Back to Journals » Risk Management and Healthcare Policy » Volume 18
Construction and Evaluation of Nomogram Prediction Model for Urinary Tract Infection After Transurethral Bipolar Plasmakinetic Prostatectomy
Authors Diao P, Zhong S, Chen D, Wang H, Zheng Y, Wang J, Tian C
Received 11 May 2025
Accepted for publication 8 December 2025
Published 17 December 2025 Volume 2025:18 Pages 3901—3910
DOI https://doi.org/10.2147/RMHP.S539684
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Pengfei Diao,* Suquan Zhong,* Dong Chen, Hangtao Wang, Yiying Zheng, Jinhua Wang, Chao Tian
Department of Urology, Yuebei People’s Hospital, Shaoguan, Guangdong, 512026, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Tian, Department of Urology, Yuebei People’s Hospital, Huimin South Road, Wujiang District, Shaoguan, Guangdong, 512026, People’s Republic of China, Email [email protected]
Objective: To explore the risk factors of urinary tract infection after transurethral bipolar plasmakinetic prostatectomy (TUPKP) in patients with prostatic hyperplasia (BPH), to construct a nomogram model for predicting postoperative urinary tract infection, and evaluate the differentiation and consistency of the model.
Methods: A total of 580 BPH patients who underwent TUPKP between October 2016 and October 2022 were included as the modeling group, and 115 patients treated from November 2022 to November 2024 formed the validation group. Patients were classified into UTI and non-UTI groups based on the occurrence of UTI within 1 month postoperatively. Clinical data were analyzed using univariate and multivariate logistic regression to identify risk factors. A nomogram was constructed using R software, and its performance was assessed with ROC and calibration curves.
Results: The incidence of postoperative UTI in the modeling group was 14.83%. Compared with the non-UTI group, the UTI group had significantly higher age, diabetes prevalence, preoperative catheterization, and routine nursing ratio, along with longer operation and catheterization times, and shorter antibiotic use duration (P< 0.05). Multivariate analysis revealed that age (OR=1.061), diabetes (OR=1.889), operation time (OR=1.063), and indwelling catheter time (OR=1.912) were independent risk factors (P< 0.05). The nomogram demonstrated good discrimination (AUC=0.825, 95% CI: 0.780– 0.869) and calibration (Hosmer-Lemeshow test P=0.390). External validation showed similar performance (AUC=0.818, 95% CI: 0.711– 0.925) with good consistency.
Conclusion: Age, diabetes, duration of surgery, and postoperative indwelling catheter time are risk factors for urinary tract infection in patients with benign prostatic hyperplasia undergoing TUPKP. The constructed nomogram model demonstrates good discrimination and consistency.
Keywords: prostatic hyperplasia, transurethral bipolar plasmakinetic prostatectomy, urinary tract infection, risk factors
Introduction
Benign prostatic hyperplasia (BPH) is a common urological condition in men, and its occurrence is closely related to age. The likelihood of developing BPH increases with advancing age; therefore, most patients with this condition in clinical practice are elderly men.1,2 Surgical treatment is generally considered when patients present with significant urinary obstruction, which can be defined based on objective findings such as hydronephrosis on imaging, persistent high post-void residual urine, or recurrent urinary retention that does not respond to medical therapy. Symptom severity assessed by the IPSS score may not always correlate with the degree of obstruction, and prostate size alone is also an imperfect predictor; therefore, clinical decisions are made using a combination of imaging, laboratory, and functional assessments.3,4 Transurethral bipolar plasmakinetic prostatectomy (TUPKP) is a major surgical procedure for treating BPH, offering advantages such as less intraoperative and postoperative bleeding and faster recovery. However, some patients still develop postoperative complications like urinary tract infections, severely impacting their normal lives.5,6 At present, there is no consensus in clinical research regarding the risk factors for postoperative urinary tract infection in patients with benign prostatic hyperplasia.6 Therefore, individualized and precise prediction of the risk of post-TUPKP urinary tract infection in BPH patients holds significant clinical importance. Currently, clinical studies often focus on using Logistic regression models to analyze risk factors affecting postoperative urinary tract infections after prostatectomy in BPH patients. The identified high-risk factors can effectively assess the likelihood of postoperative UTIs,7,8 but they cannot provide individualized, precise prediction of the risk. Nomogram models, however, can integrate risk factors identified through multivariate Logistic regression analysis to provide individualized and precise prediction of the occurrence of specific adverse events.9 Therefore, this study aims to investigate the risk factors for post-TUPKP urinary tract infection in BPH patients and construct a nomogram model for individualized prediction, providing a reference basis for personalized prevention and treatment of postoperative UTIs.
