Back to Journals » Journal of Pain Research » Volume 16
Cultural Adaptation, Reliability and Validation of the Arabic Örebro Musculoskeletal Pain Questionnaire in Patients with Low Back Pain
Authors Alanazi F ![]() , Alrwaily M
, Alrwaily M
Received 1 June 2022
Accepted for publication 17 January 2023
Published 1 February 2023 Volume 2023:16 Pages 317—325
DOI https://doi.org/10.2147/JPR.S375202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Fahad Alanazi,1 Muhammad Alrwaily2
1Department of Physical Therapy and Health Rehabilitation, College of Applied Medical Sciences, Jouf University, Sakaka, Jouf Region, Saudi Arabia; 2Division of Physical Therapy, School of Medicine, West Virginia University, Morgantown, WV, USA
Correspondence: Fahad Alanazi, Department of Physical Therapy and Health Rehabilitation, College of Applied Medical Sciences, Jouf University, Sakaka, Jouf Region, Saudi Arabia, Email [email protected]
Background: The Örebro Musculoskeletal Pain Questionnaire (ÖMPQ) assesses the psychosocial factors in people with complaints of musculoskeletal disorders and predicts those likely to develop persistent symptoms.
Objective: To culturally-adapt and assess the validity of the ÖMPQ in an Arabic population with low back pain (LBP).
Methods: This was a prospective cohort validation study of the ÖMPQ. The Arabic-ÖMPQ was created by forward translation, translation synthesis and backward translation in an Arabic population. Participants were included if they were 18 years or older, had acute or chronic LBP and were fluent in Arabic. Eighty-four patients completed the questionnaires at baseline, 2 days later and 3 months follow-up. We assessed specific agreement and test–retest reliability using the interclass correlation coefficient (ICC). We assessed predictive validity using linear regression and relative risk. We assessed content validity by investigating the ceiling and floor effects.
Results: To construct validity, the Arabic-ÖMPQ had a moderate (r≥ 0.3, < 0.5) to high (r≥ 0.5) correlation with pain, disability, fear-avoidance and catastrophizing questionnaires. The test-rest reliability was high ICC2,1=0.92 (95% CI: 0.83– 0.96). The Arabic-ÖMPQ score at baseline can significantly predict disability at 3 months F(1,82)=33.87, p< 0.01; R2=0.29.
Conclusion: The translation of the Arabic-ÖMPQ into Arabic was successful. The Arabic-ÖMPQ showed very good reliability and proper validity and thus can be used to predict the risk of developing persistent disability amongst patients with LBP in an Arabic population.
Keywords: low back pain, Örebro Musculoskeletal Pain Questionnaire, Arabic, cultural adaptation, validation
Introduction
Low back pain (LBP) is a common worldwide health problem. It affects 40% of individuals at some point in their life,1 and is a leading cause of disability and health-care financial burden.2 In the Arab region (22 countries), LBP-related disability has reached levels similar to those of the Western world.3 Among high-income Arab countries (six countries), LBP is ranked the fourth reason for years lost due to disability.3 In Saudi Arabia, LBP may be affecting 53% to 79% of people,4 and it is also considered the third leading cause of disability after motor vehicle accidents and diabetes.2 Due to the rapid rise of such conditions, the Ministry of Health in Saudi Arabia through the World Health Organization Regional Office has called for programs and policies to reduce the burden of chronic diseases in all countries in the Eastern Mediterranean.3
Given the huge burden of LBP in Saudi Arabia, it is important that primary care clinicians are able to identify patients at risk of developing persistent symptoms and make early referrals to physical therapy. In Saudi Arabia, patients with spinal disorders represent 28.1% of referrals to physical therapy clinics, of which 53.1% are due to LBP.5 From the time of referral, it seems that patients who took 16 days or more till their first physical therapy session were less likely to adhere to the treatment plan and more likely to develop persistent symptoms.6 In a Saudi community, development of persistent LBP symptoms has been associated with physical factors such as pain intensity, physical activity and body mass index, as well as psychosocial factors (ie yellow flags) such as fear-avoidance, unhelpful beliefs, poor expectation about recovery, anxiety and depression.7 These factors, despite cultural differences, are similar to those reported in the Western world.8 It is recognized that early assessment of these factors will help clinicians identify patients at risk of persistent disability and direct them to the optimal path of care early.9
