Back to Journals » Clinical Ophthalmology » Volume 16
Best Fit Sphere Back and Adjusted Maximum Elevation of Corneal Back Surface as Novel Predictors of Keratoconus Progression
Authors Ribeiro M ![]() , Barbosa C, Correia P, Torrão L
, Barbosa C, Correia P, Torrão L ![]() , Neves Cardoso P
, Neves Cardoso P ![]() , Moreira R, Falcão-Reis F, Falcão M
, Moreira R, Falcão-Reis F, Falcão M ![]() , Pinheiro-Costa J
, Pinheiro-Costa J ![]()
Received 16 September 2022
Accepted for publication 6 December 2022
Published 20 December 2022 Volume 2022:16 Pages 4239—4248
DOI https://doi.org/10.2147/OPTH.S388614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Margarida Ribeiro,1,2,* Cláudia Barbosa,3,* Paulo Correia,3 Luís Torrão,1 Pedro Neves Cardoso,1 Raúl Moreira,1 Fernando Falcão-Reis,1,4 Manuel Falcão,1,4 João Pinheiro-Costa1,2
1Department of Ophthalmology, Centro Hospitalar e Universitário São João, Porto, Portugal; 2Department of Biomedicine – Faculty of Medicine of Porto University, Porto, Portugal; 3Faculty of Medicine of Porto University, Porto, Portugal; 4Department of Surgery and Physiology, Faculty of Medicine of Porto University, Porto, Portugal
*These authors contributed equally to this work
Correspondence: Margarida Ribeiro, Department of Ophthalmology, Centro Hospitalar e Universitário São João, Alameda Prof. Hernâni Monteiro Porto, 4200-319, Portugal, Email [email protected]
Purpose: We evaluated the Maximum Elevation of Corneal Back Surface adjusted to the same Best Fit Sphere Back (BFSB) between timeline measurements (AdjEleBmax) and the BFSB radius (BFSBR) itself as new tomographic parameters for documentation of ectasia progression and compare them with the most recent and reliable parameters used on keratoconus (KC) progression.
Results: We evaluated the performance and the ideal cutoff point of Kmax, D-index, posterior radius of curvature from the 3.0 mm centered on the thinnest point (PRC), EleBmax, BFSBR, and AdjEleBmax as isolated parameters to document KC progression (defined as a significant change in two or more variables), we found a sensitivity of 70%, 82%, 79%, 65%, 51%, and 63% and a specificity of 91%, 98%, 80%, 73%, 80%, and 84% to detect KC progression. The area under the curve (AUC) for each variable was 0.822, 0.927, 0.844, 0.690, 0.695, 0.754, respectively.
Conclusion: AdjEleBmax presented a greater specificity, larger AUC, and better performance compared to EleBmax without any adjustment, with similar sensitivity. Although AdjEleBmax and BFSB demonstrated smaller AUC and specificities comparing with Kmax and D-Index, AdjEleBmax still presented a good performance with a reasonable AUC. Since the shape of the posterior surface, more aspheric and curved than the anterior, may facilitate detection of change, we suggest the inclusion of AdjEleBmax in the evaluation of KC progression in conjunction with other variables to increase the reliability of our clinical evaluation and early detection of progression.
Keywords: keratoconus, cornea, progression, best fit sphere back, maximum elevation of corneal back surface
Introduction
Keratoconus (KC) is the most common primary corneal ectasia. Currently, it is considered a bilateral (though asymmetrical) chronic progressive condition, leading to several structural changes with consequent stromal thinning and scarring.1,2 Clinically, patients present irregular astigmatism and myopia, photophobia, and/or monocular diplopia, with impairment of best corrected visual acuity (BCVA) and loss of quality of life.3,4 Manifestation of KC usually starts during the second decade of life, with progression until the fourth decade, followed by clinical stabilization. The risk and rate of progression are higher when younger than 19 years.5,6
Although there is still no curative treatment, the current management of keratoconic eyes aims at two important goals: to improve visual function and to stop ectatic progression.7,8 The former can be achieved with spectacles, rigid or semi-rigid contact lenses, intracorneal rings, or corneal transplant, when the condition is too advanced.9 The latter aim is the holy grail of the management of these patients, which is currently only possible with crosslinking. This procedure leads to an increased biomechanical resistance and stiffness of the cornea and inhibits further progression.10–13 Although it is possible to perform at any stage of the disease, greater benefit is obtained in early stages.14 Efforts should be endorsed to detect early progression and to avoid further deterioration, but also to preclude unnecessary treatments in other patients, decreasing the risk of crosslinking complications such as infections, endothelial cell loss, and severe postoperative pain.15,16
Therefore, the challenge comprises the identification of progression.
Although several studies aimed at defining and detecting progression,17–19 there is still no consistent definition of ectatic progression nor a standardized method to document it.9,20,21 The Global Consensus on Keratoconus and ectatic diseases (2015) defined KC progression by a consistent change in at least two of the following topographic parameters: steepening of the anterior corneal surface; steepening of the posterior corneal surface; thinning and/or an increase in the rate of the corneal thickness change from the periphery to the thinnest point.9 However, a more specific definition of progression is still on demand. Efforts have been made to find the most reliable variables to detect and explain progression.19,22–24
Considering the shape of the posterior corneal surface, more aspheric and curved than the anterior, may facilitate detection of change,25 the main purpose of this study was to evaluate the performance of Maximum Elevation of Corneal Back Surface adjusted to the same Best Fit Sphere Back (BFSB) between timeline measurements (AdjEleBmax) and the BFSB radius (BFSBR) itself as new parameters for documentation of ectasia progression and to compare them with the most common parameters used on KC progression.
