Back to Journals » Journal of Pain Research » Volume 19
Cost-Effectiveness of Differential Target Multiplexed Spinal Cord Stimulation for the Treatment of PSPS Type 1 from the Belgian Perspective
Authors Smet I, Billet B ![]() , van Paesschen R
, van Paesschen R ![]() , McCloskey S, Imschoot C, Mallender P, Eggington S, Kallewaard JW
, McCloskey S, Imschoot C, Mallender P, Eggington S, Kallewaard JW ![]()
Received 15 January 2026
Accepted for publication 30 April 2026
Published 27 May 2026 Volume 2026:19 596123
DOI https://doi.org/10.2147/JPR.S596123
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Iris Smet,1 Bart Billet,2,3 Raf van Paesschen,4 Sara McCloskey,5,6 Charlotte Imschoot,7 Philip Mallender,5 Simon Eggington,8 Jan Willem Kallewaard9,10
1Multidisciplinary Pain Clinic, VITAZ Hospitals, Sint-Niklaas, Belgium; 2Department of Anesthesiology, AZ Delta, Roeselare, Belgium; 3Stimulus Research Group, Vrije Universiteit Brussel, Jette, Belgium; 4Department of Neurosurgery, ZAS Hospitals, Antwerp, Belgium; 5Health Economics, Policy & Reimbursement, Medtronic, Watford, UK; 6Present Address: Department of Primary Care, Population Science and Medical Education, University of Southampton, Hampshire, UK; 7Health Economics, Policy & Reimbursement, Medtronic, Brussels, Belgium; 8Health Economics, Medtronic International Trading Sarl, Tolochenaz, Switzerland; 9Department of Anesthesiology and Pain Management, Rijnstate Ziekenhuis, Arnhem, the Netherlands; 10Department of Anesthesiology and Pain Management, Amsterdam University Medical Center (VUmc), Amsterdam, the Netherlands
Correspondence: Jan Willem Kallewaard, Department of Anesthesiology and Pain Management, Rijnstate Ziekenhuis, Arnhem, the Netherlands, Tel +31 6 2241 2029, Email [email protected]
Purpose: Spinal cord stimulation (SCS) using the Differential Target Multiplexed (DTM) waveform is an effective treatment for treating chronic neuropathic back and leg pain that is refractory to other interventions. The purpose of this research was to estimate the cost-effectiveness of this therapy in a population with Persistent Spinal Pain Syndrome Type 1 (PSPS T1) by updating an existing model with inputs from Belgian healthcare databases and Western European clinical data.
Patients and Methods: A two-phase model was built using a 24-month decision tree followed by a 13-year Markov model. Model inputs were sourced from a recent European randomized controlled trial evaluating DTM-SCS for the treatment of PSPS T1, other published literature, and publicly available Belgian healthcare data. Costs and quality-adjusted life years (QALYs) were calculated using deterministic analysis. One-way sensitivity analyses were conducted to test the effect of individual model input parameters on results. Overall model uncertainty was tested using probabilistic sensitivity analysis.
Results: The model estimated that DTM-SCS would be cost-effective versus conventional medical management (CMM) in 99.7% of 10,000 simulations, at an assumed willingness-to-pay threshold of € 30,000. DTM-SCS patients gained 1.29 QALYs compared to CMM patients, resulting in an incremental cost-effectiveness ratio (ICER) of € 11,518 and an incremental net benefit (INB) that became positive at year 5. The base-case results remained robust in scenario analyses, which found that medication use, utilities associated with suboptimal and optimal pain relief, and the time horizon were the largest drivers of uncertainty in the model.
Conclusion: The results of the model suggest that DTM-SCS is likely to be a cost-effective treatment option for PSPS T1 compared to CMM for patients in the Belgian healthcare system.
Plain Language Summary: Spinal cord stimulation (SCS) has been used for decades to help people manage chronic low-back pain when other conventional medical management (CMM) treatments do not provide adequate pain relief. In the last five years several clinical studies have evaluated the clinical outcomes of SCS among patients with Persistent Spinal Pain Syndrome (PSPS Type 1), also known as non-surgical refractory back pain (NSRBP) or patients without history of prior major back surgery. In this study, the researchers evaluated whether or not treatment with a novel form of SCS, called Differential Target Multiplexed SCS (DTM-SCS), is cost-effective compared to treatment with CMM alone, in a population of patients with pain classified as PSPS Type 1.
