Back to Journals » Clinical Ophthalmology » Volume 20
Corneal Tomography Changes After Simultaneous Topical Application of Cyclosporine and Trehalose in Keratoconus Evaluated with an Artificial Intelligence Model
Authors Shetty R, Khamar P, Kundu G, Shetty P ![]() , Honniganur D, Shah A, Narasimhan R, Sinha Roy A
, Honniganur D, Shah A, Narasimhan R, Sinha Roy A ![]()
Received 7 May 2026
Accepted for publication 11 June 2026
Published 15 July 2026 Volume 2026:20 619163
DOI https://doi.org/10.2147/OPTH.S619163
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
Rohit Shetty,1 Pooja Khamar,1 Gairik Kundu,1 Panaah Shetty,1 Deepthi Honniganur,1 Abha Shah,1 Raghav Narasimhan,2 Abhijit Sinha Roy2
1Department of Cornea and Refractive Surgery, Narayana Nethralaya Eye Hospital, Bangalore, Karnataka, India; 2Imaging, Biomechanics and Mathematical Modeling Solutions Lab, Narayana Nethralaya Foundation, Bangalore, Karnataka, India
Correspondence: Abhijit Sinha Roy, Imaging, Biomechanics and Mathematical Modeling Solutions Lab, Narayana Nethralaya Foundation, #258A Hosur Road, Bommasandra, Bangalore, Karnataka, 560099, India, Email [email protected]
Purpose: To assess corneal tomography changes in keratoconus (KC) patients after long-term simultaneous use of topical cyclosporine and trehalose.
Design: Retrospective observational study.
Methods: Corneal tomography of 362 eyes with KC was performed using Pentacam (OCULUS Optikgerate Gmbh, Germany) at 1st visit and at the last follow-up. Progression was initially evaluated based on change in maximum keratometry (Kmax). This initial classification was then assessed with an artificial intelligence model of 31 tomography variables of Pentacam to confirm the inference of progression based on Kmax alone.
Results: The mean follow-up time was 10.8 ± 6.01 months (range: 6 to 36 months). Based on a change in Kmax of 0.75, 1.0 and 1.25D criteria, more than 90% of the eyes were stable for each criterion at the last follow-up (initial classification). The AI model confirmed stability of corneal tomography in more than 95% of the eyes at the last follow-up (final classification).
Conclusion: Most KC eyes had stable tomography findings between the first and last follow-up. Topical anti-inflammatory regimens may be useful for minimizing or eliminating KC progression.
Keywords: keratoconus, cyclosporine, trehalose, inflammation, tomography, cornea
Introduction
Keratoconus (KC) is a progressive corneal ectasia characterized by stromal thinning and conical protrusion that can lead to visual impairment if left untreated.1 Inflammation, oxidative stress, and impaired autophagy play a significant role in the disease pathogenesis.2–4 In progressive KC, corneal crosslinking (CXL) is the first-line intervention to halt biomechanical weakening of the cornea.5 Both CXL and corneal transplantation can be performed in advanced KC patients. However, there remains a therapeutic void in early or mild disease, particularly in patients without definitive progression. Adjunct medical therapy with anti-inflammatory eye drops may overcome this limitation. Elevated levels of pro-inflammatory cytokines, eg, interleukin-6 (IL-6), tumor necrosis alpha-α (TNF- α), and matrix metalloproteinase-9 (MMP-9), have been identified in the tears of patients with KC, reflecting chronic inflammation.2,6 Mechanical factors, such as eye rubbing, further promote inflammatory responses and protease release, contributing to corneal degradation.3 Simultaneously, oxidative stress markers, such as lipid peroxidation products and nitrites, are elevated in KC corneas, while antioxidants like glutathione and total antioxidant capacity are diminished.7 KC corneas also demonstrate abnormal enzyme profiles, including increased catalase and cathepsin V/L2 and reduced tissue inhibitors of metalloproteinases (TIMP-1), reflecting an imbalance in matrix remodeling.8 Fibroblasts derived from KC corneas produce more reactive oxygen species (ROS) and undergo higher rates of apoptosis under oxidative challenge compared to healthy corneas.9
