Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Construction of a Nomogram Prediction Model for Individualized Prediction of the Risk of Non Suicidal Self Injury in Adolescent Depression Patients
Authors Zhao Q, Zeng L, Hu S, Lei F
Received 18 July 2025
Accepted for publication 18 November 2025
Published 3 December 2025 Volume 2025:21 Pages 2747—2758
DOI https://doi.org/10.2147/NDT.S549935
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Qingyan Zhao,1 Lingbin Zeng,2 Shaolun Hu,3 Fenfang Lei1
1School of Nursing of Shaoyang University, Shaoyang, Hunan, 422000, People’s Republic of China; 2Institute office of Shaoyang Brain Hospital, Shaoyang, Hunan, 422000, People’s Republic of China; 3The Psychiatric Clinic of Shaoyang Brain Hospital, Shaoyang, Hunan, 422000, People’s Republic of China
Correspondence: Fenfang Lei, School of nursing of Shaoyang University, Qiliping, Xueyuan Road, Daxiang District, Shaoyang, Hunan, 422000, People’s Republic of China, Tel +8615115981926, Email [email protected]
Objective: To develop a nomogram model for individualized prediction of non-suicidal self-injury (NSSI) risk in adolescent depression patients.
Methods: Clinical data from 270 adolescent depression patients (August 2022–January 2025) were randomly divided into modeling and validation groups. The modeling group was split into NSSI and non-NSSI subgroups based on NSSI occurrence. Logistic regression identified risk factors. R software was used to construct the nomogram, while ROC and DCA evaluated its discrimination and clinical utility.
Results: A total of 189 patients from our hospital were retrospectively selected, among whom 72 patients (38.10%) were identified as having engaged in NSSI behavior within the past year. Disease duration, depression level, childhood abuse, family dysfunction, school bullying, sleep disorder, and Barratt Impulsiveness were significant risk factors (P< 0.05). AUCs were 0.899 (modeling) and 0.954 (validation). H-L tests showed good fit: χ²=7.243 (P=0.721) and χ²=7.010 (P=0.711). The DCA curve indicated high clinical value when probability ranged from 0.05 to 0.97.
Conclusion: Disease course, severity of depression, childhood abuse, dysfunctional family environment during childhood, experiences of school bullying, sleep disorders, and Barratt Impulsiveness Scale scores were identified as influencing factors for NSSI in adolescents with depression. Based on these factors, a nomogram model was constructed, which showed good predictive consistency and high clinical applicability. This model can assist clinicians in identifying high-risk individuals for early prevention. Although the model may help guide interventions to reduce the incidence of NSSI, further validation through rigorously designed implementation studies is still required.
Keywords: teenagers, depression, non suicidal self injury, risk factors, nomogram
Introduction
Adolescence is a critical period for both physical and mental development. During this stage, adolescents’ psychology is fragile and sensitive, making them prone to depression, which is a mental disorder characterized by high prevalence, recurrence, and rates of self-harm and suicide. It mainly manifests as low mood, loss of interest, and fatigue, often accompanied by anxiety and sleep disorders during episodes, with each episode lasting more than two weeks, thereby affecting adolescents’ physical and mental health.1,2 Emotions are relatively unstable during adolescence, and depression may further increase emotional volatility, sometimes leading to extreme behaviors to relieve such emotions. Non-suicidal self-injury (NSSI) refers to intentional bodily harm without suicidal intent, commonly seen among adolescents as a way to escape problems and resolve distress. Studies have found that depression is closely associated with NSSI, with approximately 44.8% of patients with depression exhibiting NSSI behaviors. The etiology and mechanisms of NSSI are complex. As adolescents’ nervous systems are not yet fully developed, they tend to be emotionally unstable, impulsive, and have difficulty communicating, which makes them more prone to risky behaviors. Factors such as emotional instability, low self-esteem, childhood abuse, and internet addiction are all associated with NSSI. The occurrence of NSSI among adolescents with depression has become a serious public health concern, hindering their physical and mental well-being and increasing the social burden.3–5 Therefore, it is necessary for clinical practice to identify the factors influencing NSSI in adolescents and carry out targeted interventions to prevent self-injury. A nomogram prediction model can transform the influencing factors identified through multivariate logistic regression into easy-to-understand visual graphs, enabling clinicians to calculate the value of each variable and thus evaluate the incidence of adverse events.6,7 At present, most studies focus on analyzing the influencing factors of NSSI risk in adolescents with depression. Research has found that sleep disorders, depression, and behavioral factors are the main factors affecting the suicide risk of adolescent psychiatric inpatients,8 but these studies cannot screen or predict high-risk individuals. Currently, there is limited research on nomogram prediction modelsin this field. Hence, this study aims to investigate the construction of a nomogram prediction model to individually predict the risk of NSSI in adolescents with depression.