Materials and Methods
Study Subjects
A total of 580 BPH patients admitted to the Department of Urology, Yuebei People’s Hospital between October 2016 and October 2022 were selected as the modeling group. Additionally, 115 BPH patients admitted to the same hospital between November 2022 and October 2024 were selected as the validation group. Inclusion criteria were: (1) Diagnosis confirmed by clinical symptoms, signs, and ultrasound examination, and verified by postoperative pathological examination; (2) All patients underwent TUPKP treatment; (3) No preoperative urinary tract infection; (4) Both patients and their families provided informed consent and signed the consent form. Exclusion criteria were: (1) Severe liver or kidney dysfunction; (2) Patients with concurrent urethral stricture or bladder stones; (3) History of previous urethral surgery; (4) Incomplete clinical data; (5) Presence of cognitive or consciousness impairment. This study was approved by the Medical Ethics Committee of our hospital. See follow Figure 1.
 |
Figure 1 Flowchart of case selection. |
Surgical Method
Epidural anesthesia was administered. Patients were placed in the lithotomy position. The surgery was performed using a transurethral bipolar plasmakinetic resection system (Gyrus, UK). The irrigation fluid was 0.9% sodium chloride, used for continuous flushing. A Gyrus 27F resectoscope was inserted transurethrally. Using the bladder neck and verumontanum as distal landmarks, a deep incision reaching the capsule was made from the 6 o’clock position of the bladder neck to the verumontanum. The left and right lateral lobes were resected along the capsule, and the gland near the verumontanum was trimmed. Hemostasis of the surgical wound was then performed. Postoperatively, an F22 three-way Foley catheter (The material is medical-grade silicone) was routinely indwelled, and continuous bladder irrigation with normal saline was maintained for 2–5 days.
Diagnostic Criteria for Urinary Tract Infection
(1) Urine sediment (Urine was collected using a catheterization method on postoperative day 3) analysis showing >8 white blood cells per high-power field; (2) Positive bacterial culture with a colony count >105/mL. Diagnosis of urinary tract infection was confirmed if both criteria were met.10 Patients were divided into a UTI group and a non-UTI group based on whether they developed a urinary tract infection within 1 month postoperatively.
Clinical Data Collection
Clinical data collected for both groups included: age, disease duration, gender, body mass index (BMI), hypertension, diabetes mellitus, preoperative indwelling catheterization, intraoperative blood loss, operation time, duration of postoperative indwelling catheterization, intraoperative prostate resection volume (calculated by weighing the resected tissue and converting to volume assuming a density of 1 g/cm3), duration of antibiotic use, and nursing method (routine care or evidence-based nursing). Routine nursing care included postoperative monitoring of vital signs, catheter and wound management, diet and activity regulation, and pain and complication management. Vital signs, including blood pressure, heart rate, respiration, and temperature, were monitored hourly within the first 24 hours after surgery, with particular attention to bleeding and infection. A low-grade fever could occur within 3–5 days postoperatively; however, persistent fever above 38 °C warranted evaluation for infection. The urinary catheter was kept unobstructed to avoid kinking or compression, urine color was observed, the urethral meatus was disinfected daily, and the urine bag was replaced regularly to prevent retrograde infection. Patients were kept fasting for 6–8 hours postoperatively, then gradually transitioned to a liquid or semi-liquid diet, avoiding spicy or irritating foods. They were encouraged to drink more than 2000 mL of water daily to promote urination and flush the urethra. Bed exercises were initiated 24 hours postoperatively, with gradual ambulation after 2–3 days, while avoiding heavy lifting or strenuous activity. Mild pain was managed with oral nonsteroidal anti-inflammatory drugs (NSAIDs), while severe pain required reassessment of the analgesic regimen. Patients were closely monitored for bleeding, urinary retention, and incontinence. Evidence-based nursing interventions included infection prevention, early mobilization, thrombosis prevention, and health education. According to clinical guidelines, prophylactic antibiotics administered within 48 hours after surgery helped reduce the risk of urinary tract infection, and the prescribed course was completed as directed. During bladder irrigation, the flow rate (80–100 drops/min) and temperature (near body temperature) were controlled to minimize bladder irritation. Ankle pump exercises were initiated 24 hours after surgery, followed by gradual ambulation after 48 hours to reduce the risk of deep vein thrombosis. Before discharge, patients received education on recognizing signs of infection (eg, fever, painful urination) and were informed about the indications for seeking immediate medical attention.
Statistical Methods
Data were processed using SPSS 19.0. Measurement data (eg, age, disease duration) conforming to a normal distribution were described as mean ± standard deviation (mean ± SD), and comparisons between the two groups were made using the t-test. Count data (eg, hypertension, diabetes) were described as rates (%), and comparisons between the two groups were made using the chi-square (χ2) test. Univariate Logistic regression analysis was performed on 10 factors, including age, disease duration, and hypertension. Receiver operating characteristic (ROC) curves were plotted to determine the optimal cut-off values for factors related to post-TUPKP urinary tract infection in BPH patients. Based on these optimal cut-off values, relevant factors were converted into categorical data for multivariate Logistic regression analysis to identify the independent risk factors for post-TUPKP UTI in BPH patients. The identified risk factors were incorporated into R software version 3.6.3 and the “rms” package (https://yikeshu.shinyapps.io/inomogram/) to construct a nomogram model for predicting post-TUPKP urinary tract infection in BPH patients. ROC curves were plotted to evaluate the discriminative ability of the nomogram model for predicting UTI. Calibration curves were plotted to assess the consistency (or calibration) of the nomogram model’s predictions. A two-sided P < 0.05 was considered statistically significant.
