Back to Journals » Cancer Management and Research » Volume 14
Cost-Effectiveness Analysis from a Societal Perspective of Recurrence Index for Distant Recurrence (RecurIndex) in Women with Hormone Receptor-Positive and HER2-Negative Early-Stage Breast Cancer
Authors Pennarun N ![]() , Chiu JY, Chang HC, Huang SL, Cheng SHC
, Chiu JY, Chang HC, Huang SL, Cheng SHC
Received 15 September 2021
Accepted for publication 8 February 2022
Published 25 February 2022 Volume 2022:14 Pages 761—773
DOI https://doi.org/10.2147/CMAR.S339549
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmet Emre Eşkazan
Nicolas Pennarun,1 Jian-Ying Chiu,2 Hsun-Chen Chang,3 Sean-Lin Huang,1 Skye Hung-Chun Cheng4,5
1Amwise Diagnostics Pte. Ltd., Singapore; 2Department of Medical Operation, Amwise Diagnostics Pte. Ltd., Singapore; 3Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taipei, Taiwan; 4Department of Radiation Oncology, Koo Foundation Sun Yat-Sen Cancer Center, Taipei, Taiwan; 5Cancer Center, Taitung Christian Hospital, Taitung, Taiwan
Correspondence: Skye Hung-Chun Cheng, Department of Radiation Oncology, Koo Foundation Sun Yat-Sen Cancer Center, 125, Lide Road, Beitou District, Taipei, 112, Taiwan, Tel +886 2 2897 0011, ext. 1302, Email [email protected]
Purpose: A clinical-genomic prognostic multigene panel (RI-DR assay, RecurIndex®), predicting the risk level of distant recurrence (DR) in early-stage breast cancer (EBC) patients with an Asian background, has been validated as a valuable tool for identifying high-risk patients to develop distant recurrence (metastasis). Although the clinical benefit of adjuvant chemotherapy from the assay’s prediction is already proved, its affordability remains uncertain. This study is the first time in which the long-term cost-effectiveness of the RI-DR assay is evaluated.
Patients and Methods: A lifetime Markov decision-analytic model was developed from a societal perspective to estimate the life-years gained (LYGs), quality-adjusted life-years (QALYs), medical costs, and incremental cost-effectiveness ratios (ICERs), comparing EBC women with and without RI-DR genomic testing. A decision tree was used to classify patients in one of the fifteen end nodes (by order, each arm was stratified by a patient being tested or not with the RI-DR assay, being treated or not with adjuvant chemotherapy and had no, minor, major, or fatal toxicity after adjuvant chemotherapy). Health utilities, costs, transition probabilities, and survival data were extracted from the scientific literature. Deterministic sensitivity analysis (DSA) and probabilistic sensitivity analysis (PSA) were performed on variables to assess the robustness of the model. A willingness-to-pay (WTP) threshold of 790,000 NT$ per QALY gained was considered as a cost-effectiveness criterion.
Results: The incremental cost per QALY gained under base-case assumptions of the model was 173,842 NT$. Findings on the variation in model input parameters were robust and confirmed that every key variable was cost-effective for the benefit of RI-DR testing.
Conclusion: The clinical-genomic RI-DR assay is cost-effective in guiding adjuvant chemotherapy decisions compared to current clinical practice guidelines.
Keywords: economic evaluation, gene signature, Markov model, decision making, RI-DR assay
Introduction
Breast Cancer is the leading cause of cancer death among women worldwide, accounting in 2020 for 24.5% of all cancer diagnoses in this population.1 Fortunately, the majority of breast cancer patients are diagnosed when the disease is in an early stage of development. However, the risk of disease progression, among early-stage breast cancer (EBC) patients who have completed their treatment(s), is still relatively high and some challenges persist due to the multiple subtypes and frequent somatic mutations of the disease.2 Therefore, selecting the most appropriate treatment for EBC patients remains a challenging task for medical experts after traditionally involved, for many years, the combination of local and systemic therapies such as surgery, adjuvant chemotherapy (CT), adjuvant radiation therapy (RT), adjuvant hormone therapy (HT) and/or human epidermal growth factor receptor 2 (HER2)-targeted therapy, leading to a common phenomenon nowadays called overtreatment. A study has shown that 30% of all invasive and ductal carcinoma in situ breast cancer cases are estimated to be vulnerable to overdiagnosis and overtreatment, posing a serious harm to the target population’s health.3 Patients may suffer from the side effects of anticancer regimens (ovarian failure, cardiotoxicity, nausea, hair loss, hematological malignancies) without receiving the full benefit of adjuvant therapies, and in the most severe cases, may die from the side effects of medications.4,5
In this context, several gene expression tests, such as Oncotype DX (Genomic Health, Redwood City, CA) and MammaPrint (Agendia Inc., Irvine, CA), have been developed, in the early 2000s, through the increasing knowledge of the biological and molecular features of breast cancer cells.6,7 The main benefit of these tools is to inform prognosis and treatment selection, according to the conventional clinical and pathological investigation of EBC women. In addition, these assays help physicians to predict the degree of benefit from adjuvant chemotherapy by assessing the recurrence risk of a patient retrospectively and, de facto, the risk of overdiagnosis and overtreatment of individuals who are not at increased risk is limited. These multigene panels are widely used in Western countries and have proven to be reliable and efficient.8,9 However, they are not yet commonly adopted in Asia since they have been generated and validated by a Caucasian population. A study has even concluded that the Oncotype DX assay may overestimate the risk of recurrence among the Japanese population.10 Other findings pointed out that patients reported by the MammaPrint test were more likely to be classified as high-risk in Korea and Japan than the counter of white women.11–13 To address these disparities, a clinical-genomic multigene classifier, namely RI-DR assay (RecurIndex®), was developed in the 2010s, through the gene-expression profiling of Taiwanese EBC patients.14
The RI-DR assay is an 18-gene prognostic and predictive biomarker, using formalin-fixed paraffin-embedded (FFPE) tumor tissues, on a quantitative reverse-transcription-polymerase chain reaction (RT-qPCR) system.15 The details of the 18-gene function are listed in Table S1. Based on the gene expression profile of a patient and six clinical factors (age at diagnosis, tumor size, lymph node status, estrogen receptor status, lymphovascular invasion, and tumor grade), a continuous Recurrence Index-Distant Recurrence (RI-DR) score is calculated on a scale of 0 to 100. Patients are grouped into two categories: low- (RI-DR score < 29) or high- (RI-DR score ≥ 29) risk of having distant recurrence (DR). The clinical validity of the RI-DR assay has already been tested in a foregoing study, which was shown to independently predict DR in EBC women up to 10 years after primary surgery.16 More recently, a head-to-head comparison between the RI-DR assay and the Oncotype DX 21-gene panel was completed, and the results confirmed a high concordance between the RI-DR score and the Recurrence Score in the classification of low-risk women (Oncotype DX).17
Even although the RI-DR clinical-genomic model has been validated as a valuable tool for identifying EBC patients with an Asian background who are at low- and high-risk of DR, the long-term affordability remains uncertain and factors that would influence its appropriate use. Furthermore, several studies in the past decade have demonstrated that breast cancer has a major impact on healthcare costs, given the prevalence and the fatality rate of the disease as well as the consideration of the global population expanding and aging, the development of new technologies, and the increase of healthcare expenditures.18,19 The incidence rate of breast cancer, forecast to increase in the coming years and involving a rise in costs, implies that it is crucial to have a better understanding of the economic impact of the different potential strategies of treating the disease. Cost-effectiveness analysis is a common method for assessing the health outcomes and costs of two interventions designed to improve health.20,21
The main objective of the analysis is to evaluate the outcomes, costs, effectiveness, and cost-effectiveness of the RI-DR clinical-genomic assay for the guidance of adjuvant chemotherapy decisions in EBC women with hormone receptor-positive, either estrogen-receptor (ER+) or progesterone receptor (PR+) or both, and negative for human epidermal growth factor receptor 2 receptor (HER2-). Women should be treated with adjuvant chemotherapy and/or hormone therapy (with either Tamoxifen or an aromatase inhibitor), preconditions used in the multigene panel to determine their risk level of distant recurrence (metastasis).