Additionally, the dysregulation of autophagy may also drive progression of KC. The KC corneas exhibit elevated levels of autophagy-related markers, such as LC3, particularly in the epithelium overlying the cone apex.10 This suggests stress-induced autophagy activation, but studies also point to a dysfunctional response due to an incomplete autophagic flux.10,11 Impaired autophagy can lead to accumulation of toxic protein aggregates and uncontrolled inflammation, creating a feedback loop that exacerbates corneal thinning and degradation.12 Trehalose, a naturally occurring disaccharide composed of two glucose molecules linked via an α,α-1,1-glycosidic bond, acts as a cytoprotective, antioxidant, anti-inflammatory, and autophagy-enhancing agent.4,13,14 Trehalose stabilizes cellular proteins and membranes under extreme stress, such as dehydration and heat.13 Recently, trehalose has demonstrated efficacy in protecting corneal epithelial cells from desiccation-induced death and in managing dry eye disease.14 It promotes autophagic flux through activation of the Keap1-Nrf2 antioxidant pathway, suppresses inflammatory cytokine production, and mitigates apoptosis in corneal cells exposed to oxidative stress.4 Thus, trehalose may serve as a novel adjunctive option for modifying disease progression in early keratoconus. In this study, we evaluated the effect of a topical trehalose 3% eye drop (administered four times daily) in combination with cyclosporine 0.05% (twice daily) in patients with early to moderate keratoconus and low-moderate risk of progression. Cyclosporine, an anti-inflammatory immunomodulator, was used to address ocular surface inflammation potentially stemming from allergic eye disease or mechanical irritation. An artificial intelligence (AI)-based random forest model previously validated on longitudinal Pentacam tomography data was used to objectively assess progression status over time.15 We aimed to determine whether this pharmacologic regimen could promote disease stability and reduce tomographic signs of progression over the long-term.
Methods
This was a retrospective review of records of KC patients visiting the out-patient department of Narayana Nethralaya eye hospital, Bangalore, India. The study was approved by the ethics committee of the Narayana Nethralaya eye hospital, Bangalore (Approval # C/2016/12/05). Due to the retrospective nature of the study, the requirement of informed consent was waived off by the ethics committee. The study adhered to the tenets of the Declaration of Helsinki, and patient data confidentiality and compliances were met. All the eyes were confirmed cases of KC. All eyes were put on topical medications: cyclosporine 0.05% eye drops twice daily and 3% trehalose mixed with sodium hyaluronate four times per day for at least 6 months. The change in maximum curvature of the anterior surface (Kmax) between 2 visits (at least 6 months apart) was observed. Exclusion criteria were eyes that underwent cross-linking, other ectatic conditions such as keratoglobus, pellucid marginal degeneration, post-refractive surgery ectasia, autoimmune disorders, any ocular or corneal surgery prior to the 1st visit of the patient or during the course of disease follow-up, patients on topical drops other than the above specified drops, patients with corneal scarring, and patients using contact lenses. All eyes underwent Pentacam imaging (OCULUS Optikgerate Gmbh, Germany). Only those images unaffected by blinking or eyelashes were used. These images were automatically classified as “OK” by the Pentacam software. Further, the detected anterior and posterior edges of the corneal scans were manually confirmed so that no missing portions of the detected edges confounded the tomography of the cornea.16
We used our recently published AI model, which used the tomography parameters of the cornea from the 1st and latest follow-up visits of the patient.15 Generally, the maximum anterior curvature (Kmax) is used for evaluating progression, such as an increase by 1D. However, the anterior surface of the cornea is very fluid and undergoes dynamic topology changes due to epithelium remodeling, eye rubbing, and inflammation in KC. Hence, we devised an AI model that evaluated multiple tomography parameters from Pentacam so that a distinction between local and global progression could be ascertained.15 Here, local progression could be simply a change in Kmax (a point or local measure) with no concomitant change in other tomography parameters, whereas global would indicate simultaneous change in both Kmax and other parameters. Here, the former can be interpreted as stable, and the latter can be considered a true instance of progression.15 The Pentacam parameters were exported from each measurement as a comma-separated value (csv) file. The average of parameters from repeat scans was used if multiple image sessions were available at the same time point. The following Pentacam parameters were used to calculate the difference data:
- Flat and steep axis curvature, mean curvature, axis and magnitude of astigmatism, and asphericity (Q-factor) of the anterior and posterior corneal surface (a total of 12 parameters).
