Back to Journals » International Medical Case Reports Journal » Volume 18
Intradural Bone Cement Leakage After Vertebroplasty, An Under-Recognized Potential Catastrophe: A Case Report
Received 18 April 2025
Accepted for publication 15 August 2025
Published 22 August 2025 Volume 2025:18 Pages 1063—1069
DOI https://doi.org/10.2147/IMCRJ.S535207
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gates Colbert
Wensheng Liao,1,* Zhenxing Hou,2,* Yanzheng Gao1
1Department of Spine and Spinal Cord Surgery, Henan Provincial People’s Hospital, Zhengzhou, People’s Republic of China; 2Department of Spine and Spinal Cord Surgery, Henan University People’s Hospital, Zhengzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanzheng Gao, Department of Spinal Cord Surgery, Henan Provincial People’s Hospital, No. 7, Weiwu Road, Zhengzhou, Henan, 450003, People’s Republic of China, Email [email protected]
Abstract: Osteoporotic vertebral compression fracture (OVCF) is a common complication of osteoporosis, often resulting in vertebral collapse, chronic pain, and increased mortality. Vertebroplasty (VP) is a minimally invasive procedure used to alleviate pain by injecting bone cement into fractured vertebrae. However, bone cement leakage is a frequent complication, typically occurring in the extradural space with minimal clinical symptoms. In contrast, intradural cement leakage is rare but can lead to severe consequences such as neural compression and neurological deficits, necessitating urgent intervention. We present a case of a 70-year-old woman who developed intradural cement leakage after VP for a T12 compression fracture. The patient experienced immediate lower limb weakness, numbness, sensory loss, and urinary/defecation dysfunction following the procedure. MRI revealed posterior cement leakage compressing the spinal cord at the T12 level. She underwent surgical decompression and cement removal at our institution, including posterior fixation from T11 to L1, total laminectomy, and durotomy. Due to intraoperative neurophysiological monitoring, complete removal of intradural cement was not achieved. Postoperatively, the patient showed gradual improvement in lower limb muscle strength and sensory function, with near-complete recovery at one-month follow-up. Consequently, to prevent intradural cement leakage, surgeons must be vigilant about this rare complication and perform precise puncture and cautious cement injection. In cases of catastrophic leakage, prompt cement removal and thorough spinal canal decompression are essential. Preoperative CT imaging is crucial for confirming intradural leakage and planning precise surgery to reduce risks and improve outcomes.
Keywords: kyphoplasty, vertebroplasty, spinal fractures, intraoperative complication, bone cements
Introduction
Osteoporotic vertebral compression fracture (OVCF) is a common consequence of osteoporosis, leading to vertebral collapse, chronic pain, and increased mortality.1 Vertebroplasty (VP) is a minimally invasive procedure that involves injecting bone cement into the fractured vertebrae to alleviate pain. However, the use of bone cement may lead to complications such as cement embolism syndrome, cement leakage, pulmonary embolism, infection, and allergic reactions. The most common complications of bone cement are bone cement leakage and bone cement implantation syndrome (BCIS). This syndrome can lead to increased intraoperative mortality and morbidity, with specific manifestations including hypotension, pulmonary embolism, and cardiovascular reactions, among others.2 During the polymerization of bone cement, heat is released, and its monomer components can dilate blood vessels, leading to a drop in blood pressure. Meanwhile, when bone cement is injected into the medullary cavity, substances such as fat in the medullary cavity may enter the bloodstream to form emboli, triggering pulmonary embolism. Besides, cement leakage is also one of the most common complications,3 primarily occurring in the extradural space, and often presents without clinical symptoms. In contrast, intradural bone cement leakage is extremely rare (1.08%),4 but it can lead to severe consequences such as neural compression and neurological deficits, necessitating urgent intervention.5 Despite its rarity, clinicians must remain vigilant and take preventive measures to minimize the risk of this complication. This study presents a case of intraspinal cement leakage after VP.
