Back to Journals » Journal of Inflammation Research » Volume 15
Construction of a Nomogram for Identifying Refractory Mycoplasma pneumoniae Pneumonia Among Macrolide-Unresponsive Mycoplasma pneumoniae Pneumonia in Children
Authors Xie Q, Zhang X, Cui W, Pang Y
Received 31 August 2022
Accepted for publication 15 November 2022
Published 30 November 2022 Volume 2022:15 Pages 6495—6504
DOI https://doi.org/10.2147/JIR.S387809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Adam Bachstetter
Qiaoyi Xie,1 Xiaote Zhang,2 Wei Cui,1 Yajiao Pang1
1Department of Pediatrics, The Affiliated People’s Hospital of Ningbo University, Ningbo, People’s Republic of China; 2Department of Otolaryngology Head and Neck Surgery, Ningbo Yinzhou No.2 Hospital, Ningbo, People’s Republic of China
Correspondence: Qiaoyi Xie, Department of Pediatrics, The Affiliated People’s Hospital of Ningbo University, No. 251, Baizhang East Road, Ningbo, 315040, People’s Republic of China, Tel + 86 0574-87016888, Email [email protected]
Objective: The individualized prediction of treatment regimens of macrolide-unresponsive Mycoplasma pneumoniae pneumonia (MUMPP) is scarce. The aim of this study was, therefore, to evaluate the relevant data of patients and construct a nomogram for identifying refractory Mycoplasma pneumoniae pneumonia (RMPP) among children continued to be treated with macrolide after the confirmation of MUMPP, providing a reference for the choice of treatment regimen.
Methods: We performed a retrospective study involving 162 children who continued to be treated with macrolide (azithromycin) after the confirmation of MUMPP without antibiotic changes between January 2020 and January 2022. We collected data on clinical feature, hospitalization period, treatments, laboratory data, extrapulmonary symptoms, parapneumonic effusion, and connections with other respiratory pathogens. In addition, the independent risk factors for RMPP were determined through univariate and multivariate analyses, and then a nomogram was constructed and validated.
Results: In this study, the multivariate logistic regression analysis showed that age, leukocyte count, neutrophil proportion, serum procalcitonin, and lactate dehydrogenase were independent risk factors for RMPP. Using the five independent associated factors, the nomogram for identification of RMPP was constructed. Moreover, the area under the ROC curve (AUC) was 0.925 (95% CI: 0.882– 0.968) for the nomogram showing excellent discrimination. The calibration curve, close to the 45-degree line, exhibited good calibration of nomogram.
Conclusion: We constructed and validated a visual and user-friendly nomogram for individualized prediction of RMPP risk in children who continued to be treated with macrolide after the confirmation of MUMPP based on five variables. According to the nomogram model, continuation of macrolide should be considered rather than second-line antibiotics including tetracyclines (doxycycline or minocycline) and fluoroquinolones for MUMPP children with low predictive values.
Keywords: nomogram, refractory, Mycoplasma pneumoniae, pneumonia, children
Introduction
Community-acquired pneumonia (CAP) is an important cause of hospitalization in children, placing severe pressure on the healthcare system and patients.1 Mycoplasma pneumoniae (MP) is a common cause of CAP in children and adolescents, accounting for about 10–30% of the cases.2,3 MP infection can cause a variety of clinical symptoms, including fever, headache, cough, etc.4 Several serious respiratory illnesses caused by MP have also been documented, such as pleural effusion, acute respiratory distress syndrome, and lung abscesses.4,5 It has also been closely linked to the extrapulmonary symptoms such as hemolytic anemia, arthritis, and urticaria.4,6
Macrolide has long been recommended as the first-line antimicrobials used to treat patients with MP pneumonia (MPP), which has demonstrated satisfactory effectiveness and good tolerability for many years.4 Among macrolide antibiotics, azithromycin can improve the clinical symptoms of patients with MPP due to its effective inhibitory function against Mycoplasma.7,8 For macrolide-sensitive MP, the minimal inhibitory concentration (MIC) of azithromycin (<0.0005μg/mL) is lower than doxycycline (less than 0.25μg/mL) and levofloxacin (<0.5μg/mL).9 However, some studies have shown that the prevalence of macrolide-resistant MP (MRMP) was increasing due to the broad application of macrolides, especially in some regions of Asia with an incidence ≥90%.10–13 MRMP caused a longer duration of fever and hospitalization, even life-threatening in severe cases.14,15 The methods of polymerase chain reaction (PCR) are the gold standard for MRMP diagnosis. However, detection of mycoplasma infection using PCR should depend on the clinical condition, as Mycoplasma pneumoniae still colonized the respiratory tract for a long time after infection, even after antimicrobial treatment. Moreover, the PCR gene detection equipment is expensive; thus, this detection is not easily accessible.16 Macrolide unresponsiveness can consider as early indicators of MRMP pneumonia (MRMPP). Macrolide-unresponsive MPP (MUMPP) was documented as persistent fever for 3 days or longer after macrolide treatment.16,17 Without appropriate treatment, MUMPP may develop into refractory MPP (RMPP) which may complicate the treatment of MUMPP.