Using cost information from the Belgian healthcare system and data about clinical outcomes from a randomized, controlled clinical trial, this study developed an economic model to estimate how much Belgian healthcare payers could expect to pay for the typical patient over 15 years of DTM-SCS treatment vs CMM alone. The results of the model showed that, on average, treatment with DTM-SCS gave patients with PSPS Type 1 more years of better health (called quality-adjusted life years, or QALYs) compared to CMM, even though DTM-SCS treatment costs more upfront. The extra cost was considered reasonable for the QALY benefit by European “willingness-to-pay” standards, and therefore the researchers concluded that DTM-SCS was more likely than not to be a cost-effective treatment for PSPS Type 1 in Belgium.
Keywords: Cost-effectiveness, differential target multiplexed, low-back pain, spinal cord stimulation, Belgium
Introduction
Spinal cord stimulation (SCS) is a treatment option that has been used for more than 40 years to treat chronic neuropathic back and leg pain that is refractory to other interventions. SCS delivers mild electrical impulses to the spinal nerves to block the sensation of pain. The procedure involves implantation of a battery-powered pulse generator beneath the skin, which is connected to leads placed in the epidural space. It has been shown to improve outcomes related to pain control, health-related quality of life (HRQoL), functional capacity, and use of pain medication and healthcare resources compared with conventional medical management (CMM) for a range of diagnoses and geographies.1,2 For example, a 2025 systematic review and meta-analysis identified 19 reports of 16 unique studies evaluating the effect of SCS in non-surgical low back pain.2 The meta-analysis found significant reductions in pain with SCS compared with conventional medical management (CMM) at six-month follow-up (mean difference 5.67; 95% CI 4.60 to 6.74). Statistically significant results in favor of SCS compared with CMM were observed for physical function and HRQoL, and meta-analysis of the non-RCT data showed significant improvements in pain intensity, physical function, and HRQoL up to 24 months compared with baseline.
SCS has also been shown to be cost-effective over the long term compared to CMM.3–6 Recent technical advancements such as the stimulation waveform Differential Target Multiplexed (DTM)-SCS,7 have further improved its efficacy and cost-effectiveness versus CMM.3,7–9
The cost-effectiveness of DTM-SCS was previously evaluated using data from the United Kingdom (UK), across a broad cohort of patients with various pain indications,3 but has not yet been evaluated in the subset of patients with no history of back surgery, also known as Persistent Spinal Pain Syndrome Type 1 (PSPS T1) or non-surgical refractory back pain (NSRBP). It has also not been analyzed using economic data from countries in Western Europe. The purpose of this study was to adapt an established model for estimating cost-effectiveness to evaluate the potential cost-effectiveness of DTM-SCS in Belgium. Clinical inputs for this updated model were 24-month safety and efficacy data from a recent randomized controlled clinical trial (RCT) of DTM-SCS plus CMM compared with CMM alone in patients with PSPS T1, which enrolled 112 patients from Belgium and three other European countries.9
Materials and Methods
Model Overview and Ethics
The cost-effectiveness model used for this study is an adaptation of previous work investigating the cost-effectiveness of conventional SCS versus CMM from the perspective of the UK National Health Service,6 and a 2024 update to the UK model that evaluated the newer DTM-SCS waveform versus conventional SCS and CMM.3 The present model used DTM-SCS clinical data from a recent European RCT conducted by Kallewaard and colleagues,9 with cost data sourced from Belgian healthcare databases. Ethics approval and informed consent were not applicable to this study, as all model inputs were derived from expert clinical opinion, published literature or public, de-identified data sources.
Treatment Interventions
Two treatment options for patients with PSPS T1 were compared: CMM alone, which typically consists of pharmacological treatment, rehabilitation program, psychological treatment, and interventional treatments, like radiofrequency procedures, spinal injections, and DTM-SCS with CMM. All patients who were randomized into the DTM-SCS arm of the RCT were implanted with the Medtronic Intellis™ 97715 rechargeable SCS system (Medtronic, PLC, Ireland), and their data were used for clinical inputs to the model.
Model Structure
This model had a 15-year time horizon across two phases. First, a 24-month decision tree was used to simulate the SCS trial-stimulation phase (Figure 1), during which patients either had a successful trial and received a permanent DTM-SCS implant, or had a failed trial and transitioned to CMM. When the decision-tree period was completed, patients existed in one of five health states: optimal pain relief without complications; optimal pain relief with complications; suboptimal pain relief without complications; suboptimal pain relief with complications; or deceased.