Case Report
A 70-year-old woman visited a local hospital after a fall, where a CT scan revealed a T12 OVCF. (Figure 1a). The patient immediately felt lower limb weakness, numbness, sensory reduction, and urinary and defecation disorders after undergoing VP surgery (Figure 1b and c). Then, she was transferred to a higher-level local hospital, and MRI (Magnetic Resonance Imaging) showed: cement leakage posteriorly into the spinal canal, directly compressing the spinal cord at T12 vertebra level (Figure 1d and e); CT showed T12 spinal stenosis (Figure 1f), and at T12 vertebral body level showing cement leakage along a needle pathway from the medial to the posterior wall of a vertebral body (Figure 1g and h). Finally, she was transported to our hospital and physical examination showed: skin sensation below the T12 level was reduced, and perineal sensation was reduced. She had quadriceps strength of 2/1 (left/right) and 0 in other lower limb muscles. The CT of Our hospital showed a large amount of cement leakage into the spinal canal, causing thoracic spinal stenosis at the T12 level.
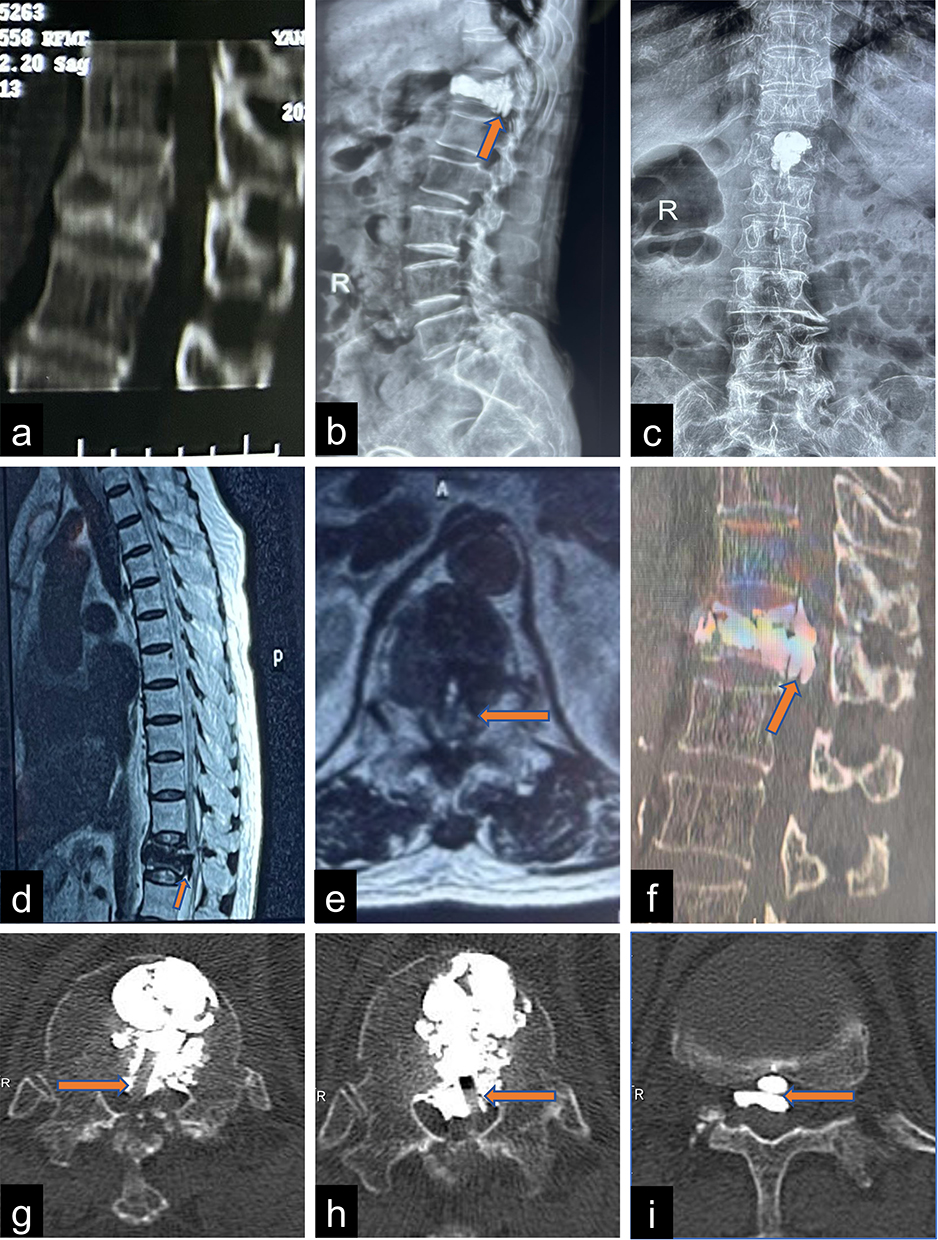 |
Figure 1 CT after the patient’s fall showed a compression fracture of the T12 vertebra (a). Post-vertebroplasty X-ray showed cement leakage into the spinal canal and the inferior edge of the T12 vertebra (b and c). Post-vertebroplasty MRI demonstrated cement leakage posteriorly into the spinal canal, directly compressing the spinal cord at the T12 level (d and e). Preoperative CT for revision surgery showed a large amount of cement at the posterior edge of the T12 vertebra (f). Before revision surgery, CT showed cement leakage from the medial wall to the posterior wall of the T12 vertebral body. Additionally, a clear needle pathway left from a failed puncture during a previous VP was visible (g and h). Before revision surgery, CT also demonstrated the layering phenomenon of cement within the spinal canal (i). |
Procedural Surgery