Methods
Patient Selection and Data
A total of 113 eyes of 76 consecutive patients diagnosed with keratoconus were examined in this retrospective cohort study in the Department of Ophthalmology at Centro Hospitalar Universitário de São João, Portugal. The study was approved by the local ethics committee of Centro Hospitalar Universitário de São João/Faculdade de Medicina da Universidade do Porto and conducted in accordance with the Helsinki Declaration. A written informed consent was obtained from all individual participants or, if participants were under 16, from a parent and/or legal guardian.
Patients with KC aged from 14 to 30 years old followed in our Ophthalmology Corneal Department were identified and consecutively included between October and December 2021.
All selected patients had more than one year of follow-up by a corneal specialist and at least three Scheimpflug tomography measurements (Pentacam®; Oculus, Wetzlar, Germany). Patients stopped wearing contact lenses at least 48 h prior to measurement. All measurements were performed by trained Orthoptists and only scans with a quality check resulting in “OK” were accepted for inclusion. When the automatic image quality assessment was not labeled with “OK”, the exam was repeated. For progression detection, only two scans per eye were analyzed, with each pair separated by 12±3 months. Eyes with subclinical KC were also included (in these cases, the other eye needed to show clear signs of clinical KC).
We excluded from analysis KC eyes with previous ocular surgery (corneal crosslinking, corneal rings, or corneal transplant) and eyes with very advanced disease (corneal thickness at thinnest point <350 μm, corneal hydrops, or deep corneal scars), as this group consistently failed an “OK” after the internal scan quality check.
Demographic, clinical, and tomographic data were collected for analysis. For detection of KC progression, we collected several tomographic variables, including maximum keratometry (Kmax), mean keratometry (Km), keratometry of flat meridian (K1), keratometry of steepest meridian (K2), corneal astigmatism (Astig = K2 – K1), minimum pachymetry (PachyMin), maximum elevation of corneal back surface (EleBmax), posterior radius of curvature from the 3.0 mm centered on the thinnest point (PRC), Belin/Ambrósio D-Index (D-Index), BFSBR and EleBmax adjusted to the BFSB (AdjEleBmax). As illustrated in Figure 1, the AdjEleBmax was obtained after we defined manually in the machine the same radius of the BFSB in both examinations, using the value of the BFSR of the second evaluation.
 |
Figure 1 Posterior elevation (Elevation Back) comparative maps of Pentacam® images in a case with true clinical progression between examinations spaced 13 months of interval. In panel 1, the EleBmax was 68μm in the first exam and 66μm in the second exam; therefore, according to this parameter, no progression was observed. The best fit sphere radius given automatically by the machine for each evaluation was 5.99mm and 5.90mm, respectively. If we click in the BFS button, a window is showed and it is possible to define manually a new BFS radius. We defined the same radius in both examinations, using the value of the BFS radius of the second measurement (5.90mm). In panel 2, the new value of the EleBmax adjusted to the same BFS between measurements (EleBmaxAdj) was 59μm in the first evaluation, which shows an increase of 7μm in the second evaluation, indicating progression according to our established cutoff of 7μm. |
For progression analysis and to assess the performance of the newly studied variables, we used parameters that are commonly accepted as progression markers (Kmax, Km, K2, Astig, PachyMin, PRC, and D-Index) with described cutoffs in the literature (although not validated). Values representing progression of each analyzed parameter are presented in Table 1. KC progression was defined when at least two of the studied variables confirmed progression.
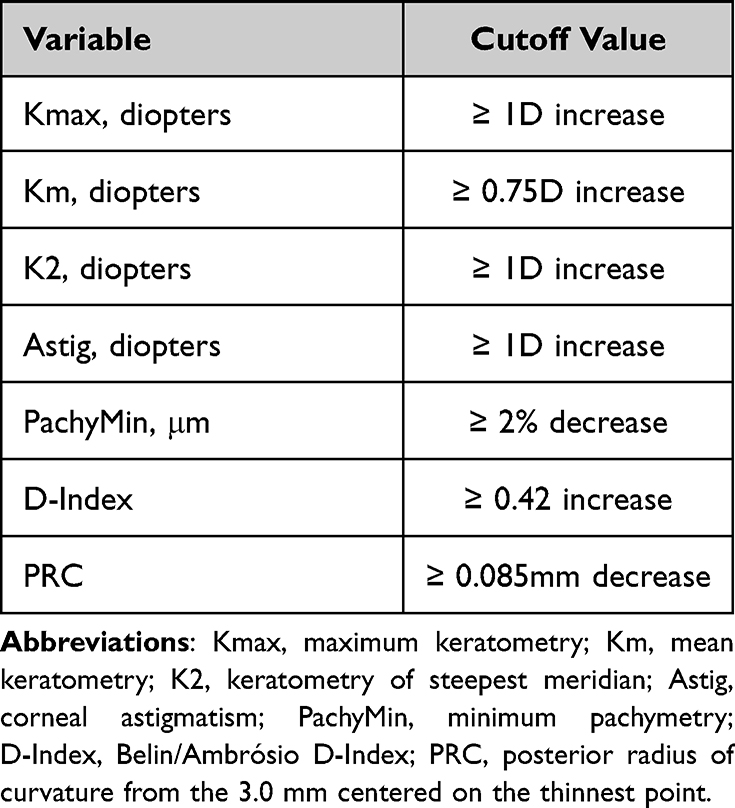 |
Table 1 Tomographic Parameters Commonly Accepted as Progression Markers for KC Progression and Respective Cutoffs Described in the Literature (Although Not Validated) |
In this study, the performance of three variables were tested for detection of progression (EleBmax, BFSB, and AdjEleBmax), taking as reference the existence of progression in at least two other variables. The ideal cutoff points of these variables were calculated and compared with the other variables.