Materials and Methods
A Markov decision-analytic model with lifetime horizon and half-cycle correction was developed to estimate the life-years gained (LYGs), quality-adjusted life-years (QALYs), total costs, and incremental cost-effectiveness ratios (ICERs) of the RI-DR assay versus current clinical practice.22 The analysis was conducted from a Taiwanese societal perspective.
The targeted population for this study was all women diagnosed with invasive EBC, ER+ and/or PR+, and HER2- tumors, who underwent primary surgery as their first treatment, including mastectomy and breast-conserving surgery (BCS) with sentinel node biopsy/axillary lymph node dissection. The population entering the model was assumed to be 43 and 58 years of age for premenopausal and postmenopausal women, respectively.23
The statistical analysis was carried out using Python 3.8 (Python Software Foundation, Delaware, USA).
Analytical Decision Tree
The rectangular decision node of the tree is related to the use or not of the RI-DR assay (Figure 1). The circular chance node shows the possible alternative events for a patient. The scheme is stratified by 1) use of the RI-DR assay versus current clinical practice, 2) RI-DR risk level, 3) treatment recommendation according to the menopausal status of a woman, and 4) the grade of adjuvant chemotherapy toxicity (no/ minor/ major/ fatal). The scheme is stratified by menopausal status due to that the National Comprehensive Cancer Network (NCCN) does not recommend the same treatment regimen for premenopausal (defined as age <50 years old) and postmenopausal women (age ≥ 50 years old).24 With this classification, each patient is assigned to one of the fifteen end nodes of the decision tree.
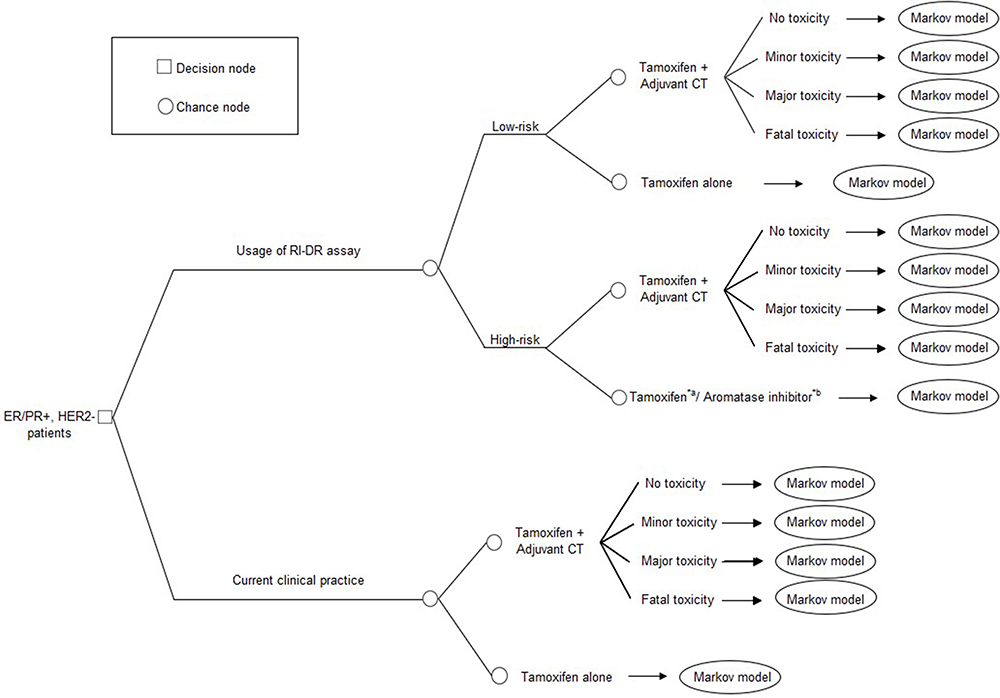 |
Figure 1 Decision tree representing the risk classification of the RI-DR assay by treatment recommendation. Notes: *Stratified by menopausal status in the analysis due to that a patient is treated with: a) Tamoxifen in premenopausal phase, b) aromatase inhibitor in postmenopausal phase. |
Markov Model Structure
Figure 2 presents a flowchart model of health states and possible state transitions of the progression of breast cancer. The Markov model was designed with three mutually exclusive health states: 1) progression-free, 2) distant recurrence, and 3) death. Patients were distributed exclusively in one of these health states over time, and events of interest were independent of each other with a transition probability affiliated to each event. Transitions between health states were designed with arrows through the Markov model.
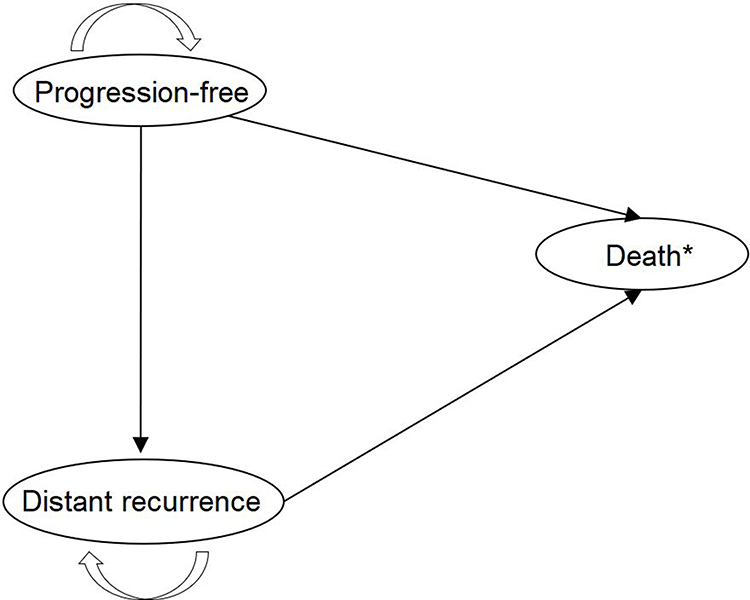 |
Figure 2 Markov model of breast cancer progression. Note: * Due to breast cancer or from other causes. |
In the initial state, all patients were alive and assumed to be diagnosed with EBC without progression of the disease. At the end of each cycle, patients could either remain progression-free or transit to a lower health state due to distant recurrence. Once in progression, patients could stay in that state or progress to death from breast cancer or chemotherapy toxicity. At any time, a patient could eventually die from a cause other than breast cancer. The process was repeated until individuals reached the estimated 2019 Taiwanese life expectancy (85 years old).25 The model measured time in 6 months-cycle. A hypothetical cohort was used for the analysis with an equal distribution among women using either the RI-DR assay or standard clinical practice. Patients, tested with the RI-DR algorithm, were categorized as low- or high-risk of distant recurrence and then oriented to a recommended treatment (Tamoxifen or an aromatase inhibitor with or without adjuvant chemotherapy). Patients, who did not receive RI-DR testing, were treated using standard clinical practice. Adjuvant chemotherapy treatment is based on the age and clinical TNM stage of individuals.