Subsequently, the patient underwent surgical decompression and removal of bone cement. Intraoperative fluoroscopy showed satisfactory positioning of the localization needle (Figure 2a and b). Then, stabilization by a posterior fixation from T11 to L1 was done (Figure 2c and d). Given the observation of a rounded mass of bone cement within the spinal canal during the procedure using C-arm fluoroscopy, we suspected that the bone cement might have leaked into the intradural space. After that, the patient underwent total laminectomy and durotomy through a posterior approach (Figure 2e). It is worth noting that during the removal of intradural cement, due to the risk of nerve injury suggested by intraoperative neurophysiological monitoring, the surgery did not completely remove all the intradural cement (The bone cement at the cauda equina and conus medullaris was not completely removed). (Figure 2f and g). Figure 2h and i show that a large amount of bone cement has been removed from both the intradural and extradural spaces.
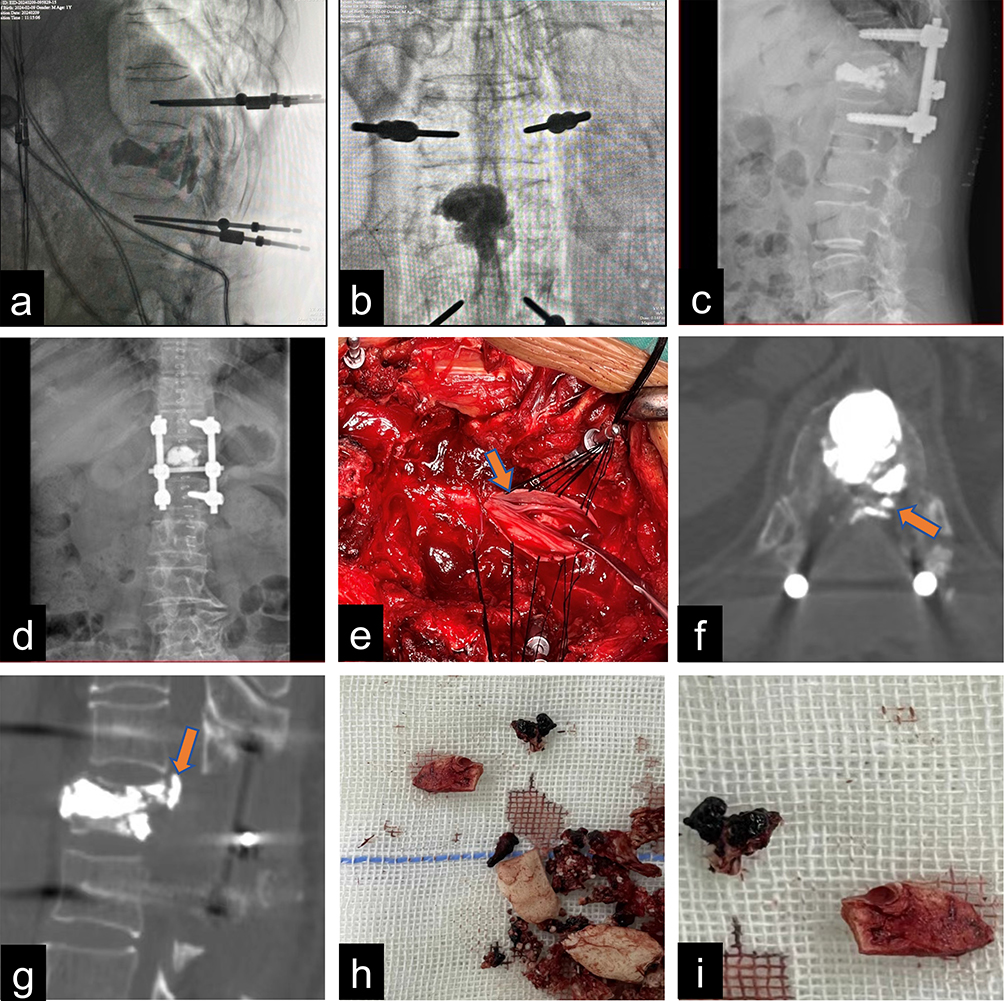 |
Figure 2 Intraoperative fluoroscopy during the revision surgery showed good positioning of the localization needle (a and b). At 9 days postoperatively, X-ray showed that the patient underwent internal fixation from T11 to L1 (c and d). Intraoperative incision of the dura mater and removal of the cement block (e). At 9 days postoperatively, CT showed a small amount of cement still existed in the spinal canal at the T12 level, not completely removed (f and g). Cement removed from the intervertebral space and epidural space (h). Cement removed from within the dural sac, measuring approximately 8×4 mm (i). |
Procedural Outcome
On the first day after the surgery, the patient reported that the pain and numbness in the lower limbs were slightly relieved compared to before the surgery. The muscle strength in the right lower limb was as follows: iliopsoas muscle strength was 2−, quadriceps muscle strength was 2+, and the muscle strength of the tibialis anterior, long toe flexor, and triceps surae was 0. The muscle strength in the left lower limb was as follows: iliopsoas muscle strength was 2−, quadriceps muscle strength was 2, and the muscle strength of the tibialis anterior, long toe flexor, and triceps surae was 0. Eleven days later, the patient’s condition was stable On physical examination: the muscle tone in both upper limbs was normal; the femoral nerve stretch