- Central and minimum corneal thickness, Belin-Ambrosio overall deviation (BAD-D) index (a total of 3 parameters). The BAD-D index is an aggregate parameter of all the D indices calculated by Pentacam.
- Index of surface variance (ISV), Index of Height Asymmetry (IHA), Index of Vertical Asymmetry (IVA), Index of Height Decentration (IHD), Keratoconus Index (KI) and Center of Keratoconus Index (CKI) (a total of 6 parameters).
- Root mean square (RMS) of coma, lower order (LOA) and higher order aberrations (HOA) along with defocus and spherical aberration (SA) of the anterior and posterior corneal surface (a total of 10 parameters). These aberrations were evaluated for the central 6 mm cornea using a Zernike order up to order 6.
- Scores A, B and C of ABCD score in Pentacam. We did not consider D in the analyses as it was related to visual acuity only.
In this study, the difference in tomography parameters between the 1st and latest visit was calculated. Then, the data was sub-divided into progression vs no-progression based on change in Kmax by 0.75D, 1.0D and 1.25D. This initial classification was used as test data in the AI model15 to determine which eyes had progressed globally (true instance) despite the use of anti-inflammatory eye drops and which eyes showed only local progression (stable). Additional technical details of the AI model are described in our earlier study.15
Statistical Analysis
The performance of the AI model was evaluated using several parameters, including area under the curve (AUC), classification accuracy (CA), precision (Pr), recall (Rec), and F1-score. The Orange3 version 3.25.0 data mining package (University of Ljubljana, Slovenia) was used. Statistical tests were conducted with MedCalc v19 (MedCalc Inc, Belgium). Mean±standard deviation was calculated for each parameter after confirming normality of distribution.
Results
A total of 362 eyes of 181 patients were analyzed, which included 98 males and 83 females with an average age of 26 ± 3.6 years. After assessing the quality of the scans, a total of 724 Pentacam scans of 362 eyes were included in the study. The mean follow-up time was 10.8 ± 6.01 months (range: 6 to 36 months). Table 1 shows the mean values of all parameters at visit 1 and visit 2 (latest follow-up after initiation of topical eye drops) for the whole group. Among all parameters, central corneal thickness, thinnest corneal thickness, BAD-D, defocus and spherical aberration changed significantly between the visits (p<0.05). However, none of these changes were clinically significant.
- Based on a change in Kmax by 0.75D, 331 and 31 eyes were classified as non-progressed and progressed, respectively. When the AI model was used, 326 out of the 331 eyes (98.5%) were confirmed as stable. However, 13 out of 31 (41.9%) eyes were reclassified from progressed to stable (or local progression only) by the AI, while the remaining 18 eyes were maintained as progressed (or global progression). The AUC, CA, Pr, Rec and F1-score of the model were 0.93, 0.95, 0.95, 0.95 and 0.95, respectively.
- Based on a change in Kmax by 1D, 343 and 19 eyes were classified as non-progressed and progressed, respectively. When the AI model was used, 342 out of the 343 eyes (99.4%) were confirmed as stable. However, 9 out of 19 (52.6%) eyes were reclassified from progressed to stable (or local progression only) by the AI, while the remaining 10 eyes were maintained as progressed (or global progression). The AUC, CA, Pr, Rec and F1-score of the model were 0.96, 0.97, 0.96, 0.97 and 0.96, respectively.