Transition Probabilities
Relevant demographic data, utilities for treatment recommendations, and toxicity from chemotherapy were derived from the published literature (Table 1). We assumed that 80% and 20% of N0 women and 60% and 40% of N1 patients were, respectively, assigned in the low- and high-risk groups.17,26 Recognizing the potential limitation that the main analysis did not target any triple-negative or HER2-overexpressing EBC patients, alternative models were constructed, including a proportion of 75% or 85% of N0 patients in the low-risk group and 55% or 65% of N1 patients with scores in the high-risk range. The probabilities of a patient being treated with adjuvant hormone therapy and/or adjuvant chemotherapy differed according to the adopted strategy. Due to possible side effects, the toxicity level of the adjuvant chemotherapy drugs was included in the analysis with probabilities based on a study by Hillner et al.27
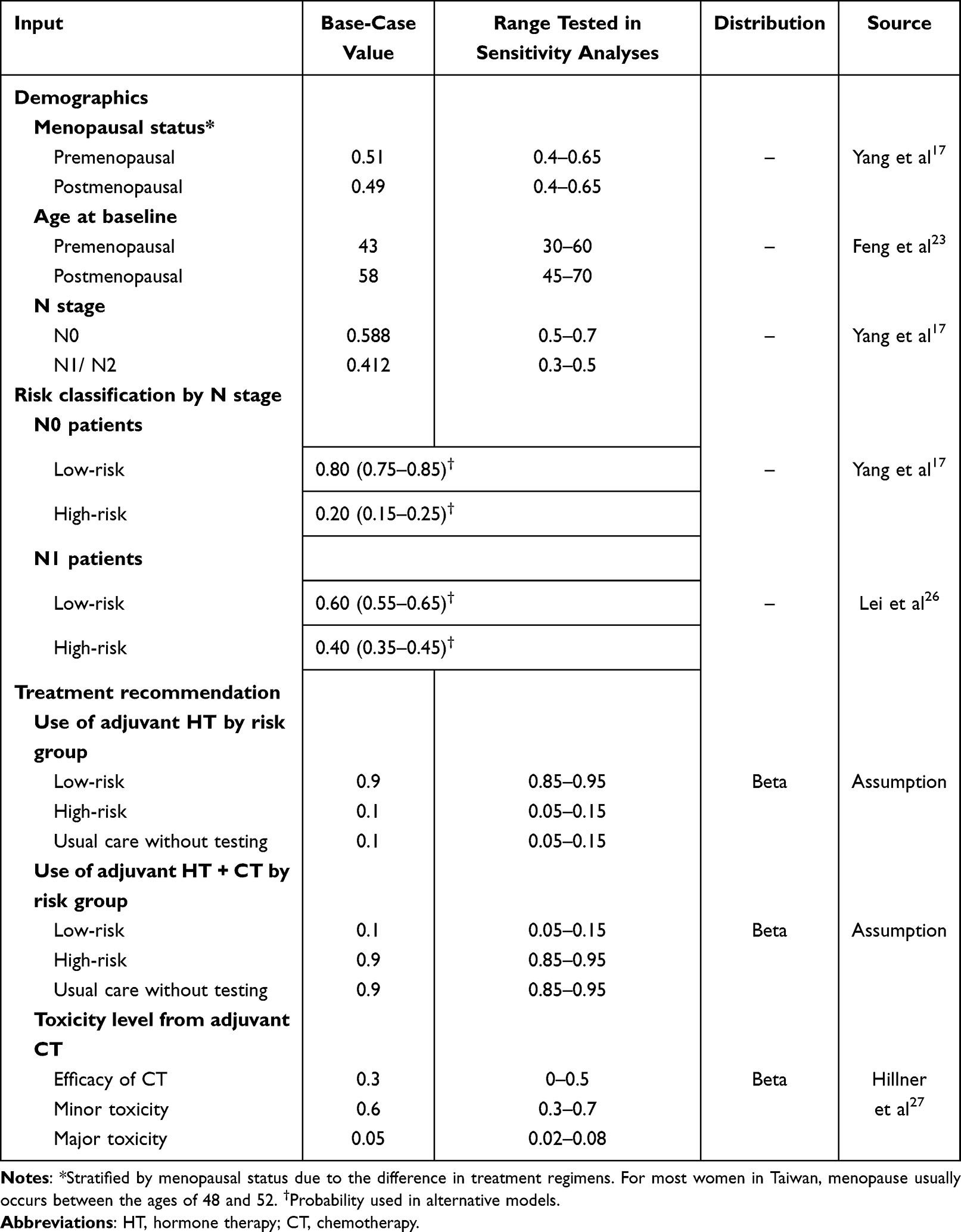 |
Table 1 Demographics and Recommendation of Treatment Regimens by Risk Group, Adverse Events, in the Base-Case Analysis |
Risk of Distant Recurrence and Death
Annual risks of recurrence and survival were obtained from various sources (Table 2). The annual female mortality rates over the extrapolated lifetime were taken from relevant age-adjusted life tables from the Department of Statistics, Ministry of the Interior, Taiwan.25 Data from Cheng et al were used to derive the risk of distant recurrence by treatment type and N stage over time.16 Investigators of this retrospective study provided Kaplan-Meier curves for distant recurrence-free survival (DRFS) and overall survival (OS) stratified by RI-DR risk classification. The annual probability of death after distant recurrence was estimated to be 40%.28
 |
Table 2 Probability of Death in the Base-Case Analysis |
Cost Analysis
Table 3 lists the direct and indirect costs used in the present study. Direct costs refer to medical and healthcare costs related to the disease. Costs related to treatment regimens were extracted from the website of the National Health Insurance Administration (NHIA) of the Ministry of Health of Taiwan.29,30 We followed the treatment recommendations made by NCCN in their clinical guidelines. The drugs used