Back to Journals » Patient Preference and Adherence » Volume 19
Barriers to Home-Based Medication Self-Management Among Older Adults with Multimorbidity: A Qualitative Study Guided by Empowerment Theory
Authors Zhang Z ![]() , Bai X, Hao L, Wang Y
, Bai X, Hao L, Wang Y
Received 23 September 2025
Accepted for publication 27 November 2025
Published 11 December 2025 Volume 2025:19 Pages 3985—3998
DOI https://doi.org/10.2147/PPA.S569526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Zhitong Zhang,1 Xiuli Bai,2 Le Hao,3 Yanli Wang2
1School of Nursing, Inner Mongolia Medical University, Hohhot, Inner Mongolia, People’s Republic of China; 2Department of Nursing, Inner Mongolia People’s Hospital, Hohhot, Inner Mongolia, People’s Republic of China; 3Geriatric Health Care Center, Inner Mongolia People’s Hospital, Hohhot, Inner Mongolia, People’s Republic of China
Correspondence: Yanli Wang, Department of Nursing, Inner Mongolia People’s Hospital, Hohhot, Inner Mongolia, People’s Republic of China, 010017, Email [email protected]
Purpose: To examine barriers to medication self-management among community-dwelling older adults with multiple chronic conditions (MCCs) and to provide evidence to guide medication safety and targeted nursing interventions.
Patients and Methods: A descriptive qualitative approach was used. Between July and September 2024, we recruited 14 community-dwelling older adults with MCCs from the geriatric medicine center of a tertiary hospital in the Inner Mongolia Autonomous Region. Face-to-face, semi-structured interviews were conducted. Empowerment theory served as the conceptual framework; data were analyzed using content analysis.
Results: Barriers to home-based medication self-management among older adults with MCCs were grouped into three domains: resources, agency, and outcomes. Resource-related barriers included (1) lack of long-term medication plans and follow-up support; (2) Inadequate aging-friendly design of medication management tools; and (3) barriers to self-medication due to excessive family intervention. Agency-related barriers included (1) health decisions primarily based on religious beliefs; (2) symptom-driven medication behavior; and (3) low-burden oriented medication management tendencies. Outcome-related barriers included disconnect between home self-monitoring and clinical feedback.
Conclusion: Community-dwelling older adults with MCCs encounter multiple challenges that hinder effective home-based medication self-management, including limited structural support, reduced self-management capacity, and a lack of effective feedback systems. The findings indicate that medication management can be optimized through improved digital and assistive tools, enhanced interprofessional collaboration, and more effective, tailored health education. Future research should prioritize high-risk populations and develop individualized intervention strategies.
Keywords: older adults, multiple chronic conditions, drug management, empowerment theory, qualitative research
Introduction
Since Feinstein introduced the term comorbidity in 1970,1 subsequent constructs, such as multimorbidity and lifelong comorbidity, have emerged.2,3 The World Health Organization defines multiple chronic conditions (MCCs) as the coexistence of two or more chronic diseases.4 The global prevalence of MCCs ranges from 4.5 to 83%,5 whereas that in China is approximately 43.65%.6 Compared with patients with a single disease, older adults with MCCs require broader medication regimens and prolonged treatment courses and often face fragmented medication guidance, heterogeneous comorbidity patterns, and limited management strategies.7 Age-related physiological decline and reduced self-management capacity further increase the overall medication-management burden.8
Medication self-management refers to an individual’s active engagement in the management of their own medications through self-awareness and self-regulatory behaviors, including proactive planning, monitoring, evaluating, and adjusting pharmacotherapy.7 Polypharmacy, commonly defined as the concurrent use of five or more medications,9 is highly prevalent among older adults, with recent estimates reaching 50.27%.10 Potential drug–drug interactions associated with polypharmacy differ according to comorbidity patterns. For example, the concurrent use of proton pump inhibitors and clopidogrel is associated with elevated cardiovascular risk,11 whereas the combination of clopidogrel and Ginkgo biloba extract increases the likelihood of bleeding and gastrointestinal events.12 This variability in comorbidity patterns makes it difficult for current management strategies to provide timely and targeted responses. As a result, medication safety risks are increased because many older adults have limited knowledge of their medications, including drug names, indications, and potential side effects. Consequently, older adults with MCCs often experience practical challenges in home-based self-medication, such as poor adherence, inconsistent drug storage, and impaired medication safety. These issues have been well documented in previous studies.13 Older adults with MCCs also frequently lack reliable support systems, including consistent family support and accessible community healthcare services, further exacerbating difficulties in medication management.14 In contrast, effective home medication practices can improve the adherence and capacity of older adults to cope with their MCCs.15
With population aging and a rising prevalence of older patients with MCCs, medication adherence and management effectiveness have become increasingly critical determinants of health among older adults. Digital health technologies, including mobile health applications, telemedicine platforms, and artificial intelligence–based decision tools, have shown strong potential to improve adherence, support health monitoring, and optimize medication use in older adults with MCCs.16,17 These technologies may reinforce health-related self-efficacy and provide new pathways for managing medications at home. However, despite these advantages, practical barriers remain, such as high cost, usability limitations, and low acceptance among older adults.18,19
Empowerment theory20 is grounded in a resources–agency–outcomes framework, with agency as its core. The theory aims to enhance individuals’ self-efficacy and capacity for health decision-making and self-behaviors by offering the necessary resources and support to enable sustained self-management. It has demonstrated positive outcomes in improving self-management among patients with MCCs. However, existing research does not sufficiently clarify the specific obstacles older adults with MCCs encounter in home-based medication management, nor does it fully elucidate the mechanisms through which empowerment processes operate in this context. This study adopts a descriptive qualitative design guided by empowerment theory. Semi-structured, in-depth interviews will be conducted to systematically explore the barriers to home-based medication self-management. Empowerment theory will inform both the development of interview questions and the interactions with participants, emphasizing their perceptions of medication-management competence and the resources and support they require to manage medications effectively.
Although prior qualitative studies have examined medication self-management in older adults with MCCs, most have focused on clinical or hospital settings. Far less attention has been given to the barriers and difficulties these patients face when managing medications in the home environment. Building on this theoretical gap, the present study examines how empowerment mechanisms influence key dimensions of medication management, administration, monitoring, evaluation, and adjustment, while identifying additional factors that contribute to ineffective home medication practices. The research will support the theoretical framework and practical evidence to inform patient-centered intervention strategies and models of home-based health management services.
Research Methods
Trustworthiness
To ensure methodological rigor and trustworthiness, this study adhered to the 《Consolidated Criteria for Reporting Qualitative Research (COREQ): 32-Item Checklist》21 to guarantee research design quality.
