Back to Journals » Journal of Pain Research » Volume 19
Core Acupoint Prescription Patterns for Primary Dysmenorrhea: Data Mining and Network-Based Analysis
Authors Yang T, Guo W, Deng C, Zhang L ![]()
Received 6 November 2025
Accepted for publication 27 February 2026
Published 16 March 2026 Volume 2026:19 579686
DOI https://doi.org/10.2147/JPR.S579686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Tingyuan Yang,1,2 Wanting Guo,3 Chengwen Deng,3 Lei Zhang1,3
1Institute of Acupuncture and Moxibustion, Jianghan University, Wuhan, Hubei, People’s Republic of China; 2First Clinical Medical College, Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China; 3School of Traditional Chinese Medicine, Faculty of Medicine, Jianghan University, Wuhan, Hubei, People’s Republic of China
Correspondence: Lei Zhang, Institute of Acupuncture and Moxibustion, Jianghan University, No. 8 Sanjiaohu Road, Economic & Technological Development Zone, Wuhan, Hubei, 430056, People’s Republic of China, Tel +86 18382284529, Email [email protected]
Objective: To identify core acupoint prescription patterns for primary dysmenorrhea (PD) using data mining and to generate hypothesis-level mechanistic insight through network-based analysis.
Methods: Nine Chinese and English databases were searched from inception to 18 January 2025. Clinical studies of body acupuncture for PD were screened, and acupoint prescriptions were extracted and standardized. Frequency analysis and Apriori association rule mining identified commonly used acupoints and stable cooccurring combinations. Through the use of a network pharmacology-based, hypothesis-generating inference framework, putative bioactive compounds and molecular targets related to the core acupoint combination were derived using STITCH and SwissTargetPrediction, after which a protein–protein interaction (PPI) network was constructed and GO/KEGG enrichment analyses performed to explore the underlying mechanism.
Results: A total of 5993 records were collected; after screening, 177 PD-related articles that produced 291 prescriptions were identified, with 124 unique effective prescriptions involving 66 acupoints included for data analysis. The most frequently used acupoints were Sanyinjiao (SP6), Guanyuan (CV4), and Diji (SP8). Association rule mining supported SP6–CV4–SP8 as a consistent core combination. Network analysis linked this core to 29 active compounds and 640 potential targets, with 94 PD-related targets overlapping. PPI analysis revealed 10 core targets. Enrichment analyses indicated involvement of inflammation, hormone, and pain pathways, especially the PI3K-Akt, cAMP, and AGE-RAGE signaling pathways.
Conclusion: Acupuncture prescriptions for PD showed consistent core acupoint patterns centered on SP6–CV4–SP8. Network-based analyses generated hypothesis-level mechanistic insights, highlighting dominant biological themes related to inflammation, hormonal regulation, and neuroendocrine–immune signaling, with multitarget and multipathway involvement. Interpretations should be made with caution due to heterogeneity in the included studies and the exploratory nature of target/pathway prediction. These findings may help prioritize candidate targets/pathways for experimental verification and inform future trial design and evidence-based optimization of acupuncture prescriptions for PD.
Keywords: primary dysmenorrhea, acupuncture therapy, core acupoint prescriptions, data mining, network acupuncture, mechanism prediction
Introduction
Primary dysmenorrhea (PD) is a gynecological condition that affects mainly women of reproductive age and is characterized by lower abdominal pain during menstruation in the absence of underlying organic pathologies such as endometriosis or adenomyosis, with epidemiological data indicating a prevalence of 45–95% and substantial impacts on physical and mental health.1 The specific cause of PD remains unclear. However, research suggests that this condition could be related to an imbalance in prostaglandin (PG) levels during menstruation in women, thus leading to intense uterine contractions and ischemia, which subsequently provoke pain.2,3 Currently, the main treatment for PD involves nonsteroidal anti-inflammatory drugs (NSAIDs). These drugs function by inhibiting cyclooxygenase enzymes, which reduce PG production. However, long-term use of NSAIDs can cause side effects such as gastrointestinal, liver, and kidney problems.4 Acupuncture has been proposed to alleviate dysmenorrhea through physiological mechanisms, including improving uterine blood flow and modulating PG levels.5 A meta-analysis revealed that acupuncture is notably more effective than NSAIDs in patients with PD because it is safer and has fewer side effects.6 Despite growing evidence that acupuncture may relieve PD symptoms, acupoint prescriptions vary substantially across clinical trials and routine practice, and a reproducible core combination has not been clearly defined. In parallel, proposed biological mechanisms are dispersed across studies, limiting systems-level interpretation and the development of standardized, evidence-informed protocols.
In recent years, only a limited number of studies have applied bioinformatics and network-topology approaches to investigate the use of acupuncture interventions in disease management. These studies have primarily aimed to elucidate the potential mechanistic advantages of acupuncture and to provide a rationale for more targeted acupuncture strategies. To address this gap, we conducted the present study within a network pharmacology framework by constructing an integrative network linking acupoints, molecular targets, and disease-related pathways. Using this approach, we systematically generated hypothesis-level predictions of the potential mechanisms of acupuncture for PD and identified core acupoint prescription patterns, with the goal of informing future evidence-based treatment planning and targeted acupuncture research for this condition.7–9
Methods
Literature Search
A comprehensive literature search was conducted in the following databases from inception through January 18, 2025:These databases included Chinese sources such as the China National Knowledge Infrastructure (CNKI, https://www.cnki.net), Wanfang Data Knowledge Service Platform (Wanfang, http://wanfangdata.com.cn), VIP Information (VIP, http://qikan.cqvip.com/), the Chinese Medical Journals Fulltext Database (CMJFD, http://www.yiigle.com/), and the Chinese Biomedical Literature Database (CBM, http://www.sinomed.ac.cn/). The English-language databases included the Cochrane Library, Embase, PubMed (including PubMed Central, or PMC), and Web of Science.
The search strategy combined subject headings and free-text terms related to PD and acupuncture. The complete database-specific search strategies are provided in the Supplementary Table 1.
