Back to Journals » International Medical Case Reports Journal » Volume 19
Concurrent Acute Ischemic Stroke and Acute Coronary Syndrome: A Case Report on Sequential Endovascular Intervention and Peri-Procedural Antiplatelet Management with Tirofiban
Authors Luo H, Zhao Z, Chen Y, Li S, Wu X, Cao X, Liu X, Liu S, Liu B
Received 22 October 2025
Accepted for publication 4 February 2026
Published 10 February 2026 Volume 2026:19 573876
DOI https://doi.org/10.2147/IMCRJ.S573876
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Han Luo, Zengxia Zhao, Yongzhen Chen, Shanshan Li, Xiangfeng Wu, Xiongbin Cao, Xiangyu Liu, Shuyun Liu, Bo Liu
Department of Neurology, Shenzhen Longhua District Central Hospital, Shenzhen, Guangdong, People’s Republic of China
Correspondence: Bo Liu, Department of Neurology, Shenzhen Longhua District Central Hospital, Shenzhen, Guangdong, 518110, People’s Republic of China, Email [email protected]
Abstract: Cases involving both cerebral infarction due to internal carotid artery occlusion and acute coronary syndrome are clinically rare and challenging to treat. A 50-year-old male patient was admitted to the hospital due to coexistence of internal carotid artery occlusion ischemic stroke and acute coronary syndrome. After coronary angiography and percutaneous coronary intervention (PCI), immediately perform cerebral angiography, followed by right internal carotid artery occlusion balloon dilation and stent formation, intracranial artery thrombectomy, and complete recovery of cerebral blood flow. His condition improved significantly after 15 days, and the weakness of the left limbs and alalia improved a lot. The patient who was followed up for 1 years had stable conditions and was able to take care of himself, with an mRS score of 1. Patients with acute cerebral infarction typically receive rt-PA treatment within 4.5 hours. If head and neck CTA reveals occlusion of a large artery, endovascular therapy can be used as a bridge. The therapeutic sequence of coronary stenting followed by endovascular thrombectomy and carotid artery stenting may have been critical to the patient’s favorable clinical outcome. While Antiplatelet aggregation is crucial during the perioperative period of carotid artery stenting or/and coronary stent implantation, its initiation within 24 hours of intravenous thrombolysis must balance efficacy against bleeding risk. Tirofiban represents a potential option during this high-risk period.
Keywords: acute ischemic stroke, endovascular treatment, acute coronary syndrome, percutaneous coronary intervention, antiplatelet aggregation, cardiocerebral infarction
Introduction
Cardiocerebral infarction (CCI) refers to the rare occurrence of acute ischemic stroke and acute myocardial infarction either simultaneously or in close succession,1 with an estimated prevalence ranging from 0.29% to 0.79%.1,2 Cases involving both cerebral infarction due to internal carotid artery occlusion and acute coronary syndrome are clinically rare and challenging to treat. Experiencing both an acute ischemic stroke and acute coronary syndrome simultaneously is a medical emergency, and failure to treat these conditions promptly results in a poor prognosis. Currently, there is a lack of standardized treatment protocols specifically for cardiocerebral infarction. In recent years, advancements in rational drug therapy and interventional cardiology have significantly lowered mortality and effectively improved the functional prognosis of patients with this condition. Clinical decision-making requires a careful risk-benefit analysis, often prioritizing the lesion that poses the most immediate threat to life.3 However, the etiological factors and contributing factors of cerebral infarction due to internal carotid artery occlusion combined with acute coronary syndrome can vary among patients. The shared pathological foundation between acute myocardial infarction and large-artery atherosclerotic stroke is constituted by the interplay of multiple mechanisms, including atherosclerosis, vascular endothelial dysfunction, activation of the coagulation system, catecholamine storm in Takotsubo syndrome, cytokine storm in systemic inflammation, patent foramen ovale, aortic mural thrombus, and genetic susceptibility.4 Although guidelines support the use of intravenous thrombolysis in cardiocerebral infarction, its application warrants cautious evaluation.5 Concerns include the potential risk of cardiac rupture and the limitation of anti-thrombotic therapy within 24 hours post-thrombolysis, which may impact the feasibility and timing of subsequent percutaneous coronary intervention.2,5 The potent and reversible antiplatelet effect of tirofiban supports its potential role in the perioperative setting of endovascular therapy for acute cardiocerebral infarction.6–8 As a result, different patients may require individualized medications and treatment plans to improve their survival rate and functional prognosis. This paper presents a case of a patient with both cerebral infarction due to internal carotid artery occlusion and acute coronary syndrome, aiming to offer new insights into the diagnosis and treatment of patients with cardiocerebral infarction.
