Back to Journals » Advances in Medical Education and Practice » Volume 17
Conscientiousness and Academic Performance in Medical Students: A Systematic Review Across Training Stages and Assessment Types
Authors Qazi S ![]() , Shahab R
, Shahab R ![]() , Siddiqui IA, Hossain A, Syed Z, Oloriegbe MG, Akhtar Siddiqui A, Mazhar MA
, Siddiqui IA, Hossain A, Syed Z, Oloriegbe MG, Akhtar Siddiqui A, Mazhar MA ![]() , Obeidat A
, Obeidat A ![]()
Received 20 January 2026
Accepted for publication 8 April 2026
Published 15 April 2026 Volume 2026:17 591397
DOI https://doi.org/10.2147/AMEP.S591397
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Sadia Qazi,1 Rida Shahab,2 Iman Akhtar Siddiqui,2 Afsana Hossain,2 Zahra Syed,2 Maryam G Oloriegbe,2 Asma Akhtar Siddiqui,2 Muhammad Atif Mazhar,1 Akef Obeidat1
1Department of Anatomy, College of Medicine, Alfaisal University, Riyadh, Saudi Arabia; 2College of Medicine, Alfaisal University, Riyadh, Saudi Arabia
Correspondence: Sadia Qazi, Department of Anatomy, College of Medicine, Alfaisal University, Riyadh, Saudi Arabia, Email [email protected] Muhammad Atif Mazhar, Department of Anatomy, College of Medicine, Alfaisal University, Riyadh, Saudi Arabia, Email [email protected]
Background: Cognitive measures explain only part of why some medical students perform well while others struggle. Conscientiousness is a promising non-cognitive factor, but evidence in medical education remains scattered, particularly regarding whether its association with performance varies across assessment types and stages of training.
Methods: This systematic review followed PRISMA 2020 guidance and examined the association between conscientiousness and academic performance in undergraduate medical students. PubMed, ScienceDirect, and PsycINFO were searched on 5 October 2025. Twelve studies involving 3847 medical students met the eligibility criteria. Because the included studies reported heterogeneous outcomes and statistical metrics, findings were synthesized narratively.
Results: Across the included studies, conscientiousness showed a generally positive association with academic performance, with reported estimates typically ranging from 0.18 to 0.48. Associations appeared somewhat stronger in clinical assessments than in preclinical written examinations and were minimal in procedural skills, although formal subgroup meta-analysis was not performed. Longitudinal studies also suggested that the predictive relevance of conscientiousness may become more apparent across later stages of training.
Conclusion: Conscientiousness is a modest and generally consistent correlate of academic performance in medical students. Its relevance appears greater in learning environments that require sustained self-regulation and autonomous effort. These findings do not support the use of conscientiousness for high-stakes admissions decisions. Instead, they support using these findings to guide targeted educational support and curriculum design that strengthen students’ planning, follow-through, and adaptive self-regulation.
Plain Language Summary: Standard tests and past grades do not fully explain why some medical students do well while others struggle. We studied whether conscientiousness, a personality trait linked to being organized, reliable, and hardworking is associated with academic performance in medical school, and whether this association changes as students move through training.
We reviewed 12 studies involving 3,847 medical students from different countries. Overall, students with higher conscientiousness tended to perform better academically. This association appeared more apparent in later, more independent stages of training, especially in clinical settings, where students must manage their own time, stay organized, and maintain effort with less external structure.
These findings suggest that medical schools should not use conscientiousness measures for high-stakes admissions decisions. Instead, this information may be useful for:Identifying students who may benefit from extra support with organization and self-managementProviding coaching in time management, planning, and goal settingDesigning curricula that gradually increase student independence while still providing structure and feedback
In practical terms, the findings support educational approaches that help students build the self-regulation skills needed to succeed throughout medical training.
Keywords: conscientiousness, personality traits, academic performance, medical education, self-regulated learning, systematic review
Introduction
Many competent medical students do not perform as expected academically or during clinical training, while educators often identify struggling learners only after failure has already occurred. This delay can affect academic progression, confidence, and well-being. Although prior academic achievement and standardized test scores remain important predictors of performance, they explain only part of the variation in how students perform in medical school, and selection processes based mainly on knowledge testing may overlook applicants with potentially valuable non-cognitive attributes.1 Non-cognitive factors therefore warrant closer attention when trying to understand why some students adapt successfully to training while others struggle.
One construct of particular interest is conscientiousness, one of the five broad domains of the Five-Factor Model of personality.2,3 The model was formalized in psychometric research from the late 1980s to the early 1990s through the work of Digman2 and McCrae and Costa.3 The Five-Factor Model describes personality in terms of conscientiousness, extraversion, agreeableness, neuroticism, and openness to experience. Within this framework, conscientiousness reflects organization, reliability, diligence, self-discipline, and goal-directed behavior. These characteristics align closely with the behavioral demands of medical education, where students must manage heavy workloads, meet repeated deadlines, and sustain effort across both classroom-based and clinical settings.
The educational relevance of conscientiousness is strengthened by its links to self-regulated learning (SRL). SRL refers to the processes through which learners plan, monitor, and adapt their cognition, motivation, and behavior in pursuit of academic goals.4,5 In medical education, SRL becomes especially important as students move from relatively structured preclinical curricula, including formats such as problem-based learning, toward more independent and socially complex clinical learning environments.6,7 From this perspective, conscientiousness may matter not simply as a stable trait label, but because it supports behaviors such as planning, persistence, time management, and follow-through.
At the broader higher-education level, systematic review and meta-analytic evidence has identified conscientiousness as one of the most consistent psychological correlates of academic achievement.8,9 However, these reviews were not specific to undergraduate medical education, where assessment formats, clinical transitions, and autonomy demands differ substantially from those in general university settings. As a result, it remains unclear whether findings from broader higher-education populations can be applied directly to medical students. This question is especially relevant because conscientiousness has also been linked to psychological functioning and academic outcomes in medical students, while emerging evidence suggests that performance may reflect interactions between personality and other biological or contextual factors.10,11
Evidence within medical education is generally suggestive rather than uniform. Several studies have reported positive associations between conscientiousness and academic performance, including written assessments, anatomy performance, grade-point outcomes, and some clinical measures.12–14 At the same time, the strength of association varies across contexts, and not all studies report clear independent effects after adjustment for other factors.15 Some findings also suggest that related constructs, such as maladaptive perfectionism, may operate differently from adaptive conscientiousness and may even impair performance under pressure.16,17 Taken together, the current literature suggests promise, but not yet clarity, regarding when and how conscientiousness matters most in medical training.