Literature Selection Criteria
Inclusion Criteria
The following inclusion criteria were adopted. (1) Study design: Clinical studies reporting specific acupoint prescriptions for PD were included, specifically randomized controlled trials (RCTs) and nonrandomized controlled clinical trials (CCTs) that included a detailed acupuncture protocol. (2) Participants: Patients diagnosed with PD according to established traditional Chinese medicine (TCM) or Western medicine criteria10,11 were included. Pain was not attributable to secondary causes (eg, endometriosis) or other gynecological comorbidities. The minimum sample size was 10 participants per study. (3) Intervention: Eligible interventions were WHO-standardized body acupuncture–related therapies, defined as treatments delivered at standardized body meridian acupoints (WHO nomenclature), with the acupoint prescription explicitly reported. After classifying the included studies according to WHO-standardized acupuncture modalities, we found that manual body acupuncture alone was the most frequently represented intervention type (Figure 1A). Therefore, to ensure methodological consistency and sufficient comparability across studies, only studies using manual body acupuncture as the sole intervention were included in the subsequent analysis of acupoint prescription.12
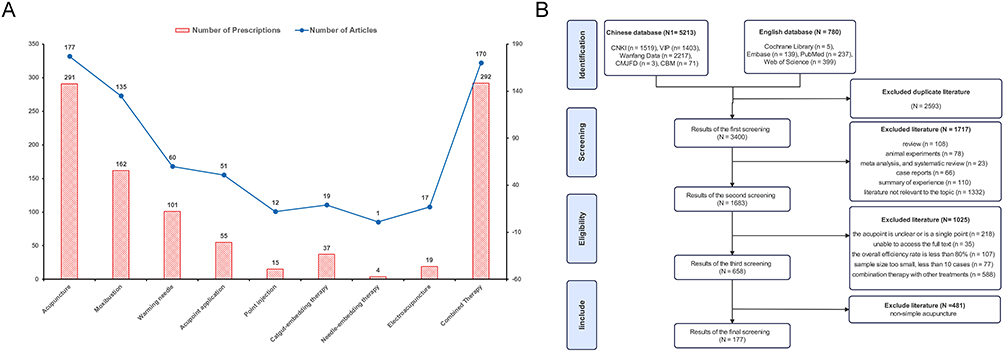 |
Figure 1 (A) represents the distribution of Acupuncture Points and Literature Frequency for Different Acupuncture Treatments. (B) represents the flow chart of literature screening. |
Exclusion Criteria
The following exclusion criteria were employed: (1) Inappropriate literature types: reviews, meta-analyses, theoretical discussions, case reports, animal studies, degree theses, and conference papers. (2) Participant-related exclusions: Studies were excluded if participants were not clearly diagnosed with PD, including unclear or unverifiable diagnostic descriptions, or if the population included secondary dysmenorrhea or major gynecological/medical comorbidities likely to confound pain outcomes (eg, pelvic inflammatory disease). Studies with a total sample size < 10 were also excluded. (3) Intervention-related exclusions: Studies were excluded if the acupuncture intervention did not focus on WHO-standardized body acupoints or if acupuncture was delivered only as an adjunct within a multicomponent regimen in which the independent contribution of acupuncture could not be determined. (4) Outcome-related exclusions: Studies were excluded if outcomes were not primarily related to pain relief or if the overall response rate was < 80%. (5) Publication- and data-related exclusions: Duplicate publications, articles without accessible full texts, or reports with obvious data errors were excluded.
Literature Screening Process
One researcher searched nine databases by using the terms listed in Literature Search and subsequently performed a secondary screening on the basis of the inclusion and exclusion criteria. A second researcher reviewed this process to verify the accuracy of the recorded matches. Any disagreements were resolved through group discussion or by a third researcher.
Database Establishment and Data Processing
Data Extraction and Entry
NoteExpress literature management software was used to deduplicate, categorize, and screen the literature. Studies meeting the inclusion criteria were compiled to create the “Acupuncture Treatment for Primary Dysmenorrhea” database. All of the extracted data were deemed accurate and fully entered into Microsoft Excel (Office 2019) for centralized management. With respect to the acupoint data, classification and extraction followed the descriptions provided in the literature.
Data Standardization
When extracted data are normalized, the acupoint names should first be standardized.13,14 For example, “Jue Gu” should be standardized as “Xuan Zhong”.
Data Classification and Establishment of a New Database
After standardizing the management procedure of the acupoint formula data, we categorized the information on the basis of different acupuncture treatment methods. We carefully reviewed existing studies on various protocols; after recognizing the unique advantages and potential of acupuncture in treating PD, we decided to investigate key acupoint formulas for this condition. This effort aimed to identify common acupoint combinations and their typical clinical applications for managing this disorder. Through the use of an established literature review and data processing techniques, we created a new thematic database denoted “Acupuncture Treatment for Primary Dysmenorrhea” to support further research.
Data Mining Analysis
After duplicate entries from the “Acupuncture Treatment for Primary Dysmenorrhea” database were removed, the data were imported into R. The itemFrequency function was used to analyze how often each acupoint appeared and to explore frequency distributions. Through the use of the arules and arulesViz packages, association rule mining was performed using the Apriori algorithm to identify frequently cooccurring acupoint combinations for PD. The minimum support was set to 15%, the minimum confidence was set to 80%, and the maximum antecedent length was set to 2. Rules with lift values > 1 were considered to indicate positive associations. To examine the stability of patterns, networks were visualized at support thresholds of 15%, 20%, and 30%. This process helped to identify the most common acupoint combinations and extract key acupoint prescriptions.
Core Acupoint Formula Target Identification and Database Construction
Identification of Active Substances and Database Establishment
Searches were performed within the databases described in Literature Search by utilizing acupoint names from core formulas, disease names, and keywords such as “experiment”, “molecule”, and “mechanism” (Supplementary Table 2). The search included the period from the inception of each database to February 22, 2025. Databases were created to catalog active substances linked to each core acupoint formula and their effects. The following inclusion criteria were adopted: (1) Study acupoints: research should involve at least one acupoint from the core formula (without combining noncore acupoints), and any treatments beyond acupuncture should be excluded. (2) Study type: animal experimental studies or human clinical trials were utilized. (3) Target disease: animal studies should focus on dysmenorrhea models, whereas human trials should target PD without other conditions. (4) Outcome measures: the active substance should be clearly identified, with results demonstrating statistical significance.
Identification of Active Substance-Related Targets
To systematically identify targets linked to the active substances responsible for the effects of core acupoint formulas, we used a multidatabase analysis approach. First, we obtained standardized names and SMILES codes for these active substances from PubChem (https://pubchem.ncbi.nlm.nih.gov/). Afterward, we predicted the targets of these compounds using SwissTargetPrediction (http://www.swisstargetprediction.ch/) and STITCH (http://stitch.embl.de/cgi/), with the species set to “Homo sapiens”. We applied screening criteria of “probability > 0” and “combined score > 0.4” to ensure that the selected targets were reliably predicted. The results from both databases were combined and deduplicated to create a comprehensive list of targets for the active compounds.
Acquisition of Potential Disease Targets
Disease targets were obtained from the Genecards (https://www.genecards.org), OMIM (https://www.omim.org/), and DisGeNET (https://www.disgenet.com) databases by using “primary dysmenorrhea”. These results were merged and deduplicated to create a list of PD-related targets. A Venn diagram was subsequently generated by using the online tool Venny 2.1 (https://bioinfogp.cnb.csic.es/tools/venny/index.html) to compare acupoint targets with PD targets. The overlapping targets that were identified through this process were considered potential targets for the core acupoint formula in the treatment of PD.
Construction of the Core Target Interaction Network
The intersecting targets were imported into the STRING 12.0 database (https://cn.string-db.org); moreover, the species was assigned to “Homo sapiens”, and the confidence threshold was 0.4. The disconnected targets were hidden, and the data were exported as a “tsv” file. This file was imported into Cytoscape 3.10.1. Afterward, Cytoscape 3.10.1 was used to visualize the “Core Formula Active Substance Target-PD” network. This network displays the key acupoints in core formulas, the active substances linked to these formulas, and the intersection targets between acupoints and disease targets, thereby illustrating their relationships through a topological network.
Construction of Protein‒Protein Interaction (PPI) Networks
The intersection targets between the core formula and PD were input into the STRING 12.0 database (https://cn.string-db.org/). The species were limited to “Homo sapiens”, with a “minimum required interaction score” greater than 0.4. After the protein interaction network was analyzed, the resulting TSV file from the STRING database was downloaded and imported into Cytoscape 3.10.1 to construct a protein interaction network diagram. Moreover, CentiScape 2.2 was used to calculate topological parameters for each target node, including betweenness centrality, closeness centrality, degree centrality, eigenvector centrality, and radiality. Targets with parameter values equal to or above the median were considered potential core targets for Xuefang’s treatment of PD.