Case Report
Clinical Presentation
A 50-year-old male patient was admitted to the hospital on April 14, 2022 due to 1 day of chest tightness and 1 hour of weakness in his left limb. The patient experienced chest tightness and chest pain accompanied by profuse sweating before April 13, 2022. He exhibited weakness in his left limb one hour before arriving at the hospital and also experienced alalia, a speech disorder. He had no prior history of hypertension and diabetes. No bad habits of tobacco or alcohol use. He denied any family history of strokes or acute coronary syndrome, and he had healthy, nonconsanguineous parents. The physical examination upon admission revealed 36.8°C (T), 89 beats/min (P), 19 beats/min (R), and 125/89 mmHg (BP). The patient was agitated, but no moist rales or dry or moist crackles were detected in the lungs. His heart beat was rhythmic with 89 beats/min, and no significant pathologic murmurs were noted in each valve auscultation area. The abdomen was soft, with no tenderness, rebound tenderness, muscle tension, or edema in the lower limb. The liver and spleen could not be touched under the ribs. Further check-ups indicated that the patient had dysarthria but could provide relevant answers to questions. His pupils were equal in size, measuring 3 mm in diameter, with both direct and indirect pupillary light reflexes intact. Eyeball movements were found to be normal, and both eyeballs were centered. Additionally, the left nasolabial fold was shallow, the mouth slanted to the right, and the tongue was centered. Muscle strength in the left limb was graded at 1, while the right limb was graded at 5. Muscle tone was normal, and 2+ symmetrical tendon reflexes were observed in all limbs. The Hoffmann’s sign, Rossolimo’s sign, Babinski’s sign, and Chaddock’s sign were all negative for both limbs. The patients did not cooperate with the examination for sensory ataxia. The examination results also revealed soft neck muscles, indicating no abnormalities and Kernig’s sign for bilateral limbs was negative. The NIHSS (National Institutes of Health Stroke Scale) score was 12.
Assistant Examinations
Pre admission assistant examination at 10:51 on April 14, 2022, cardiac troponin I (cTn I) 0.013ng/mL (reference range: 0 to 0.034ng/L). Myocardial enzyme: creatine kinase 82.1 U/L, creatine kinase-myocardial band 3.41 ug/L, lactate dehydrogenase 138 U/L. Electrocardiogram: II, III, AVF leads: ST segment depression, V2-V4 leads: T wave peak.
Admission assistant examination at 11:12 on April 14, 2022, Brain CT: high density of right middle cerebral artery, no other obvious abnormalities found (Figure 1A and B). At 18:09 on April 14, 2022, blood lipid: total cholesterol 5.73 mmol/L, high-density lipoprotein 0.77 mmol/L, and low-density lipoprotein 3.96 mmol/L. Cardiac troponin I (cTn I) 12.8ng/mL. Myocardial enzyme: creatine kinase 729 U/L, creatine kinase-myocardial band 75.20 ug/L, lactate dehydrogenase 228 U/L. No significant abnormalities were found in blood routine, urine routine, stool routine, coagulation panel (four items), thyroid panel (three items), erythrocyte sedimentation rate, fasting blood-glucose, glycosylated hemoglobin, renal function, C-reactionprotein, uric acid, electrolyte, and liver function examinations. Electrocardiogram at 15:32 on April 15, 2022: sinus bradycardia; abnormal Q-wave in the anterior septal wall, suggesting anterior septal myocardial infarction; occasional ventricular premature contractions.
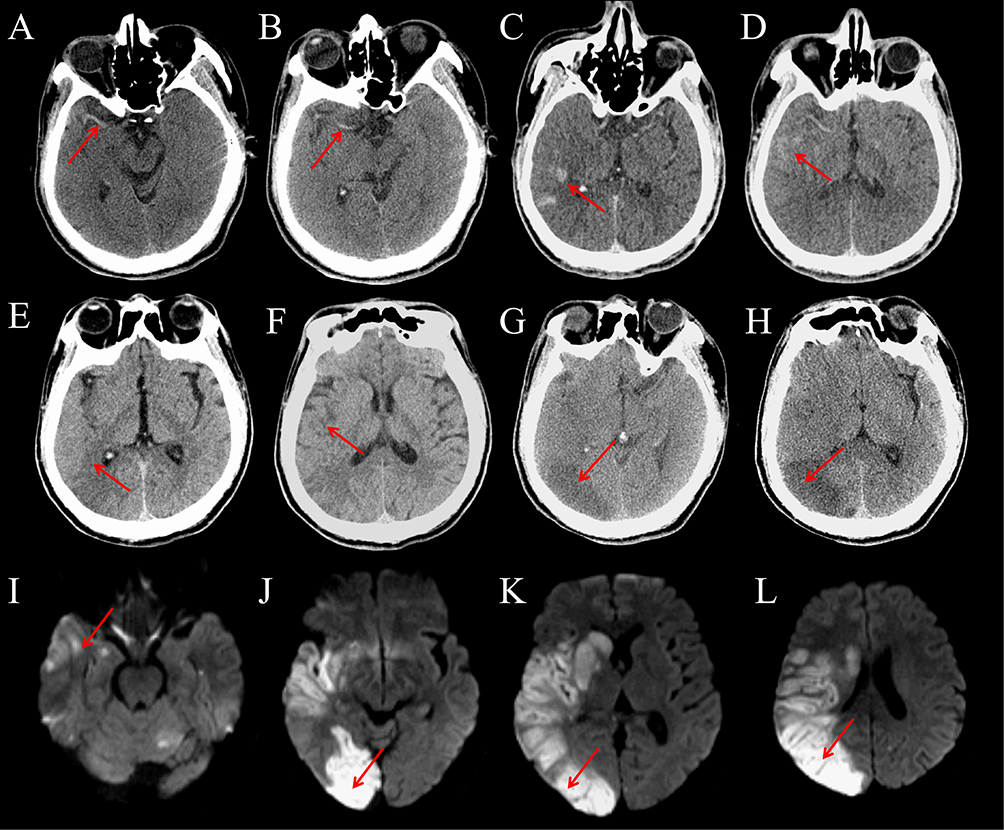 |