Results
Univariate Analysis of Post-TUPKP Urinary Tract Infection in BPH Patients in the Modeling Group
In the modeling group of 580 BPH patients, 86 developed urinary tract infection (UTI) after TUPKP, resulting in an incidence rate of 14.83% (86/580). Patients in the UTI group were significantly older, had a higher proportion of diabetes mellitus, a higher proportion with preoperative indwelling catheterization, and a higher proportion receiving routine nursing care compared to the non-UTI group. Furthermore, the operation time and duration of postoperative indwelling catheterization were significantly longer in the UTI group, while the duration of antibacterial drug usage was significantly shorter (P < 0.05). There were no statistically significant differences in the other indicators between the two groups (P > 0.05). See Table 1.
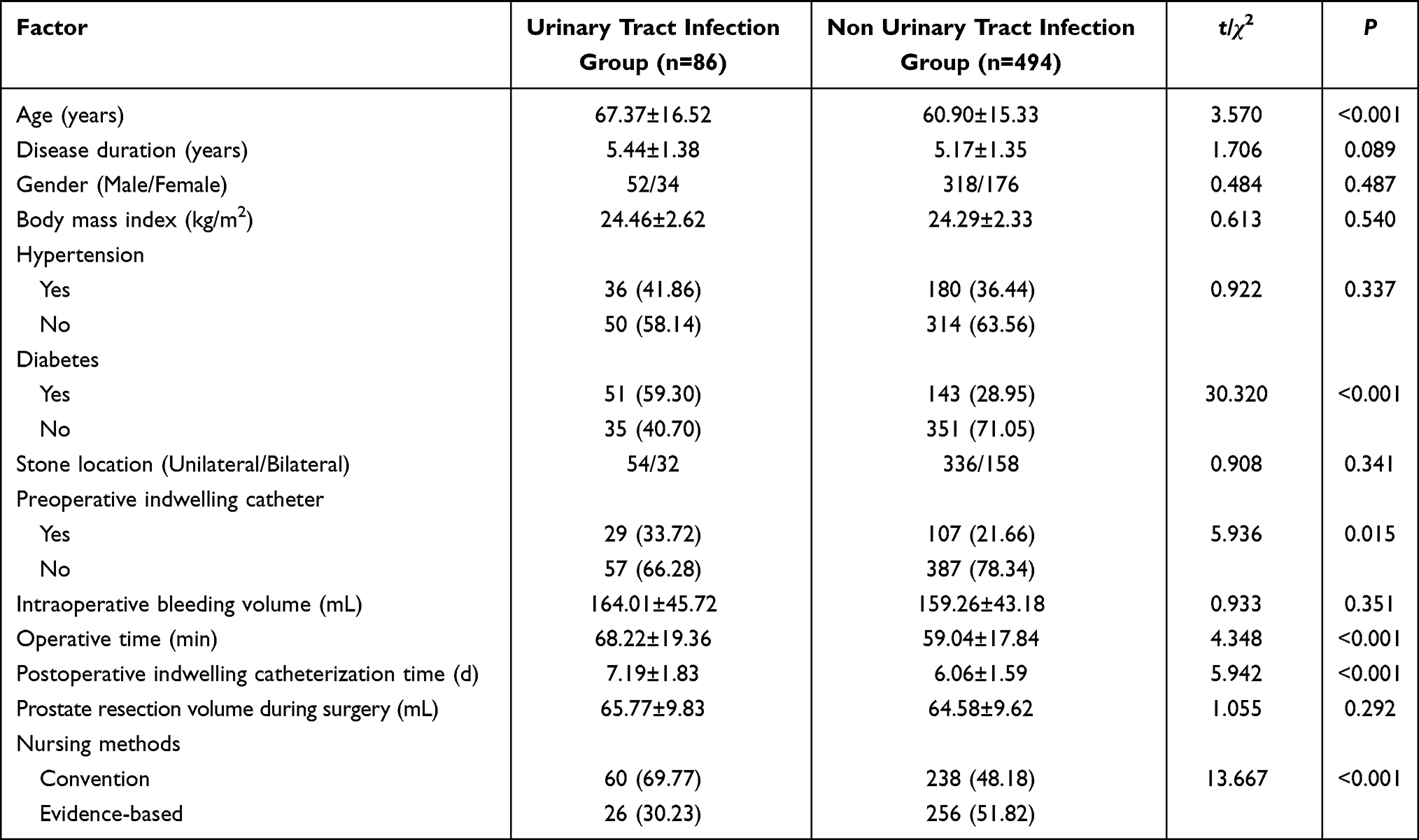 |
Table 1 Univariate Analysis of Post-TUPKP Urinary Tract Infection in BPH Patients in the Modeling Group [n (%)/(mean±SD)] |
ROC Curve Analysis of Factors Related to Post-TUPKP Urinary Tract Infection in BPH Patients
This study utilized receiver operating characteristic (ROC) curves to determine the optimal cut-off values for the continuous variables: age, operation time, duration of postoperative indwelling catheterization, and duration of antibacterial drug usage. See Table 2. Based on these optimal cut-off values, age, operation time, duration of postoperative indwelling catheterization, and duration of antibacterial drug usage were converted into categorical data for multivariate Logistic regression analysis.
