")
Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Characteristics and Outcomes of Vaccinated VS Non-Vaccinated Critically Ill COVID-19 Patients: Retrospective Observation Study
Authors AlQahtani SY , Alabdulqader AA, Al Mashhour WA, Aldawood ZM, Al Masari OA , Alotaibi T, AlGhamdi ZM , Alzahrani IM , Albaloushi NN
Received 6 March 2023
Accepted for publication 18 May 2023
Published 29 May 2023 Volume 2023:16 Pages 3329—3338
DOI https://doi.org/10.2147/IDR.S411299
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Shaya Yaanallah AlQahtani,1 Ahmed Anwer Alabdulqader,2 Waleed Abdulrahman Al Mashhour,3 Zahra Mohammed Aldawood,4 Osama Ali Al Masari,1 Thabit Alotaibi,1 Zeead M AlGhamdi,5 Ibrahim M Alzahrani,6 Noor Nabil Albaloushi7
1Department of Internal Medicine and Critical Care Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2King Fahad Hospital Hofuf, Hofuf, Saudi Arabia; 3Dammam Medical Complex, Dammam, Saudi Arabia; 4King Khalid Hospital- AlKharaj, Alkharaj, Saudi Arabia; 5Thoracic Surgery Division, Department of Surgery, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 6Department of Internal medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 7Ministry of Health, Dammam, Saudi Arabia
Correspondence: Shaya Yaanallah AlQahtani, Department of Internal Medicine and Critical Care Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, P.O. Box. 2208, Dammam, 31952, Saudi Arabia, Email [email protected]
Objective: We aim to identify the clinical characteristics and outcome of vaccine breakthrough infection in critically ill COVID-19 patients and to compare the clinical course of disease between vaccinated and non-vaccinated patients.
Methods: A retrospective review of all adult patients aged ≥ 18 years admitted to the ICU in King Fahd Hospital of the University in Saudi Arabia with positive COVID-19 RT-PCR test between the period of January 1st to August 31st, 2021, were included. The recruited patients were grouped in to “vaccinated and non-vaccinated group” based on their immunization status. The demographic data, co-morbidities, modality of oxygen support, ICU length of stay (ICU LOS) and mortality were collected and analyzed.
Results: A total of 167 patients were included. Seventy-two patients (43%) were vaccinated. Cardiovascular diseases were higher among the vaccinated group (33.3% vs 12.6%, p value < 0.001). Requirements of Non-invasive ventilation was significantly lower in vaccinated group compared to non-vaccinated group (73.6% vs 91.6%, p value < 0.011). The rates of intubation were similar between both groups. The total intubation days was longer in non-vaccinated patients compared to vaccinated patients and the median duration of intubation was 8 days vs 2 days, respectively (p value 0.027). In subgroup analysis, the P/F ratio was significantly higher in patients who received two doses of vaccine compared to single dose (p value < 0.002).
Conclusion: In critically ill COVID-19 patients, the vaccinated group has significantly less need for Non-invasive ventilation, fewer intubation days and less hypoxia compared to non-vaccinated patients. We recommend more policies and public education nationwide and worldwide to encourage vaccination and raise awareness of the general population.
Keywords: COVID-19 vaccine, breakthrough infection, intensive care unit, vaccine effectiveness, inflammatory markers
Introduction
Coronavirus disease 2019 (COVID-19) was initially discovered in Wuhan, China, in December 2019. COVID-19 primarily affects the respiratory system and is caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2).1 In March 2020, the disease was declared a pandemic by the World Health Organization (WHO).2,3 The ongoing pandemic is an unpredictable challenge to global health that has never been experienced before. Since the pandemic started and until December 2021, nearly 518 million positive cases were discovered, and over 6 million deaths were reported internationally.4 Introducing the COVID-19 vaccine gave new hope to fight against the pandemic and to contain the disease. In Saudi Arabia, three vaccines have been approved to be used against SARS-CoV-2 infection: Pfizer/BioNTech, Oxford-AstraZeneca, and Moderna. These vaccines have demonstrated a good safety profile and provide high efficacy against symptomatic COVID-19 infections.5,6 The vaccines’ effectiveness was found to be 87% in preventing hospitalization after receiving the second dose of the vaccine in an early case-control study.7 Recently, reports from multiple countries demonstrated the efficacy of the vaccines in reducing hospitalization and disease severity. A study from the United States showed 94% reduction in disease severity after receiving two doses of an mRNA vaccine.8 Moreover, two studies from the United Kingdom revealed that the vaccine efficacy of a single dose of BNT162b2 reached up to 80–91% in preventing hospitalization.9,10 In Saudi Arabia, since the beginning of the vaccination campaign, more than 65 million vaccine doses have been given.11 However, despite the effectiveness of the COVID-19 vaccine in reducing the disease severity and hospitalization, a minority of vaccinated individuals might still acquire the infection and experience significant morbidity. The data on the incidence of COVID-19 vaccine breakthrough infections are limited. However, as reported in previous studies, most breakthrough infections occur in older patients with multiple co-morbidities.12 According to the literature, the data on clinical characteristics and outcomes of patients suffering severe SARS-CoV-2 illness leading to Intensive Care Unit (ICU) admission after their first or second dose of vaccine compared to non-vaccinated individuals are scarce.
Therefore, our aim was to describe the clinical characteristics, disease severity, and outcomes in individuals with SARS-CoV-2 infection requiring ICU admission after their first or second dose of vaccination and comparing them with non-vaccinated individuals.