Materials and Methods
General Data
Clinical data of 270 adolescents with depression who were admitted to our hospital from August 2022 to January 2025 were collected. The sample size was calculated using PASS 15 software (two-sided test, with α = 0.05, power = 80%, and d = 0.50). The total required sample size was 251 cases, and considering a 10% dropout rate, a total of 270 patients were finally included. They were randomly divided into a modeling group (189 patients) and a validation group (81 patients) in a 7:3 ratio (random number table method). Based on whether NSSI occurred in the past year, the modeling group was further divided into an NSSI group and a non-NSSI group. The flowchart of case collection is shown in Figure 1. Inclusion criteria: (1) Meeting the diagnostic criteria for depression;9 (2) All patients were adolescents; (3) First onset; (4) 12 ≤ age < 18 years; (5) Complete clinical data. Exclusion criteria: (1) Other mental disorders; (2) Organic brain diseases; (3) Patients with major organ failure; (4) History of drug abuse; (5) Hearing impairment; (6) Severe self-injury. Dropout criteria: (1) participants who withdraw midway; (2) participants who are transferred to another hospital for treatment. This study was approved by the Ethics Committee of our hospital.
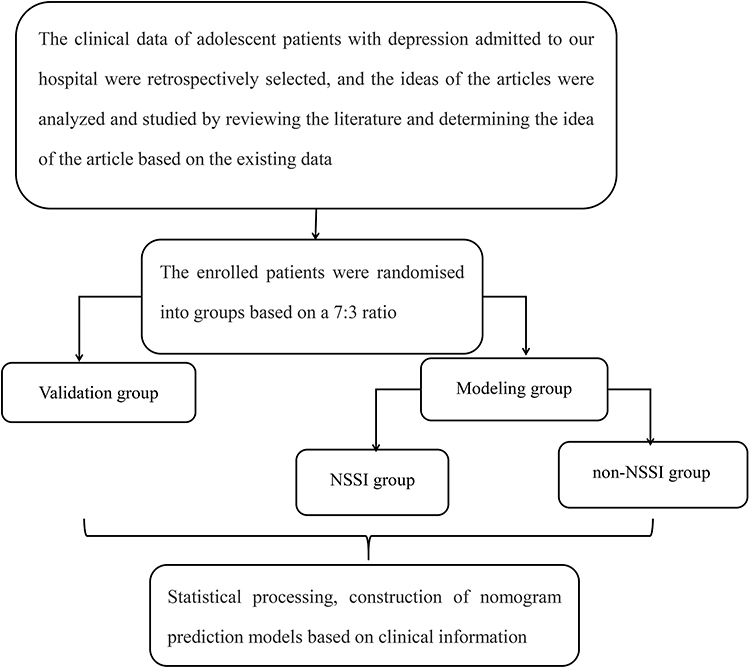 |
Figure 1 Case flow collection diagram. |
NSSI Judgment Criteria
Within the past year, patients were assessed using an NSSI evaluation questionnaire consisting of 12 items.10 It includes two dimensions: (1) self-injurious behaviors without obvious tissue damage (such as pinching oneself, scratching oneself, hitting hard objects like walls or tables with one’s head or fists); and (2) self-injurious behaviors with obvious tissue damage (such as stabbing, cutting, biting oneself, pulling out one’s hair, burning oneself, deliberately rubbing the skin until bleeding, or carving words on the skin). If the patient had any one of these 12 items, they were classified into the NSSI group. The questionnaire demonstrated good reliability, with a Cronbach’s α coefficient of 0.921, a split-half reliability of 0.851, and a test-retest reliability of 0.843.
Observation Indicators
(1) Comparison of clinical data between the modeling group and the validation group, including age, gender, course of disease, place of residence, whether they are an only child, left-behind experience, current smoking, current drinking, living in a boarding school, single-parent family, depression severity (The Self-Rating Depression Scale was used, with scores of 50–59 indicating mild depression and scores of 60 or above indicating severe depression),11 childhood abuse (Childhood Trauma Questionnaire was used for assessment, which includes 5 items; if 2 or more items reach the threshold score, it is considered abuse),12 childhood family dysfunction (The Family Assessment Device was used, including 7 core functions; a Z-score≥1 in the overall functioning dimension indicates dysfunctional family functioning),13 history of school bullying, educational level, study pressure, anxiety, sleep disorders, peer rejection/discrimination, relationship with teachers, history of trauma, Barratt Impulsiveness Scale score, already or preparing to drop out of school, loneliness, parents’ marital status, and exposure to domestic violence. (2) Comparison of clinical data between the NSSI group and the non-NSSI group. (3) Analysis of factors influencing NSSI in adolescents with depression. (4) Construction of a nomogram model. (5) Validation of the nomogram model. (6) Analysis of the Decision Curve Analysis (DCA) for the nomogram model.
Statistical Analysis
SPSS 25.0 software was used for independent sample t-tests and χ²-tests. Logistic regression was used to analyze the influencing factors; the nomogram model was built using R software. The ROC curve was used to evaluate the model’s discrimination, and DCA was used to evaluate its clinical application value. P<0.05 indicated statistical significance.
Results
Comparison of Clinical Data Between the Modeling Group and the Validation Group
There were no significant differences in clinical data such as age or gender between the two groups (P>0.05). See Table 1.
