Back to Journals » Journal of Pain Research » Volume 19
Current Evidence and Clinical Implications of Full-Endoscopic Spine Surgery for Post-Vertebroplasty Lumbar Radiculopathy: A Comprehensive Review
Received 3 February 2026
Accepted for publication 30 March 2026
Published 11 April 2026 Volume 2026:19 600821
DOI https://doi.org/10.2147/JPR.S600821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Yong Ahn,1 Sol Lee,2 Chang Won Lee1
1Department of Neurosurgery, Kyung Hee University Hospital at Gangdong, Kyung Hee University College of Medicine, Seoul, Republic of Korea; 2Department of Clinical Research, Biobytes Inc, Seoul, Republic of Korea
Correspondence: Yong Ahn, Department of Neurosurgery Kyung Hee University Hospital at Gangdong, Kyung Hee University College of Medicine, 892 Dongnam-ro, Gangdong-gu, Seoul, 05278, Republic of Korea, Tel +82-2-440-6147, Fax +82-2-440-7494, Email [email protected]
Abstract: Percutaneous vertebroplasty (PVP) and kyphoplasty relieve pain associated with osteoporotic vertebral compression fractures. However, the underlying heterogeneous mechanisms of new-onset and post-vertebroplasty radiculopathy, together with ambiguous imaging findings, can complicate diagnoses. This review summarizes the etiologies, diagnostic processes, and therapeutic roles of full-endoscopic spine surgery (FESS) in treating radiculopathy after vertebroplasty. A comprehensive search of PubMed, Embase and Cochrane Library was performed using the following terms: (“percutaneous vertebroplasty” OR “kyphoplasty”) AND (“radiculopathy” OR “nerve root compression” OR “foraminal stenosis” OR “cement leakage”) AND (“endoscopic spine surgery” OR “full-endoscopic” OR “percutaneous endoscopic” OR “transforaminal endoscopic” OR “TELF” OR “FESS”). Nine of the 428 retrieved studies met the inclusion criteria and were analyzed for etiology, imaging, technique, anesthesia, and outcomes. All included studies were case reports or small case series, and their methodological quality was assessed using established critical appraisal tools for descriptive research. Cement leakage emerged as the main cause of postvertebroplasty radiculopathy, which is managed using FESS via transforaminal or interlaminar approaches. Most patients experienced pain relief and neurological improvement with low perioperative morbidity rates. Endoscopic exploration under local anesthesia may serve as a valuable diagnostic tool to identify and localize neural compression that remains ill-defined on preoperative imaging. Given the limited and heterogeneous nature of the current evidence, conclusions regarding the safety and effectiveness of FESS should be interpreted with caution. Nevertheless, FESS might serve as a feasible diagnostic and therapeutic option when conventional imaging modalities fail to identify the pain generator.
Keywords: cement leakage, endoscopic spine surgery, kyphoplasty, radiculopathy, vertebroplasty
Introduction
Vertebral compression fractures (VCFs) in fragile older adults are common, particularly when osteoporosis is involved. The incidence of VCFs increases sharply with advancing age and low bone mineral density, affecting up to 40% of women and 20% of men aged > 70 years.1,2 Such fractures cause severe back pain, spinal deformities, and functional decline and are associated with increased morbidity and mortality rates.3,4 Conservative treatments, such as bed rest, bracing, and analgesics, often do not provide early pain relief or prevent further collapse.
Percutaneous vertebroplasty (PVP) and balloon kyphoplasty are minimally invasive procedures designed to provide rapid pain relief, mechanical stabilization, and early mobilization.5–7 These techniques restore vertebral height and alignment, and significantly improve pain and functional outcomes with relatively low complication rates.8–10 Consequently, PVP and kyphoplasty have become key treatment options for older patients who are unfit for open surgeries.
Despite generally favorable safety profiles, complications such as cement leakage into the spinal canal or neural foramina remain clinically relevant, as they can result in nerve root compression, epidural irritation, or spinal cord compression, leading to acute or delayed radiculopathy and neurological deficits.11–13 Although cement leakage after vertebral augmentation is relatively common (20%–65% of cases depending on imaging modality) symptomatic neurological complications, such as radiculopathy are rare and occur in approximately 1%–3% of patients.11–15
To diagnose radiculopathy after vertebroplasty can be challenging. Radiological findings are often ambiguous because tiny cement leaks can become partially embedded within bone or masked by imaging artifacts. Susceptibility effects frequently limit the value of magnetic resonance imaging (MRI), whereas computed tomography (CT) is superior for visualizing cement distribution, but might not reliably reveal nerve irritation, adhesions, or subtle foraminal pathology. Consequently, the underlying pain generator might be underdiagnosed or misinterpreted, particularly among older patients with multilevel degenerative changes or coexisting spinal stenosis.16 Furthermore, open revision surgery in this population has been associated with substantial risks owing to poor bone quality, medical comorbidities, and the need for general anesthesia.
In this clinical context, full-endoscopic spine surgery (FESS) has emerged as a minimally invasive alternative with diagnostic and therapeutic potential. It can be applied under local anesthesia, which reduces anesthetic risk in older and medically compromised patients. The percutaneous endoscopic approach allows direct visualization of neural structures and adjacent pathological elements, including cement fragments, fibrotic adhesions, and foraminal narrowing, which enables real-time confirmation at the symptomatic level. Targeted decompression can be applied during the same procedure after pathology is identified.17–19 Subtle mechanical or inflammatory nerve irritation can be identified and addressed with minimal collateral tissue damage by magnified endoscopic visualization and continuous saline irrigation.
Several case reports and small case series describe the success of FESS for treating radiculopathy or neurological symptoms after PVP or kyphoplasty, in terms of rapid pain relief, functional improvement, and low perioperative morbidity rates.20–28 However, quantitative and qualitative evidence are scant and consist mostly of descriptive studies without analytical comparisons. To date, the etiologies of post-vertebroplasty radiculopathy and the role of FESS in its management have not been critically appraised in a focused review.
Therefore, this review aimed to integrate the findings of current clinical literature through a comprehensive narrative review and critical appraisal, and to summarize reported causes of radiculopathy after PVP or kyphoplasty to highlight diagnostic challenges in clinical practice. We also aimed to determine the potential roles and limitations of FESS as a minimally invasive diagnostic and therapeutic option for selected patients.
Materials and Methods
Literature Search Strategies
We comprehensively searched the PubMed, Embase, and Cochrane Library databases. The final search proceeded on December 16, 2025. The search strategy was designed around the conceptual domains of causative procedure (“percutaneous vertebroplasty” OR “kyphoplasty”), clinical presentation (“radiculopathy” OR “nerve root compression” OR “foraminal stenosis” OR “nerve injury” OR “cement leakage”), and treatment modality (“endoscopic spine surgery” OR “full endoscopic” OR “percutaneous endoscopic” OR “transforaminal endoscopic” OR “TELF” OR “FESS”) using Boolean operators and database-specific syntax. No restrictions were imposed on the types of reports, year of publication, or language.
Study Eligibility Criteria
Studies were eligible for analysis if they met the following criteria: patients who developed radiculopathy or neurological symptoms after PVP or kyphoplasty were treated with FESS as the primary surgical intervention, and clinical information about symptoms, imaging findings, surgical techniques, and postoperative outcomes were provided.
Original clinical study designs, case reports, technical notes, case series, and observational cohort studies were assessed. The exclusion criteria comprised endoscopic procedures that were not the primary treatment, investigated non-vertebroplasty-related pathology, lacked sufficient clinical or surgical detail, or were animal studies, cadaveric investigations, editorials, or narrative commentaries without original patient data.
Study Selection and Data Extraction
Titles and abstracts identified through database searches were screened for relevance. Full-text articles were reviewed to determine final eligibility. We selected studies using a stepwise approach, and the reasons for exclusion at the full-text stage were documented. Given the descriptive nature and limited number of available studies, formal adjudication processes were not required.