Materials and Methods
Research Design and Settings
This is a retrospective observational study that evaluated all patients admitted to the Intensive Care Unit (COVID-19 ICU) at King Fahad Hospital of the University (KFHU), Al Khobar, Eastern Province, Kingdom of Saudi Arabia. The study followed the ethical standards of the institutional and national research committees and the Helsinki Declaration. Ethical approval for this study was obtained from the institutional review board at Imam Abdulrahman Bin Faisal University (IRB-2022-01-173). This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).
We reviewed the records of 167 adults who were confirmed to be positive for SARS-CoV-2 infection and were admitted to ICU (COVID-19 ICU) at KFHU between January and August 2021. We included patients aged 18 years and above, who were Saudi and residents of Al Khobar, Eastern Province, Saudi Arabia. Patients who were under the age of 18 years, pregnant women and those who had an incidental positive test for SARS-CoV-2 without symptoms were excluded. All admitted patients to the ICU who were diagnosed to have COVID-19 infection were recruited from the electronic medical records system (QuadraMed).
Viral Assays
According to the recommendations from the Saudi Center for Disease Prevention and Control guidelines, the diagnosis of COVID-19 disease was made by taking swabs from the patient’s oropharyngeal and nasopharyngeal orifice/s by experienced personnel. Certified laboratory personnel ran the sample investigation according to the manufacturer’s recommendations for each target gene’s defined cut-off cycle threshold value by using RNA using ViiA7 RT-PCR (Thermo Fisher Scientific, Waltham, MA, USA) and Altona reagents (Altona Diagnostics, Hamburg, Germany).13,14
Data Collection and Analysis
Data of eligible patients were extracted from the Electronic Medical Records (QuadraMed). All recruited patients’ profiles were distributed into two groups based on their immunization status: non-immunized patients (patients who did not receive the COVID-19 vaccine) and immunized patients (partially or fully vaccinated patients).15–17 For both groups, the following parameters were collected: 1) baseline characteristics and demographic data (age, gender, body mass index [BMI], and smoking status), date of first positive COVID-19 PCR test, co-morbidities (obesity, diabetes mellitus, hypertension, chronic pulmonary diseases, cardiovascular diseases, chronic kidney diseases, and immunosuppressed status), and immunization status; 2) Laboratory investigations (white blood cells, with lymphocytic count, ferritin level, C-reactive protein [CRP], D-dimer, lactate dehydrogenase level [LDH]; 3) Modality of oxygen support required (high flow nasal cannula (HFNC), non-invasive ventilation including Bilevel-positive airway pressure [BIPAP], Continuous positive airway pressure [CPAP], Helmet ventilation, and invasive mechanical ventilation and its duration); 4) ICU length of stay (LOS); 5) Mortality.
Data analysis was done by using the Statistical Package for the Social Sciences (IBM SPSS version 22.2). A descriptive analysis of the clinical and laboratory parameters was performed by using Fisher’s exact probability test or chi-square test for categorical variables, while the Mann–Whitney U-test or Student’s t-test was used for continuous variables. Significance was deemed at a p-value < 0.05 with a confidence interval set at 95%.
The main goal of this study is to identify the clinical characteristics and demographic risk factors associated with breakthrough infections among vaccinated individuals admitted to ICU. In addition to compare the clinical course of the disease between vaccinated and non-vaccinated individuals (number of patients who required HFNC, non- invasive ventilation, invasive mechanical ventilation, duration of invasive mechanical ventilation, ICU LOS and mortality).
Results
A total of 167 patients with positive SARS-CoV-2 infection admitted to the ICU were included in our study. Of these patients, nearly two-thirds (n=95) were not vaccinated, and one-third received at least a single dose of the vaccine (n=72). The vaccinated group consisted of 55.5% males and 44.5% females. The mean age was 58.7 years (±16.1 years) (n=72). On the other hand, the non-vaccinated group included 62.1% males and 37.9% females, the mean age was 60.6 years (±17.2 years) (n=95). Less than 10% of the patients were smokers in both groups. Moreover, the vast majority of patients had underlying comorbidities. The predominant comorbid conditions identified were diabetes mellitus (54%), hypertension (51.5%), obesity (41%), and cardiovascular disease (22%). The percentage of patients with a history of cardiovascular disease (coronary artery disease and congestive heart failure) was higher among the vaccinated group compared to the non-vaccinated group [(33.3%, 12.6%), respectively]. This difference in proportion was significant with a P value < 0.05. However, such significance was not noted among other ailments such as chronic renal disease, chronic lung disease, or even immunosuppression status (Table 1).
