOi) living donor kidney transplantation was contraindicated, due to its immunological impediment based on the presence of isohemagglutinins, natural antibodies reacting with non-self ABO antigens.7 Nevertheless, in 1987, Alexandre et al reported the first results of their pioneering program of ABOi living donor kidney transplantation. They laid the basis for the recipient preconditioning, commonly termed desensitization, a combination of treatments and procedures aiming at reducing isohemagglutinins levels.8
Nowadays, preconditioning consists in the combination of immunosuppressive agents, administered before transplantation (ie, rituximab) to prevent the production of new antibodies, apheresis techniques and maintenance immunosuppressants.9 No consistent data regarding the non-inferiority or superiority of individual regimens are currently available, due to the paucity of randomized controlled trials.
Outcomes in ABOi kidney transplantation have markedly improved over the years. Recently, a meta-analysis including 21 studies reporting the outcome of ABOi kidney transplant by comparing ABO compatible (ABOc) has revealed that there is no difference in terms of graft failure, biopsy-proven acute rejection and patient survival.9 In their consistent series including 62 ABOi kidney transplant, Barnett et al reported a three-year graft survival of 98.4%, a T-cell mediated rejection rate of 27.4% and an antibody mediated rejection rate of 4.8% at one-year post transplant. No statistically significant differences were found between the ABOi group and the group of ABOc kidney transplant performed in the same time period and in the same Transplant Center.10
The aim of this review is to summarize the principal aspects of ABOi kidney transplantation and the techniques and strategies used to treat recipients to overcome the isohemagglutinin barrier.
The ABO System
The ABO system is based on the expression of genetically determined A, B and H blood group antigens on the surface of different cell types, including red blood cells (RBCs), endothelial cells and kidney parenchymal cells.11 Blood group O is determined by the antigen H, an oligosaccharide produced by the enzyme α-1,2-fucosyltransferase which is able to add a fucose molecule on a core-chain.12 The antigen H serves as a matrix for the A and B antigens by a terminal α-d-galactose residue, which consists of a carbohydrate backbone bound to glycolipids or proteins. In individuals with A blood group, the terminal α-d-galactose residue is modified by the enzyme α-1,3-n-acetylgalactosaminyltransferase (A transferase), which attaches β-n-acetylgalactosamine, leading to the expression of A antigen. In individuals with B blood group the α-1,3-galactosyltransferase (B transferase), modifies the α-d-galactose residue of antigen H, by attaching α-d-galactose, leading to the expression of B antigen. Subjects who co-dominantly express the genes of the human ABO system have AB blood group because are able to produce both A and B transferases. Conversely, O group individuals do not have detectable A or B transferase activity and their H antigen remains unmodified. Blood group A consists of two subtypes, A1 and A2 (or, more appropriately, not-A1 subtype).13 The A1 subtype is more frequent, including about the 80% of individuals with A blood group. The quantitative or qualitative expression of ABO antigens may vary substantially between individuals. Individuals with A1 and A2 subtypes differ considerably with respect to the A antigen expression. Subjects with A2 subtypes express a small amount of A antigen and/or have a low A transferase activity.14 For these reasons, their immunological risk associated to ABO incompatibility in kidney transplant is significantly low.15–17
The Isohaemagglutinins Barrier in ABO Incompatible Transplantation
The immunological barrier of ABOi kidney transplant is related to the presence of preformed isohaemagglutinins, that are natural antibodies with the intrinsic ability to agglutinate erythrocytes reacting against non-self ABO antigens.17 Isohaemagglutinins emerge in early childhood, increase their strength in the first decade of life and persist in adults.18 They are probably induced upon contact with the cell membrane polysaccharides of the gut commensal bacteria.19 In addition, the repertoire of antibodies towards ABO antigens may include autoantibodies against the terminal monosaccharide, disaccharide or trisaccharide residues of the “self” blood group or autoantibodies against the core chain. However, most of these autoantibodies have low-affinity and their clinical relevance is still unknown.20 Isohaemagglutinins consist of IgM, IgG and IgA, with levels and distribution pattern which have consistent variability between individuals. The pathogenic potential of anti-A/B reactivity patterns might markedly differ with regard to the distribution of IgG subclasses and antibody avidity.18 It depends on the quality of the B-cell response, particularly the relative contribution of B-1 cell versus B-2 cell driven immunity.21 CD5+ B-1 are a small population of long-lived, self-renewing B cells, which produce low avidity, polyreactive natural IgM. By contrast, the larger CD5– B-2 cell pool produces