We extracted the demographics of innominate patients, vertebral levels, and presumed etiologies of radiculopathy, as well as diagnostic imaging modalities, the type and approach of FESS, anesthetic methods, and clinical outcomes from the included studies. Quantitative syntheses or meta-analyses were unfeasible due to the heterogeneity in study design, outcome measures, and follow-up duration. Therefore, we summarized the results using a qualitative narrative approach.
Critical Appraisal of Methodological Quality
All included studies were descriptive and consisted exclusively of case reports, case series, or technical notes. Therefore, we assessed the methodological quality using the Joanna Briggs Institute (JBI) Critical Appraisal Tools for Case Reports and Case Series to systematically evaluate reporting transparency and potential sources of bias in non-comparative clinical evidence.29 The appraisal focused on key methodological domains, including the clarity of patient selection and clinical presentation, adequacy of diagnostic assessment, description of the endoscopic intervention, outcome reporting, and follow-up duration. The purpose of this assessment was not to exclude studies based on quality thresholds but to transparently characterize the limitations of the existing literature and contextualize the interpretation of the reported outcomes. Consistent with the narrative review design, no numerical quality scoring or grading of the evidence certainty was performed.
Results
Literature Search results
We identified 428 publications in the PubMed, Embase, and Cochrane Library databases, among which 71 were duplicates. A screen of 357 article titles led to the exclusion of 92 editorials, narrative reviews, systematic reviews, or meta-analyses. Screening abstracts of the remaining 265 studies excluded 231 that were irrelevant to endoscopic procedures, vertebroplasty, kyphoplasty, or radiculopathy, leaving 34 articles for full text reviews. Of these, 25 studies were excluded due to insufficient surgical details, lack of postoperative outcome data, or absence of full-endoscopic intervention. Finally, nine studies met the inclusion criteria and were included in the qualitative synthesis of the results.20–28 These studies comprised case reports and small case series that described the management of radiculopathy or neurological symptoms after PVP or kyphoplasty using FESS. Figure 1 shows the flow of publications through the study.
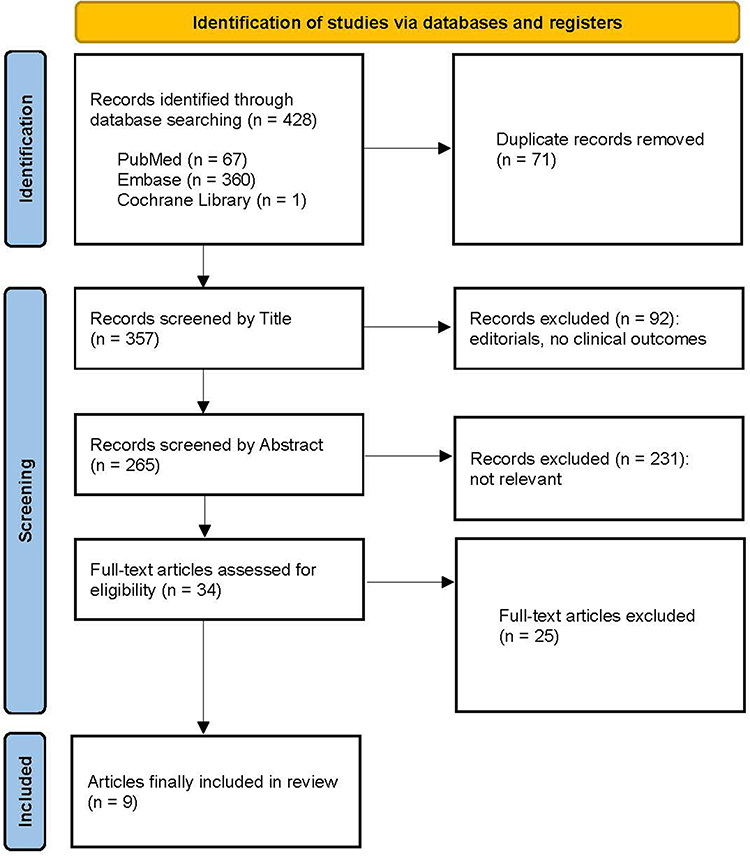 |
Figure 1 Flow of literature search through the study. |
Characteristics of Studies
The nine studies were published between 2016 and 2025, comprised five technical case reports, two case series, and two retrospective observational studies. Tables 1 and 2 summarize the clinical characteristics, technical approaches, and outcomes of 93 patients (male, n = 43; female, n = 50; mean age, 68.8 years). All studies described single-level thoracolumbar procedures to treat radiculopathy or neurological deficits that developed after PVP or kyphoplasty. The predominant surgical approach was transforaminal endoscopic lumbar decompression, including transforaminal endoscopic lumbar foraminotomy (TELF) or foraminoplasty.20,22–28 Ventral or foraminal cement deposits were accessed by partial pediculotomy or trench drilling in some patients.22 An interlaminar endoscopic approach was combined with partial laminotomy in two studies.21,28 General24,28 and