Back to Journals » Journal of Inflammation Research » Volume 14
Composite Inflammatory Indicators as Early Predictor of Intra-abdominal Infections after General Surgery
Received 23 September 2021
Accepted for publication 1 December 2021
Published 21 December 2021 Volume 2021:14 Pages 7173—7179
DOI https://doi.org/10.2147/JIR.S340745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Jiakun Song, Yurong Lu
Emergency Department, Sandun District of Zhejiang Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Yurong Lu
Emergency Department, Sandun District of Zhejiang Hospital, 1229 Gudun Road, Xihu District, Hangzhou, Zhejiang 310030, People’s Republic of China
Tel +86-137-0581-4277
Email [email protected]
Objective: To identify rapid and accurate early diagnostic indicators for intra-abdominal infection (IAI) after general surgery.
Methods: We conducted a retrospective analysis of 3,810 general surgical patients in our hospital from August 2017 to July 2018. The predictive value of PCT, CRP, TNFα, and IL6 on postoperative days (PODs) 1 and 3 and composite indicators for complicated IAIs among surgical patients was clarified.
Results: There were 271 patients in the infected group and 614 patients in the uninfected group using IAI diagnostic criteria in this study. CRP, PCT, TNFα, and IL6 in the infected group were significantly higher than the uninfected group on POD1 and POD3. In the infected group, the composition of the four indicators on POD1 (AUC 0.819) and POD3 (AUC 0.848) showed higher predictive efficiency than the individual indicators (AUC 0.670– 0.805).
Conclusion: The composite of CRP, PCT, TNFα, and IL6 can be used as a predictor of postoperative abdominal infectious complications with high sensitivity and specificity on POD1 and POD3, which can provide a basis for early diagnosis of postoperative abdominal infectious complications.
Keywords: procalcitonin, C-reactive protein, TNFα, IL6, intra-abdominal infection
Introduction
One of the most common clinical treatments, general surgery can treat acute abdominal infections (AIs) quickly and effectively, as well as many other abdominal diseases. However, abdominal surgery has a higher risk of infectious complications than surgery on other body parts, due to human abdominal characteristics of anatomic structure and a large number of microbiota colonizing the gastrointestinal tract.1,2 Intra-AI (IAI) is a common infectious complication after abdominal surgery. Studies have shown that postoperative infections following abdominal surgery account for 2%–20% of nosocomial infections.3,4 Moreover, the local infection may expand and develop into bacteremia, which can cause death when the infection is severe.3,4 Therefore, prediction of infectious comorbidities at an early stage by reliable methods is very important for the diagnosis and anti-infective treatment of patients undergoing abdominal surgery.
Inflammatory factors and protein mediators (cytokines, chemokines, acute-phase proteins) play an important role in IAIs.5 A meta-analysis comparing the predictive abilities of CRP and PCT for IAIs after elective colorectal surgery6 indicated that these biomarkers could be used to ensure safe early discharge after elective colorectal surgery.6 Serum levels of PCT and CRP have also correlated with IAIs after colorectal cancer operation.7 Patients with IAIs after colorectal cancer surgery show increased IL6 in serum.8 Some biomarkers associated with intestinal injury have been explored to identify AI, such as iFABP. Surgical trauma and severe intestinal sepsis can lead to elevated iFABP concentrations in plasma, providing a direction for new biomarker development.9 Even so, inflammation is one of the most important responses caused by infection.10,11 Currently, a single inflammatory indicator is used to evaluate infectious comorbidities in most studies in this field, such as white blood–cell count,12 CRP,13 PCT, and IL6.14 However, these traditional indicators are frequently affected by many other factors or one another, which makes them unable to accurately predict or reflect the situation and severity of infection comorbidities after abdominal surgery.12–16 In this study, we conducted a retrospective analysis of levels of CRP, PCT, and other inflammatory factors in patients who had undergone abdominal surgery, aiming to evaluate the combined predictive value of these indicators for postoperative IAIs.