Gene Ontology (GO) and KEGG Pathway Enrichment Analyses
The intersection of acupoint targets and disease targets was imported into the DAVID database (https://davidbioinformatics.nih.gov) for GO and KEGG pathway enrichment analyses. The “OFFICIAL_GENE_SYMBOL” was used as the symbol identifier, with the species set to “Homo sapiens”. The analyses included GOTERM BP DIRECT, GOTERM CC DIRECT, GOTERM MF DIRECT, and KEGG PATHWAY approaches, with the results being downloaded after each analysis. Pathways were filtered for a P value < 0.05 and ranked according to gene ratios, with the top 15 pathways being selected. The Bioinformatics Online Platform (https://www.bioinformatics.com.cn/) was used to visualize these pathways and create charts.
Results
Literature Search and Screening Results
This study initially retrieved 5,993 articles related to Chinese and foreign literature from nine databases. After rigorous screening on the basis of the inclusion and exclusion criteria, 658 articles were selected for further review. These articles were then categorized according to different acupuncture treatments, with detailed records of the number of acupoint combinations and corresponding literature counts being determined for each protocol (Figure 1A). The analysis revealed that acupuncture was the most commonly used treatment, followed by moxibustion. For PD, 177 articles were identified, resulting in 291 acupoint prescriptions. After duplicates were removed, 124 effective prescriptions involving 66 unique acupoints were included. The detailed screening process is illustrated in Figure 1B. (The cited literature and relevant prescription information can be found in Supplementary Table 3).
Analysis of Acupoint Usage Frequency and Distribution
In this study, 124 acupuncture prescriptions, with each prescription averaging 5–6 acupoints, were analyzed, resulting in a total of 650 occurrences. Seventeen acupoints were used more than 10 times, which accounted for 82.46% of all the uses. The details are shown in Table 1. The three most commonly used acupoints included Sanyinjiao (SP6), Guanyuan (CV4), and Diji (SP8), with each demonstrating a usage rate of more than 42.74%. Sanyinjiao (SP6) had the highest frequency, at 76.61%.
 |
Table 1 High-Frequency Acupoints for Treating Primary Dysmenorrhea (Frequency≥10) |
Association Rule Analysis Results
Association rule mining revealed 17 frequently cooccurring acupoint combinations for PD acupuncture treatment (Table 2). All the identified rules had a lift value > 1, indicating positive associations among the acupoints. Network visualizations at different support thresholds are shown in Figure 2. With a support of 15%, the network contained multiple common combinations with several peripheral acupoints (Figure 2A). When the support increased to 20%, the overall pattern became clearer, with Sanyinjiao (SP6) emerging as a central node that was strongly associated with multiple acupoints (Figure 2B). At 30% support, fewer peripheral acupoints remained, and the combinations appeared more stable, highlighting Sanyinjiao (SP6), Guanyuan (CV4), and Diji (SP8) as a core cooccurring group (Figure 2C).
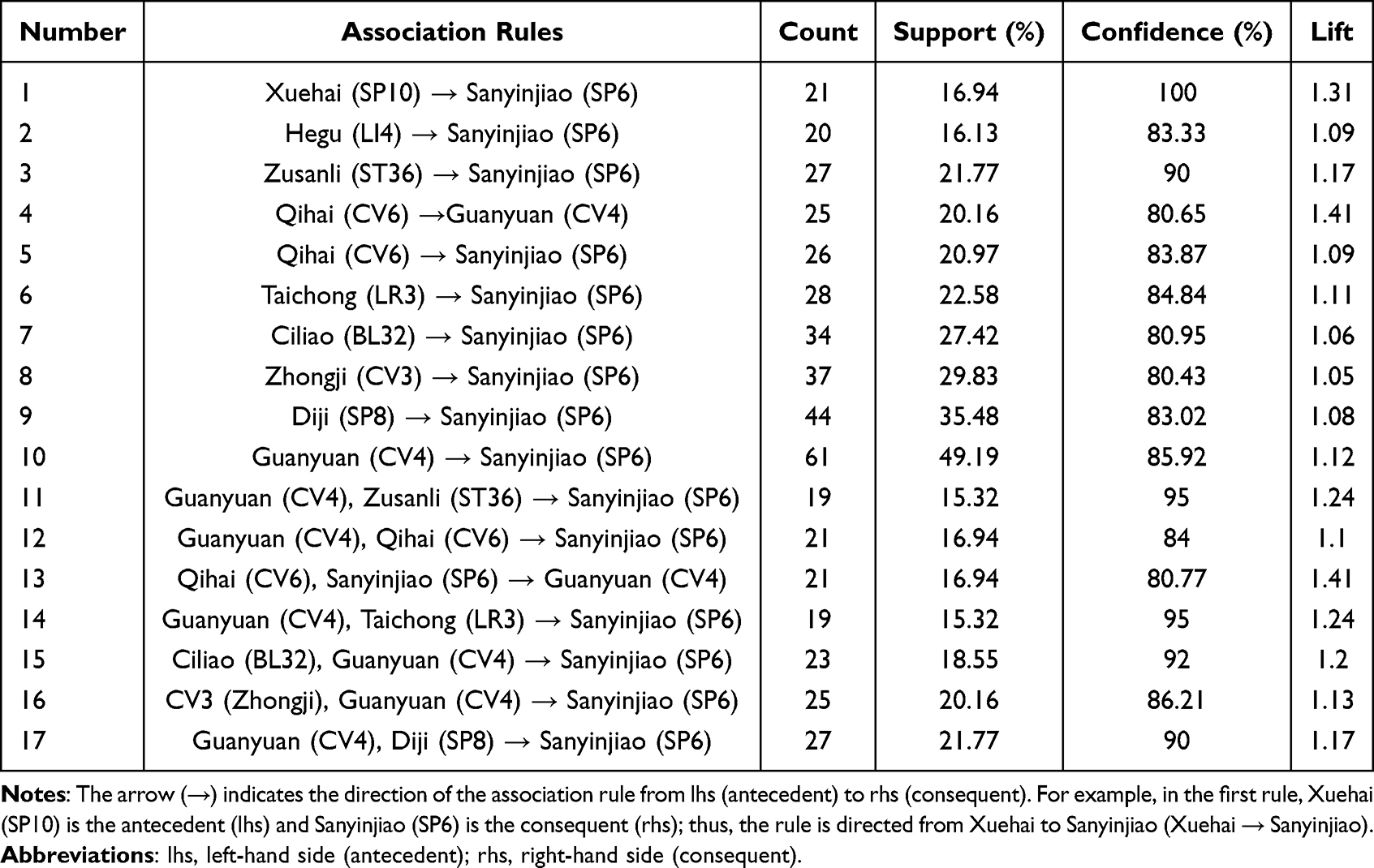 |
Table 2 Analysis of Association Rules for Acupoint Prescription |
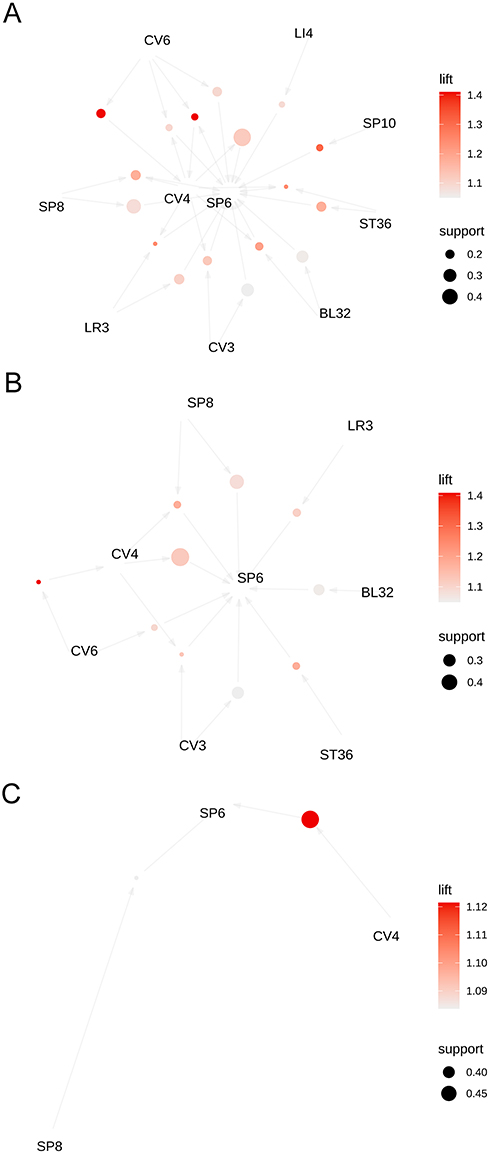 |
Figure 2 Acupuncture treatment for primary dysmenorrhea: bubble chart of high-frequency acupoint association rules and core formula diagram; larger bubbles indicate higher support, and darker colors show greater lift; arrows denote the support direction; more common acupoint combinations suggest higher occurrence rates. (A) Support = 15%, Confidence = 80%; (B) Support = 20%, Confidence = 80%; (C) Support = 30%, Confidence = 80%. |
Identification of Potential Target Molecules for Core Acupoint Formulas
In Core Acupoint Formula Target Identification and Database Construction, we conducted a second-round literature search. After screening nine databases, an initial search revealed 262 articles in both the Chinese literature and the foreign literature. Following a review process, 19 articles that met the inclusion criteria were selected (The information of the included literatures can be found in the Supplementary Table 4). After duplicates were removed, these articles included a total of 29 active substances, as indicated in Table 3. The literature coverage of the acupoints was as follows: Sanyinjiao (SP6) appeared in 17 articles, Guanyuan (CV4) appeared in 6 articles, and Diji (SP8) appeared in 2 articles. The number of active substances linked to each acupoint was 29 for Sanyinjiao (SP6), 10 for Guanyuan (CV4), and 5 for Diji (SP8). After collating, calibrating, and removing duplicate targets, 640 potential targets were identified, thereby representing the possible action targets of the core acupoint formula.