Second-line antibiotics, such as tetracyclines (doxycycline or minocycline) and fluoroquinolones, are recommended for patients with MUMPP.18 The efficacy of tetracyclines (doxycycline or minocycline) and fluoroquinolones is uplifting.19 However, tetracycline is only used in children aged ≥8 years old due to the side effects of tooth discoloration and tooth enamel hypoplasia.20 Fluoroquinolones can be used in children <8 years with MUMPP.21 In addition, fluoroquinolones have been reported to be linked to a risk of musculoskeletal toxicities.22 Moreover, some studies have demonstrated that macrolide is still effective in patients with MUMPP, although second-line antibiotics have been recommended for the treatment of MUMPP.23
To sum up, individualized prediction of treatment regimens of MUMPP is scarce. The aim of this study was, therefore, to evaluate the relevant data of patients and construct a nomogram for identifying RMPP among children continued to be treated with macrolide after the confirmation of MUMPP without antibiotic changes, providing a reference for the choice of treatment regimen.
Methods
Subjects and Study Design
Medical records of patients with MPP under the age of 18 years admitted to the Affiliated People’s Hospital of Ningbo University from January 2020 to January 2022 were retrospectively analyzed. MPP can be diagnosed as follows: (1) the presence of fever, cough, tachypnoea, difficult breathing; (2) chest X-ray examination results compatible with pneumonia; and (3) the detection of MP IgM antibody conducted using enzyme-linked immunosorbent assay during the illness. The patients with MUMPP were assigned to the non-refractory MPP (NRMPP) and RMPP groups, respectively. RMPP was documented as persistent fever, aggravated clinical signs, and progressive imaging findings despite the administration of macrolide for 7 days or more. The remaining children were NRMPP defined as the reduction of fever and improvement in clinical signs or imaging findings within 7 days of macrolide treatment. RMPP was diagnosed if fever persisted, clinical signs deteriorated, and imaging findings progressed despite the administration of macrolide for 7 days or more. NRMPP was diagnosed on the basis of the reduction of fever and improvement of clinical signs or imaging findings within 7 days of macrolide treatment.
Patients were enrolled if they (1) were under the age of 18 years, (2) had MPP, (3) were confirmed as MUMPP, (4) continued to be treated with macrolide (azithromycin) after the confirmation of MUMPP without antibiotic changes. Patients were excluded according to the exclusion criteria: (1) After treatment with macrolide, the patient’s fever had subsided within 3 days; (2) In spite of positive MP IgM, the clinical symptoms and imaging findings were not consistent with pneumonia; and (3) The patient were allergic to macrolide; (4) The information of treatment was lost.
All enrolled patients with MUMPP were treated with 10mg/kg/day of intravenous azithromycin (Zhejiang Asia-Pacific Pharmaceutical Co., Ltd.). According to the recommendations of our hospital, informed consents were acquired from patient’s guardians before the treatment of azithromycin.
The ethical committee of the Affiliated People’s Hospital of Ningbo University approved the study (No. 107-P-066). Data were collected after written informed consents were obtained from patient’s guardians.
Data Collection
The data were retrospectively recorded in this study including clinical features (age, sex, weight), hospitalization period, treatments, laboratory data (leukocyte, neutrophil proportion, platelet count, C-reactive protein, albumin, erythrocyte sedimentation rate, lactate dehydrogenase, procalcitonin), extrapulmonary symptoms (urticaria, arthralgia, somnolence, anemia, and vomiting), parapneumonic effusion, coinfection with other respiratory pathogens (bacterial, viral, or fungal infection).
Statistical Analysis
Analyses were carried out using R statistical software version 4.2.0 or MedCalc version 18.2.1. The data retrospectively collected in this study were summarized as mean ± standard deviation or frequency count (percentage). Independent-samples t-test was used to compare continuous variables between the two groups, and Chi-square test was used for categorical variables such as sex and parapneumonic effusion. Multivariate logistic regression was applied for the evaluation of associated factors of NRMPP and RMPP. Then, a nomogram was constructed to build a predictive model. Discrimination of the model was analyzed using the receiver operating characteristic (ROC) curve. The calibration ability of the nomogram was assessed using the 1000 bootstrap samples (calibration curves). P<0.05 was deemed significant.