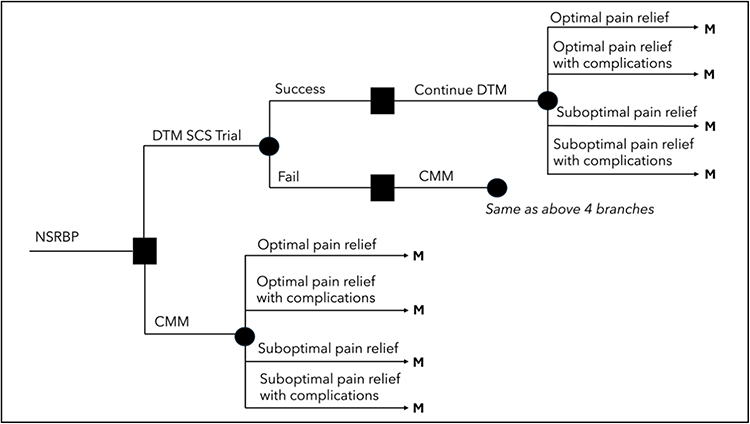 |
Figure 1 Decision tree structure, 24-month horizon. Abbreviations: DTM, differential target multiplexed; M, Markov model begins. |
Patients then entered a 13-year Markov model (Figure 2), during which they could move between health states in 3-month cycles. In the base-case scenario, optimal pain relief was defined as ≥ 50% improvement in the visual analog scale (VAS) for back pain, and suboptimal pain relief was defined as any lesser amount of pain relief. Death could occur from any health state, according to the Belgian age- and gender-matched life expectancy tables,10 and was treated as unrelated to pain status. DTM-SCS patients could withdraw from therapy at any time, after which they were assumed to continue CMM treatment only, through the end of the model. All costs and quality-adjusted life years (QALYs) accrued during the Markov model phase were discounted at 3% and 1.5%, respectively. As Belgium does not have an explicit willingness-to-pay threshold, a threshold of €30,000 per QALY was assumed for the analysis, in line with thresholds often cited in other European countries.
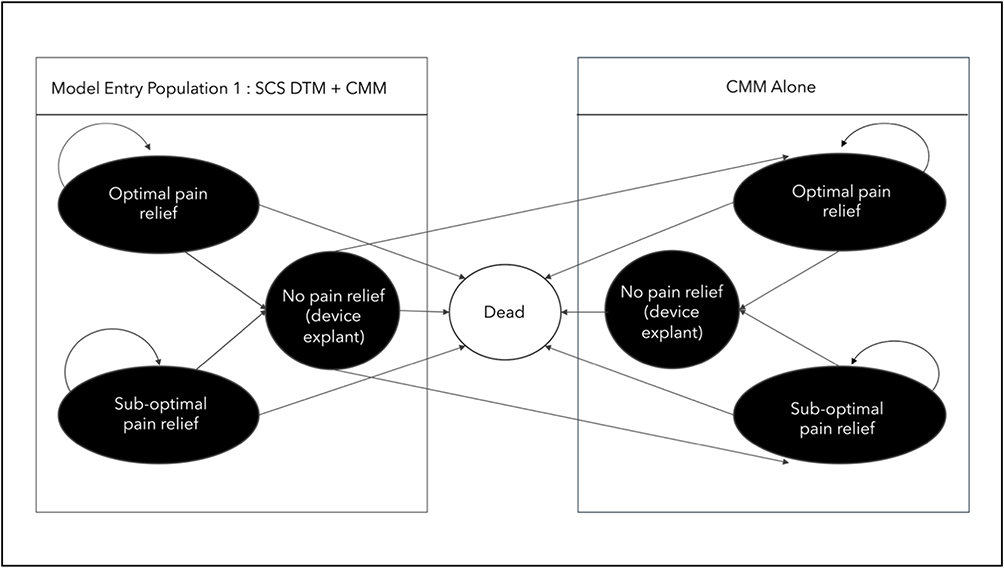 |
Figure 2 Markov model structure, month 25 through year 15, cycle length 3 month. Abbreviation: DTM, differential target multiplexed. |
Model Inputs
A full description of all model inputs is available in the Supplementary Online Material 1. Briefly, the primary source of clinical data inputs for the model was a published clinical trial of DTM-SCS versus CMM only, conducted by Kallewaard et al.9 This European multicenter RCT, which evaluated 112 patients from Belgium, Germany, the Netherlands, and Spain, gathered data efficacy (Table S1), adverse events (Table S2), health-related quality of life as measured by EQ-5D-5L (Table S4), medication use, and healthcare resource use (HCRU) (Table S5). These data were supplemented by internal Medtronic data on rate of long-term adverse events (Table S3),11 along with published literature on the rate of therapy explants,12 HCRU,6 and medication use.6
Unit costs were calculated from Belgian data (Table S6), using the National Institute for Sickness and Disability Insurance (RIZIV) nomenclature,13 medication tariffs,14 and device costs.15 In accordance with Belgian Health Care Knowledge Centre guidelines, the least-expensive generic option for a given medication was always used.16 Given that SCS was not reimbursed in Belgium for the PSPS T1 indication at the time of model development, the model assumed that device costs would be the same as for PSPS T2 (ie, “failed back surgery syndrome”). The mean local cost of adverse events occurring in the Kallewaard RCT was assigned during the decision-tree phase, using RIZIV nomenclature and internal Medtronic data to calculate the mean cost of long-term adverse events.11,13
Utility values for each health state were calculated by applying Belgian preference weights to the EQ-5D-5L data gathered during the Kallewaard RCT. The mean pooled utility value for each health state was calculated using patient-level trial data (Table S4).
