Back to Journals » International Journal of General Medicine » Volume 17
COVID-19 Vaccines Breakthrough Infections and Adverse Effects Reported by the Birzeit University Community in Palestine
Authors Abukhalil AD ![]() , Abushehadeh RR, Shatat SS, Al-Shami N
, Abushehadeh RR, Shatat SS, Al-Shami N ![]() , Naseef HA
, Naseef HA ![]() , Ladadweh H
, Ladadweh H ![]() , Madia R
, Madia R
Received 17 May 2024
Accepted for publication 20 July 2024
Published 30 July 2024 Volume 2024:17 Pages 3349—3360
DOI https://doi.org/10.2147/IJGM.S466838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Abdallah Damin Abukhalil,* Raya Riyad Abushehadeh,* Sireen Sultan Shatat,* Ni’meh Al-Shami,* Hani A Naseef,* Hosniyeh Ladadweh,* Raed Madia*
Faculty of Pharmacy, Nursing and Health Professions, Birzeit University, Birzeit, West Bank, Palestine
*These authors contributed equally to this work
Correspondence: Abdallah Damin Abukhalil; Hosniyeh Ladadweh, Faculty of Pharmacy, Nursing and Health Professions, Birzeit University, Birzeit, West Bank, Palestine, Email [email protected]; [email protected]
Background: Coronavirus disease (COVID-19) vaccines play an essential role in boosting immunity, preventing severe diseases, and alleviating the Covid-19 health crisis.
Objective: This study aimed to explore the type and severity of short-term adverse reactions associated with BNT162 (Pfizer-BioNTech), mRNA 1273 (Moderna), and viral vector vaccines and to compare the incidence of post-vaccination Covid-19 infection among the Birzeit University community in Palestine.
Methods: This questionnaire-based retrospective cross-sectional study was conducted among individuals who were vaccinated with at least one dose of any COVID-19 vaccine offered in Palestine during the COVID-19 pandemic. The study included participants aged 18 years and older who were vaccinated with Pfizer, Moderna, Sputnik Light, or Sputnik v.
Results: A total of 558 participants who were administered COVID-19 vaccine were included in the study. Sputnik (239), Pfizer vaccine recipients (236), and Moderna vaccine recipients (83). Of the viral vector vaccine recipients, 57 (23.8%) had a post-vaccination infection, compared to 30 (12.7%) for Pfizer and seven (8.4%) for Moderna. Furthermore, the reported adverse effects in the viral victor group were higher than those in the Moderna and Pfizer groups (71.7, 66.3, and 61.9%, respectively). Chills, headache, fatigue, abdominal pain, and joint pain were significantly higher in the Viral Vector vaccine group than the Moderna and Pfizer vaccine. Vomiting, tiredness, and fatigue were significantly less likely to be complained of by Pfizer vaccine recipients compared to Moderna and Viral Vector vaccine recipients (p < 0.05).
Conclusions: Breakthrough infections were associated with both viral vectors and mRNA; however, the mRNA vaccine had less reported post-vaccine infection. Furthermore, the Pfizer/BioNTech COVID-19 vaccine group reported fewer commonly reported side effects (fever, chills, headache, fatigue, muscle pain, joint pain, nausea, and dizziness), followed by the Moderna and viral vector vaccines. Females and underweight participants experienced more adverse effects with both vaccines, and fewer common side effects were reported by all participants.
Keywords: Covid-19 vaccine, viral vector vaccine, Sputnik, Moderna, Pfizer, breakthrough infection, adverse effects, Palestine
Background
The COVID-19 pandemic has disrupted people’s normal living and taken many people’s lives, resulting in extensive economic closures and curfews in many countries at the beginning of 2020.1 As of May 2024, there have been over 7 million cases and 7.5 million deaths caused by COVID-19 worldwide.2,2 This health crisis has caused a greater responsibility for the medical research community to race for both a cure and vaccine to halt this pandemic. Furthermore, governments have introduced laws and regulations allowing for the rapid development of new COVID-19 vaccines to halt the spread of the virus and save human lives.3,4 Furthermore, rapid global pharmaceutical collaboration and effective medical technology were necessary to introduce vaccines to provide protection and immunization against the SARS-CoV virus, leading to rapid advances in vaccine development virology, molecular biology, and vaccinology.5,6
SARS-Cov-2 vaccines have been granted an Emergency Use Listing (EUL) worldwide by the WHO or Emergency Use Authorization by the Food and Drug Administration, allowing for the use of unapproved vaccination in an emergency or critical situation.4,7,8 Vaccines were manufactured to enhance body immunity using different technologies such as mRNA (Pfizer-BioNTech, Moderna), viral vector (Johnson & Johnson, and Sputnik V), protein subunit (Novavax), and whole or inactivated virus (Sinopharm, COVAXIN, and Sinovac) vaccines.3,9
Each COVID-19 vaccine has specific handling, dosage, storage, administration instructions, efficacy rates, and side effect profiles. Adverse effects associated with COVID-19 vaccines include mild-to-moderate symptoms such as redness, swelling, and pain at the injection site, as well as fatigue, chills, fever, myalgia, headache, diarrhea, and nausea.10–12 In addition to severe reactions such as myocarditis, pericarditis, deep vein thrombosis, transverse myelitis, and even anaphylactic shock.13,14 Furthermore, a rare and serious side effect has been reported with viral vector vaccines, including Guillain-Barre syndrome (GBS), an immune disorder of the nervous system, and thrombocytopenia syndrome (TTS), a fatal blood clotting disorder, and myocarditis, which is cardiac inflammation has been reported with mRNA vaccines.15 As reports of adverse effects about the safety and efficacy of vaccines continue to evolve, information about the safety and efficacy of the COVID-19 vaccines via media has caused considerable anxiety and worries.4 Worldwide, there is a need to continue monitoring and reporting adverse effects associated with COVID-19 vaccines. In addition to adverse effects, breakthrough infections pose a major challenge to COVID-19 vaccination, and it has been established that they are caused by a declining humoral response.16,17 Furthermore, the emergence of SarsCov2 variants has increased the chances of breakthrough infections owing to their increased transmissibility and immune-invasive characteristics. A recent study in Palestine explored the adverse effects associated with Pfizer-BioNTech vaccine. To the best of our knowledge, no study has explored the effectiveness and associated adverse effects of different vaccines used in Palestine during the pandemic.18
This study’s objective is to compare the adverse effects and post-vaccination rates for SARS-CoV-2 infection among individuals vaccinated with various COVID-19 vaccines, including BNT162 (Pfizer-BioNTech), mRNA 1273 (Moderna), Sputnik V, and Sputnik Light (Gamaleya), in Palestine. This study will evaluate the occurrence, extent, type, and severity of adverse reactions associated with vaccinations. Furthermore, this study compared the incidence of Post-vaccination Covid-19 infection among BNT162 (Pfizer-BioNTech), mRNA 1273 (Moderna), and viral vector vaccines.