 |
Table 2 Results of ROC Curve Analysis for Factors Related to Postoperative Urinary Tract Infection |
Multivariate Logistic Regression Analysis of Post-TUPKP Urinary Tract Infection in BPH Patients
The occurrence of post-TUPKP urinary tract infection (UTI) in BPH patients was set as the dependent variable (non-occurrence = 0, occurrence = 1). Variables that were statistically significant in the univariate analysis (age, diabetes mellitus, preoperative indwelling catheterization, operation time, duration of postoperative indwelling catheterization, duration of antibacterial drug usage, and nursing method) were included as independent variables. The variable assignment method is shown in Table 3. Multivariate Logistic regression analysis revealed that age (OR=1.061, 95% CI=1.034–1.088), diabetes mellitus (OR=1.889, 95% CI=1.274–2.801), operation time (OR=1.063, 95% CI=1.040–1.086), and duration of postoperative indwelling catheterization (OR=1.912, 95% CI=1.498–2.439) were independent risk factors for post-TUPKP UTI in BPH patients (P < 0.05). See Table 4.
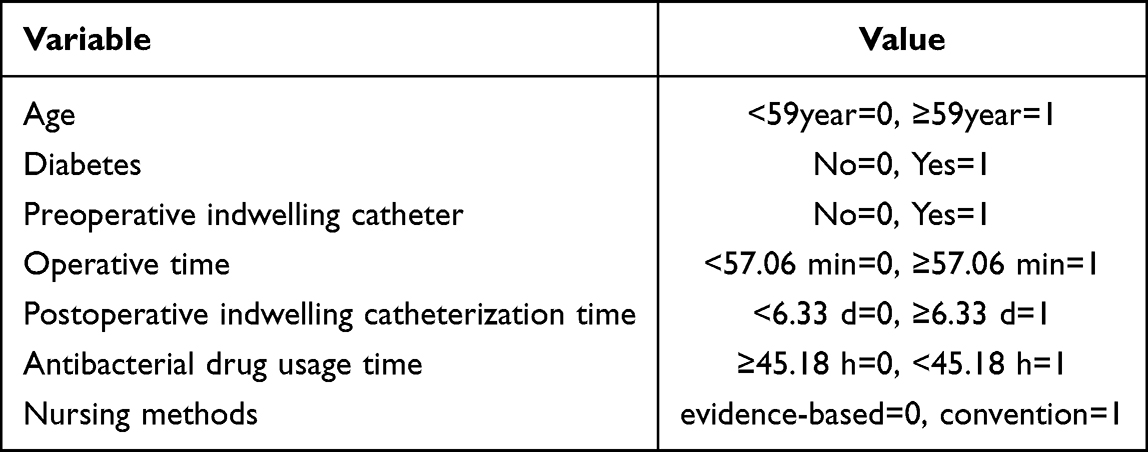 |
Table 3 Variable Assignment Method |
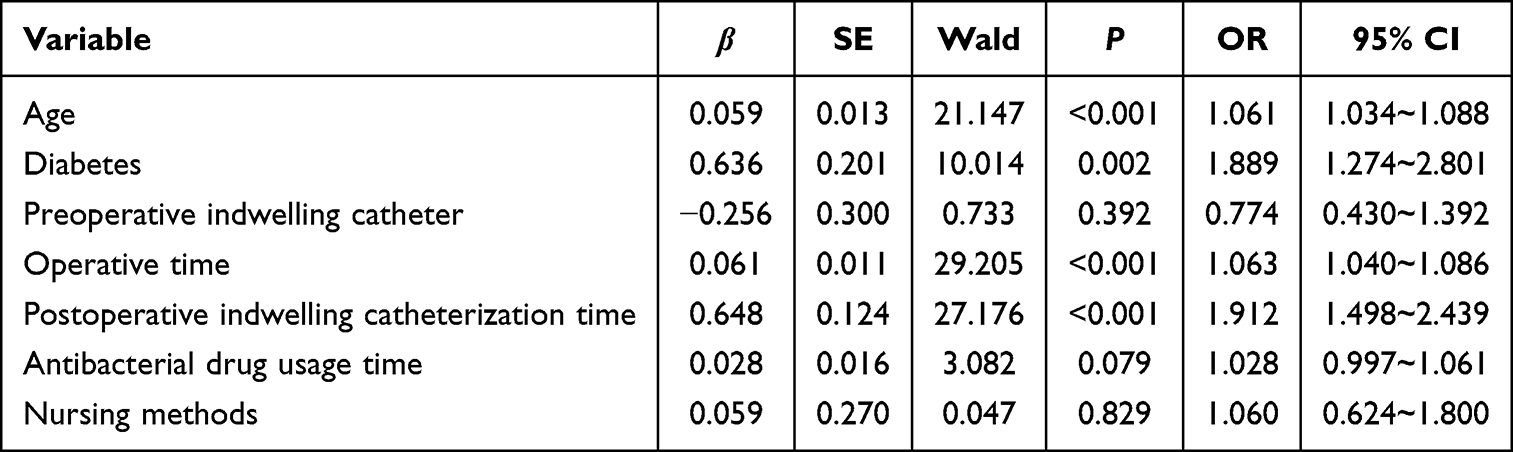 |
Table 4 Multivariate Logistic Regression Analysis of Post-TUPKP Urinary Tract Infection in BPH Patients |
Construction of the Nomogram Model for Predicting Post-TUPKP Urinary Tract Infection in BPH Patients
The identified independent risk factors—age, diabetes mellitus, operation time, and duration of postoperative indwelling catheterization—were incorporated using R software to construct a nomogram predicting the risk of post-TUPKP urinary tract infection in BPH patients. The results showed that for every 5-year increase in age, the nomogram score increases by 8.1 points; for every 5-minute increase in operation time, the score increases by 8.3 points; for every 0.5-day increase in the duration of postoperative indwelling catheterization, the score increases by 8.9 points; and the presence of diabetes mellitus contributes 17.5 points. See Figure 2.
 |
Figure 2 Nomogram constructed for predicting post-TUPKP urinary tract infection in BPH patients. |
Internal Validation of the Nomogram Model for Predicting Post-TUPKP Urinary Tract Infection in BPH Patients