local20–23,25–27 anesthesia was applied in two and seven studies, respectively. Preoperative imaging typically included magnetic resonance imaging and computed tomography. Diagnoses based only on MRI were inconclusive in most reports and were confirmed by CT imaging and intraoperative endoscopic exploration. The mean surgical duration was 88.3 min, and the mean postoperative hospital stay was 5.0 days. Cement leakage into the epidural or foraminal space was the most frequent etiology of post-vertebroplasty radiculopathy. While earlier reports focused primarily on single-level cement leakage, the inclusion of a large-scale cohort expanded the etiologies to include aggravated foraminal stenosis and mobile bone fragment compression.28
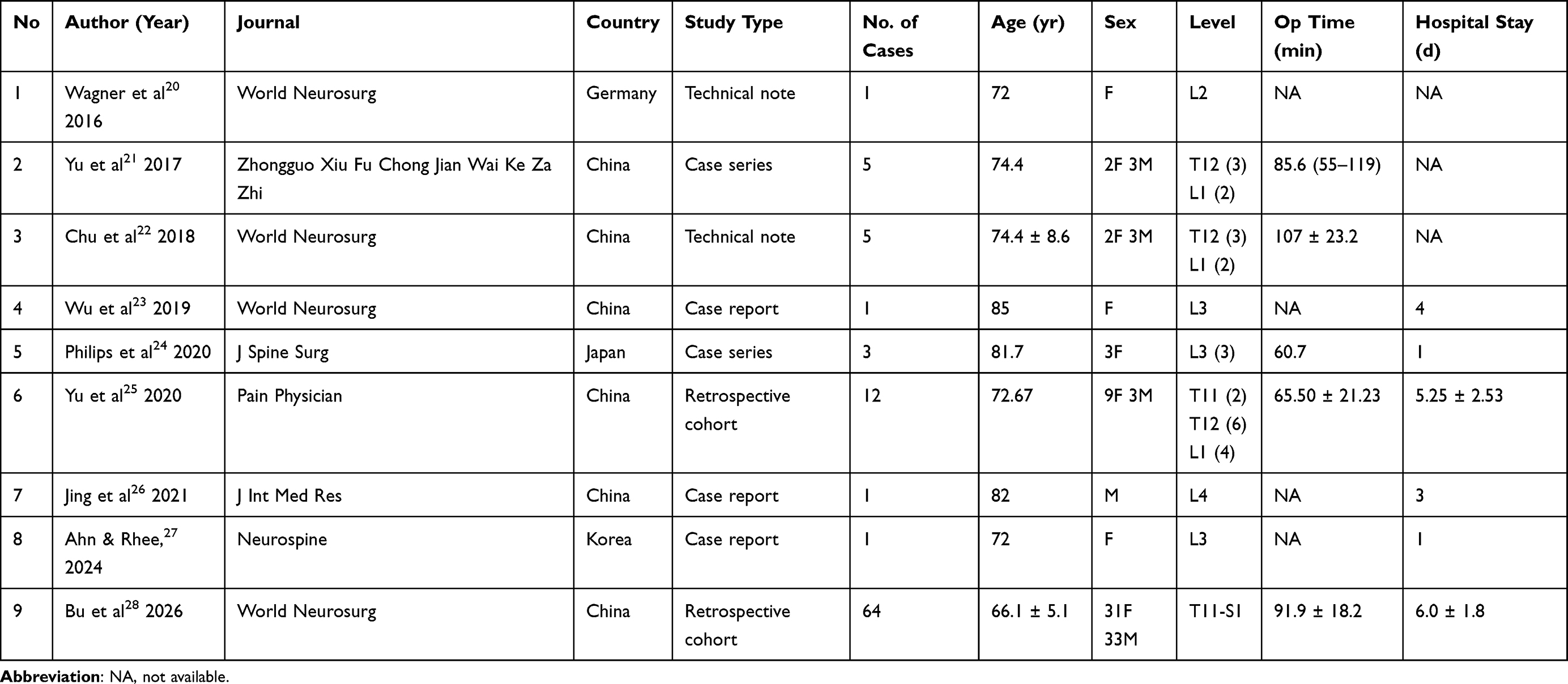 |
Table 1 Summary of the Included Studies and Patient Demographics |
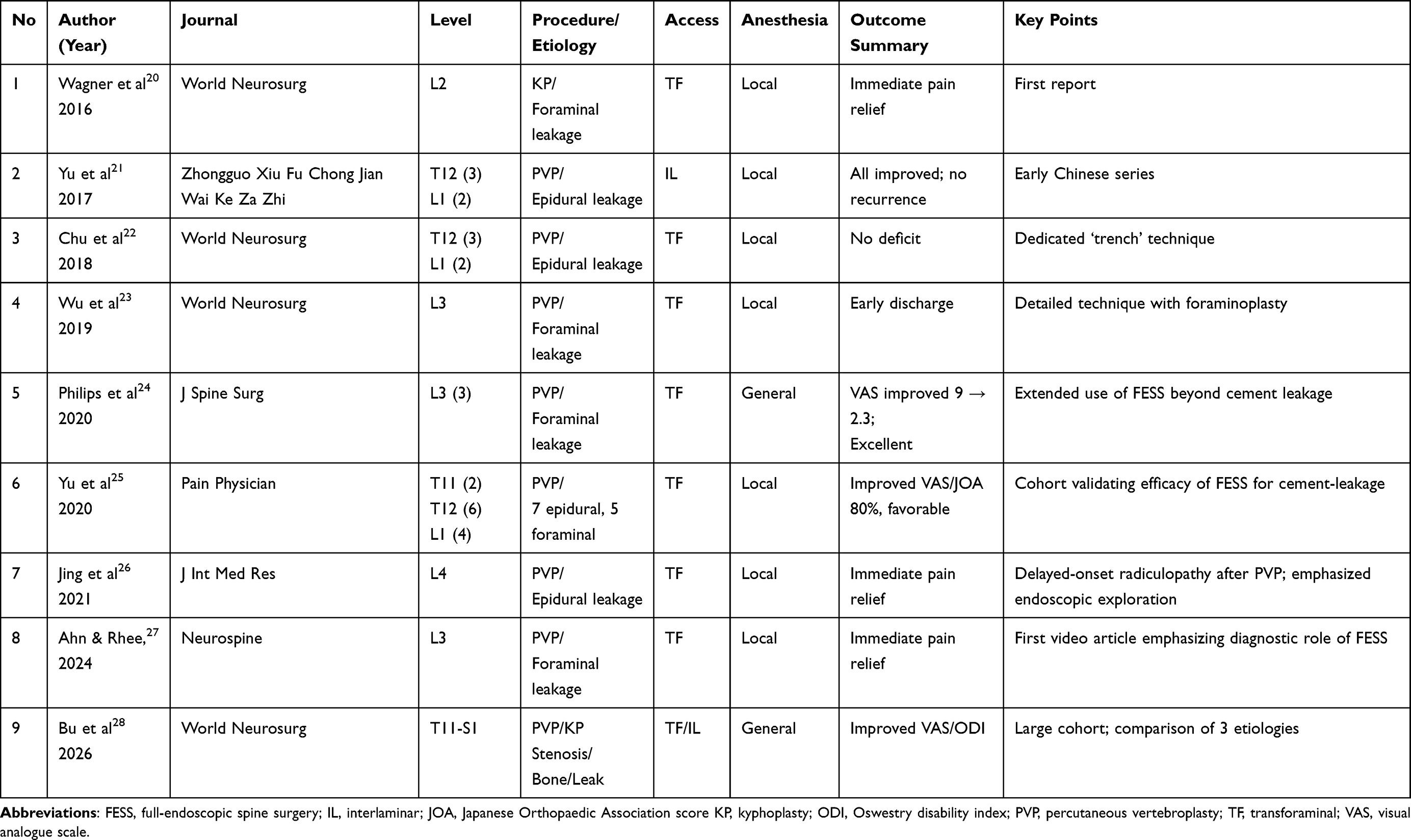 |
Table 2 Technical and Clinical Characteristics of Full-Endoscopic Spine Surgery for Post-Vertebroplasty Radiculopathy |
Clinical Outcomes
Postoperative clinical outcomes were reported in all nine articles, with the majority of patients experiencing immediate relief of radicular pain. According to the modified MacNab criteria reported in the largest cohort, the “excellent/good” recovery rate was 87.5% for Group A (foraminal stenosis), 80.9% for Group B (bone fragment compression), and 68.4% for Group C (bone cement leakage). All groups showed significant improvements in Visual Analogue Scale (VAS) scores for both back and leg pain, as well as Oswestry Disability Index (ODI) scores at the final follow-up (P < 0.05).28 Another clinical series included 12 patients with intraspinal cement leakage treated by percutaneous endoscopic spinal surgery under local anesthesia, which achieved an 80% (good-to-excellent) rate while significantly improving pain and Japanese Orthopaedic Association (JOA) scores.25 Postoperative pain was immediately relieved in other representative patients who were ambulatory within 1–2 days.24,27 Reported complications were minimal, with negligible blood loss and no major perioperative adverse events. Neurological deterioration or recurrence during 2–30 months of follow-up was not described in any of the articles. Although outcome measures such as VAS, ODI, and JOA scores varied among the nine studies, the overall trend consistently favored symptomatic improvement after endoscopic decompression of cement-related or foraminal pathologies.
Methodological Quality Assessment
We applied the JBI Critical Appraisal Tools for Case Reports and Case Series to assess methodological quality. Evidence in the eight studies met the minimum criteria for inclusion and were classified as Level IV. Table 3 shows the overall appraisal results. The characteristics of the patients, diagnostic workup, and full-endoscopic surgical techniques were adequately described. Clinical outcomes were clearly described, and postoperative symptom improvement, as well as a low incidence of procedure-related complications, were consistently documented. However, the methodological limitations comprised small samples, no controls, comparators, or standardized outcome measures, and variable or limited follow-ups. Consecutive or complete patient inclusion was unclear in the three case series, introducing potential selection bias.21,22,25 In addition, most reports were generated at single high-volume endoscopic centers, which might limit their generalizability.