Figure 1 The patient’s cranial CT and MRI images. (A and B) The initial cranial CT scan after admission revealed a high-density sign in the right middle cerebral artery (red arrows). (C and D) The immediate post-surgery cranial CT scan showed slight leakage of contrast agent in the right cerebral hemisphere (red arrows). (E and F) The cranial CT scan taken 8 hours after surgery indicated absorption of the contrast agent with no signs of hemorrhage (red arrows). (G and H) The cranial CT scan taken 2 days after surgery displayed cerebral infarction foci in the right cerebral hemisphere (red arrows). (I–L) The DWI (Diffusion-Weighted Imaging) cranial MRI scan taken 4 days after surgery indicated multiple cerebral infarction foci in the right cerebral hemisphere (red arrows). |
Interventions
When cardiovascular interventional physicians and cerebrovascular interventional physicians arrive on the scene simultaneously, efficient collaboration is essential to ensure optimal patient care. After obtaining informed consent from the patient and their authorized representative, intravenous administration of 0.9 mg/kg of Alteplase was immediately initiated for thrombolytic therapy, as the patient experienced an acute cerebral infarction within 4.5 hours and had no relevant contraindications. While using alteplase infusion, endovascular diagnosis and treatment were promptly conducted without waiting for further evaluation of whether the patient’s symptoms and signs had improved. First, coronary interventional diagnosis and treatment were performed, followed by cerebrovascular interventional diagnosis and treatment. After intravenous thrombolysis, tirofiban was continuously intravenously infused at a rate of 0.4 μg/(kg·min) for 30 minutes, followed by an intravenous infusion at a rate of 0.1 μg/(kg·min) for 24 hours.
The coronary angiography revealed plaque infiltration with multiple mild-to-moderate coronary stenoses, as well as a significant stenosis (approximately 90%) in the proximal-to-mid segment of the left anterior descending artery (LAD), spanning approximately 25 mm in length, with TIMI (Thrombolysis In Myocardial Infarction) flow grade 3. According to the preoperative plan, balloon dilation and stenting were immediately performed on the LAD. A successful implantation of an Abbott drug-eluting stent (2.5*38mm) was achieved, with good stent apposition after adequate post-dilation and no residual stenosis observed. TIMI flow grade 3 was restored in the LAD, and the coronary interventional procedure was completed (Figure 2A and B).
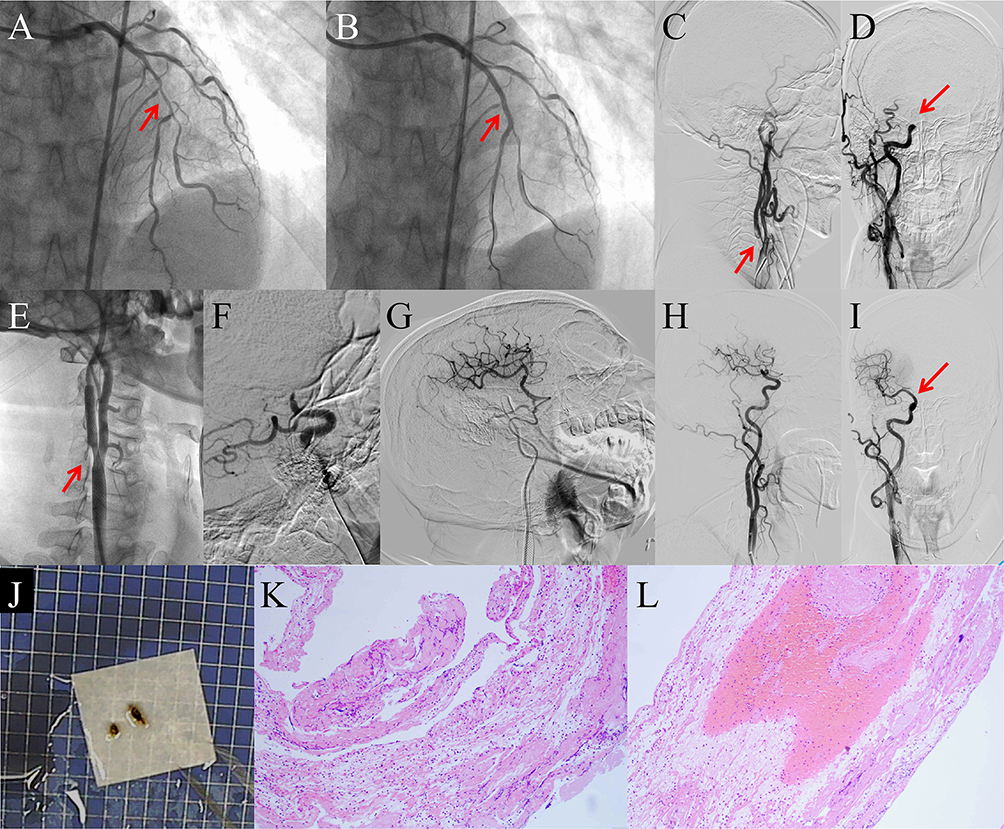 |
Figure 2 Images of the intravascular treatment process and pathology of the embolus. (A and B) Images before and after stent implantation in the left anterior descending coronary artery (red arrows indicate the site of coronary stenosis). (C–I) Images of the cerebral angiography, right carotid artery stent implantation, and intracranial artery thrombectomy process (red arrows indicate the key location during the procedure). (J–L) Pathology of the embolus indicated thrombosis. |
Immediately following the coronary angiography and PCI (Percutaneous Coronary Intervention) treatment, a cerebral angiography was performed, which indicated a significant stenosis at the origin of the right internal carotid artery (ICA) and occlusion at the terminal end of the right ICA. No obvious abnormalities were noted in the morphology and course of other cerebral arteries. Based on the cerebral angiography results, the diagnosis was considered to be thromboembolism from the origin of the right ICA, occluding the C7 segment of the right ICA.