Results
Patient Characteristics
A total of 1460 MPP patients within the study period were screened; of those, 162 patients were included in this study. Among those, 106 children were in the NRMPP group, and 56 were in the RMPP group. The mean±SD age of patients in the NRMPP and RMPP groups was 6.44±3.64 years and 8.93±4.19 years, respectively (P<0.001) (Table 1). Patients in the RMPP group were significantly older than those in the NRMPP group. Higher proportions of patients in the NRMPP group were aged 1–3 years, 3–5 years, 5–8 years compared to the RMPP group. In patients aged >8 years, the proportion of patients in the RMPP and NRMPP groups was comparable. The leukocyte count (×109/L) in each group was 17.38±4.63 and 22.29±6.30, respectively (P<0.001), and the neutrophil proportion (%) was 81.07±9.38 and 86.61±3.72 in the NRMPP and RMPP groups, respectively (P<0.001) (Table 1). Compared with patients in the NRMPP group, patients in the PMPP group had higher level of C-reactive protein (P=0.002), erythrocyte sedimentation rate (P=0.044), serum procalcitonin (P<0.001), and lactate dehydrogenase (P<0.001) (Table 1). The two groups were balanced for sex (P=0.989), weight (P=0.242), platelet count (P=0.063), albumin (P=0.260), and coinfection with other respiratory pathogens (P=0.059) (Table 1). The above results of the independent-samples t-test and chi-square test were confirmed by the univariate logistic analysis (Supplementary Table 1). Among the MUMPP patients continuously treated with macrolide, the patients in the RMPP group had longer duration of corticosteroid treatment and hospital stay than those in the NRMPP group (P=0.001 and 0.015, respectively) (Table 2). The number of patients with extrapulmonary symptoms in the NRMPP and RMPP groups was 15 (14.2%) and 16 (28.6%), respectively (P=0.045), and the patients with parapneumonic effusion was 28 (26.4%) and 37 (66.1%), respectively (P<0.001) (Table 2). The results in Table 2 show that patients in the RMPP group had a more severe disease than those in the NRMPP group.