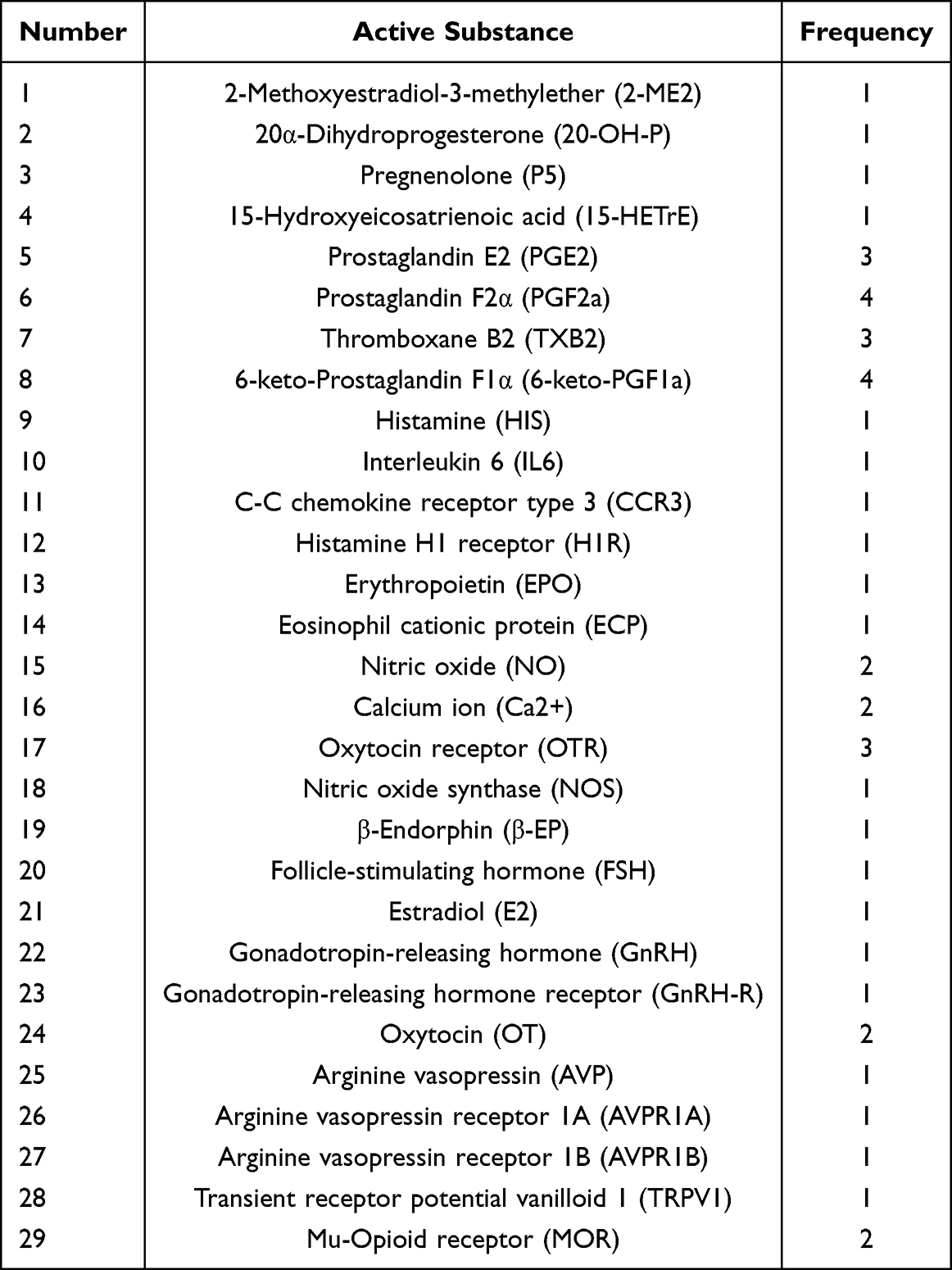 |
Table 3 Frequency Statistics of Active Substances Targeted by Core Acupoints |
Screening of Additional Potential Targets for Core Acupoint Formulas in Primary Dysmenorrhea Treatment
Through the use of the GeneCards database, 294 targets related to PD were identified. These targets were combined with 453 targets from the OMIM database and 29 from Disgenet. After duplicates were removed, 760 PD targets were observed. The overlap between these targets and the 640 targets obtained from the core acupoint formula was subsequently determined (Figure 3A), resulting in 94 potential targets for the acupuncture intervention, which represented 7.2% of all the targets. Cytoscape 3.10.1 software was used to develop the “Core Formula Active Substance Intersection Target Primary Dysmenorrhea” network (Figure 3B).