Data Analysis
The model was built and executed in Microsoft Excel with Visual Basic. The deterministic (base-case) analysis fixed all continuous model inputs to their mean values and calculated an incremental cost-effectiveness ratio (ICER) for treatment with DTM-SCS versus CMM. Direct healthcare costs were discounted at 3% and outcomes measured in QALYs were discounted at 1.5%.
One-way sensitivity analyses were conducted to test individual model input parameters for uncertainty, and probabilistic sensitivity analyses were used to test for overall model uncertainty (see Supplementary Analytical Methods 1). Three specific scenario analyses included 1) adjusting the trial population evaluated to the actual proportion of patients who received a permanent SCS implant during the Kallewaard RCT (92.2%) instead of the proportion who had a successful trial stimulation (94.1%); 2) changing the threshold of optimal pain relief to ≥ 80% improvement in back pain VAS; and 3) excluding medication use for a single CMM patient who could be considered an outlier due to high medication costs associated with ketamine treatment.
Results
Deterministic Results
In the base-case scenario, DTM-SCS treatment resulted in 1.29 more QALYs than CMM (7.84 versus 6.55). The incremental cost for DTM-SCS versus CMM was €14,804 (€48,210 vs €33,405). The corresponding ICER for the base case was calculated as €11,518 (Figure 3).
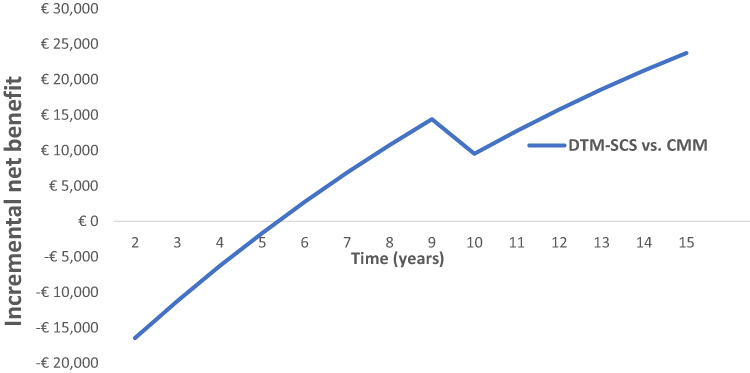 |
Figure 3 Incremental net benefit, DTM-SCS versus CMM, 15-year time horizon. Abbreviations: CMM, conservative medical management; DTM, differential target multiplexed; SCS, spinal-cord stimulation. Notes: Incremental net benefit based on nominal willingness-to-pay threshold of €30,000. |
One-Way Sensitivity Analyses
DTM-SCS remained cost-effective compared to CMM in all one-way sensitivity analyses. Because Belgium does not publish a willingness-to-pay threshold, an informal €30,000 per QALY, which is lower than the published GDP per capita of Belgium, was applied as a benchmark to assess cost-effectiveness (Figure 4A). In the base case, the main drivers of cost-effectiveness were the cost of medication in the CMM group, the time horizon, and the utility associated with suboptimal pain relief.
 |
Figure 4 One-way sensitivity analyses. The vertical line at the center represents the base-case ICER, expressed as the incremental net benefit. (A) base case. (B) scenario excluding the ketamine patient. |
Probabilistic Sensitivity Analysis
DTM-SCS was estimated to be cost-effective in 99.7% of the 10,000 simulations at an assumed willingness-to-pay threshold of €30,000 (Figure 5). Additionally, DTM-SCS always generated more QALYs than CMM (Figure 6A). Incremental costs varied widely, driven largely by the single CMM patient who received ketamine treatment.