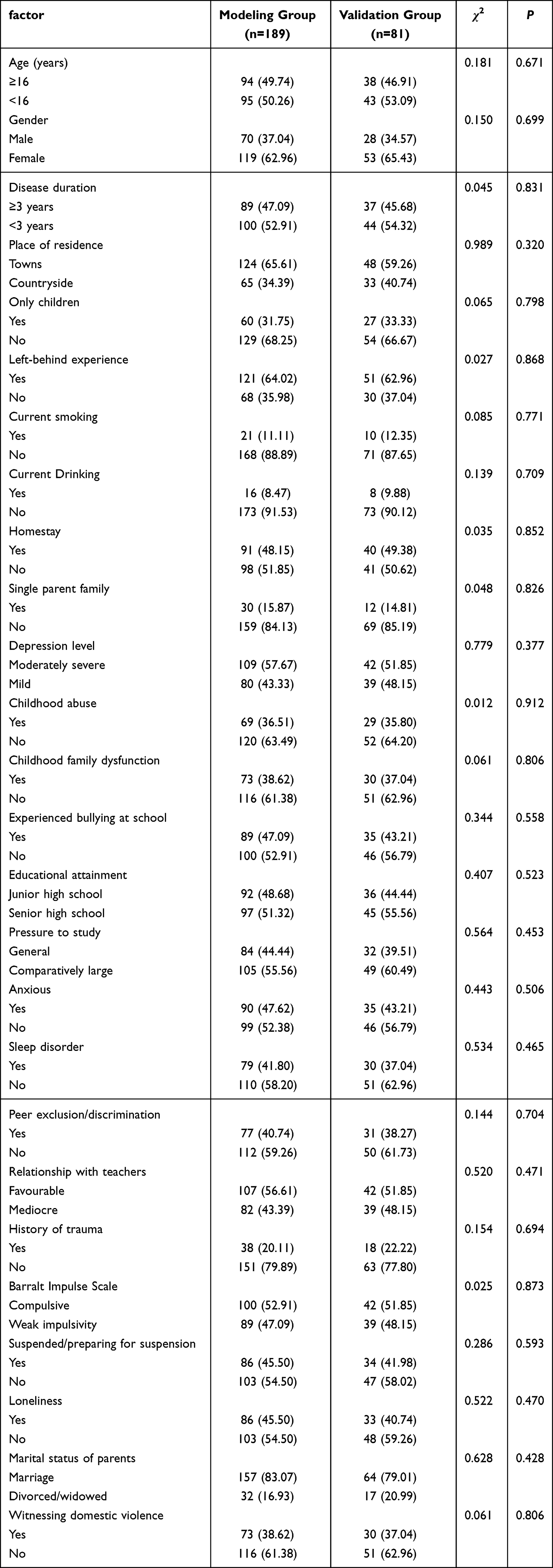 |
Table 1 Comparison of Clinical Data Between the Modeling Group and the Validation Group |
Comparison of Clinical Data Between the NSSI Group and the Non-NSSI Group
Among the 189 patients in the modeling group, 72 patients experienced NSSI, with an incidence of 38.10%. There were significant differences between the two groups in terms of course of disease, depression severity, childhood abuse, childhood family dysfunction, history of school bullying, sleep disorders, and Barratt Impulsiveness Scale (P<0.05). Other clinical data showed no significant differences (P>0.05). See Table 2.
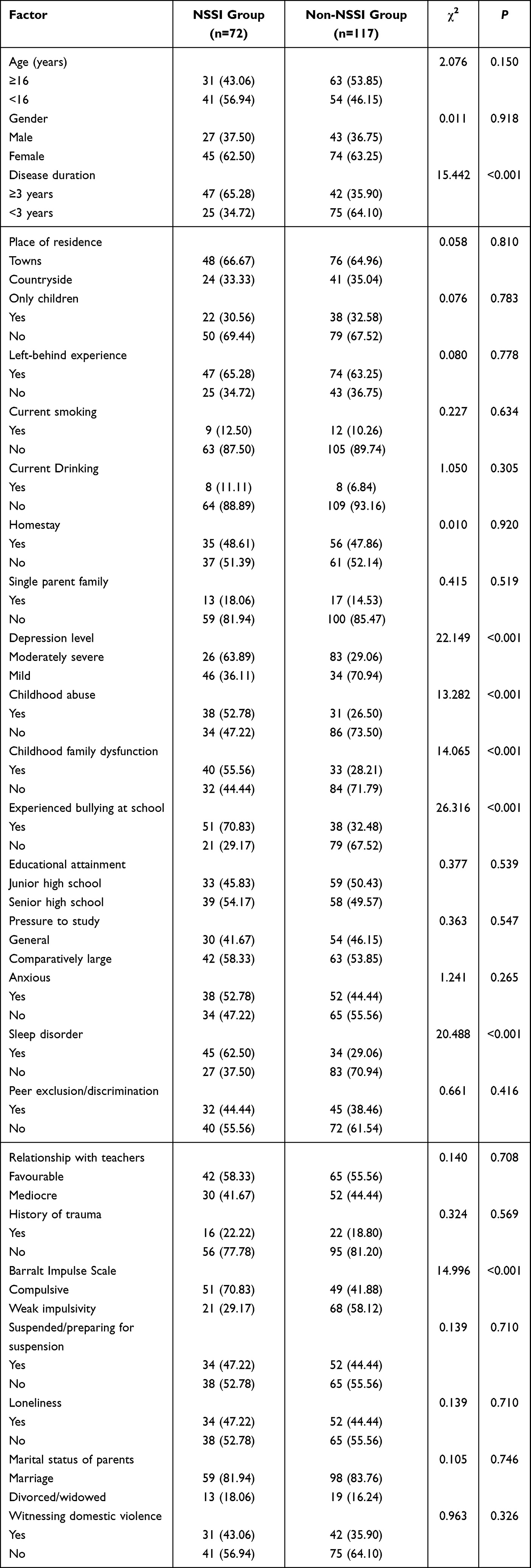 |
Table 2 Comparison of Clinical Data Between NSSI and Non-NSSI Groups |
Analysis of Factors Influencing NSSI in Adolescents with Depression
The dependent variable was NSSI in adolescents with depression (yes=1, no=0). The independent variables and their assignments are shown in Table 3. Multivariate Logistic regression (forward stepwise regression) analysis showed that course of disease, depression severity, childhood abuse, childhood family dysfunction, history of school bullying, sleep disorders, and Barratt Impulsiveness Scale score were risk factors (P<0.05). See Table 4.