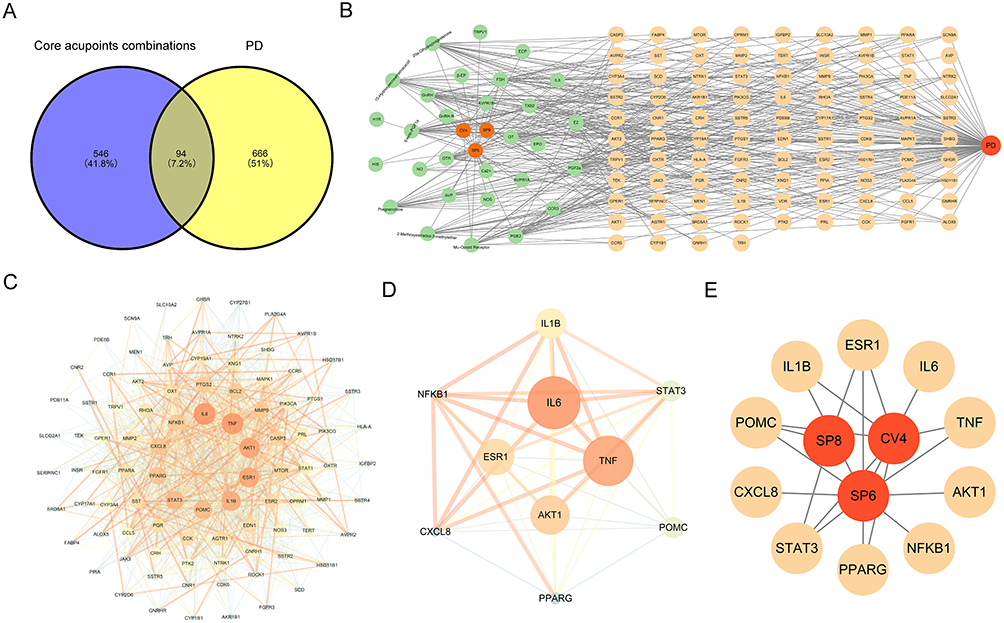 |
Figure 3 (A) represents the Venn diagram of core prescription targets and primary dysmenorrhea targets. (B) represents the “Core Prescription-Active Ingredients-Intersecting Targets-Primary Dysmenorrhea” network diagram. (C) represents PPI network of core acupoint prescription in treating primary dysmenorrhea. (D) represents network visualization of core targets. (E) represents the “Core Prescription-Targets-Primary Dysmenorrhea” network diagram. |
Protein–Protein Interaction Network Analysis
The target intersections were added to the STRING database, with the “Homo sapiens” setting utilized for the protein‒protein interaction (PPI) analysis. The establishment of a “minimum required interaction score” above 0.4 resulted in a network with 94 nodes, 1094 edges, and an average node degree of 23. Afterward, CentiScape 2.2 was used to analyze the network’s topological properties, including betweenness, closeness, degree, eigenvector, and radiality centralities (Table 4). An optimized PPI network diagram was then created (Figure 3C). By using the median values of these indices as cutoffs, ten core targets were identified (Figure 3D). In this figure, darker colors and larger node areas indicate higher degree values. The top five core genes (ranked according to degree) included interleukin 6 (IL6), tumor necrosis factor (TNF), AKT serine/threonine kinase 1 (AKT1), estrogen receptor 1 (ESR1), and interleukin 1β (IL1B). With the use of Cytoscape 3.10.1, the frequencies of the key acupoints and core targets were visualized in a network diagram, as shown in Figure 3E.
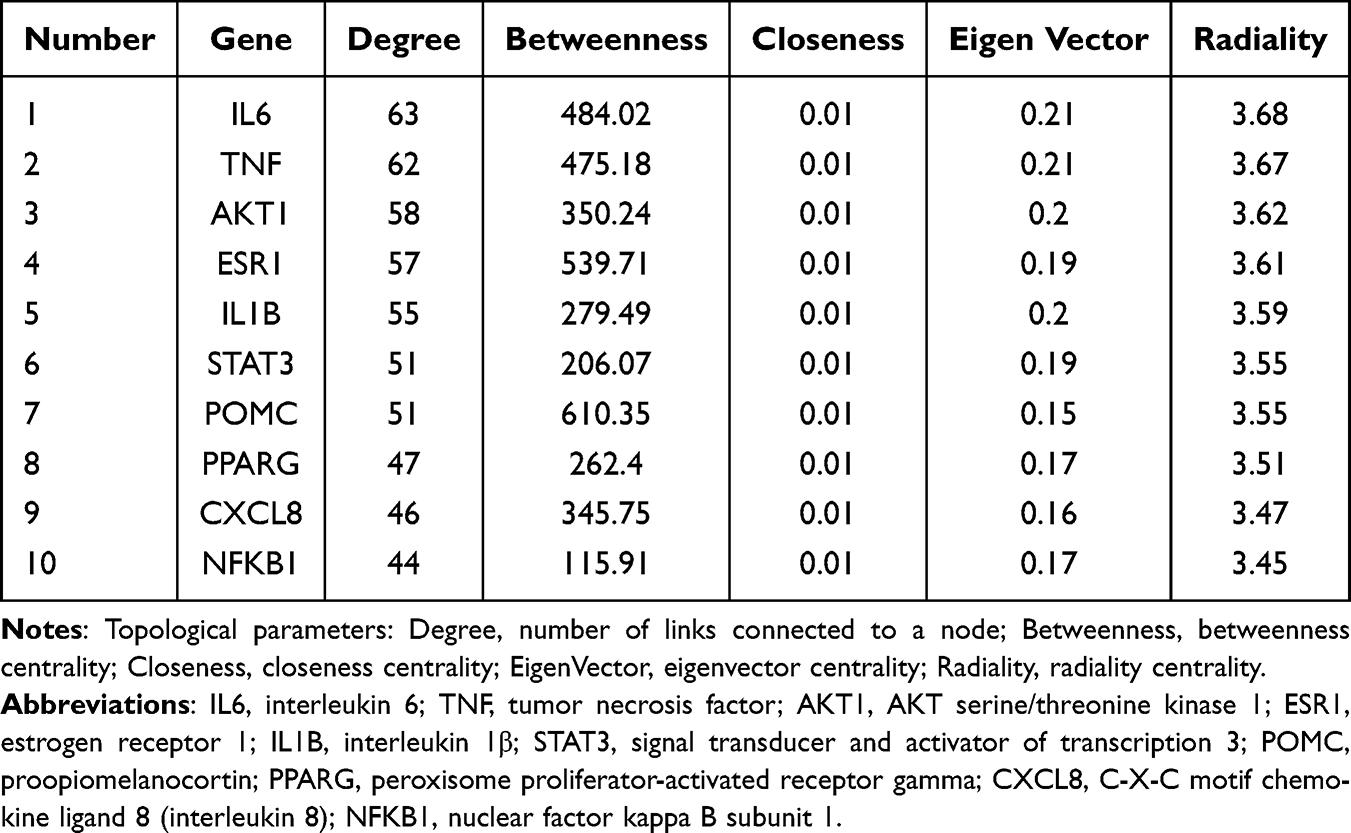 |
Table 4 Topological Parameters of Intersection Targets (Top 10 in Degree) |
GO Functional Enrichment and KEGG Pathway Enrichment Analysis
Bioinformatics analysis of the 94 intersecting target points was performed using the DAVID database to explore the potential mechanisms underlying core acupoints in the treatment of PD. GO analysis revealed 619 entries, comprising 462 biological process (BP), 43 cellular component (CC), and 114 molecular function (MF) categories. The top 15 enriched genes for the BP, CC, and MF categories were primarily associated with the inflammatory response, as well as increased cell proliferation, oxidoreductase activity, and DNA-binding transcription factor activity (Figure 4A). KEGG analysis revealed 149 pathways. The top 15 pathways (ranked according to the gene ratios) were visualized using a bar chart, which included pathways such as the PI3K-Akt signaling pathway, cAMP signaling pathway, and AGE-RAGE signaling pathway, as shown in Figure 4B.