high-affinity antibodies, including complement-activating IgG isotypes, which typically arise after stimulation with non-self antigens.22,23 In a cytofluorimetric study evaluating B cell subsets in 10 ABOi kidney transplant patients, Ishida et al found an initial increase in CD5+ B-1 cell, which was accompanied by an increase in levels of IgG2 and IgM. Interestingly, those patients who experienced rejection showed a change in the B cell subset distribution towards an increase of CD5– B-2 cells and high levels of complement-fixing IgG1.24 The exact mechanism by which ABO antigens are able to induce B-1 and B-2 cell activation to produce and sustain high-affinity immunoglobulin responses remains unclear. Some evidences suggest that thymus-independent antigens with highly repetitive epitopes induce the production of IgM via B-cell-receptor crosslinking and can cause an isotype switch (Figure 1).25 Further mechanisms of antibodies production may include cytokine secretion by the B cells or T helper cells in response to the antigens,26 or by invariant natural killer T cells, activated by the recognition of the glycolipid compounds of the CD1d MHC-like molecule expressed on B-cells or dendritic cells surface.27,28
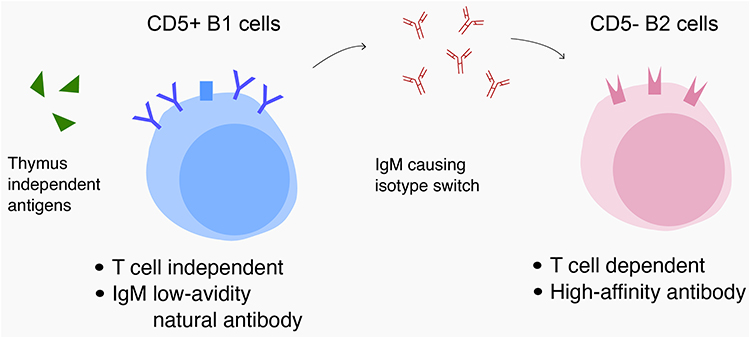 |
Figure 1 The possible pathogenetic mechanism of different B cell response in patients receiving AB0i kidney transplant. Thymus-independent antigens may cause the switch from B1 cells producing low avidity IgM to B2 cells able to produce high levels of complement-fixing IgG1, which can predispose to rejection. |
Mechanisms of Tolerance in ABOi Transplantation
In ABOi transplantation, preformed anti-A/B antibodies are responsible for a severe antibody-mediated rejection (ABMR) and in the worst cases, for a hyperacute rejection which lead to immediate renal allograft loss. Recipient desensitization allows the acceptance of ABOi graft both immediately after transplantation and in the long-term follow up even after the recurrence of detectable levels of isohemagglutinins.10,17 In ABOi transplantation, the presence of circulating antibodies against the graft (isohemagglutinins) activate the complement system resulting in C4d deposition along peritubular capillaries at kidney biopsy. However, differently from HLA-incompatible transplantation, in which persistent or recurrent donor-specific antibodies frequently leads to rejection and chronic tissue injury, in ABOi transplant this process does not cause graft damage. This phenomenon is called “accommodation”.29–31
The mechanisms of accommodation are still unclear. An analysis in vitro evaluating the effects of anti-A/B antibody binding on complement-mediated cytotoxicity and signal transduction, have revealed that anti-A/B antibodies increase the expression of complement regulatory proteins such as CD55 and CD59 and inactivate ERK1/2 pathway, contributing to this phenomenon.30 The upregulation of the complement regulatory proteins CD59 and CD46 and of the anti-apoptotic proteins Bcl-2 and clusterin has also been demonstrated in a pre-sensitized non-human primate study. Interestingly, in this study, the inhibition of complement activation with the Yunnan-cobra venom factor (Y-CVF) successfully prevented accelerated ABMR and facilitated accommodation.32 Other proposed mechanisms that potentially contribute to the acceptance of ABOi transplants include blood group chimerism or shift. In 2004, Koestner et al described the case of an O blood group patient who accidentally received a B blood group heart transplant. The patient survived for five years. The monitoring of the antigenic profile of the graft endothelial cells by immunohistology demonstrated that it changed progressively from B to O.33 In kidney transplantation has been suggested that endothelial chimerism related to immunological or non-immunological injury may also facilitate accommodation.34 The possible formation of a soluble A or B transferase inhibitor, able to reduce transferases activity, is another mechanism postulated to prevent isohemagglutinin injury in ABOi transplants.35 Based on the finding that isohemagglutinins titer remains low during the first months of life, West et al performed a trial including ABOi infant heart transplant recipients treated with standard immunosuppression without splenectomy. No cases of hyperacute or acute humoral rejection were demonstrated in this study.36 The same group reported in a subsequent study a persistent and selective deficiency of circulating antibodies to donor A and B antigens in the children followed up to eight years after heart transplantation. Authors speculated that these children have acquired a tolerance through the elimination of ABO-specific B cells. Interestingly, in children with ABOi heart transplantation has been shown a less frequency of donor-specific antibodies and class II antibodies, suggesting that the specific B-cell tolerance may be associated also with an altered response to HLA antigens.37
Antibodies Depletion Strategies and Results
The desensitization protocols for ABOi kidney transplantation are based on pre-existing anti-A/B isohemagglutinins removal by combining extracorporeal techniques with immunosuppressive therapy.