Promptly, balloon dilation and stenting were performed on the stenotic area of the right ICA, with a successful placement of a WALLSTENT (9*50mm). Mild residual stenosis (30%) was noted. Subsequently, intracranial thrombectomy was conducted using a cat6 intracranial support catheter and a distal occlusion double-basket embolectomy device, EMBOTRAP2, successfully retrieving the embolus. Complete blood flow restoration was achieved in the occluded intracranial artery, with TIMI flow grade 3. The surgical procedure was then concluded (Figure 2C–I).
Outcome and Follow-Up
Post-surgery, continuous intravenous infusion of Tirofiban was maintained at a rate of 0.1 μg/(kg·min) for 24 hours, followed by a bridging therapy with dual antiplatelet aggregation using Aspirin and Clopidogrel. Additionally, statins were administered to stabilize plaques, blood pressure was controlled, and rehabilitation therapy was provided. The embolus pathology indicates thrombosis (Figure 2J–L). The cranial CT scans conducted post-intervention (Figure 1C and D), 8 hours post-surgery (Figure 1E and F), and 2 days post-surgery (Figure 1G and H) revealed no hemorrhagic transformation. The cerebral infarction lesion in the right cerebral hemisphere gradually appeared and remained stable Four days post-surgery, the cranial MRI also indicated multiple large infarction lesions in the right cerebral hemisphere (Figure 1I–L). His condition improved significantly after 15 days, and the weakness of the left limbs and alalia improved a lot. The physical examination indicated that the patient was conscious and could talk normally. The muscle strength of the limbs was graded 5. The NIHSS score was 1. The patient was discharged from the hospital without complications and prescribed long-term antiplatelet aggregation therapy and intensive statin treatment for outpatient care. The patient who was followed up for 1 years had stable conditions and was able to take care of himself, with an mRS score of 1.
Discussion
Challenges in Diagnosing and Treating Patients with Both Acute Ischemic Stroke and Acute Coronary Syndrome
Acute ischemic stroke and acute coronary syndrome are two life-threatening diseases that can occur simultaneously. The incidence of stroke after acute myocardial infarction ranges from 1% to 5%, with 73% of patients exhibiting atrial fibrillation and 15% having multiple blocked branches of the coronary artery.9 However, how to diagnose and treat these two kinds of diseases is different. The causes of acute cerebral infarction due to internal carotid artery occlusion vary, including in situ atherosclerotic thrombosis (ISAT), cardiac embolism, and takayasu’s arteritis. In contrast, coronary artery occlusion in cases of acute coronary syndrome is more likely caused by atherosclerosis with thrombosis.10 Blood clots from cardiac embolism can migrate from the aortic arch or carotid vascular into the intracranial arteries. Additionally, increased catecholamine release and autonomic dysfunction in patients experiencing acute myocardial infarction exacerbate platelet aggregation and contribute to thrombosis. These factors may represent the pathophysiological mechanisms that lead to acute ischemic stroke.11 When treating patients with both acute ischemic stroke and acute coronary syndrome, the initial placement of a stent to preserve myocardial function may delay stroke treatment, potentially resulting in permanent disability. Conversely, if the endovascular treatment for internal carotid artery occlusion is given first, the patient may experience cardiogenic shock or malignant arrhythmias, leading to serious consequences. Rt-PA is currently the only thrombolytic drug approved for use in treating both acute ischemic stroke and acute myocardial infarction. Patients with cerebral infarction can usually be treated with rt-PA within 4.5 hours, and bridging therapy can be provided if head and neck CTA suggest large artery occlusion.12 For cerebral infarction patients undergoing rt-PA thrombolytic therapy, the initiation of antiplatelet aggregation therapy with aspirin and clopidogrel is typically delayed to between 24–48 hours to avoid intracranial bleeding or other organ-related bleeding complications.12 The time window for thrombolysis in acute myocardial infarction is within 12 hours of onset,13 which is longer than that for acute ischemic stroke. If a coronary stent is implanted, the administration of aspirin and clopidogrel for antiplatelet therapy is typically required after the procedure. However, for patients with atrial fibrillation besides infarction, the use of drugs alone for antiplatelet aggregation may increase the risk of thrombosis due to atrial fibrillation. Vitamin K antagonist (VKA) in combination with single antiplatelet therapy (SAPT) may be the most effective treatment plan for preventing stroke for these patients.9 However, current data do not show that anticoagulation therapy is suitable for patients with acute coronary syndrome following stent placement. Similarly, patients who have undergone emergency carotid artery stenting also require antiplatelet aggregation therapy with aspirin and clopidogrel to prevent blood clot formation and subsequent vascular reocclusion. Therefore, there exists a therapeutic contradiction: for cerebral infarction patients who have undergone rt-PA intravenous thrombolysis, the administration of aspirin and clopidogrel for antiplatelet aggregation is typically delayed by more than 24 hours; however, immediate use of aspirin and clopidogrel for antiplatelet aggregation is necessary after coronary artery stenting and/or carotid artery stenting procedures. Tirofiban is a highly effective intravenous antiplatelet drug, characterized by its rapid onset and short half-life. It is particularly suited for patients undergoing coronary stent implantation and/or emergency carotid stent implantation procedures. Continuous intravenous infusion of Tirofiban can effectively prevent in-stent thrombosis while maintaining a low risk of bleeding. The specific administration method is as follows: an initial intravenous infusion at a rate of 0.4 micrograms per kilogram of body weight per minute for 30 minutes, followed by a continuous intravenous infusion at a rate of 0.1 micrograms per kilogram of body weight per minute for 24 to 72 hours. When performing endovascular treatment on patients, the adequate and timely use of Tirofiban concurrently addresses the challenge of withholding