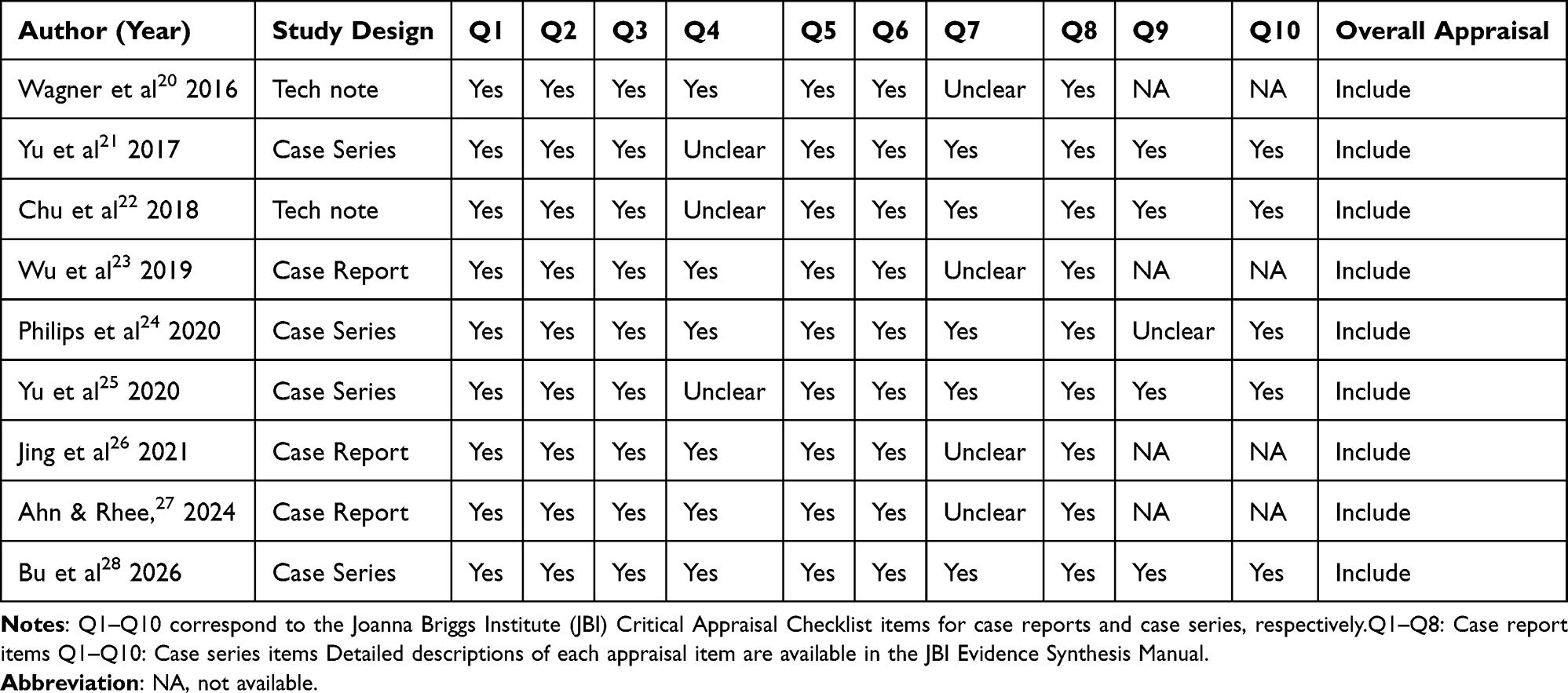 |
Table 3 Methodological Quality Assessment of Included Studies Using the Joanna Briggs Institute (JBI) Critical Appraisal Tools |
Discussion
Methodological considerations and limitations
Current literature regarding full-endoscopic spine surgery for radiculopathy after vertebroplasty is limited to case reports, small case series, and technical notes. This reflects both the rarity of clinically significant post-vertebroplasty radiculopathy and the practical constraints associated with comparative or randomized studies of predominantly elderly and medically fragile patients. Under these circumstances, a formal systematic review or meta-analysis is unlikely to yield robust quantitative conclusions. The current evidence base predominantly comprises retrospective case reports and small series, which inherently introduces significant publication bias and limits the strength of clinical recommendations. Instead, a comprehensive narrative review combined with a critical appraisal provides a more appropriate framework for synthesizing heterogeneous clinical observations, contextualizing reported outcomes, and transparently acknowledging the limitations of current evidence.
The methodological appraisal of the included studies revealed several common limitations, including small sample sizes, absence of control groups, non-standardized outcome measures, and variable follow-up durations. In addition, most reports originated from specialized centers with extensive endoscopic experience, raising concerns regarding selection bias, operator dependence, and limited generalizability. Collectively, these factors preclude definitive conclusions about comparative effectiveness or long-term outcomes. Specifically, the lack of standardized reporting on potential confounders and limited long-term follow-up data necessitate a cautious interpretation of the reported success rates.
Hence, the present findings should be interpreted primarily as evidence of clinical feasibility and diagnostic utility rather than as proof of superiority or efficacy. Within these constraints, the consistent reporting of symptom improvement and low perioperative morbidity across heterogeneous studies suggests that full-endoscopic approaches may represent a reasonable option in carefully selected patients, particularly when conventional imaging and conservative treatments fail to identify or resolve the pain generator.
Clinical Characteristics and Pathophysiology of Radiculopathy After Vertebroplasty
Cement leakage is a common complication after PVP or kyphoplasty, with an incidence of 20%–65%, depending on the imaging modality and diagnostic criteria.13,14,30 Although most patients were asymptomatic, 1%–3% develop neurological symptoms due to epidural or foraminal cement extrusion.11,12 High-resolution CT and real-time fluoroscopy have revealed far more frequent minor subclinical leakages than were previously thought.30 This is because they tend to occur more frequently when large volumes of low-viscosity cement are injected under high pressure in osteoporotic or burst-type fractures.30–32 Leakage rates are slightly lower for kyphoplasty than for vertebroplasty because balloon expansion forms a cavity. Regardless, clinically significant neurological events have occurred after both procedures.9
Cement leakage is influenced by patient- and procedure-related factors. Severe vertebral collapse, posterior wall disruption, cortical defects, and osteonecrosis increase the risk of leakage.33 Technically, low-viscosity cement, excessive injection volume, high injection pressure, and insufficient fluoroscopic control significantly contribute to cement leakage.34–36 Early learning curves are also associated with higher leakage rates in patients.37 After polymethylmethacrylate (PMMA) penetrates the epidural or foraminal space, even a small volume can cause clinically relevant neural compression because of limited anatomical tolerance in these areas.38 Furthermore, beyond immediate neural compromise, cement leakage is an independent risk factor for subsequent vertebral fractures. A recent comparative study reported that patients with cement leakage experienced significantly higher rates of fracture recurrence at both treated and adjacent levels, suggesting that leakage may reflect suboptimal cement distribution and compromised biomechanical stability.39
The pathophysiology of radiculopathy secondary to cement leakage involves mechanical, thermal, and chemical mechanisms. Extravasated cement fragments can directly compress the nerve root or dural sac, particularly within the foramen or lateral recess.22 Thermal injury might occur because the exothermic polymerization of PMMA can exceed 70 °C, which leads to local neural and vascular damage.40 Residual monomers or incomplete polymerization can trigger sterile inflammation, fibrosis, and delayed neural irritation. Progressive vertebral collapse or segmental kyphosis after the initial procedure might further aggravate foraminal narrowing, resulting in delayed-onset symptoms.41 Figure 2 shows these pathophysiological mechanisms and endoscopic access routes.