Statistical Analysis
Statistical analysis was performed using the SPSS statistical software (version 27.0 for Mac OS; SPSS Inc., Chicago, IL, USA). The sample’s characteristics were summarized, and data were exposed as counts and proportions for categorical variables. Continuous variables were described as mean and standard deviation (or median and interquartile range, when distributions were skewed). The variation of the keratometric indices was obtained by subtracting the values at baseline from the second measurement (ie a positive delta value indicates an increase in the values of the specific parameter). To evaluate the distribution of keratometric variables across patients classified as progressors or non-progressors, parametric and nonparametric tests were performed, including independent samples t-tests, Mann–Whitney U, Chi-square, and Fisher’s exact tests, as suitable. The statistical significance level was set at 0.05. To assess the performance of Kmax, D-index, PRC, BFSBR, EleBmax, and AdjEleBmax as single predictors of progression, we performed receiver operating characteristic (ROC) curves and calculated the ideal cutoff points, sensitivity, specificity, positive (PPV) and negative predictive values (NPV), and the area under the curve (AUC), taking as reference the classification of progression when at least two variables exceeded the defined thresholds (as previously stated).
Results
A total of 113 eyes of 76 KC patients were included in this study. Most patients were male (n=87, 77%) and mean age at first evaluation was 24.09 ± 3.93 years. Concerning the stratification of KC based on the Belin/Ambrosio enhanced ectasia total deviation value (BAD-D index), the majority (n=68, 60.2%) of eyes were moderate. A cutoff value of 7.0 was selected by investigator consensus and according to literature26 to differentiate mild from moderate keratoconus. However, the rest of the analysis included the entire sample. Demographic, clinical, and tomographic characterization of the sample, including mean average values, minimum, maximum, Standard Deviation (SD), and Confidence Interval at 95% (IC95%) of the measurements, and the difference between the first and the second measurements after 12±3 months can be found in Table 2.
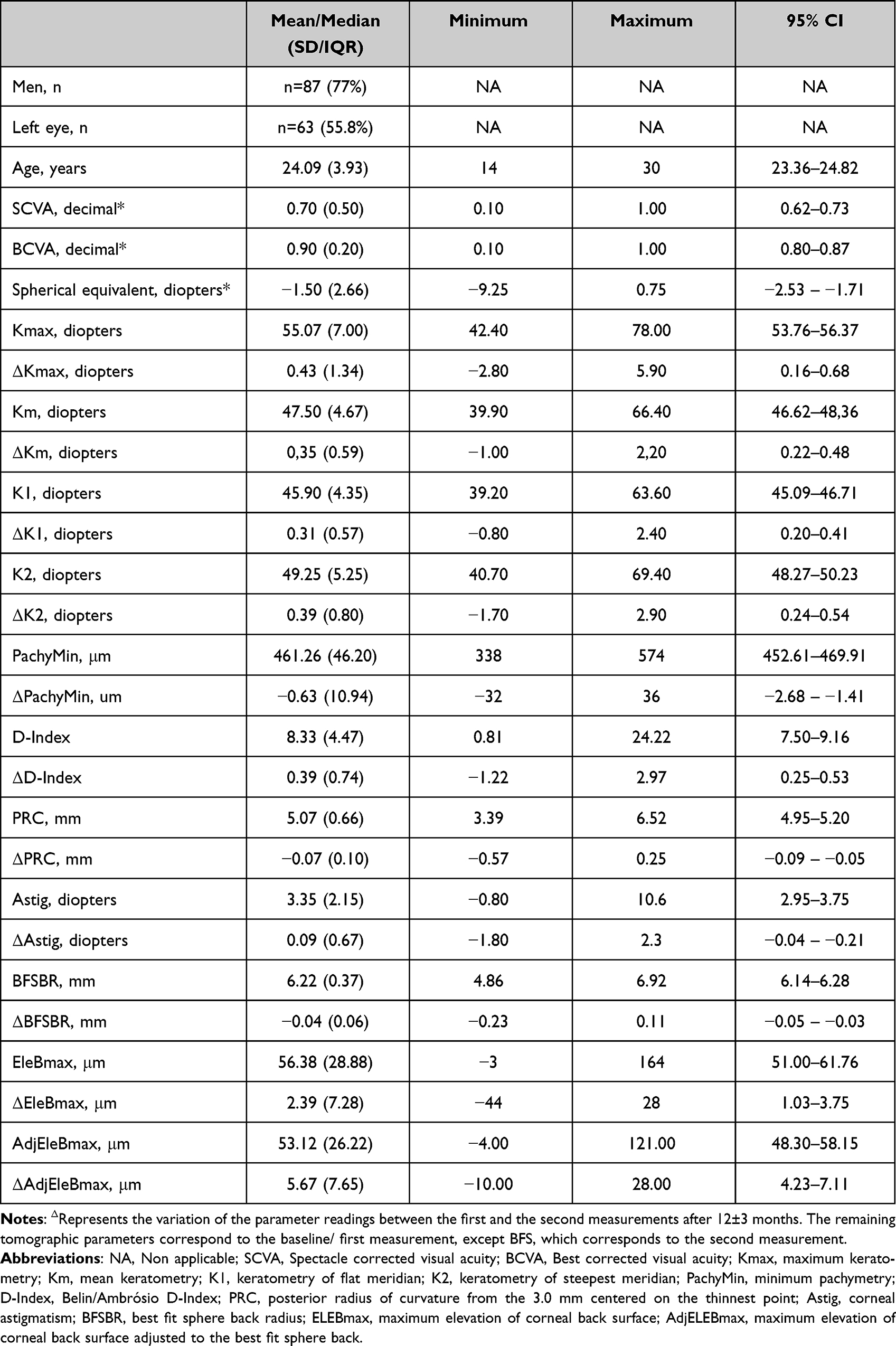 |
Table 2 Demographic, Clinical, and Tomographic Characterization of the Patients. Results Were Expressed as Mean ± SD for Continuous Variables (*results Expressed as Median ± IQR), 95% Confidence Intervals (95% CI), and Male Gender and Right Eyes Were Expressed as Count and Percentage |
Table 3 depicts the number of eyes classified as progressors, considering each tomographic parameter individually (Kmax, Km, K2, Astig, PachyMin, PRC, and D-Index). Considering KC progression defined by change observed in at least two of these tomographic variables, 57 eyes (50.4%) showed progression.