test, straight leg raise test, and FABER test in both lower limbs were negative; light touch and pinprick sensations were decreased from T12 to S2 bilaterally, and absent from S3 to S5 bilaterally; knee and Achilles reflexes could not be elicited bilaterally; Babinski signs were not elicited bilaterally; Hoffmann signs were negative bilaterally; abdominal reflexes were normal; and the anal sphincter reflex was diminished. The patient was then transferred to the rehabilitation department of our hospital for further treatment. At discharge, the muscle strength in the right lower limb was as follows: quadriceps muscle strength was 3−, and tibialis anterior muscle strength was 1. The muscle strength in the left lower limb was as follows: quadriceps muscle strength was 2+, with no significant changes in the remaining muscle strength. One month later, the patient returned to our hospital for a follow-up visit. The muscle strength in both lower limbs was as follows: quadriceps and triceps surae muscle strength were both 4, and bowel and bladder function had returned to normal.
Discussion
VP is an effective treatment for OVCF, offering pain relief and kyphosis correction. However, complications such as extradural cement leakage, can lead to nerve damage and multi-organ embolism.6 Intradural cement leakage, though rare (1.08%),4,5 can cause catastrophic outcomes such as paralysis and requires immediate intervention. Given its low incidence, clinicians often struggle to identify this complication and make optimal surgical decisions.
Regarding the incidence of cement leakage, a retrospective study included 245 patients, among which 176 underwent VP and 69 underwent kyphoplasty (KP), showing that the occurrence of cement leakage in the VP group and KP group were 104 cases (58.5%) and 31 cases (41.9%) respectively.7 It can be seen that cement leakage after VP or KP is quite common. However, we found that intradural cement leakage is very rare, and there are only 10 related case reports worldwide (Table 1), and all these patients without exception had severe limb weakness. Although they underwent surgery, the muscle power of the patients was often not fully restored to normal at the last follow-up.