This uncertainty has practical implications. Admissions committees, curriculum designers, and student-support teams need clearer evidence on whether conscientiousness adds meaningfully beyond prior academic achievement, whether its relevance differs across assessment formats, and whether its importance changes as students progress from preclinical to clinical training. These questions matter because clinical learning places increasing demands on independence, sustained preparation, and self-management.18,19 If conscientiousness is more strongly related to success in these settings, its value may lie less in selection and more in the design of targeted educational support.
Accordingly, this systematic review aimed to synthesize the association between conscientiousness and academic performance in undergraduate medical students. This review advances the field by focusing specifically on medical education and by examining whether conscientiousness-performance associations vary across assessment types and stages of training. Three focused questions guided the review: (1) How consistent are conscientiousness-performance associations across medical schools and measurement approaches? (2) Do these associations vary by assessment type, including knowledge-based, clinical, and high-stakes examinations? (3) Do they differ across stages of training, particularly between preclinical and clinical education?
Materials and Methods
Protocol
This review followed the PRISMA 2020 statement.20 The protocol was prospectively registered with PROSPERO before study selection commenced (registration number: CRD420251240333). Ethical approval was not required because the review analyzed only previously published data. The full protocol is publicly available through the PROSPERO registry, and no deviations from the registered protocol occurred after registration. The completed PRISMA 2020 checklist is provided in Supplementary Table S1.
Eligibility Criteria
Eligibility criteria were defined using the PECO framework.21
Population
Undergraduate medical students enrolled in MD or MBBS programs, including both preclinical and clinical stages.
Exposure
Conscientiousness measured using validated instruments, such as the NEO Personality Inventory—Revised (NEO-PI-R), NEO Five-Factor Inventory (NEO-FFI), Big Five Inventory (BFI)-derived measures, DECAS Personality Inventory (DECAS), or USM Personality Inventory-15 (USMaP-15).
Comparator
Higher versus lower conscientiousness, when a comparator was reported.
Outcomes
Academic performance outcomes, including grade point average, written examinations, OSCEs, licensing examinations, or progression indicators.
Eligible studies were observational empirical studies, including cross-sectional, cohort, and case-control designs, published in peer-reviewed journals in English. Studies were excluded if they involved postgraduate trainees or non-medical health professions, did not measure conscientiousness, used non-validated personality scales, or were qualitative studies, reviews, case reports, editorials, conference abstracts without full text, or other non-empirical sources.
Search Strategy
A systematic search was conducted on 5 October 2025 in PubMed, ScienceDirect, and PsycINFO. These databases were selected to provide coverage of biomedical, psychological, and educational research relevant to the review question. Controlled vocabulary and free-text terms related to medical students, conscientiousness, personality, and academic performance were combined using Boolean operators. The full database-specific search strategies are provided in Appendix A.
Study Selection
Records were imported into Rayyan for deduplication and screening.22 Two reviewers independently screened all titles and abstracts, followed by full-text assessment of potentially eligible studies. Inter-reviewer agreement for full-text inclusion was high (Cohen’s κ = 0.87), indicating almost perfect agreement according to conventional benchmarks.23 Disagreements were resolved through consensus discussion, with consultation from a senior reviewer when required. The study selection process is presented in Figure 1.
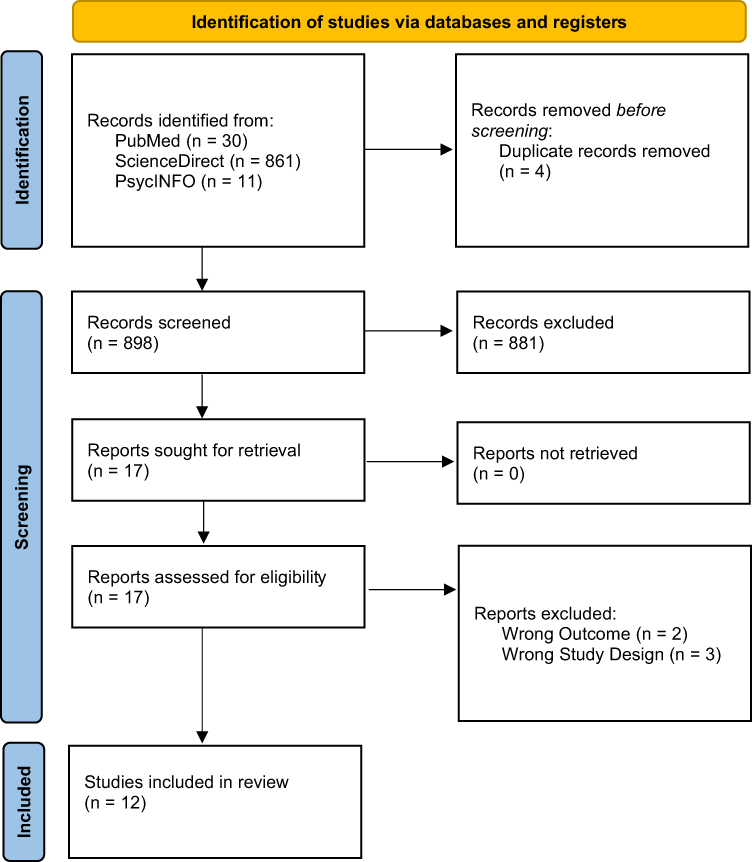 |
Figure 1 PRISMA 2020 flow diagram depicting the study-selection process. |
Data Extraction
A standardized data extraction form was used to capture study characteristics, participant details, personality instruments, academic outcomes, reported associations, covariates, and study limitations. Data extraction was performed independently by two reviewers. Discrepancies were resolved through discussion with reference to the original publications. Full study-level extraction data are provided in Supplementary Table S2.
Quality Assessment
Risk of bias was assessed using the Newcastle-Ottawa Scale for cohort and case-control studies24 and the Joanna Briggs Institute checklist for analytical cross-sectional studies.25 All studies were retained, and appraisal results were used to inform interpretation rather than determine exclusion.
Formal assessment of reporting bias using funnel plots or statistical tests was not feasible because no meta-analysis was performed and the included studies reported heterogeneous statistical metrics. Certainty of evidence was considered using a GRADE-informed approach based on core domains, including risk of bias, inconsistency, indirectness, imprecision, and potential publication bias.26 Because the review did not include pooled quantitative synthesis, this assessment was used to support interpretation rather than generate formal pooled certainty ratings.