Materials and Method
Study Design and Sample
A retrospective cross-sectional analytical study was performed among the Birzeit University community in Palestine between December 13, 2021, and March 29, 2022. A Google platform link to a self-administered questionnaire was distributed online through a university website (Ritaj), social media platforms (eg, Facebook and Telegram), and in-person interviews. The study targeted employees, academics, postgraduates, and undergraduates aged 18 years and older who received at least one dose of COVID-19 vaccines, including Pfizer, Moderna, Sputnik Light, or Sputnik v.
Questionnaire (Survey)
The questionnaire was prepared through a standardized method, based on a literature review of similar studies,13,18 and by revising the reports from WHO and Center for Disease Control and Prevention (CDC) websites to review the globally registered adverse effects.19,20
The research team developed, reviewed, evaluated, and rephrased the questionnaire during several meetings to assess content validity. A pilot study was conducted with 32 vaccinated individuals. They were requested to fill out the questionnaire and provide feedback regarding its clarity, consistency, and appropriateness. Based on the pilot response, the final draft was published in Arabic, the respondents’ original language. It must also be noted that the final questionnaire comprised five sections with 27 questions structured as open- and closed-ended multiple-choice questions, and two short essay questions. The first section included sociodemographic data. The second was regarding the infection status of SARSCov-2 before vaccination. Third, the COVID-19 vaccine type and number of doses received. And the fourth section is “COVID-19 vaccines adverse effects”, consisting of 23 possible side effects registered in WHO and CDC leaflets and reports published by randomized control trials on the different COVID-19 vaccines.18,21,22 A space was provided at the end to report any other adverse effects that respondents complained about and were not mentioned. Other questions in this section included the onset and duration of side effects, the participant’s attitude after vaccination, and any doctor visits or hospital admissions due to severe side effects. The last section included four questions regarding the infection status of SARS-Cov-2 after vaccination. (Supplementary file)
Statistical Analysis
Data were analyzed using IBM Statistical Package for the Social Sciences (SPSS) version 22. A descriptive analysis was performed to present the data. Data were imported into SPSS, cleared, categorized, and recoded as needed. BMI was computed from height and weight and classified as underweight (<18.5), normal weight (18.5–24.9), overweight (25.0–29.9), and obese (≥30.0). Age was recoded into two subgroups: <20 years and ≥20 years. Next, vaccine adverse effects were categorized into less common and more common adverse effects according to the CDC classification. Categorical data are presented as frequencies and percentages, whereas means and standard deviations were measured for continuous data. The number of adverse effects reported by each patient was counted to form a new continuous not normally distributed variable, according to the Shapiro–Wilk normality test results. Chi-square (χ2) tests with 95% CI were performed to compare the incidence of COVID-19 infection post-vaccination between viral vector, Pfizer, and Moderna vaccines. Chi-square (χ2) tests with 95% CI were also performed to compare the 23 post-vaccination side effects incidence for the Viral vector, Pfizer, and Moderna vaccines. Mann–Whitney and Kruskal–Wallis H-tests were conducted to establish the association between participant demographics and the counts of the most and least common post-vaccination side effects of COVID-19, respectively. Statistical significance was set at P < 0.05.
Ethical Considerations
The ethical committee of the Faculty of Pharmacy, Nursing, and Health Professions at Birzeit University approved this study (reference number: BZU-PNH-2103). The study complied with the ethical guidelines of the Declaration of Helsinki. Informed consent was obtained from the participants prior to participation in the study.
Results
Demographic Characteristics
In total, 558 participants met the inclusion criteria. The mean age of the patients was 24.547 ± 10.184 years, and the majority 72.2% were 20 years or older. In addition, more than half of them were female (60.8%) and free from chronic diseases (89.6%). 28.3% of the respondents were smokers and 15.2% had drug/food allergies. (Further information on each vaccine is provided in Table 1).