Methods
Patients
Patients who had had emergency surgery, including acute appendicitis, alimentary canal perforation, and acute cholecystitis, at our hospital from August 2017 to July 2018 (n=3,810) were enrolled in this study. Demographic information and the clinical test results were collected, mainly routine blood tests on postoperative days (PODs) 1 and 3, bacteriology tests, imaging tests, and infection-related indicators. Inclusion criteria were age >18 years, no other surgery within 6 months, and no history of tumors, autoimmune disease, or urinary system disease. Exclusion criteria were incomplete clinical data, fungal infections, neoplastic disease, preoperative body temperature >37.2°C, preoperative white blood–cell count >10×109/L, and other related wasting or primary disease. This study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Zhejiang Hospital (2021, 71K).
Based on postoperative clinical symptoms and bacteriological test results, patients were divided into a postoperative intra-abdominal infected group and postoperative abdominal uninfected group. IAI was defined as one or more of the following symptoms appearing within 30 days after surgery:17 positive bacterial culture of abdominal drainage fluid, peritoneal puncture fluid or other specimens; negative bacterial culture but abdominal pain with fever lasting >3 days; pus identified from abdominal secretions or drainage fluid; celiac abscess proven by abdominal paracentesis and imaging tests; and definite IAI supported by further surgery. The remaining patients were included in the uninfected group.
Bacterial Culture and Identification
Patients’ incision secretions, peritoneal puncture fluid, peripheral blood, urine, and other specimens were collected to be used for bacterial culture and identification, conducted strictly in accordance with National Clinical Laboratory Procedures. Bacterial cultures were obtained and identified using a VITEK 2 automatic microorganism analyzer (BioMérieux).
Detection Methods for Inflammatory Indicators
Peripheral venous blood (5 mL) collected from all patients on POD1 and POD3 were used for CRP and PCT testing. Based on manufacturers’ instructions, CRP was tested using an Omlipo automatic specific protein analyzer (Guosai Biotechnology) and PCT using a Maglumi 1000 automated chemiluminescence immunoassay analyzer (Snibe). Another 5 mL peripheral venous blood was taken from each patient’s arm, then serum collected by centrifugation for 15 minutes at 3,000 rpm. Serum levels of TNFα and IL6 were measured using ELISA kits (Cusabio Biotech) in accordance with the manufacturer’s protocols. Briefly, 50 µL of calibrators samples per well and a series of standards with known concentrations were added to a 96-well plate and incubated for 1 hour at 37°C. After that, the plate was washed five times and incubated with streptavidin–HRP for 1 hour at 37°C. After being washed another five times, the plate was incubated with a substrate mix for 15 minutes at 37°C in the dark. Finally, the reaction was terminated with a stop solution and the plate read at 450 and 570 nm using a Multiskan FC (Thermo Fisher Scientific).
Statistical Analyses
SPSS 22.0 was used for statistical analysis. Correlations of intra-abdominal infected parameters and levels of inflammatory indicators on POD1 and POD3 were analyzed using t-tests. Normally distributed measurement data are expressed as means ± SD, and were analyzed using ANOVA. Receiver-operating characteristic (ROC) curves were used to assess the predictive value of inflammatory indicators for postoperative IAIs. Statistical significance was set at P<0.05.
Results
Patient Characteristics
Of the 3,810 general abdominal surgery cases, 885 patients met the inclusion and exclusion criteria. Postoperative infectious complications were diagnosed in 271 patients, comprising the infected group (Figure 1). The remaining 614 patients without postoperative infections comprised the uninfectious group. Basic information on the infected and uninfected groups is listed in Table 1 and Supplementary Table 1. No significant differences in terms of age and sex were found between the groups (P>0.05). Maximum body temperature in the infected group was higher than the uninfected group (P=0.008). There were 320 strains of pathogenic bacteria cultured from specimens in 271 cases with postoperative IAIs. Among them, 203 were Gram-negative bacilli (63.58%), mainly Escherichia coli (24.10%), Pseudomonas aeruginosa (14.97%), and Klebsiella (8.30%). In 117 strains of Gram-positive bacilli (36.42%), the dominant strain was Staphylococcus aureus, accounting for 13.39%, followed by S. haemolyticus (7.41%) (Table 2).