- Based on a change in Kmax by 1.25D, 346 and 16 eyes were classified as non-progressed and progressed, respectively. When the AI model was used, all 346 eyes (100%) were confirmed as stable. However, 9 out of 16 (56.2%) eyes were reclassified from progressed to stable (or local progression only) by the AI, while the remaining 6 eyes were maintained as progressed (or global progression). The AUC, CA, Pr, Rec and F1-score of the model were 0.94, 0.98, 0.98, 0.98 and 0.97, respectively.
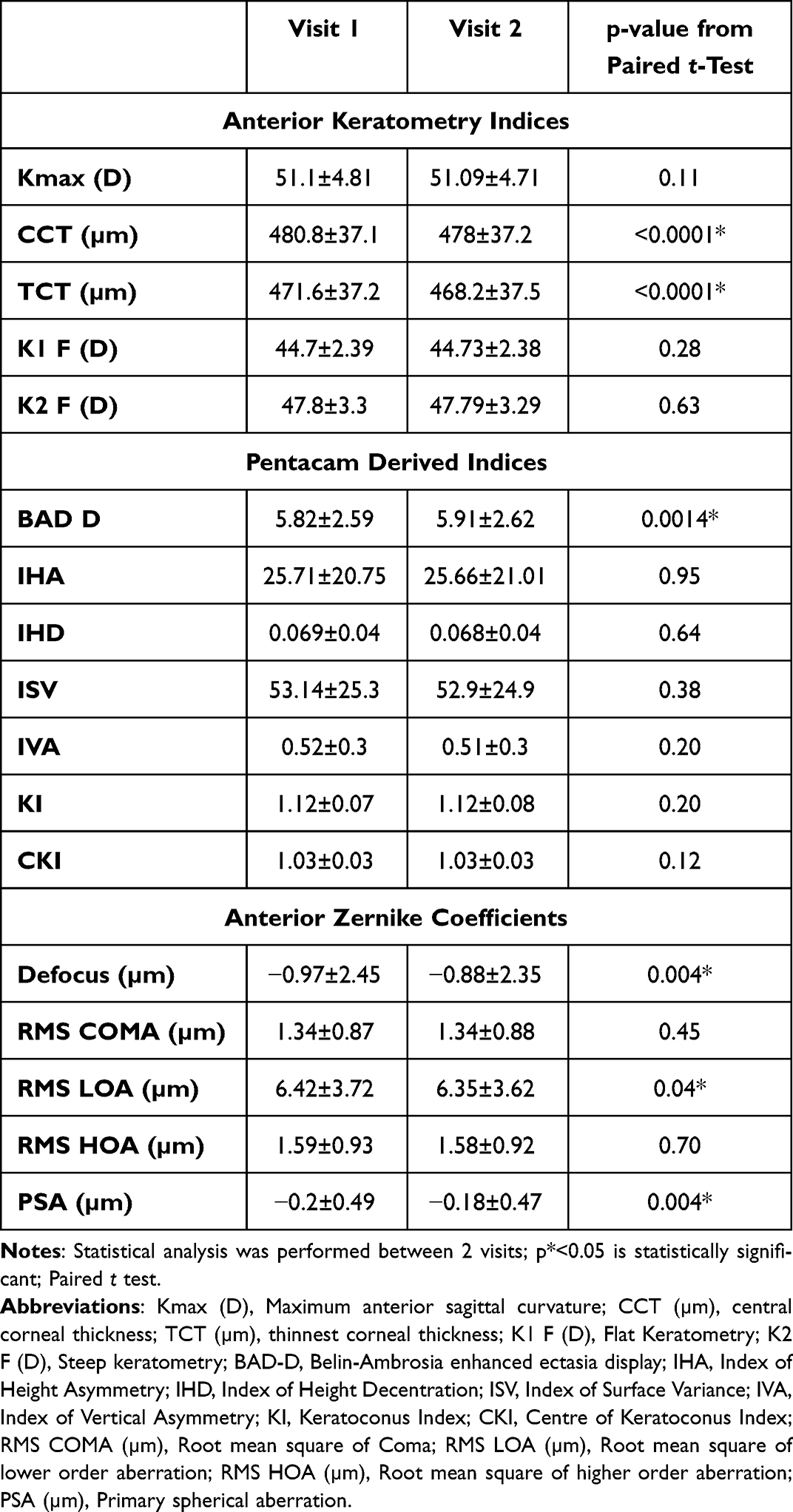 |
Table 1 Mean and Standard Deviation of Tomographic Parameters at Both Visits |
Thus, both the change in Kmax and the AI model showed that most of the eyes were stable upon long-term follow-up with the use of cyclosporine and trehalose. Further, the AI helped in identifying eyes that showed only local progression based on change in Kmax and stability of other Pentacam tomography parameters. Interestingly, a combination of change in Kmax and the AI showed that overall, 339 to 355 eyes were stable depending on the cut-off criteria for change in Kmax. An example of why this combinational strategy of assessing progression works better than using the change in Kmax is shown in Table 2.