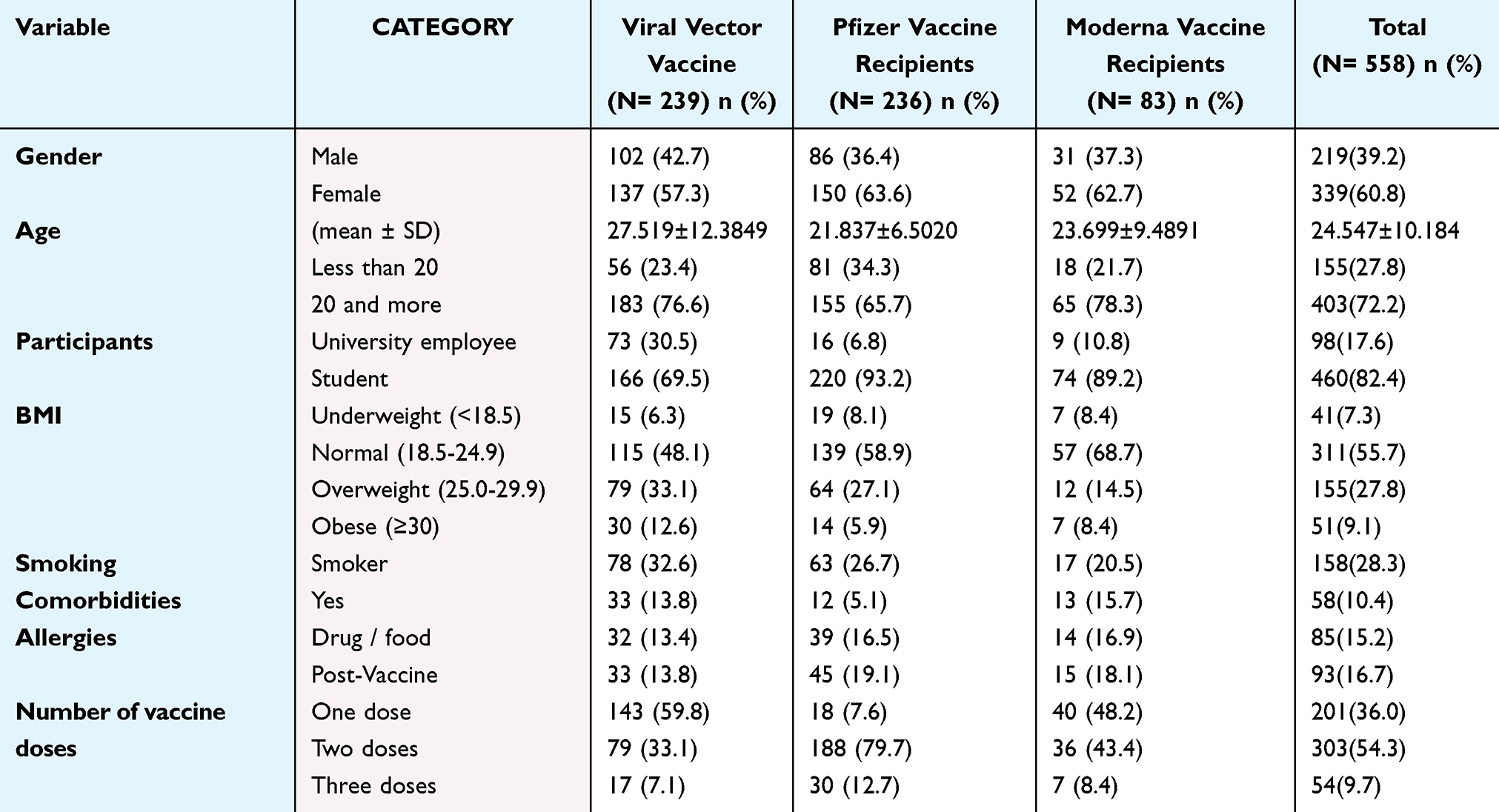 |
Table 1 Demographic Characteristics of Covid-19 vaccines recipients (N= 558) |
COVID-19 Infection
The Covid-19 infection status of participants both before and after they received the COVID-19 vaccination is shown in Figure 1. A total of 158 (28.3%) participants were infected with SARS-CoV-2 before COVID-19 vaccination and 94 (16.9%) patients were infected post-vaccination. Depending on the type of vaccination, 57 (23.8%) viral vector vaccine recipients were infected post-vaccination at a time ranging from less than one month to six months after receiving the vaccine. However, the percentage is lower in mRNA-based vaccines, which are 30 (12.7%) for Pfizer and 7 (8.4%) for Moderna. (Figure 2)
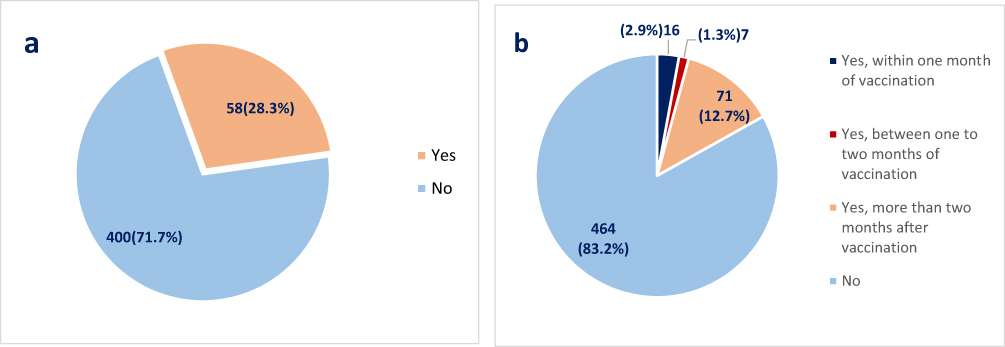 |
Figure 1 Covid-19 infection Status (N= 558). (a) Pre-vaccination, (b) post-vaccination. |
 |
Figure 2 Comparison of Post-vaccination Covid-19 infection between viral vector, Pfizer, Moderna vaccines (N= 94), chi-square test (p-value <0.001). |
Post-Vaccination Side Effects
BioNTech, Pfizer vaccine
The most frequently reported side effects after administration of the initial dose of the BioNTech Pfizer vaccine were fever (41.9%), headache (38.1%), tiredness and fatigue (32.2%), muscle pain (31.4%), pain, redness, or swelling at the site of the vaccine injection (30.9%), chills (28.4%), joint pain (23.7%), and dizziness (19.1%). Other side effects that are reported less commonly (<15%) are persistent cough, shortness of breath, menstrual cycle changes in females, increased heart rate, nausea, sleep disturbances, chest pain, hoarseness of the voice, diarrhea, ear tinnitus, abdominal pain, increase in blood pressure, vomiting, armpit swelling, and knee swelling (Figures 3 and 4). However, 38.1% of the participants who received the BNT162 vaccine did not experience any side effects. As shown in Figure 5, side effects began to manifest within 12 h of vaccination, according to 50% of the participants who received the Pfizer vaccine, and in 39.8% of those people, the side effects that appeared after vaccination continued for one–three days.