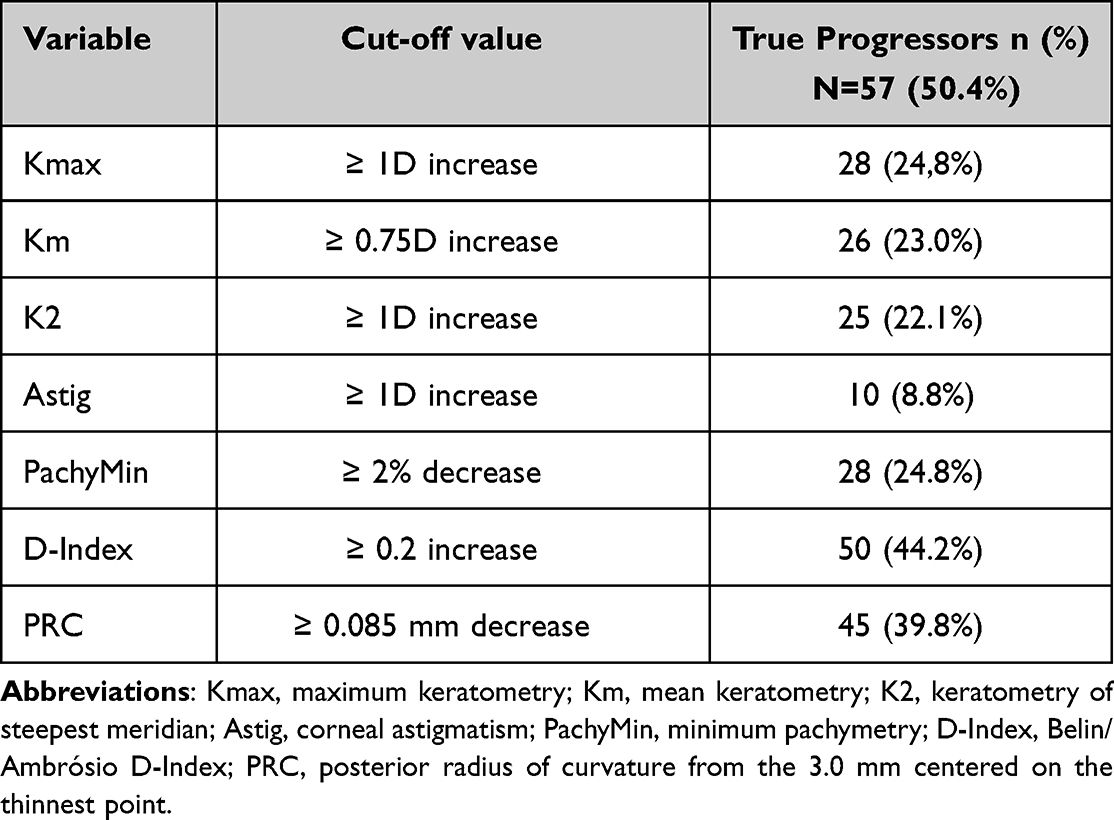 |
Table 3 Number and Frequency of Eyes Classified as Progressors Considering Each Tomographic Parameter Individually |
The performance of Kmax, D-index, PRC, EleBmax, BFSB, and AdjEleBmax as isolated predictors of KC progression are presented in Table 4. As an example, if we define a cutoff of 1 diopter (D) increase in Kmax as a marker of progression, although this parameter presents a sensitivity of 49%, it has a specificity of 100% (all cases identified as progressors by this parameter are in fact true progressors), a positive predictive value (PPV) of 100%, a negative predictive value (NPV) of 66% and an area under the curve (AUC) of 0.822. However, the calculated ideal cutoff point for kmax was 0.4 with a sensitivity of 70%, a specificity of 91%, a PPV of 89%, and a NPV of 75%.