One tool that to assist in the early identification of yellow flags and patients risking the development of persistent disability due to pain is the Örebro Musculoskeletal Pain Questionnaire (ÖMPQ).10 The ÖMPQ uses multiple domains to predict disability including physical factors such as pain intensity and location and psychological factors such as fear-avoidance, unhelpful beliefs, poor recovery expectations, catastrophizing, anxiety and depression. The ÖMPQ consists of 25 items of which 21 are scored. Each scored item can take a value from 1 to 10, for a total score of 210. A score of 105 or less indicates a low risk of developing persistent disability (accuracy of 95%), a score of more than 105 and less than 130 indicates a moderate risk of developing persistent disability and a score of 130 or more indicates a high risk of persistent disability (accuracy of 86%) at 6 months.10,11 In the original study, an ÖMPQ score of 90 points had a sensitivity of 89% and a specificity of 65% for absenteeism due to sickness, and a sensitivity of 74% and a specificity of 79% for functional ability.10 The ÖMPQ has been shown to have satisfactory reliability and predictive validity.10
The ÖMPQ can benefit clinicians, researchers, and patients. It can aid primary care providers in evaluating the risk of developing persistent disability upon first contact with the patient. This can help researchers design studies that account for baseline variables that predict disability or explain variability in response to intervention. It helps patients receive proper treatment that addresses the reasons for their persistent disability. Additionally, primary health-care clinics are often not equipped with trained personnel to screen for psychosocial factors associated with LBP. Furthermore, many psychosocial variables have been identified in the literature, which makes their assessment overwhelming and time-consuming. Therefore, using the ÖMPQ can offer multiple stakeholders better allocation of resources and utilization of time.
Since its release in 1998, the ÖMPQ English version has been translated, culturally adapted and validated into several languages and populations.12–15 However, there is no translation, cultural adaptation or validation in an Arabic population thus far. Arabic is one of the most commonly used languages in the world and considered one of the six official languages by the United Nations.16 Therefore, the aim of this study is to culturally-adapt and evaluate the ability of the ÖMPQ to predict disability in a primary care clinic in Saudi Arabia.
Materials and Methods
Translation of the Arabic ÖMPQ
Based on Beaton et al guidelines,17 we conducted a multistep translation of the ÖMPQ. The first step was a forward translation where two translators whose native language was Arabic and proficient in English translated the ÖMPQ into Arabic. The two Arabic translations were synthesized into a single form. The second step was backward translation, where two translators whose native language was English and proficient in Arabic translated the synthesized Arabic ÖMPQ back into English. In the third step, an expert committee was formed to examine all the translations from the forward, backward and synthesized versions, and create a prefinal version of the Arabic ÖMPQ. The expert committee consisted of two researchers and three clinicians familiar with Saudi culture who worked to resolve any discrepancy in the translation process and ensure that the prefinal version is appropriate for use in Saudi culture. The prefinal version was distributed on 23 consecutive patients at a primary care outpatient facility to examine the comprehension of each item and resolve any misinterpretation. Since there were no issues with the prefinal version, the expert committee decided to use it as the final version.
Validation of the Arabic ÖMPQ
Design
The final version of the Arabic ÖMPQ was used to test the psychometric properties in a primary care outpatient clinic in a hospital in Saudi Arabia. Participants were asked to complete questionnaires at baseline, 2 days later and then 3 months follow-up. The study was supported, for reliability and validity, by using the minimum required number of participants of 50.18 To account for dropout, we aimed to increase the number of participants to 80. This study was approved by the Office of Research Integrity and Compliance in the authors’ hospital.
Participants
The inclusion period was between March 2018 and February 2019. Participants were included if they were 18 years or older, had acute or chronic LBP and were fluent in Arabic. Participants were excluded if they had fracture, cancer, inflammatory conditions, infections, severe neurological deficits, post-surgical, psychiatric disorder or pregnant. Participants who consented to participate were asked to complete the questionnaires and then received the usual care.
The purpose of the study was explained, and informed consents were signed by all participants. The study planned to include at least 50 participants, the minimum required to measure the reliability and validity of a questionnaire adequately, according to Terwee et al.