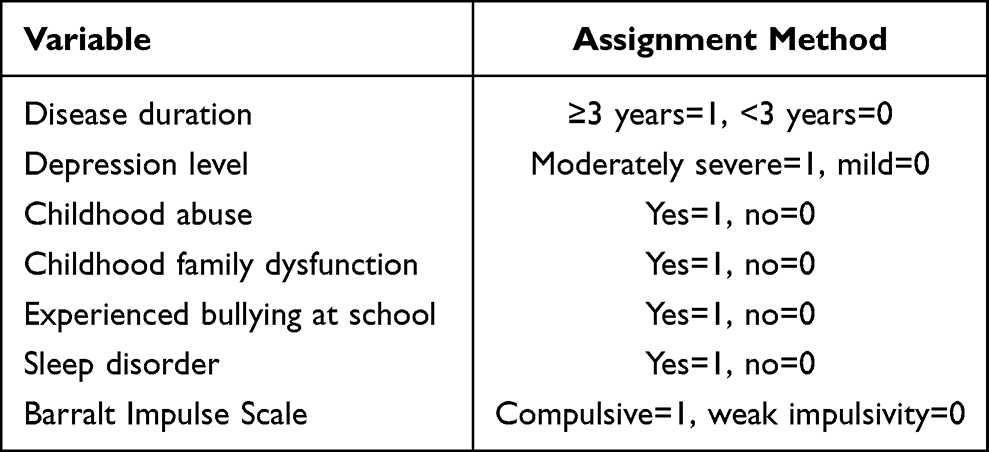 |
Table 3 Assignment Methods of Argument Variables |
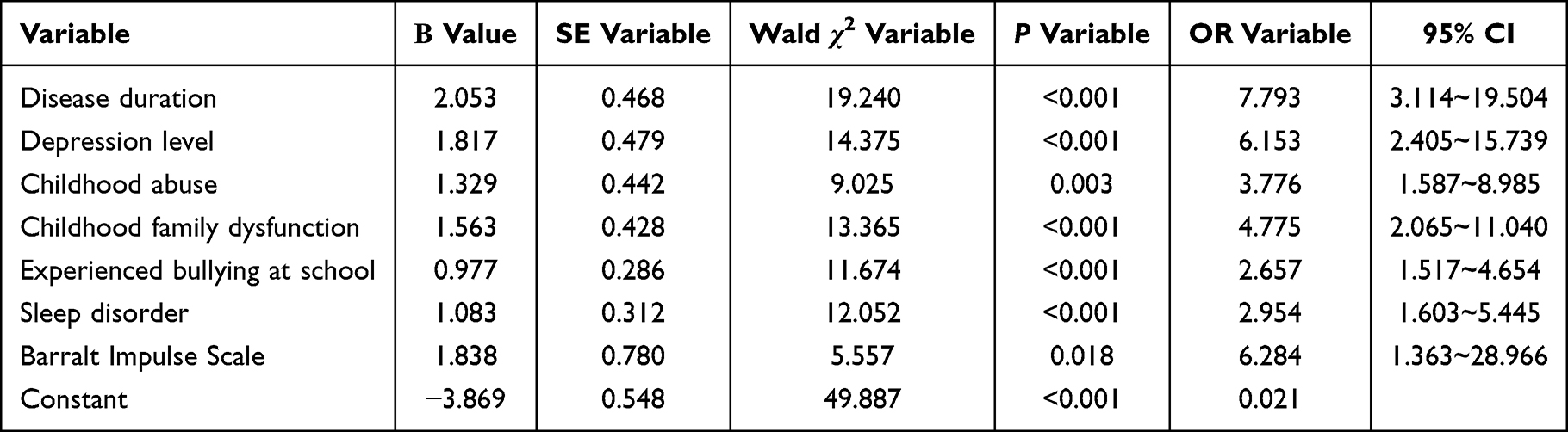 |
Table 4 Analysis of Factors Influencing NSSI in Adolescents with Depression |
Construction of a Nomogram Model for NSSI in Adolescents with Depression
A nomogram model was constructed based on the risk factors screened above: P=ex/ (1+ex), x=7.793× (course of disease) + 6.153 × (depression severity) + 3.776 × (childhood abuse) + 4.775 × (childhood family dysfunction) + 2.657 × (history of school bullying) + 2.954 × (sleep disorders) + 6.284 × (Barratt Impulsiveness Scale). In this model, the influencing factors are, in descending order: course of disease, depression severity, childhood family dysfunction, childhood abuse, sleep disorders, history of school bullying, and Barratt Impulsiveness Scale. For example, one patient’s disease course is <3 years (0 points), depression severity is moderate-to-severe (89.5 points), childhood abuse (65 points), childhood family dysfunction (76.5 points), no history of school bullying (0 points), sleep disorders (35.5 points), and weak impulsivity on the Barratt Impulsiveness Scale (0 points), giving a total score of 266.5 points. Dropping a perpendicular line at 266.5 on the total points scale yields a predicted probability of 84%. See Figure 2.