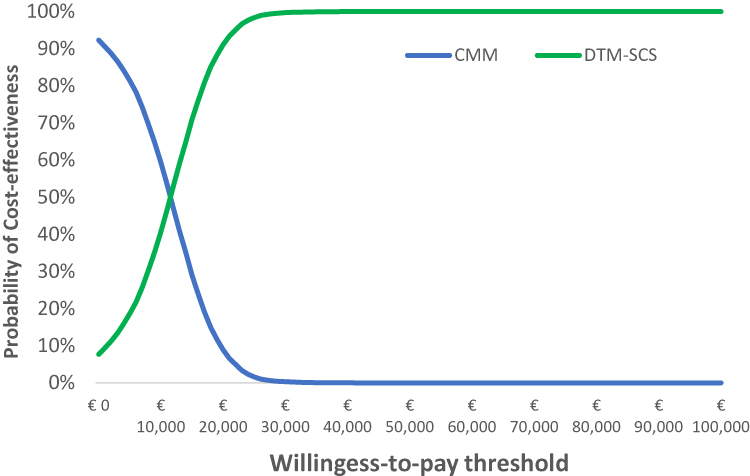 |
Figure 5 Cost-effectiveness acceptability curve, 15-year horizon. |
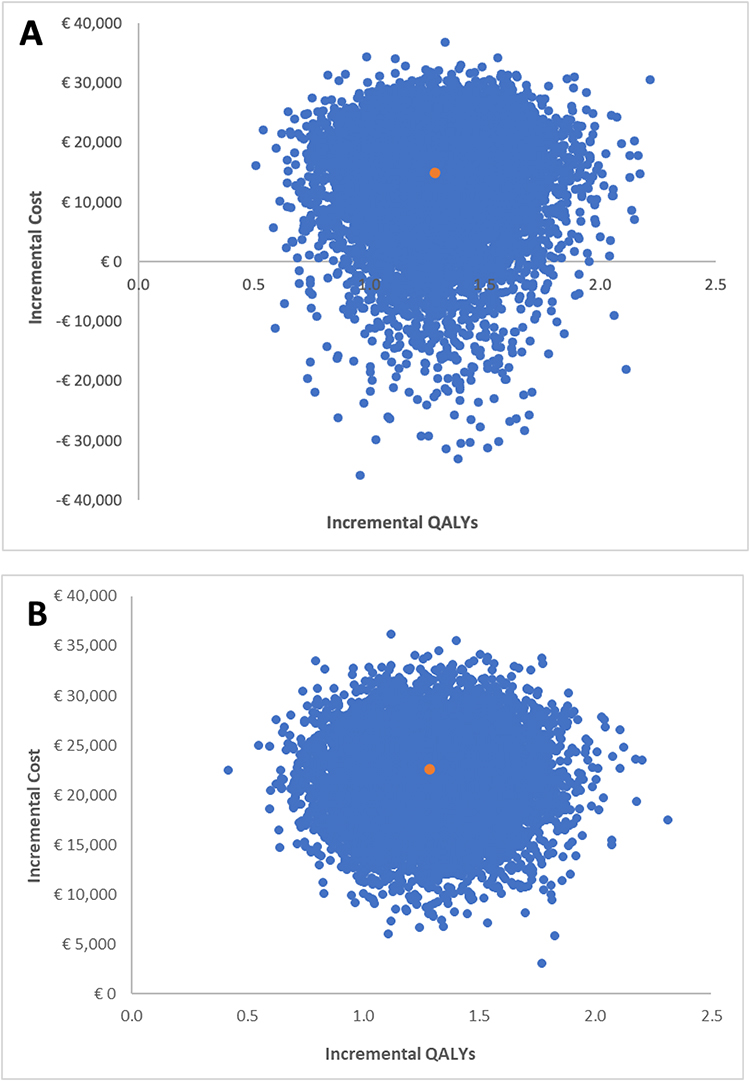 |
Figure 6 Cost-effectiveness scatter plot, DTM-SCS vs CMM. (A) base case. (B) scenario excluding the ketamine patient. |
Scenario Analyses
Three scenario analyses were conducted (Table 1). First, when the actual rate of implantation (92.2%) was used instead of the rate of successful trial stimulation (94.1%), the ICER increased by €89 (a relative change of 0.7% over the base-case ICER). When the threshold for optimal pain relief was increased to ≥ 80% (defined in the RCT as “profound” pain relief) versus the base case of ≥ 50%, the ICER increased by €10,590 (a 91.9% relative increase). Finally, exclusion of one outlier CMM patient with high medication costs resulted in an increase in the ICER of €6,026 (a 52.3% relative increase).