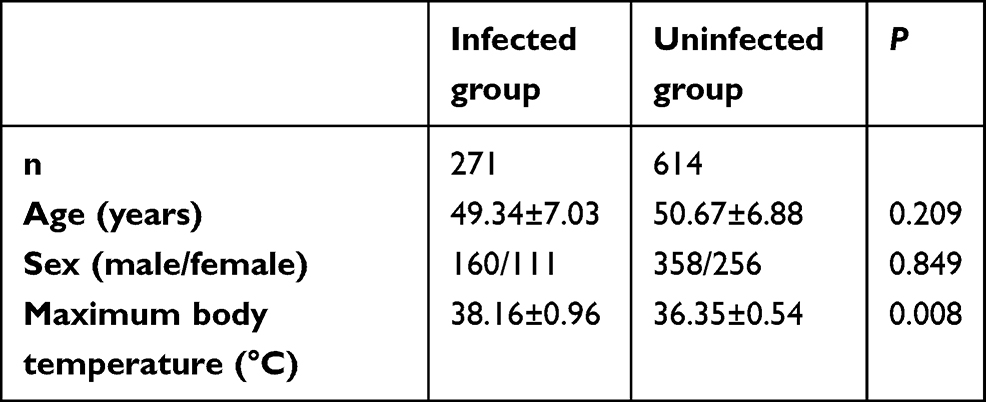 |
Table 1 Characteristics of patients after emergency operation |
 |
Table 2 Detection of pathogenic bacteria detection in patients with postoperative infections |
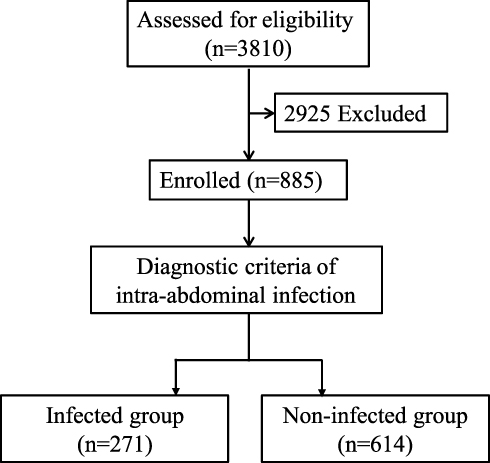 |
Figure 1 Flowchart of this study. Abbreviation: POD, postoperative day. |
Laboratory Outcomes of Patients after General Abdominal Surgery
When compared with patients without postoperative infections, blood levels of CRP, PCT, TNFα, and IL6 on POD1 were significantly increased in patients with postoperative infections (P<0.001, Figure 2). On POD3, blood levels of inflammatory indicators between patients with and without postoperative infections were more pronounced for CRP (8.93±9.46 mg/L versus 5.17±0.83 mg/L,P<0.001), PCT (4.52±5.59 mg/L versus 2.47±0.46 mg/L, P<0.001), TNFα (14.05±13.16 pg/mL versus 5.95±2.14 pg/mL, P<0.001), and IL6 (14.14±16.21 pg/mL versus 5.21±1.69 pg/mL, P<0.001; Figure 2).