Measurements
Session One (at Baseline)
Participants completed a demographics form, the Arabic versions of the ÖMPQ, Oswestry Disability Index (ODI),19 Numeric Pain Rating Scale (NPRS), Fear-Avoidance Behavior Questionnaire-Physical Activity and Work scales (FABQ-PA; FABQ-W),20 and the Pain Catastrophizing Scale (PCS).21
Session Two (Two Days Later)
Each participant was asked if their symptoms changed from last session? Participants were also asked to complete the Arabic NPRS and ÖMPQ again to investigate the retest reliability.
Session Three (Three Months Later)
Participants were asked to complete the Arabic versions of ODI and NPRS. They were also asked if their symptoms changed from last sessions.
Statistical Analysis
All statistical analysis was conducted using SPSS 25 (Armonk, NY: IBM Corp.). We used descriptive statistics to describe participants’ characteristics and the prevalence of the three risk profiles: low, medium, and high on the Arabic ÖMPQ.
For Construct Validity
We analyzed the characteristics of pain, disability, fear-avoidance behavior and catastrophizing across the ÖMPQ risk profile to determine the discriminant validity. We also calculated Pearson’s correlation coefficient between specific ÖMPQ items and their respective questionnaires according to each item domain. We used Bier et al,22 a priori expectations that there would be moderate (r≥0.3, <0.5) to high (r≥0.5) correlation between pain items 9, 10 and 11 with the NPRS; catastrophizing items 12, 13, 14 and 15 with PCS; fear-avoidance of physical activity items 18 and 19 with FABQ-PA scale; and fear-avoidance of work item 20 with FABQ-W scale; disability items 6, 20, 21, 22, 23, 24 and 25 with ODI. We expected a low correlation r<0.3 between items 8 (perception of work demands), 16 (expectation to return to work) and 17 (work satisfaction) with FABQ-W scale.
For Reliability
We assessed the agreement between two measurements in a group of participants whose conditions remained stable between sessions 1 and 2. We considered a stable condition when the participant responded “yes” to the question “Have your symptoms changed from the last session?” and the NPRS score did not change more than ± 1 point. We calculated the interclass coefficient (ICC2,1) and the specific agreement. The ICC2,1 was interpreted as follows: ≤0 = poor; 0.01–0.02 = slight; 0.21–0.4 = fair; 0.41–0.60 = moderate; 0.61–0.80 = substantial; and 0.81–1 = perfect. We also calculated specific agreement using a 3×3 table similar to that reported Bier et al.22
For Predictive Validity
We calculated a simple linear regression to determine whether ÖMPQ at baseline can predict ODI at 3 months. We also calculated the relative risk ratio (RR) for the medium-risk group and high-risk group relative to the low-risk group. For RR, we considered persistent disability when the ODI score at 3 months remained above the median of the baseline score.
For Content Validity
We investigated floor and ceiling effects by calculating the percentage of participants scoring 0 (floor) or 210 (ceiling). If the percentage was >15%, then floor or ceiling effect was present.
Results
We recruited 84 participants whose demographics are listed in Table 1. At baseline, 53.6% of participants were in the low-risk group, 38.1% were in the medium-risk group and 8.3% were in the high-risk group.
 |
Table 1 Demographics and Clinical Characteristics at Baseline |
For Construct Validity
It appeared that for each increase in risk profile on the ÖMPQ, there was an increase in clinical characteristics of pain, disability, fear-avoidance and catastrophizing (Table 2). Also, the Pearson’s [r] correlation between each ÖMPQ item and its corresponding clinical outcome is reported in Table 3. There was moderate to high correlation between the pain items 9, 10 and 11 with the NPRS. There was a low correlation between the catastrophizing item 12 with PCS; however, moderate to high correlation between the catastrophizing items 13, 14 and 15 with PCS. There was a high correlation between the fear-avoidance (physical activity) items 18 and 19 with FABQ-PA scale. There was a high correlation between the perception of work demands item 8 with FABQ-W scale; however, there was a low correlation between the fear-avoidance (work) item 20, expectation to return to work item 16 and work satisfaction item 17 with FABQ-W scale. There was a moderate to high correlation between the disability items 6, 21, 22, 23, 24 and 25 with ODI.
 |
Table 2 Clinical Characteristic Across Risk Profiles of Arabic-ÖMPQ |
 |
Table 3 Pearson’s Correlation Between Each Arabic-ÖMPQ Item and Outcome Measures |
For Reliability
There was 45 participants whose status was determined to be stable, so they were included in the assessment of reliability. The ICC2,1 for the ÖMPQ was 0.92 (95% CI: 0.83–0.96). The specific agreement for the low-risk group was 78.26%, medium-risk group was 71.79% and high-risk group was 40% (Table 4).