The key point for desensitization is currently based on apheresis techniques. Serial antibodies titers monitoring is used to tailor the need of adjunctive apheresis treatments after transplantation, in order to prevent the rebound in isohemagglutinins levels until tolerance or accommodation occur.17,38
The apheresis techniques can be either non-selective or selective. Plasma exchange (PEX) is a non-selective apheresis technique, in which the plasma is separated from the whole blood by centrifugation or filtration and then eliminated; the discharged plasma is replaced with albumin, colloid solutions or fresh frozen plasma. PEX has the important disadvantage of losses in coagulation factors, hormones, albumin, anti-bacterial and anti-viral immunoglobulins. For this reason, the total plasma volume that can be treated in each session is limited. Conversely, the advantage respect to more selective strategies, is that it can remove also other antibodies, such as anti-HLA antibodies, and complement components that may be implicated in the pathogenesis of allograft injury mediated by isohemagglutinins. Moreover, PEX is the less expensive and more widely and rapidly available apheresis technique.38,39
An alternative apheresis technique, the double-filtration plasmapheresis (DFPP), has been designed to selectively remove the immunoglobulin fraction from the serum and, as a result, to minimize the volume of substitution fluid required. In this method, plasma is firstly separated by a plasma separator and later it passes through a second filter (the plasma fractionator) which remove the gamma globulin fraction. Thus, the amount of immunoglobulin eliminated in one DFPP session is equivalent to that concentrated in 5 L of plasma, but only 1 L of substitution fluid is necessary to replace the plasma removed.40
The most selective apheresis technique is ABO-specific immunoadsorption (IA), in which the separated plasma pass through an antigen-specific absorber, consisting of blood group A or B antigens immobilized on a sepharose matrix, and then it is returned to the patient. This technique provides a highly efficient elimination of ABO antibodies without the loss of essential plasma components.17 It can also reduce complement components levels, which can contribute to prevent the antibody-mediated rejection related to isohemagglutinins, resulting in a high treatment efficiency. Biglarnia et al demonstrated a decline in complement components (C3a and C3a/C3 ratio) with the start of IA in 19 ABOi living donor kidney transplant and that these proteins were detected in the eluate. The binding of C3a could be explained by its high isoelectric point which may result in the affinity with the negative charged resin of the immunoadsorbent.41 The main disadvantage of this approach is represented by the high costs of the ABO-columns. However, in their prospective trial, Schiesser et al have demonstrated that the reuse after restoration of these columns does not reduce the antibody-depletion capability and has the same safety and tolerability profile, resulting in a consistent cost saving.42
There are no randomized controlled trials comparing PEX and IA techniques and the decision on which antibody depletion protocol to choose depends on physicians’ experience. PEX is the favorite preconditioning treatment in Transplant Centers from the USA and Japan. The John Hopkins Hospital and the Mayo Clinic use similar preconditioning methods. In the first group, as reported by Montgomery et al, the PEX treatment plan is based on anti-A and anti-B titers with the goal of achieving isohemoagglutins title of 1:16 or less before surgery. The number of PEX sessions before transplantation is estimated by the titers. Each PEX treatment consists of 1-plasma-volume exchange replaced at 100% volume with 5% serum albumin. PEX sessions are usually performed every other day. After each procedure, low-dose cytomegalovirus immunoglobulins intravenous are administered because of their immunomodulatory effect. After transplantation, all patients receive at least two PEX sessions; patients who have high starting titers, antibody rebound, or antibody mediated rejection undergo to further session.43,44 There is no general agreement about the sufficient lowering of antibody titer before kidney transplant. Some centers require anti-A/B IgG titers of less than or equal to 1:8, others require titer less than or equal to 1:32 at the time of transplantation. Actually, no randomized control studies are available in order to compare the outcome of higher versus lower titers in ABOi kidney transplant.
In the experience reported by Tyden et al, 60 consecutive ABOi kidney transplant were performed in Stockholm, Uppsala and Freiburg, using antigen-specific IA, rituximab, intravenous immunoglobulin and conventional tacrolimus, mycophenolate mofetil, and prednisolone immunosuppression as desensitization. The target preoperative isohemagglutinins titer was <1:8. Graft survival was 97% for the ABOi compared with 95% in the control group of 267 ABO-compatible living donor kidney transplant performed in the same period. No late rebound of antibodies or humoral rejections were observed.45
Montgomery et al reported of 60 ABOi kidney transplant which received the John Hopkins desensitization protocol with cytomegalovirus immunoglobulin, immunosuppression, splenectomy at the time of transplant (later replaced by a single-dose anti-CD20 administered the night before transplantation and, recently, both interventions have been stopped). Graft survival was comparable with the United Network for Organ Sharing data for compatible live donor transplants. There were no cases of hyperacute rejection or graft losses from acute mediated rejection (AMR). Ten patients experienced AMR (four were mixed, ABMR and cellular mediated rejection); no significant difference in starting (pre-treatment) isohemagglutinin titers were detected, but a rise in the post-operative titers, compared with no rejection patients.46
Outcomes in ABOi kidney transplantation have markedly improved over the years. Graft survival and patients’ safety is comparable to those in ABO-compatible kidney transplant.10,47–50 The main studies which compare the outcome of patients who underwent ABOi kidney transplant with patients who received ABOc kidney transplant have been reported in Table 1.