Internal validation showed that the area under the receiver operating characteristic (ROC) curve (AUC) for the nomogram predicting post-TUPKP urinary tract infection (UTI) in BPH patients was 0.825 (95% CI = 0.780–0.869), indicating good discrimination (Figure 3A). The calibration curve demonstrated good consistency between the nomogram-predicted probabilities and the actual observed outcomes, with a slope close to 1 (Figure 3B). The Hosmer-Lemeshow goodness-of-fit test result was χ2 = 8.460 (P = 0.390), further supporting the model’s good calibration.
 |
Figure 3 Internal validation of the nomogram model. (A) ROC curve; (B) Calibration curve. |
External Validation of the Nomogram Model for Predicting Post-TUPKP Urinary Tract Infection in BPH Patients
In the validation group comprising 115 BPH patients, 19 developed post-TUPKP urinary tract infection (UTI), yielding an incidence rate of 16.52% (19/115). Patients in the UTI group were significantly older and had a higher proportion of diabetes mellitus compared to the non-UTI group; their operation time and duration of postoperative indwelling catheterization were also significantly longer (P < 0.05). See Table 5. External validation of the nomogram yielded an AUC of 0.818 (95% CI = 0.711–0.925), confirming its good discriminative ability (Figure 4A). The calibration curve also showed good consistency, with a slope approaching 1 (Figure 4B).
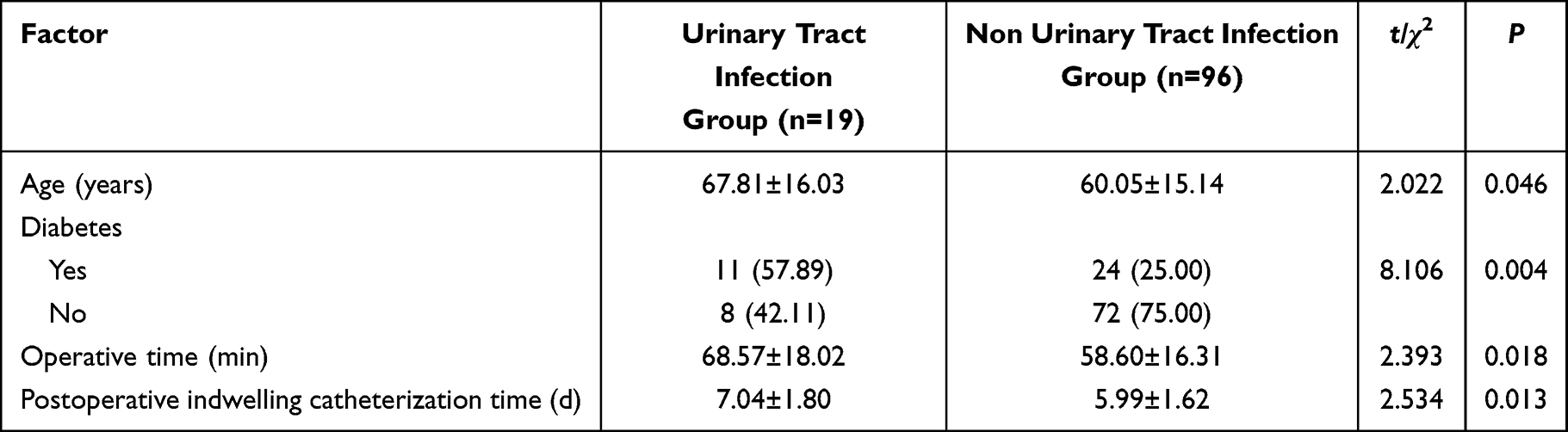 |
Table 5 Comparison of Clinical Data Between UTI and Non-UTI Groups in the Validation Set [n (%)/(mean±SD)] |
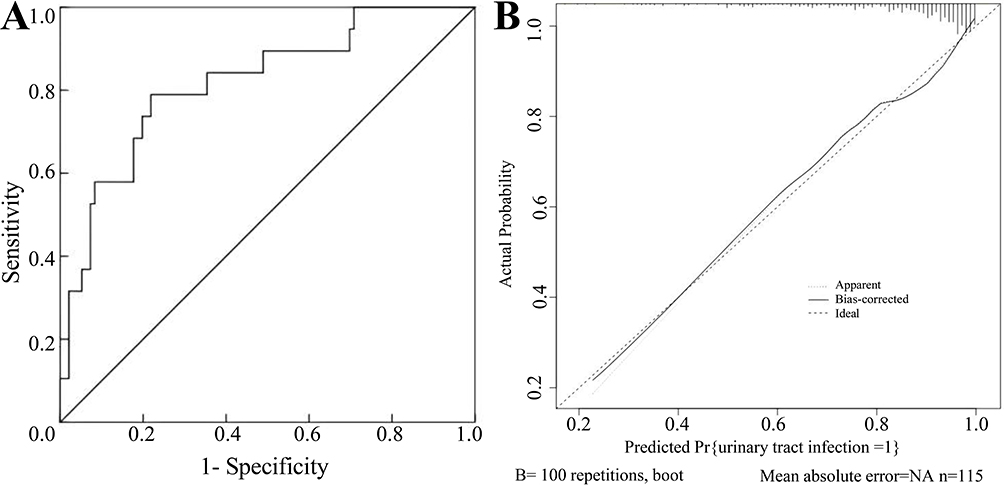 |
Figure 4 External validation of the nomogram model. (A) ROC curve; (B) Calibration curve. |
DCA Curve
The Decision Curve Analysis (DCA) curve was plotted with the high-risk threshold probability on the x-axis and the net benefit on the y-axis. The results indicated that applying this nomogram to predict post-TUPKP urinary tract infection in BPH patients provides considerable clinical net benefit when the threshold probability ranges between 0.08 and 0.92 (Figure 5).
 |
Figure 5 Decision Curve Analysis (DCA) curve. |
Discussion