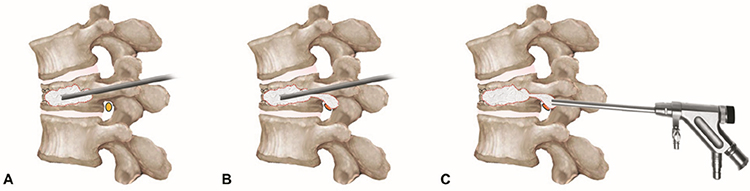 |
Figure 2 Schema of radiculopathy pathophysiology after vertebroplasty and corresponding endoscopic approach. (A) Percutaneous vertebroplasty: bone cement is injected into the fractured vertebral body through a transpedicular approach (bone cement indicated by a dotted outline). (B) Nerve root compression resulting from bone cement leakage or other factors, such as vertebral collapse, aggravated stenosis, or mobile bone fragments. (C) Transforaminal endoscopic approach allows direct visualization, identification, and removal of compressive or irritating elements under local anesthesia. |
Clinical presentation depends on the leakage site. Epidural leakage commonly causes central canal compression or axial pain, whereas foraminal leakage leads to dermatomal pain, paresthesia, or weakness corresponding to the affected nerve root. Although the preferred modality for confirming cement migration is still CT imaging, correlations with clinical findings are essential because even CT might miss subtle nerve impingement or perineural fibrosis.27 In previous literature, cement leakage was identified as the primary pathophysiological mechanism for post-PVP radiculopathy. However, recent findings by Bu et al in a larger cohort expanded this understanding by categorizing the etiologies into three main groups: aggravated foraminal stenosis, mobile bone fragment compression, and bone cement leakage28 While cement leakage remains a significant factor, our analysis shows that pre-existing or aggravated stenosis and bony retropulsion are also critical contributors. Notably, although the cement leakage group required longer operative times and showed slower initial recovery, full-endoscopic decompression was ultimately effective across all pathophysiological types.
Diagnostic Ambiguity and the Role of Endoscopic Exploration
Accurate diagnosis of radiculopathy after vertebroplasty remains challenging, due to incomplete or inconclusive information delivered by conventional imaging modalities. Simple radiographs and intraoperative fluoroscopy depict cement distribution only in projections and might fail to notice small foraminal deposits or partially embedded epidural tracts. Although MRI is essential for evaluating edema, neuritis, and epidural reactions, it recognizes PMMA as a low signal, and metallic hardware and susceptibility effects could further obscure the cement-nerve interface, yielding equivocal or indeterminate findings in a nontrivial subset of patients. In contrast, thin-slice CT with multiplanar or three-dimensional reconstruction remains the modality of choice for localizing cement extravasation within the foramen or lateral recess and for characterizing associated bony contributors such as osteophytes and retropulsed fragments. Nevertheless, even CT can be inconclusive when faced with multiple treatments, cement intimately incorporated into bone, or a pain generator that is functional by tethering or perineural adhesion rather than a purely mass effect. A selective nerve root block is diagnostically valuable under such conditions; a short-acting anesthetic injected into a suspected root can produce immediate relief, increase the likelihood that the visualized lesion is clinically relevant, and guide the operative level when planning minimally invasive decompression.25,27,42–44
Epidurally injected therapeutic steroids or a periradicular block might transiently palliate inflammatory irritation, but mechanical impingement by epidural or foraminal cement or post-fracture bony overgrowth is often refractory, prompting surgical considerations. Conventional open revision under general anesthesia for older patients with osteoporosis or significant medical comorbidities entails substantial risks, such as dural tears, destabilization requiring instrumentation, blood loss, and prolonged recovery. These risks are amplified when imaging findings are ambiguous because the target might be uncertain. This clinical dilemma has contributed to the notion that FESS offers a potential bridge between diagnosis and treatment. Percutaneous endoscopic exploration under local anesthesia can verify symptomatic levels in real time by provoking pain, probing, and receiving immediate feedback. After confirmation, the procedure can seamlessly continue to targeted decompression and cement removal via the same working channel. Contemporary case series and technical reports describe favorable short-term outcomes, including pain relief, minimal morbidity, and short hospital stays. This suggests that full endoscopy represents a reasonable surgical option when nerve blocks fail, imaging findings are equivocal, and focal cement-related compression is suspected.20–28,43
Therapeutic Implications and Clinical Feasibility of Full-Endoscopic Spine Procedures
Full-endoscopic spine procedure has recently emerged as a potentially useful and minimally invasive solution for managing radiculopathy or neurological symptoms secondary to cement leakage after PVP or kyphoplasty. The eight studies summarized in Tables 1 and 2 show that FESS is primarily a transforaminal endoscopic lumbar decompression technique, but it can achieve diagnostic clarity and improve symptoms in selected older and medically fragile patients and others who are not appropriate candidates for open revision.
The diagnostic strength of FESS lies in its ability to directly visualize pathological structures in real time. Epidural or foraminal cement fragments, fibrotic adhesions, and nerve root compression can be visualized under local anesthesia while simultaneously evaluating patient feedback during probing or stimulation. This conscious feedback enables a functional correlation between anatomical findings and symptoms that helps to identify the symptomatic level, particularly when MRI or CT findings are ambiguous. Unlike indirect imaging- or fluoroscopy-guided interventions, endoscopic inspection allows the integration of anatomical and physiological assessments within a single procedure. This real-time diagnostic capability has been highlighted as a practical advantage for resolving uncertain findings.21,25,27
The reviewed studies suggest that FESS can provide meaningful symptom improvement. The transforaminal approach allows access to the foramen and extraforaminal regions without compromising spinal stability or requiring general anesthesia. Key technical maneuvers included foraminoplasty, removal of cement fragments, partial pediculotomy, and decompressing the exiting nerve root using high-speed drills and endoscopic forceps. Patients have experienced immediate postoperative pain relief and regained ambulation within 1–2 days, with minimal blood loss and no major complications.24,27
These findings suggest that FESS could serve as a combined diagnostic and therapeutic option for post-vertebroplasty radiculopathy in selected patients. It bridges the gap between conservative management and invasive open surgery, offering direct decompression under local anesthesia with minimal risk. This is particularly beneficial for older patients with osteoporosis and multiple comorbidities, for whom general anesthesia and fusion instrumentation increase risk. Furthermore, FESS is associated with early mobilization, short hospital stays, and preserved spinal integrity, which are consistent with the principles of minimally invasive geriatric spine care.
Despite these encouraging outcomes, current evidence is limited to small case series and technical notes, with no randomized or comparative studies. Most reports originate from specialized centers with extensive endoscopic experience, introducing potential publication and operator bias. The steep learning curve for transforaminal endoscopy and the need for fluoroscopic accuracy in accessing narrow foraminal spaces might limit generalizability. Furthermore, although FESS can effectively treat focal cement impingement, diffuse canal compromise, or combined instability, open or hybrid decompression might still be required.
Collectively, the literature suggests that FESS could be a feasible minimally invasive approach for managing cement leakage–related neural compression after PVP or kyphoplasty. Its strengths are the ability to combine diagnostic exploration and targeted decompression under local anesthesia, direct visualization of nerve–cement interactions, facilitated selective neural release, limited surgical morbidity with rapid postoperative recovery in high-risk older patients, and the ability to serve as a bridge between radiological ambiguity and more invasive surgical interventions. However, these advantages should be interpreted within the context of low-level evidence and careful patient selection.
Technical Details of Full-Endoscopic Transforaminal Lumbar Decompression
The present study found that FESS for post-vertebroplasty radiculopathy caused by cement leakage primarily proceeds via the transforaminal approach. Based on the reviewed literature and our clinical experience, the transforaminal FESS approach is the most commonly used and versatile technique for managing this complication. Therefore, several key technical details are summarized below to facilitate successful clinical outcomes and help surgeons navigate potential challenges during endoscopic decompression in this setting (Figures 3 and 4).