 |
Table 2 The Mean ± Standard Deviation of Change in Tomographic Parameters of the Eyes. The Eyes Were Grouped Based on 2×2 Confusion Matrix. Here, the Initial Classification Was Based on Change in Kmax by 1D |
Table 2 shows the mean ± standard deviation of tomographic parameters of eye groups based on the initial classification of the eyes as no-progression and progression based on a change in Kmax by 1D. The AI reclassified the no-progression eyes as local progression (or stable; column 2 of Table 1) and global progression (true progression; column 3 in Table 1). The change in Kmax was less than 1D in both groups but note the difference between the change in BAD-D, ie, a mean of 0.036 vs a mean of 0.55. Similarly, the eyes with initial classification of progression and reclassification by the AI mode to local progression (or stable) had a mean change in BAD-D of 0.35 (column 4 in Table 1) despite a mean change in Kmax of 1.51D (column 4 in Table 1). This highlights the differential change in tomographic parameters with progression of disease. The more the number of tomographic parameters undergoing a change, the more confidence is associated with the diagnosis of true progression.
Discussion
Conventional management of KC is driven by laser treatments,17 scleral contact lenses,18 intracorneal rings,19 tissue addition,20 and corneal crosslinking.21 These methods are expensive and sometimes invasive but capable of providing significant visual benefits to the patient. For example, significant reductions in higher-order aberrations were observed after topography-guided laser ablation of KC eyes.22 However, non-surgical methods of prevention of KC progression have not received much attention. A recent study showed that the time of eye rubbing could have a mechanical bearing on the stiffness of the cornea, leading to progression of KC.23 Both eye rubbing and environmental factors can act as feedforward instigators to promote inflammation in KC eyes, leading to progression of the disease.23,24 Therefore, it is clear that therapeutic management of inflammation could be a useful strategy to manage KC patients who do not have access to more expensive methods or wish to avoid surgery.