In this study, the incidence of post-TUPKP urinary tract infection (UTI) among the 580 benign prostatic hyperplasia (BPH) patients was 14.83%. Research indicates that postoperative UTI not only increases patient suffering but also adversely affects treatment outcomes.11 Therefore, identifying the risk factors for post-TUPKP UTI in BPH patients is crucial for guiding the early prevention and treatment of these infections.
This study investigated 10 potential factors (age, disease duration, hypertension, diabetes mellitus, preoperative indwelling catheterization, intraoperative blood loss, operation time, duration of postoperative indwelling catheterization, duration of antibacterial drug use, and nursing method) through univariate and multivariate Logistic regression analyses. The results identified age, diabetes mellitus, operation time, and duration of postoperative indwelling catheterization as independent risk factors for post-TUPKP UTI in BPH patients. Nomograms integrate significant risk factors identified from multivariate models into a graphical tool composed of aligned scales, enhancing readability and enabling personalized prediction of clinical outcomes or adverse event risks, thereby demonstrating high clinical practicality.12,13 Previous research has validated the use of nomograms14–16 for predicting various clinical scenarios, such as postoperative recurrence in patients with intermediate-risk non-muscle-invasive bladder cancer, the dynamic risks of recurrence and progression following transurethral resection of bladder tumor with intravesical Bacillus Calmette-Guérin (BCG) instillation, and the risk of reoperation due to secondary hemorrhage after transurethral resection of the prostate (TURP). Based on the four identified risk factors (age, diabetes mellitus, operation time, and duration of postoperative indwelling catheterization), this study developed a nomogram to predict the risk of post-TUPKP UTI in BPH patients. This model helps urology medical and nursing staff to more intuitively assess the impact weight of each risk factor on the probability of postoperative UTI, enabling the identification of high-risk patients and the implementation of personalized preventive strategies to lower UTI incidence.