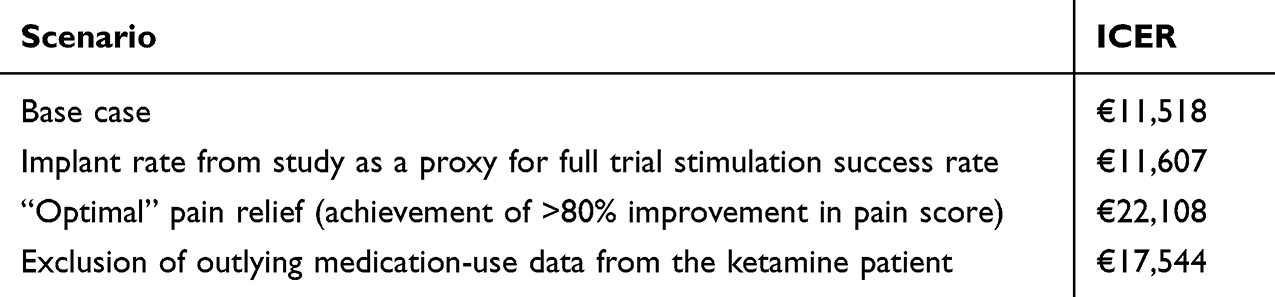 |
Table 1 ICERs from Scenario Analyses, DTM-SCS vs. CMM |
When including the CMM patient taking Ketamine, all parameter ranges, except the time horizon produce incremental net benefits (INB) greater than the baseline ICER (Figure 4A). Because of the impact on the ICER related to one outlier CMM patient from the RCT, the one-way and probabilistic sensitivity analyses were recalculated excluding the outlier patient. After this modification, the utilities associated with suboptimal and optimal pain relief, as well as the time horizon, became the biggest drivers of uncertainty in the one-way sensitivity analysis (Figure 4B). In probabilistic sensitivity analyses, the variation in incremental costs decreased significantly (Figure 6B). At the willingness-to-pay threshold of €30,000, DTM-SCS remained cost-effective 98.8% of the time and therefore, the initial findings remained robust to the uncertainty introduced by this patient.
Discussion
This study adapted previously published models, one evaluating the cost-effectiveness of SCS for treatment of PSPS T2,6 and the other investigating cost-effectiveness of DTM-SCS for treatment of chronic intractable low-back pain,3 to estimate the cost-effectiveness of SCS for PSPS T1 from the perspective of Belgian payers. After updating the model inputs to reflect contemporary data from a multicenter, European trial of DTM-SCS for treatment of PSPS T1 and local Belgian cost data, the present study determined that DTM-SCS was cost-effective at the assumed willingness-to-pay threshold of €30,000, with the incremental net benefit becoming positive in year 5.
The findings of our deterministic model are consistent with prior literature estimating the cost-effectiveness of DTM-SCS in UK patients with PSPS T2 and chronic pain,3,6 as well as the cost-effectiveness in the United States (US) of high-frequency SCS or passive recharge burst (PRB)-SCS for the treatment of PSPS T1.4,17 In one of the first models evaluating the cost-effectiveness of SCS in the UK, published in 2010 by Taylor and colleagues,6 the authors concluded that, conventional SCS was cost-effective for PSPS T2 in selected patients compared to CMM, with an ICER of £5,624 per QALY compared with CMM and £6,392 per QALY compared with reoperation. In another analysis of UK data, Gulve and colleagues in 2024 reported the results of an analysis comparing DTM-SCS, conventional SCS, and CMM for treatment of chronic intractable low-back pain using an updated version of the model first published by Taylor and colleagues.3,6 That study found that, in the UK, DTM-SCS was more cost-effective than conventional SCS; when both were compared to CMM (DTM-SCS ICER of £6,101 and conventional SCS ICER of £10,111 per QALY gained).
In the US, Patel and colleagues estimated the cost-effectiveness of high-frequency SCS versus CMM as part of an RCT of SCS for PSPS T1.4 They found that use of 10 kHz-SCS significantly improved patient quality of life and reduced healthcare utilization with consequent reduction in costs compared to CMM (dominant ICER of −$4,964 at 12 months). This differs from our finding of cost-effectiveness versus theirs of cost-dominance; however, our methods differed from the Patel study in that they did not use a Markov modeling approach and limited follow-up to one year.
A recent publication from Deer and colleagues reported outcomes from a prospective RCT (DISTINCT) and analyzed the US cost-effectiveness of PRB-SCS versus CMM in 270 patients with chronic low-back pain meeting the definition of PSPS T1.17 Authors concluded that, in the US, treatment with SCS was cost-effective in this trial population at 2.7 years. The results were also compared to an externally matched, real-world CMM control cohort, showing costs in the real-world CMM group were higher than in the trial-based CMM cohort. This result suggested that potential pre-crossover bias in the trial arm skewed to lesser healthcare resource use knowing there was the option for crossover to the treatment arm at six months. The cost-effectiveness results from this study are not directly comparable to ours, as the Deer et al modeling did not follow a Markov approach.17
Limitations
This study has several limitations. First, the model relied on extrapolation of 24-month health outcomes data collected via an RCT to estimate long-term (15-year) benefits in each group. Previous studies have shown that the effect of SCS may wane over time,18–20 and this has been captured in the model in the form of probability of therapy explant. In the future, long-term real-world follow-up data will be useful for testing the assumption that short-term benefits translate into long-term improvement in quality of life.