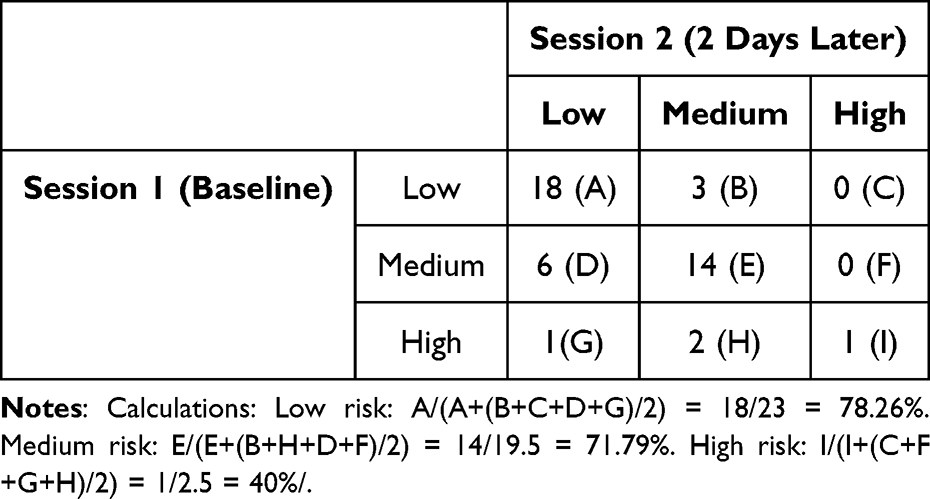 |
Table 4 Specific Agreement Between Session 1 (Baseline) and Session 2 (48 Hours Later) |
For the Predictive Validity
A simple linear regression shows that the ÖMPQ at baseline can significantly predict the ODI at 3 months F (1,82)=33.87, p<0.01; with R2 of 0.29. To calculate the RR, persistent disability at 3 months was set at or above the ODI baseline median score of 26. The RR for the medium-risk group compared with the low-risk group was 1.9 (95% CI: 1.2–3.3). The RR for the high-risk group compared with the low-risk group was 2.3 (95% CI: 0.7–7.7).
For Content Validity
We investigated the floor and ceiling and there was no participant scoring 0 (floor effect) or 210 (ceiling effect).
Discussion
This study translated the ÖMPQ into Arabic and tested its reliability and validity. The translation of the ÖMPQ was appropriate as the expert committee ensured that the items are reader-friendly and close to Saudi Arabian culture and dialect. The Arabic ÖMPQ was understood well by patients in primary care clinics, and we did not have any issues with items comprehension.
Face validity refers to whether an instrument appears to measure what it is intended to measure at face value. Since the instrument of Arabic ÖMPQ is intended to measure risk of developing persistent disability in people with LBP, its face validity can be determined by checking the domains that constitutes LBP disability. LBP disability can stem from pain, physical, and psychosocial factors; all of which appear to be included in the Arabic ÖMPQ.
Content validity refers to how well an instrument covers the aspects or spectrum of a construct. Limited content validity is indicated by the presence of more than 15% of the patients reaching either the floor (0/210 points) or ceiling effects (210/210 points) on the Arabic ÖMPQ. Since there was no participant scoring 0 (floor effect) or 210 (ceiling effect), we determined that the Arabic ÖMPQ showed good content validity.
For the construct validation, it was important that the Arabic ÖMPQ can distinguish between patients with LBP who have low, medium, or high psychosocial status. We did not use receiver operating curve because we did not want to dichotomize the scores. To that end, this study shows that for each increase in psychosocial risk status on the Arabic ÖMPQ, there was an associated increase in the outcome measures of pain, disability, fear-avoidance and catastrophizing. This suggested that the Arabic ÖMPQ had good discriminant validity between low-, medium- and high-risk groups.