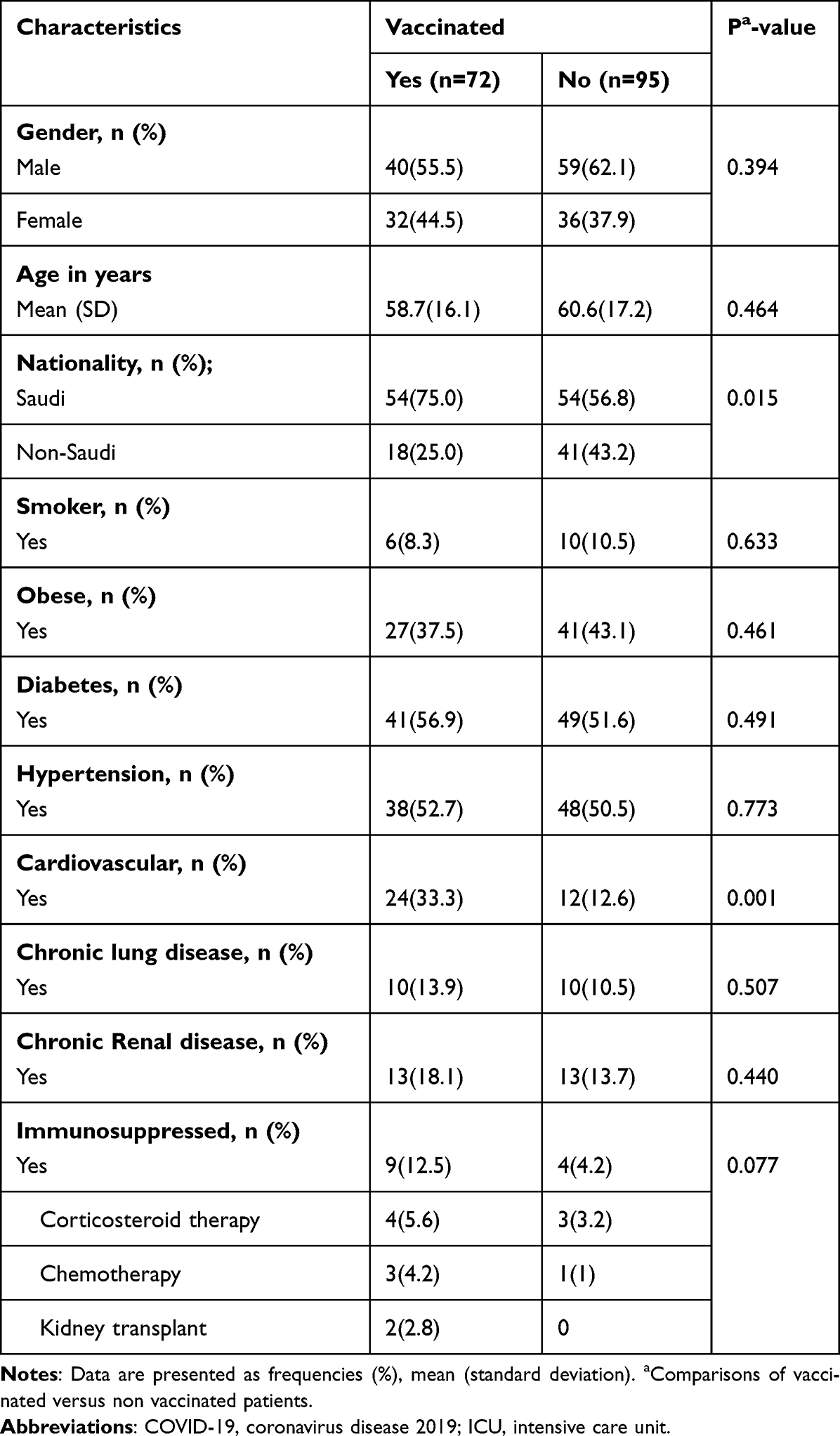 |
Table 1 Demographic and Clinical Characteristics of 167 COVID-19 Patients Admitted to ICU |
The outcomes of the patients are represented in Table 2. The outcomes for both groups were assessed by the need for HFNC, non-invasive mechanical ventilation (BIPAP, CPAP, Helmet ventilation), invasive Mechanical Ventilation, partial pressure of oxygen to fractional inspired oxygen (P/F) ratio, duration of intubation, ICU LOS, need for renal replacement therapy (RRT), and total deaths. Out of the 72 patients who were vaccinated, three-fourths (72.2%) required HFNC, 29 patients (40.2%) required BIPAP, 17 patients (23.6%) required CPAP, and around 10% received helmet ventilation. However, in the non-vaccinated group, 66 patients (69.5%) required HFNC, 39 patients (41%) required BIPAP, 38 patients (40%) required CPAP, and around 10% received helmet ventilation (P value< 0.05). The number of patients who required endotracheal intubation and mechanical ventilation was numerically higher in the non-vaccinated group compared to the vaccinated group [(n=58), (n=37), respectively], yet it did not reach statistical significance. Both these results show that there was a higher need for respiratory support in the non-vaccinated group when compared to the vaccinated group. Furthermore, the patients who were not vaccinated needed more invasive or non-invasive mechanical ventilation. A significantly longer duration of invasive mechanical ventilation was observed in non-vaccinated patients. The median duration of intubation for non-vaccinated patients was 8 days (Range 0–38) compared to 2 days (Range 0–33) in vaccinated patients (P value 0.027).