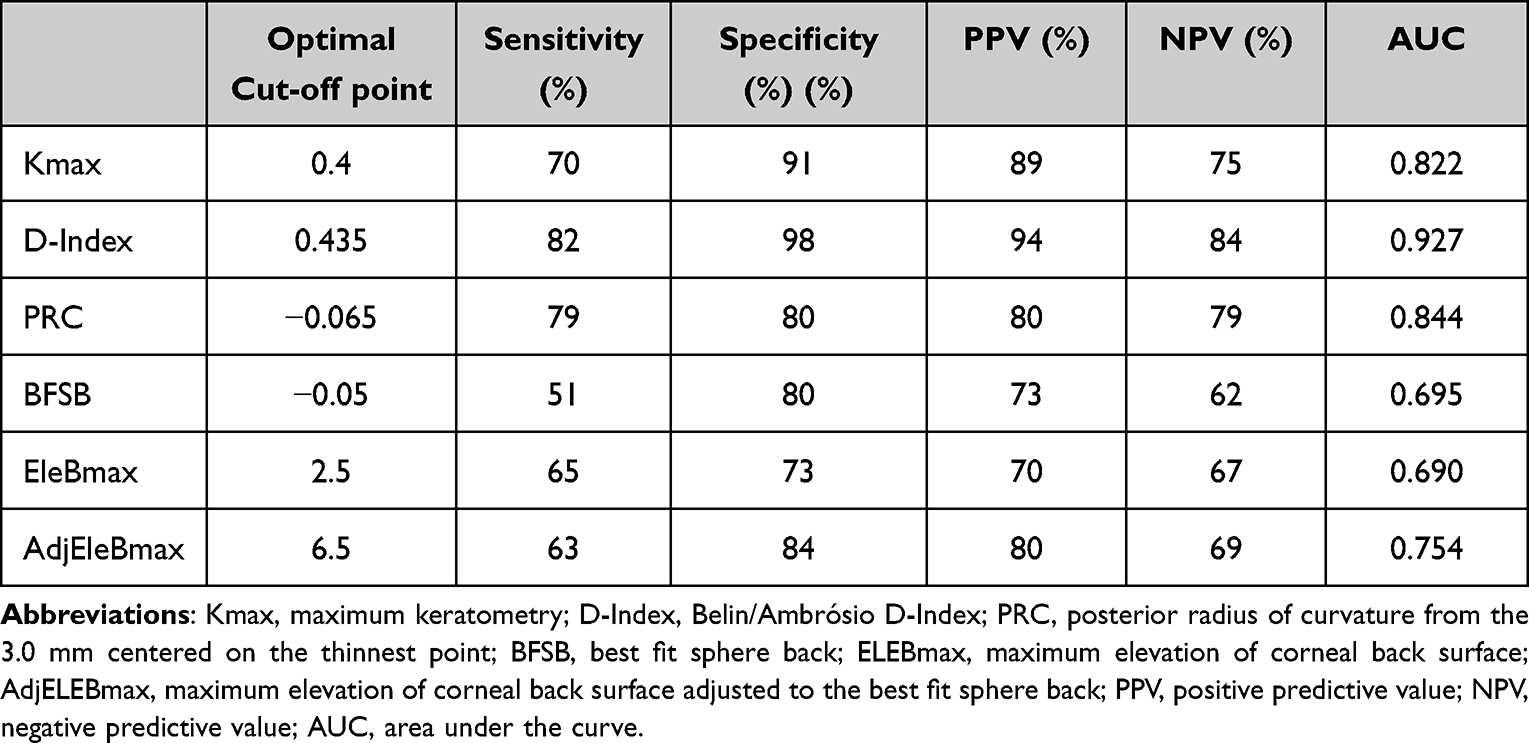 |
Table 4 The Performance of Kmax, D-Index, PRC, BFSB, EleBmax, and AdjEleBmax as Isolated Predictors of KC Progression (Defined as a Significant Change in Two or More Variables) |
As far as the D-Index is concerned, the ideal cutoff point was 0.435, with a sensitivity of 82%, a specificity of 98%, a PPV of 94%, a NPV of 84%, and an AUC of 0.927. We verified that among the 50 eyes that showed progression, only 3 patients did not show progression in 2 or more other parameters. Ten (15.9%) of the 63 eyes that did not progress in D-index showed progression in at least two other parameters.
For PRC, the ideal cutoff for definition of progression was a decrease of 0.065, with a sensitivity of 79%, a specificity of 80%, a PPV of 80%, a NPV of 79%, and an AUC of 0.844.
Regarding the elevation of the posterior surface (EleBmax), the ideal cutoff for definition of progression was an increase of 2.5 um, presenting a sensitivity of 65% and a specificity of 73%. When adjusted to the BSFB of the second measurement, the new parameter AdjEleBmax presented a sensitivity of 63% and a raised specificity of 84% with an ideal cutoff point of 6.5um. The BFSB by itself demonstrated an ideal cutoff of 0.05 mm decrease, with a sensitivity of 51%, and a specificity of 80%.
Figure 2 shows the ROC curves for each evaluated tomographic parameter (Kmax, D-Index, PRC, EleBmax, BFSB, and AdjEleBmax). We observed that D-Index is a test with greater performance, with a larger AUC (0.927), followed by PRC and Kmax. The AUC for EleBmax was 0.690. When adjusted to BFSB, this parameter (AdjEleBmax) improved its performance, enlarging the AUC to 0.754. BFSB by itself showed an AUC of 0.690.