Patient Participants
Purposeful sampling was performed to sample the respondents of diverse age groups, sex, education, living situation, method of payment of medication, type and length of chronic diseases, and the duration of long-term medication use, thereby finding the different barriers to home-based medication self-management. The inclusion criteria employed in the study were as follows: (1) age ≥60 years; (2) diagnosis of at least two chronic diseases meeting ICD-10 criteria and confirmed by a secondary-level or higher hospital;22 (3) regular use of five or more medications with a history of long-term use (≥3 months) in a non-hospital setting;23 (4) clinically stable and able to self-administer medications; and (5) able to communicate normally and willing to participate. The exclusion criteria were as follows: (1) diagnosed psychiatric disorders; (2) severe communication barriers; and (3) severe heart, lung, liver, or kidney disease, or advanced malignancy. The sample size was determined based on data saturation, which is defined as the point at which no new themes emerged during the analysis.24 The study commenced in July 2024 at the Geriatric Medicine Center of a tertiary hospital in the Inner Mongolia Autonomous Region. The interviews were conducted at participants’ homes approximately 1 week after discharge, as this was a high-risk period for medication management issues.25 Recruitment and data analysis proceeded concurrently. By September 2024, as per the preliminary analysis, additional interviews did not yield any new information; therefore, the recruitment was concluded. Based on the research questions and existing literature,13,26 we estimated that 12–30 participants would achieve saturation. During the research, 21 patients were contacted. Seven of the patients decided not to participate after the researchers provided them with elaborate explanations about the study objectives, procedures, confidentiality, and the principle of voluntary participation. The cause particulars were three fatigue in 3 patients and physical discomfort in 4. Finally, 14 patients consented to participate and provided their signed informed consent forms.
Interview Guide Development
This research was conducted by using the empowerment theory, and a rough interview guide was created based on the literature analysis, after discussion with the research team. Then, two participants, based on the inclusion criteria, were interviewed as pilots. According to the preliminary results, the specialists in the corresponding areas (ie, a geriatrician, a nurse, a clinical pharmacist, and a scholar with knowledge of qualitative research) were invited to update the guide in a successive manner. This process ensured that the questions addressed all three domains of the framework while remaining open-ended and accommodating responses beyond the framework. The last semi-structured interview guide included the following questions: (1) What is your standard practice of handling medications at home? (2) In the process, what resources or individuals do you counsel to get some help or information? (3) What are the challenges that you face when taking medicine every day? (4) Who usually makes changes or decisions regarding medication change, or what is your role in this process? (5) What have been the impacts of your experiences with the medication on your everyday life and health? (6) What area(s) would you most prefer to have help with? (Supplementary File 1).
Data Collection
This paper employed a descriptive qualitative methodology, whereby data were gathered through face-to-face semi-structured interviews conducted a week after the discharge. The research team visited the wards during the pre-discharge nursing activities to create a rapport with the potential participants. A week before the interview, the participants were approached on the phone and provided a comprehensive exposition of the purpose, procedures, and importance of the study. The process of audio-recording and confidentiality concerns were clarified to ease the issues, and informed consent was obtained. Each participant was informed about the time and the place of the interview. The interviews were held in cozy and relaxing, familiar environments (eg, at the home of the participants). The interviews were conducted by two Master’s-level nursing students trained in qualitative research techniques and semi-structured interviewing. The discussion was guided by one researcher, and the other made field notes and recorded the audio (ZZT and HL). The interviewer read the interview topics before the interview, explained the relevant concepts, and ensured the completion of the consent form. The interviewer acted as a good listener and they changed the order of the questions, if required, based on the questions’ guide and the situation of the interviewee.Probing questions were used to obtain detailed descriptions, and the facial expressions, body language, and changes in affect were noted. The interviewer also avoided leading and being evaluative in the interview and remained focused on listening as much as possible to avoid influencing the participants. An unjudgmental attitude was taken by using a neutral and respectful back-channeling attitude. The interviews were recorded and transcribed word-for-word; field notes were used to record the nonverbal behaviors. The duration of the interviews was 30–45 min. Data saturation was achieved after interviewing 12 patients, and further interviews did not yield any new information, marking the data saturation point as the end of the interviews. A patient who had MCCs was forced to stop the interview because of acute physical discomfort, for which a follow-up interview was rescheduled. Finally, all 14 patients were analyzed in terms of their data.
Data Analysis
After each interview, the two interviewers transcribed the audio recordings verbatim within 24 h and supplemented the transcripts with field-note annotations describing relevant nonverbal behaviors. The data were managed using NVivo 12, and qualitative content analysis was conducted.27 Any uncertainties during transcription were resolved by replaying the audio recordings and, when needed, through group discussion. Relevant literature was consulted to standardize terminology. Two researchers independently coded the data, and discrepancies were resolved through discussion until consensus was reached. The qualitative content analysis proceeded through the following steps: (1) development of an a priori coding framework based on empowerment theory, using the primary categories of resources, agency, and outcomes; (2) repeated reading of the raw transcripts and listening to recordings to ensure familiarity with the data; (3) open coding by identifying meaning units (words, phrases, sentences, or paragraphs); and (4) refinement of themes by grouping similar meaning units into corresponding categories, with iterative abstraction and subdivision to generate overarching themes and subthemes, while allowing emergent themes to be identified inductively; (5) member checking through follow-up interviews to solicit participants’ feedback on the researchers’ interpretations; and (6) inductive analysis of content not adequately captured within the initial framework, which was reported separately.
Rigor
All researchers had received formal training in qualitative methodologies and regularly refined their interview techniques. The preinterviews were guided and supervised by an experienced qualitative research professor. Voluntary participation and confidentiality were strictly upheld, and participants were free to withdraw at any time. Interview and medical information were carefully protected by the research team to prevent unauthorized access. The interview pace was adjusted to real-life situations, and unclear statements were verified. To ensure reliability and validity during data analysis, team members engaged in group discussion and cross-checked all codes, subthemes, and themes. Audio recordings and field notes were used to support accurate interpretation. All data were repeatedly reviewed for accuracy, and selected participants were invited to provide feedback on the analysis outcomes to ensure that the findings authentically reflected their experiences.