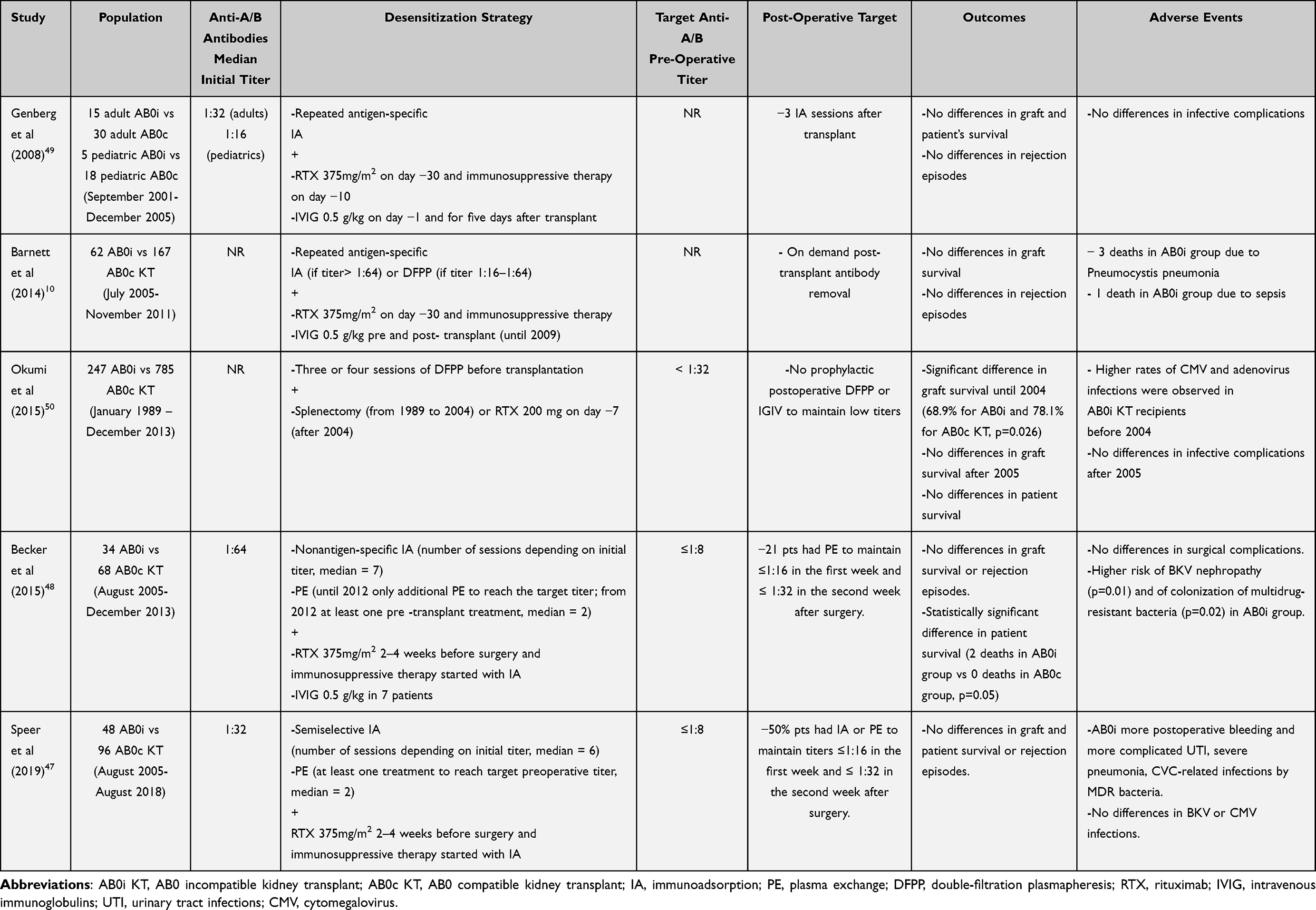 |
Table 1 Main Papers Comparing the Outcome of Patients Who Underwent ABOi Kidney Transplant with Patients Who Received ABOc Kidney Transplant |
Indeed, some reports show even a better renal function and a less incidence of chronic ABMR in patients with ABOi kidney transplant than patients receiving an ABO-compatible living transplant.51,52
Immunomodulation and Immunosuppressive Therapy
In the initial era of ABOi kidney transplantation the desensitization protocol included also splenectomy, because the spleen contains a large pool of antibody-secreting B cells. In the last decades, splenectomy has been replaced with a single dose of rituximab, an antibody anti-CD20.53,54 The effect of rituximab on blood-group-specific immunity is still incompletely understood. It is able to effectively deplete peripheral B cells, but it might not reduce B-cell counts in secondary lymphoid organs. However, rituximab may result also in a modulation of B cell and T cell immunity by the changes in the pattern of B-cell subpopulations, including a disappearance of transitional B cells and an increase in memory B cells in lymph nodes.55
Importantly, in ABOi kidney transplantation, excellent outcomes have been shown also for desensitization protocols that employ reduced rituximab dosages or even do not use rituximab.