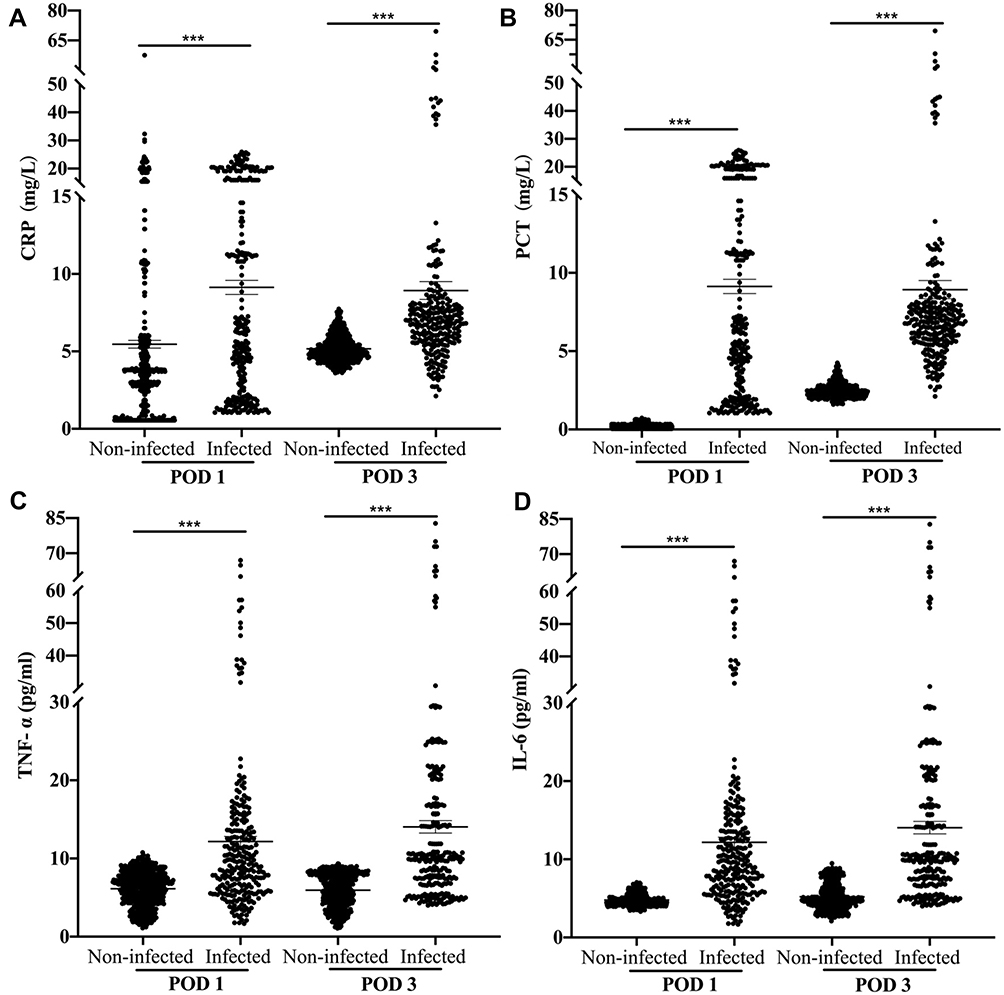 |
Figure 2 Inflammatory indicators in patients with or without postoperative infections on POD1 and POD3. Bars represent means ± SEM. ***P<0.001. (A) The level of CRP in patients on POD1 and POD3; (B) the level of PCT in patients on POD1 and POD3; (C) the level of TNF-α in patients on POD1 and POD3; (D) the level of IL-6 in patients on POD1 and POD3. Abbreviation: POD, postoperative day. |
Predictive Power of Each Marker for Postoperative Infections
We calculated the ROCs of PCT, CRP, IL6, and TNFα on POD1 and POD3, and there were with high AUC values (Figure 3). In detail, for PCT, CRP, IL6, and TNFα on POD1 (Figure 3A), AUCs for postoperative infection versus noninfection were 0.670, 0.797, 0.741, and 0.698, respectively. Similarly, inflammatory indicators on POD3 showed significantly different AUCs for postoperative infection versu uninfection (PCT 0.714, CRP0.794, TNFα 0.796, and IL6 0.786; Figure 3B). AUCs of all indicators increased from POD1 to POD3.