Reflexivity Statement
The research team is dedicated to advancing knowledge and practice in geriatric care. The first author (ZZT), a graduate student specializing in geriatric care, was mindful of the substantial age difference between themselves and the older participants. Recognizing that generational differences could influence communication, ZZT adopted a learner-oriented stance, actively listening to participants’ experiences to foster a more relaxed, open, and respectful interview environment. HL, with 8 years of clinical experience in geriatric care and a Master of Science in Nursing, brought extensive expertise in chronic disease management. Their long-term clinical rapport with the participants enabled them to bridge generational barriers effectively and encouraged participants to share sensitive information regarding medication self-management. WYL, the Director of Nursing at the study hospital. BXL, who holds a Master’s degree in Nursing, provided strong theoretical grounding and substantial practical experience in managing patients with chronic diseases. Their academic background offered essential guidance for the study’s theoretical framework and methodology, especially during study design and data analysis.
Empowerment theory served as the guideline to explore barriers faced by community-dwelling older adults with MCCs during home-based medication self-management. Participant recruitment was conducted by ZZT, who had no clinical care relationship with the participants. HL’s clinical familiarity with older adults helped build trust and facilitate deeper exploration during interviews. The interviews were conducted in accordance with naturalism principles,28 where the research team did not instruct the process or predetermine the outcomes. Clarification and summarization techniques were used during interviews, supplemented by post-interview team discussions and reflective practice to ensure accurate interpretation of participants’ narratives. Data analysis emphasized transparency and depth through the use of detailed field notes and reflective journals, which were reviewed collectively to refine coding, categorization, and theme development.
Results
Sample Characteristics
This study conducted in-depth interviews with 14 community-dwelling older adults with MCCs (9 females and 5 males, mean age: 78.64 ±7.63 years) receiving home-based care. Their sociodemographic characteristics are summarized in Table 1. The participants were assigned codes N1–N14. On average, the participants had 3.79 ±1.05 chronic conditions, were taking 6.79 ±1.37 medications, and had been using long-term medications for 17.50 ±9.11 years. Most participants relied on employment-based insurance or resident basic medical insurance (RBMI) to cover medication expenses. The total interview duration across all participants was approximately 432 min, yielding about 39,000 words of transcribed data.
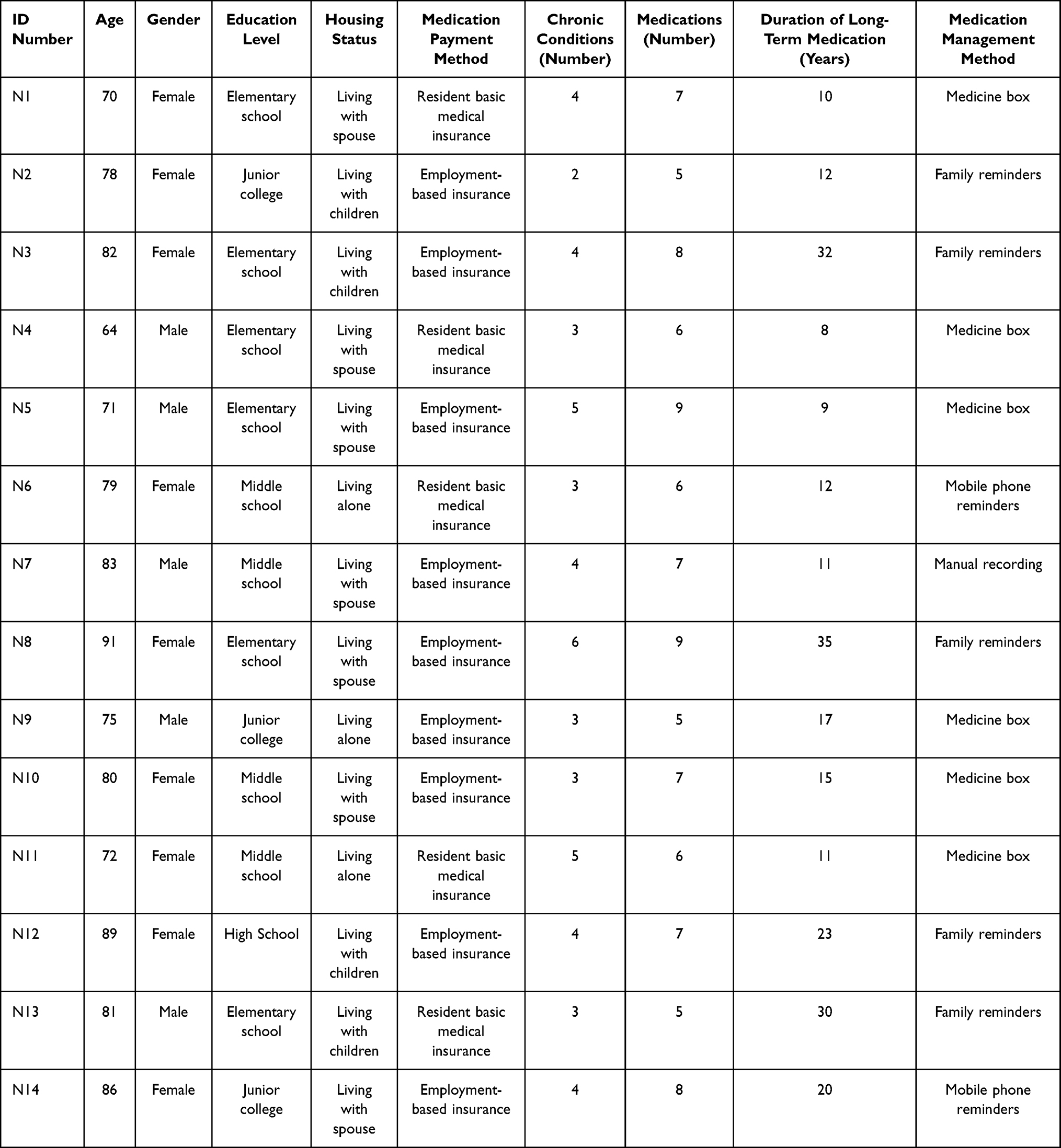 |
Table 1 General Characteristics of Respondents (N=14) |
Barriers Affecting Home-Based Medication Self-Management Among Older Adults with MCCs
Figure 1 summarizes the home-based medication self-management barriers identified among older adults with MCCs. Guided by empowerment theory, these barriers were categorized into three domains: resources, agency, and outcomes, each comprising multiple themes derived from the interview data.