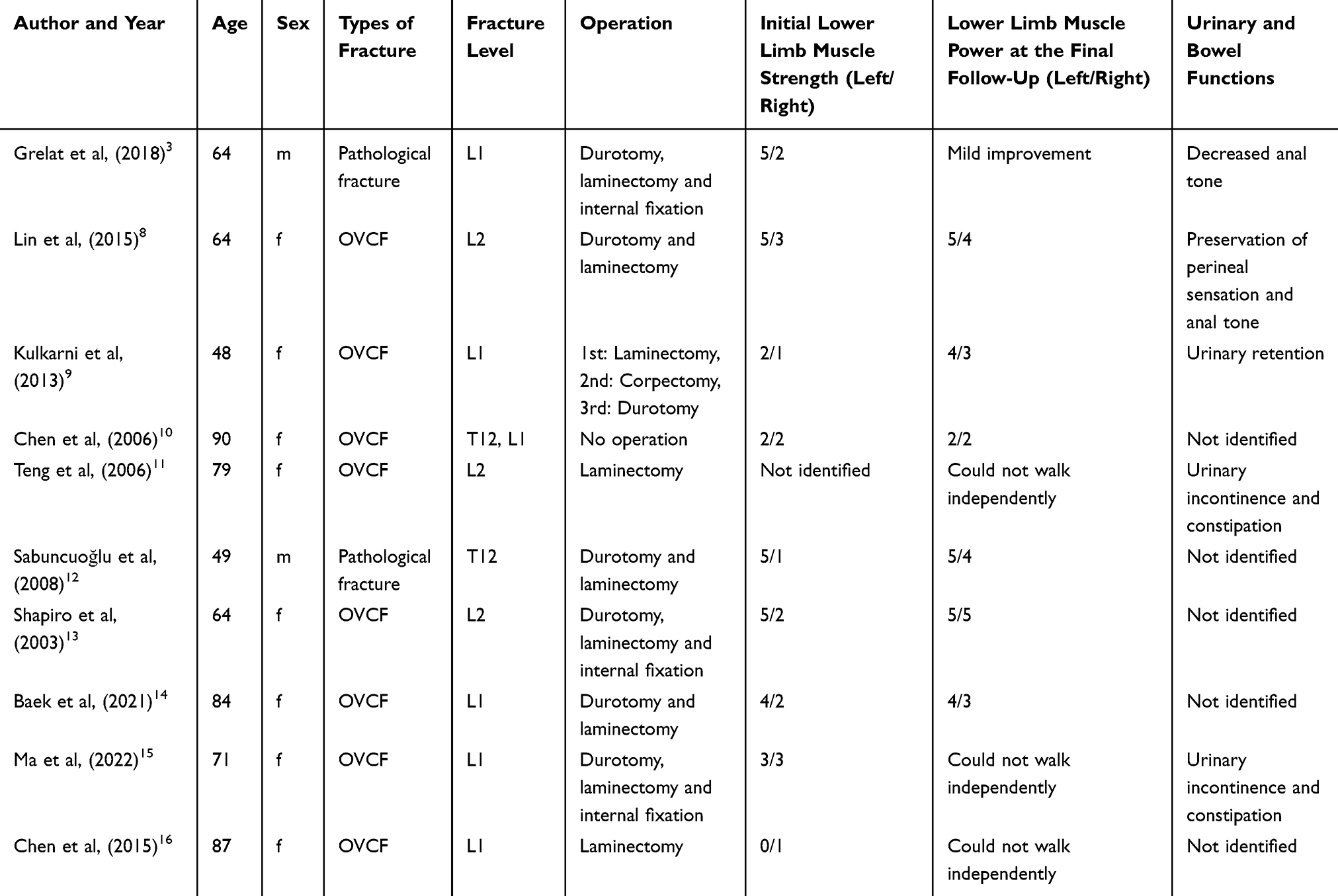 |
Table 1 Previously Reported Cases of Intradural Bone Cement Leakage (m=male, f=female) |
Currently, cases of intradural bone cement leakage showed that most patients underwent durotomy, laminectomy, or short segmental fixation to treat intradural cement leakage, and their neurologic deficits were significantly improved after surgery. Only 1 case patient refused surgery due to old age, and her sensory abnormalities and lower limb weakness and other symptoms still persisted after 4 months.10 In our study, we removed as much intradural cement as possible through durotomy to thoroughly decompress the spinal canal and performed short segmental fixation to further enhance spinal stability. The patient’s lower limb muscle power was basically restored to grade 4, and neurologic deficit symptoms gradually disappeared. Therefore, in the face of intradural cement leakage, we suggest that surgery for decompression and removal of cement should be performed according to the specific situation of the patient.