for adjuvant chemotherapy regimen without concomitant Trastuzumab include: for premenopausal women, 1) Tamoxifen (20 mg orally daily for 10 years) or 2) aromatase inhibitor therapy (ie, Anastrozole, Letrozole, Exemestane) for 5 years, in addition to an ovarian suppression or ablation; for postmenopausal women, 1) adjuvant docetaxel, doxorubicin, and cyclophosphamide (TAC regimen) given 3-weekly for six cycles, 2) adjuvant doxorubicin and cyclophosphamide (AC regimen) given 3-weekly for four cycles, and 3) adjuvant AC given 3-weekly for four cycles, followed by docetaxel given 3-weekly for four cycles.24 The impact of indirect costs combined with long-term income loss was considered in the analysis. One of the strongest effects for not returning to work after treatment for breast cancer is associated with receiving adjuvant CT.31 Absence from work attributable to adjuvant CT was calculated using the data from the Directorate General of Budget, Accounting and Statistics, Executive Yuan, Taiwan. The excess cumulative time lost from work was estimated to be 4.1 months among women who received adjuvant chemotherapy compared with women who did not.32,33
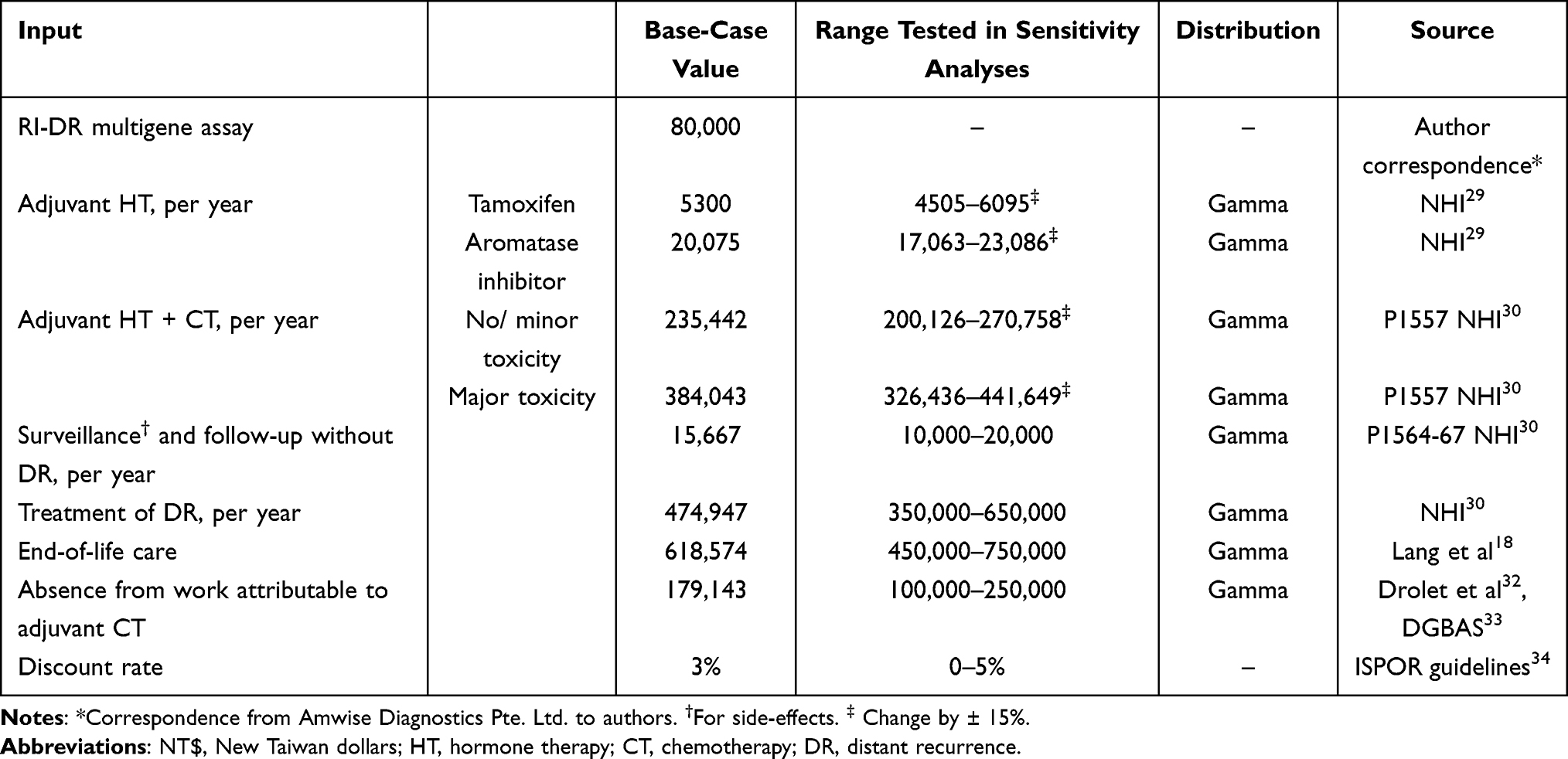 |
Table 3 Direct and Indirect Medical Cost (in NT$) |
The cost of surveillance/ follow-up of any invasive EBC patient, in the absence of clinical signs and symptoms suggesting a progression of the disease from the primary site to distant lymph nodes, involves having a physical exam 1 to 4 times per year for 5 years and a mammography every 12 months. In addition, all women, having a uterus and receiving Tamoxifen, should undergo a gynecologic examination every 12 months and for women receiving an aromatase inhibitor, a baseline health monitoring of the bone mineral density (BMD) carried out periodically thereafter.24 Patients treated for a distant recurrence are candidates for systemic adjuvant chemotherapy or hormone therapy following radiation therapy.24 The end-of-life costs are estimated according to a study conducted by Lang et al and are defined as all costs 12 months prior to the date of death of a patient, including outpatient, inpatient visits, and prescription medications.18 All costs are reported in New Taiwan dollars (NT$, 1 US dollar = 28 NT$).