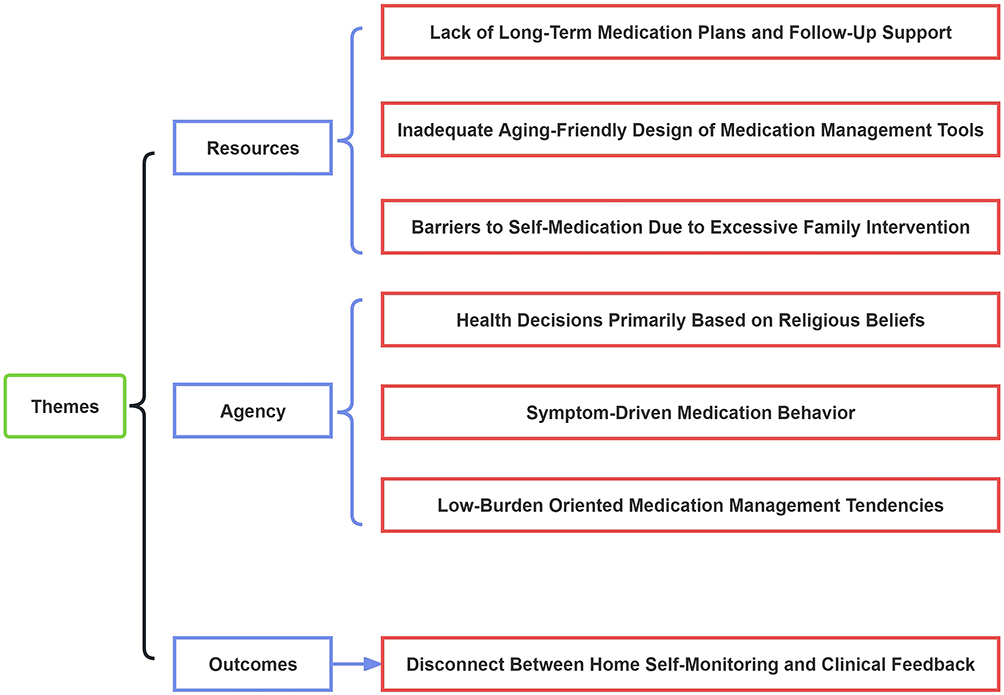 |
Figure 1 Themes and Subthemes of Qualitative Research Findings. |
Resource-Related Barriers
Lack of Long-Term Medication Plans and Follow-Up Support
In this study, numerous MCCs patients reported that due to the absence of clear medication regimens and follow-up support, they often relied solely on verbal instructions from doctors and medication labels to maintain treatment. N8: “The doctor never mentioned how long I should take these medications; they just told me to take them.” This uncertainty about treatment duration makes it difficult for patients to fully grasp their therapeutic progress, thereby intensifying their concerns about treatment efficacy and disease control. N4: “During treatment, I consulted several doctors, and each prescribed different medications. I really wish there could be a stable regimen to avoid frequent changes”. The constant alteration in prescriptions also undermine patients’ confidence in adhering to long-term medication. N5: “I just go to the pharmacy on the 15th of every month to buy my medicine and take it. I’m not really sure how effective it is.” This lack of regular assessment and feedback on treatment outcomes leaves patients both dependent on the treatment, as well as constantly anxious.
Inadequate Aging-Friendly Design of Medication Management Tools
During the study, many patients—particularly those MCCs patients with impaired vision and limited hand mobility—reported difficulties operating common pill organizers. N10: “I keep my medications in plain sight without using a pill organizer. Mainly, I find the process of loading pills unhygienic.” This indicates current pill organizer designs fail to adequately address elderly users’ needs for convenience and hygiene. N11: “I do have a pill organizer, but it bulges in my bag and is inconvenient to retrieve”. This highlights unreasonable volume or form factor designs that create additional burdens for particular users. N5: “The pill organizer is too small. I take over ten different medications, and it simply can’t hold them all. I end up just piling them all in a drawer”. Although pill organizers are often recommended for standardized medication management, their practical effectiveness is often unsatisfactory for elderly patients who need to take multiple medications simultaneously and whose vision and hand function have deteriorated.
Barriers to Self-Medication Due to Excessive Family Intervention
Respecting patients’ autonomy in decision-making is paramount in medical care. However, when family members dominate treatment decisions without thorough communication or consideration of the patient’s wishes, it can strip individuals of their sense of control over their own health management. N6: “I have trouble sleeping and sometimes need sleeping pills to fall asleep. Once my daughter visited and took my medication away, saying she feared I’d misuse it. She told me to call her if I needed more, but asking her for medicine is always such a hassle”. Yet as age and cognitive decline set in, MCCs patients face genuine difficulties managing complex medications independently. Lacking family support can further exacerbate confusion. N12: “My spouse is hospitalized long-term, leaving me alone at home. My daughter comes over at noon to cook for me. But now my vision is getting worse—I can’t see the insulin syringe’s markings clearly, so I have to rely on feel and sound to administer it”. N8: “My son doesn’t live with us. Not only do I have to remember my own medications, but I also have to make sure my spouse takes hers on time.”
Barriers to Agency
Health Decisions Primarily Based on Religious Beliefs
Research has found that for some MCCs patients, religious beliefs play a central role in managing their health, even serving as an alternative source of empowerment for making medication decisions. N1: “I am religious. I believe everything is in God’s plan, and illness is predestined.” This attribution of health to divine will leads them to defer decision-making to their faith rather than fully relying on medical advice or evidenced-based treatment methods. Religious beliefs profoundly shape their understanding and acceptance of illness, while also significantly diminishing their active role in health management within the conventional medical system. N3: “I habitually rely on prayer and religious rituals to help alleviate my suffering.” This emphasis on spiritual strength may lead them to prioritize seeking spiritual support during treatment, thereby reducing their willingness to accept medication or other clinical interventions.
Symptom-Driven Medication Behavior
Research indicates that MCCs patients frequently self-adjust medication dosages and usage based on their symptom fluctuations in daily practice. N7: “I adjust my medication dosage at home, trying to take as little as possible. When symptoms improve, I reduce the frequency. If I can tolerate it during the day, I take less; at night, I try to skip it altogether”. N8: “I often wake up at night due to high blood pressure or angina pain. I have to take two or three doses of rescue pills to manage it—I simply can’t endure it without them”. This medication behavior indicates that sudden symptom onset and pain intensity directly dictate dosage frequency and amounts. However, such symptom-based self-adjustment carries potential risks, including inadequate or excessive dosing, improper dosing intervals, and unstable drug efficacy. These factors increase the likelihood of adverse events and disease fluctuations.