aspirin combined with clopidogrel for antiplatelet aggregation therapy within the first 24 hours after intravenous thrombolysis.14 Although patients may be within the time window for intravenous thrombolysis, the treatment outcomes for cerebral infarction and myocardial infarction are still influenced by the volume of the infarct core, the area of the ischemic penumbra, the size and nature of the thrombus, and collateral circulation. Additionally, there is a risk of reinfarction and hemorrhagic transformation, with cardiac rupture and pericardial tamponade being the most severe thrombolytic complications in patients with acute myocardial infarction. Therefore, maintaining a delicate balance between ischemia and hemorrhage simultaneously is crucial. For acute myocardial infarction patients who are in the stroke thrombolysis phase and have unstable hemodynamic status, emergency coronary stent implantation may provide benefits.15 However, the central therapeutic dilemma lies in the fact that urgent reperfusion therapy for one condition may delay or increase the risk of treatment for the other.3,16 No standardized guidelines currently exist for this scenario. A case series suggests that intravenous tissue plasminogen activator at stroke dose may be the preferred initial step, followed by endovascular coronary or cerebrovascular intervention as needed.2 However, the use of rt-PA requires careful consideration of the associated risk of cardiac rupture and the limitation of antithrombotic therapy within the subsequent 24-hour window.5 Tirofiban represents a potential antiplatelet option during this critical perioperative period following thrombolysis and subsequent coronary or neurovascular intervention.7 Therefore, the treatment steps for this patient were as follows: first, intravenous thrombolytic therapy was administered; immediately after, coronary stent implantation surgery was performed; and finally, cerebrovascular intervention was carried out. Perioperative antiplatelet coverage with tirofiban was administered within the first 24 hours post-procedure.
Safety and Prognosis of Mechanical Embolectomy After Intravenous Thrombolysis versus Mechanical Embolectomy Alone for Acute Ischemic Stroke
Previous studies have shown that the probability of restoring the blood flow within 3 hours after intravenous thrombolysis for occlusion of the intracranial segment of the internal carotid artery is quite low (4%). In contrast, this probability increases to 21% and 38% for occlusions in the M1 and M2 segments of the middle cerebral artery, respectively.17 This indicates that in anterior circulation infarction, the closer the occluded blood vessel is to the distal segment of the middle cerebral artery, the higher the probability of restoring blood flow. Conversely, the closer the blocked vessel is to the internal carotid artery and the heart, the lower the probability. Therefore, an increasing number of studies have shown that, in patients with acute ischemic stroke caused by large vessel occlusion, compared to intravenous alteplase bridging with mechanical thrombectomy within 4.5 hours after the onset of neurological deficit symptoms, mechanical thrombectomy alone results in no poorer functional prognosis over 90 days, and there is no significant difference in the incidence of complications such as cerebral hemorrhage.18–22 However, the combination of intravenous thrombolysis and mechanical embolectomy may not lead to the desired outcomes. This is partly because the use of recombinant tissue plasminogen activator (rtPA) for intravenous thrombolysis can delay the execution of mechanical thrombectomy. More importantly, rtPA increases the risk of symptomatic cerebral hemorrhage or cardiac rupture. Therefore, the risks of cerebral hemorrhage and other hemorrhagic complications are slightly higher when both methods are used together compared to mechanical thrombectomy alone. However, some scholars argue that intravenous thrombolysis, approved for the acute management of both conditions has been suggested as the best approach to the treatment of simultaneous cardiocerebral infarction if there is no contraindication, and both presentations are within the time frame for the administration of a thrombolytic.23 Several meta-analyses indicate that early intravenous administration of tirofiban within at least 24 hours after rt-PA thrombolysis, as well as its use as rescue therapy during mechanical thrombectomy when bridging with intravenous thrombolysis, is acceptably safe and does not increase the risk of intracranial hemorrhage, symptomatic intracranial hemorrhage, or distal embolization.7,8 For the patient in this study, we performed intravenous thrombolysis before mechanical thrombectomy, with perioperative administration of tirofiban. The imaging indicated a relatively large area of cerebral infarction; however, the prognosis remained favorable, with no significant symptomatic cerebral hemorrhage observed. This paper contends that the bridging treatment of intravenous thrombolysis and endovascular intervention is more suitable for treating acute stroke caused by large vessel occlusion of the anterior circulation within 4.5 hours of onset. However, during intravenous thrombolysis and mechanical thrombectomy, it is essential not to wait to assess the outcomes of thrombolysis. Without imaging indicating the site of vascular stenosis, we cannot determine whether the infarct site of anterior circulation infarction is located in the internal carotid artery or the middle cerebral artery. The probability of restoration of blood flow is low after intravenous thrombolysis for occlusion of the internal carotid artery; however, this probability is higher in cases of occlusion within the cerebral artery. It does not require preparation or puncture before the surgery, which saves time for treatment and allows for prompt reperfusion to increase the blood flow. Despite the favorable clinical outcome achieved in this patient, the single-case nature of this report is evident. Consequently, the specific management approach and positive result cannot be generalized. In summary, the decision on whether to bridge intravenous thrombolysis before mechanical thrombectomy needs to comprehensively consider the specific condition of the patient, the location and size of the thrombus, as well as the experience of the clinician. Each case should be analyzed individually to determine the most appropriate treatment approach.