Based on the recognition that accommodation occur rapidly after ABOi transplantation and AMR is relatively uncommon and usually experienced in the first two weeks after transplant, Montgomery et al eliminated both splenectomy and anti-CD20 therapy, in favor of a tight control of isohemagglutinin titers with PEX treatment during the window of graft major vulnerability.46 In their series including 60 ABOi transplant, they report that the recipient who did not receive rituximab or splenectomy had the same outcome in renal function than those who were treated with the conventional antibody depletion therapy.
In order to improve immunological outcome, desensitization protocols include induction with an IL-2 receptor antibody and maintenance immunosuppression with tacrolimus and mycophenolate mofetil (MMF) which is commonly initiated before transplantation. Retrospective studies have suggested a greater outcome with the use of these two immunosuppressive agents compared to ciclosporin-based regimens. Alternative immunosuppressive strategies have been proposed in few case series including a low number of patients. The conversion from MMF and standard-dose calcineurin inhibitors (CNIs) to everolimus and low-dose CNIs in a cohort of 16 stable ABOi kidney transplant recipients has been reported effective and safe.56
In Figure 2, we reported the desensitization strategy commonly performed in patients who undergo ABOi kidney transplant.
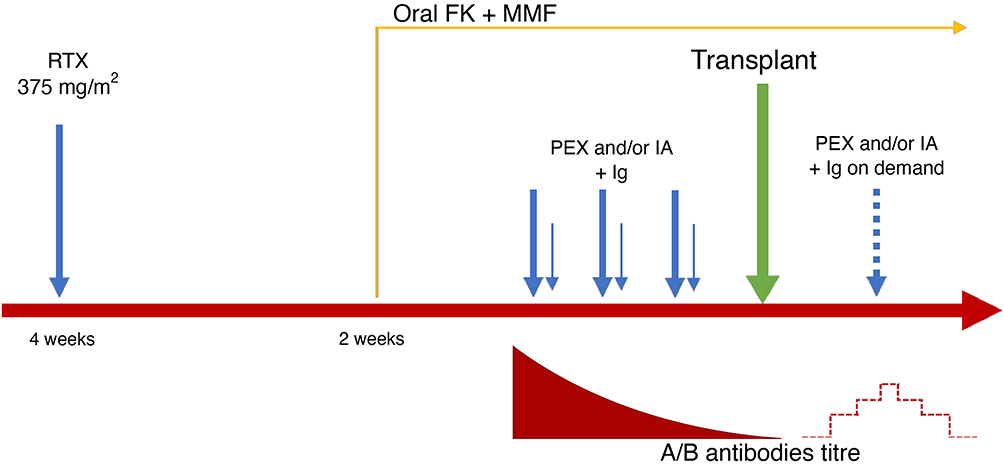 |
Figure 2 The desensitization strategy performed in ABOi kidney transplant patients. A single infusion of rituximab 375 mg/mq is administrated four weeks before kidney transplant. Two weeks before kidney transplant, patient starts oral immunosuppressive therapy (tacrolimus and mycophenolate mofetil). A variable number of immunoadsorption and/or plasma exchange (PEX) sessions is performed before kidney transplant, until a titer < or = at 1:8 is achieved. The isohemagglutinin titer is measured every day after ABOi kidney transplant and further PEX sessions are performed on demand. |
Future Perspectives and Conclusions
Many innovative strategies have been recently proposed in order to overcome immunological barriers in ABOi kidney transplant. Kobayashi et al have proposed the goal to reduce the blood group antigen expression in the kidney, by applying a recombinant endo-β-galactosidase (ABase) produced in E. coli BL-21. In vivo experiments performed in blood type A, baboons revealed a marked reduction of A antigen expression in the glomeruli.57 Another target could be the interference with the binding of anti-A/B antibodies to blood group antigens by using a monoclonal anti-A or B antibody Fab fragment or by neutralizing preformed antibody with an ABO blood group trisaccharide carbohydrate epitope.58,59 The terminal complement inhibitor eculizumab in the induction of ABOi transplantation has also been proposed, with the aim of interfering with the antibody-triggered complement activation induced by anti-A/B antibodies.60
However, it is crucial, in the management of ABOi kidney transplant, to be aware of the risks related to the high degree of immunosuppression. This is the topic which needs for further improvements. More data regarding the tailored approach based on pre-transplant isohemagglutinins titers and/or donor/recipient blood group are warrants. A better understanding of the underlying immunologic mechanisms of anti-A/B immune responses and ABOi graft tolerance will provide the basis for the development of new and safer desensitization strategies.