Data Synthesis
A meta-analysis was not conducted because quantitative synthesis was methodologically infeasible. The included studies reported heterogeneous statistical metrics, including Pearson’s r, Spearman’s ρ, and standardized β coefficients. In addition, several studies did not report variance estimates or confidence intervals, outcome measures varied substantially across academic settings, and confounder adjustment was inconsistent across studies. Together, these factors limited direct statistical comparability.
A structured narrative synthesis was therefore undertaken and reported in line with SWiM principles.27 The synthesis was organized around three predefined questions:
- Consistency of conscientiousness-performance associations across contexts;
- Variation by assessment type; and
- Temporal patterns across stages of training.
Reported associations were extracted as presented in the original studies. Where multiple estimates were available, adjusted estimates were prioritized. Because statistical reporting was heterogeneous, findings were summarized descriptively rather than transformed to a common effect-size metric. Risk-of-bias assessments informed the interpretation of findings. No pooled sensitivity analyses were applicable because no meta-analysis was performed.
Results
Study Selection
The search yielded 902 records in total. After removal of four duplicates, 898 titles and abstracts were screened for eligibility. Seventeen reports were sought for retrieval, and 17 full-text articles were assessed for eligibility. Five full-text articles were excluded, leaving 12 studies for inclusion in the review. The study-selection process is shown in Figure 1. A list of full-text articles excluded after eligibility assessment, with reasons, is provided in Supplementary Table S3.
Study Characteristics
The 12 included studies spanned nine countries. Belgium contributed two longitudinal cohort studies: Lievens et al12 which followed 607 students across three training years, and Lievens et al13 which extended the follow-up to seven years across 627 students, with both studies reporting increasing predictive validity of conscientiousness for GPA as training progressed. China was represented by Xie et al11 a cross-sectional study of 448 students examining associations between personality and GPA across four academic domains. Finland contributed one prospective observational study by Helle et al15 which examined whether conscientiousness predicted microscopy and knowledge examination performance in preclinical students. Malaysia provided two longitudinal studies examining personality in relation to GPA across mixed training stages: Yusoff et al10 and Yusoff,28 both using the USM Personality Inventory-15. The Netherlands contributed the only experimental laboratory study in the review: Kleinrensink et al,16 which assessed perfectionism-related constructs in 30 students undergoing surgical simulation training. Romania was represented by Muntean et al29 a cross-sectional study of 179 final-year students examining personality and national residency examination scores. Switzerland contributed two studies: Schrempft et al14 a cross-sectional study of 268 Year 3 students examining case-based and OSCE performance, and Abbiati and Cerutti,30 a six-year longitudinal cohort tracking conscientiousness from entry to graduation in relation to federal licensing examination scores. The United Kingdom contributed a cross-sectional study by Finn et al31 which examined personality facets and anatomy practical performance in 85 students in Years 1 and 2. The United States was represented by Stratton and Elam,32 a multi-cohort study examining conscientiousness as a predictor of first-year GPA and risk of academic underperformance. Among studies reporting analyzable sample sizes, these ranged from 3016 to 627;13 studies from Malaysia10,28 and the Swiss longitudinal cohort30 did not report final retained sample sizes clearly.
Conscientiousness measurement approaches varied across the included studies. Yusoff et al10 and Yusoff.,28 both used the USM Personality Inventory-15 (USMaP-15), a context-specific instrument developed for Malaysian medical students. Xie et al 11 combined the Tridimensional Personality Questionnaire (TPQ) with NEO instruments. Lievens et al12,13 used the NEO Personality Inventory—Revised (NEO-PI-R), which permitted facet-level analysis alongside global conscientiousness scores. Schrempft et al14 and Abbiati and Cerutti30 each applied the NEO Five-Factor Inventory (NEO-FFI). Helle et al15 used a Big Five measure, though the specific instrument was not reported. Kleinrensink et al16 used the Perfectionism Inventory, an indirect measure of a conscientiousness-related construct rather than global conscientiousness directly Muntean et al29 used the DECAS Personality Inventory Finn et al31 applied International Personality Item Pool (IPIP) Big Five measures Stratton and Elam.,32 used the NEO-PI-R alongside an emotional intelligence measure. Academic outcomes spanned GPA,10–13,28,32 written and knowledge-based examinations11,15 licensing examinations,29,30 Objective Structured Clinical Examinations (OSCEs) and case-based assessments,14,30 anatomy practical performance,31 and simulator-based procedural skills.16 Most studies reported generally positive associations between conscientiousness and academic performance, although effect sizes and statistical reporting varied considerably across studies. Table 1 presents all study-level details.