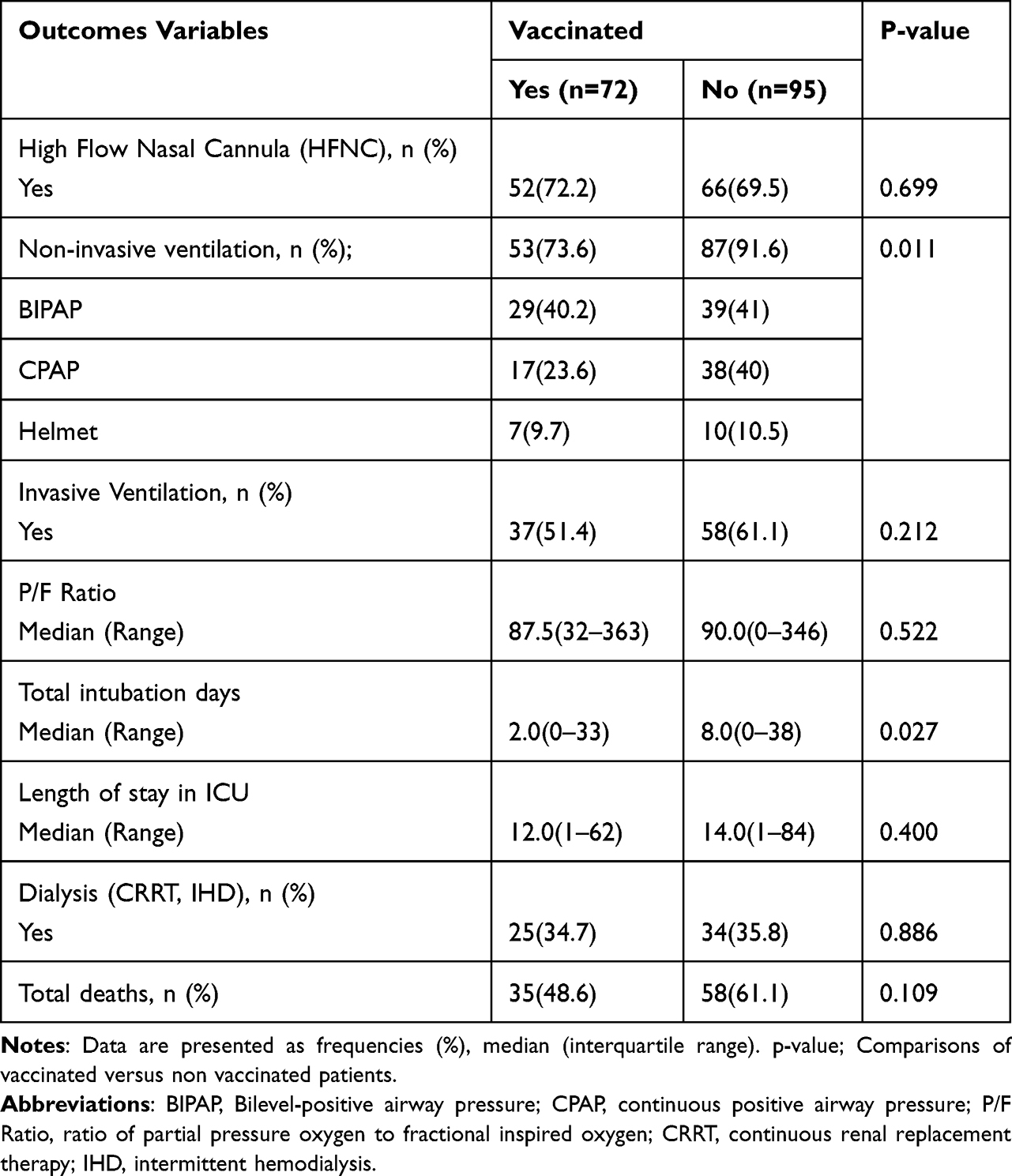 |
Table 2 Comparison of the Outcomes Between Vaccinated and Non-Vaccinated Patients |
The non-vaccinated patients suffering severe COVID-19 infection requiring ICU admission had a longer ICU LOS with a median of 14 days (Range 1–84) compared to 12 days (Range 1–62) in those who received at least one dose of vaccination. However, this result did not show any statistical significance. The total number of deaths was similar between both groups.
A comparison of laboratory parameters between both groups is shown in Table 3. Taking into consideration the risk for progression to severe SARS-CoV-2 infection, the laboratory parameters were assessed using CRP, ferritin, D-dimer, and LDH. Non-vaccinated patients with COVID-19 infection had significantly higher ferritin, D-dimer, and LDH compared to vaccinated patients. Moreover, in non-vaccinated patients, the ferritin levels were significantly higher with a median of 939 (range 56–5172) while they were 377.7 (range 47–3956) in vaccinated patients with at least a single dose of the vaccine (P value < 0.001). A similar significant effect was seen in the median D- Dimer and LDH values, reporting an average of 0.94 and 469.5, respectively in the vaccinated group compared to 1.16 and 531, respectively in the non-vaccinated group (P value < 0.05). CRP levels was similar between both groups.