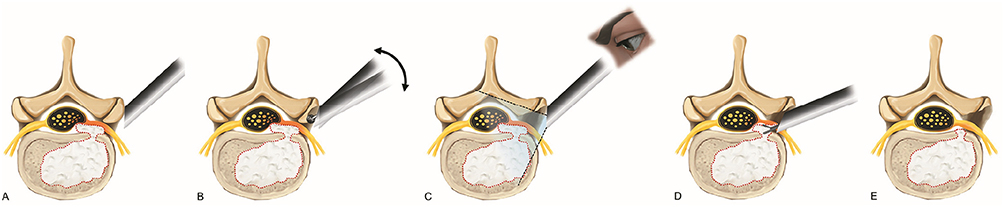 |
Figure 3 Stepwise surgical procedure of transforaminal full-endoscopic lumbar decompression. (A) Percutaneous transforaminal approach with working sheath placed in front of the foraminal zone to avoid irritating the exiting nerve root (bone cement indicated by a dotted outline). (B) Foraminal unroofing by removing the hypertrophic superior articular process and ligamentum flavum with dynamic movement of the endoscope during decompression (double-sided arrow). (C) Wide endoscopic field of view (dashed lines) demonstrating cement leakage compressing a hyperemic nerve root. (D) Foraminal and epidural decompression with removal of leaked cement and hypertrophic ligaments. (E) Final view of complete neural release after full-scale decompression. |
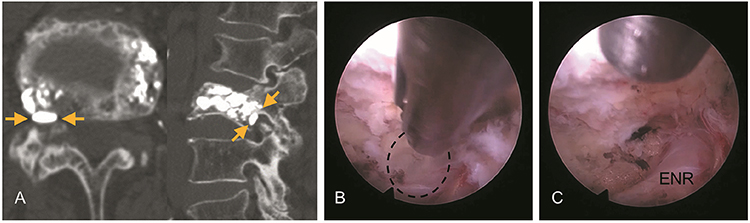 |
Figure 4 Representative case. Transforaminal endoscopic lumbar foraminotomy (TELF) at the right L3–4 level in an 82-year-old woman who developed right-sided radiculopathy due to foraminal cement leakage after percutaneous vertebroplasty at L3. (A) Preoperative CT image of foraminal cement leakage (arrows) compressing the exiting nerve root (ENR). (B) Intraoperative endoscopic view demonstrating cement leakage compressing the ENR in the foraminal space (outlined). (C) Final endoscopic view of full-scale foraminal decompression with adequate neural release. |
Safe Percutaneous Transforaminal Endoscopic Approach
A selective nerve root block is recommended before surgery to confirm the symptomatic root and rule out multilevel pathologies. Preoperative MRI and thin-slice CT are essential for delineating leakage pathways, foraminal dimensions, and safe entry trajectories. The entry point and approach angle should be planned individually based on the anatomy of patients and cement distribution. As the procedure usually proceeds under local anesthesia, a gentle outside-in approach is recommended to maximize patient comfort and minimize neural irritation. The initial cannula should target the lateral margin of the superior articular process (SAP) under fluoroscopic control to avoid direct contact with the exiting root. Gradual serial dilation through the working corridor minimizes pain and the risk of irritation during cannula advancement. These principles are consistent with the techniques described by Knight et al and Ahn et al, who emphasized patient comfort and safety during awake endoscopic decompression.17,27,45–47
Full-Scale Foraminal and Spinal Canal Decompression
Endoscopic visualization allows surgeons to directly identify heterogeneous compressive elements, such as cement fragments, hypertrophic facet joints, ossified ligaments, fibrotic adhesions, scar tissue within the foraminal corridor, and differentiate mechanical compression from inflammatory adhesion Endoscopic probing or electrically stimulating the nerve root using a radiofrequency probe in conscious patients might reproduce concordant pain, thereby providing functional confirmation of the pain generator.17,27
Decompression should proceed stepwise from the bony unroofing of the SAP toward the axillary epidural and lateral exit zones. Cement particles, overgrown bone, and thickened ligamentum flavum can be removed using endoscopic burrs and punches under continuous irrigation. Extended decompression from the lower to the upper pedicle (“pedicle-to-pedicle” principle) is recommended to ensure durable results by exposing the proximal epidural and distal lateral exit zones.46,47 This technique ensures complete neural release even when foraminal stenosis is complex or iatrogenic.
Tips for Achieving Adequate Decompression
Neural pulsation and dural sac mobility should be restored after decompression, and the exiting nerve root should be confirmed as the endpoint. A clean bony margin should be achieved by removing all residual fibrous tissue and debris around the decompressed field to reduce the risk of postoperative adhesions and restenosis. Maintaining a clear operative field through meticulous hemostasis using a tip-controllable radiofrequency probe and careful irrigation pressure control prevents a blurred surgical field (red-sun phenomenon) and ensures optimal endoscopic visibility throughout the procedure.46,47
Continuous surgical orientation must be maintained during the procedure. This implies knowing precisely where the working instruments are and which structures are evident at every moment. Losing orientation, even briefly, can lead to incomplete decompression or neural injury. As endoscopic surgery inherently provides a limited field of view, to “see the trees but not the forest” demands a thorough understanding of endoscopic anatomy and disciplined spatial awareness. Surgeons can prevent disorientation by precise recognition of details and accumulating hands-on experience through systematic training and repetition.
Prevention of Cement Leakage in Vertebroplasty
Although FESS provides an effective, minimally invasive option for managing cement leakage–related radiculopathy, prevention remains the most critical step. Cement extravasation can be avoided mainly through meticulous injection techniques, appropriate cement viscosity, and real-time fluoroscopic monitoring.13,14,30–32 A small incremental volume should be initially injected under low pressure at the ventral third of the vertebral body while continuously observing cement spread in anteroposterior and lateral projections. Termination of the injection is mandatory once the cement approaches the posterior quarter of the vertebral body or when any venous channel is visualized. High-viscosity or radio-opaque PMMA formulations, and calcium phosphate–based or bioactive cements can further reduce leakage risk.48–51 Adequate preoperative CT/MRI evaluation to identify cortical defects and balloon kyphoplasty in extremely collapsed fractures also contribute to safer augmentation. Ultimately, careful patient selection and disciplined injection control are essential to effectively manage and prevent cement leakage.
Future Perspectives
Although PVP and kyphoplasty have revolutionized the management of osteoporotic vertebral compression fractures, the risks of cement leakage and neural compression remain significant concerns. Preventing such complications requires refined intraoperative imaging, cement materials, and injection systems. Real-time fluoroscopy, cone-beam CT, and augmented reality guidance have improved intraoperative visualization and enabled more precise cement control. Nonetheless, inadvertent leakage can still develop in the face of cortical wall defects or severe osteoporosis.30–32 The development of new biomaterials with improved viscosity control and bioresorbable or thermally neutral properties could further reduce leakage risk while maintaining mechanical strength.52,53 Moreover, intelligent injection systems with real-time pressure feedback and automatic shut-off mechanisms represent promising innovations for safer vertebral augmentation.
Despite the increasing success of FESS in managing post-vertebroplasty radiculopathy, some limitations have persisted. The technique requires a steep learning curve, a restricted visual field, and limited instrument maneuverability, particularly under complex or multilevel stenotic situations.54,55 Overcoming these challenges requires structured training curricula, standardized competence evaluations, and the continued development of advanced surgical instruments. Current advances in high-definition optics, multi-channel endoscopes, and irrigation pressure control systems have already enhanced the procedural safety and effectiveness of endoscopic decompression.
The next frontier for FESS is the integration of artificial intelligence (AI), navigation-assisted imaging, and robotic guidance. Real-time image segmentation, intraoperative navigation overlays, and robotic positioning systems based on AI can enhance spatial accuracy, reduce learning curves, and enable safer procedures even for less-experienced surgeons.56–59 These technologies should render FESS more intuitive and accessible while minimizing intraoperative risks.
Conclusion
Radiculopathy following vertebral augmentation is an uncommon but serious complication, most often resulting from cement leakage or foraminal compromise. This review suggests that full-endoscopic spine procedures represent a feasible, minimally invasive approach for real-time diagnostic exploration and targeted decompression, particularly for patients with inconclusive imaging findings. Although current evidence is limited to small-scale retrospective reports, the observed clinical utility warrants further validation. Future research should prioritize prospective comparative cohorts and standardized outcome reporting to definitively establish the comparative effectiveness and safety of this endoscopic approach.
Abbreviations
VCF, Vertebral Compression Fracture; PVP, Percutaneous Vertebroplasty; MRI, Magnetic Resonance Imaging; CT, Computed Tomography; FESS, Full-Endoscopic Spine Surgery; TELF, Transforaminal Endoscopic Lumbar Foraminotomy; JBI, Joanna Briggs Institute; VAS, Visual Analogue Scale; ODI, Oswestry Disability Index; JOA, Japanese Orthopaedic Association score.