Low-Burden Oriented Medication Management Tendencies
This study found that some MCCs patients tend to adopt strategies that minimize management burdens during long-term medication use. While generally adhering to prescribed regimens, they exhibit low initiative in seeking medication information and weak willingness to actively monitor their own conditions. They often tolerate mild discomfort symptoms, setting treatment goals solely at maintaining basic symptom control. N5: “I just take the meds the doctor prescribed on time. I don’t really care about the side effects. The package insert lists a bunch of side effects, but I don’t read it—I don’t want to know. If I knew too much, I’d probably be too scared to take the medicine at all”. N9: “I just take my meds as the doctor told me to. I don’t actively monitor myself or pay much attention. If I feel dizzy, I just tough it out. If I feel tired, I don’t make a big deal out of it”.
Barriers to Outcomes
Disconnect Between Home Self-Monitoring and Clinical Feedback
This study reveals frequent communication gaps between home health monitoring data and clinical treatment feedback for MCCs patients. Patients generally engage in infrequent daily self-monitoring, relying primarily on single outpatient test results or subjective assessments to evaluate their condition. This prevents timely feedback of treatment efficacy dynamics to clinicians, hindering dynamic prescription adjustments and optimization. N1: “They only discovered my high blood sugar when I was hospitalized, and my blood pressure had dropped to 70/40 mmHg. I had no idea about these conditions before admission. If I hadn’t come to the hospital for testing, how would I have known my blood sugar had risen to 20 mmol/L!” N3: “I test my blood sugar and blood pressure at home occasionally, maybe once a month. I hardly ever check otherwise.” Faced with daily fluctuations in physiological indicators, patients often adjust medication based on subjective feelings, lacking clinical professional assessment and timely guidance. N3: “Sometimes when I feel dietary discomfort, I reduce my dosage on my own, splitting pills in half.” N6: “During this hospitalization, the doctor didn’t seem to ask in detail about my usual medications, and I forgot to bring it up proactively.”
Discussion
Resource Level: Discontinuity of Information and Lack of Care Support in Home Settings
This study found substantial barriers in translating available resources into effective home medication management of older adults with MCCs. One of the major reasons is the hierarchical nature of the healthcare system in China, where most of the patients receive uncoordinated care across various hospitals without coordinated management or comprehensive medication counselling. Such discontinuity undermines the effective use of resources to support stable medication adherence, which is consistent with the conclusions reached by Jones et al.29 Information discontinuity not only increases short-term risks but also disrupts evidence-based follow-up. As a result, clinical interventions often occur reactively, after adverse outcomes have already emerged, rather than preventively. The current follow-up model makes it difficult to establish a systematic and continuous management cycle, which stands in contrast to the dynamic closed-loop process recommended by expert consensus: assessment, decision-making, multidisciplinary intervention, follow-up, and reassessment. Such a process enables healthcare providers to rapidly access, update, and reconcile patient medication records, reducing risks arising from incomplete or inconsistent prescription information.30 Medical workers should actively initiate regular contact with patients to shift the follow-up process from a reactive to a proactive process. This requires a systematic and cyclical management process that involves medication reconciliation, individualized guidance, efficacy monitoring, and treatment plan optimization, ensuring continuous monitoring of medication adherence and the health status of patients.
This study also found that traditional, instructive, and one-way health-education models hinder the development of medication self-management capacity among older adults, consistent with the findings of Chen et al.31 Patients with less education often struggle to understand the importance of medication self-management and its long-term consequences, which are consistent with the findings of Kamau et al.32 Thus, healthcare providers can deliver more comprehensive health education by first identifying patient needs and tailoring the content to their specific capabilities and participation characteristics. This includes conducting a comprehensive review of medication-related needs in patients with MCCs and developing tailored educational strategies, such as individualized medication lists and simplified management tools to enable patients to comprehend and comply with their medication regimens. Physicians and pharmacists should deliver patient-specific medication-management education based on each individual’s condition and learning needs, while also encouraging engagement in medication-safety workshops and related programs.
Despite the strong endorsement of pill organizers and other medication-management aids in both clinical and home settings, their real-world effectiveness in older adults with MCCs has been limited, a finding also consistent with the findings of the research by Liu Weibin et al.33 This suggests shortcomings in the age-friendly design and user acceptance of these tools. The usability and technological acceptance are central determinants of whether older adults adopt digital health technologies.34 As the artificial intelligence continues to advance, its highly developed data-processing and analysis features, as well as the possibilities of remote-controlled interventions, have slowly promoted its implementation in home-based medication management of patients with chronic diseases. This will give the patients more intelligent and customized treatment plans. These technologies can provide patients with smarter and customized treatment plans.35 Nevertheless, the number of patients using smart tools in this study was very limited. This could be attributed to the pragmatic mindset common among older adults, as well as the high purchase and maintenance costs of current smart medication products. These aspects make older adults resist such tools because of the fear of service discontinuation, unaffordable fees, and the long-term financial burden, particularly for those covered under employment-based insurance or the Resident Basic Medical Insurance(RBMI).Therefore, age-friendliness in medication management tools must extend beyond technological sophistication to include thoughtful design principles that match the real-world needs of older users. Attention to device capacity, operational simplicity, hygiene, and overall usability is essential. Medical workers should actively offer hands-on training to help older adults overcome technological anxiety and enhance their desire and capacity to use novel technologies.
In addition, existing evidence shows that family caregivers play a critical yet complex role in home-based medication management and are key facilitators of medication safety, consistent with the findings of Sarkhosh et al.36 Appropriate family support can improve medication adherence and safety, thereby enhancing medication-taking behavior and psychological well-being in older adults.37 However, excessive involvement may undermine patients’ autonomy and overlook their preferences and needs,38 which is caused by the absence of role definitions, poorly coordinated division of responsibilities, and insufficient caregiver training, which together create role conflicts and hinder effective involvement in the medication management of older adults with MCCs. Compared with cohabiting older adults, those living alone face not only greater health risks and lower functional status but also more difficulties in managing medications due to limited family supervision and support, contributing to poorer overall health maintenance.39 Role boundary theory, as described by Ashforth et al40 defines role integration as a process through which work and family roles interact and support one another, helping to coordinate expectations and reduce role conflict. To mitigate role overlap and conflict among family caregivers assisting older adults with MCCs, digital health technologies, including real-time monitoring and data-feedback systems, can help caregivers overcome the temporal and spatial limitations of traditional care models. These technologies enable more effective tracking of medication adherence and coordination across multiple caregiving responsibilities.41 However, because digital literacy is essential for the successful use of such technologies, limited technological competence among caregivers may impede their ability to effectively support medication self-management. Thus, it is necessary to conduct specific digital literacy education courses for improving the technological skills of caregivers.