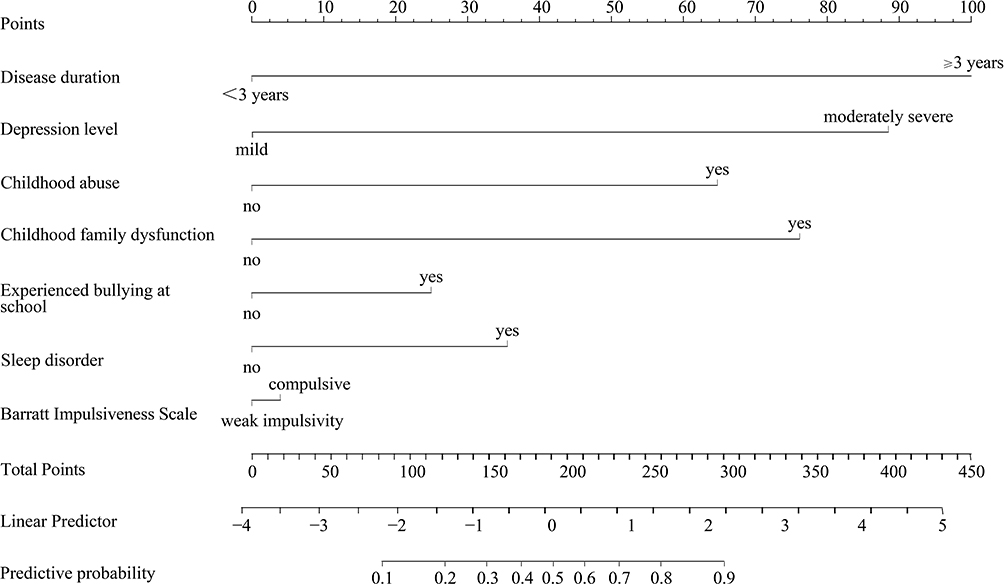 |
Figure 2 The nomogram model for NSSI behaviour in adolescents with depression. |
Validation of the Nomogram Model for NSSI in Adolescents with Depression
The ROC curve showed that the AUC of the modeling group was 0.899 (95% CI=0.824–0.976), and the AUC of the validation group was 0.954 (95% CI=0.899–0.999), as shown in Figure 3. The Hosmer-Lemeshow (H-L) test for the modeling group was χ²=7.243 (P=0.721), and for the validation group was χ²=7.010 (P=0.711), indicating that the predicted probability of NSSI in adolescents with depression was close to the actual probability, as shown in Figure 4.
 |
Figure 3 ROC curve (A) ROC curve of modeling group; (B) ROC curve of validation group. |
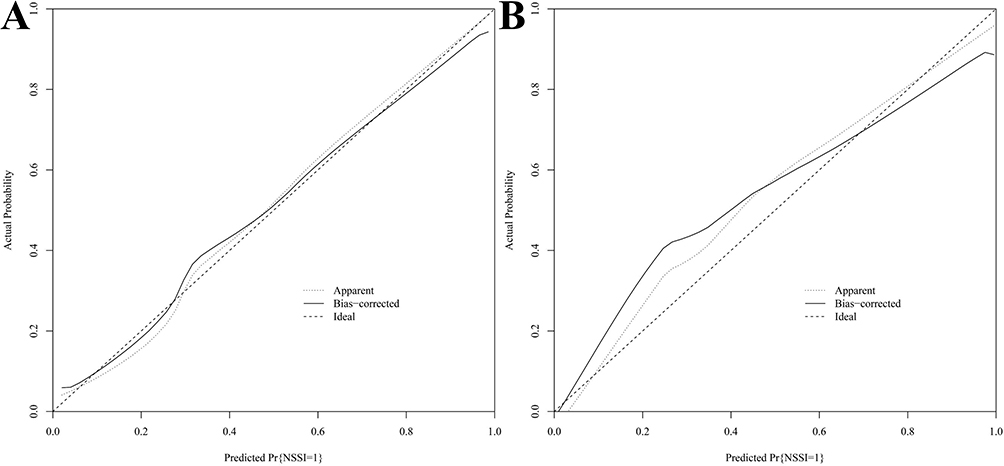 |
Figure 4 Calibration curve (A) Calibration curve of modeling group; (B) Calibration curve of validation group. |
Curve of the Nomogram Model
The DCA curve indicates that when the probability is between 0.05 and 0.97, the nomogram model has high clinical value in assessing NSSI in adolescents with depression, with a higher net benefit. See Figure 5.