Ethics Statement
Ethical review and approval were waived for this study as it is a narrative and technical review of published literature and is based on the clinical experience of the author. New patient data were not collected or analyzed.
Acknowledgments
The authors would like to thank Hwa-Young Kim and Jae-Min Son for administrative and technical support during the preparation of this manuscript.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cooper C, Atkinson EJ, O’Fallon WM, Dr. Melton JL. Melton LJ, III. Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985-1989. J Bone Miner Res. 1992;7(2):221––15. doi:10.1002/jbmr.5650070214
2. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–1733. doi:10.1007/s00198-006-0172-4
3. Silverman SL, Minshall ME, Shen W, Harper KD, Xie S. Health-related quality of life subgroup of the multiple outcomes of raloxifene evaluation study. the relationship of health-related quality of life to prevalent and incident vertebral fractures in postmenopausal women with osteoporosis: results from the multiple outcomes of raloxifene evaluation study. Arthritis Rheum. 2001;44(11):2611–2619. doi:10.1002/1529-0131(200111)44:11<2611::aid-art441>3.0.co;2-n
4. Kim DH, Vaccaro AR. Osteoporotic compression fractures of the spine; current options and considerations for treatment. Spine J. 2006;6(5):479–487. doi:10.1016/j.spinee.2006.04.013
5. Galibert P, Deramond H, Rosat P, Le Gars D. Note préliminaire sur le traitement des angiomes vertébraux par vertébroplastie acrylique percutanée [Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty]. Neurochirurgie. 1987;33(2):166–168.
6. Jensen ME, Evans AJ, Mathis JM, Kallmes DF, Cloft HJ, Dion JE. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. AJNR Am J Neuroradiol. 1997;18(10):1897–1904.
7. Lieberman IH, Dudeney S, Reinhardt MK, Bell G. Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine. 2001;26(14):1631–1638.
8. Hulme PA, Krebs J, Ferguson SJ, Berlemann U. Vertebroplasty and kyphoplasty: a systematic review of 69 clinical studies. Spine. 2006;31(17):1983–2001.9. doi:10.1097/01.brs.0000229254.89952.6b
9. Taylor RS, Taylor RJ, Fritzell P. Balloon kyphoplasty and vertebroplasty for vertebral compression fractures: a comparative systematic review of efficacy and safety. Spine. 2006;31(23):2747–2755. doi:10.1097/01.brs.0000244639.71656.7d
10. Wang B, Zhao CP, Song LX, Zhu L. Balloon kyphoplasty versus percutaneous vertebroplasty for osteoporotic vertebral compression fracture: a meta-analysis and systematic review. J Orthop Surg Res. 2018;13(1):264. doi:10.1186/s13018-018-0952-5
11. Ratliff J, Nguyen T, Heiss J. Root and spinal cord compression from methylmethacrylate vertebroplasty. Spine. 2001;26(13):E300–E302. doi:10.1097/00007632-200107010-00021
12. Lee BJ, Lee SR, Yoo TY. Paraplegia as a complication of percutaneous vertebroplasty with polymethylmethacrylate: a case report. Spine. 2002;27(19):E419–E42213. doi:10.1097/00007632-200210010-00022
13. Lin EP, Ekholm S, Hiwatashi A, Westesson PL. Vertebroplasty: cement leakage into the disc increases the risk of new fracture of adjacent vertebral body. AJNR Am J Neuroradiol. 2004;25(2):175–180.
14. Ryu KS, Park CK, Kim MC, Kang JK. Dose-dependent epidural leakage of polymethylmethacrylate after percutaneous vertebroplasty in patients with osteoporotic vertebral compression fractures. J Neurosurg. 2002;96(1):56–61. doi:10.3171/spi.2002.96.1.0056
15. Jang JS, Lee SH, Jung SK. Pulmonary embolism of polymethylmethacrylate after percutaneous vertebroplasty: a report of three cases. Spine. 2002;27(19):E416–E418. doi:10.1097/00007632-200210010-00021
16. Schmidt R, Cakir B, Mattes T, Wegener M, Puhl W, Richter M. Cement leakage during vertebroplasty: an underestimated problem? Eur Spine J. 2005;14(5):466–473. doi:10.1007/s00586-004-0839-5
17. Knight MTN, Jago I, Norris C, Midwinter L, Boynes C. Transforaminal endoscopic lumbar decompression & foraminoplasty: a 10 year prospective survivability outcome study of the treatment of foraminal stenosis and failed back surgery. Int J Spine Surg. 2014;8:21. doi:10.14444/1021
18. Ahn Y. Endoscopic spine discectomy: indications and outcomes. Int Orthop. 2019;43(4):909–916. doi:10.1007/s00264-018-04283-w
19. Yeung A, Lewandrowski KU. Five-year clinical outcomes with endoscopic transforaminal foraminoplasty for symptomatic degenerative conditions of the lumbar spine: a comparative study of inside-out versus outside-in techniques. J Spine Surg. 2020;6(suppl 1):S66–S83. doi:10.21037/jss.2019.06.08
20. Wagner R, Telfeian AE, Iprenburg M, et al. Transforaminal endoscopic solution to a kyphoplasty complication: technical note. World Neurosurg. 2016;91:195–198. doi:10.1016/j.wneu.2016.04.013
21. Yu Q, Chen L, Yan Z, Chu L, Shi L, Deng Z. Effectiveness of percutaneous endoscopic technique in treatment of intraspinal cement leakage after percutaneous vertebroplasty. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2017;31(6):690–695. doi:10.7507/1002-1892.201612139
22. Chu L, Yang JS, Yu KX, Chen CM, Hao DJ, Deng ZL. Percutaneous endoscopic retrieval of intraspinal cement leakage: technical note. World Neurosurg. 2018;118:150–155. doi:10.1016/j.wneu.2018.07.044
23. Wu C, Lee CY, Huang TJ, Wu MH. Full-endoscopic lumbar foraminoplasty for symptomatic cement leakage with exiting nerve root impingement. World Neurosurg. 2019;132:253–257. doi:10.1016/j.wneu.2019.09.007
24. Philips GAC, Oshima Y, Inoue H, et al. Full-endoscopic spine surgery for radiculopathy after osteoporotic vertebral compression fractures: a case report. J Spine Surg. 2020;6(2):466–471. doi:10.21037/jss.2019.10.11
25. Yu Q, Shi L, Xu Z, et al. Therapeutic effectiveness of percutaneous endoscopic spinal surgery for intraspinal cement leakage following percutaneous vertebroplasty: an early clinical study of 12 cases. Pain Physician. 2020;23(4):E377–E388.