Since the ÖMPQ had multiple constructs such as pain, disability, fear-avoidance and catastrophizing, we investigated if these constructs are correlated with their respective outcome measures. Similar to correlations found in other studies,12–15 the constructs within the Arabic ÖMPQ show significant moderate to high correlations with their respective outcome measures. The correlations were as expected a priori and suggest that the Arabic ÖMPQ is capable of capturing various levels of psychological factors.
There were three items in the Arabic ÖMPQ that correlated differently than what was set a priori: item 8 (perception of work demands), item 12 (pain control), and item 20 (fear-avoidance of work). Item 8 was expected to have a low correlation (r < 0.3) with FAB-W, but it was found to have a high correlation (r ≥ 0.5), suggesting a better than expected correlation between perception of work demands and fear-avoidance of work. Item 12 was expected to have at least a moderate correlation with pain catastrophizing but the correlation was low, suggesting that item 12 should be considered in light of other pain catastrophizing items 13, 14 and 15. Item 20 was expected to have at least moderate correlation with the FABQ-W but had low correlation, suggesting that items 8 and 20 should be evaluated together when assessing work demands or fear avoidance of work.
The reliability of the Arabic ÖMPQ was tested between session 1 (baseline) and session 2 (2 days later). Since LBP could change rapidly, the 2-day time interval was considered long enough to reduce recall bias and short enough to prevent substantial change in status. The reliability was tested with ICC2,1 showed perfect reliability, which was similar to the levels reported in the Norwegian and Brazilian translated versions.12,15 We also investigated specific agreements for each risk status between session 1 and 2. It appeared that for low and medium risk status, there was very good agreement. However, for the high-risk status, there was a fair agreement likely due to smaller number of participants in this category.
We investigated the predictive validity of the Arabic ÖMPQ in two ways. One, we used simple linear regression to investigate if the ÖMPQ score at baseline is predictive of the disability score on ODI at 3 months. The simple regression showed that the ÖMPQ at baseline can predict disability at 3 months and can explain 29% of the variability in disability at 3 months. Two, we used RR to determine if being in one risk category increases the chances of developing persistent disability. Participants in the medium-risk profile have 1.9 higher chance of developing persistent disability compared to the low-risk group. Also, participants in the high-risk group have 2.3 higher chances of developing disability compared to the low-risk group. The confidence interval of medium-risk and high-risk groups were overlapped, and also the confidence interval of high-risk group crossed 1. This could be due to patient receiving treatment “usual care”, or due to smaller number of participants in the high-risk group.
We recognized that the original ÖMPQ had been modified to address several limitations such as inconsistent wording, reduced practicality, and lack of independent validation.23 So, just like in Gabel et al,23 we carefully selected wording of the questions that are related to symptom duration, activity, function variables, and psychosocial constructs. Also, we attempted to divide the Arabic ÖMPQ into themed sections for ease of response and grading. However, unlike Gabel et al,23 we did not renumber the questions nor did we modify the construct “pain” to “pain/problem” or reduce the number of body regions. We did so because we were hoping that the Arabic ÖMPQ would be used for conditions other than LBP.
There were several reasons to choose the ÖMPQ for cultural adaptation and validation in Arabic population. At the time of the study, there were not validated psychosocial screening tools for Arabic people with musculoskeletal pain. Also, the ÖMPQ may be more useful clinically as the responses to its items are scaled from 0 to 10 as opposed to dichotomized with “yes” and “no”, which can help clinicians’ probe on constructs that need further assessment.24 Finally, the ÖMPQ is commonly recommended by clinical practice guidelines of LBP.25,26
Several limitations of this study can be identified. We only validated the Arabic ÖMPQ patients with LBP, and we do not know if it generalizes to other musculoskeletal cases. We only used the level disability as a predicted variable of poor outcome, and we do not know if other clinical outcomes can be predicted with Arabic ÖMPQ. Future research should investigate whether the Arabic ÖMPQ improves the delivery of healthcare and reduces its cost.