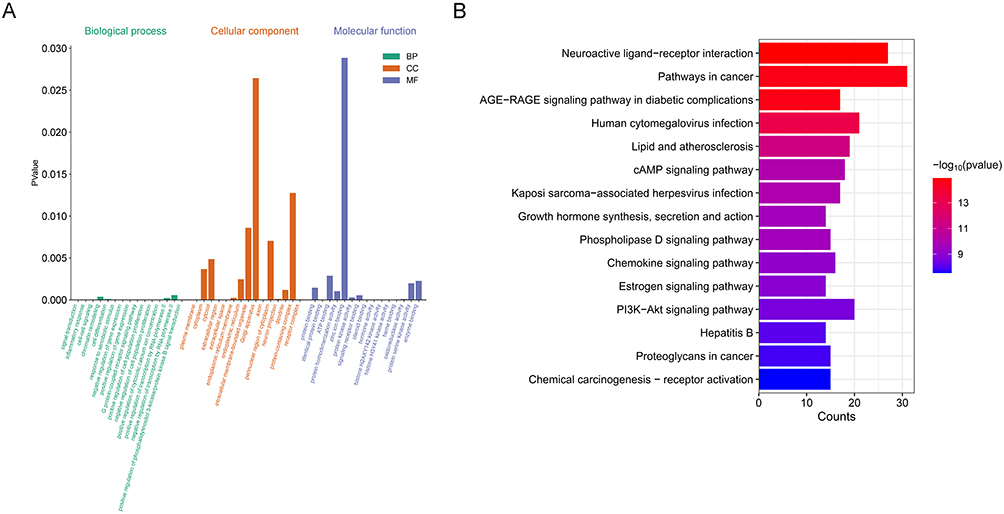 |
Figure 4 (A) represents the GO enrichment analysis of core acupoint prescription in treating primary dysmenorrhea. (B) represents the KEGG pathway enrichment analysis of core acupoint prescription in treating primary dysmenorrhea (Top 15). |
Discussion
PD is a common gynecological issue that is characterized mainly by cramping uterine pain during menstruation. This discomfort can extend to the thighs and calves and is often associated with symptoms such as nausea, vomiting, abdominal pain, and diarrhea.15,16 Research has demonstrated that acupuncture and moxibustion can safely and effectively reduce menstrual cramps.17,18 The mechanism of this technique may involve the regulation of estrogen and inflammatory cytokine levels, which helps to maintain the balance of the neuroendocrine-immune system. This scenario correspondingly reduces inflammatory responses, enhances uterine microcirculation, and alleviates lower abdominal pain.19 Acupuncture treatment for PD offers benefits such as easy administration and minimal side effects.20,21 Therefore, acupuncture treatment is highly valuable for managing this condition in clinical settings and provides useful guidance for healthcare practice.
This study analyzed 124 acupuncture prescriptions, highlighting 17 acupoints that were used at least 10 times, which together accounted for 82.46% of the total use. These findings support the targeted selection of acupoints for treating PD. The most frequently used acupoints were Sanyinjiao (SP6), Guanyuan (CV4), and Diji (SP8). Additionally, association rule analysis with the Apriori algorithm revealed a strong connection among these three acupoints. Sanyinjiao (SP6) is widely used in the management of gynecological pain conditions. Experimental studies have suggested that deep need at Sanyinjiao (SP6) may engage endogenous analgesic systems in a dysmenorrhea model, including the activation of descending pain modulatory pathways and increased release of analgesia-related mediators, thereby alleviating pain responses.22,23 Guanyuan (CV4), located on the anterior midline of the lower abdomen, is frequently selected for pelvic and reproductive symptoms. From a biomedical perspective, stimulation at CV4 may influence pelvic autonomic regulation, uterine contractility, and local perfusion, which are relevant to pain generation in PD. A controlled trial reported that the combination of Sanyinjiao (SP6), Guanyuan (CV4), and Diji (SP8) was associated with significant symptom improvement in patients with PD after a defined treatment course.24 Diji (SP8) has also been investigated for dysmenorrhea management; a randomized controlled trial reported that needling at SP8 and nearby tender points resulted in symptom improvement over 2–3 months in female university students.25 Consistent with prior clinical and experimental findings, our data mining revealed Sanyinjiao (SP6)–Guanyuan (CV4)–Diji (SP8) as a core cooccurring acupoint combination for PD. The collective evidence suggests that the effects of this combination may involve central/peripheral pain modulation, neuroendocrine regulation, inflammatory/prostaglandin-related pathways, and improved uterine perfusion, but these mechanisms remain hypothesis-generating and require further experimental validation.26–29
In this study, a network acupuncture methodology was applied to investigate how core acupuncture point prescriptions can treat PD. By predicting relevant target points and constructing a PPI network, we identified ten key target points that are primarily associated with the therapeutic effects of the core acupoint formula on PD. These genes are ranked as follows: IL6, TNF, AKT1, ESR1, IL1B, STAT3, POMC, PPARG, CXCL8, and NFKB1. Notably, IL6 is a multifunctional cytokine30 that serves as a vital link between the physiological processes of the menstrual cycle and pathological pain and inflammation. As a potent inflammatory mediator, IL6 activates inflammatory signaling pathways (such as the JAK/STAT and NF-κB pathways), enhances inflammatory responses, and increases the production of prostaglandins (PGs). This process leads to uterine smooth muscle contractions, spasms, and ischemia, which further intensify contractions and pain.31,32 TNF is a proinflammatory cytokine that is produced mainly by activated immune cells, including macrophages and T cells.33 TNF-α acts as a key initiator in the main inflammatory pathway of dysmenorrhea. Specifically, it increases cyclooxygenase-2 (COX-2) expression, which enhances PG production and the release of inflammatory mediators, thereby orchestrating local uterine inflammation and pain sensitization.34–36 AKT1 (also known as protein kinase B or PKB) plays a vital role in the PI3K/AKT/mTOR pathway, whereby it responds to various stimuli (such as estrogen and inflammatory cytokines) to control cell growth, survival, metabolism, blood vessel formation, and inflammation. Ultimately, it promotes uterine smooth muscle contraction, ischemia, and pain perception.37–39 ESR1 plays a vital role in female estrogen signaling and is a member of the nuclear receptor family that performs both ligand-activated and transcription factor functions. When estradiol binds to ESR1, it initiates the transcription of various target genes, such as COX-2, the progesterone receptor, and other inflammatory mediators. This process supports endometrial angiogenesis and promotes conditions that facilitate the release of PGs and inflammatory factors during menstruation.40,41 These aforementioned core targets function together in the development of PD in women and involve pathways such as inflammatory responses, hormone signaling interactions, and pain sensitization. This initial discovery highlights possible mechanisms underlying the effectiveness of acupuncture, thereby guiding future research into this disease.
A thorough analysis of the GO and KEGG enrichment results revealed that the core acupoint prescription for treating PD involves several key signaling pathways, including the AGE-RAGE, cAMP, phospholipase D, chemokine, estrogen, and PI3K-Akt pathways. The AGE-RAGE pathway primarily promotes inflammation and oxidative stress. When AGEs bind to RAGE, they activate transcription factors such as NF-κB, which then trigger the release of proinflammatory cytokines such as IL6 and TNF-α. This process can worsen local inflammation in the uterus and lead to increased production of pain-causing substances such as PGs.42,43 PGs are a primary cause of uterine smooth muscle spasms and pain. Therefore, blockage of their synthesis and release can decrease uterine inflammation and help to ease pain.3 The main function of the cAMP signaling pathway is to relax uterine smooth muscle and alleviate pain. This pathway primarily functions by increasing cAMP levels, which inhibit myosin light chain kinase activity, thereby causing muscle relaxation. Many medications that are used to treat dysmenorrhea (such as β2-adrenergic agonists) function by increasing cAMP levels.44,45 The main role of the phospholipase D (PLD) signaling pathway is to facilitate the production and release of inflammatory cytokines from immune cells. Specifically, this pathway aims to hydrolyze membrane phospholipids to produce phosphatidic acid and diacylglycerol, which then activate downstream pathways, such as the mTOR pathway. These signals help to regulate the expression of inflammatory mediators. In PD, PLD can be triggered by inflammatory signals, thus potentially intensifying the inflammatory response; moreover, blockage of this activity may reduce pain transmission.46–48 Additionally, the estrogen signaling pathway activates the downstream PI3K-Akt pathway via the ESR1, which then regulates the expression of key inflammatory mediators, such as TNF-α and IL6. This process leads to increased PG production, ultimately causing menstrual abdominal pain in women.3,49 Together, these six signaling pathways form a complex, interconnected network involved in the pathophysiology of PD that regulates uterine inflammation, contractions, and pain perception. Therefore, we can conclude that PD is essentially a locally inflammatory and painful condition driven by hormonal control that involves multiple pathways.