Few studies have investigated oral supplementation for management of KC progression. Oral supplementation with a highly concentrated docosahexaenoic acid (DHA) triglyceride was investigated in a randomized controlled trial of 34 patients over 3 months.25 The study showed that inflammatory markers were reduced due to supplementation, and statistically significant differences were in a few tomography parameters.25 Another study investigated the effects of Vitamin D supplementation on disease progression, systemic inflammation, collagen degradation, and oxidative stress in 40 patients with a follow-up time of 12 months.26 Overall, 75% of the eyes remained stable after 12 months.26 Furthermore, these patients (75% cohort) exhibited a downregulation in inflammatory and platelet activation pathways and an upregulation of proteoglycan metabolism/biosynthesis enrichment.26 Select tomography parameters such as Kmax and thickness remained stable in these eyes.26 A similar outcome was obtained in another study where Vitamin D supplementation was given to 20 patients (age range of 16–19 years).27 Nearly 72% of the eyes remained stable after a 12 month follow-up.27 These studies showed that molecular strategies of KC management may have a clinical role and require further long-term studies.28
Most studies rely on Kmax and corneal thickness to evaluate the progression of KC. Both Kmax and corneal thickness are local parameters, ie, measure at a point. Thus, they may not be true descriptors of extensive disease-driven remodeling of the entire cornea. Our earlier study showed that not all tomography parameters indicated progression when Kmax increased by 1D.15 Thus, combining all tomography parameters in an AI model provided a more efficient differentiator between local and global progression.15 In this study, more than 91% of the eyes were stable based on both Kmax and parameters evaluated by the AI. However, ~50% of the remaining eyes, which were indicated as progressed based on change in Kmax, were reclassified as stable (or having only local progression) by the AI. Thus, a more refined evaluation of the efficacy of topical application of cyclosporine and trehalose was enabled by the AI. Table 1 showed that overall, the eyes exhibited minimal tomography change over the course of follow-up. This study extended the findings of an earlier study on 20 patients who were topically treated with cyclosporine.28 The study showed that MMP9 levels decreased, and in some eyes, corneal curvature also showed a decrease after 6 months of topical application.28
One of the limitations of this study is the lack of a control group of KC eyes. In a study, more than 80% of the children showed progression when followed longitudinally.29 In another study on adult eyes, 23.4% of the eyes progressed over an average follow-up period of 74.38 ± 42.21 months.30 Progression was more severe in young patients (age from 19 to 24) compared to young adults (age from 25 to 30).30 Interestingly, the progression percentage varied depending on the choice of metric of progression, eg, Kmax and ABC parameters showed a progression proportion of 14.9% and 12%, respectively while E-Staging showed a progression proportion of 16.4% in young adults.30 In this study, the progression proportion was less than 5% and, therefore, indicated an improved clinical outcome compared to Vitamin D and DHA supplementation. Another limitation of this study is the lack of randomized controlled design and inclusion of primarily a young adult population. Future studies need to investigate whether pediatric population can equally benefit with simultaneous application of cyclosporine and trehalose. The impact of these eye drops on the thickness maps of epithelium also needs to be evaluated in future studies. Another avenue of research could be to investigate the anti-inflammatory effects of this combination of eye drops to manage inflammation and adverse responses in KC patients after surgical interventions. Additional limitations of the study include a lack of progression status prior to topical eyedrops, retrospective study design, and heterogenous follow-up due to irregular patient compliance for regular follow-up visits. In some patients, data from both eyes was used as prior inflammation status of the eyes cannot be ascertained by any known clinically approved methods. Hence, we consider this study as a pilot data for future studies with longer follow-up. In summary, simultaneous application of topical cyclosporine and trehalose may provide stable corneal tomography of KC in young adult eyes. A combination of change in Kmax and other parameters evaluated with AI showed that less than 5% of the eyes progressed over the follow-up period.