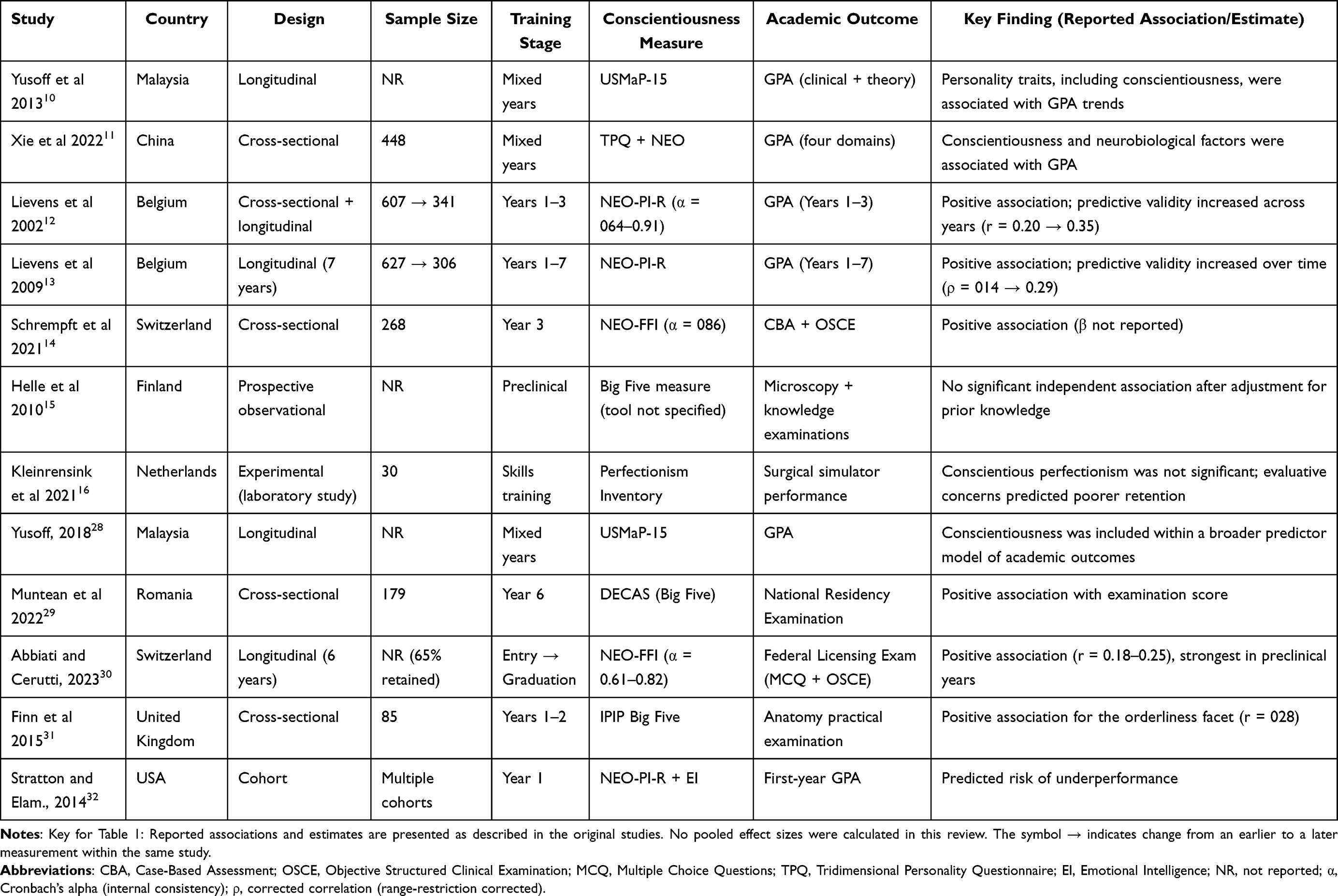 |
Table 1 Characteristics of Included Studies (n = 12) |
Quality Assessment
Risk of bias assessment indicated generally low-to-moderate concerns across the included studies. Most studies used validated personality instruments and objective academic outcomes. Common limitations included incomplete confounder adjustment, attrition in longitudinal cohorts, and single-institution sampling, all of which may limit generalizability. No study was excluded based on quality assessment. Table 2 presents the domain-level ratings and Figure 2 presents summary of risk of bias of included studies. Studies reporting stronger conscientiousness-performance associations were often rated as low risk across exposure and outcome domains, whereas several moderate-risk studies were characterized by incomplete confounder adjustment or restricted institutional sampling. Facet-level analyses were limited to three studies, two of which were judged to have moderate risk because of small sample size and attrition, reducing confidence in conclusions regarding specific conscientiousness dimensions.
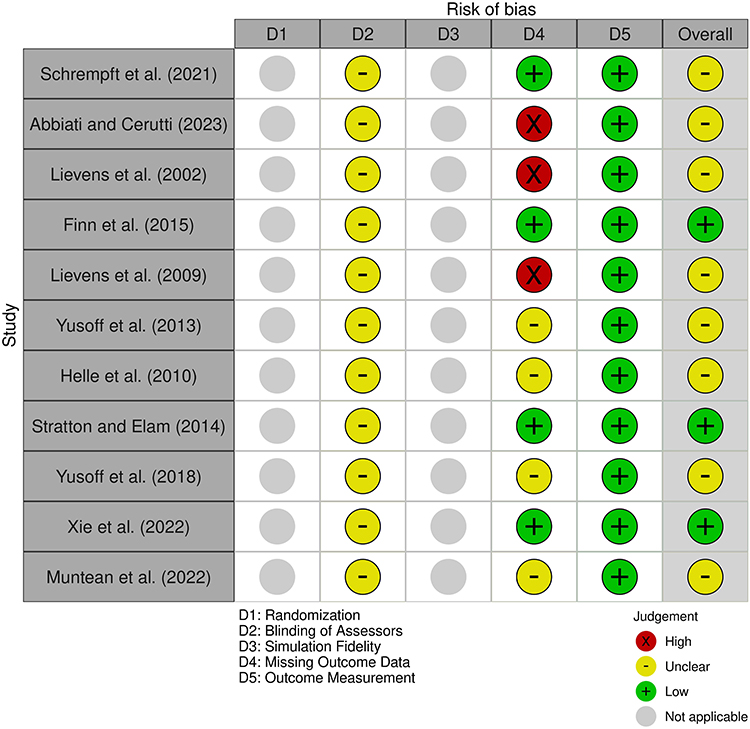 |
Figure 2 Summary of risk of bias of included studies. |
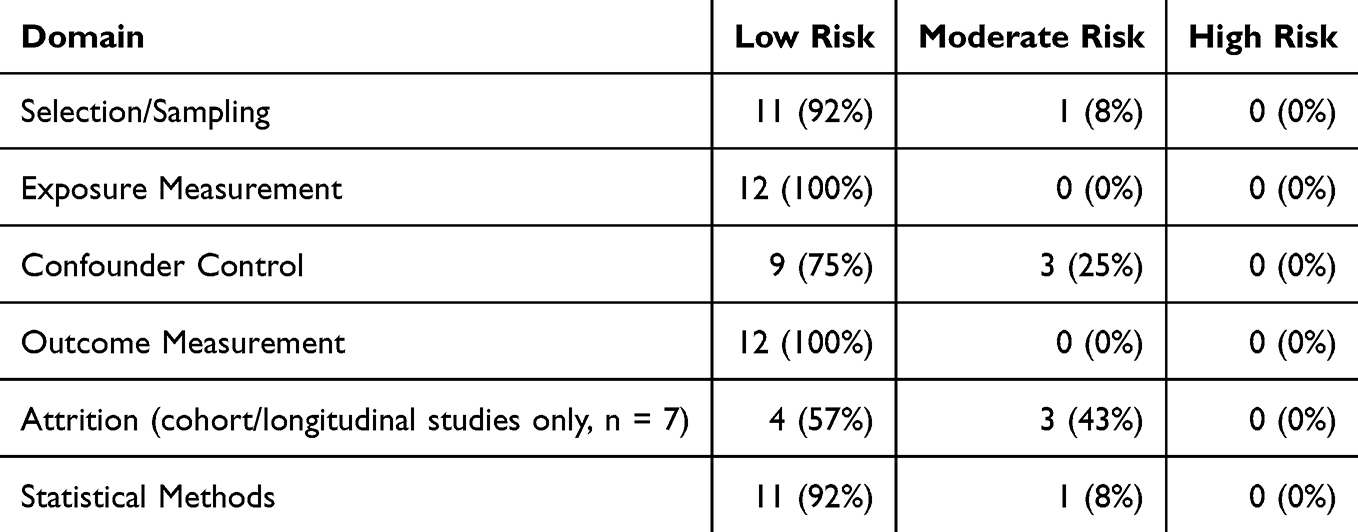 |
Table 2 Summary of Risk of Bias Assessment |
Synthesis of Findings
Overall Association
Across the 12 included studies, representing a reported total of 3,847 students, conscientiousness generally showed a positive association with academic performance. Reported associations were usually small to moderate, although the included studies used heterogeneous statistical metrics and not all studies reported significant independent effects. For example, Muntean et al29 found a positive association with national residency examination scores among final-year students in Romania, while Stratton and Elam32 identified conscientiousness as a predictor of first-year underperformance risk across multiple cohorts in the United States Several longitudinal studies also suggested that the predictive relevance of conscientiousness may become more apparent across later stages of training. Detailed study-level estimates are provided in Supplementary Table S2.