 |
Figure 3 Comparison of the frequencies of the most common side effects of Pfizer, Moderna, and viral vector COVID-19 vaccines. |
 |
Figure 4 Comparison of the frequencies of less common side effects between Pfizer, Moderna, and viral vector COVID-19 vaccines. |
 |
Figure 5 Side effects after Covid-19 vaccination (a) Onset of side effects, (b) Duration of side effects. |
Figure 3 shows how different vaccines affected the recipients’ daily activities; less than one-fifth of the participants had experienced post-vaccination allergic reactions or shoulder injuries. Furthermore, over 95% of the respondents revealed that they had overcome the adverse effects either by rest or painkiller administration, and approximately three-fourths of the participants did not miss any working days.
Moderna’s mRNA-1273
The most frequent side effects reported after administration of the Moderna vaccine were fever (47.0%), fatigue (44.6%), headache (42.2%), muscle pain (32.5%), chills (31.3%), joint pain (28.9%), pain, redness, or swelling at the site of vaccine injection (27.7%), dizziness (22.9%), shortness of breath (19.3%), and nausea (18.1%). Other side effects that are reported less commonly (<15%) are menstrual cycle changes in females, an increase in heart rate, chest pain, sleep disturbances, ear tinnitus, persistent cough, increased blood pressure, vomiting, abdominal pain, hoarseness of the voice, diarrhea, armpit swelling, and knee swelling (Figures 3 and 4). However, 33.7% of the participants who received the mRNA-1273 vaccine did not experience any side effects. As shown in Figure 5, side effects began to manifest within 12 h of vaccination, according to 53% of the participants who received the Moderna vaccine. In 48.2% of the participants, the side effects that appeared after vaccination continued for one–three days.
Viral Vector Vaccines (Sputnik V and Light; Gam-COVID-Vac)
The most frequently reported side effects of viral vector vaccines were tiredness and fatigue (52.3%), fever and headache (51.5%), chills (41.0%), joint pain (37.2%), muscle pain (35.6%), redness, swelling, and pain at the site of the vaccine injection (27.6%), dizziness (26.8%), menstrual cycle changes (17.5%), and shortness of breath (16.3%). Other side effects that are reported less commonly (<15%) are nausea, chest pain, abdominal pain, sleep disturbances, increased heart rate, persistent cough, ear tinnitus, hoarseness of the voice, vomiting, diarrhea, increased blood pressure, armpit swelling, and knee swelling (Figures 4 and 5). However, 29.3% of the participants who received the Sputnik vaccine did not experience any side effects. As shown in Figure 3, the side effects began to manifest within 12 h of vaccination, according to 51% of the participants who received the Sputnik vaccine, and in 43.2% of those participants, the side effects that appeared after vaccination continued for one–three days.
Variation in Post-Vaccination Side Effects Among Vaccinations
Table 2 presents the variation of side effects reported among the three vaccines; chills, headache, fatigue, abdominal pain, and joint pain were significantly reported by participants who received the Viral Vector vaccine than by Moderna and Pfizer vaccine recipients. Vomiting, tiredness, and fatigue were significantly less likely to be complained of by Pfizer vaccine recipients compared to Moderna and Viral Vector vaccine recipients (p < 0.05). However, there were no significant differences among the other reported side effects.
 |
Table 2 Post-vaccination side effects reported by Viral vector, Pfizer, and Moderna vaccine recipients (N= 558) |
Most Common Side Effects Intensity and Patient Characteristics
Table 3 shows the patterns of the intensity of the side effects reported by the participants for the different vaccines, based on patient characteristics. Females, underweight participants, and participants without chronic diseases who received viral vectors experienced significantly more common side effects. Females, underweight, patients who complained of at least one chronic disease, participants with a history of allergy, or had a history of COVID-19 infection and received Pfizer vaccine reported significantly more common side effects. Furthermore, Moderna vaccine recipients, who were younger or had a history of allergies, had significantly more common side effects.