Funding
This study was supported by research fundings from the Italian Health Ministery.
Disclosure
The authors have no conflict of interest to declare.
References
1. Alexander JW, Zola JC. Expanding the donor pool: use of marginal donors for solid organ transplantation. Clin Transplant. 1996;10(1 Pt 1):1–19.
2. Ojo AO, Hanson JA, Meier-kriesche H-U, et al. Survival in recipients of marginal cadaveric donor kidneys compared with other recipients and wait-listed transplant candidates. J Am Soc Nephrol. 2001;12(3):589–597. doi:10.1681/ASN.V123589
3. Ministry of Health. Transplants. Italian and European data.Available from: http://www.trapianti.salute.gov.it/trapianti/archivioDatiCnt.jsp.
4. Henderson ML, Thomas AG, Shaffer A, et al. The national landscape of living kidney donor follow-up in the United States. Am J Transplant. 2017;17(12):3131–3140. doi:10.1111/ajt.14356
5. Stewart DE, Klassen DK. Kidney transplants from HLA-incompatible live donors and survival. N Engl J Med. 2016;375(3):287–288. doi:10.1056/NEJMc1604523
6. Starzl TE, Marchioro TL, Holmes JH, et al. Renal homografts in patients with major donor-recipient blood group incompatibilities. Surgery. 1964;55:195–200.
7. Cook DJ, Graver B, Terasaki PI. ABO incompatibility in cadaver donor kidney allografts. Transplant Proc. 1987;19(6):4549–4552.
8. Alexandre GP, Squifflet JP, De Bruyère M, et al. Present experiences in a series of 26 ABO-incompatible living donor renal allografts. Transplant Proc. 1987;19(6):4538–4542.
9. Lee HR, Kim K, Lee SW, et al. Effect of rituximab dose on induction therapy in ABO-incompatible living kidney transplantation: a network meta-analysis. Medicine. 2021;100(10):e24853. doi:10.1097/MD.0000000000024853
10. Barnett AN, Manook M, Nagendran M, et al. Tailored desensitization strategies in ABO blood group antibody incompatible renal transplantation. Transpl Int. 2014;27(2):187–196. doi:10.1111/tri.12234
11. Oriol R. ABH and related tissue antigens. Biochem Soc Trans. 1987;15(4):596–599. doi:10.1042/bst0150596
12. Mollicone R, Cailleau A, Oriol R. Molecular genetics of H, Se, Lewis and other fucosyltransferase genes. Transfus Clin Biol. 1995;2(4):235–242. doi:10.1016/S1246-7820(05)80089-8
13. Yamamoto F, Clausen H, White T, et al. Molecular genetic basis of the histo-blood group ABO system. Nature. 1990;345(6272):229–233. doi:10.1038/345229a0
14. Oriol R, Cartron JP, Cartron J, et al. Biosynthesis of ABH and Lewis antigens in normal and transplanted kidneys. Transplantation. 1980;29(3):184–188. doi:10.1097/00007890-198003000-00003
15. Rydberg L, Breimer ME, Brynger H, et al. ABO-incompatible kidney transplantation (A2 to O). Qualitative and semiquantitative studies of the humoral immune response against different blood group A antigens. Transplantation. 1990;49(5):954–960. doi:10.1097/00007890-199005000-00023
16. Rydberg L, Breimer ME, Samuelsson BE, et al. Blood group ABO-incompatible (A2 to O) kidney transplantation in human subjects: a clinical, serologic, and biochemical approach. Transplant Proc. 1987;19(6):4528–4537.