Concerning the cost analysis, the model relies on HCRU data and medication-use data collected during the Kallewaard RCT. However, those data have some limitations, such as high degree of variability in medication and HCRU and a 6-month limitation on data availability for CMM due to the crossover trial design. There was also no way to determine when HCRU was associated with treatment of an adverse event, potentially resulting in some double-counting. However, this would only affect the treatment arm of the model and adversely influence the ICER, thus rendering our base-case ICER a conservative estimate.
Typically, cost-effectiveness calculations require local reimbursement rates and willingness-to-pay thresholds as model inputs. These inputs were not available for the present study, as reimbursement for SCS in the treatment of PSPS T1 was not available in Belgium when the model was developed, and Belgium does not publish a formal willingness-to-pay threshold. Therefore, these two inputs had to be derived based on assumptions, introducing a degree of uncertainty into the model. Other potential sources of uncertainty include differences between Belgian payer rules and those of the UK or US, and cultural differences in patient selection and prescribing patterns for pain-relief therapies.
The RCT from which the present study derived its data inputs was conducted at multiple European centers, meaning that the study population was not limited to Belgian patients. Therefore, the HCRU and drug use data may vary somewhat from the Belgian standard-of-care. Nevertheless, the Kallewaard data currently represent the best-available evidence about DTM-SCS in Belgium. The sensitivity analyses, scenarios, and exclusion of outlying medication use were intended to address this limitation and showed that the results remained robust across a range of contexts.
Finally, when considering the generalizability of our results, it is important to appreciate that this analysis was based on data from a carefully selected group of patients with PSPS T1. Thus, implementation of these results in daily practice or guidelines should follow strict patient-selection criteria to determine eligibility for SCS therapy among patients with no history of back surgery.
Conclusion
The results of this model suggest that DTM-SCS is likely to be a cost-effective treatment option for PSPS T1 for Belgian payers, relative to CMM. The model results remained robust across a range of sensitivity and scenario analyses. These findings should be useful in the context of national funding decisions for indications covered for SCS therapy, with PSPS T1 representing a population that may benefit from treatment.
Abbreviations
CMM, conventional medical management; DTM, differential target multiplex; HCRU, healthcare resource use; HRQoL, healthcare related quality of life; ICER, incremental cost-effectiveness ratio; INB, incremental net benefit; PSPS T1, persistent spinal pain syndrome type 1; QALY, quality-adjusted life year; RCT, randomized controlled clinical trial; RIZIV, National Institute for Sickness and Disability Insurance (Belgium); SCS, spinal cord stimulation; UK, United Kingdom; US, United States of America; VAS, visual analog scale.
Data Sharing Statement
Most of the data used in this study are available from public sources as noted in the text. The model, as well as data internal to Medtronic, Plc., are not available due to confidentially agreements.
Ethics Approval and Informed Consent
Ethics approval and informed consent were not applicable to this study, as all model inputs were derived from published literature or public, de-identified data sources.
Acknowledgments
Jeanne McAdara PhD provided professional medical writing assistance, which was funded by Medtronic, Plc. The authors maintained full freedom of investigation and control over manuscript development.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Professional medical writing assistance was funded by Medtronic, Plc.
Disclosure
IS: Advisory board for Medtronic, Abbott and Nevro. Consultant for Medtronic, Nevro and Boston Scientific BB: Consultant for Saluda, Medtronic, Abbott and Salvia Bioelectronics. RvP: No conflicts to disclose. SM, CI, PM and SE, are or were full-time employees of Medtronic at the time of this research. SE reports stock in Medtronic. JWK: Advisory board for Saluda Medical, Medtronic, and Boston Scientific. The authors report no other conflicts of interest in this work.
References
1. Aryal V, Poudel S, Zulfiqar F, et al. Updates on the role of spinal cord stimulation in the management of non-surgical chronic lower back pain. Cureus. 2021;13(10):e18928. doi:10.7759/cureus.18928
2. Kallewaard JW, Nevitt S, Maden M, et al. Systematic review and meta-analysis of spinal cord stimulation for chronic nonsurgical refractory back pain with or without leg pain (Persistent Spinal Pain Syndrome Type 1). Neuromodulation. 2025;S1094-7159(25):01048.