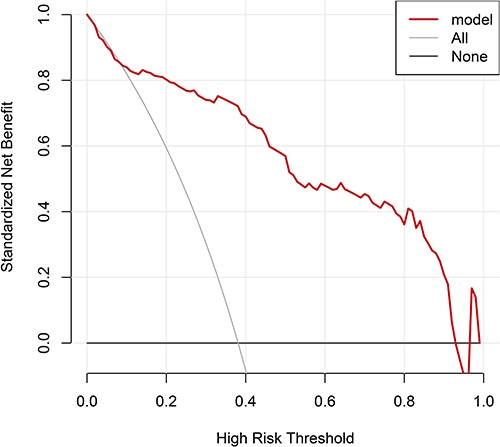 |
Figure 5 DCA curve for the nomogram. |
Discussion
Adolescents are a relatively special population, and adolescence is a critical period for shaping personality and developing self-identity. During this stage, self-awareness is strong, and if current pressures or conflicts cannot be resolved promptly and effectively, deviations may occur in their emotions and behaviors. Consequently, when confronted with stress, they cannot effectively alleviate problems and distress, leading to persistent depression. Adolescent depression is more complex, with atypical clinical symptoms, and because adolescents’ psychology, physiology, and emotions are volatile, symptoms can vary significantly among different individuals.14,15 NSSI is a way of releasing psychological pain by harming the body; moreover, it is covert. If patients are not promptly managed, their condition may worsen, potentially escalating the severity of self-injurious behavior, increasing treatment difficulty, and posing a threat to their lives.16 In this study, 72 out of 189 patients experienced NSSI (38.10%), which is close to the 42.48% reported by Shao et al,17 though slightly lower. The difference may be related to different sample sources and levels of depression severity. Nonetheless, the incidence remains relatively high, indicating that clarifying the factors influencing NSSI and intervening as early as possible are essential for reducing the risk of self-injury.
This study identified seven risk factors influencing NSSI (course of disease, depression severity, childhood abuse, childhood family dysfunction, history of school bullying, sleep disorders, and Barratt Impulsiveness Scale) and analyzed them as follows: (1) Patients with a course of disease exceeding three years require continuous medication to control the condition and alleviate symptoms. However, repeated relapses can worsen central lesions, diminish treatment confidence, foster negative emotions, and reduce disease stability, making NSSI more likely.18 (2) A higher degree of depression indicates more severe low mood. Such patients may resist social interaction and have fewer opportunities to release negative emotions. Adolescents are particularly sensitive and impulsive, with marked irritability and limited emotional regulation. Immersion in their inner world can trigger self-injurious impulses and increase NSSI risk.19 Thus, prompt and positive therapeutic measures are crucial for this group to alleviate the condition and reduce the risk of NSSI. (3) Childhood abuse involves physical and verbal violence from parents or guardians, inflicting both physical and psychological harm and thereby increasing the risk of NSSI.20 In clinical settings, psychological counseling should be provided to patients with such experiences to reduce the occurrence of NSSI. (4) Childhood family dysfunction, typically stemming from parental divorce, death, or domestic violence, disrupts family structure. Such patients often harbor negative emotions and, because of family-related issues, cannot appropriately regulate their emotions or release stress, making them more prone to engaging in NSSI or other negative behaviors.21 For these patients, collaboration with family is necessary to explore the causes of the disease, build a harmonious family environment, encourage close relatives to communicate frequently, and use positive, constructive methods to release emotions, thereby reducing NSSI. (5) Patients who have experienced school bullying lack a sense of security and tend to harbor negative emotions. They are often isolated by classmates and adopt avoidance strategies, and they cannot relieve stress through healthy outlets. Consequently, their risk of NSSI increases.22 Therefore, it is recommended that those closest to them—teachers, family members, and friends—provide care and encouragement. When facing difficulties, they should seek help in a positive manner, alleviating negative emotions and reducing the risk of NSSI. (6) Depressed patients frequently experience sleep disorders, which exacerbate impulsiveness and reduce their ability to self-regulate emotions. Coupled with academic pressures, these negative emotions accumulate without proper relief, prompting patients to resort more readily to NSSI.23 Close attention should be paid to patients’ sleep quality, and proactive measures to improve sleep should be adopted. (7) Higher scores on the Barratt Impulsiveness Scale indicate more frequent impulsive behaviors and weaker self-control. Moreover, impulsive behaviors may bring about a sense of release or pleasure, further increasing the likelihood of impulsive behaviors and triggering NSSI.24 Hence, rigorous supervision and behavioral constraints are essential for such patients. In this study, the lack of differences in some factors may be related to the small sample size and the potential bias inherent in retrospective research. Based on the multiple influencing factors mentioned above and the complexity of treatment itself, the prevention of NSSI in patients requires a comprehensive and multidisciplinary approach, including pharmacological, psychological, and family support. It is also important to promote awareness of NSSI-related knowledge, create a positive environment, encourage interaction with optimistic and proactive peers, and help patients learn positive attitudes toward life and effective coping strategies, thereby mitigating the cognitive and behavioral impacts of adverse factors.