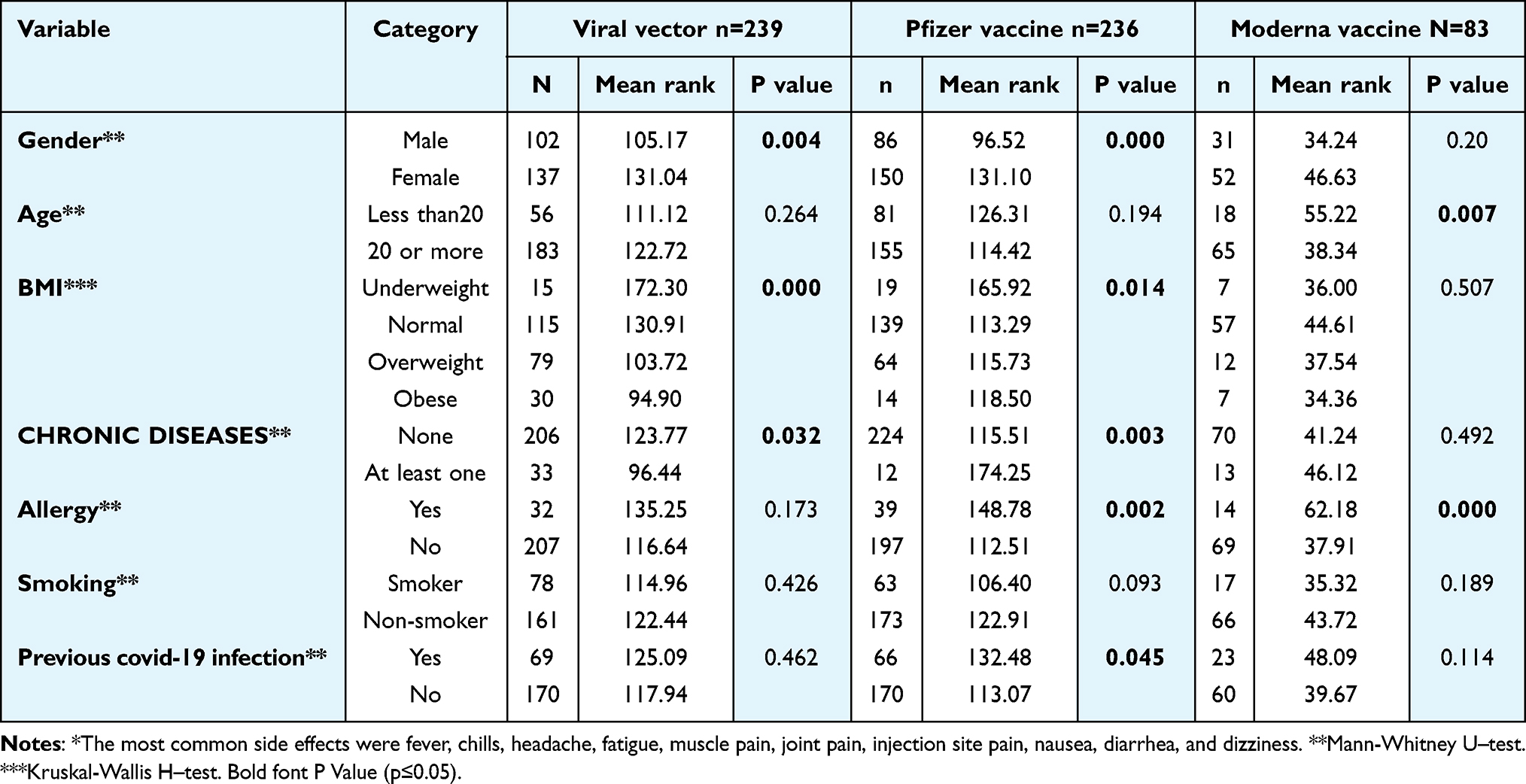 |
Table 3 Association between post-vaccination most common side effects *reported by the participants and their predisposing factors. (N= 558) |
Fewer Common Side Effects Intensity and Patient Characteristics
Table 4 shows the patterns of fewer common side effects reported by different vaccine recipients based on patient characteristics. Male and overweight participants who received viral vectors were significantly less likely to report fewer common side effects. Females, patients who complained of at least one chronic disease, or with a history of allergy and received Pfizer vaccine, reported significantly fewer common side effects. Moreover, younger participants with a history of allergies who received Moderna vaccine had significantly fewer common side effects.
 |
Table 4 Association between post-vaccination fewer common side effects* Reported by the Participants and their predisposing factors. (N= 558) |
Discussion
Several covid-19 vaccines have been authorized for human use to compact SARS-Cov2 infections. In this study, we explored and compared the prevalence of side effects and reinfection rates following the administration of three different types of Covid-19 vaccines BNT162 (Pfizer-BioNTech), mRNA 1273 (Moderna), and a viral vector. Both classes of vaccines have been effective in targeting SARS Cov2 viruses. mRNA vaccines do not use a live virus, whereas the viral vector vaccine uses a modified version of the non-replicating virus and does not cause the disease.