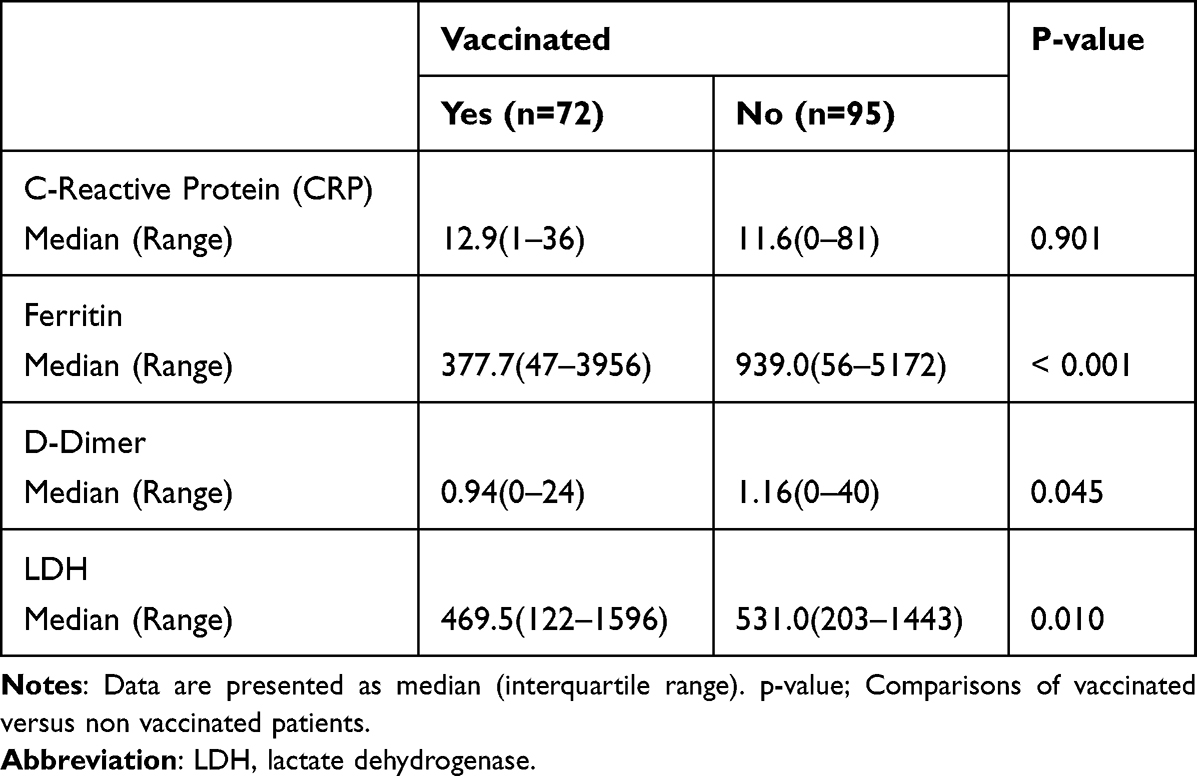 |
Table 3 Laboratory Parameters for the Risk of Severe COVID-19 Infection |
To further delve into the effects of vaccination, a subgroup analysis was done considering the number of vaccine doses taken. We then compared the measurable outcomes and laboratory findings between partially and fully immunized patients (Table 4). We found that 58% of the patients received a single dose of the vaccine, while 40% received two or more doses of the vaccine. Of those patients who received a single dose of the vaccine, 78.6% required non-invasive ventilation compared to 69% of patients who received two or more doses of the vaccine (P value 0.026). Additionally, the P/F ratio was significantly higher in patients who received two or more doses of the vaccine with a median of 100 (IQR 44–363) compared to a median of 75 (IQR 32–270) in those who received a single dose (P value 0.002). The number of patients who required HFNC was numerically lower in fully vaccinated patients in comparison to partially vaccinated patients [(69%, 73.8%), respectively]. However, this finding did not reach a statistical significance. Further statistical analysis showed that the rates of invasive mechanical ventilation, intubation days and length of ICU stay were similar between both groups. Considering the laboratory findings for the risk of severe COVID-19 infection, the levels of CRP were significantly lower in fully immunized patients with a median of 9 (range 1–36), in contrast to 14.8 (range 2–32) in partially immunized patients. The other laboratory parameters were statistically not significant between both groups.
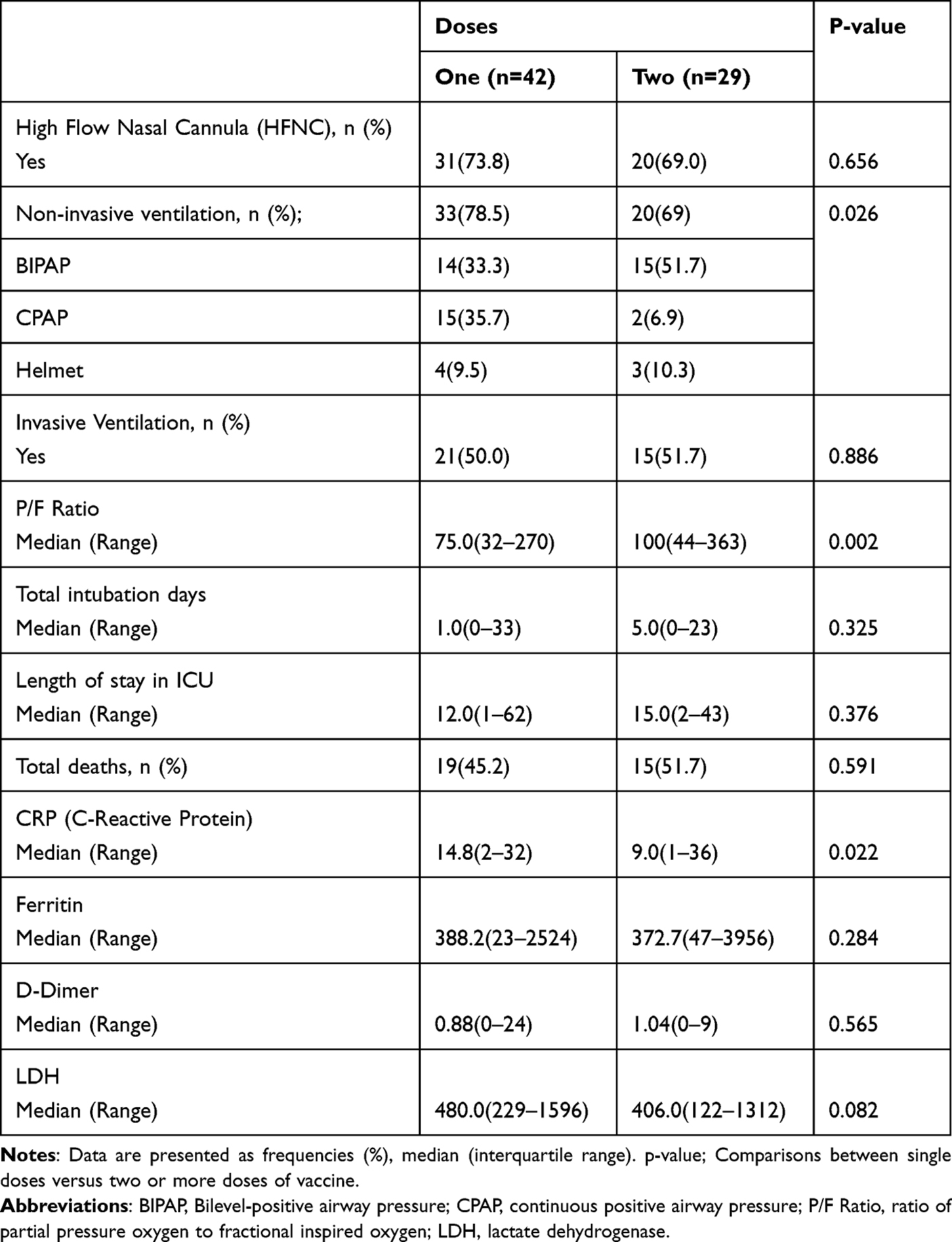 |
Table 4 Subgroup Analysis Comparison of the Outcome Between Single Dose VS Two Doses of Vaccination |
Our study failed to demonstrate any significant difference in mortality between vaccinated and non-vaccinated patients. However, the number of deaths were numerically lower in fully immunized patients compared to partially vaccinated patients [15(51.7%), 19(45.2%), respectively] with a P value of 0.591.
Discussion
We included 167 patients with confirmed COVID-19 infection leading to ICU admission with different demographic and comorbidity profiles during the study period. Ninety-five patients (56.9%) were not vaccinated, and seventy-two (43.1%) were vaccinated. Of those vaccinated groups, only 29 patients (40.2%) received two or more vaccine doses.