Preventing cement leakage starts with understanding its causes. A researcher highlighted that needle tip penetration into the spinal canal’s dura mater is a risk.14 In addition, multiple studies8,9,12,13,16 have identified deviations in puncture direction, improper cement injection techniques, and abnormal vertebral structure as significant factors contributing to intradural cement leakage. Our study identified three main causes: puncture errors damaging the dura mater, excessive cement injection, and failure to promptly detect leakage via lateral X-ray. As seen from the axial CT images (Figure 1g and h), there are clear repeated puncture needle path marks. There are puncture marks on both sides, indicating that after one side failed, the puncture needle was withdrawn and another attempt was made from the other side to inject bone cement. However, both puncture paths show that the puncture site was too far to the medial side, which may have directly led to dural damage and ultimately caused intradural bone cement leakage. In addition, the puncture angle (the angle between the puncture needle and the midline) during the initial surgery was too large, which further caused the puncture needle to deviate to the medial side. How can we prevent intradural cement leakage? First, on the lateral X-ray, the needle tip should be carefully punctured before it reaches the posterior cortex of the vertebral body, and avoid going beyond the medial edge of the pedicle on the frontal position X-ray, which can effectively prevent errors.11 Second, Ma et al believed that cement should be injected to the anterior 2/3 of the vertebra, and it must be stopped when the cement flows into the posterior 1/3 of the vertebra.15 Third, Guo et al suggested that cement of toothpaste viscosity was not easy to penetrate the venous drainage of the spine through sparse trabeculae, and this helped to prevent the occurrence of bone cement leakage.17
This study indicates that when X-ray suggests intradural cement leakage and the patient exhibits neurological deficits, prompt emergency revision surgery should be considered to decompress the spinal canal and remove the cement block. Preoperative CT can differentiate intradural from extradural leakage based on four key points: (1) The puncture site is on the inner side; (2) Layering phenomena (Figure 1i) (gaps between cement) on CT; (3) No cement is found outside the dura during surgery but is visible on X-ray; (4) The blunt shape of cement matches the contour of the dural sac. This study first identifies the CT layering phenomenon, which is crucial for diagnosis and surgical planning.
In the treatment of vertebral compression fractures, non-surgical alternatives and surgical treatments (VP and KP) each have their own characteristics in preventing leakage. Conservative treatment is suitable for mild leakage, involving bed rest, head elevation, and antibiotic prophylaxis to reduce pressure on the leakage site and minimize the risk of infection. However, due to individual differences and the causes of leakage, the treatment period is long and the outcomes are unstable VP stabilizes the fracture by injecting bone cement into the fractured vertebra, but it cannot restore vertebral height or shape. If performed improperly, the risk of cement leakage is high, especially when the posterior wall of the vertebra is compromised, making it more likely for cement to leak into the spinal canal. Preoperative assessment of the fracture using CT or MRI is necessary, and during the procedure, attention should be paid to puncture site, injection speed control, and close monitoring. KP not only repairs the fracture but also restores vertebral height and shape. It first creates a cavity within the vertebra using a balloon catheter, reducing the pressure of cement injection and effectively decreasing the risk of leakage compared to VP. Overall, conservative treatment is suitable for mild leakage, while VP and KP each have their own advantages. All three approaches require emphasis on preoperative assessment and procedural details. Further research is needed in the future to optimize treatment protocols, reduce leakage risks, and improve therapeutic outcomes.
Conclusion
To prevent intradural cement leakage after VP, surgeons must be aware of this rare complication and perform precise puncture and cautious cement injection. In case of catastrophic leakage, prompt cement removal and thorough spinal canal decompression are required. For revision surgery, preoperative CT imaging should confirm whether cement has leaked into the dura mater. This assessment is vital for planning precise surgery, reducing risks, and improving outcomes. Future research should focus on developing more sensitive intraoperative monitoring techniques. For instance, real-time imaging modalities with higher resolution could be explored to detect early signs of bone cement leakage during the procedure. Additionally, further investigation into the biomechanics of the vertebral body during and after VP is needed. Understanding how different factors (such as patient bone quality, the location of the treated vertebra, and the volume of cement injected) affect the overall spinal stability can help optimize surgical techniques. Long-term follow-up studies are also essential to assess the durability of repairs and the incidence of late-onset complications, including the potential impact of bone cement on adjacent vertebral segments over time.
Ethics Statement
A written informed consent has been obtained from the patient to allow the publication of the case details and any accompanying images. According to the regulations of Henan Provincial People’s Hospital’s ethics committee, case reports do not require approval.