26. Jing Z, Li L, Song J. Delayed neurological deficits caused by cement extravasation following vertebroplasty: a case report. J Int Med Res. 2021;49(6):3000605211019664. doi:10.1177/03000605211019664
27. Ahn Y, Rhee DY. Transforaminal endoscopic lumbar foraminotomy for iatrogenic foraminal stenosis following vertebroplasty. Neurospine. 2024;21(4):1137–1140. doi:10.14245/ns.2449052.526
28. Bu J, He Y, Wang Z, et al. Clinical study on percutaneous spinal endoscopic treatment for new-onset lumbosacral pain following vertebral augmentation procedures. World Neurosurg. 2026;205:124722. doi:10.1016/j.wneu.2025.124722
29. Munn Z, Barker TH, Moola S, et al. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evid Synth. 2020;18(10):2127–2133. doi:10.11124/JBISRIR-D-19-00099
30. Nieuwenhuijse MJ, Van Erkel AR, Dijkstra PDS. Cement leakage in percutaneous vertebroplasty for osteoporotic vertebral compression fractures: identification of risk factors. Spine J. 2011;11(9):839–848. doi:10.1016/j.spinee.2011.07.027
31. Ding J, Zhang Q, Zhu J, et al. Risk factors for predicting cement leakage following percutaneous vertebroplasty for osteoporotic vertebral compression fractures. Eur Spine J. 2016;25(11):3411–3417. doi:10.1007/s00586-015-3923-0
32. Zhan Y, Jiang J, Liao H, Tan H, Yang K. Risk factors for cement leakage after vertebroplasty or kyphoplasty: a meta-analysis of published evidence. World Neurosurg. 2017;101:633–642. doi:10.1016/j.wneu.2017.01.124
33. Kallmes DF, Comstock BA, Heagerty PJ, et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med. 2009;361(6):569–579. doi:10.1056/NEJMoa0900563
34. Ren H, Shen Y, Zhang YZ, et al. Correlative factor analysis on the complications resulting from cement leakage after percutaneous kyphoplasty in the treatment of osteoporotic vertebral compression fracture. J Spinal Disord Tech. 2010;23(7):e9–e15. doi:10.1097/BSD.0b013e3181c0cc94
35. Zhu SY, Zhong ZM, Wu Q, Chen JT. Risk factors for bone cement leakage in percutaneous vertebroplasty: a retrospective study of four hundred and eighty five patients. Int Orthop. 2016;40(6):1205–1210. doi:10.1007/s00264-015-3102-2
36. Fu Z, Hu X, Wu Y, Zhou Z. Is there a dose-response relationship of cement volume with cement leakage and pain relief after vertebroplasty? Dose Response. 2016;14(4):1559325816682867. doi:10.1177/1559325816682867
37. Trout AT, Kallmes DF, Kaufmann TJ. New fractures after vertebroplasty: adjacent fractures occur significantly sooner. AJNR Am J Neuroradiol. 2006;27(1):217–223.
38. Chen WC, Tsai SHL, Goyal A, Fu TS, Lin TY, Bydon M. Comparison between vertebroplasty with high or low viscosity cement augmentation or kyphoplasty in cement leakage rate for patients with vertebral compression fracture: a systematic review and network meta-analysis. Eur Spine J. 2021;30(9):2680–2690. doi:10.1007/s00586-020-06636-9
39. Tabanli A, Yilmaz H, Benek HB, et al. Incidence of new fractures in patients treated with kyphoplasty/vertebroplasty or conservative methods. Medicina. 2025;61(11):2012. doi:10.3390/medicina61112012
40. Belkoff SM, Molloy S. Temperature measurement during polymerization of polymethylmethacrylate cement used for vertebroplasty. Spine. 2003;28(14):1555–1559. doi:10.1097/01.BRS.0000076829.54235.9F
41. Zhao QL, Hou KP, Wu ZX, Xiao L, Xu HG. Full-endoscopic spine surgery treatment of lumbar foraminal stenosis after osteoporotic vertebral compression fractures: a case report. World J Clin Cases. 2022;10(2):656–662. doi:10.12998/wjcc.v10.i2.656
42. Park JH, Kim HS, Kim SW. Cement leakage into adjacent vertebral body following percutaneous vertebroplasty. Korean J Spine. 2016;13(2):74–76. doi:10.14245/kjs.2016.13.2.74
43. Beynon R, Elwenspoek MMC, Sheppard A, et al. The utility of diagnostic selective nerve root blocks in the management of patients with lumbar radiculopathy: a systematic review. BMJ Open. 2019;9(4):e025790. doi:10.1136/bmjopen-2018-025790
44. Cavka M, Delimar D, Rezan R, et al. Complications of percutaneous vertebroplasty: a pictorial review. Medicina. 2023;59(9):1536. doi:10.3390/medicina59091536
45. Knight M, Goswami A. Management of isthmic spondylolisthesis with posterolateral endoscopic foraminal decompression. Spine. 2003;28(6):573–581. doi:10.1097/01.BRS.0000050400.16499.ED
46. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. Spine. 2008;33(9):931–939. doi:10.1097/BRS.0b013e31816c8af7
47. Ahn Y, Park HB, Son S, Yoo BR. Clinical efficacy of extended transforaminal endoscopic lumbar foraminotomy compared with the conventional technique. J Clin Med. 2025;14(18):6446. doi:10.3390/jcm14186446
48. Zhang L, Wang J, Feng X, et al. A comparison of high viscosity bone cement and low viscosity bone cement vertebroplasty for severe osteoporotic vertebral compression fractures. Clin Neurol Neurosurg. 2015;129:10–16. doi:10.1016/j.clineuro.2014.11.018
49. Luo AJ, Liao JC, Chen LH, Lai PL. High viscosity bone cement vertebroplasty versus low viscosity bone cement vertebroplasty in the treatment of mid-high thoracic vertebral compression fractures. Spine J. 2022;22(4):524–534. doi:10.1016/j.spinee.2021.12.013
50. Verlaan JJ, van Helden WH, Oner FC, Verbout AJ, Dhert WJ. Balloon vertebroplasty with calcium phosphate cement augmentation for direct restoration of traumatic thoracolumbar vertebral fractures. Spine. 2002;27(5):543–548. doi:10.1097/00007632-200203010-00021
51. Nakano M, Hirano N, Ishihara H, Kawaguchi Y, Matsuura K. Calcium phosphate cement leakage after percutaneous vertebroplasty for osteoporotic vertebral fractures: risk factor analysis for cement leakage. J Neurosurg Spine. 2005;2(1):27–33. doi:10.3171/spi.2005.2.1.0027
52. Lim TH, Brebach GT, Renner SM, et al. Biomechanical evaluation of an injectable calcium phosphate cement for vertebroplasty. Spine. 2002;27(12):1297–1302. doi:10.1097/00007632-200206150-00010
53. Demir-Oğuz Ö, Boccaccini AR, Loca D. Injectable bone cements: what benefits the combination of calcium phosphates and bioactive glasses could bring? Bioact Mater. 2022;19:217–236. doi:10.1016/j.bioactmat.2022.04.007
54. Saravi B, Zink A, Ülkümen S, Couillard-Despres S, Lang G, Hassel F. Artificial intelligence-based analysis of associations between learning curve and clinical outcomes in endoscopic and microsurgical lumbar decompression surgery. Eur Spine J. 2024;33(11):4171–4181. doi:10.1007/s00586-023-08084-7
55. Ahn Y. Full-endoscopic spine surgery: its roles and limitations. J Korean Neurosurg Soc. 2025;68(5):511–527. doi:10.3340/jkns.2024.0227
56. Joshi RS, Lau D, Ames CP. Artificial intelligence and the future of spine surgery. Neurospine. 2019;16(4):637–639. doi:10.14245/ns.1938410.205
57. Hahn BS, Park JY. Incorporating new technologies to overcome the limitations of endoscopic spine surgery: navigation, robotics, and visualization. World Neurosurg. 2021;145:712–721. doi:10.1016/j.wneu.2020.06.188
58. Schmidt BT, Chen KT, Kim J, Brooks NP. Applications of navigation in full-endoscopic spine surgery. Eur Spine J. 2024;33(2):429–437. doi:10.1007/s00586-023-07918-8
59. Scheer JK, Ames CP. Artificial intelligence in spine surgery. Neurosurg Clin N Am. 2024;35(2):253–262. doi:10.1016/j.nec.2023.11.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bone Cements Used in Vertebral Augmentation: A State-of-the-art Narrative Review
Williams TD, Adler T, Smokoff L, Kaur A, Rodriguez B, Prakash KJ, Redzematovic E, Baker TS, Rapoport BI, Yoon ES, Beall DP, Dordick JS, De Leacy RA
Journal of Pain Research 2024, 17:1029-1040
Published Date: 13 March 2024
Intradural Bone Cement Leakage After Vertebroplasty, An Under-Recognized Potential Catastrophe: A Case Report
Liao W, Hou Z, Gao Y
International Medical Case Reports Journal 2025, 18:1063-1069
Published Date: 22 August 2025