A nomogram is a visual predictive tool constructed based on a multivariate regression model. By integrating multiple predictive variables, it provides individuals with a quantitative assessment of outcome risk. The generalizability of a nomogram depends on the target population. It enables precise population stratification in risk screening, facilitates early intervention in warning systems, optimizes treatment plan selection in clinical decision-making, and allows rational resource allocation in prognostic management, thereby assisting clinicians in providing quantitative predictions for specific clinical scenarios. The ROC curve of the nomogram constructed in this study showed good discrimination, and the H-L test indicated a good model fit, suggesting that the model has robust predictive capabilities. According to the DCA curve, between 0.05 and 0.97, the nomogram model exhibits high clinical applicability in assessing NSSI among adolescents with depression, enabling targeted prevention.
Conclusion
In conclusion, the course of disease, depression severity, childhood abuse, childhood family dysfunction, history of school bullying, sleep disorders, and Barratt Impulsiveness Scale are factors influencing NSSI among adolescents with depression. The constructed nomogram model demonstrated good consistency and high clinical application value, which can help clinicians identify high-risk populations and implement early prevention. Although the model can guide interventions through predictive assessment to reduce the incidence of NSSI, it still requires validation through rigorous implementation studies. However, this study has several limitations. First, as a retrospective study, there may be inherent biases in data collection. Second, being a single-center study with a relatively small sample size, it did not cover all variables across different regions, which may limit the generalizability of the results. Third, the short follow-up period may affect the accuracy of the findings. Future research should expand the sample size and conduct prospective multicenter studies for further validation.
Data Sharing Statement
The original contributions presented in the study are included in the article.
Ethics Approval
The study involving human participants was reviewed and approved by the Ethics Committee of Shaoyang Brain Hospital and was conducted in accordance with the 1964 Helsinki Declaration and its later amendments. Written informed consent was obtained from the legal guardians of all adolescent patients, and assent was also obtained from the patients themselves.
Funding
Hunan Provincial Natural Science Foundation (Project Number: 2024JJ7493).
Disclosure
All author(s) declares that they have no Conflict of interest.
References
1. Beck A, Leblanc JC, Morissette K, et al. Screening for depression in children and adolescents: a protocol for a systematic review update. Syst Rev. 2021;10(1):24. doi:10.1186/s13643-020-01568-3
2. Waraan L, Siqveland J, Hanssen-bauer K, et al. Family therapy for adolescents with depression and suicidal ideation: a systematic review and meta-analysis. Clin Child Psychol Psychiatry. 2023;28(2):831–849. doi:10.1177/13591045221125005
3. J Zhu, Chen Y, Su B. Non-suicidal self-injury in adolescence: longitudinal evidence of recursive associations with adolescent depression and parental rejection. J Adolesc. 2020;84:36–44. doi:10.1016/j.adolescence.2020.08.002
4. Huang Z-Y, Ruan Q-N, Zheng Y, et al. Adolescent suicidal ideation: dissecting the role of sex in depression and NSSI predictors. Child Adolesc Psychiatry Ment Health. 2024;18(1):68. doi:10.1186/s13034-024-00741-z
5. H LEI, Yang Y, T ZHU, et al. Network analysis of the relationship between non-suicidal self-injury, depression, and childhood trauma in adolescents. BMC Psychol. 2024;12(1):234. doi:10.1186/s40359-024-01729-2
6. Shen G, Li C-H, Ruan Q-N, et al. Assessing the contributions of gender, clinical symptoms, and psychometric traits to non-suicidal self-injury behaviors in Chinese adolescents: a nomogram approach. Child Adolesc Psychiatry Ment Health. 2024;18(1):139. doi:10.1186/s13034-024-00832-x
7. Zhou J-C, Y Cao, Xu X-Y, et al. Analysis of risk factors of suicidal ideation in adolescent patients with depression and construction of prediction model. World J Psychiatry. 2024;14(3):388–397. doi:10.5498/wjp.v14.i3.388
8. Baldini V, Gnazzo M, Maragno M, et al. Suicidal risk among adolescent psychiatric inpatients: the role of insomnia, depression, and social-personal factors. Eur Psychiatry. 2025;68(1):e42. doi:10.1192/j.eurpsy.2025.29