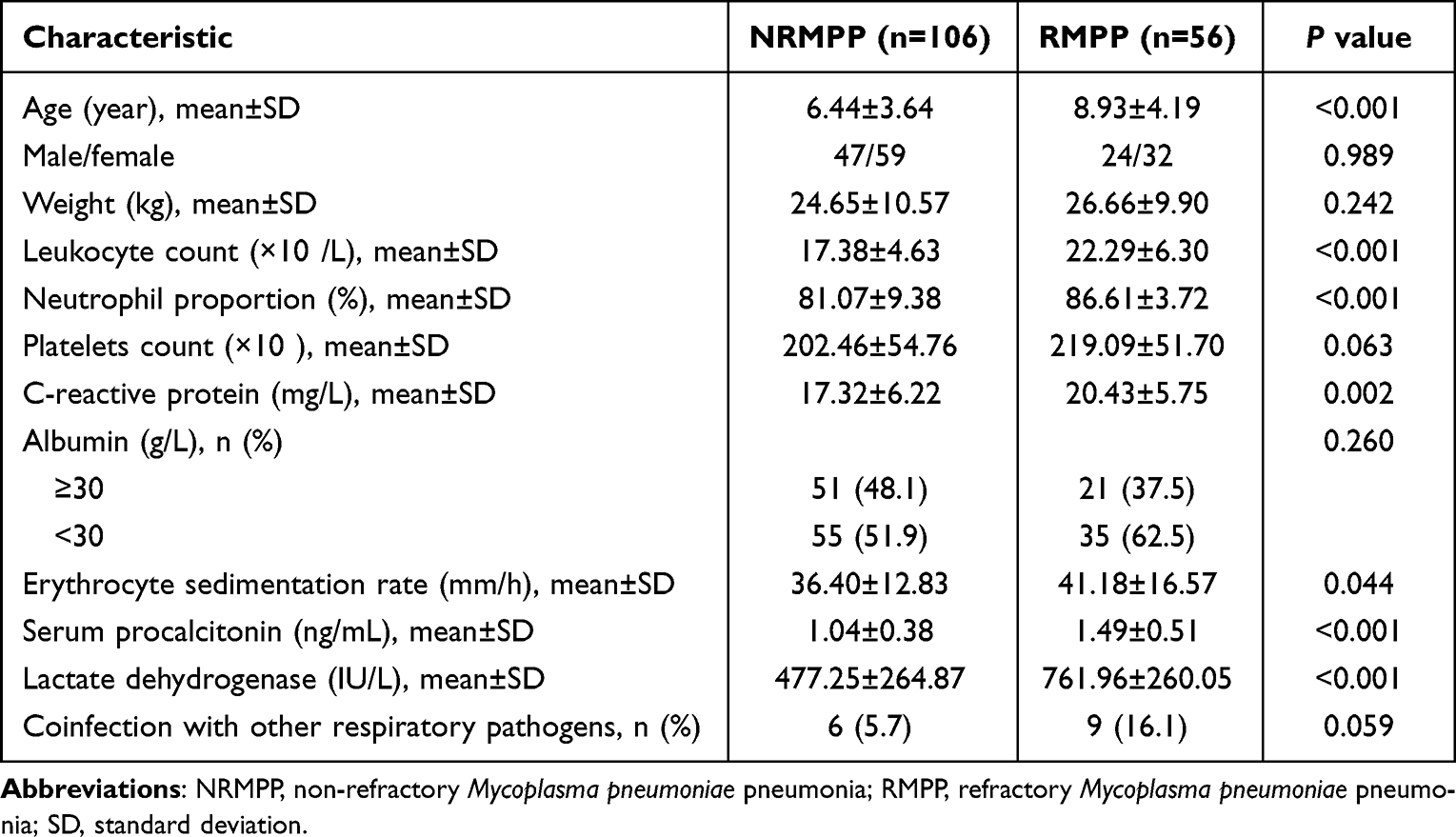 |
Table 1 Patient Characteristics |
 |
Table 2 Severity of MUMPP Continuing to Receive Macrolide After the Confirmation of MUMPP |
Risk Factors for RMPP Among MUMPP Patients Continuously Treated with Macrolide
Based on the above results, we assessed the associated factors of NRMPP and RMPP by multivariate logistic regression. As Table 3 shows, age (odds ratio=1.201, 95% CI: 1.056–1.383, P=0.007), leukocyte count (odds ratio=1.223, 95% CI: 1.103–1.382, P=0.000), neutrophil proportion (odds ratio=1.198, 95% CI: 1.075–1.372, P=0.004), serum procalcitonin (odds ratio=6.439, 95% CI: 2.202–22.203, P=0.001), and lactate dehydrogenase (odds ratio=1.003, 95% CI: 1.002–1.006, P=0.001) were independently associated risk factors for increased odds of RMPP.
 |
Table 3 Variables Associated with RMPP Among MUMPP Children Continuing to Receive Macrolide After the Confirmation of MUMPP in Multivariable Logistic Regression Analysis |
Construction of a Nomogram for Identification of RMPP
Using the five independent associated factors (age, leukocyte count, neutrophil proportion, serum procalcitonin, and lactate dehydrogenase), the nomogram for identification of RMPP was constructed (Figure 1). For example, a 14-year-old patient who had 26×109/L of leukocyte count, 80% of neutrophil proportion, 1.5ng/mL of serum procalcitonin, and 600IU/L of lactate dehydrogenase, the total point was 209 (34+50+67+37+21). The risk was 0.76.
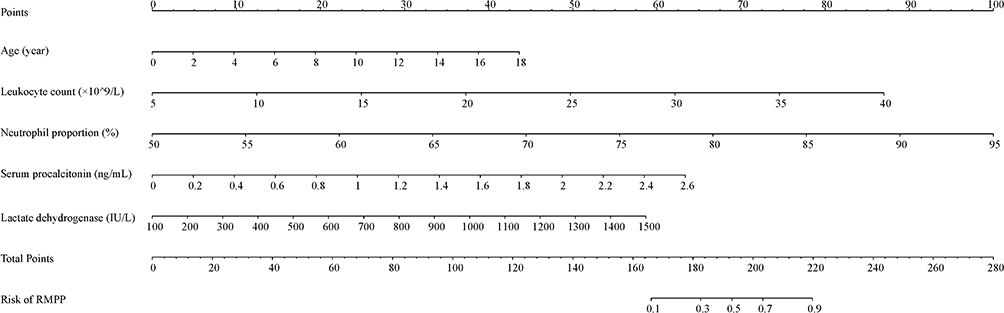 |
Figure 1 Nomogram for predicting RMPP in children continuing to receive macrolide after the confirmation of MUMPP. Abbreviations: RMPP, refractory Mycoplasma pneumoniae pneumonia; MUMPP, macrolide-unresponsiveMycoplasma pneumoniae pneumonia. |
Validation of a Nomogram for Identification of RMPP
The area under the ROC curve (AUC) was 0.925 (95% CI: 0.882–0.968) for the nomogram showing excellent discrimination (Figure 2). The calibration curve, close to the 45-degree line, exhibited good calibration of nomogram (Figure 3).