Our nomogram model revealed several key findings regarding risk factors. For every 5-year increase in age, the nomogram score increased by 8.1 points, corresponding to a higher risk of postoperative UTI. This is likely because elderly patients generally exhibit a gradual decline in various bodily functions, leading to reduced resistance to bacteria and lower tolerance to surgical trauma, making them more prone to postoperative infections.17 The model also showed that for every 5-minute prolongation of the operation time, the score increased by 8.3 points, correlating with an increased risk of postoperative UTI. This may be attributed to surgical trauma suppressing the body’s immune function, thereby increasing susceptibility to infection; longer surgical durations might inherently increase exposure and risk.18 Furthermore, for every 0.5-day extension in the duration of postoperative indwelling catheterization, the nomogram score increased by 8.9 points, indicating a heightened risk of postoperative UTI. Indwelling catheters, while necessary for managing retention, are invasive and disrupt the urethral barrier, facilitating bacterial ascension and colonization in the urinary tract, thus increasing infection risk.19 In addition, the results of this study showed that patients with diabetes had 17.5 points higher nomogram scores than those without diabetes, which was similar to the findings reported by Gravas et al.20 This significant contribution is likely due to factors such as higher urinary glucose levels in diabetic patients, which promote bacterial growth, and impaired immune cell function (eg, macrophages, neutrophils) due to hyperglycemia, increasing susceptibility to postoperative UTI.21 In light of these findings, strategies to mitigate UTI risk should include heightened vigilance for older BPH patients, minimizing surgical duration and postoperative catheterization time whenever feasible, and ensuring adequate preoperative glycemic control for diabetic patients.
This study employed ROC curves and calibration curves to evaluate the performance of the developed nomogram for predicting post-TUPKP UTI in BPH patients. The internal validation yielded an AUC of 0.825, signifying good discriminative ability. The calibration plot showed good agreement between predicted and observed outcomes (slope close to 1), supported by a non-significant Hosmer-Lemeshow test (χ2 = 8.460, P = 0.390), indicating good calibration. External validation further confirmed the model’s good discrimination and consistency, supporting its potential clinical value. Decision Curve Analysis (DCA) demonstrated that the nomogram offers considerable clinical net benefit across a wide range of threshold probabilities (0.08 to 0.92) for predicting post-TUPKP UTI. By integrating multiple risk factors, the nomogram provides individualized risk assessment and a basis for precise intervention in the prevention of postoperative urinary tract infection. It can help physicians quickly determine whether enhanced monitoring or adjustment of antibiotic use is needed, allowing for early identification and timely treatment of high-risk patients. While this study confirms the favorable performance of the nomogram in predicting postoperative urinary tract infection, the sample size was relatively small, and no multicenter validation was conducted. The analysis was based on a limited set of factors, which might introduce potential bias. Future studies with larger sample sizes and more influencing variables are needed for further validation.
Conclusions
In conclusion, age, diabetes mellitus, operation time, and duration of postoperative indwelling catheterization were identified as risk factors for urinary tract infection after TUPKP in patients with benign prostatic hyperplasia. The nomogram model developed based on these four risk factors demonstrated good discrimination and calibration, providing valuable guidance for developing targeted and individualized prevention and treatment strategies in clinical practice.
Data Sharing Statement
Data is available from the corresponding author on request.
Ethics Approval and Consent to Participate
This study involving human participants was in accordance with the ethical standards of the Medical Ethics Committee of Yuebei People’s Hospital (No: KY-2023-002) and with the 1964 Helsinki Declaration. And obtain the informed consent form of the patient.
Acknowledgments
Pengfei Diao and Suquan Zhong contributed equally as first authors.
Funding
No funding was provided for this research.