The demographic and clinical profile of the vaccinated patients are typical of other COVID-19 infections leading to ICU admission. These include, being elderly, male, and having multiple significant comorbidities. These characteristics were linked to the severity of COVID-19 infection. In our study, we observed high rates of vaccine breakthrough infections among patients with a history of cardiovascular disease (congestive heart failure and coronary artery disease) compared to the non-vaccinated group [33.3% vs 12.6%,]. Our results are congruent with a recent study conducted in Israel by T. Brosh-Nissimov et al, which reported a higher rate of vaccine breakthrough infections among patients with a history of cardiovascular disease compared with a large case series on non-vaccinated patients [(32% versus 5.8–12.8%), respectively].12,18,19 In our study, the number of immunosuppressed patients was numerically higher in the vaccinated cohort, with 12.5% of patients suffering from any type, including active chemotherapy, long-term corticosteroid therapy, and kidney transplant. These results may be attributed to the lower seroconversion rates after receiving the COVID-19 vaccine in immunosuppressed patients, as demonstrated in the previous literature.20–22 However, testing the vaccine’s efficacy is beyond the scope of this study.
In the current study, we observed that the number of patients who required non-invasive ventilation was significantly lower in the vaccinated cohort compared to the non-vaccinated cohort (73.6% vs 91.6%, P value < 0.05). However, the requirement for HFNC was similar between both groups. Our results are consistent with a recent study by Thompson et al which demonstrated that receiving two doses of mRNA-based COVID-19 vaccine provides up to 90% protection from acquiring severe COVID-19 infection leading to ICU stay secondary to increased oxygen requirements (95% CI, 86 to 93).23 On the contrary to the recent literature, our study did not demonstrate any significant difference in the rates of intubation and mechanical ventilation between both groups. However, the number of patients who required intubation and mechanical ventilation was numerically lower in the vaccinated group (51.4%) compared to the non-vaccinated group (61.1%). A recent study by Tenforde MW et al reported that receiving full doses of the COVID-19 vaccine protects against invasive mechanical ventilation reaching up to 90% (95% CI, 88–91%), including 88% (95% CI, 86–90%) after receiving two doses and 94% (95% CI, 91–96%) after receiving three doses.24
Our study showed that vaccinated patients suffering from severe COVID-19 infection who required invasive mechanical ventilation had a significantly lower duration of intubation and mechanical ventilation compared to non-vaccinated patients; the median duration for vaccinated patients was 2 days (Range 0–33) in contrast to 8 days (Range 0–38) for non-vaccinated patients (P value < 0.05). Moreover, the length of ICU stay was shorter in the vaccinated cohort which was not statistically significant. In line with previous studies, our study shows that non-vaccinated patients had greater morbidity in their illness compared to those who received at least one dose of the vaccine.