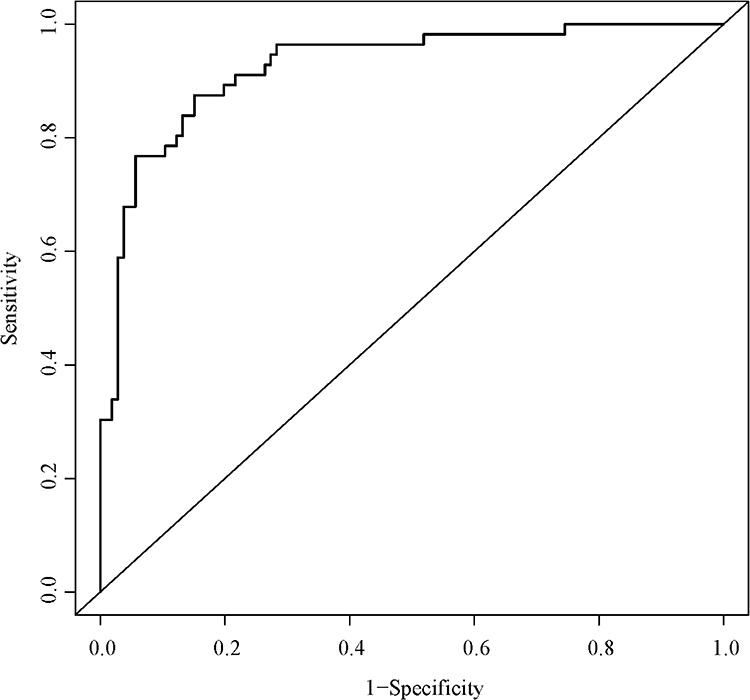 |
Figure 2 The ROC analysis for the predictive model. Abbreviation: ROC, receiver operating characteristic. |
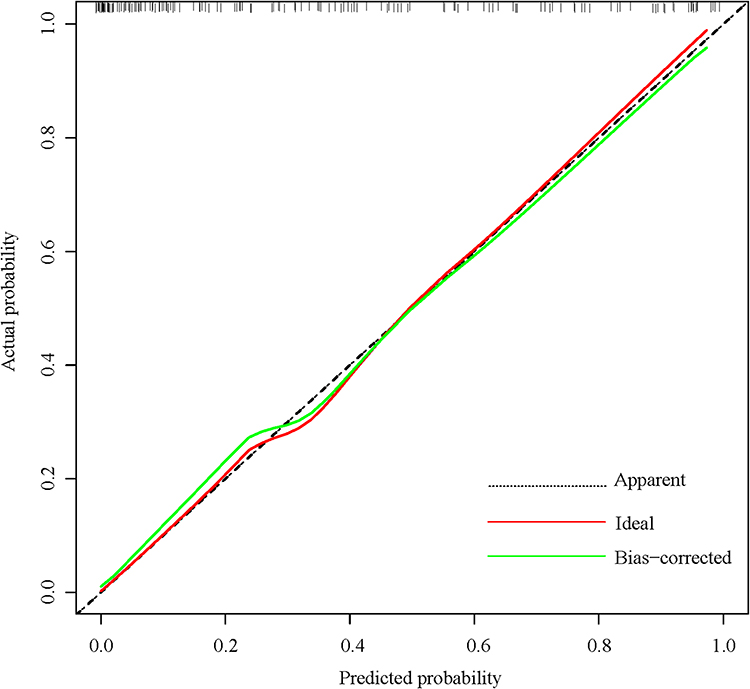 |
Figure 3 The calibration curve indicated good consistency between the actual diagnosed RMPP and the predicted probability. Abbreviation: RMPP, refractory Mycoplasma pneumoniae pneumonia. |
Discussion
In the present study, we analyzed a total of 162 children to construct and validate a nomogram for identifying RMPP among MUMPP in children continued to be treated with macrolide after the confirmation of MUMPP without antibiotic changes. Our findings showed that the nomogram included five key risk factors (age, leukocyte count, neutrophil proportion, serum procalcitonin, and lactate dehydrogenase).
Adequate immune response can effectively eliminate MP and help alleviate disease through the activation of lymphocyte and the secretion of cytokine.24 Children more likely develop an infection to certain bacteria due to the inability to develop a strong humoral response.25 However, an inappropriate immune response to MP will generate an excessive inflammatory response, which can aggravate the disease and even lead to the occurrence of RMPP. Data showed that pulmonary lesions in children with immunodeficiency were generally mild.26 This theory provides a good explanation for the selectivity of RMPP for children’s age. Children older than 5 years have more developed immune system compared to the younger children. Coincidentally, children over the age of 5 years happen to be more susceptible to MP, exhibiting more severe disease.27 Consistent with previous results, this study showed that older children were more likely to develop RMPP than younger children.
In addition, leukocytes, including neutrophils, eosinophils, basophils, monocytes, and lymphocytes, can release antimicrobial substances until more specialized cells (macrophage) reach the site of inflammation where a more effective attack is launched.28 However, recent study suggests that leukocytes are more sophisticated cells than previously recognized. They could show phenotypic and functional heterogeneity and play an extremely important role in human health.29,30 Neutrophils, making up 50–70% of the leukocytes in human, are involved in multiple stages of inflammation, including initiation, modulation, and resolution, contributing to wound healing, and are essential for maintaining tissue homeostasis.29,31 In addition, the recruitment and activation of neutrophils must be tightly controlled to prevent excessive tissue or organ damage.32 Excessive inflammation response was an important cause of the development of MPP.33 In the present study, we assessed the RMPP risk of patients with different leukocyte count and neutrophil proportion. Both univariate and multivariate analyses suggested that higher leukocyte count and neutrophil proportion implied higher RMPP risks, which showed that children with RMPP may have more excessive inflammation due to abnormal increase in leukocyte count and neutrophil proportion.