Funding
This study is supported by Henan Association for Science and Technology, Innovation and Collaboration Service Platform of Science and Technology in Central Plains (2023KCZY336).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kim DH, Vaccaro AR. Osteoporotic compression fractures of the spine; current options and considerations for treatment. Spine J. 2006;6(5):479–487. doi:10.1016/j.spinee.2006.04.013
2. Moldovan F. Bone cement implantation syndrome: a rare disaster following cemented hip arthroplasties-clinical considerations supported by case studies. J Pers Med. 2023;13(9):1381. doi:10.3390/jpm13091381
3. Grelat M, Le Van T, Fahed E, Beaurain J, Madkouri R. Rare complication of percutaneous technique: intradural cement leakage and its surgical treatment. World Neurosurg. 2018;118:97. doi:10.1016/j.wneu.2018.07.045
4. Lee BJ, Lee SR, Yoo TY. Paraplegia as a complication of percutaneous vertebroplasty with polymethylmethacrylate: a case report. Spine. 2002;27(19):E419–422. doi:10.1097/00007632-200210010-00022
5. Yaltirik K, Ashour AM, Reis CR, Özdoğan S, Atalay B. Vertebral augmentation by kyphoplasty and vertebroplasty: 8 years experience outcomes and complications. J Craniovertebr Junction Spine. 2016;7(3):153–160. doi:10.4103/0974-8237.188413
6. Jay B, Ahn SH. Vertebroplasty. Semin Intervent Radiol. 2013;30(3):297–306. doi:10.1055/s-0033-1353483
7. Ding Y, Dong S, Wang J, et al. Comparison between hyperextension and neutral positions for vertebroplasty and kyphoplasty: which is best for osteoporotic vertebral compression fractures? J Pain Res. 2020;13:2509–2518. doi:10.2147/jpr.S268610
8. Lin BJ, Li CC, Ma HI. Intradural cement leakage after percutaneous vertebroplasty. Turk Neurosurg. 2015;25(6):940–942. doi:10.5137/1019-5149.Jtn.11079-14.1
9. Kulkarni AG, Shah SP, Deopujari CE. Epidural and intradural cement leakage following percutaneous vertebroplasty: a case report. J Orthop Surg. 2013;21(3):365–368. doi:10.1177/230949901302100320
10. Chen YJ, Tan TS, Chen WH, Chen CC, Lee TS. Intradural cement leakage: a devastatingly rare complication of vertebroplasty. Spine. 2006;31(12):E379–382. doi:10.1097/01.brs.0000219495.57470.67
11. Teng MM, Cheng H, Ho DM, Chang CY. Intraspinal leakage of bone cement after vertebroplasty: a report of 3 cases. AJNR Am J Neuroradiol. 2006;27(1):224–229.
12. Sabuncuoğlu H, Dinçer D, Güçlü B, et al. Intradural cement leakage: a rare complication of percutaneous vertebroplasty. Acta Neurochir. 2008;150(8):811–815. doi:10.1007/s00701-008-1503-3
13. Shapiro S, Abel T, Purvines S. Surgical removal of epidural and intradural polymethylmethacrylate extravasation complicating percutaneous vertebroplasty for an osteoporotic lumbar compression fracture. Case report. J Neurosurg. 2003;98(1 Suppl):90–92. doi:10.3171/spi.2003.98.1.0090
14. Baek IH, Park HY, Kim KW, Jang TY, Lee JS. Paraplegia due to intradural cement leakage after vertebroplasty: a case report and literature review. BMC Musculoskelet Disord. 2021;22(1):741. doi:10.1186/s12891-021-04625-7
15. Ma QH, Liu GP, Sun Q, Li JG. Delayed complications of intradural cement leakage after percutaneous vertebroplasty: a case report. World J Clin Cases. 2022;10(25):8998–9003. doi:10.12998/wjcc.v10.i25.8998
16. Chen CH, Chuang MT, Wang CK. Intradural cement leakage after vertebroplasty. Spine J. 2015;15(6):1493–1494. doi:10.1016/j.spinee.2015.03.025
17. Guo HZ, Tang Y-C, Guo D-Q, et al. The cement leakage in cement-augmented pedicle screw instrumentation in degenerative lumbosacral diseases: a retrospective analysis of 202 cases and 950 augmented pedicle screws. Eur Spine J. 2019;28(7):1661–1669. doi:10.1007/s00586-019-05985-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Current Evidence and Clinical Implications of Full-Endoscopic Spine Surgery for Post-Vertebroplasty Lumbar Radiculopathy: A Comprehensive Review
Ahn Y, Lee S, Lee CW
Journal of Pain Research 2026, 19:600821
Published Date: 11 April 2026