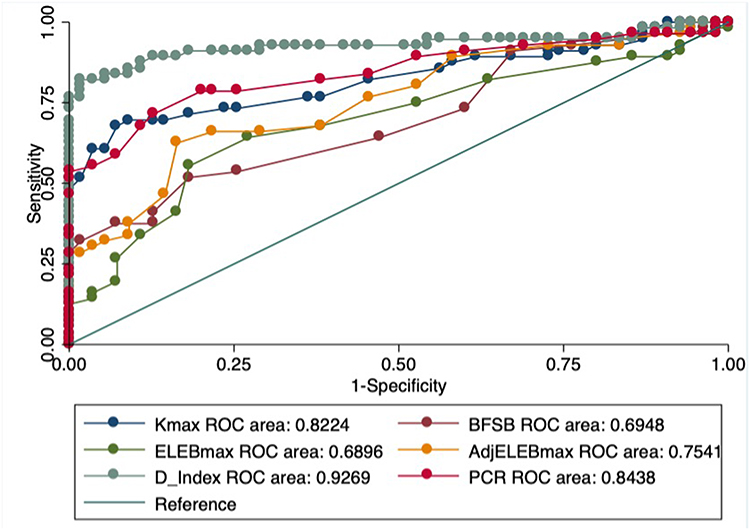 |
Figure 2 Receiver operating characteristic (ROC) curve shows that high sensitivity and specificity levels are achieved with D-Index for determination of keratoconus progression, followed by PRC and Kmax. AdjEleBmax is still considered a reasonable parameter and is generally better than Elebmax without adjustment with BFSB. Abbreviations: Kmax, maximum keratometry; D-Index, Belin/Ambrósio D-Index; PRC, posterior radius of curvature from 3.0 mm centered on the thinnest point; BFSB, best fit sphere back; ELEBmax, maximum elevation of corneal back surface; AdjELEBmax, maximum elevation of corneal back surface adjusted to the best fit sphere back. |
Taking the EleBmax, BFSB, and AdjEleBmax individually into account, we verified that 53 (46.9%), 40 (35.3%), and 45 (39.8%) eyes showed progression according to each isolated parameter, respectively. Within those eyes, 16 (30.2%), 11 (27.5%), and 9 (45%) did not show true progression defined by at least 2 other parameters, respectively. Of the 60 eyes not considered as progressors according to EleBmax, 20 (33%) eyes progressed in 2 or more other parameters. Twenty-eight (38.4%) and 21 (30.9%) eyes considered non-progressors according to BFSB and AdjEleBmax alone showed true progression, respectively.
Discussion
We intended to study the performance of the BFSB and, more importantly, the maximum elevation of corneal back surface adjusted to the BFSB (AdjEleBmax) as new parameters for prediction and detection of KC progression and compare them with other tomographic parameters commonly accepted as progression markers with described cutoffs in the literature (although not validated), namely Kmax and D-Index.20
When adjusting the EleBmax to the BFSB radius (AdjEleBmax), we observed an important increase in the specificity – the non-adjusted parameter with 73% and the adjusted one with a specificity of 84% -, without compromising the value of sensitivity (65% and 63%, respectively). We also evaluated the BFSB radius itself as another potential predictor of ectatic progression. However, this parameter presented lower sensitivity (51% vs 63%), specificity (80% vs 84%), and AUC (0.69 vs 0.75) than AdjEleBmax.
Kmax is a well-known parameter used in predicting KC progression.27 There is no consensus on which cutoff would be more adequate.12,28 In our study, we considered an increase of 1D or more for the definition of progression. With this cutoff, we observed that all patients identified as progressors were confirmed by at least two other parameters, which means a specificity of 100%. However, its sensitivity was relatively low (49%), failing to identify 29 eyes with progression. Even so, in our study, the ideal cutoff for Kmax was 0.4 D, with a sensitivity of 70% and specificity of 91%, which means that with a relative reduction of specificity (from 100% to 91%), we potentiated the sensitivity from 49% to 70%. However, the clinical relevance of this new cutoff is questionable. According to Kreps study of repeatability of Pentacam® measurements, the Kmax showed a repeatability of 0.61 in mild KC and 1.66 in moderate KC,19 meaning that the statistically obtained cutoff in this sample is not clinically relevant, since it would detect as progressive as many stable cases when applicable in other samples. On the other hand, Kmax characterizes the steepest anterior corneal curvature from a small area29 and fails to reproduce changes that occur in other areas of anterior cornea, posterior cornea, and pachymetry.30–32 Compared with the new posterior surface parameter, AdjEleBmax presented a higher sensitivity (63% vs 49%). Twenty progressing eyes were correctly identified with this parameter and missed with Kmax (vs 12 progressors detected with Kmax but not with AdjEleBmax). This finding corroborates the fact that the posterior corneal surface is centrally steeper and more prolate compared to the anterior surface, which may facilitate detection of change.25,32,33
D-Index was the isolated parameter with the highest sensitivity (82%), specificity (95%), and AUC (0.927), in accordance with other studies.34 In fact, it is not surprising since this is a multiparametric index. PRC was the second most sensitive variable (79%), followed by AdjEleBmax (63%). As stated, the higher the sensitivity, the lesser the false negatives and the better the parameter for screening of progression.35 Therefore, we propose AdjEleBmax (with a cutoff for progression of 7um and not 6.5um since the numerical scale integrated in Pentacam® does not include decimal numbers for this parameter), instead of the non-adjusted EleBmax, to be included in the evaluation of keratoconus progression in conjunction with other variables to increase the reliability of our clinical evaluation and early detection of progression.