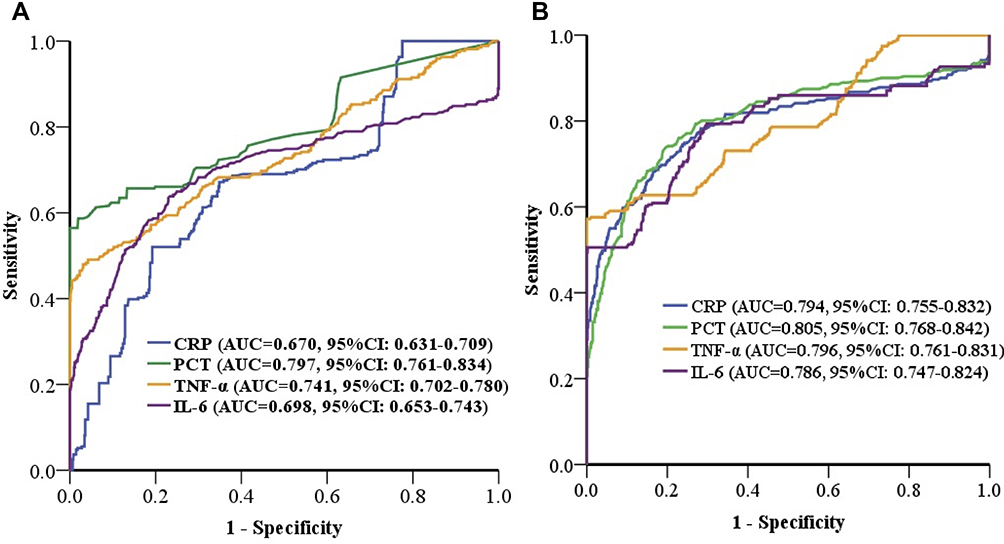 |
Figure 3 Performance of inflammatory indicators in prediction of postoperative infections. (A) ROC curves for CRP, PCT, TNFα, and IL6 on POD1; (B) ROC curves of CRP, PCT, TNFα, and IL6 on POD3. |
Predictive Power of Composite Markers for Postoperative Infection
We further tested whether combinations of PCT, CRP, IL6, and TNFα as composite indicators were more powerful for the prediction of postoperative infections. Two, three, and four composites were evaluated by logistic regression analysis and compared by ROC analyses. AUCs of composites on POD1 and POD3 were 0.819 and 0.848, respectively. AUCs of composites on POD1 and POD3 were significantly higher than those of each single indicator (Figure 4). Furthermore, the AUC of a composite of all four biomarkers was higher than that of any other composites (Supplementary Figure 1).
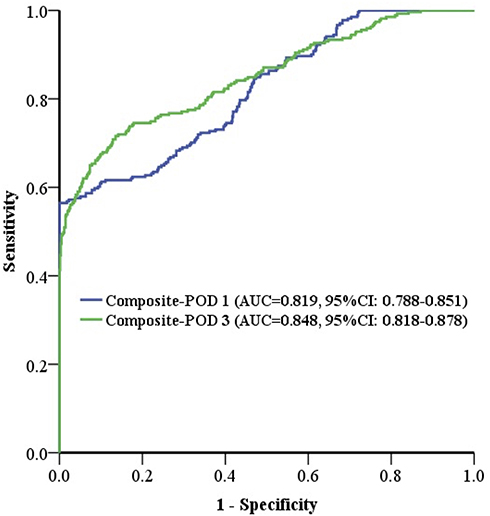 |
Figure 4 Performance of the combined inflammatory indicators for prediction of postoperative infections. Abbreviation: POD, postoperative day. |
Discussion
IAIs was a common complication after general surgery, which has become one of the primary reasons for postoperative infection.18 In our study, there were 320 strains of pathogenic bacteria cultured from specimens in 271 cases with postoperative IAIs, suggesting one patient could be infected by more than one bacterium. Among them, the dominant strain was S. aureus, accounting for 13.39%, followed by S. haemolyticus (7.41%). Therefore, in the surgical procedures, it was necessary to pay more attention to preventing infection by Gram-negative bacilli while simultaneously avoiding infection by Gram-positive bacilli, particularly S. aureus.19,20
Currently, one of the standards for etiological diagnosis of IAIs is bacterial cultures; however, the long time spent on bacterial cultures and the low positive rate of bacteria cannot meet the clinical requirements for rapid and accurate pathogenic diagnosis.21,22 Therefore, looking for fast and reliable indicators could help in the diagnosis of IAIs after general surgery at an early stage, which has important clinical significance for anti-infective treatment.23–25 As one of the most common inflammatory indicators, CRP was used to distinguish bacterial infections from viral infections, and there were significant increases bacterial infection. However, there was also an aspecific increase in CRP in some situations without infection, such as uninfectious inflammatory reactions, which could decrease the specificity of CRP in diagnosing postoperative infection.13,26,27 A sensitive indicator of bacterial pathogen infection, PCT had become an important inflammatory biomarker for identifying bacterial respiratory infections, bloodstream infections, and urinary system infections.28 Serum PCT can rise rapidly and last for a long time in patients with bloodstream infection, which is valuable in the early diagnosis of bacterial infections.29–31 In this study, AUCs of PCT for the postoperative infection were high on both POD1 and POD3.