Conclusion
The Arabic ÖMPQ should be used in primary care and physical therapy clinics to assist in early screening of patients with LBP with elevated psychosocial profile and determine patients with LBP at risk of developing persistent disability. The Arabic ÖMPQ has been translated and validated for patients with LBP in primary care clinics in a Saudi Arabian population. The translation was appropriate, and the Arabic ÖMPQ showed satisfactory reproducibility, construct, content and predictive validity.
Abbreviations
FABQ-PA, Fear-Avoidance Behavior Questionnaire-Physical Activity; FABQ-W, Fear-Avoidance Behavior Questionnaire-Work; ICC, Interclass Correlation Coefficient; LBP, low back pain; NPRS, Numeric Pain Rating Scale; ODI, Oswestry Disability Index; ÖMPQ, Örebro Musculoskeletal Pain Questionnaire; PCS, Pain Catastrophizing Scale; RR, Risk Ratio.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author upon request.
Ethical Approval and Consent of Participants
This study was approved by the Office of Research Integrity and Compliance at both the Qurayyat General Hospital in Saudi Arabia and the West Virginian University School of Medicine # 1710818925. Our study complies with the Declaration of Helsinki.
Acknowledgment
We would like to thank Samuel Lee Harris, Sarah Tarabichi, Jawaher Alshalan, Alanood Alshammary, and Smar Alothman for their contribution in the translation and data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–2037. doi:10.1002/art.34347
2. Murray CJ, Barber RM, Foreman KJ, et al.; DALYs GBD, Collaborators H. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. Lancet. 2015;386(10009):2145–2191. doi:10.1016/S0140-6736(15)61340-X
3. Mokdad AH, Jaber S, Aziz MI, et al. The state of health in the Arab world, 1990–2010: an analysis of the burden of diseases, injuries, and risk factors. Lancet. 2014;383(9914):309–320. doi:10.1016/S0140-6736(13)62189-3
4. Awaji M. Epidemiology of low back pain in Saudi Arabia. J Ddv Med Pharm Sci. 2016;6(4):1–9. doi:10.9734/JAMPS/2016/24173
5. Alshami AM. Prevalence of spinal disorders and their relationships with age and gender. Saudi Med J. 2015;36(6):725–730. doi:10.15537/smj.2015.6.11095
6. Al-Eisa E. Indicators of adherence to physiotherapy attendance among Saudi female patients with mechanical low back pain: a clinical audit. BMC Musculoskelet Disord. 2010;11:124. doi:10.1186/1471-2474-11-124
7. Alamam D, Moloney N, Leaver A, Alsobayel HI, Mackey MG. Pain intensity and fear avoidance explain disability related to chronic low back pain in a Saudi Arabian Population. Spine. 2019;44(15):E889–E898. doi:10.1097/BRS.0000000000003002
8. Ramond A, Bouton C, Richard I, et al. Psychosocial risk factors for chronic low back pain in primary care--a systematic review. Fam Pract. 2011;28(1):12–21. doi:10.1093/fampra/cmq072
9. Hill JC, Whitehurst DG, Lewis M, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet. 2011;378(9802):1560–1571. doi:10.1016/S0140-6736(11)60937-9
10. Linton SJ, Boersma K. Early identification of patients at risk of developing a persistent back problem: the predictive validity of the Örebro Musculoskeletal Pain Questionnaire. Clin J Pain. 2003;19(2):80–86. doi:10.1097/00002508-200303000-00002
11. Brown G. The Orebro Musculoskeletal Pain Questionnaire. Occup Med. 2008;58(6):447–448. doi:10.1093/occmed/kqn077
12. Grotle M, Vollestad NK, Brox JI. Screening for yellow flags in first-time acute low back pain: reliability and validity of a Norwegian version of the Acute Low Back Pain Screening Questionnaire. Clin J Pain. 2006;22(5):458–467. doi:10.1097/01.ajp.0000208243.33498.cb
13. Nonclercq O, Berquin A. Predicting chronicity in acute back pain: validation of a French translation of the Orebro Musculoskeletal Pain Screening Questionnaire. Ann Phys Rehabil Med. 2012;55(4):263–278. doi:10.1016/j.rehab.2012.03.002
14. Heneweer H, van Woudenberg NJ, van Genderen F, Vanhees L, Wittink H. Measuring psychosocial variables in patients with (sub) acute low back pain complaints, at risk for chronicity: a validation study of the acute low back pain Screening Questionnaire-Dutch Language Version. Spine. 2010;35(4):447–452. doi:10.1097/BRS.0b013e3181bd9e3b
15. Fagundes FRC, Costa LOP, Fuhro FF, Manzoni ACT, de Oliveira NTB, Cabral CMN. Örebro Questionnaire: short and long forms of the Brazilian-Portuguese version. Qual Life Res. 2015;24(11):2777–2788. doi:10.1007/s11136-015-0998-3
16. The United Nations. Official languages; 2019. Available from: http://www.un.org/en/sections/about-un/official-languages/.
17. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
18. Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
19. Algarni AS, Ghorbel S, Jones JG, Guermazi M. Validation of an Arabic version of the Oswestry index in Saudi Arabia. Ann Phys Rehabil Med. 2014;57(9–10):653–663. doi:10.1016/j.rehab.2014.06.006
20. Alanazi F, Gleeson P, Olson S, Roddey T. Translation and validation of the Arabic version of the fear-avoidance beliefs questionnaire in patients with low back pain. Spine. 2017;42(7):E411–E416. doi:10.1097/BRS.0000000000001802
21. Terkawi AS, Sullivan M, Abolkhair A, et al. Development and validation of Arabic version of the pain catastrophizing scale. Saudi J Anaesth. 2017;11(Suppl 1):S63–S70. doi:10.4103/sja.SJA_130_17
22. Bier JD, Ostelo R, van Hooff ML, Koes BW, Verhagen AP. Validity and reproducibility of the start back tool (Dutch version) in patients with low back pain in primary care settings. Phys Ther. 2017;97(5):561–570. doi:10.1093/ptj/pzx023
23. Gabel CP, Melloh M, Yelland M, Burkett B, Roiko A. Predictive ability of a modified Örebro Musculoskeletal Pain Questionnaire in an acute/subacute low back pain working population. Eur Spine J. 2011;20(3):449–457. doi:10.1007/s00586-010-1509-4
24. Linton SJ, Nicholas M, MacDonald S. Development of a short form of the Örebro Musculoskeletal Pain Screening Questionnaire. Spine. 2011;36(22):1891–1895. doi:10.1097/BRS.0b013e3181f8f775
25. van Tulder M, Becker A, Bekkering T, et al. Chapter 3European guidelines for the management of acute nonspecific low back pain in primary care. Eur Spine J. 2006;15(2):s169–s91. doi:10.1007/s00586-006-1071-2
26. Delitto A, George SZ, Van Dillen LR, et al. Low back pain. J Orthop Sports Phys Ther. 2012;42(4):A1–A57. doi:10.2519/jospt.2012.42.4.A1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Translation, Cross-Cultural Adaptation, and Psychometric Properties of the Revised Fibromyalgia Impact Questionnaire (FIQR) for Use in Arabic-Speaking Patients in Saudi Arabia
Alaujan SS, Almalag HM, Almazrou SH, Alkhudair NA, Alodaibi FA, Omair MA
Patient Preference and Adherence 2024, 18:1017-1025
Published Date: 27 May 2024
The Creation of the Arabic Version of the Hyperhidrosis Quality of Life Index (HidroQoL©) with Validation and Cross-Cultural Adaptation
Almuhaideb QA, AbuDujain NM, Alghamdi KM
Clinical, Cosmetic and Investigational Dermatology 2025, 18:251-263
Published Date: 25 January 2025
Psychometric Validation of the Arabic Version of the Irrational Procrastination Scale (IPS) Among Lebanese Young Adults
Chahine A, Yakın E, Malaeb D, Hallit R, Obeid S, Hallit S, Fekih-Romdhane F
Psychology Research and Behavior Management 2025, 18:2167-2177
Published Date: 16 October 2025
Validation of the Arabic Version Post-COVID-19 Symptom Scale (PCSS-Ar) for Assessing Long COVID-19 Severity Among Arabic-Speaking Populations: A Factor Analysis and Rasch Analysis Study
Al-Qerem W, Baaj R, Jarab A, Al Bawab AQ, Hasan Agha MI, Eberhardt J, Al-Sa’di L, Obidat R, Abu Hour S
Risk Management and Healthcare Policy 2026, 19:572130
Published Date: 4 February 2026