However, our study faced some limitations. First, we only used tomographic parameters using Scheimpflug imaging for definition and evaluation of progression, but currently there are other technologies for the same purpose, such as biomechanical analysis, that can precede any topographic or tomographic change.36 Second, we used single measurements for all the tested parameters and according to Ivo Guber et al, averaging across several images results in lower level of measurement noise.28 Despite the high repeatability of measurements with Pentacam® among healthy eyes, this is lower in eyes with corneal irregularities and ectasia.37 In this study, we only included eyes with a good quality scan verification integrated in the Pentacam® system, implicating the exclusion of advanced disease.17 Third, we defined true progressors as those with at least two parameters documenting progression according to values described in the literature, but not validated yet. Finally, and perhaps more importantly, the measurement variability of Pentacam® is of clinical relevance when assessing for progression of keratoconus.18,26 Among our sample of 113 eyes, when stratifying according to the BAD-D index, the majority (n=68, 60.2%) of eyes were moderate and the remaining were subclinical or mild. However, we kept the global analysis irrespective of the severity of the KTC, given the small sample. The cutoffs we used were the most suitable for our entire sample, but we admit it will probably increase the noise of the measurements (variability) and raise concerns about the repeatability of the measurements. The repeatability of the measurements depends on the severity of the KTC as demonstrated by Kreps, Gustafsson et al.18,26 Therefore, we strongly recommend that future studies should henceforth take into account the different stages of the disease and evaluate the ideal cutoff points for progression accordingly.
In conclusion, it is of utmost importance to detect early progression in order to endorse a timely management to stop progression (with crosslinking)38 and promote visual preservation and quality of life of our patients.34 The main purpose of our work was to demonstrate that de EleBmax, when adjusted to the same BFS radius between time measurements, has a greater performance than EleBmax itself. This parameter demonstrated a higher specificity and performance compared to EleBmax, it is one of the parameters with the highest sensitivity (and consequentially, better screening performance) and, therefore, it is a potential biomarker of early progression. The creation of multiparametric indexes are highly recommended. Future studies encompassing multiparametric analysis of progression should include AdjEleBmax.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Margarida Ribeiro and Cláudia Barbosa are co-first authors of this study. The authors report no conflicts of interest in this work.
References
1. Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28(4):293–322. doi:10.1016/0039-6257(84)90094-8
2. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. doi:10.1016/S0039-6257(97)00119-7
3. Tambe DS, Ivarsen A, Hjortdal J. Photorefractive keratectomy in keratoconus. Case Rep Ophthalmol. 2015;6(2):260–268. doi:10.1159/000431306
4. Kymes SM, Walline JJ, Zadnik K, Sterling J, Gordon MO; Collaborative Longitudinal Evaluation of Keratoconus Study G. Changes in the quality-of-life of people with keratoconus. Am J Ophthalmol. 2008;145(4):611–617. doi:10.1016/j.ajo.2007.11.017
5. McMahon TT, Edrington TB, Szczotka-Flynn L, Olafsson HE, Davis LJ, Schechtman KB. Longitudinal changes in corneal curvature in keratoconus. Cornea. 2006;25(3):296–305. doi:10.1097/01.ico.0000178728.57435.df
6. Ferdi AC, Nguyen V, Gore DM, Allan BD, Rozema JJ, Watson SL. Keratoconus natural progression: a systematic review and meta-analysis of 11,529 eyes. Ophthalmology. 2019;126(7):935–945. doi:10.1016/j.ophtha.2019.02.029
7. Andreanos KD, Hashemi K, Petrelli M, Droutsas K, Georgalas I, Kymionis GD. Keratoconus treatment algorithm. Ophthalmol Ther. 2017;6(2):245–262. doi:10.1007/s40123-017-0099-1
8. Madeira C, Vasques A, Beato J, et al. Transepithelial accelerated versus conventional corneal collagen crosslinking in patients with keratoconus: a comparative study. Clin Ophthalmol. 2019;13:445–452. doi:10.2147/OPTH.S189183
9. Gomes JA, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359–369. doi:10.1097/ICO.0000000000000408
10. Cunha AM, Sardinha T, Torrão L, Moreira R, Falcão-Reis F, Pinheiro-Costa J. Transepithelial accelerated corneal collagen cross-linking: two-year results. Clin Ophthalmol. 2020;14:2329–2337. doi:10.2147/OPTH.S252940
11. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. doi:10.1016/S0002-9394(02)02220-1
12. O’Brart DP, Chan E, Samaras K, Patel P, Shah SP. A randomised, prospective study to investigate the efficacy of riboflavin/ultraviolet A (370 nm) corneal collagen cross-linkage to halt the progression of keratoconus. Br J Ophthalmol. 2011;95(11):1519–1524. doi:10.1136/bjo.2010.196493
13. Hafezi F, Kling S, Gilardoni F, et al. Individualized corneal cross-linking with riboflavin and UV-A in ultrathin corneas: the sub400 protocol. Am J Ophthalmol. 2021;224:133–142. doi:10.1016/j.ajo.2020.12.011