Proactive Level: Insufficient Motivation for Home Self-Management and Behavioral Avoidance
Home-based medication self-management fundamentally depends on patient agency. This study found that older adults with MCCs often exhibit low initiative and weak motivation for self-management. Religious beliefs also influenced medication behaviors; some participants relied more on faith over medicine to control the illness, thus reducing their reliance on pharmacotherapy. This does not mean that medical practitioners should disregard patients’ religious beliefs when encouraging consistent medication at home in cases of MCCs. Although such beliefs may provide emotional comfort and reduce anxiety, they can weaken proactive engagement with medical recommendations, a pattern consistent with findings by Sturm et al.42 Healthcare professionals should respect patients’ religious beliefs while clearly communicating the importance of consistent medication use. Developing culturally aligned self-management education plans and supporting patients in harmonizing their faith with scientific treatment are essential to improving adherence.
Moreover, cultural background also shapes medication self-management. In many cultural contexts, family roles are integral to the health management of older adults. In collectivist cultures, family involvement can substantially enhance medication adherence.43 Moreover, the Chinese cultural preferences may lead some patients to rely more on traditional medicine and be less accepting of pharmacological treatments. For instance, patients may prefer traditional Chinese medicine and express distrust toward Western medicine in the form of pills.44 Such a cultural trend can contribute to the deviation in medication self-management and affect adherence and treatment outcomes. Therefore, healthcare providers must proactively understand patients’ cultural beliefs, religious practices, and cognitive styles when managing chronic disease. This approach helps minimize medication disparities stemming from cultural or religious influences and supports safer and more effective home-based medication practices.
This study also found that, despite following prescribed regimens, some older adults with MCCs adjusted their medications on their own or avoided receiving information about potential adverse effects. Differences in coping strategies result in varied behavioral, cognitive, and emotional responses, which in turn affect individuals’ medication self-management, consistent with the findings of Yang Shuling.45 This highlights substantial interindividual variation in how older adults with MCCs manage medications and cope with illness. Golinelli et al46 suggest that risk stratification tools can help identify high-risk patients based on their health data and guide tailored interventions. Such tools use digital technologies to collect and update patient information in real time, enabling healthcare teams to provide personalized, timely support based on stratified risk levels. High-risk patients may require more intensive, multicomponent interventions, including medication optimization, enhanced family support, and technology-assisted adherence strategies, to manage key risk factors and reduce readmission rates.47 Conversely, lower-risk patients may benefit from fundamental education and regular examinations. The purpose of this strategy is to prevent excessive intervention while strengthening self-efficacy and achievable self-management behavior.
Outcome Level: Disconnect Between Home Monitoring and Clinical Feedback and Its Impact
This study also identified a substantial disconnect between home-based monitoring performed by older adults with MCCs and its integration into clinical decision-making Although patients engaged in self-monitoring and kept medication records at home, the information was fragmented and rarely incorporated into clinical workflows in a timely or systematic manner, consistent with findings by Chang et al.48 This gap arises largely because healthcare providers pay limited attention to home-based medication information. Current service models rely primarily on one-time discharge counseling or occasional phone follow-ups, focusing mainly on disease knowledge rather than standardized collection, interpretation, and integration of home monitoring data, which leads to dissociation between the monitoring data and the clinical care. Consequently, remote monitoring technology can support real-time, systematic delivery of patient health data to the medical teams. This allows timely adjustment of treatment plans and targeted medication guidance based on the condition of each patient. Real-time monitoring also enables healthcare practitioners to implement early diagnoses and treatment, avoid complications, and eliminate hospital visits, particularly benefiting older adults with chronic illnesses and eventually delivering better health outcomes.49 Moreover, this study indicates that older adults with MCCs often demonstrate limited home-based medication self-management skills, consistent with the findings of Pan Wanyu et al.15 Contributing factors include inadequate medication knowledge, doubts regarding treatment effectiveness, and entrenched traditional beliefs about medication use. These issues frequently lead patients to discontinue medications on their own or adjust dosages arbitrarily, resulting in home-monitoring data that fail to accurately reflect their true health status. In response, healthcare institutions should strengthen training on home-based self-management skills by providing structured guidance plans, standardized monitoring methods, unified documentation protocols, and basic instruction on interpreting routine health data, supported by appropriate medication administration tools. Such measures would improve the standardization, accuracy, and reliability of patient-recorded data. Additionally, periodic review of patient records through online platforms or telephone follow-ups is essential to verify their accuracy and comprehensiveness. Moreover, enhanced multidisciplinary collaboration reduces medication errors and adverse drug events.50 Establishing a multidisciplinary home medication support system, comprising physicians, pharmacists, community nurses, and other relevant specialists, can clarify professional responsibilities, create a coordinated management process, and address patients’ needs for expert counseling and timely feedback.This collaborative model helps connect home monitoring and clinical feedback, which is important in encouraging the continuity and effectiveness of home-based medication management.
Limitation
This study was conducted in a single Grade III Class A hospital in the Inner Mongolia Autonomous Region, and all interviews took place within 1 week after discharge. Future research should expand the study setting and include patients at different stages of home care to generate more comprehensive and generalizable evidence. Moreover, the information in the interviews was mostly obtained by patients on patient self-report and did not incorporate socioeconomic data (such as household income) or include family caregivers and healthcare professionals. As a result, some themes lack sufficient explanatory depth. Incorporating socioeconomic indicators and perspectives from caregivers and clinicians in future studies will provide richer insights into how socioeconomic context influences medication management behaviors and will strengthen the foundation for developing personalized intervention strategies.
Conclusion
This systematic review identified key barriers to home-based medication self-management in older adults with MCCs through the lens of the empowerment framework (resources–agency–outcomes). The main challenges include insufficient resource support, weakened patient agency, and fragmented outcome feedback mechanisms. Addressing these issues will require improved technical support through digital health tools, strengthened interprofessional collaboration, and enhanced patient-centered education. Such efforts can support effective medication monitoring and timely treatment adjustments. Future work should focus on developing individualized intervention strategies and predictive models to assess self-management risk, identify high-risk patient groups, and improve the precision and effectiveness of home-based medication interventions.
Abbreviations
MCCs, Multiple Chronic Conditions.
Data Sharing Statement
Due to ethical constraints, participants’ raw data will not be shared. The processed data supporting this study’s findings are available from the corresponding author upon reasonable request.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Committee of Inner Mongolia People’s Hospital (202502703L).Prior to the study’s commencement, researchers fully explained the research objectives and procedures to all participants at the survey site. All subjects voluntarily and anonymously participated with full informed consent, having signed written informed consent forms authorizing the use of their anonymized data for publication.