Thoughts About Whether to Perform CT Perfusion Imaging for Stroke Diagnosis
When a patient presents with stroke and requires intervention, it is essential to consider five key questions: (1) is it a stroke with hemodynamic instability? (2) Can we identify an irreversible infarct core and a treatable ischemic semidarkness? (3) Is there a thrombosis or embolism that can be treated?(4) Is there sufficient collateral circulation compensation? (5) Is there a risk of injury due to hyperperfusion? Recent studies increasingly suggest that computed tomography perfusion (CTP) plays a crucial role in assessing the efficacy of intravenous thrombolysis for cerebral infarction and guiding the decision-making regarding interventional therapy.24 As we all know, CTP reveals the cerebral blood flow (CBF) and cerebral blood volume (CBV) below the normal range when acute ischemic stroke occurs, whereas the mean transit time (MTT) of the contrast agent, the transit time to peak (TTP) of the contrast agent and the time-to-maximum (Tmax) of cerebral blood flow were above the normal range.25–27 Infarcted and non-infarcted tissues can be distinguished using CBF and CBV parameters.25,26 The ischemic area can be predicted by MTT, TTP, and Tmax.27 However, it remains uncertain whether CTP plays a role in the early cerebral infarction treated with rt-PA for intravenous thrombolysis within 4.5 hours or treated with embolectomy within 6 hours. Therefore, we cannot exclude patients from treatment with mechanical embolectomy based solely on the infarct core volume predicted by CTP, particularly in patients with short onset time.28 Additionally, CTP requires approximately 20–30 min from image acquisition to reconstruction and patient transportation, which can result in delays in the emergency treatment for some patients with acute ischemic stroke. However, for cerebral infarctions exceeding 6 hours due to large vessel occlusion, this delay is irrelevant, regardless of whether there is infarcted brain tissue present. That is because the collateral circulation compensation may play an important role rather than the time window at the time.29 Furthermore, CTA of the head and neck and CTP of the head significantly elevate the level of contrast agents in the body, thereby increasing the risk of contrast agents damaging the brain tissue or contrast-induced encephalopathy (CIE). Therefore, for cerebral infarction caused by large vessel occlusion of the anterior circulation within 6 hours after onset, patients who have the indications can receive endovascular therapy without requiring perfusion imaging or other imaging examinations. If the condition persists beyond 6 hours, CTP should be performed first to find the infarct core area and the volume of the ischemic penumbra, and then endovascular treatment should be provided after assessing the risk.30 In this case, we determined that the cerebral infarction occurred within 6 hours, and the patient also had acute coronary syndrome; therefore, we opted not to perform CTA and CTP examinations to expedite treatment. Additionally, our clinical experience indicates that the peak edema of infarcted brain tissue occurs earlier after endovascular treatment compared to conservative drug therapy, and glucocorticoid could delay this peak. Glucocorticoids can inhibit the inflammatory response, reduce the infiltration of inflammatory cells in brain tissue, make cerebral blood vessels less permeable, improve the interstitial edema, increase cerebral blood flow, improve the blood supply of brain tissue, reduce the effect of contrast agent on brain tissue edema, lower the risk of cerebral hernia due to the peak of edema, and improve the functional prognosis for patients with large cerebral infarction.31 Although among patients with acute ischemic stroke due to large-vessel occlusion undergoing endovascular thrombectomy, adjunctive methylprednisolone added to endovascular thrombectomy did not significantly improve the degree of overall disability, it could significantly reduce mortality, severe disability, and symptomatic intracranial hemorrhage risk.31 So we prophylactically administered medium-dose glucocorticosteroids (methylprednisolone 2–3 mg/kg for 3 days) which resulted in favorable outcomes.