A breakthrough COVID-19 infection is defined by the Centers for Disease Control and Prevention (CDC) as a positive COVID-19 test 14 days or more after completing all recommended doses of an FDA-approved COVID-19 vaccine. However, the World Health Organization (WHO) states that vaccinations certified for emergency use or allowed for use by regulatory agencies in various countries are very effective in reducing the risk and severity of infection, particularly serious disease and death. The effectiveness of a vaccine can vary based on the vaccine, the viral variations in circulation, and the period since inoculation.23
Vaccine efficacy deterioration over time is a major concern that calls for further research to improve vaccine effectiveness.22,24 In This study, 71% of breakthrough infections developed within 2–6 months of the full vaccination date. Another study found that 52.9% of those who received the second dose of vaccine experienced a breakthrough infection after 28 days.25 The frequency of breakthrough infections in vaccine recipients differed significantly based on the type of vaccine administered, as our study revealed that viral vector vaccines displayed a higher breakthrough rate than mRNA vaccines. Interestingly, a similar observation was made in a prospective cohort study conducted in Belgium.26 Furthermore, a systemic meta-analysis concluded that mRNA vaccines had the highest likelihood of being effective against systemic COVID-19 infections compared to other types of vaccines.27
Breakthrough infections post-vaccination are still an area of research, and no COVID-19 vaccine has demonstrated 100% effectiveness. As a result, despite full immunization, a subset of the population remains susceptible to SARS CoV-2.28 Possible explanations include a rise in the number of vaccinated people, a decline in vaccine-induced antibody levels, the emergence of variations with reduced sensitivity to vaccine-induced antibodies, and a reduction in preventive recommendations for the community.29
In addition to vaccine efficacy, side effects are another major factor that can be considered when selecting or comparing vaccines. Transient side effects are expected during or after vaccine administration owing to immune system activation and trauma to the injection site. The CDC reports that the most frequent side effects of COVID-19 immunization include swelling, pain, and redness at the injection site, as well as fatigue, chills, fever, muscle aches, headaches, and nausea.20
In this study, the commonly reported side effects were lower in the Pfizer group, followed by the Moderna and viral vector vaccines. This is true for all the common side effects reported except for the injection site pain, which was more common with the Pfizer vaccine; diarrhea, which was least common in the Moderna vaccine; and nausea, which was more common in the Moderna group than in the other types of vaccines. This finding contradicts that of a recent comprehensive review conducted by Pordanjani. et, where the occurrence of local side effects was more common with mRNA-based vaccines, which includes Pfizer and Moderna vaccines, as compared to viral vector vaccines.30 Furthermore, in a regional study in Saudi Arabia, viral vector recipient reported fewer side effects.31 The Advisory Committee on Immunization Practices (ACIP) prefers mRNA over viral vector vaccines because mRNA vaccines have not been associated with the rare side effect, Guillain-Barre syndrome, which can occur with viral vector vaccines. Moreover, mRNA vaccines have proven to be more effective.32
Several factors may influence the prevalence of adverse effects. In this study, there was no statistically significant association between age and common adverse effects associated with the administration of Pfizer and viral vector vaccines. In contrast, Moderna vaccine recipients who were younger had significantly more common side effects. Different finding was reported by other studies, a British study by Menni et al, reported that people aged 55 and under had a significantly higher rate of side effects after both mRNA-based and viral vector-based vaccines.33 A regional study in Saudi Arabia reported adults aged 60 years or older had a substantially higher level of local side effects, including injection site pain than their younger counterparts who received the BNT162b2 vaccine.34
Female patients showed significantly more common side effects for both the viral vectors and Pfizer vaccines. That completely different according to a study published in Jordan by Abu Hammad et al, there were no significant differences between males and females in the development of systemic adverse effects.35 Where Alghamdi et al, 2021 discovered within a viral vector-based vaccine recipients group that the occurrence of post-vaccination side effects was substantially higher in females than males.36 This study also showed that patient with Pfizer and Moderna vaccines with history of allergy experienced significantly more common side effects. Therefore, according to the Medicines and Healthcare Products Regulatory Agency (MHRA), it is recommended to provide the vaccine with caution to those who have any history of an adverse reaction to vaccination, drug, or food, especially people who have an adrenaline auto-injector in emergency situations.37
The three vaccines have reported fewer common side effects (<15%), including persistent cough, shortness of breath, increased heart rate, sleep disturbances, chest pain, hoarseness of the voice, ear tinnitus, abdominal pain, increase in blood pressure, vomiting, armpit swelling, and knee swelling. This is similar to the study by Abu Hammad et al, which found that a small number of patients reported gastrointestinal (nausea, vomiting, and diarrhea) and respiratory side effects (dyspnea). As well as ear complaints, facial pain, drowsiness, and diuresis.35
Underweight patients who were administered Pfizer and viral vector vaccines experienced more adverse effects after vaccination. A study in Spain which was published in 2021 studied the association between COVID19 vaccines side effects and body mass index (BMI) found that after controlling for sex and age, the majority of the substantial effects in the relationship between COVID-19 vaccination adverse effects and weight status were no longer significant.38 Also a systemic review study published in China in 2023 discovered that newer coronavirus vaccinations may produce higher adverse effects in non-obese adults, providing some new recommendations for the design and emphasis of follow-up research.39
In this study, 39.8% of the participants experienced adverse effects one–three days after vaccination. This is comparable to the study conducted among healthcare workers in Germany indicating good safety findings for both forms of vaccinations.40
Strengths and Limitations
This is the first study conducted in Palestine during the covid-19 pandemic that compares mRNA vaccines and viral vectors among higher education communities. The data collected were self-reported based on participant perception of side effects and were not evaluated by healthcare providers due to the retrospective nature of the study, which might have led to information bias. The questionnaire was distributed online; therefore, there was a possibility of selection bias. Furthermore, most participants were younger, which might have affected the results because elderly participants might have had different comorbidities that might affect vaccine efficacy and toxicity. Further research is needed to extrapolate these results to the general population.
Conclusion
As the pandemic of Sars Cov-2 is unfolding, post-vaccine long-term immunity and adverse effects continue to be challenging for the medical and research community; therefore, continuous research, long-term studies, and reporting of adverse effects that might be associated with covid −19 vaccines are essential to ensure vaccine safety and efficacy.