Acknowledgments
Sincere thanks to all the participants who took part in the interviews.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Program of the Joint Fund of Scientific Research for the Public Hospitals of Inner Mongolia Academy of Medical Sciences (Grant No. 2023GLLH0055).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Feinstein AR. The pre-therapeutic classification of co-morbidity in chronic disease. J Chronic Dis. 1970;23(7):455–468. doi:10.1016/0021-9681(70)90054-8
2. Brandlmeier P. Multimorbidität unter den älteren patienten in einer städtischen allgemeinpraxis [Multimorbidity among elderly patients in an urban general practice. ZFA. 1976;52(25):1269–1275.
3. Whitty CJM, MacEwen C, Goddard A, et al. Rising to the challenge of multimorbidity. BMJ. 2020;368:16964.
4. World Health Organization. The world health report: Primary health care now more than ever.Geneva,Switzerland:world health organization;2008.
5. Pati S, Swain S, Hussain MA, et al. Prevalence and outcomes of multimorbidity in South Asia: a systematic review. BMJ Open. 2015;5(10):e007235. doi:10.1136/bmjopen-2014-007235
6. Yan W, Lu Y, Zhang R, et al. Multimorbidity status of the elderly in China-research based on CHARLS data. Chin J Dis Control Prev. 2019;23(4):426–430. doi:10.16462/j.cnki.zhjbkz.2019.04012
7. Yang C, Zhu S, Lee DTF, et al. Interventions for improving medication adherence in community-dwelling older people with multimorbidity: a systematic review and meta-analysis. Int J Nurs Stud. 2022;126:104154. doi:10.1016/j.ijnurstu.2021.104154
8. Yang C, Lee DTF, Wang X, et al. Effects of a nurse-led medication self-management intervention on medication adherence and health outcomes in older people with multimorbidity: a randomised controlled trial. Int J Nurs Stud. 2022;134:104314. doi:10.1016/j.ijnurstu.2022.104314
9. Lipska KJ, Krumholz H, Soones T, et al. Polypharmacy in the aging patient: a review of glycemic control in older adults with type 2 diabetes. JAMA. 2016;315(10):1034–1045. doi:10.1001/jama.2016.0299
10. Chang YN, Wang N. Analysis of chronic disease comorbidity characteristics and polypharmacy in hospitalized elders. Chin J Hosp Pharm. 2024;44(17):2032–2037. doi:10.13286/j.1001-5213.2024.1712
11. Alhumaidi RM, Bamagous GA, Alsanosi SM, et al. Risk of polypharmacy and its outcome in terms of drug interaction in an elderly population: a retrospective cross-sectional study. J Clin Med. 2023;12(12):3960. doi:10.3390/jcm12123960
12. Hoerr R, Zimmermann A, Seitz F, et al. Single and repeated doses of EGb 761® do not affect pharmacokinetics or pharmacodynamics of rivaroxaban in healthy subjects. Front Pharmacol. 2022;13:868843. doi:10.3389/fphar.2022.868843
13. Ming Q, YL T, Wang MZ, et al. A Meta-integration of qualitative studies on medication self-management experiences in older adults with comorbidities. J Nurs Train. 2025;40(6):645–652. doi:10.16821/j.cnki.hsjx.2025.06014
14. Previdoli G, Cheong V, Alldred D, et al. A rapid review of interventions to improve medicine self‐management for older people living at home. Health Expectations. 2023;26(3):945–988. doi:10.1111/hex.13729
15. Pan WY, Zhang FY, Niu YX, et al. Implementation of medication self-management intervention program for home-residing elderly patients with multiple chronic conditions. J Nurs Sci. 2024;39(10):97–102. doi:10.3870/j.issn.1001-4152.2024.10097
16. Peng YH, Xie LL, Liang Y, et al. Efficacy of intelligent medication management system in elderly people in care institutions. J Chinese J Nurs. 2021;56(5):680–686. doi:10.3761/j.issn.0254-1769.2021.05006
17. Zhou TT, Wang R, Gu SJ, et al. Effectiveness of mobile medical apps in ensuring medication safety among patients with chronic diseases: systematic review and meta-analysis. JMIR mHealth uHealth. 2022;10(11):e39819. doi:10.2196/39819
18. Yoon H, Jang Y, Vaughan PW, et al. Older adults’ internet use for health information: digital divide by race/ethnicity and socioeconomic status. J Appl Gerontol. 2020;39(1):105–110. doi:10.1177/0733464818770772
19. Singareddy S, SN VP, Jaramillo AP, et al. Artificial intelligence and its role in the management of chronic medical conditions: a systematic review. Cureus. 2023;15(9):e46066. doi:10.7759/cureus.46066
20. Kabeer N. Resources agency, achievements: reflections on the measurement of women’s empowerment. Dev Chang. 1999;30(3):435–464. doi:10.1111/1467-7660.00125
21. Du KJ, Li GS, Zhang K, et al. Prof. Karin hannes: COREQ (consolidated criteria for reporting qualitative studies). Ann translat Med. 2022;10(19):1073. doi:10.21037/atm-2022-23
22. Ministry of Health Health Statistics Information Center, WHO Collaborating Center for the Family of International Classifications. Practical Guide for the Application of ICD-10(International Classification of Diseases, 10th Revision). Beijing: Peking Union Medical College Press, 2001.
23. Pazan F, Wehling M. Polypharmacy in older adults: a narrative review of definitions, epidemiology and consequences. Eur Geriatr Med. 2021;12(3):443–452. doi:10.1007/s41999-021-00479-3
24. Takona JP. Research design: qualitative, quantitative, and mixed methods approaches.6th ed. Thousand Oaks, CA: SAGE publications; 2023. Book Rev. 2024;58(1):1011.