17. Bohmig GA, Farkas AM, Eskandary F, et al. Strategies to overcome the ABO barrier in kidney transplantation. Nat Rev Nephrol. 2015;11(12):732–747. doi:10.1038/nrneph.2015.144
18. Rieben R, Buchs JP, Fluckiger E, et al. Antibodies to histo-blood group substances A and B: agglutination titers, Ig class, and IgG subclasses in healthy persons of different age categories. Transfusion. 1991;31(7):607–615. doi:10.1046/j.1537-2995.1991.31791368336.x
19. Andersson M, Carlin N, Leontein K, et al. Structural studies of the O-antigenic polysaccharide of Escherichia coli O86, which possesses blood-group B activity. Carbohydr Res. 1989;185(2):211–223. doi:10.1016/0008-6215(89)80036-9
20. Spalter SH, Kaveri SV, Bonnin E, et al. Normal human serum contains natural antibodies reactive with autologous ABO blood group antigens. Blood. 1999;93(12):4418–4424. doi:10.1182/blood.V93.12.4418
21. Schlosser HA, Thelen M, Dieplinger G, et al. Prospective analyses of circulating B cell subsets in ABO-compatible and ABO-incompatible kidney transplant recipients. Am J Transplant. 2017;17(2):542–550. doi:10.1111/ajt.14013
22. Mond JJ, Vos Q, Lees A, Snapper CM. T cell independent antigens. Curr Opin Immunol. 1995;7(3):349–354. doi:10.1016/0952-7915(95)80109-X
23. Herzenberg LA. B-1 cells: the lineage question revisited. Immunol Rev. 2000;175:9–22. doi:10.1111/j.1600-065X.2000.imr017520.x
24. Ishida H, Tanabe K, Ishizuka T, et al. Differences in humoral immunity between a non-rejection group and a rejection group after ABO-incompatible renal transplantation. Transplantation. 2006;81(5):665–671. doi:10.1097/01.tp.0000185193.77929.96
25. Snapper CM, McIntyre TM, Mandler R, et al. Induction of IgG3 secretion by interferon gamma: a model for T cell-independent class switching in response to T cell-independent type 2 antigens. J Exp Med. 1992;175(5):1367–1371. doi:10.1084/jem.175.5.1367
26. Mond JJ, Lees A, Snapper CM. T cell-independent antigens type 2. Annu Rev Immunol. 1995;13:655–692. doi:10.1146/annurev.iy.13.040195.003255
27. Tonti E, Fedeli M, Napolitano A, et al. Follicular helper NKT cells induce limited B cell responses and germinal center formation in the absence of CD4 + T cell help. J Immunol. 2012;188(7):3217–3222. doi:10.4049/jimmunol.1103501
28. Nemes B, Barta A, Ivádi G, et al. T cell subset profile and appearance of donor-specific antibodies in primary and retransplanted kidney recipients. Transplant Proc. 2019;51(4):1215–1225. doi:10.1016/j.transproceed.2019.04.002
29. Park WD, Grande JP, Ninova D, et al. Accommodation in ABO-incompatible kidney allografts, a novel mechanism of self-protection against antibody-mediated injury. Am J Transplant. 2003;3(8):952–960. doi:10.1034/j.1600-6143.2003.00179.x
30. Iwasaki K, Miwa Y, Ogawa H, et al. Comparative study on signal transduction in endothelial cells after anti-a/b and human leukocyte antigen antibody reaction: implication of accommodation. Transplantation. 2012;93(4):390–397. doi:10.1097/TP.0b013e3182424df3
31. Takahashi K, Saito K. ABO-incompatible kidney transplantation. Transplant Rev. 2013;27(1):1–8. doi:10.1016/j.trre.2012.07.003
32. Chen Song S, Zhong S, Xiang Y, et al. Complement inhibition enables renal allograft accommodation and long-term engraftment in presensitized nonhuman primates. Am J Transplant. 2011;11(10):2057–2066. doi:10.1111/j.1600-6143.2011.03646.x
33. Koestner SC, Kappeler A, Schaffner T, et al. Histo-blood group type change of the graft from B to O after ABO mismatched heart transplantation. Lancet. 2004;363(9420):1523–1525. doi:10.1016/S0140-6736(04)16179-5
34. Tanabe T, Ishida H, Horita S, et al. Endothelial chimerism after ABO-incompatible kidney transplantation. Transplantation. 2012;93(7):709–716. doi:10.1097/TP.0b013e31824612b5
35. Barbolla L, Mojena M, Cienfuegos JA, et al. Presence of an inhibitor of glycosyltransferase activity in a patient following an ABO incompatible liver transplant. Br J Haematol. 1988;69(1):93–96. doi:10.1111/j.1365-2141.1988.tb07608.x
36. West LJ, Pollock-Barziv SM, Dipchand AI, et al. ABO-incompatible heart transplantation in infants. N Engl J Med. 2001;344(11):793–800. doi:10.1056/NEJM200103153441102
37. Urschel S, Campbell PM, Meyer SR, et al. Absence of donor-specific anti-HLA antibodies after ABO-incompatible heart transplantation in infancy: altered immunity or age? Am J Transplant. 2010;10(1):149–156. doi:10.1111/j.1600-6143.2009.02877.x
38. Genberg H, Kumlien G, Wennberg L, et al. Isoagglutinin adsorption in ABO-incompatible transplantation. Transfus Apher Sci. 2010;43(2):231–235. doi:10.1016/j.transci.2010.07.016
39. Cen M, Wang R, Kong W, et al. ABO-incompatible living kidney transplantation. Clin Transplant. 2020;34(9):e14050. doi:10.1111/ctr.14050