Procalcitonin, a protein secreted by thyroid C cells, is a precursor of calcitonin. Due to the interaction of inflammatory cytokines and bacterial toxins, procalcitonin is produced in large quantities, making its detection value significantly improved. It has been reported that patients with the higher detection value of procalcitonin have more severe infections.34 At present, the level of procalcitonin can be regarded as a reference index for antibiotic treatment of children with Mycoplasma pneumonia, providing guidance on medication. Experts believe that when serum procalcitonin of children ≥0.5 ng/mL, antibiotics should be used in time, thereby shortening the course of antibiotics and improving the efficacy.35 In this study, the level of serum procalcitonin was an independent risk factor for RMPP among MUMPP patients who continued to be treated with macrolide. Patients with low value of procalcitonin were regarded as the low risk for RMPP, but the incidence of RMPP increased with increasing serum procalcitonin level. Low serum procalcitonin level was a potential indicator of continued macrolide therapy in patients with MUMPP.
Lactate dehydrogenase is seen as a clinically meaningful biomarker of RMPP, as its expression is upregulated in this disease. According to multiple reports, the cut-off level of LDH for the treatment of RMPP is 379–480 IU/L.36–38 Other biomarkers of inflammation, including C-reactive protein,39 erythrocyte sedimentation rate,37 interleukin-1039 etc, can also predict RMPP, but lactate dehydrogenase remains a very reliable biomarker now. Our study showed that high concentrations of lactate dehydrogenase were associated with the occurrence of RMPP. A potential cause might be that lung tissue damage was more severe with RMPP than with NRMPP, resulting in the release of large amounts of lactate dehydrogenase from damaged cells.
Having assessed the potential risk factors including age, leukocyte count, neutrophil proportion, serum procalcitonin, and lactate dehydrogenase, we constructed a nomogram for prediction of RMPP. This nomogram allows for an individualized assessment of RMPP risk in children who continued to be treated with macrolide after the confirmation of MUMPP without antibiotic changes. Accordingly, continuation of macrolide may be used in patients with MUMPP at low risk of RMPP as predicted by the developed model.
Our study constructed and validated a visual and user-friendly nomogram for prediction of RMPP risk in children who continued to be treated with macrolide after the confirmation of MUMPP. However, the data were derived from a retrospective study, and the information may be biased, affecting the final results. In addition, the use of single IgM antibody for the detection of MPP is generally not accepted by hospitals in developed countries. Moreover, external validation of the nomogram model was not performed due to the small sample size, so we will carry out external validation of this model in a subsequent study.
Compared with other published papers,40–42 the enrolled patients in our study differed in two points: 1) patients were confirmed as macrolide-unresponsive MPP (MUMPP); 2) patients continued to be treated with macrolide (azithromycin) after the confirmation of MUMPP without antibiotic changes. In addition, the purpose of this study is different from other studies. The purpose of this study is to provide medication guidance for patients with MUMPP based on their risk of developing RMPP. According to the nomogram model, continuation of macrolide should be considered rather than second-line antibiotics including tetracyclines and fluoroquinolones for MUMPP children with low predictive risk of RMPP.
In conclusion, we constructed and validated a visual and user-friendly nomogram for individualized prediction of RMPP risk in children who continued to be treated with macrolide after the confirmation of MUMPP based on five variables including age, leukocyte count, neutrophil proportion, serum procalcitonin, and lactate dehydrogenase. According to the nomogram model, continuation of macrolide should be considered rather than second-line antibiotics including tetracyclines (doxycycline or minocycline) and fluoroquinolones for MUMPP children with low predictive values.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethical Approval
This study complies with the Declaration of Helsinki. The ethical committee of the Affiliated People’s Hospital of Ningbo University approved the study (No. 107-P-066).
Informed Consent
Written informed consents were obtained from patient’s guardians.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Conception and design: Qiaoyi Xie and Wei Cui.
Development of methodology: Xiaote Zhang.
Acquisition of data: Qiaoyi Xie and Wei Cui.
Analysis and interpretation of data: Xiaote Zhang and Yajiao Pang.
Writing, review, and/or revision of the manuscript: Xiaote Zhang and Yajiao Pang.
Study supervision: Qiaoyi Xie and Wei Cui.