A list price of the RI-DR assay of 80,000 NT$ was used in the base-case analysis. An annual discount rate of 3% was applied to costs and health effects in accordance with the recommendations made by The Professional Society for Health Economics and Outcomes Research (ISPOR) in Taiwan.34
Health Utility Weights
Health utility is a concept that has been widely adopted for the economic evaluation of the societal burden of diseases and the cost-effectiveness of interventional activities. Utilities are measured on a range from 0 to 1, in which 0 indicates death, 1 represents perfect health, and values between 0 and 1 express degrees between these two extremes. Utility weights are used for the estimation of QALYs, by calculating the length of time spent in a health state multiplied by the utility weight of that state.21 Utility weights of each health state and toxicity grade during adjuvant chemotherapy were identified from published literature (Table 4). The weight change for a health state after the completion of adjuvant hormone therapy or chemotherapy without any toxicity or distant recurrence was assumed to be 0.98.35 The health state during adjuvant chemotherapy in preventing distant recurrence or the progression of the disease weighted 0.75.35 Derived from a study published by Gold et al, the weights for toxicity of adjuvant chemotherapy were, respectively, 0.80 and 0.70 for minor toxicity and major toxicity, of which a patient could be exposed for 6 months.21
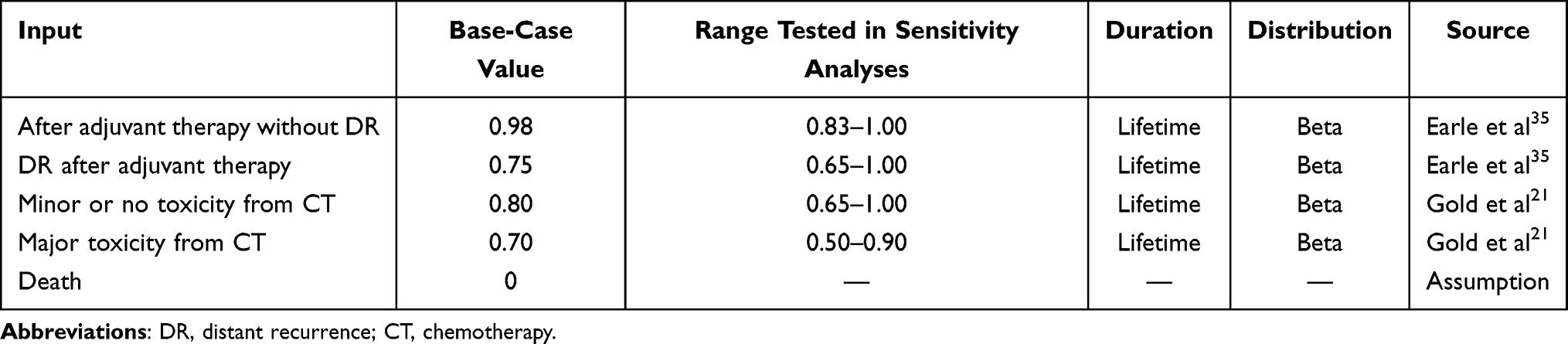 |
Table 4 Health Utility Weights Assigned to Various Disease Phases in the Base-Case Scenario |
Outcomes
The main health outcomes were measured in terms of QALYs, producing a cost per additional QALY gained, expressed as an incremental cost-effectiveness ratio (ICER). This ratio is defined as the additional cost of a specific strategy divided by its health benefit compared with an alternative strategy. The numerator of the ICER was the average total lifetime cost and the denominator was the average QALYs. A strategy is deemed cost-effective by comparing the ICER with an established societal willingness-to-pay (WTP) threshold. According to WHO’s standard requirements and the International Monetary Fund, the RI-DR assay was considered cost-effective if the ICER was less than a WTP threshold of 1-time the annual gross domestic product (GDP) per capita of the country in 2020, equals to 790,000 NT$/QALY.36 LYGs were considered in the analysis as additional outcomes.
Sensitivity Analyses
Multiple sensitivity analyses were performed. First, deterministic sensitivity analysis (DSA) with one-way sensitivity analysis was performed on all variables to assess the robustness of the Markov model due to the uncertainty associated with the assumptions, utility weights, transition probabilities, and costs included in the base-case model. Each input variable of the model was varied one at a time while other factors remained unchanged. The impact of plausible variation in assumptions was evaluated by calculating ICERs. Model input parameters were then sorted by decreasing levels of importance and plotted using a Tornado diagram with the order of importance on the vertical axis and the change in ICER on the horizontal axis. Second, probabilistic sensitivity analysis (PSA) using Monte Carlo simulation of 10,000 iterations was implemented to examine the multiparameter uncertainty around the estimates of survival rates, costs, and health effects. Distributions were assigned to model parameters for second-order uncertainty.37 Utility weight values and probabilities of disease events followed a beta distribution to ensure these were bound between 0 and 1. Cost parameters followed a gamma distribution as these could not include negative values. The result of each simulation was subsequently shown on an incremental cost-effectiveness scatterplot with the horizontal axis representing the incremental effect and the vertical axis showing the incremental cost.
Results
Base-Case Analysis
Table 5 summarizes the results of the base-case scenario. In the first scheme, the average total cost associated with breast cancer care over a lifetime horizon for women assessed through RI-DR testing was 715,877 NT$ compared to a total cost of 886,698 NT$ for women using current clinical practice. Therefore, cost savings of 170,821 NT$ were associated with the use of the RI-DR assay. The use of the gene-expression profile and current clinical practice resulted in respectively, 18.27 and 17.29 QALYs, hence the RI-DR assay expected a health lifetime gain of 0.98 additional QALYs. The ICER was estimated at 173,842 NT$ per QALY gained. In addition, RI-DR assay-guided treatment was associated with a gain of 0.95 life-years without considering utility weights.
 |
Table 5 Results of Incremental Cost-Effectiveness Ratio in the Base-Case Scenario |
Alternative Analysis
A summary comparing the cost-effectiveness of the RI-DR assay with base-case and alternative parameters is given in Table 6. The RI-DR assay was still likely to be cost-effective in any alternative scenario. In the second scenario in which 85% of N0 women and 65% of N1 women are classified in the low-risk group, the ICER of the RI-DR assay versus standard clinical practice was 163,368 NT$ per QALY gained. In the third scenario having more N0 and N1 patients in the high-risk group, the ICER was 216,356 NT$/ QALY gained.
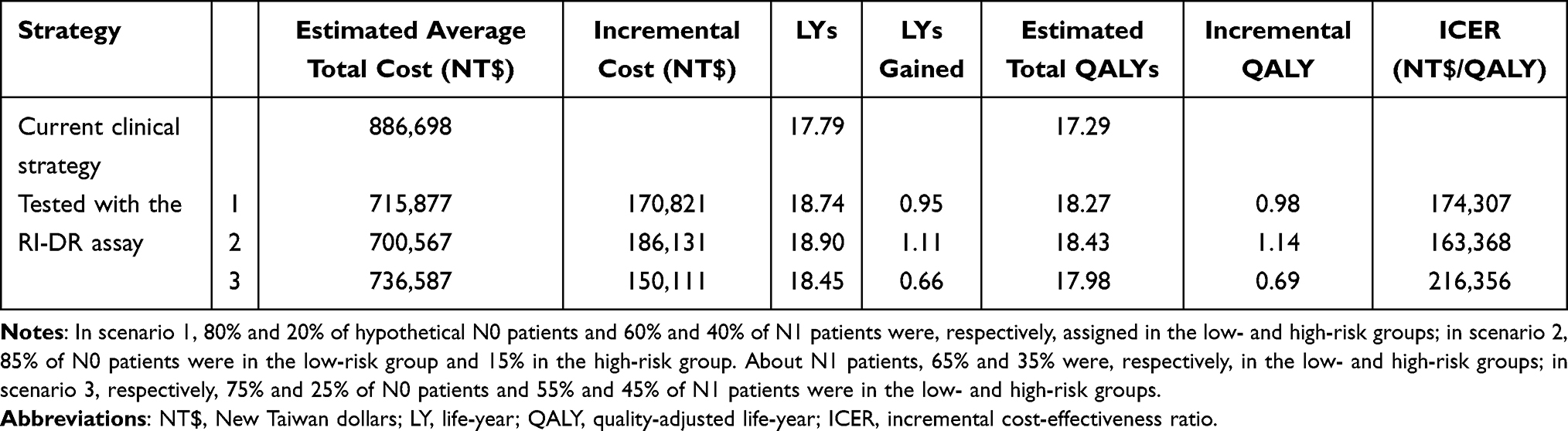 |
Table 6 Incremental Cost-Effectiveness Ratio Results in the Base-Case and Alternative Scenarios |
Sensitivity Analyses
One-way sensitivity analyses confirmed that the study findings were robust. The Tornado diagram shows that the ICER results were relatively unaffected by changes in individual model assumptions and inputs from the base-case scenario (Figure 3). Variables that have the highest impact on our analysis are presented from top to bottom and identified as the age at baseline of premenopausal patients and the proportion of N0 patients in the hypothetical cohort. The respective ICERs increase to a maximum of, respectively, approximately 373,000 NT$ and 244,000 NT$ per QALY gained for these two input parameters. On the other hand, the ICER was relatively insensitive to varying parameters of direct and indirect medical costs, probabilities by treatment recommendation, probabilities of distant recurrence, death from breast cancer or other causes, utility weights, and discount rates.