Variation by Outcome Type
Clinical Performance
Four studies examined clinical outcomes, including OSCE scores, case-based assessments, and licensing examinations with clinical components.14,28–30 Associations appeared somewhat stronger in these settings than in purely preclinical written outcomes, although the small number of studies and heterogeneous reporting preclude firm comparative ranking. Two Swiss studies reported positive relationships between conscientiousness and OSCE or computer-based assessments. One study also suggested that students’ perceptions of the learning environment modified the strength of this association.
Preclinical Examinations
Preclinical outcomes generally showed smaller, though still positive, associations. Anatomy and biomedical science examinations demonstrated modest correlations, including facet-level effects such as orderliness.31 In one study, conscientiousness did not predict microscopy performance after adjustment for prior knowledge, indicating that domain-specific knowledge may attenuate personality-related effects in highly structured settings.
Specialized Assessment Contexts
Two studies focused on specialized procedural or technical skills.16,30 Finn et al31 reported a small positive association with anatomy practical performance, whereas Kleinrensink et al16 found no association between conscientiousness and surgical simulation performance These findings suggest that narrow technical or fine-motor tasks may depend more strongly on specific skill acquisition and deliberate practice than on broad personality traits.
Negative or Mixed Findings
One study identified a negative pattern: self-evaluative perfectionism, characterized by self-criticism and fear of mistakes, predicted poorer retention of surgical skills.16 The conscientiousness-related perfectionism facet did not show negative effects. Because this study had a small sample and limited reporting, the finding should be interpreted cautiously; it nonetheless argues for carefully distinguishing adaptive conscientiousness from maladaptive perfectionism. Study-level details of null and mixed findings are provided in Supplementary Table S2.
Measurement Tools
Measurement approaches varied across studies. NEO-family instruments were the most frequently used, while other studies relied on shorter Big Five measures, local adaptations, or hybrid personality-related constructs. Despite this measurement heterogeneity, the direction of association was generally positive across studies. However, few studies examined facet-level predictors, limiting insight into whether specific dimensions such as orderliness, deliberation, or self-discipline account for the observed relationships. Table 3 summarizes the measurement approaches used across the included studies.
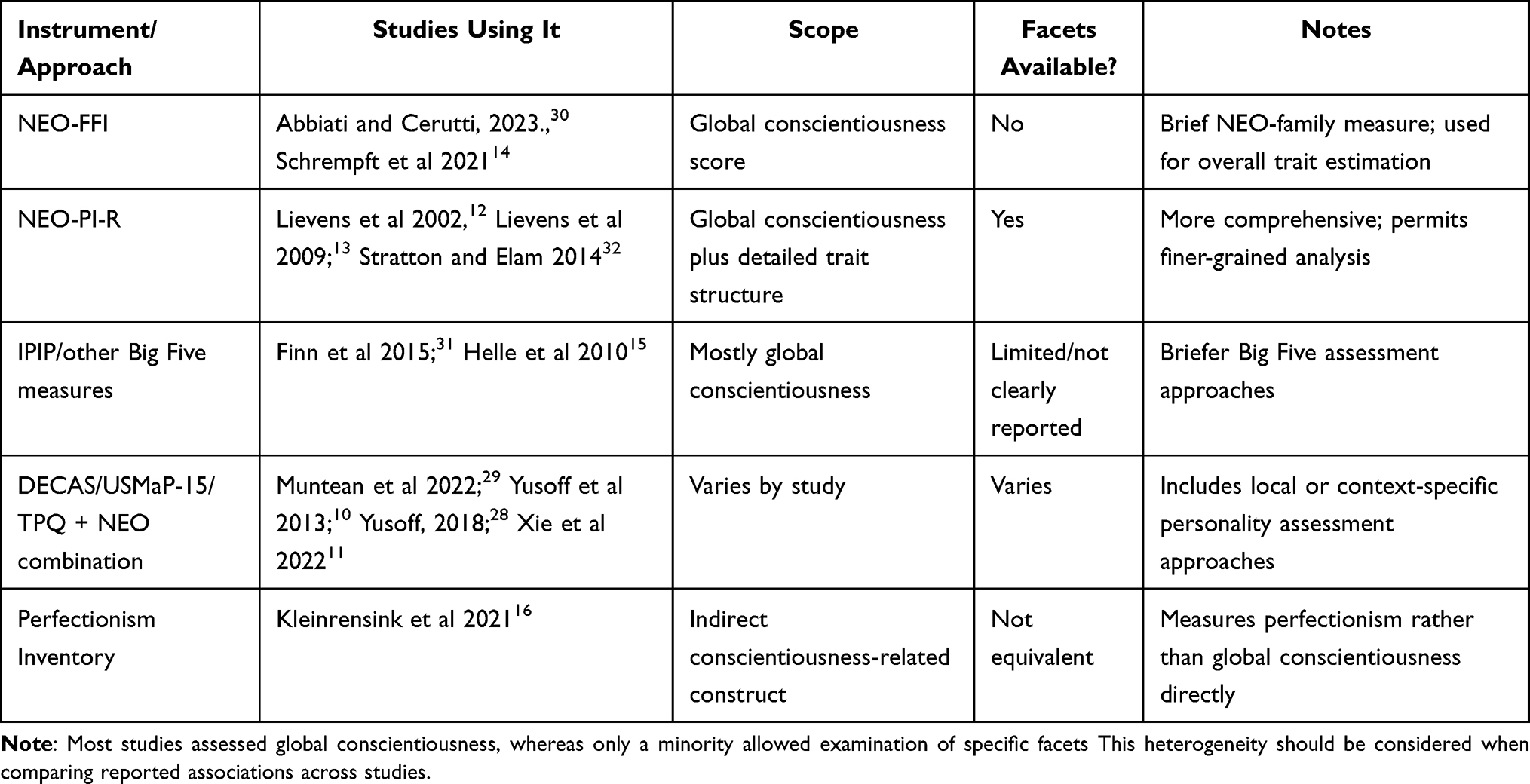 |
Table 3 Summary of Conscientiousness Measurement Approaches Across Included Studies |
No sensitivity analyses were performed because the review used narrative synthesis and did not generate pooled quantitative estimates. Formal assessment of reporting bias was also not performed because no meta-analysis was conducted and outcome reporting methods were highly heterogeneous across studies.