14. Koller T, Mrochen M, Seiler T. Complication and failure rates after corneal crosslinking. J Cataract Refract Surg. 2009;35(8):1358–1362. doi:10.1016/j.jcrs.2009.03.035
15. Pollhammer M, Cursiefen C. Bacterial keratitis early after corneal crosslinking with riboflavin and ultraviolet-A. J Cataract Refract Surg. 2009;35(3):588–589. doi:10.1016/j.jcrs.2008.09.029
16. Kymionis GD, Portaliou DM, Diakonis VF, Kounis GA, Panagopoulou SI, Grentzelos MA. Corneal collagen cross-linking with riboflavin and ultraviolet-A irradiation in patients with thin corneas. Am J Ophthalmol. 2012;153(1):24–28. doi:10.1016/j.ajo.2011.05.036
17. Cunha AM, Correia PJ, Alves H, et al. Keratoconus enlargement as a predictor of keratoconus progression. Sci Rep. 2021;11(1):21079. doi:10.1038/s41598-021-00649-0
18. Gustafsson I, Bergstrom A, Cardiakides A, Ivarsen A, Hjortdal JO. The interday repeatability of parameters for the assessment of progressive disease in subjects with less advanced keratoconus. Am J Ophthalmol. 2021;225:38–46. doi:10.1016/j.ajo.2020.12.028
19. Jimenez-Garcia M, Kreps EO, Ni Dhubhghaill S, Koppen C, Group RS. Determining the most suitable tomography-based parameters to describe progression in keratoconus. the retrospective digital computer analysis of keratoconus evolution project. Eye Contact Lens. 2021;47(9):486–493. doi:10.1097/ICL.0000000000000800
20. Duncan JK, Belin MW, Borgstrom M. Assessing progression of keratoconus: novel tomographic determinants. Eye Vis. 2016;3:6. doi:10.1186/s40662-016-0038-6
21. Vazirani J, Basu S. Keratoconus: current perspectives. Clin Ophthalmol. 2013;7:2019–2030. doi:10.2147/OPTH.S50119
22. Belin MW, Villavicencio OF, Ambrósio RR
23. Hashemi H, Heirani M, Ambrósio R
24. Pinheiro-Costa J, Correia PJ, Pinto JV, et al. Increased choroidal thickness is not a disease progression marker in keratoconus. Sci Rep. 2020;10(1):19938. doi:10.1038/s41598-020-77122-x
25. Gatinel D, Malet J, Hoang-Xuan T, Azar DT. Corneal elevation topography: best fit sphere, elevation distance, asphericity, toricity, and clinical implications. Cornea. 2011;30(5):508–515. doi:10.1097/ICO.0b013e3181fb4fa7
26. Kreps EO, Jimenez-Garcia M, Issarti I, Claerhout I, Koppen C, Rozema JJ. Repeatability of the pentacam HR in various grades of keratoconus. Am J Ophthalmol. 2020;219:154–162. doi:10.1016/j.ajo.2020.06.013
27. Wittig-Silva C, Chan E, Islam FM, Wu T, Whiting M, Snibson GR. A randomized, controlled trial of corneal collagen cross-linking in progressive keratoconus: three-year results. Ophthalmology. 2014;121(4):812–821. doi:10.1016/j.ophtha.2013.10.028
28. Guber I, McAlinden C, Majo F, Bergin C. Identifying more reliable parameters for the detection of change during the follow-up of mild to moderate keratoconus patients. Eye Vis. 2017;4:24. doi:10.1186/s40662-017-0089-3
29. Epstein RL, Chiu YL, Epstein GL. Pentacam HR criteria for curvature change in keratoconus and postoperative LASIK ectasia. J Refract Surg. 2012;28(12):890–894. doi:10.3928/1081597X-20121115-04
30. Mahmoud AM, Nuñez MX, Blanco C, et al. Expanding the cone location and magnitude index to include corneal thickness and posterior surface information for the detection of keratoconus. Am J Ophthalmol. 2013;156(6):1102–1111. doi:10.1016/j.ajo.2013.07.018
31. Tomidokoro A, Oshika T, Amano S, Higaki S, Maeda N, Miyata K. Changes in anterior and posterior corneal curvatures in keratoconus. Ophthalmology. 2000;107(7):1328–1332. doi:10.1016/S0161-6420(00)00159-7
32. de Sanctis U, Loiacono C, Richiardi L, Turco D, Mutani B, Grignolo FM. Sensitivity and specificity of posterior corneal elevation measured by Pentacam in discriminating keratoconus/subclinical keratoconus. Ophthalmology. 2008;115(9):1534–1539. doi:10.1016/j.ophtha.2008.02.020
33. Choi JA, Kim MS. Progression of keratoconus by longitudinal assessment with corneal topography. Invest Ophthalmol Vis Sci. 2012;53(2):927–935. doi:10.1167/iovs.11-8118
34. Shajari M, Steinwender G, Herrmann K, et al. Evaluation of keratoconus progression. Br J Ophthalmol. 2019;103(4):551–557. doi:10.1136/bjophthalmol-2017-311651
35. Eusebi P. Diagnostic accuracy measures. Cerebrovasc Dis. 2013;36(4):267–272. doi:10.1159/000353863
36. Vinciguerra R, Ambrósio R
37. Wonneberger W, Sterner B, MacLean U, Claesson M, Zetterberg M. Repeated same-day versus single tomography measurements of keratoconic eyes for analysis of disease progression. Cornea. 2018;37(4):474–479. doi:10.1097/ICO.0000000000001513
38. Caporossi A, Mazzotta C, Baiocchi S, Caporossi T, Denaro R. Age-related long-term functional results after riboflavin UV a corneal cross-linking. J Ophthalmol. 2011;2011:608041. doi:10.1155/2011/608041
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Combined Utilization of Epithelial Thickness Mapping and Tomography in Keratorefractive Surgery Screening: One Imaging Modality is Not Sufficient
Corbin WM, Payne CJ, Momeni-Moghaddam H, Ronquillo YC, Hoopes Snr PC, Moshirfar M
Clinical Ophthalmology 2023, 17:1457-1463
Published Date: 24 May 2023
Corneal Tomography Changes After Simultaneous Topical Application of Cyclosporine and Trehalose in Keratoconus Evaluated with an Artificial Intelligence Model
Shetty R, Khamar P, Kundu G, Shetty P, Honniganur D, Shah A, Narasimhan R, Sinha Roy A
Clinical Ophthalmology 2026, 20:619163
Published Date: 15 July 2026