Funding
This research received no external funding.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Lanks CW, Musani AI, Hsia DW. Community-acquired pneumonia and hospital-acquired pneumonia. Med Clin North Am. 2019;103(3):487–501. doi:10.1016/j.mcna.2018.12.008
2. Hung HM, Chuang CH, Chen YY, et al. Clonal spread of macrolide-resistant Mycoplasma pneumoniae sequence type-3 and type-17 with recombination on non-P1 adhesin among children in Taiwan. Clin Microbiol Infect. 2021;27(8):1169.e1161–1169.e1166. doi:10.1016/j.cmi.2020.09.035
3. Wu TH, Wang NM, Liu FC, et al. Macrolide resistance, clinical features, and cytokine profiles in Taiwanese children with Mycoplasma pneumoniae infection. Open Forum Infect Dis. 2021;8(9):ofab416.
4. Waites KB, Xiao L, Liu Y, Balish MF, Atkinson TP. Mycoplasma pneumoniae from the respiratory tract and beyond. Clin Microbiol Rev. 2017;30(3):747–809.
5. Kim SH, Lee E, Song ES. Clinical significance of pleural effusion in mycoplasma pneumoniae pneumonia in children. Pathogens. 2021;10(9):1.
6. Narita M. Classification of extrapulmonary manifestations due to mycoplasma pneumoniae infection on the basis of possible pathogenesis. Front Microbiol. 2016;7:23.
7. Amza A, Kadri B, Nassirou B, et al. Community-level association between clinical trachoma and ocular chlamydia infection after MASS azithromycin distribution in a mesoendemic region of Niger. Ophthalmic Epidemiol. 2019;26(4):231–237.
8. Levine A, Kori M, Kierkus J, et al. Azithromycin and metronidazole versus metronidazole-based therapy for the induction of remission in mild to moderate paediatric Crohn’s disease: a randomised controlled trial. Gut. 2019;68(2):239–247.
9. Waites KB, Crabb DM, Duffy LB. Comparative in vitro susceptibilities of human Mycoplasmas and ureaplasmas to a new investigational ketolide, CEM-101. Antimicrob Agents Chemother. 2009;53(5):2139–2141.
10. Yang HJ. Benefits and risks of therapeutic alternatives for macrolide resistant Mycoplasma pneumoniae pneumonia in children. Korean J Pediatr. 2019;62(6):199–205. doi:10.3345/kjp.2018.07367
11. Qu J, Chen S, Bao F, Gu L, Cao B. Molecular characterization and analysis of Mycoplasma pneumoniae among patients of all ages with community-acquired pneumonia during an epidemic in China. Int J Infect Dis. 2019;83:26–31. doi:10.1016/j.ijid.2019.03.028
12. Waites KB, Ratliff A, Crabb DM, et al. Macrolide-resistant Mycoplasma pneumoniae in the United States as determined from a national surveillance program. J Clin Microbiol. 2019;57(11):2. doi:10.1128/JCM.00968-19
13. Pereyre S, Goret J, Bébéar C. Mycoplasma pneumoniae: current knowledge on macrolide resistance and treatment. Front Microbiol. 2016;7:974. doi:10.3389/fmicb.2016.00974
14. Chen YC, Hsu WY, Chang TH. Macrolide-resistant Mycoplasma pneumoniae infections in pediatric community-acquired pneumonia. Emerg Infect Dis. 2020;26(7):1382–1391. doi:10.3201/eid2607.200017
15. Hsieh YC, Tsao KC, Huang CG, et al. Life-threatening pneumonia caused by macrolide-resistant Mycoplasma pneumoniae. Pediatr Infect Dis J. 2012;31(2):208–209. doi:10.1097/INF.0b013e318234597c
16. Tsai TA, Tsai CK, Kuo KC, Yu HR. Rational stepwise approach for Mycoplasma pneumoniae pneumonia in children. J Microbiol Immunol Infect. 2021;54(4):557–565. doi:10.1016/j.jmii.2020.10.002
17. Aliberti S, Dela Cruz CS, Amati F, Sotgiu G, Restrepo MI. Community-acquired pneumonia. Lancet. 2021;398(10303):906–919. doi:10.1016/S0140-6736(21)00630-9
18. Uehara S, Sunakawa K, Eguchi H, et al. Japanese guidelines for the management of respiratory infectious diseases in children 2007 with focus on pneumonia. Pediatr Int. 2011;53(2):264–276. doi:10.1111/j.1442-200X.2010.03316.x
19. Tong L, Huang S, Zheng C, Zhang Y, Chen Z. Refractory Mycoplasma pneumoniae pneumonia in children: early recognition and management. J Clin Med. 2022;11(10):1. doi:10.3390/jcm11102824
20. Sánchez AR, Rogers RS 3rd, Sheridan PJ. Tetracycline and other tetracycline-derivative staining of the teeth and oral cavity. Int J Dermatol. 2004;43(10):709–715. doi:10.1111/j.1365-4632.2004.02108.x