GRADE-Informed Certainty Assessment
Using a GRADE-informed narrative approach, the overall certainty of evidence for the association between conscientiousness and academic performance in medical students was judged to be moderate. This rating reflects the generally consistent direction of findings across studies despite reliance on observational designs. Certainty was downgraded because of attrition in longitudinal cohorts, incomplete confounder adjustment in several studies, heterogeneity in personality measures and academic outcomes, and the predominance of single-institution samples.
Certainty regarding variation by assessment type, temporal strengthening across training stages, facet-level effects, and environmental moderation was lower because subgroup evidence was limited, indirect, and inconsistently reported. A detailed summary of the certainty assessment is provided in Supplementary Table S4.
Discussion
Summary of Findings
This systematic review synthesized 12 studies involving 3,847 medical students and found that conscientiousness was generally associated with better academic performance, although the observed effects were typically modest and were reported using heterogeneous statistical metrics. Three broad patterns emerged. First, the direction of association was generally positive across studies conducted in different countries, using different personality measures and outcome formats. Second, the strength of association appeared to vary by assessment type, with somewhat stronger relationships in clinical or mixed clinical outcomes than in preclinical written examinations, while highly technical procedural tasks showed weaker or null associations. Third, limited longitudinal evidence12,13 suggested that the predictive relevance of conscientiousness may become more apparent across later stages of training.
Taken together, these findings suggest that conscientiousness does not operate as a context-independent trait with uniform effects across all forms of assessment. Rather, its educational relevance may depend on the extent to which success requires sustained preparation, self-management, and follow-through in relatively autonomous learning environments.
Interpretation Through a Self-Regulated Learning Perspective
The observed pattern is consistent with self-regulated learning theory, which conceptualizes effective learning as a cyclical process involving forethought, planning, strategic action, monitoring, and adaptation.4,5 From this perspective, conscientiousness may matter because it supports behaviors that are central to self-regulated learning, including organization, persistence, disciplined study routines, and adherence to long-term goals.
This interpretation is particularly relevant in medical education. Early preclinical training is usually more structured, with fixed schedules, defined content boundaries, and relatively explicit external regulation. As students progress into clinical environments, they are increasingly expected to identify learning opportunities, manage competing responsibilities, regulate their own study behavior, and sustain effort in settings with less direct structure.6 In such contexts, individual differences in conscientiousness may become more visible because students must rely more heavily on self-management to maintain performance.
Motivational theory further supports this interpretation. Self-determination theory distinguishes between controlled motivation and autonomous motivation, the latter reflecting engagement driven by personal endorsement and internalized value.31,32 It is plausible that conscientiousness contributes to academic performance partly by supporting the internalization of goals and the disciplined pursuit of valued learning activities. This may help explain why conscientiousness appears particularly relevant in settings that demand repeated independent effort rather than simple compliance with externally structured requirements.
Explaining Variation by Assessment Type and Training Stage
Variation across assessment types offers a useful way to interpret when conscientiousness may matter most. Clinical and mixed clinical assessments may show stronger associations because they require integration of knowledge, sustained preparation, judgment under uncertainty, and repeated follow-through across time. These assessment formats often reward behaviors that depend not only on what students know, but also on how consistently they prepare, organize their work, and manage themselves in complex settings.19
By contrast, preclinical written examinations may show smaller associations because they are embedded in more structured curricula with clearly defined content and timelines. In such settings, external organization may partially reduce the degree to which individual differences in self-regulation shape outcomes. This does not mean conscientiousness is irrelevant in preclinical education, but rather that its contribution may be less visible when the educational environment itself provides substantial structure.
The weakest findings were seen in specialized procedural contexts. This likely reflects the fact that narrow technical or fine-motor tasks may depend more strongly on deliberate practice, psychomotor ability, feedback quality, and task-specific training than on broad personality traits. The study on surgical skill retention is informative in this regard: maladaptive self-evaluative perfectionism was associated with poorer retention, whereas conscientious perfectionism was not.16 This distinction suggests that adaptive conscientiousness should not be conflated with anxiety-driven perfectionistic striving, particularly in performance settings where pressure may impair execution.
The apparent strengthening of associations across training stages should also be interpreted cautiously. Although several longitudinal studies suggested that conscientiousness became more predictive over time, this pattern may reflect both genuine contextual change and methodological issues such as selective retention.12,13 Even so, the overall direction of evidence supports the idea that conscientiousness becomes more educationally relevant as training places greater demands on self-directed effort.
Integration with Broader Literature
These findings are consistent with broader higher-education literature showing that conscientiousness is one of the most reliable psychological correlates of academic achievement.8,9 The present review extends that literature by focusing specifically on undergraduate medical education, where learning environments, assessment formats, and developmental transitions differ from those in general university settings.
The findings are also consistent with work on self-regulated learning in medical education, which emphasizes that students’ performance depends not only on knowledge acquisition but also on how effectively they regulate their learning in clinical and academic settings.33 In parallel, research on procrastination supports a related interpretation, because procrastination is often conceptualized as a form of self-regulatory failure that is negatively related to conscientiousness and its facets.34 Together, these literatures suggest that the educational significance of conscientiousness may arise less from trait labeling itself than from the learning behaviors it helps sustain.