Conclusions
The selection of the most effective treatment plan for cerebral infarction caused by internal carotid artery occlusion and acute coronary syndrome varies significantly among individuals. Intravenous thrombolysis, mechanical thrombectomy, and percutaneous coronary intervention are all viable treatment options. The therapeutic sequence of coronary stenting followed by endovascular thrombectomy and carotid artery stenting may have been critical to the patient’s favorable clinical outcome. While Antiplatelet aggregation is crucial during the perioperative period of carotid artery stenting or/and coronary stent implantation, its initiation within 24 hours of intravenous thrombolysis must balance efficacy against bleeding risk. Tirofiban represents a potential option during this high-risk period. This strategy proved effective in this specific patient, but its efficacy needs to be validated in larger-scale studies. Additionally, for cerebral infarction caused by large vessel occlusion in the anterior circulation within 6 hours after onset, patients who meet the criteria can receive endovascular treatment without the need for perfusion imaging examinations.
Ethical Approval
All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Ethical approval was obtained from The Medical Ethics Committee of Shenzhen Longhua District Central Hospital, and separate approval for the publication of the case details was not required.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Acknowledgments
We would like to express our gratitude to the patient for granting permission to use the patient’s clinical data in this paper and for the publication of this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Key Medical Discipline Construction Fund of Shenzhen Longhua District.
Disclosure
The authors report no competing interests in this work.
References
1. de Castillo LLC, Diestro JDB, Tuazon CAM, et al. Cardiocerebral infarction: a single institutional series. J Stroke Cerebrovasc Dis. 2021;30(7):105831. doi:10.1016/j.jstrokecerebrovasdis.2021.105831
2. Chong CZ, Tan BY, Sia CH, et al. Simultaneous cardiocerebral infarctions: a five-year retrospective case series reviewing natural history. Singapore Med J. 2022;63(11):686–10. doi:10.11622/smedj.2021043
3. Pastore C, White M, Henry M, et al. Simultaneous cardiocerebral infarction associated with postcoital activity. J Emerg Med. 2023;65(6):e554–e558. doi:10.1016/j.jemermed.2023.08.008
4. Zou L, Han R. Inflammatory response and immune regulation in brain-heart interaction after stroke. Cardiovasc Ther. 2022;2022:2406122. doi:10.1155/2022/2406122
5. Kume H, Maeda T, Tsukagoshi E, et al. Cardiocerebral infarction presenting in a neurosurgical emergency: a case report and literature review. Cureus. 2024;16(7):e65124. doi:10.7759/cureus.65124
6. Kong W, Liu G, Zhu H, et al. Effect of intravenous tirofiban on the efficacy and safety of stent retriever versus aspiration first-line thrombectomy secondary analysis of the RESCUE BT trial. Int J Surg. 2025. doi:10.1097/JS9.0000000000003886
7. Liu Q, Lu X, Yang H, et al. Early tirofiban administration for patients with acute ischemic stroke treated with intravenous thrombolysis or bridging therapy: systematic review and meta-analysis. Clin Neurol Neurosurg. 2022;222:107449. doi:10.1016/j.clineuro.2022.107449
8. Bai P, Yao Y, Zhen J, et al. The efficacy and safety of tirofiban plus thrombolysis and thrombolysis alone for acute ischemic stroke: a meta-analysis. Am J Emerg Med. 2026;99:416–423. doi:10.1016/j.ajem.2025.10.048
9. Boyanpally A, Cutting S, Furie K. Acute ischemic stroke associated with myocardial infarction: challenges and management. Semin Neurol. 2021;41(4):331–339. doi:10.1055/s-0041-1726333
10. Yadav V, Gajurel RM, Poudel CM, et al. A rare coexistence of simultaneous cardio-cerebral infarction. Case Rep Cardiol. 2023;2023:9986712. doi:10.1155/2023/9986712
11. Hattori Y, Tagawa N, Nakamura M, et al. Impact of blood flow volume in determining the destination of intracardiac thrombi using computational fluid dynamics. eNeurologicalSci. 2022;29:100437. doi:10.1016/j.ensci.2022.100437
12. Liu L, Chen W, Zhou H, et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of ischaemic cerebrovascular diseases. Stroke Vasc Neurol. 2020;5(2):159–176. doi:10.1136/svn-2020-000378
13. Mora-Solorzano L, Gutierrez-Diaz GI, Gudino-Amezcua DA, et al. Clinical characteristics of patients with acute myocardial infarction treated with thrombolysis] [J. Rev Med Inst Mex Seguro Soc. 2020;58(2):100–107. doi:10.24875/RMIMSS.M20000006
14. Zhang Y, Wang J, Ma Z, et al. Prospective pilot study of tirofiban in progressive stroke after intravenous thrombolysis. Front Neurol. 2022;13:982684. doi:10.3389/fneur.2022.982684
15. Bao CH, Zhang C, Wang XM, et al. Concurrent acute myocardial infarction and acute ischemic stroke: case reports and literature review. Front Cardiovasc Med. 2022;9:1012345. doi:10.3389/fcvm.2022.1012345