Acknowledgments
This paper has been uploaded to [Simultaneous topical application of cyclosporine and trehalose appears to keep keratoconus eyes stable: a prospective, longitudinal case series evaluated with artificial intelligence methods] as a preprint: https://www.researchgate.net/publication/396731785_Simultaneous_topical_application_of_cyclosporine_and_trehalose_appears_to_keep_keratoconus_eyes_stable_a_prospective_longitudinal_case_series_evaluated_with_artificial_intelligence_methods.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;41(4):297–8. doi:10.1016/s0039-6257(97)00119-7
2. Lema I, Durán JA. Inflammatory molecules in the tears of patients with keratoconus. Ophthalmology. 2005;112(4):654–659. doi:10.1016/j.ophtha.2004.11.050
3. Balasubramanian SA, Pye DC, Willcox MDP. Effects of eye rubbing on the levels of protease, protease activity and cytokines in tears: relevance to keratoconus. Clin Exp Optom. 2013;96(2):214–218. doi:10.1111/cxo.12038
4. Panigrahi T, Shivakumar S, Shetty R, et al. Trehalose augments autophagy to mitigate stress-induced inflammation in human corneal cells. Ocul Surf. 2019;17(4):699–713. doi:10.1016/j.jtos.2019.08.004
5. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-A–induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. doi:10.1016/s0002-9394(02)02220-1
6. Arnal E, Peris-Martínez C, Menezo JL, Johnsen-Soriano S, Romero FJ. Oxidative stress in keratoconus? Invest Ophthalmol Vis Sci. 2011;52(12):8592–8597. doi:10.1167/iovs.11-7732
7. Kenney MC, Chwa M, Atilano SR, et al. Increased catalase and cathepsin V/L2 but decreased TIMP-1 in keratoconus corneas. Invest Ophthalmol Vis Sci. 2005;46(3):823–829. doi:10.1167/iovs.04-0549
8. Chwa M, Atilano SR, Reddy V, Jordan N, Kim DW, Kenney MC. Increased stress-induced generation of ROS and apoptosis in keratoconus fibroblasts. Invest Ophthalmol Vis Sci. 2006;47:1902–1910. doi:10.1167/iovs.05-0828
9. Iqbal O, Fisher G, Vira S, et al. Increased expression of secreted frizzled-related protein-1 and microtubule-associated protein light chain 3 in keratoconus. Cornea. 2013;32(5):702–707. doi:10.1097/ICO.0b013e318282987a
10. Mizunoe Y, Kobayashi M, Sudo Y, et al. Trehalose protects against oxidative stress by regulating Keap1–Nrf2 and autophagy. Redox Biol. 2018;15:115–124. doi:10.1016/j.redox.2017.09.007
11. Panigrahi T, Shetty R, Shivapriya S, Nelson EJR, Jeyabalan N, Ghosh A. Modulation of inflammation and autophagy pathways by trehalose containing eye drop formulation in corneal epithelial cells: implications for dry eye disease. Can J Biotechnol. 2017;1:145.
12. Elbein AD. New insights on trehalose: a multifunctional molecule. Glycobiology. 2003;13(4):17–27. doi:10.1093/glycob/cwg047
13. Cejka C, Kubinova S, Cejkova J. Trehalose in ophthalmology. Histol Histopathol. 2019;34(6):611–618. doi:10.14670/HH-18-082
14. Matsuo T. Trehalose protects corneal epithelial cells from death by drying. Br J Ophthalmol. 2001;85(5):610–612. doi:10.1136/bjo.85.5.610
15. Shetty R, Kundu G, Narasimhan R, et al. Artificial intelligence efficiently identifies regional differences in the progression of tomographic parameters of keratoconic corneas. J Refract Surg. 2021;37(4):240–248. doi:10.3928/1081597X-20210120-01
16. Matalia H, Narasimhan R, Chinnappaiah N, Kumar V, Sinha Roy A. An interesting case of data gaps in measurement of corneal curvature with Scheimpflug tomography. J Refract Surg. 2020;36(5):350–351. doi:10.3928/1081597X-20200325-02
17. Achiron A, Yahalomi T, Knyazer B, et al. Efficacy comparison of combining cross-linking and refractive laser ablation in progressive keratoconus: systematic review and meta-analysis. Can J Ophthalmol. 2024;59(6):e661–e672. doi:10.1016/j.jcjo.2024.02.017