The review also fits with a broader, multifactorial view of academic performance. Conscientiousness is unlikely to operate in isolation; rather, its effects probably intersect with motivation,35 prior achievement, metacognitive skills, contextual support, and possibly biological factors.10,11 This is important because it argues against simplistic interpretations in which conscientiousness is treated as a single stable determinant of success. Instead, the current evidence supports a more contextual view in which conscientiousness contributes to performance most clearly when environmental demands require sustained self-direction and behavioral consistency.
Strengths and Limitations: Interpretive Perspective
Key strengths of this review include the exclusive use of validated personality instruments, reliance on objective academic performance measures, and the ability to compare findings across training stages and assessment formats. The repeated observation of a positive direction of association across methodologically diverse studies supports the presence of a likely association between conscientiousness and academic performance in medical students.
Several limitations shape interpretation. Approximately 67% of included participants were drawn from single-institution studies, limiting generalizability and suggesting that conscientiousness-performance relationships may be context-dependent. Longitudinal attrition represents another important limitation. Differential loss to follow-up may partially explain the observed temporal strengthening if students with lower conscientiousness were more likely to withdraw or be lost to follow-up. Although attrition alone is unlikely to explain all observed patterns, future studies that explicitly track dropout mechanisms are needed to clarify this issue.
Facet-level evidence is also sparse, with only three studies examining specific dimensions of conscientiousness. This limits the ability to determine whether orderliness, self-discipline, deliberation, or achievement striving drive effects in different contexts. Measurement heterogeneity across personality instruments introduced additional variability. Because instrument scope and reporting varied substantially, it remains unclear whether more comprehensive inventories outperform briefer tools in detecting educationally relevant effects.
All included studies were observational, which limits causal inference. Conscientiousness may co-occur with unmeasured factors such as study strategies, metacognitive skills, social support, and help-seeking behaviors that directly influence performance. In addition, publication bias cannot be excluded because the review was limited to English-language peer-reviewed studies and formal reporting-bias assessment was not feasible without meta-analysis. Applying a GRADE-informed approach suggests moderate certainty for the overall conscientiousness-performance association, but lower certainty for variation across assessment types and for temporal strengthening across training stages. Evidence for facet-level effects and environmental moderation remains low because of limited data.
Future Directions
Future research should move beyond prediction toward mechanism and intervention. Multi-institutional longitudinal studies are needed to clarify whether the apparent strengthening of conscientiousness across training stages reflects developmental change, contextual shifts, selective attrition, or a combination of these factors. More detailed facet-level work is also needed to determine whether specific components of conscientiousness, such as orderliness or self-discipline, are differentially related to performance in distinct educational contexts.
Intervention research is especially important. Studies should test whether explicitly strengthening self-regulated learning skills, including planning, implementation intentions,35,36 effort regulation, and follow-through, improves outcomes for students with different conscientiousness profiles. Future work should also examine environmental moderation more directly by evaluating how autonomy support, feedback quality, learning climate, and curricular structure shape the relationship between conscientiousness and performance.
Finally, research should explore modifiable mechanisms that translate these findings into practice. Structured mentoring, tailored academic coaching, and interventions targeting maladaptive perfectionism may offer more educational value than attempts to use conscientiousness as a selection tool. This direction is more consistent with the current evidence, which supports using conscientiousness as a guide for student support and curricular design rather than as a high-stakes screening criterion.
Conclusion
This systematic review indicates that conscientiousness is a modest and generally consistent correlate of academic performance in medical students, with some evidence suggesting that its predictive relevance may strengthen as training progresses from preclinical to clinical stages. The findings suggest that conscientiousness is not a context-independent trait; rather, its relevance may increase in educational environments that demand sustained self-regulated learning and autonomous effort.
These results do not support the use of conscientiousness for high-stakes admission or selection decisions. The evidence instead points toward the trait’s primary value for guiding targeted educational support and evidence-informed curricular design. Students across the full spectrum of conscientiousness can succeed when learning environments provide appropriate structure, progressive autonomy, and feedback that actively support self-regulation.
These findings should be interpreted in light of the observational design of the included studies, heterogeneity in personality measures and academic outcomes, attrition in longitudinal cohorts, and the predominance of single-institution samples. Future research should prioritize multi-institutional longitudinal studies, clearer facet-level analyses, and intervention studies testing whether strengthening self-regulatory skills improves outcomes for students with different conscientiousness profiles.
Abbreviations
CBA, Case-Based Assessment; EI, Emotional Intelligence; GPA, Grade Point Average; MCQ, Multiple Choice Questions; NEO-FFI, NEO Five-Factor Inventory; NEO-PI-R, Revised NEO Personality Inventory; NR, Not Reported; OSCE, Objective Structured Clinical Examination; SRL, Self-Regulated Learning; TPQ, Tridimensional Personality Questionnaire.
Data Sharing Statement
The original contributions presented in this study are included in the article and its Supplementary Materials. Further inquiries can be directed to the corresponding author; Dr Sadia Qazi; [email protected].
Acknowledgments
During the preparation of this manuscript, the authors used Paperpal, a language-editing tool, for grammar correction. The authors reviewed and edited the output and take full responsibility for the content of this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding. The APC was covered by Alfaisal University.
Disclosure
The authors declare no conflicts of interest.