Based on the number of vaccines received, we performed a subgroup analysis comparing the outcome of concern between patients who received a single dose and two doses of the vaccine. We observed that, the patients who completed the doses of vaccination tended to have less hypoxia (higher P/F ratio) and lower rates of non-invasive ventilation use. Additionally, the number of patients who required endotracheal intubation was numerically lower. These findings are congruent with previous reports which demonstrated the protective effect of vaccination in preventing poor outcomes among patients who had vaccine breakthrough infections.24
The relationship between inflammatory markers and COVID-19 infections was extensively reviewed in literature. An elevated level of inflammatory markers, namely CRP, ferritin, lactate dehydrogenase, and D-dimer in COVID-19 infections, were found to be associated with disease severity and poor outcome.25,26 Moreover, COVID-19 patients having high CRP and LDH on admission tend to have more hypoxia and respiratory failure compared to other patients.27 However, the data on the impact of vaccination on inflammatory markers are scarce. Our study found a significant reduction in inflammatory markers in the vaccinated cohort compared to the non-vaccinated cohort. However, the CRP levels were similar between both cohorts. To further delve into the effects of vaccination on inflammatory markers, we undertook a subgroup analysis comparing between a single dose and two doses of the vaccine. It demonstrated a significant reduction in CRP level in patients who received two doses of COVID-19 vaccine. In line with literature, our study has demonstrated the vaccine’s effectiveness in reducing disease severity and preventing poor outcomes in patients suffering from COVID-19 disease.
Considering the transmissibility of COVID-19 infection, the reports in the epidemiological data are fluctuating, especially regarding the mortality rate. In Saudi Arabia, the incidence of COVID-19 infection and the mortality rates have been significantly reduced compared to the beginning of the pandemic, reflecting the implementation of successful preventive measures including, vaccination campaigns, social distancing, and mask-wearing in public areas.
Reviewing our study analysis, the reported deaths in the ICU were 93 (55.7%) COVID-19 positive patients, of whom 58 (61.1%) were unvaccinated. In comparison, 35 patients (48.6%) were vaccinated with one or two doses. This result was not statistically significant, primarily because the small sample size precluded the results. However, vaccinated patients had numerically lower death rates than non-vaccinated patients. A recent study by Bernal et al showed that vaccinated patients with either the Pfizer-BioNTech BNT162b2 or OxfordAstra-Zeneca ChAdOx1-S vaccine had a 51% lower risk of death compared to the non-vaccinated population.28 Recently, an analysis of data on severe COVID-19 outcomes in the United States found that receiving two or three doses of an mRNA-based vaccine will provide 90% protection from in-hospital death in adults. Most patients who died in the hospital were immunocompromised or had multiple significant comorbidities.24
The strength of our study is that it was conducted on ICU patients who experienced severe breakthrough infections, which will genuinely reflect the vaccine’s benefit in reducing significant morbidity and mortality. The vaccination record is universal nationwide through a vaccination program supervised by the ministry of health.
The main limitation of our study was that it was conducted in a single center with a small sample size which could affect the generalizability and preclude the results of valuable outcomes such as intubation rates and mortality. In addition, due to the study’s retrospective design, it is difficult to confirm the association between different factors and the risk of developing a breakthrough infection. Therefore, future prospective studies are crucial for better understanding the risk factors associated with breakthrough infection among COVID-19 patients admitted to the ICU.
Conclusion
Vaccination remains to be a valuable strategy for protecting vulnerable populations. A minority of vaccinated patients still might develop severe SARS-CoV-2 disease requiring ICU admission. This group of patients is characterized by older age and having multiple co-morbidities predisposing them to severe COVID-19 disease. Furthermore, patients with a history of cardiovascular disease have a higher risk of developing vaccine breakthrough infection, among other co-morbidities. Vaccinated patients had significantly lower rates of using non-invasive ventilation, duration of mechanical ventilation, and reduction in inflammatory markers compared to non-vaccinated patients. Moreover, patients who received two doses of the COVID-19 vaccine had less hypoxia (higher P/F ratio) compared to patients who received a single dose of the vaccine. Ultimately, we encourage COVID-19 vaccination, particularly for all high-risk populations through public education and the contribution of all healthcare systems nationwide and worldwide. Moreover, we advise continuing with a public health mitigation approach including vaccine booster dose, social distancing and mask-wearing for all high-risk populations.
Data Sharing Statement
Raw data can be submitted on a justifiable request. Please Contact the corresponding author for any data requests or inquiries.
Ethics Statement
Approval of the Institutional Review Board for this study was obtained (IRB-2022-01-173).
Consent for Publication
Consent from participants was obtained as per the ethics code of the World Medical Association (Declaration of Helsinki).
Acknowledgments
We would like to show our sincere gratitude to Prof. Mohammad AlShahrani for his support and for reviewing the manuscript. We would like to thank our great nursing staff in the department for their hard work and sacrifice during the pandemic. We extend our thanks to all healthcare providers who sacrificed during the COVID-19 pandemic.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of in this work.
References
1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
2. Coronavirus disease (COVID-19) pandemic; 2021. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
3. Coronavirus disease 2019 (COVID-19): situation summary; 2021. Available from: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/summary.html.