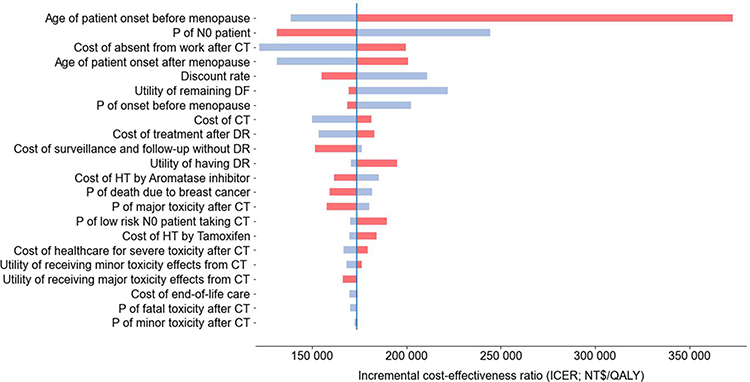 |
Figure 3 Tornado diagram of one-way sensitivity analyses. Abbreviations: P, probability; DF, disease-free. Notes: At the lowest range of each parameter, the RI-DR assay benefits more patients and saves more costs. The blue vertical line represents the ICER from the base-case scenario (173,842/NT$), providing a reference for the changes. Bars colors indicate the direction of the input value of a parameter (blue is for the low-level value and red is for the high-level value). |
The results of the probabilistic sensitivity analysis are summarized in a cost-effectiveness scatterplot in Figure 4. The incremental costs across all 10,000 simulations of the RI-DR assay versus current clinical practice ranged from 151,000 NT$ to 192,000 NT$. The incremental effects are estimated between 0.42 and 1.58, showing with confidence the use of RI-DR testing as a cost-effective strategy.
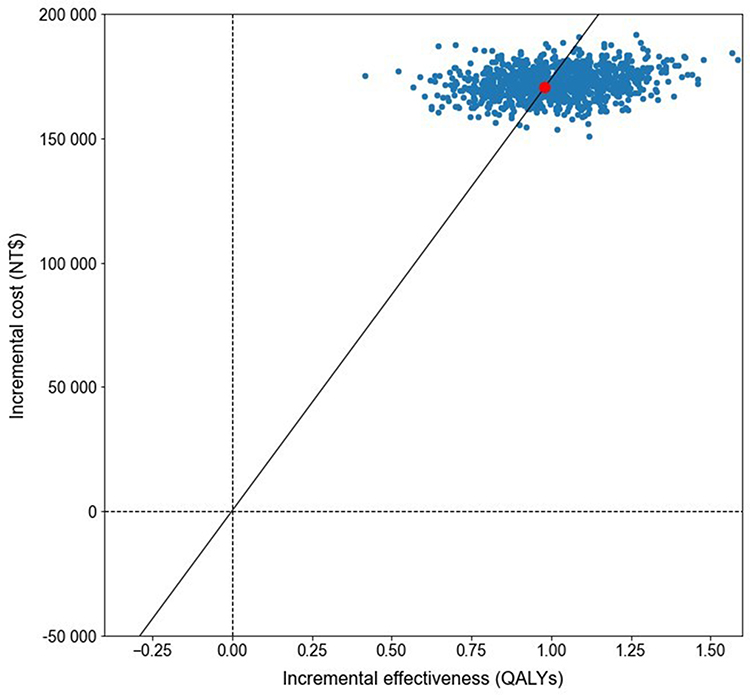 |
Figure 4 Incremental cost-effectiveness scatterplot based on Monte Carlo simulations. Note: The red dot represents the incremental cost and the incremental effect in the base-case scenario. |
Discussion
In this study, a decision-analytic modeling approach was conducted to investigate for the first time the potential economic benefit of the RI-DR assay in a Taiwanese population diagnosed with early-stage invasive breast cancer. The Markov decision-analytic model considers various input parameters to estimate direct and indirect lifetime costs, LYGs, QALYs, and ICERs. The results reveal that RI-DR testing to support adjuvant therapy decision making versus current clinical practice is associated with an estimated average total cost saving of the disease of 170,821 NT$ per patient in favor of the RI-DR assay. By combining estimated cost increases with expected gains in quality-adjusted survival with the RI-DR guided strategy, the incremental cost-effectiveness ratio is approximately 173,842 NT$/QALY gained, below the 790,000 NT$ per QALY threshold. With an initial cost of the RI-DR assay of 80,000 NT$, our findings are robust with respect to parameter changes in the PSA to assume a willingness-to-pay for genetic testing that is likely to yield reduced expenditures for payers, health systems, patients, and society in the long term. Therefore, the RI-DR assay is cost-effective in the Taiwan healthcare setting and should be considered by health policymakers for patients with early-stage invasive breast cancer. In addition, women, who are classified as low-risk of distant recurrence and treated with adjuvant chemotherapy, could benefit from fewer side effects after being tested with the RI-DR assay. Analysis of alternative scenarios with more or less patients in the low-risk classification group demonstrates that the ability of a clinical-genomic multigene assay to identify a higher proportion of low-risk patients is a key factor to consider a multigene test cost-effective. As a result, supplementary analysis of the cost-effectiveness of the genomic test should be carried out in patients with triple-negative or HER2-overexpressing EBC, who are less commonly classified as low-risk and who are candidates to different treatment options.