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Trifunovski A, Severova G, Atanasova A, et al. Percutaneous nephrostomy as a procedure in the treatment of urinary tract obstruction - experiences in the University Clinic of Urology in Skopje. Prilozi. 2024;45(1):31–40. doi:10.2478/prilozi-2024-0004
2. Zhou X-Z, Huang P, Wu Y-K, et al. Autophagy in benign prostatic hyperplasia: insights and therapeutic potential. BMC Urol. 2024;24(1):198. doi:10.1186/s12894-024-01585-7
3. Lokeshwar SD, Harper BT, Webb E, et al. Epidemiology and treatment modalities for the management of benign prostatic hyperplasia. Transl Androl Urol. 2019;8(5):529–539. doi:10.21037/tau.2019.10.01
4. Haile ES, Sotimehin AE, Gill BC. Medical management of benign prostatic hyperplasia. Cleve Clin J Med. 2024;91(3):163–170. doi:10.3949/ccjm.91a.23027
5. Deng W, Chen L, Liu X, et al. Bipolar plasmakinetic transurethral enucleation and resection versus bipolar plasmakinetic transurethral resection for surgically treating large (≥60 g) prostates: a propensity score-matched analysis with a 3-year follow-up. Minerva Urol Nephrol. 2020;73(3):376–383. doi:10.23736/S2724-6051.20.03804-7
6. Otaola-Arca H, Álvarez-Ardura M, Molina-Escudero R, et al. A prospective randomized study comparing bipolar plasmakinetic transurethral resection of the prostate and monopolar transurethral resection of the prostate for the treatment of Benign Prostatic Hyperplasia: efficacy, sexual function, Quality of Life, and complications. Int Braz J Urol. 2021;47(1):131–144. doi:10.1590/S1677-5538.IBJU.2019.0766
7. Qi Q, Hu Y, Hou B, et al. Risk factors and nomogram for predicting urinary tract infection in patients with ureterolithiasis complicated with hydronephrosis. Transl Androl Urol. 2024;13(9):1946–1954. doi:10.21037/tau-24-217
8. Rabi R, Enaya A, Jomaa DM, et al. Catheter-associated urinary tract infections in critical care: understanding incidence, risk factors, and pathogenic causes in Palestine. PLoS One. 2024;19(8):e0309755. doi:10.1371/journal.pone.0309755
9. Lee YJ, Lee JK, Kim JJ, et al. Development and validation of a clinical nomogram predicting bladder outlet obstruction via routine clinical parameters in men with refractory nonneurogenic lower urinary tract symptoms. Asian J Androl. 2019;21(5):486–492. doi:10.4103/aja.aja_127_18
10. Nelson Z, Aslan AT, Beahm NP, et al. Guidelines for the prevention, diagnosis, and management of urinary tract infections in pediatrics and adults: a WikiGuidelines Group Consensus Statement. JAMA Network Open. 2024;7(11):e2444495.
11. Zeng X-T, Jin Y-H, Liu T-Z, et al. Clinical practice guideline for transurethral plasmakinetic resection of prostate for benign prostatic hyperplasia (2021 Edition). Mil Med Res. 2022;9(1):14. doi:10.1186/s40779-022-00371-6
12. Wang C, Huang H-Z, He Y, et al. A new nomogram based on early postoperative NLR for predicting infectious complications after gastrectomy. Cancer Manag Res. 2020;12:881–889. doi:10.2147/CMAR.S238530
13. Zhu F, Li Y, Guo Z, et al. Nomogram to predict postoperative intra-abdominal septic complications after bowel resection and primary anastomosis for Crohn’s disease. Dis Colon Rectum. 2020;63(5):629–638. doi:10.1097/DCR.0000000000001602
14. Xu M-Y, Sun J-X, Xiang Y-X, et al. A novel nomogram for predicting post-operative recurrence for patients with intermediate and high-risk non-muscle invasive bladder cancer after thulium laser resection of bladder tumors or conventional transurethral resection of bladder tumors followed by intravesical bacille Calmette-Guérin immunotherapy. Transl Androl Urol. 2025;14(1):91–102. doi:10.21037/tau-24-535
15. Sun J-X, An Y, Xu M-Y, et al. Development of a dynamic risk system for predicting the risk of recurrence and progression in patients with non-muscle-invasive bladder cancer after thulium laser resection of bladder tumor or transurethral resection of bladder tumor followed by intravesical BCG instillation. Front Oncol. 2023;13:1133161. doi:10.3389/fonc.2023.1133161
16. Gu Z, Zheng Z, Zhang W, et al. The development and assessment of a predicting nomogram for the recovery of immediate urinary continence following laparoscopic radical prostatectomy. Front Surg. 2022;9:1071093. doi:10.3389/fsurg.2022.1071093
17. Farsi AH. Risk factors and outcomes of postoperative catheter-associated urinary tract infection in colorectal surgery patients: a retrospective cohort study. Cureus. 2021;13(5):e15111. doi:10.7759/cureus.15111
18. Lim EJ, Castellani D, Somani BK, et al. High-power holmium laser versus thulium fiber laser for endoscopic enucleation of the prostate in patients with glands larger than 80 mL: results from the Prostate Endoscopic EnucLeation study group. Prostate Int. 2024;12(1):40–45. doi:10.1016/j.prnil.2023.12.001
19. Shuai M, Li Y. Indwelling catheter increases the risk of urinary tract infection in total knee arthroplasty: a meta-analysis of randomized controlled trials. Medicine. 2021;100(15):e25490.
20. Gravas S, De Nunzio C, Campos Pinheiro L, et al. Development and validation of a clinical nomogram to predict prostatic inflammation in men with lower urinary tract symptoms. Prostate Cancer Prostatic Dis. 2024;28(2):405–410. doi:10.1038/s41391-024-00857-5
21. Confederat L-G, Condurache M-I, Alexa R-E, et al. Particularities of urinary tract infections in diabetic patients: a concise review. Medicina. 2023;59(10):1747. doi:10.3390/medicina59101747
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Associated Factors of Urinary Tract Infection in Patients with Diabetic Neuropathy: A Hospital-Based Cross-Sectional Study
Wang X, Wang Y, Luo L, Tan L, Cai W, Chen L, Ren W
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1261-1270
Published Date: 3 May 2023