4. World Health Organization. Weekly epidemiological update—15 May 2022; 2022.
5. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383:2603–2615. doi:10.1056/NEJMoa2034577
6. Sadoff J, Le Gars M, Shukarev G, et al. Interim results of a Phase 1–2a Trial of Ad26.COV2. S Covid-19 vaccine. N Engl J Med. 2021;384(19):1824–1835. doi:10.1056/NEJMoa2034201
7. Dagan N, Barda N, Kepten E, et al. BNT162b2 mRNA Covid-19 vaccine in a nationwide mass vaccination setting. N Engl J Med. 2021;384:1412e23. doi:10.1056/NEJMoa2101765
8. Tenforde MW, Olson SM, Self WH, et al. Effectiveness of Pfizer-BioNTech and moderna vaccines against COVID-19 among hospitalized adults aged 65 years in United States, January - March 2021. MMWR Morb Mortal Wkly Rep. 2021;70(18):674–679. doi:10.15585/mmwr.mm7018e1
9. Vasileiou E, Simpson CR, Shi T, et al. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: a national prospective cohort study. Lancet. 2021;397:1646e57. doi:10.1016/S0140-6736(21)00677-2
10. Bernal JL, Andrews N, Gower C, et al. Early effectiveness of COVID-19 vaccination with BNT162b2 mRNA vaccine and ChAdOx1 adenovirus vector vaccine on symptomatic disease, hospitalizations, and mortality in older adults in England. MedRxiv. 2021. doi:10.1101/2021.03.01.21252652
11. Ministry of Health. COVID-19 dashboard 2021. Available from: https://covid19.moh.gov.sa.
12. Brosh-Nissimov T, Orenbuch-Harroch E, Chowers M, et al. BNT162b2 vaccine breakthrough: clinical characteristics of 152 fully vaccinated hospitalized COVID-19 patients in Israel. Clin Microbiol Infect. 2021;27(11):1652–1657. doi:10.1016/j.cmi.2021.06.036
13. Public Health Authority. Laboratory diagnosis. Available from: https://covid19.cdc.gov.sa/professionals-health-workers/laboratorydiagnosis/.
14. Saudi Center for Disease Prevention and Control (Weqaya). Laboratory diagnosis of COVID-19 in suspected cases. Available from: https://covid19.cdc.gov.sa/professionals-health-workers/laboratory-diagnosis/.
15. Walsh EE, Frenck RW, Falsey AR, et al. Safety and Immunogenicity of Two RNA-Based Covid-19 vaccine candidates. N Engl J Med. 2020;383(25):2439–2450. doi:10.1056/NEJMoa2027906
16. Barrett JR, Belij-Rammerstorfer S, Dold C, et al. Phase 1/2 trial of SARS-CoV-2 vaccine ChAdOx1 nCoV-19 with a booster dose induces multifunctional antibody responses. Nat Med. 2021;27(2):279–288. doi:10.1038/s41591-020-01179-4
17. Anderson EJ, Rouphael NG, Widge AT, et al. Safety and immunogenicity of SARS-CoV-2 mRNA-1273 vaccine in older adults. N Engl J Med. 2020;383(25):2427–2438. doi:10.1056/NEJMoa2028436
18. Myers LC, Parodi SM, Escobar GJ, Liu VX. Characteristics of hospitalized adults with COVID-19 in an integrated health care system in California. JAMA. 2020;323(21):2195–2198. doi:10.1001/jama.2020.7202
19. Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369:m1966. doi:10.1136/bmj.m1966
20. Choi B, Choudhary MC, Regan J, et al. Persistence and evolution of SARS-CoV-2 in an immunocompromised host. N Engl J Med. 2020;383(23):2291–2293. doi:10.1056/NEJMc2031364
21. Akalin E, Azzi Y, Bartash R, et al. Covid-19 and Kidney Transplantation. N Engl J Med. 2020;382(25):2475–2477. doi:10.1056/NEJMc2011117
22. Reischig T, Kacer M, Vlas T, et al. Insufficient response to mRNA SARS-CoV-2 vaccine and high incidence of severe COVID-19 in kidney transplant recipients during pandemic. Am J Transplant. 2022;22(3):801–812. doi:10.1111/ajt.16902
23. Thompson MG, Stenehjem E, Grannis S, et al. Effectiveness of Covid-19 vaccines in ambulatory and inpatient care settings. N Engl J Med. 2021;385(15):1355–1371. doi:10.1056/NEJMoa2110362
24. Tenforde MW, Self WH, Gaglani M, et al. Effectiveness of mRNA vaccination in preventing COVID-19-associated invasive mechanical ventilation and death - United States, March 2021-January 2022. MMWR Morb Mortal Wkly Rep. 2022;71(12):459–465. doi:10.15585/mmwr.mm7112e1
25. Huang I, Pranata R, Lim MA, Oehadian A, Alisjahbana B. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: a meta-analysis. Ther Adv Respir Dis. 2020;14:1753466620937175. doi:10.1177/1753466620937175
26. Pan F, Yang L, Li Y, et al. Factors associated with death outcome in patients with severe coronavirus disease-19 (COVID-19): a case-control study. Int J Med Sci. 2020;17(9):1281–1292. doi:10.7150/ijms.46614
27. Poggiali E, Zaino D, Immovilli P, et al. Lactate dehydrogenase and C-reactive protein as predictors of respiratory failure in CoVID-19 patients. Clin Chim Acta. 2020;509:135–138. doi:10.1016/j.cca.2020.06.012
28. Lopez Bernal J, Andrews N, Gower C, et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: test negative case-control study. BMJ. 2021;373:n1088. doi:10.1136/bmj.n1088
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.