This pattern of results is consistent with the previous literature from the Oncotype DX assay and other gene expression profiling assays (MammaPrint, Endopredict, Mammostrat, Prosigna) validated by a Caucasian population. Several systematic reviews of economic evaluations of these predictive tests reported favorable economic outcomes in different national health policies.38,39 In overall, genomic testing for breast cancer was cost-effective in 90% of the evaluations.40 However, the estimated costs/ QALY gained are susceptible to be discordant across studies for the same panel depending on the assumptions made.41
Nevertheless, the economic evaluation was conducted from a Taiwanese societal perspective, but the target population of the RI-DR assay, defined as Asian women, is larger. This analysis is not applicable and generalizable to other Asian countries, which have different healthcare policies and payment systems. The costs and resources in the base-case analysis might vary greatly from one country’s context to another and are expected to change over time, making the cost-effectiveness of the assay complex to interpret Asia-wide. A recommended approach for further analysis in the future would be to distinguish the relative costs and health outcomes of countries other than Taiwan to estimate the cost-effectiveness of the assay.
This study has a few limitations that must be considered when interpreting the results. First, the main limitation is associated with the lack of available data in the scientific literature specific to the Taiwanese population, which forced us to make several assumptions including transition probabilities for treatment recommendations. Second, the study evaluated the risk of having a distant recurrence, but not other outcomes, such as local/regional recurrence or 2nd cancer. These outpoints are considered as competing risks of breast cancer mortality, potentially leading to a wrong interpretation of the cumulative incidence.42 Third, to date, ICER thresholds are not yet clearly defined in Taiwan. A league table based on the costs per QALY could be the most suitable approach in the country’s context, but there is no consensus yet.43 Although all of the ICER values are much lower than 790,000 NTD, national payers should take into account the social context of the country and the unclear consensus of an appropriate WTP threshold.
Conclusion
In summary, this study assessed the cost-effectiveness from a societal perspective of the RI-DR assay for the treatment of early-stage invasive breast cancer women in Taiwan. The results reveal that this panel versus current clinical practice is cost-effective in the base-case scenario and in the sensitivity analyses, which should facilitate both patients and physicians in the use of RI-DR testing. Further studies evaluating the cost-effectiveness of the assay with other outcomes in the presence of competing risks and in other Asian countries having different healthcare policies and payment systems are recommended in the future.
Abbreviations
EBC, early-stage breast cancer; CT, chemotherapy; RT, radiation therapy; HT, hormone therapy; HER2, human epidermal growth factor receptor 2; FFPE, formalin-fixed, paraffin-embedded; RT-qPCR, quantitative reverse transcription-polymerase chain reaction; RI-DR, Recurrence Index-Distant Recurrence; DR, distant recurrence; ER, estrogen receptor; PR, progesterone receptor; LYG, life-year gained; QALY, quality-adjusted life-year; ICER, incremental cost-effectiveness ratio; BCS, breast-conserving surgery; NCCN, National Comprehensive Cancer Network; DRFS, distant recurrence-free survival; OS, overall survival; NHIA, National Health Insurance Administration; TAC, adjuvant docetaxel, doxorubicin, and cyclophosphamide; AC, adjuvant doxorubicin and cyclophosphamide; BMD, bone mineral density; NT$, New Taiwan dollars; WTP, willingness-to-pay; GDP, gross domestic product; DSA, deterministic sensitivity analysis; PSA, probabilistic sensitivity analysis; P, probability.
Data Sharing Statement
The raw data and Python code supporting the conclusions of this article are available upon request to the authors ([email protected]).
Ethics Approval and Informed Consent
The study was conducted in accordance with the guidelines of the Declaration of Helsinki. This study was based on mathematical modeling. For this reason, no ethical approval was required by the ethics committee.
Acknowledgments
The authors thank Zoe Chan and Rubi Wei for their administrative support, Rae Lin for her help on the interpolation and extrapolation of costs associated with breast cancer management, and Kuan-Hui Shih for her valuable input into the design of this study.
Author Contributions
All authors made a significant contribution to the work reported, either in the conception, study design, execution, acquisition of data, analysis, and/or interpretation of data; took part in the drafting, revising, and/or critically reviewing of the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Amwise Diagnostics Pte. Ltd. [grant number AMW0804].
Disclosure
Nicolas Pennarun is a consultant for Amwise Diagnostics Pte. Ltd. Jian-Ying Chiu and Sean-Lin Huang are employees of Amwise Diagnostics Pte. Ltd. All other authors have no conflicts of interest to declare for this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Waks AG, Winer EP. Breast cancer treatment: a review. JAMA. 2019;321(3):288–300. doi:10.1001/jama.2018.19323
3. Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev. 2013;2013(6):Cd001877. doi:10.1002/14651858.CD001877.pub5
4. Esserman LJ, Thompson IM
5. Cheng SHC, Yu BL, Horng CF, et al. Long-term survival and stage I breast cancer subtypes. J Cancer Res Pract. 2016;3(1):1–8. doi:10.1016/j.jcrpr.2015.10.005
6. Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351(27):2817–2826. doi:10.1056/NEJMoa041588
7. Van’t Veer LJ, Dai H, van de Vijver MJ, et al. Gene expression profiling predicts clinical outcome of breast cancer. Nature. 2002;415(6871):530–536. doi:10.1038/415530a
8. Albain KS, Barlow WE, Shak S, et al. Prognostic and predictive value of the 21-gene recurrence score assay in post-menopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: a retrospective analysis of a randomised trial. Lancet Oncol. 2010;11(1):55–65. doi:10.1016/S1470-2045(09)70314-6
9. Paik S, Tang G, Shak S, et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol. 2006;24(23):3726–3734. doi:10.1200/JCO.2005.04.7985
10. Toi M, Iwata H, Yamanaka T, et al. Clinical significance of the 21-gene signature (Oncotype DX) in hormone receptor-positive early stage primary breast cancer in the Japanese population. Cancer. 2010;116(13):3112–3118. doi:10.1002/cncr.25206
11. Kwon MJ, Lee JE, Jeong J, et al. Comparison of genesWell BCT score with Oncotype DX recurrence score for risk classification in asian women with hormone receptor-positive, HER2-negative early breast cancer. Front Oncol. 2019;9(667). doi:10.3389/fonc.2019.00667
12. Na KY, Kim KS, Lee JE, et al. The 70-gene prognostic signature for Korean breast cancer patients. J Breast Cancer. 2011;14(1):33–38. doi:10.4048/jbc.2011.14.1.33
13. Ishitobi M, Goranova TE, Komoike Y, et al. Clinical utility of the 70-gene MammaPrint profile in a Japanese population. Jpn J Clin Oncol. 2010;40(6):508–512. doi:10.1093/jjco/hyp195
14. Cheng SH, Horng CF, Huang TT, et al. An eighteen-gene classifier predicts locoregional recurrence in post-mastectomy breast cancer patients. EBioMedicine. 2016;5:74–81. doi:10.1016/j.ebiom.2016.02.022
15. Huang TT, Lei L, Chen CA, Lu TP, Jen CW, Cheng SH. A new clinical-genomic model to predict 10-year recurrence risk in primary operable breast cancer patients. Sci Rep. 2020;10(1):4861. doi:10.1038/s41598-020-61535-9
16. Cheng SH, Huang TT, Cheng YH, et al. Validation of the 18-gene classifier as a prognostic biomarker of distant metastasis in breast cancer. PLoS One. 2017;12(9):e0184372. doi:10.1371/journal.pone.0184372
17. Yang PS, Lee YH, Chung CF, et al. A preliminary report of head-to-head comparison of 18-gene-based clinical-genomic model and Oncotype DX 21-gene assay for predicting recurrence of early-stage breast cancer. Jpn J Clin Oncol. 2019;49(11):1029–1036. doi:10.1093/jjco/hyz102
18. Lang HC, Wu SL. Lifetime costs of the top five cancers in Taiwan. Eur J Health Econ. 2012;13(3):347–353. doi:10.1007/s10198-011-0307-1
19. Luengo-Fernandez R, Leal J, Gray A, Sullivan R. Economic burden of cancer across the European Union: a population-based cost analysis. Lancet Oncol. 2013;14(12):1165–1174. doi:10.1016/S1470-2045(13)70442-X
20. Weinstein MC, Stason WB. Foundations of cost-effectiveness analysis for health and medical practices. N Engl J Med. 1977;296(13):716–721. doi:10.1056/NEJM197703312961304