TNFα and IL6 are important proinflammatory factors that are released early in the course of inflammation.32,33 The former can be activated by endotoxins and mediate the synthesis of a variety of inflammatory factors and severe infection complications, continuously increasing the severity of the inflammatory response by activating the massive secretion of IL6 and other inflammatory factors. IL6 can also regulate immunoresponse, acute-phase response, and hematopoietic function.34 Elevated IL6 levels are found at the onset of disease. It has been shown that IL6 is directly related to the severity and duration of severe infection, and dynamic detection of IL6 is useful in assessment to determine the outcome and prognosis of patients with sepsis.35,36 In this study, we found that serum expression of IL6 and TNFa were associated with IAIs in patients after operation, especially high levels of IL6, analogous to variations in CRP levels, consistent with a previous study.37 PCT, IL6, and TNFα can be used to judge the severity of surgical IAIs at an early stage.37 We found a composite of these indicators can also increase the reliability of prediction of postoperative infections. Moreover, the predictive value on POD3 was better than POD1, which can be used for clinical diagnosis for postoperative infections. As shown in our study and others,4,7,38 inflammatory factors and protein mediators, such as PCT, CRP, IL6, and TNFα, can play an important role in patients with IAIs after emergency surgery. Although the key mechanism in disease is still not completely understood, their prognostic value in identifying patients with complicated IAIs can be applied to clinical diagnostic. Multiple combinations could increase their value in clinical application. Although the inflammation response was thought to be directly related to infection, there are also some biomarkers associated with other pathology and mechanisms of infection, such as iFABP,9 which has been identified as a sensitive biomarker for abdominal surgery and AIs. These studies also provide guidance in the development of new diagnosis and treatment for IAIs.
Conclusion
We verified that the peripheral blood inflammatory indicators PCT, CRP, IL6, and TNFα may indicate an infection after an abdominal operation. A composite of the four had higher predictive efficiency than each individually, and thus has the capacity to predict postoperative IAIs, which might further provide guidance on the antimicrobial treatment of patients with IAIs. However, these findings need further confirmation in larger-scale clinical studies.
Acknowledgment
We gratefully acknowledge the editor and two anonymous reviewers for their review and suggestions. We would also like to thank Dr Si Yang for providing language help.
Disclosure
The authors declare no conflicts of interest that pertain to this work.