25. Zhao LB, Huang HH, Xiao F, et al. Medication discrepancies in elderly patients with polypharmacy during the hospital-to-home transitional period. J Nurs Sci. 2023;38(6):121–126. doi:10.3870/j.issn.1001-4152.2023.06121
26. Wang CL, Han SS, Zhang WZ, et al. Experiences of drug self-management in elderly patients with multimorbidities:a qualitative meta-synthesis. J Chinese J Nurs. 2024;59(12):1505–1511. doi:10.3761/j.issn.0254-1769.2024.12015
27. Assarroudi A, Heshmati Nabavi F, Armat MR, et al. Directed qualitative content analysis: the description and elaboration of its underpinning methods and data analysis process. J Res Nurs. 2018;23(1):42–55. doi:10.1177/1744987117741667
28. Mcinnes S, Peters K, Bonney A, et al. An exemplar of naturalistic inquiry in general practice research. Nurse Res. 2017;24(3):36–41. doi:10.7748/nr.2017.e1509
29. Jones CD, Jones J, Richard A, et al. “connecting the dots”: a qualitative study of home health nurse perspectives on coordinating care for recently discharged patients. J Gen Intern Med. 2017;32(10):1114–1121. doi:10.1007/s11606-017-4104-0
30. Zhu ML, Liu XH, Dong BR, et al. Chinese expert consensus on management of elderly patients with multimorbidity. Chin J Clin Healthc. 2023;26(5):577–584. doi:10.3969/J.issn.1672-6790.2023.05001
31. Chen C, Wang L, Chi HL, et al. Comparative efficacy of social media delivered health education on glycemic control: a meta-analysis. Int J Nurs Sci. 2020;7(3):359–368. doi:10.1016/j.ijnss.2020.04.010
32. Kamau M, Nyanja N, Lusambili AM, et al. Knowledge, attitudes and beliefs toward polypharmacy among older people attending family medicine clinic, Nairobi, Kenya. BMC Geriatr. 2024;24(1):132. doi:10.1186/s12877-024-04697-9
33. Liu WB, Cheng SH, Jiang N. Research progress on the application of artificial intelligence technology in medication management of elderly patients with chronic diseases. Chin Nurs Res. 2025;39(7):1206–1210. doi:10.12102/j.issn.1009-6493.2025.07024
34. Mishra V, Stuckler D, Mcnamara CL. Digital interventions to reduce hospitalization and hospital readmission for chronic obstructive pulmonary disease (COPD) patient: systematic review. BMC Digital Health. 2024;2(1):46. doi:10.1186/s44247-024-00103-x
35. Xie Y, Lu L, Gao F, et al. Integration of artificial intelligence, blockchain, and wearable technology for chronic disease management: a new paradigm in smart healthcare. Curr Med Sci. 2021;41(6):1123–1133. doi:10.1007/s11596-021-2485-0
36. Sarkhosh S, Abdi Z, Ravaghi H. Engaging patients in patient safety: a qualitative study examining healthcare managers and providers’ perspectives. BMC Nurs. 2022;21(1):374. doi:10.1186/s12912-022-01152-1
37. Huang CY, Liu XC, Luo LH. The impact of family supervision and companionship on stigma perception and medication adherence among elderly patients with acquired immunodeficiency syndrome. Chin J Gerontol. 2021;41(19):4414–4417. doi:10.3969/j.issn.1005-9202.2021.19075
38. Manias E, Bucknall T, Hughes C, et al. Family involvement in managing medications of older patients across transitions of care: a systematic review. BMC Geriatr. 2019;19(1):95. doi:10.1186/s12877-019-1102-6
39. Abdi S, Spann A, Borilovic J, et al. Understanding the care and support needs of older people: a scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. 2019;19(1):195. doi:10.1186/s12877-019-1189-9
40. Ashforth BE, Kreiner GE, Fugate M. All in a day’s work: boundaries and micro role transitions. Acad Manage Rev. 2000;25(3):472–491. doi:10.2307/259305
41. Zainal H, Xiaohui X, Thumboo J, et al. Exploring caregiver challenges, digital health technologies, and healthcare support: a qualitative study. Front Digital Health. 2025;7:1587162. doi:10.3389/fdgth.2025.1587162
42. Sturm N, Stolz R, Schalhorn F, et al. Self-efficacy, social activity, and spirituality in the care of elderly patients with polypharmacy in Germany-a multicentric cross-sectional study within the HoPES3 trial. Healthcare. 2021;9(10):1312. doi:10.3390/healthcare9101312
43. Osokpo O, Riegel B. Cultural factors influencing self-care by persons with cardiovascular disease: an integrative review. Inter J Nurs Stud. 2021;116:103383. doi:10.1016/j.ijnurstu.2019.06.014
44. Wang J, Matthews JT. Chronic disease self-management: views among older adults of Chinese descent. Geriatric Nurs. 2010;31(2):86–94. doi:10.1016/j.gerinurse.2009.11.001
45. Yang SL. Correlation of self-management ability with family function and coping style in patients with chronic obstructive pulmonary disease. J Bengbu Med Univ. 2024;49(2):264–269. doi:10.13898/j.cnki.issn.1000-2200.2024.02027
46. Golinelli D, Pecoraro V, Tedesco D, et al. Population risk stratification tools and interventions for chronic disease management in primary care: a systematic literature review. BMC Health Serv Res. 2025;25(1):526. doi:10.1186/s12913-025-12690-0
47. Wang J, Wang J, Qiu S, et al. Pharmaceutical care program for ischemic stroke patients: a randomized controlled trial. Inter J Clin Pharm. 2021;43(5):1412–1419. doi:10.1007/s11096-021-01272-9
48. Chang L, Lin LL. Addressing the needs of rural elderly with chronic diseases from a health management perspective: a case study of yantai high-tech zone. Manag Observer. 2015;(25):185–187. doi:10.3969/j.issn.1674-2877.2015.25056
49. Park Y, Kim EJ, Park S, et al. Digital health intervention effect on older adults with chronic diseases living alone: systematic review and meta-analysis of randomized controlled trials. J Med Internet Res. 2025;27(1):e63168. doi:10.2196/63168
50. Aires-Moreno GT, Silvestre CC, Araújo DCSA, et al. Perceptions of nurses, pharmacists and physicians about medication reconciliation: a multicenter study. Saudi Pharm J. 2020;28(11):1435–1439. doi:10.1016/j.jsps.2020.09.009
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Health Priorities in Chronic Obstructive Pulmonary Disease Patients with Multimorbidity: A Qualitative Study
Cai M, Cui M, Nong Y, Qin J, Mo S
Patient Preference and Adherence 2022, 16:2521-2531
Published Date: 13 September 2022
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Critical Care Nurses’ Experiences with Endotracheal Suctioning in Critically Ill Older Adults Patients: A Phenomenological Study
Tang J, Lyv J, Wu NH, Chen X, Bai JJ
Journal of Multidisciplinary Healthcare 2026, 19:586847
Published Date: 7 March 2026
Multidisciplinary Stakeholder Perspectives on the Design Needs of a Smart Walker for Fall Prevention Among Older Adults: A Qualitative Study in West Java, Indonesia

Dharmansyah D, Rahayuwati L, Pramukti I, Mutyara K
Journal of Multidisciplinary Healthcare 2026, 19:605216
Published Date: 6 May 2026