References
1. Abbiati M, Baroffio A, Gerbase MW. Personal profile of medical students selected through a knowledge-based exam only: are we missing suitable students? Med Educ Online. 2016;21(1):29705. doi:10.3402/meo.v21.29705
2. Digman JM. Personality structure: emergence of the five-factor model. Annu Rev Psychol. 1990;41:417–14. doi:10.1146/annurev.ps.41.020190.002221
3. McCrae RR, Costa PT. Validation of the five-factor model of personality across instruments and observers. J Pers Soc Psychol. 1987;52(1):81–90. doi:10.1037/0022-3514.52.1.81
4. Zimmerman BJ. Becoming a self-regulated learner: an overview. Theory Into Pract. 2002;41(2):64–70. doi:10.1207/S15430421TIP4102_2
5. Dent AL, Koenka AC. The relation between self-regulated learning and academic achievement. Educ Psychol Rev. 2016;28(3):425–474. doi:10.1007/s10648-015-9320-8
6. Berkhout JJ, Helmich E, Teunissen PW, van der Vleuten CPM, Jaarsma ADC. How clinical medical students perceive others to influence their self-regulated learning. Med Educ. 2017;51(3):269–279. doi:10.1111/medu.13131
7. Schmidt HG, Rotgans JI, Yew EHJ. The process of problem-based learning: what works and why. Med Educ. 2011;45(8):792–806. doi:10.1111/j.1365-2923.2011.04035.x
8. Poropat AE. A meta-analysis of the five-factor model of personality and academic performance. Psychol Bull. 2009;135(2):322–338. doi:10.1037/a0014996
9. Richardson M, Abraham C, Bond R. Psychological correlates of academic performance: a systematic review and meta-analysis. Psychol Bull. 2012;138(2):353–387. doi:10.1037/a0026838
10. Yusoff MSB, Esa AR, Mat Pa MN, See CM, Abdul Aziz R, Abdul Rahim AF. A longitudinal study of relationships between previous academic achievement, emotional intelligence and personality traits with psychological health of medical students during stressful periods. Educ Health. 2013;26(1):39–47. doi:10.4103/1357-6283.112800
11. Xie Y, Yuan C, Sun M, et al. Personality and brain contribute to academic achievements of medical students. Front Neurosci. 2022;16:964904. doi:10.3389/fnins.2022.964904
12. Lievens F, Coetsier P, De Fruyt F, De Maeseneer J. Medical students’ personality characteristics and academic performance. Med Educ. 2002;36(11):1050–1056. doi:10.1046/j.1365-2923.2002.01328.x
13. Lievens F, Ones DS, Dilchert S. Personality scale validities increase throughout medical school. J Appl Psychol. 2009;94(6):1514–1535. doi:10.1037/a0016137
14. Schrempft S, Piumatti G, Gerbase MW, Baroffio A. Pathways to performance in undergraduate medical students: role of conscientiousness and the perceived educational environment. Adv Health Sci Educ Theory Pract. 2021;26(5):1537–1554. doi:10.1007/s10459-021-10059-6
15. Helle L, Nivala M, Kronqvist P, Ericsson KA, Lehtinen E. Do prior knowledge, personality and visual perceptual ability predict student performance in microscopic pathology? Med Educ. 2010;44(6):621–629. doi:10.1111/j.1365-2923.2010.03625.x
16. Kleinrensink VEE, Lange JF, Kleinrensink GJ. Perfectionistic concerns are detrimental to skill learning for minimally invasive surgery. J Surg Educ. 2021;78(2):630–637. doi:10.1016/j.jsurg.2020.08.022
17. Eley DS, Bansal V, Leung J. Perfectionism as a mediator of psychological distress in medical students. Med Teach. 2020;42(11):1301–1307. doi:10.1080/0142159X.2020.1805101
18. van Houten-Schat MA, Berkhout JJ, van Dijk N, Endedijk MD, Jaarsma ADC, Diemers AD. Self-regulated learning in the clinical context: a systematic review. Med Educ. 2018;52(10):1008–1015. doi:10.1111/medu.13615
19. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–645. doi:10.3109/0142159X.2010.501190
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
21. Morgan RL, Whaley P, Thayer KA, Schünemann HJ. Identifying the PECO: a framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ Int. 2018;121(Pt 1):1027–1031. doi:10.1016/j.envint.2018.07.015
22. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi:10.1186/s13643-016-0384-4
23. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174. doi:10.2307/2529310
24. Gualdi-Russo E, Zaccagni L. The Newcastle–Ottawa Scale for assessing the quality of studies in systematic reviews. Publications. 2026;14(1):4. doi:10.3390/publications14010004
25. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. Adelaide: JBI; 2020. doi:10.46658/JBIMES-20-08
26. Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–406. doi:10.1016/j.jclinepi.2010.07.015
27. Campbell M, McKenzie JE, Sowden A, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 2020;368:l6890. doi:10.1136/bmj.l6890
28. Yusoff MSB. The outcomes that an interview-based medical school admission process has on academic performance, psychological health, personality traits, and emotional intelligence. J Taibah Univ Med Sci. 2018;13(6):503–511. doi:10.1016/j.jtumed.2018.09.003
29. Muntean LM, Nireștean A, Sima-Comaniciu A, Mărușteri M, Zăgan CA, Lukacs E. The relationship between personality, motivation and academic performance at medical students from Romania. Int J Environ Res Public Health. 2022;19(15):8993. doi:10.3390/ijerph19158993
30. Abbiati M, Cerutti B. Do students’ personality traits change during medical training? A longitudinal cohort study. Adv Health Sci Educ. 2023;28(4):1079–1092. doi:10.1007/s10459-023-10205-2
31. Finn GM, Laughey W, McLachlan J, et al. The relationship between personality and anatomy performance. Anat Sci Educ. 2015;8(6):547–554. doi:10.1002/ase.1516
32. Stratton TD, Elam CL. A holistic review of the medical school admission process: examining correlates of academic underperformance. Med Educ Online. 2014;19:22919. doi:10.3402/meo.v19.22919
33. Lucieer SM, Jonker L, Visscher C, Rikers RMJP, Themmen APN. Self-regulated learning and academic performance in medical education. Med Teach. 2016;38(6):585–593. doi:10.3109/0142159X.2015.1073240
34. Steel P. The nature of procrastination: a meta-analytic and theoretical review of self-regulatory failure. Psychol Bull. 2007;133(1):65–94. doi:10.1037/0033-2909.133.1.65
35. Kusurkar RA, ten Cate TJ, van Asperen M, Croiset G. Motivation as an independent and a dependent variable in medical education: a review of the literature. Med Teach. 2011;33(5):e242–e262. doi:10.3109/0142159X.2011.558539
36. Gollwitzer PM. Implementation intentions: strong effects of simple plans. Am Psychol. 1999;54(7):493–503. doi:10.1037/0003-066X.54.7.493
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of English Learning Motivation on Academic Performance Among English Majors in China: The Moderating Role of Certain Personality Traits
Zhang Y, Wang H
Psychology Research and Behavior Management 2023, 16:2187-2199
Published Date: 14 June 2023
A Cross-Sectional Study on Inequity and Unmet Needs in Conducting Systematic Reviews (SRMA) and Meta-Analysis Among Medical Students and Junior Doctors
Manku B, Saffari TM, Sandhu V, Khajuria A
Advances in Medical Education and Practice 2023, 14:647-655
Published Date: 20 June 2023
Mapping the Landscape: A Systematic Review of Technology Trends in Medical Education and Competency Development

Toofaninejad E, Mirzaei S, Mahdavi Shakib A, Gholipour Morad Dashtaki D, Raoufian H, Mirmoghtadaie Z, Sohrabi S
Advances in Medical Education and Practice 2025, 16:2369-2383
Published Date: 20 December 2025