3. Gulve A, Mehta V, Provenzano DA, et al. Differential target multiplexed spinal cord stimulation: a UK cost-effectiveness analysis. Neuromodulation. 2024;27(5):908–11. doi:10.1016/j.neurom.2024.02.009
4. Patel NP, Wu C, Lad SP, et al. Cost-effectiveness of 10-kHz spinal cord stimulation therapy compared with conventional medical management over the first 12 months of therapy for patients with nonsurgical back pain: randomized controlled trial. J Neurosurg Spine. 2023;38(2):249–257. doi:10.3171/2022.9.SPINE22416
5. Taylor RS, Bentley A, Campbell B, Murphy K. High-frequency 10 kHz spinal cord stimulation for chronic back and leg pain: cost-consequence and cost-effectiveness analyses. Clin J Pain. 2020;36(11):852–861. doi:10.1097/AJP.0000000000000866
6. Taylor RS, Ryan J, O’Donnell R, Eldabe S, Kumar K, North RB. The cost-effectiveness of spinal cord stimulation in the treatment of failed back surgery syndrome. Clin J Pain. 2010;26(6):463–469. doi:10.1097/AJP.0b013e3181daccec
7. Medtech innovation briefing: differential target multiplexed spinal cord stimulation for chronic lower back and leg pain. National Institute for Health and Care Excellence (NICE). Available from: www.nice.org.uk/guidance/mib305.
8. Fishman M, Cordner H, Justiz R, et al. Twelve-Month results from multicenter, open-label, randomized controlled clinical trial comparing differential target multiplexed spinal cord stimulation and traditional spinal cord stimulation in subjects with chronic intractable back pain and leg pain. Pain Pract. 2021;21(8):912–923. doi:10.1111/papr.13066
9. Kallewaard JW, Billet B, Van Paesschen R, et al. European randomized controlled trial evaluating differential target multiplexed spinal cord stimulation and conventional medical management in subjects with persistent back pain ineligible for spine surgery: 24-month results. Eur J Pain. 2024;28(10):1745–1761. doi:10.1002/ejp.2306
10. [Life expectancy and life tables: evolution of life expectancy at birth in years, Belgium (1996-2023)]. STATBEL. Available from: https://statbel.fgov.be/en/themes/population/mortality-life-expectancy-and-causes-death/life-expectancy-and-life-tables#panel-12.
11. Medtronic Plc. Product Performance Report. Summary of data from the Medtronic post-market registry; 2020.
12. Van Buyten JP, Wille F, Smet I, et al. Therapy-related explants after spinal cord stimulation: results of an international retrospective chart review study. Neuromodulation. 2017;20(7):642–649. doi:10.1111/ner.12642
13. [Nomenclature - Texts]. National Institute for Sickness and Disability Insurance (Belgium). Available from: https://www.riziv.fgov.be/nl/nomenclatuur/nomenclatuur-teksten.
14. [Reimbursable medicines and radiopharmaceutical products]. National Institute for Sickness and Disability Insurance (Belgium). Available from: https://webappsa.riziv-inami.fgov.be/ssp/ProductSearch.
15. [Implants and invasive medical devices: list of supplies and nominative lists of individual devices]. National Institute for Sickness and Disability Insurance (Belgium). Available from: https://www.riziv.fgov.be/nl/professionals/individuele-zorgverleners/verstrekkers-van-implantaten/implantaten-en-invasieve-medische-hulpmiddelen-lijst-van-de-verstrekkingen-en-nominatieve-lijsten-van-de-individuele-hulpmiddelen.
16. Neyt M, Thiry N, Cleemput I. Belgian Guidelines for Economic Evaluations and Budget Impact Analyses.
17. Deer T, Heros R, Scarfo K, et al. A cost effectiveness analysis of spinal cord stimulation versus conventional medical management for the treatment of low back pain using data from DISTINCT RECT and medical claims from a U.S. commercial payer database. J Pain Res. 2025;18:2823–2838. doi:10.2147/JPR.S486759
18. Goudman L, Rigoard P, Billot M, Duarte RV, Eldabe S, Moens M. Patient selection for spinal cord stimulation in treatment of pain: sequential decision-making model - a narrative review. J Pain Res. 2022;15:1163–1171. doi:10.2147/JPR.S250455
19. Kaye AD, Armistead G, Amedio LS, et al. Evolving treatment strategies for neuropathic pain: a narrative review. Medicina. 2025;61(6):1063. doi:10.3390/medicina61061063
20. Wahezi SE, Yener U, Naeimi T, et al. Spinal cord stimulation explantation and chronic pain: a systematic review and technology recommendations. J Pain Res. 2025;18:1327–1340. doi:10.2147/JPR.S514732
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Spinal Cord Stimulation Explantation and Chronic Pain: A Systematic Review and Technology Recommendations
Wahezi SE, Yener U, Naeimi T, Lewis JB, Yerra S, Sgobba P, Ciftci HB, Vydyanathan A, Chiu E, Cherkalin D, Darji JY, Masterson R, Lee D, Jarusriwanna A, Palee S, Ortiz NR, Caparo M, Dayon E, Fontaine C, Bikson M, Schatman ME, Pritzlaff SG, Deer TR, Hunter CW
Journal of Pain Research 2025, 18:1327-1340
Published Date: 18 March 2025