40. Tanabe K. Double-filtration plasmapheresis. Transplantation. 2007;84(12 Suppl):S30–2. doi:10.1097/01.tp.0000296103.34735.b8
41. Biglarnia AR, Nilsson B, Nilsson Ekdahl K, et al. Desensitization with antigen-specific immunoadsorption interferes with complement in ABO-incompatible kidney transplantation. Transplantation. 2012;93(1):87–92. doi:10.1097/TP.0b013e31823bb689
42. Schiesser M, Steinemann DC, Hadaya K, et al. The reuse of immunoadsorption columns in ABO-incompatible kidney transplantation is efficient: the Swiss experience. Transplantation. 2015;99(5):1030–1035. doi:10.1097/TP.0000000000000457
43. Tobian AA, Shirey RS, Montgomery RA, et al. The critical role of plasmapheresis in ABO-incompatible renal transplantation. Transfusion. 2008;48(11):2453–2460. doi:10.1111/j.1537-2995.2008.01857.x
44. Tobian AA, Shirey RS, Montgomery RA, et al. Therapeutic plasma exchange reduces ABO titers to permit ABO-incompatible renal transplantation. Transfusion. 2009;49(6):1248–1254. doi:10.1111/j.1537-2995.2008.02085.x
45. Tyden G, Donauer J, Wadström J, et al. Implementation of a protocol for ABO-incompatible kidney transplantation–a three-center experience with 60 consecutive transplantations. Transplantation. 2007;83(9):1153–1155. doi:10.1097/01.tp.0000262570.18117.55
46. Montgomery RA, Locke JE, King KE, et al. ABO incompatible renal transplantation: a paradigm ready for broad implementation. Transplantation. 2009;87(8):1246–1255. doi:10.1097/TP.0b013e31819f2024
47. Speer C, Kälble F, Nusshag C, et al. Outcomes and complications following ABO-incompatible kidney transplantation performed after desensitization by semi-selective immunoadsorption - a retrospective study. Transpl Int. 2019;32(12):1286–1296. doi:10.1111/tri.13482
48. Becker LE, Siebert D, Süsal C, et al. Outcomes following ABO-incompatible kidney transplantation performed after desensitization by nonantigen-specific immunoadsorption. Transplantation. 2015;99(11):2364–2371. doi:10.1097/TP.0000000000000753
49. Genberg H, Kumlien G, Wennberg L, et al. ABO-incompatible kidney transplantation using antigen-specific immunoadsorption and rituximab: a 3-year follow-up. Transplantation. 2008;85(12):1745–1754. doi:10.1097/TP.0b013e3181726849
50. Okumi M, Toki D, Nozaki T, et al. ABO-incompatible living kidney transplants: evolution of outcomes and immunosuppressive management. Am J Transplant. 2016;16(3):886–896. doi:10.1111/ajt.13502
51. Kohei N, Hirai T, Omoto K, et al. Chronic antibody-mediated rejection is reduced by targeting B-cell immunity during an introductory period. Am J Transplant. 2012;12(2):469–476. doi:10.1111/j.1600-6143.2011.03830.x
52. Subramanian V, Gunasekaran M, Gaut JP, et al. ABO incompatible renal transplants and decreased likelihood for developing immune responses to HLA and kidney self-antigens. Hum Immunol. 2016;77(1):76–83. doi:10.1016/j.humimm.2015.10.014
53. Sonnenday CJ, Warren DS, Cooper M, et al. Plasmapheresis, CMV hyperimmune globulin, and anti-CD20 allow ABO-incompatible renal transplantation without splenectomy. Am J Transplant. 2004;4(8):1315–1322. doi:10.1111/j.1600-6143.2004.00507.x
54. Gloor J, Stegall M. ABO-incompatible kidney transplantation with and without splenectomy. Transplantation. 2006;82(5):720. doi:10.1097/01.tp.0000229428.03414.b2
55. Kamburova EG, Koenen HJ, Borgman KJE, et al. A single dose of rituximab does not deplete B cells in secondary lymphoid organs but alters phenotype and function. Am J Transplant. 2013;13(6):1503–1511. doi:10.1111/ajt.12220
56. Uchida J, Machida Y, Iwai T, et al. Conversion of stable ABO-incompatible kidney transplant recipients from mycophenolate mofetil with standard exposure calcineurin inhibitors (CNIs) to everolimus with very low exposure CNIs-a short-term pilot study. Clin Transplant. 2014;28(1):80–87. doi:10.1111/ctr.12281
57. Kobayashi T, Liu D, Ogawa H, et al. Removal of blood group A/B antigen in organs by ex vivo and in vivo administration of endo-beta-galactosidase (ABase) for ABO-incompatible transplantation. Transpl Immunol. 2009;20(3):132–138. doi:10.1016/j.trim.2008.09.007
58. Hasegawa Y, Kato Y, Kaneko MK, et al. Neutralization of blood group A-antigen by a novel anti-A antibody: overcoming ABO-incompatible solid-organ transplantation. Transplantation. 2008;85(3):378–385. doi:10.1097/TP.0b013e3181612f84
59. Ye Y, Niekrasz M, Kehoe M, et al. Cardiac allotransplantation across the ABO-blood group barrier by the neutralization of preformed antibodies: the baboon as a model for the human. Lab Anim Sci. 1994;44(2):121–124.
60. Wongsaroj P, Kahwaji J, Vo A, Jordan SC. Modern approaches to incompatible kidney transplantation. World J Nephrol. 2015;4(3):354–362. doi:10.5527/wjn.v4.i3.354
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.