In this study, breakthrough infection was associated with both viral victors and mRNA; however, the mRNA vaccine had fewer reported post-vaccine infections. Furthermore, the Pfizer/BioNTech COVID-19 vaccine group reported fewer commonly reported side effects (fever, chills, headache, fatigue, muscle pain, joint pain, nausea, and dizziness), followed by the Moderna and Viral Vector vaccines. Females and underweight participants experienced more adverse effects with both vaccines, and fewer common side effects were reported by all participants. The findings of this study can be used to inform the general population about the adverse effects of the Sars-Cov-2 vaccine.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mofijur M, Fattah IMR, Alam MA. et al. Impact of COVID-19 on the social, economic, environmental and energy domains: lessons learnt from a global pandemic. Sustain Prod Consum. 2021;26:343–359. doi:10.1016/j.spc.2020.10.016
2. World Health Organization. WHO Coronavirus (COVID-19 Dashboard); Available from: https://data.who.int/dashboards/covid19/cases?n=c.
3. Badgujar KC, Badgujar VC, Badgujar SB. Vaccine development against coronavirus (2003 to present): an overview, recent advances, current scenario, opportunities and challenges. Diabetes Metab Syndr. 2020;14(5):1361–1376. doi:10.1016/j.dsx.2020.07.022
4. Kashte S, Gulbake A, El-Amin SF, Gupta A. COVID-19 vaccines: rapid development, implications, challenges and future prospects. Hum Cell. 2021;34(3):711–733. doi:10.1007/s13577-021-00512-4
5. Kesselheim AS, Darrow JJ, Kulldorff M, et al. An overview of vaccine development, approval, and regulation, with implications for COVID-19. Health Aff. 2021;40(1):25–32. doi:10.1377/hlthaff.2020.01620
6. Lurie N, Saville M, Hatchett R, Halton J. Developing Covid-19 vaccines at pandemic speed. N Engl J Med. 2020;382(21):1969–1973. doi:10.1056/NEJMp2005630
7. World Health Organization (WHO). 12 Vaccines Granted Emergency Use Listing (EUL) by WHO. COVID 19 VACCINE TRACKER; 2022.
8. U.S. Food and Drug Administration. Emergency use authorization for vaccines explained; Available from: https://www.fda.gov/vaccines-blood-biologics/vaccines/emergency-use-authorization-vaccines-explained.
9. Deng S, Liang H, Chen P, et al. Viral vector vaccine development and application during the COVID-19 Pandemic. Microorganisms. 2022;10(7):1450. doi:10.3390/microorganisms10071450
10. Omeish H, Najadat A, Al-Azzam S, et al. Reported COVID-19 vaccines side effects among Jordanian population: a cross sectional study. Hum Vaccin Immunother. 2022;18(1). doi:10.1080/21645515.2021.1981086
11. Karuppannan M, Ming LC, Abd Wahab MS, Mohd Noordin Z, Yee S, Hermansyah A. Self-reported side effects of COVID-19 vaccines among the public. J Pharm Policy Pract. 2024;17(1). doi:10.1080/20523211.2024.2308617
12. Mahmood A, Shujaat SA, Hayat M, et al. Acute adverse effects of vaccines against SARS-COV-2. Cureus. 2022. doi:10.7759/cureus.27379
13. Azimi M, Dehzad WM, Atiq MA, Bahain B, Asady A. Adverse effects of the COVID-19 vaccine reported by lecturers and staff of Kabul University of medical sciences, Kabul, Afghanistan. Infect Drug Resist. 2021;Volume 14:4077–4083. doi:10.2147/IDR.S332354
14. Qashqari FS, Alfelali M, Barasheed O, et al. Evaluation of the most visible symptoms associated with COVID-19 vaccines among the residents of Makkah, Saudi Arabia: an observational, cross-sectional study. Infect Drug Resist. 2023;Volume 16:5107–5119. doi:10.2147/IDR.S409200
15. Rosenblum HG, Hadler SC, Moulia D, et al. Use of COVID-19 vaccines after reports of adverse events among adult recipients of Janssen (Johnson & Johnson) and mRNA COVID-19 vaccines (Pfizer-BioNTech and Moderna): update from the advisory committee on immunization practices — United States. MMWR Morb Mortal Wkly Rep. 2021;70(32):1094–1099. doi:10.15585/mmwr.mm7032e4
16. Ghattas M, Dwivedi G, Lavertu M, Alameh MG. Vaccine technologies and platforms for infectious diseases: current progress, challenges, and opportunities. Vaccines (Basel). 2021;9(12). doi:10.3390/vaccines9121490
17. Notarte KI, Ver AT, Velasco JV, et al. Effects of age, sex, serostatus, and underlying comorbidities on humoral response post-SARS-CoV-2 Pfizer-BioNTech mRNA vaccination: a systematic review. Crit Rev Clin Lab Sci. 2022;59(6):373–390. doi:10.1080/10408363.2022.2038539
18. Abukhalil AD, Shatat SS, Abushehadeh RR, Al-Shami N, Naseef HA, Rabba A. Side effects of Pfizer/BioNTech (BNT162b2) COVID-19 vaccine reported by the Birzeit University community. BMC Infect Dis. 2023;23(1):5. doi:10.1186/s12879-022-07974-3
19. World Health Organization. “Side Effects of COVID-19 Vaccines”. World Health Organization. 2024; Available from: https://www.who.int/news-room/feature-stories/detail/side-effects-of-covid-19-vaccines.
20. Centers for Disease Control and Prevention. Safety Information for Covid-19 Vaccines. CDC Vaccine Safety. Published February. 2024; 13.
21. Hause AM, Baggs J, Marquez P, et al. Safety monitoring of COVID-19 vaccine booster doses among persons aged 12–17 years — United States, December 9, 2021–February 20, 2022. MMWR Morb Mortal Wkly Rep. 2022;71(9):347–351. doi:10.15585/mmwr.mm7109e2
22. World Health Organization. World health organization. global manual on surveillance of adverse events following immunization. Availble from: https://www.who.int/publications/i/item/10665206144..