16. Kijpaisalratana N, Chutinet A, Suwanwela NC. Hyperacute simultaneous cardiocerebral infarction: rescuing the brain or the heart first? Front Neurol. 2017;8:664. doi:10.3389/fneur.2017.00664
17. Seners P, Turc G, Maier B, et al. Incidence and predictors of early recanalization after intravenous thrombolysis: a systematic review and meta-analysis. Stroke. 2016;47(9):2409–2412. doi:10.1161/STROKEAHA.116.014181
18. LeCouffe NE, Kappelhof M, Treurniet KM, et al. A randomized trial of intravenous alteplase before endovascular treatment for stroke. N Engl J Med. 2021;385(20):1833–1844. doi:10.1056/NEJMoa2107727
19. Quang Anh N, Dang Luu V, Hoang Khoe L, et al. Effect of mechanical thrombectomy with vs. without intravenous thrombolysis in acute ischemic stroke. Clin Ter. 2022;173(3):257–264. doi:10.7417/CT.2022.2429
20. Sallustio F, Koch G, Alemseged F, et al. Effect of mechanical thrombectomy alone or in combination with intravenous thrombolysis for acute ischemic stroke. J Neurol. 2018;265(12):2875–2880. doi:10.1007/s00415-018-9073-7
21. Jadhav AP, Zaidat OO, Liebeskind DS, et al. Emergent management of tandem lesions in acute ischemic stroke. Stroke. 2019;50(2):428–433. doi:10.1161/STROKEAHA.118.021893
22. Wang J, Qian J, Fan L, et al. Efficacy and safety of mechanical thrombectomy for M2 segment of middle cerebral artery: a systematic review and meta-analysis. J Neurol. 2021;268(7):2346–2354. doi:10.1007/s00415-020-09710-w
23. Akinseye OA, Shahreyar M, Heckle MR, et al. Simultaneous acute cardio-cerebral infarction: is there a consensus for management? Ann Transl Med. 2018;6(1):7. doi:10.21037/atm.2017.11.06
24. Broocks G, McDonough RV, Bechstein M, et al. Thrombectomy in patients with ischemic stroke without salvageable tissue on CT perfusion. Stroke. 2024;55(5):1317–1325. doi:10.1161/STROKEAHA.123.044916
25. Shankar JJ, Langlands G, Doucette S, et al. CT perfusion in acute stroke predicts final infarct volume- inter-observer study. Can J Neurol Sci. 2016;43(1):93–97. doi:10.1017/cjn.2015.349
26. Jovin TG, Saver JL, Ribo M, et al. Diffusion-weighted imaging or computerized tomography perfusion assessment with clinical mismatch in the triage of wake up and late presenting strokes undergoing neurointervention with Trevo (Dawn) trial methods. Int J Stroke. 2017;12(6):641–652. doi:10.1177/1747493017710341
27. Dababneh H, Bashir A, Guerrero WR, et al. Mean transit time on Aquilion ONE and its utilization in patients undergoing acute stroke intervention. J Vasc Interv Neurol. 2014;7(5):73–81.
28. Xu XQ, Ma G, Lu SS, et al. Predictors of ghost infarct core on baseline computed tomography perfusion in stroke patients with successful recanalization after mechanical thrombectomy. Eur Radiol. 2023;33(3):1792–1800. doi:10.1007/s00330-022-09189-1
29. Alexandre AM, Pedicelli A, Valente I, et al. May endovascular thrombectomy without CT perfusion improve clinical outcome? Clin Neurol Neurosurg. 2020;198:106207. doi:10.1016/j.clineuro.2020.106207
30. Wu RR, Cao YZ, Xu XQ, et al. ASPECTS-based net water uptake outperforms target mismatch for outcome prediction in patients with acute ischemic stroke and late therapeutic window. Eur Radiol. 2023;33(12):9130–9138. doi:10.1007/s00330-023-09965-7
31. Yang Q, Guo C, Yue C, et al. Methylprednisolone as adjunct to endovascular thrombectomy for large-vessel occlusion stroke: the MARVEL randomized clinical trial. JAMA. 2024;331(10):840–849. doi:10.1001/jama.2024.0626
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognosis of Ischemic Stroke Patients Undergoing Endovascular Thrombectomy is Influenced by Systemic Inflammatory Index Through Malignant Brain Edema
Ji Y, Xu X, Wu K, Sun Y, Wang H, Guo Y, Yang K, Xu J, Yang Q, Huang X, Zhou Z
Clinical Interventions in Aging 2022, 17:1001-1012
Published Date: 2 July 2022
Combination of TyG Index and GRACE Risk Score as Long-Term Prognostic Marker in Patients with ACS Complicated with T2DM Undergoing PCI
Qin Z, Xu S, Yuan R, Wang Z, Lu Y, Xu Y, Lv Y, Yu F, Bai J, Zhang H, Zhang L, Zhang J, Tang J
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3015-3025
Published Date: 28 September 2022
Advanced Lung Cancer Inflammation Index for Predicting Prognostic Risk for Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention
Wang X, Wei C, Fan W, Sun L, Zhang Y, Sun Q, Liu Y, Liu J
Journal of Inflammation Research 2023, 16:3631-3641
Published Date: 23 August 2023
Prognostic Nutritional Index Combined with Triglyceride-Glucose Index to Contrast a Nomogram for Predicting Contrast-Induced Kidney Injury in Type 2 Diabetes Mellitus Patients with Acute Coronary Syndrome After Percutaneous Coronary Intervention
Zhu Y, He H, Qiu H, Zhang X, Wang L, Li W
Clinical Interventions in Aging 2023, 18:1663-1673
Published Date: 3 October 2023
The Impact of Patient Adherence to Dual Antiplatelet Medication Following Percutaneous Coronary Intervention on the Occurrence of Adverse Cardiovascular Events
Mansurova JA, Orekhov A, Zhunuspekova AS, Kassymova AA, Karazhanova LK
Patient Preference and Adherence 2024, 18:425-434
Published Date: 17 February 2024