9. First MB, Reed GM, Hyman SE, et al. The development of the ICD-11 clinical descriptions and diagnostic guidelines for mental and behavioural disorders. World Psychiatry. 2015;14(1):82–90. doi:10.1002/wps.20189
10. Hu Z, Yu H, J Zou, et al. Relationship among self-injury, experiential avoidance, cognitive fusion, anxiety, and depression in Chinese adolescent patients with nonsuicidal self-injury. Brain Behav. 2021;11(12):e2419. doi:10.1002/brb3.2419
11. W Xie, Liang L, Lu Y, et al. Interpreting depression from question-wise long-term video recording of SDS evaluation. IEEE J Biomed Health Inform. 2022;26(2):865–875. doi:10.1109/JBHI.2021.3092628
12. Georgieva S, Tomas JM, Navarro-pérez JJ. Systematic review and critical appraisal of childhood trauma questionnaire—short form (CTQ-SF). Child Abuse Negl. 2021;120:105223. doi:10.1016/j.chiabu.2021.105223
13. A CG, Rodríguez-naranjo C. The McMaster family assessment device (FAD) dimensions involved in the prediction of adolescent depressive symptoms and their mediating role in regard to socioeconomic status. Fam Process. 2023;63(1):414–427. doi:10.1111/famp.12867
14. Zhang B, Zhang W, L Sun, et al. Relationship between alexithymia, loneliness, resilience and non-suicidal self-injury in adolescents with depression: a multi-center study. BMC Psychiatry. 2023;23(1):445. doi:10.1186/s12888-023-04938-y
15. Başgöze Z, Wiglesworth A, Carosella KA, et al. Depression, non-suicidal self-injury, and suicidality in adolescents: Common and distinct precursors, correlates, and outcomes. J Psychiatr Brain Sci. 2021;6(5). doi:10.20900/jpbs.20210018.
16. Shen Y, Zhou Y, Hu Y, et al. Non-suicidal self-injury function: prevalence in adolescents with depression and its associations with non-suicidal self-injury severity, duration and suicide. Front Psychiatry. 2023;14:1188327. doi:10.3389/fpsyt.2023.1188327
17. Shao C, Wang X, Ma Q, et al. Analysis of risk factors of non-suicidal self-harm behavior in adolescents with depression. Ann Palliat Med. 2021;10(9):9607–9613. doi:10.21037/apm-21-1951
18. Zheng Y, Xiao L, Wang H, et al. A retrospective research on non-suicidal self-injurious behaviors among young patients diagnosed with mood disorders. Front Psychiatry. 2022;13:895892. doi:10.3389/fpsyt.2022.895892
19. Poudel A, Lamichhane A, Magar KR, et al. Non suicidal self injury and suicidal behavior among adolescents: co-occurrence and associated risk factors. BMC Psychiatry. 2022;22(1):96. doi:10.1186/s12888-022-03763-z
20. Li X, Liu X-L, Wang Y-J, et al. The effects of childhood maltreatment on adolescent non-suicidal self-injury behavior: mediating role of impulsivity. Front Psychiatry. 2023;14:1139705. doi:10.3389/fpsyt.2023.1139705
21. S SUHAILUSMANI, Mehendale M, M YOUSIFSHAIKH, et al. Understanding the impact of adverse childhood experiences on non-suicidal self-injury in youth: a systematic review. Alpha Psychiatry. 2024;25(2):150–164. doi:10.5152/alphapsychiatry.2024.231139
22. Y LIU, Xu X, Huang X, et al. The mediating effects of school bullying victimization in the relationship between childhood trauma and NSSI among adolescents with mood disorders. BMC Pediatr. 2024;24(1):524. doi:10.1186/s12887-024-04986-7
23. Chen H, Hong L, Tong S, et al. Cognitive impairment and factors influencing depression in adolescents with suicidal and self-injury behaviors: a cross-sectional study. BMC Psychiatry. 2023;23(1):247. doi:10.1186/s12888-023-04726-8
24. Y XIE, Wu S, Li J, et al. Impulse control deficits among patients with nonsuicidal self-injury: a mediation analysis based on structural imaging. J Psychiatry Neurosci. 2025;50(2):E73–E84. doi:10.1503/jpn.240129
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Depression and Associated Risk Factors Among Type 2 Diabetic Patients: A Cross Sectional Study on a Convenience Sample from the Diabetic Center, Khamis Mushait; Saudi Arabia
Abuhegazy H, Mujairi A, Banah F, Agdi Y, Elkeshishi H, Kamel A, Abdullah A, Elsheikh M
Neuropsychiatric Disease and Treatment 2022, 18:1975-1984
Published Date: 31 August 2022
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023
Development and Validation of a Nomogram Model for Accurately Predicting Depression in Maintenance Hemodialysis Patients: A Multicenter Cross-Sectional Study in China
Zhou X, Zhu F
Risk Management and Healthcare Policy 2024, 17:2111-2123
Published Date: 3 September 2024