23. Pollard AJ, Bijker EM. A guide to vaccinology: from basic principles to new developments. Nat Rev Immunol. 2021;21(2):83–100. doi:10.1038/s41577-020-00479-7
24. Kandeel A, Fahim M, Deghedy O, et al. Clinical features and severe outcome predictors of COVID-19 vaccine breakthrough infection among hospitalized patients: results from Egypt severe acute respiratory infections sentinel surveillance, 2021–2022. BMC Infect Dis. 2023;23(1):130. doi:10.1186/s12879-023-08097-z
25. Hussein AARM, Hashem MK, Azizeldine MG, Shaddad AM. Prevalence and characteristics of COVID-19 vaccine breakthrough infection in Upper Egypt. Egypt J Bronchol. 2023;17(1):21. doi:10.1186/s43168-023-00196-4
26. Stouten V, Hubin P, Haarhuis F, et al. Incidence and risk factors of COVID-19 vaccine breakthrough infections: a prospective cohort study in Belgium. Viruses. 2022;14(4):802. doi:10.3390/v14040802
27. Rotshild V, Hirsh-Raccah B, Miskin I, Muszkat M, Matok I. Comparing the clinical efficacy of COVID-19 vaccines: a systematic review and network meta-analysis. Sci Rep. 2021;11(1):22777. doi:10.1038/s41598-021-02321-z
28. Singh CM, Singh PK, Naik BN, Pandey S, Nirala SK, Singh PK. Clinico-epidemiological profile of breakthrough COVID-19 infection among vaccinated beneficiaries from a COVID-19 vaccination centre in bihar, India. Ethiop J Health Sci. 2022;32(1):15–26. doi:10.4314/ejhs.v32i1.3
29. Bates TA, McBride SK, Winders B, et al. Antibody response and variant cross-neutralization after SARS-CoV-2 breakthrough infection. JAMA. 2022;327(2):179. doi:10.1001/jama.2021.22898
30. Pordanjani SR, Pordanjani AR, Askarpour H, et al. A comprehensive review on various aspects of SARS-CoV-2 (COVID-19) Vaccines. Int J Prev Med. 2022;13(1):151. doi:10.4103/ijpvm.ijpvm_513_21
31. Almughais ES, Alharbi AH, Aldarwish HA, et al. Side-effects of COVID-19 vaccines among the Saudi population: a cross-sectional study. Saudi Med J. 2022;43(4):386–393. doi:10.15537/smj.2022.43.4.20210905
32. Oliver SE, Wallace M, See I, et al. Use of the Janssen (Johnson & Johnson) COVID-19 Vaccine: updated interim recommendations from the advisory committee on immunization practices — United States, December 2021. MMWR Morb Mortal Wkly Rep. 2022;71(3):90–95. doi:10.15585/mmwr.mm7103a4
33. Menni C, Klaser K, May A, et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: a prospective observational study. Lancet Infect Dis. 2021;21(7):939–949. doi:10.1016/S1473-3099(21)00224-3
34. El-Shitany NA, Harakeh S, Badr-Eldin SM, et al. Minor to moderate side effects of pfizer-bioNTech COVID-19 Vaccine among Saudi residents: a retrospective cross-sectional study. Int J Gen Med. 2021;14:1389–1401. doi:10.2147/IJGM.S310497
35. Abu-Hammad O, Alduraidi H, Abu-Hammad S, et al. Side effects reported by Jordanian healthcare workers who received COVID-19 vaccines. Vaccines (Basel). 2021;9(6). doi:10.3390/vaccines9060577
36. Alghamdi AA. Impact of the COVID-19 pandemic on the social and educational aspects of Saudi University students’ lives. PLoS One. 2021;16(4):e0250026. doi:10.1371/journal.pone.0250026
37. Gov UK. MHRA Guidance on Coronavirus (COVID-19).1:1.
38. Iguacel I, Maldonado AL, Ruiz-Cabello AL, Casaus M, Moreno LA, Martínez-Jarreta B. Association between COVID-19 vaccine side effects and body mass index in Spain. Vaccines. 2021;9(11):1321. doi:10.3390/vaccines9111321
39. Fu C, Lin N, Zhu J, Ye Q. Association between overweight/obesity and the safety and efficacy of COVID-19 vaccination: a systematic review. Vaccines (Basel). 2023;11(5). doi:10.3390/vaccines11050996
40. Klugar M, Riad A, Mekhemar M, et al. Side effects of mRNA-based and viral vector-based COVID-19 vaccines among German healthcare workers. Biology. 2021;10(8). doi:10.3390/biology10080752
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Immune Thrombocytopenia Relapse in Patients Who Received mRNA COVID-19 Vaccines
Qasim H, Rahhal A, Husain A, Alammora A, Alsa’ed K, Alsayed AAM, Faiyoumi B, Maen AbuAfifeh L, Abu-Tineh M, Alshurafa A, Yassin MA
Journal of Blood Medicine 2023, 14:295-302
Published Date: 14 April 2023
Clinical Characteristics and Outcomes of Vaccinated VS Non-Vaccinated Critically Ill COVID-19 Patients: Retrospective Observation Study
AlQahtani SY, Alabdulqader AA, Al Mashhour WA, Aldawood ZM, Al Masari OA, Alotaibi T, AlGhamdi ZM, Alzahrani IM, Albaloushi NN
Infection and Drug Resistance 2023, 16:3329-3338
Published Date: 29 May 2023