21. Gold MR, Siegel JE, Russell LB, Weinstein MC, eds. Cost-Effectiveness in Health and Medicine.
22. Sonnenberg FA, Beck JR. Markov models in medical decision making: a practical guide. Med Decis Making. 1993;13(4):322–338. doi:10.1177/0272989X9301300409
23. Feng F, Wei Y, Zheng K, et al. Comparison of epidemiological features, clinicopathological features, and treatments between premenopausal and postmenopausal female breast cancer patients in western China: a retrospective multicenter study of 15,389 female patients. Cancer Med. 2018;7(6):2753–2763. doi:10.1002/cam4.1503
24. National Comprehensive Cancer Network (NCCN) [website on the Internet]. NCCN clinical practice guidelines in oncology™: breast cancer. Fort Washington, PA: NCCN; 2017. Ver. 3.2021. Available from: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf.
25. Department of Statistics, Ministry of the Interior, Taiwan, ROC [website on the Internet]. Table 1 Abridged life table of Republic of China area-Female; 2019. Available from: https://www.moi.gov.tw/english/cl.aspx?n=7780.
26. Lei L, Wang XJ, Mo YY, Cheng SH, Zhou Y. DGM-CM6: a new model to predict distant recurrence risk in operable endocrine-responsive breast cancer. Front Oncol. 2020;10:783. doi:10.3389/fonc.2020.00783
27. Hillner BE, Smith TJ. Efficacy and cost effectiveness of adjuvant chemotherapy in women with node-negative breast cancer. A decision-analysis model. N Engl J Med. 1991;324(3):160–168. doi:10.1056/NEJM199101173240305
28. Elkin EB, Weinstein MC, Winer EP, Kuntz KM, Schnitt SJ, Weeks JC. HER-2 testing and trastuzumab therapy for metastatic breast cancer: a cost-effectiveness analysis. J Clin Oncol. 2004;22(5):854–863. doi:10.1200/JCO.2004.04.158
29. Health Insurance Drug Database [website on the Internet]. National Health Insurance Administration; 2021. Available from: https://www.nhi.gov.tw/QueryN/Query1.aspx.
30. National Health Insurance Administration Database [website on the Internet]. Breast cancer medical benefit improvement plan report; March, 2021. Available from: https://www.nhi.gov.tw/Content_List.aspx?n=907AA899425E01AF&topn=5FE8C9FEAE863B46.
31. Johnsson A, Fornander T, Rutqvist LE, Vaez M, Alexanderson K, Olsson M. Predictors of return to work ten months after primary breast cancer surgery. Acta Oncol. 2009;48(1):93–98. doi:10.1080/02841860802477899
32. Drolet M, Maunsell E, Mondor M, et al. Work absence after breast cancer diagnosis: a population-based study. CMAJ. 2005;173(7):765–771. doi:10.1503/cmaj.050178
33. Industry and Service Sector Earnings Statistics, April 2021 [website on the Internet] Directorate General of Budget, Accounting and Statistics (DGBAS), Executive Yuan, Taiwan; 2021. Available from: https://eng.stat.gov.tw/public/Attachment/1610154727MKFOK1MR.pdf.
34. Research ISPOR. Pharmacoeconomic guidelines around the world [website on the Internet]; 2018. Available from: https://tools.ispor.org/PEguidelines/countrydet.asp?c=31&t=1.
35. Earle CC, Chapman RH, Baker CS, et al. Systematic overview of cost-utility assessments in oncology. J Clin Oncol. 2000;18(18):3302–3317. doi:10.1200/JCO.2000.18.18.3302
36. Edejer TTT, Baltussen R, Adam T, et al. World Health Organization. Making choices in health: who guide to cost-effectiveness analysis [website on the Internet]; 2003. Available from: https://www.who.int/choice/publications/p_2003_generalised_cea.pdf.
37. Briggs A, Sculpher MJ, Claxton K. Chapter 4: making decision models probabilistic. In: Decision Modelling for Health Economic Evaluation. Oxford, United Kingdom: Oxford University Press; 2006:77–120.
38. Hornberger J, Alvarado MD, Rebecca C, Gutierrez HR, Yu TM, Gradishar WJ. Clinical validity/utility, change in practice patterns, and economic implications of risk stratifiers to predict outcomes for early-stage breast cancer: a systematic review. J Natl Cancer Inst. 2012;104(14):1068–1079. doi:10.1093/jnci/djs261
39. Rouzier R, Pronzato P, Chéreau E, Carlson J, Hunt B, Valentine WJ. Multigene assays and molecular markers in breast cancer: systematic review of health economic analyses. Breast Cancer Res Treat. 2013;139(3):621–637. doi:10.1007/s10549-013-2559-1
40. Blok EJ, Bastiaannet E, Van den Hout WB, et al. Systematic review of the clinical and economic value of gene expression profiles for invasive early breast cancer available in Europe. Cancer Treat Rev. 2018;62:74–90. doi:10.1016/j.ctrv.2017.10.012
41. Wang SY, Dang W, Richman I, Mougalian SS, Evans SB, Gross CP. Cost-effectiveness analyses of the 21-gene assay in breast cancer: systematic review and critical appraisal. J Clin Oncol. 2018;36(16):1619–1627. doi:10.1200/JCO.2017.76.5941
42. Rueda OM, Sammut SJ, Seoane JA, et al. Dynamics of breast-cancer relapse reveal late-recurring ER-positive genomic subgroups. Nature. 2019;567(7748):399–404. doi:10.1038/s41586-019-1007-8
43. Lee NC, Li Y, Wu GH, Gau C. The potential methods of icer threshold estimation in Taiwan. Value Health. 2016;19(3):A287. doi:10.1016/j.jval.2016.03.765
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.