References
1. Colas-Ruiz E, Del-Moral-Luque JA, Gil-Yonte P, et al. Incidence of surgical site infection and risk factors in rectal surgery: a prospective cohort study. Cir Esp. 2018;96(10):640–647. doi:10.1016/j.ciresp.2018.06.007
2. Eeftinck Schattenkerk LD, Musters GD, Nijssen DJ, et al. The incidence of abdominal surgical site infections after abdominal birth defects surgery in infants: a systematic review with meta-analysis. J Pediatr Surg. 2021;56(9):1547–1554. doi:10.1016/j.jpedsurg.2021.01.018
3. de Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, Vaughn BB. Surgical site infection: incidence and impact on hospital utilization and treatment costs. Am J Infect Control. 2009;37(5):387–397. doi:10.1016/j.ajic.2008.12.010
4. Lytvyn L, Quach K, Banfield L, Johnston BC, Mertz D. Probiotics and synbiotics for the prevention of postoperative infections following abdominal surgery: a systematic review and meta-analysis of randomized controlled trials. J Hosp Infect. 2016;92(2):130–139. doi:10.1016/j.jhin.2015.08.028
5. Xiao Z, Wilson C, Robertson HL, et al. Inflammatory mediators in intra-abdominal sepsis or injury - a scoping review. Crit Care. 2015;19:373. doi:10.1186/s13054-015-1093-4
6. Cousin F, Ortega-Deballon P, Bourredjem A, Doussot A, Giaccaglia V, Fournel I. Diagnostic accuracy of procalcitonin and C-reactive protein for the early diagnosis of intra-abdominal infection after elective colorectal surgery: a meta-analysis. Ann Surg. 2016;264(2):252–256. doi:10.1097/SLA.0000000000001545
7. Michno M, Sydor A, Wałaszek M, Sułowicz W. Microbiology and drug resistance of pathogens in patients hospitalized at the nephrology department in the South of Poland. Polish J Microbiol. 2018;67(4):517–524. doi:10.21307/pjm-2018-061
8. Alonso S, Pascual M, Salvans S, et al. Postoperative intra-abdominal infection and colorectal cancer recurrence: a prospective matched cohort study of inflammatory and angiogenic responses as mechanisms involved in this association. Eur J Surg Oncol. 2015;41(2):208–214. doi:10.1016/j.ejso.2014.10.052
9. Bingold TM, Franck K, Holzer K, et al. Intestinal fatty acid binding protein: a sensitive marker in abdominal surgery and abdominal infection. Surg Infect. 2015;16(3):247–253. doi:10.1089/sur.2014.073
10. Pleuger C, Silva EJR, Pilatz A, Bhushan S, Meinhardt A. Differential immune response to infection and acute inflammation along the epididymis. Front Immunol. 2020;11:599594. doi:10.3389/fimmu.2020.599594
11. Grondman I, Pirvu A, Riza A, Ioana M, Netea MG. Biomarkers of inflammation and the etiology of sepsis. Biochem Soc Trans. 2020;48(1):1–14. doi:10.1042/BST20190029
12. Yu CW, Juan LI, Wu MH, Shen CJ, Wu JY, Lee CC. Systematic review and meta-analysis of the diagnostic accuracy of procalcitonin, C-reactive protein and white blood cell count for suspected acute appendicitis. Br J Surg. 2013;100(3):322–329. doi:10.1002/bjs.9008
13. Adamina M, Warschkow R, Naf F, et al. Monitoring c-reactive protein after laparoscopic colorectal surgery excludes infectious complications and allows for safe and early discharge. Surg Endosc. 2014;28(10):2939–2948. doi:10.1007/s00464-014-3556-0
14. Facy O, Paquette B, Orry D, et al. Inflammatory markers as early predictors of infection after colorectal surgery: the same cut-off values in laparoscopy and laparotomy? Int J Colorectal Dis. 2017;32(6):857–863. doi:10.1007/s00384-017-2805-9
15. Katz JA, Mustafa MM, Bash RO, Cash JV, Buchanan GR. Value of C-reactive protein determination in the initial diagnostic evaluation of the febrile, neutropenic child with cancer. Pediatr Infect Dis J. 1992;11(9):708–712. doi:10.1097/00006454-199209000-00007
16. Facy O, Paquette B, Orry D, et al. Diagnostic accuracy of inflammatory markers as early predictors of infection after elective colorectal surgery: results from the IMACORS study. Ann Surg. 2016;263(5):961–966. doi:10.1097/SLA.0000000000001303