Limitations
This study has several limitations. First, the inclusion of both Chinese and English publications may introduce language bias. Additionally, the quality of the included studies varied, with some studies demonstrating methodological issues such as limited scientific rigor in randomized controlled trials or a lack of blinding, which could affect the reliability of our results. Second, the key identified mechanisms are based on bioinformatics predictions and network analysis without validation from in vitro experiments; therefore, these mechanisms remain theoretical and require further laboratory testing. Finally, PD is characterized by different traditional Chinese medicine syndromes. Although this study focused on core acupoint formulas for PD, it did not analyze acupoint–target–pathway interactions across various syndromes. As a result, our conclusions are somewhat general and require more precise follow-up research. Future validation should include large-scale, multicenter clinical trials and detailed mechanistic studies to accurately elucidate the mechanisms by which acupuncture functions in PD.
Conclusion
In this study, data mining revealed SP6–CV4–SP8 as a reproducible core acupoint combination across 124 prescriptions for PD. Network acupuncture analysis further highlighted a set of candidate targets and pathways related to inflammation, hormone regulation, and pain signaling, providing testable mechanistic hypotheses for future validation. Overall, our findings support a data-driven basis for prioritizing acupoint combinations and guiding subsequent experimental and clinical research in PD.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Ethics Approval and Consent to Participate
Not applicable. This study is a secondary analysis based on publicly available published literature and does not involve any new direct participation of human subjects or animal experiments. Therefore, ethical approval from an institutional review board and individual consent to participate were not required for this research.
Disclosure
The authors declare no competing interests in this work.
References
1. Proctor M, Farquhar C. Diagnosis and management of dysmenorrhoea. BMJ. 2006;332:1134–14. doi:10.1136/bmj.332.7550.1134
2. Guimarães I, Póvoa AM. Primary dysmenorrhea: assessment and treatment. Rev Bras Ginecol Obstet. 2020;42:501–507. doi:10.1055/s-0040-1712131
3. Iacovides S, Avidon I, Baker FC. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update. 2015;21:762–778. doi:10.1093/humupd/dmv039
4. Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2015;2015:CD001751. doi:10.1002/14651858.CD001751.pub3
5. Afshari Fard MR, Mohammadi A, Ma LX, et al. Comparison of the immediate analgesic effect of perpendicular needling and transverse needling at SP6 in patients with primary dysmenorrhea: study protocol for a randomized controlled trial. Medicine. 2020;99:e18847. doi:10.1097/MD.0000000000018847
6. Yang J, Xiong J, Yuan T, et al. Effectiveness and safety of acupuncture and moxibustion for primary dysmenorrhea: an overview of systematic reviews and meta-analyses. Evid Based Complement Alternat Med. 2020;2020:8306165. doi:10.1155/2020/8306165
7. Ong SS, Tang T, Xu L, et al. Research on the mechanism of core acupoints in electroacupuncture for functional constipation based on data mining and network acupuncture. Front Med. 2024;11:1482066. doi:10.3389/fmed.2024.1482066
8. Li F, Liu Z, Xu Y, et al. Potential mechanisms of acupuncture treatment for rheumatoid arthritis: a study based on network topology and machine learning. Chin Med. 2025;20:164. doi:10.1186/s13020-025-01209-8
9. Han Z, Zhang Y, Wang P, Tang Q, Zhang K. Is acupuncture effective in the treatment of COVID-19 related symptoms? Based on bioinformatics/network topology strategy. Brief Bioinform. 2021;22:bbab110. doi:10.1093/bib/bbab110
10. Liang X, Song Y. Diagnostic and therapeutic criteria for traditional Chinese medicine: primary dysmenorrhea (Revised). Chin J Tradit Chin Med Pharm. 2024;39:1884–1887.
11. Burnett M, Lemyre M. No. 345-primary dysmenorrhea consensus guideline. J Obstet Gynaecol Can. 2017;39:585–595. doi:10.1016/j.jogc.2016.12.023
12. WHO standard acupuncture point locations in the Western Pacific Region. World Health Organization; 2008.
13. State Administration for Market Regulation, Administration of the People’s Republic of China. Nomencla - ture and location of extra points in common use: GB/T 40997-2021. Beijing: Standards Press of China; 2021 [Cited September 21, 2025]. Available from: https://openstd.samr.gov.cn/bzgk/gb/newGbInfo?hcno=D2AEF8AD07C0150E19859079579EF99F.
14. State Administration for Market Regulation, Administration of the People’s Republic of China. Nomencla - ture and location of Meridian points: GB/T 12346-2021. Beijing: Standards Press of China; 2021 [Cited September 21, 2025]. Available from: https://openstd.samr.gov.cn/bzgk/gb/newGbInfo?hcno=397548AE7248D3D87DD15E0AB8107185&refer=outter.
15. Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstet Gynecol. 2006;108:428–441. doi:10.1097/01.AOG.0000230214.26638.0c
16. Banikarim C, Chacko MR, Kelder SH. Prevalence and impact of dysmenorrhea on hispanic female adolescents. Arch Pediatr Adolesc Med. 2000;154:1226–1229. doi:10.1001/archpedi.154.12.1226
17. Xu Y, Zhao W, Li T, et al. Effects of acupoint-stimulation for the treatment of primary dysmenorrhoea compared with NSAIDs: a systematic review and meta-analysis of 19 RCTs. BMC Complement Altern Med. 2017;17:436. doi:10.1186/s12906-017-1924-8
18. Chen B, Liu S, Jin F, et al. Efficacy of acupuncture-related therapy in the treatment of primary dysmenorrhea: a network meta-analysis of randomized controlled trials. Heliyon. 2024:10:e30912. doi:10.1016/j.heliyon.2024.e30912
19. Yu WY, Ma LX, Zhang Z, et al. Acupuncture for primary dysmenorrhea: a potential mechanism from an anti-inflammatory perspective. Evid-Based Complement Altern Med: Ecam. 2021;2021:1907009. doi:10.1155/2021/1907009
20. Shen X, Xia J, Adams C. Acupuncture for schizophrenia. Schizophr Bull. 2014;40:1198–1199. doi:10.1093/schbul/sbu135
21. Xu M, Yang C, Nian T, et al. Adverse effects associated with acupuncture therapies: an evidence mapping from 535 systematic reviews. Chin Med. 2023;18:38. doi:10.1186/s13020-023-00743-7
22. Lin C, Zhang L, Ma L. Characteristics of SP6 immediate analgesic effect in treating primary dysmenorrhea. Scientia Sinica(Vitae). 2016;46:1015–1022. doi:10.1360/N052016-00030
23. Song Y, Ma L, Gan Y. Effects of perpendicular needling and transverse needling at Sanyinjiao (SP6) on oxytocinand its receptor in dysmenorrhea rats with cold stagnation syndrome. Chin J Tradit Chin Med. 2020;35:2046–2049.