21. Kawai Y, Miyashita N, Kubo M, et al. Therapeutic efficacy of macrolides, minocycline, and tosufloxacin against macrolide-resistant Mycoplasma pneumoniae pneumonia in pediatric patients. Antimicrob Agents Chemother. 2013;57(5):2252–2258. doi:10.1128/AAC.00048-13
22. Grady RW. Systemic quinolone antibiotics in children: a review of the use and safety. Expert Opin Drug Saf. 2005;4(4):623–630. doi:10.1517/14740338.4.4.623
23. Ha SG, Oh KJ, Ko K-P. Therapeutic efficacy and safety of prolonged macrolide, corticosteroid, doxycycline, and levofloxacin against macrolide-unresponsive Mycoplasma pneumoniae pneumonia in children. J Korean Med Sci. 2018;33(43):e268. doi:10.3346/jkms.2018.33.e268
24. Lai JF, Zindl CL, Duffy LB, et al. Critical role of macrophages and their activation via MyD88-NFκB signaling in lung innate immunity to Mycoplasma pneumoniae. PLoS One. 2010;5(12):e14417. doi:10.1371/journal.pone.0014417
25. Roifman CM, Rao CP, Lederman HM, et al. Increased susceptibility to Mycoplasma infection in patients with hypogammaglobulinemia. Am J Med. 1986;80(4):590–594. doi:10.1016/0002-9343(86)90812-0
26. Foy HM, Ochs H, Davis SD, Kenny GE, Luce RR. Mycoplasma pneumoniae infections in patients with immunodeficiency syndromes: report of four cases. J Infect Dis. 1973;127(4):388–393. doi:10.1093/infdis/127.4.388
27. Wang M, Wang Y, Yan Y, et al. Clinical and laboratory profiles of refractory Mycoplasma pneumoniae pneumonia in children. Int J Infect Dis. 2014;29:18–23. doi:10.1016/j.ijid.2014.07.020
28. Metzemaekers M, Gouwy M, Proost P. Neutrophil chemoattractant receptors in health and disease: double-edged swords. Cell Mol Immunol. 2020;17(5):433–450.
29. Liew PX, Kubes P. The neutrophil’s role during health and disease. Physiol Rev. 2019;99(2):1223–1248.
30. Silvestre-Roig C, Hidalgo A, Soehnlein O. Neutrophil heterogeneity: implications for homeostasis and pathogenesis. Blood. 2016;127(18):2173–2181.
31. Headland SE, Norling LV. The resolution of inflammation: principles and challenges. Semin Immunol. 2015;27(3):149–160.
32. Rossaint J, Margraf A, Zarbock A. Role of platelets in leukocyte recruitment and resolution of inflammation. Front Immunol. 2018;9:2712.
33. Chen Z, Shao X, Dou X, et al. Role of the Mycoplasma pneumoniae/Interleukin-8/neutrophil axis in the pathogenesis of pneumonia. PLoS One. 2016;11(1):e0146377.
34. Piacentini E, Sánchez B, Arauzo V, et al. Procalcitonin levels are lower in intensive care unit patients with H1N1 influenza A virus pneumonia than in those with community-acquired bacterial pneumonia. A pilot study. J Crit Care. 2011;26(2):201–205.
35. Cao X. Monitoring mycoplasma pneumoniae-specific antibody, C-reactive protein, and procalcitonin levels in children with Mycoplasma pneumonia is important. Comput Math Methods Med. 2022;2022:7976858.
36. Liu TY, Lee WJ, Tsai CM, et al. Serum lactate dehydrogenase isoenzymes 4 plus 5 is a better biomarker than total lactate dehydrogenase for refractory Mycoplasma pneumoniae pneumonia in children. Pediatr Neonatol. 2018;59(5):501–506.
37. Lu A, Wang C, Zhang X, Wang L, Qian L. Lactate dehydrogenase as a biomarker for prediction of refractory Mycoplasma pneumoniae pneumonia in children. Respir Care. 2015;60(10):1469–1475.
38. Zhang Y, Zhou Y, Li S, et al. The clinical characteristics and predictors of refractory Mycoplasma pneumoniae pneumonia in children. PLoS One. 2016;11(5):e0156465.
39. Zhang Y, Mei S, Zhou Y, et al. Cytokines as the good predictors of refractory Mycoplasma pneumoniae pneumonia in school-aged children. Sci Rep. 2016;6:37037.
40. Wen J, Su Y, Sun H, et al. The combination of initial markers to predict refractory Mycoplasma pneumoniae pneumonia in Chinese children: a case control study. Respir Res. 2021;22(1):89.
41. Cheng S, Lin J. Development and validation of a simple-to-use nomogram for predicting refractory Mycoplasma pneumoniae pneumonia in children. Pediatr Pulmonol. 2020;55(4):968–974.
42. Shen F, Dong C, Zhang T, et al. Development of a nomogram for predicting refractory Mycoplasma pneumoniae pneumonia in children. Front Pediatr. 2022;10:813614.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.