18. Gindina S, Kang JJ, Jacobs DS. Scleral lenses for correction of irregular astigmatism: advances and limitations. Curr Opin Ophthalmol. 2025;36(4):282–287. doi:10.1097/ICU.0000000000001149
19. Morales P, Durán JA. Advances in Intracorneal Ring Segment (ICRS) implantation for keratoconus: a comprehensive literature review, clinical insights, and future prospects. J Clin Med. 2025;14(13):4454. doi:10.3390/jcm14134454
20. Liu Y, He Y, Deng Y, Wang L. Lenticule addition keratoplasty for the treatment of keratoconus: a systematic review and critical considerations. Indian J Ophthalmol. 2024;72:S167–S175. doi:10.4103/IJO.IJO_695_23
21. Raiskup F, Herber R, Lenk J, Pillunat LE, Spoerl E. Crosslinking with UV-A and riboflavin in progressive keratoconus: from laboratory to clinical practice–Developments over 25 years. Prog Retin Eye Res. 2024;102:101276. doi:10.1016/j.preteyeres.2024.101276
22. Kundu G, Khamar P, Modak D, et al. Simultaneous topography-guided custom ablation with corneal cross-linking for keratoconus: 10-year prospective outcomes. J Refract Surg. 2023;39(11):759–766. doi:10.3928/1081597X-20230926-01
23. Yang K, Tu R, Xu L, et al. Mediating roles of corneal biomechanical and topographic parameters in eye rubbing and keratoconus based on the Chinese keratoconus cohort study. Front Bioeng Biotechnol. 2025;13:1595671. doi:10.3389/fbioe.2025.1595671
24. Shirzadeh E, Shomoossi N, Hasani H. On the urgency of air pollution control to manage chronic eye rubbing and probable risk of keratoconus. J Optom. 2025;18(4):100554. doi:10.1016/j.optom.2025.100554
25. Peris-Martínez C, Piá-Ludeña JV, Rog-Revert MJ, Fernández-López E, Domingo JC. Antioxidant and anti-inflammatory effects of oral supplementation with a highly concentrated Docosahexaenoic Acid (DHA) triglyceride in patients with keratoconus: a randomized controlled preliminary study. Nutrients. 2023;15(5):1300. doi:10.3390/nu15051300
26. Bartolomeo N, Pederzolli M, Palombella S, et al. The effects of Vitamin D on keratoconus progression. Am J Ophthalmol. 2025;276:235–251. doi:10.1016/j.ajo.2025.04.009
27. Aslan MG, Findik H, Okutucu M, et al. Serum 25-Hydroxy Vitamin D, Vitamin B12, and folic acid levels in progressive and nonprogressive keratoconus. Cornea. 2021;40(3):334–341. doi:10.1097/ICO.0000000000002475
28. Shetty R, Ghosh A, Lim R, et al. Elevated expression of matrix metalloproteinase-9 and inflammatory cytokines in keratoconus patients is inhibited by cyclosporine A. Invest Ophthalmol Vis Sci. 2015;56(2):738–750. doi:10.1167/iovs.14-14831
29. Jamali A, Hashemi H, Nabovati P, Khabazkhoob M. Progression and regression of keratoconus in an Iranian population. Sci Rep. 2025;15(1):28525. doi:10.1038/s41598-025-08296-5
30. Kosekahya P, Flockerzi E, Munteanu C, Sideroudi H, Seitz B. Comparison of keratoconus progression rate between adolescents aged 19–24 years and young adults: impact on indication for crosslinking. Curr Eye Res. 2025;50(6):572–578. doi:10.1080/02713683.2025.2470408
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Best Fit Sphere Back and Adjusted Maximum Elevation of Corneal Back Surface as Novel Predictors of Keratoconus Progression
Ribeiro M, Barbosa C, Correia P, Torrão L, Neves Cardoso P, Moreira R, Falcão-Reis F, Falcão M, Pinheiro-Costa J
Clinical Ophthalmology 2022, 16:4239-4248
Published Date: 20 December 2022
The Combined Utilization of Epithelial Thickness Mapping and Tomography in Keratorefractive Surgery Screening: One Imaging Modality is Not Sufficient
Corbin WM, Payne CJ, Momeni-Moghaddam H, Ronquillo YC, Hoopes Snr PC, Moshirfar M
Clinical Ophthalmology 2023, 17:1457-1463
Published Date: 24 May 2023
Influential Factors and Outcome of High-Risk Keratoplasty in a Tertiary Referral Corneal Center: A Retrospective Study
Aschauer J, Klimek M, Donner R, Steiner I, Lammer J, Schmidinger G
Clinical Ophthalmology 2025, 19:653-662
Published Date: 21 February 2025