24. Smith CA, Crowther CA, Petrucco O, Beilby J, Dent H. Acupuncture to treat primary dysmenorrhea in women: a randomized controlled trial. Evid Based Complement Altern Med. 2011;2011:612464. doi:10.1093/ecam/nep239
25. Sun Y, Hou X, Wu J, Tian HF, Zhao JP. Acupuncture treatment of primary dysmenorrhea by needling acupoints of the spleen meridian with positive reactions: a randomized controlled clinical trial. Zhen Ci Yan Jiu. 2018;43(5):307–310. doi:10.13702/j.1000-0607.170989
26. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85:355–375. doi:10.1016/j.pneurobio.2008.05.004
27. Jie S, Yaoli Y, Hongxiao LI, et al. Effect of moxibustion on expression profile of miRNAs in Tripterygium glycoside-induced decreased ovarian reserve. J Tradit Chin Med. 2024;44:745–752. doi:10.19852/j.cnki.jtcm.2024.04.002
28. Qu F, Li R, Sun W, et al. Use of electroacupuncture and transcutaneous electrical acupoint stimulation in reproductive medicine: a group consensus. J Zhejiang Univ Sci B. 2017;18:186–193. doi:10.1631/jzus.B1600437
29. Jin X, Zhang Y, Chang B, et al. Analgesic effect of “zhibian” (BL54)-toward-”shuidao” (ST28) needling technique of acupuncture on primary dysmenorrhea based on NOD1/RIP2/NF-κB signaling pathway in the rats. Zhongguo Zhen Jiu. 2025;45:209–216. doi:10.13703/j.0255-2930.20240331-k0001
30. Soler MF, Abaurrea A, Azcoaga P, Araujo AM, Caffarel MM. New perspectives in cancer immunotherapy: targeting IL-6 cytokine family. J Immuno Ther Cancer. 2023;11e007530. doi:10.1136/jitc-2023-007530
31. Li J, Xiao Y, Yu H, Jin X, Fan S, Liu W. Mutual connected IL-6, EGFR and LIN28/Let7-related mechanisms modulate PD-L1 and IGF upregulation in HNSCC using immunotherapy. Front Oncol. 2023;13:1140133. doi:10.3389/fonc.2023.1140133
32. Leimert KB, Verstraeten BSE, Messer A, et al. Cooperative effects of sequential PGF2α and IL-1β on IL-6 and COX-2 expression in human myometrial cells†. Biol Reprod. 2019;100:1370–1385. doi:10.1093/biolre/ioz029
33. Körner H, McMorran B, Schlüter D, Fromm P. The role of TNF in parasitic diseases: still more questions than answers. Int J Parasitol. 2010;40:879–888. doi:10.1016/j.ijpara.2010.03.011
34. Yoo J, Rodriguez Perez CE, Nie W, Sinnett-Smith J, Rozengurt E. TNF-α and LPA promote synergistic expression of COX-2 in human colonic myofibroblasts: role of LPA-mediated transactivation of upregulated EGFR. BMC Gastroenterol. 2013;13:90. doi:10.1186/1471-230X-13-90
35. Andrade P, Visser-Vandewalle V, Hoffmann C, Steinbusch HW, Daemen MA, Hoogland G. Role of TNF-alpha during central sensitization in preclinical studies. Neurol Sci. 2011;32:757–771. doi:10.1007/s10072-011-0599-z
36. Zhang L, Berta T, Xu ZZ, Liu T, Park JY, Ji RR. TNF-α contributes to spinal cord synaptic plasticity and inflammatory pain: distinct role of TNF receptor subtypes 1 and 2. Pain. 2011;152:419–427. doi:10.1016/j.pain.2010.11.014
37. Edlind MP, Hsieh AC. PI3K-AKT-mTOR signaling in prostate cancer progression and androgen deprivation therapy resistance. Asian J Androl. 2014;16:378–386. doi:10.4103/1008-682X.122876
38. Browne IM, Okines AFC. Resistance to targeted inhibitors of the PI3K/AKT/mTOR pathway in advanced oestrogen-receptor-positive breast cancer. Cancers. 2024;16:2259. doi:10.3390/cancers16122259
39. Yin X, Pavone ME, Lu Z, Wei J, Kim JJ. Increased activation of the PI3K/AKT pathway compromises decidualization of stromal cells from endometriosis. J Clin Endocrinol Metab. 2012;97:E35–43. doi:10.1210/jc.2011-1527
40. Yaşar P, Ayaz G, User SD, Güpür G, Muyan M. Molecular mechanism of estrogen-estrogen receptor signaling. Reprod Med Biol. 2016;16:4–20. doi:10.1002/rmb2.12006
41. Hewitt SC, Wu SP, Wang T, et al. The estrogen receptor α cistrome in human endometrium and epithelial organoids. Endocrinology. 2022;163:bqac116. doi:10.1210/endocr/bqac116
42. Dong H, Zhang Y, Huang Y, Deng H. Pathophysiology of RAGE in inflammatory diseases. Front Immunol. 2022;13:931473. doi:10.3389/fimmu.2022.931473
43. Balistreri CR, Candore G, Accardi G, Colonna-Romano G, Lio D. NF-κB pathway activators as potential ageing biomarkers: targets for new therapeutic strategies. Immun Ageing. 2013;10:24. doi:10.1186/1742-4933-10-24
44. Yuan W, López Bernal A. Cyclic AMP signalling pathways in the regulation of uterine relaxation. BMC Pregnancy Childbirth. 2007;7(1):S10. doi:10.1186/1471-2393-7-S1-S10
45. Fedorowicz Z, Nasser M, Jagannath VA, Beaman JH, Ejaz K, van Zuuren EJ. Beta2-adrenoceptor agonists for dysmenorrhoea. Cochrane Database Syst Rev. 2012;2012:CD008585. doi:10.1002/14651858.CD008585.pub2
46. Gomez-Cambronero J. New concepts in phospholipase D signaling in inflammation and cancer. Scientific World J. 2010;10:1356–1369. doi:10.1100/tsw.2010.116
47. Frondorf K, Henkels KM, Frohman MA, Gomez-Cambronero J. Phosphatidic acid is a leukocyte chemoattractant that acts through S6 kinase signaling. J Biol Chem. 2010;285:15837–15847. doi:10.1074/jbc.M109.070524
48. Zhu L, Jones C, Zhang G. The role of phospholipase C signaling in macrophage-mediated inflammatory response. J Immunol Res. 2018;2018:5201759. doi:10.1155/2018/5201759
49. Pedram A, Razandi M, Aitkenhead M, Hughes CC, Levin ER. Integration of the non-genomic and genomic actions of estrogen. Membrane-initiated signaling by steroid to transcription and cell biology. J Biol Chem. 2002;277:50768–50775. doi:10.1074/jbc.M210106200
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Bibliometric Analysis of Acupuncture Therapy in the Treatment of Primary Dysmenorrhea from 2001 to 2021
Zhu D, Xiao Y, Zhong G, Wei X, Wu J, Chen R, Jiao L
Journal of Pain Research 2022, 15:3043-3057
Published Date: 27 September 2022
Mechanistic Insights into Acupuncture for Chronic Prostatitis/Chronic Pelvic Pain Syndrome via Integrated Network Topology and Bioinformatics Analysis
Liang C, Wang H, Chang H, Liu M, Wang F
Journal of Pain Research 2026, 19:592476
Published Date: 17 April 2026