17. Wu XW, Ren JA. [Interpretation of domestic and foreign guidelines on diagnosis and treatment of abdominal infection]. Zhonghua Wei Chang Wai Ke Za Zhi. 2020;23(11):1023–1027. Chinese. doi:10.3760/cma.j.cn.441530-20200810-00466
18. De Simone B, Sartelli M, Coccolini F, et al. Intraoperative surgical site infection control and prevention: a position paper and future addendum to WSES intra-abdominal infections guidelines. World J Emerg Surg. 2020;15(1):10. doi:10.1186/s13017-020-0288-4
19. Ejaz A, Schmidt C, Johnston FM, Frank SM, Pawlik TM. Risk factors and prediction model for inpatient surgical site infection after major abdominal surgery. J Surg Res. 2017;217:153–159. doi:10.1016/j.jss.2017.05.018
20. Salem F, Almquist M, NordenstroM E, et al. A nested case–control study on the risk of surgical site infection after thyroid surgery. World J Surg. 2018;42(8):2454–2461. doi:10.1007/s00268-018-4492-2
21. Rasilainen SK, Juhani MP, Kalevi LA. Microbial colonization of open abdomen in critically ill surgical patients. World J Emerg Surg. 2015;10:25. doi:10.1186/s13017-015-0018-5
22. Wang T, Wang H, Yang DL, Jiang LQ, Zhang LJ, Ding WY. Factors predicting surgical site infection after posterior lumbar surgery: a multicenter retrospective study. Medicine. 2017;96(5):e6042. doi:10.1097/MD.0000000000006042
23. Leone S, Damiani G, Pezone I, et al. New antimicrobial options for the management of complicated intra-abdominal infections. Eur J Clin Microbiol Infect Dis. 2019;38(5):819–827. doi:10.1007/s10096-019-03533-y
24. GlobalSurg C. Surgical site infection after gastrointestinal surgery in high-income, middle-income, and low-income countries: a prospective, international, multicentre cohort study. Lancet Infect Dis. 2018;18(5):516–525.
25. Wick EC, Hobson DB, Bennett JL, et al. Implementation of a surgical comprehensive unit-based safety program to reduce surgical site infections. J Am Coll Surg. 2012;215(2):193–200. doi:10.1016/j.jamcollsurg.2012.03.017
26. Li P, Han Y, Yang Y, et al. Retrospective review of laparoscopic versus open surgery in the treatment of appendiceal abscess in pediatric patients: laparoscopic versus open surgery for appendiceal abscess. Medicine. 2017;96(30):e7514. doi:10.1097/MD.0000000000007514
27. Li Y, Zhu WM, Gong JF, Guo Z, Cao L. The value of postoperative C-reactive protein in predictive diagnosis of postoperative intra-abdominal septic complications for patients with Crohn disease. Zhonghua Wai Ke Za Zhi. 2016;54(8):620–623. doi:10.3760/cma.j.issn.0529-5815.2016.08.014
28. Wang S, Xie Z, Shen Z. Serum procalcitonin and C-reactive protein in the evaluation of bacterial infection in generalized pustular psoriasis. An Bras Dermatol. 2019;94(5):542–548. doi:10.1016/j.abd.2019.09.022
29. Oberhofer D, Rumenjak V, Lazic J, Vucic N. Inflammatory indicators in patients after surgery of the large intestine. Acta Med Croatica. 2006;60(5):429–433.
30. Caluianu EI, Alexandru DO, Georgescu M, Mercut D, Trasca ET, Iancau M. Utilizing multiparameter scores and procalcitonin as prognosis markers for the degree of severity of acute pancreatitis. Curr Health Sci J. 2017;43(4):311–317. doi:10.12865/CHSJ.43.04.04
31. Umefune G, Kogure H, Hamada T, et al. Procalcitonin is a useful biomarker to predict severe acute cholangitis: a single-center prospective study. J Gastroenterol. 2017;52(6):734–745. doi:10.1007/s00535-016-1278-x
32. Dostert C, Grusdat M, Letellier E, Brenner D. The TNF family of ligands and receptors: communication modules in the immune system and beyond. Physiol Rev. 2019;99(1):115–160. doi:10.1152/physrev.00045.2017
33. Dulay AT, Buhimschi IA, Zhao G, et al. Compartmentalization of acute phase reactants interleukin-6, C-reactive protein and procalcitonin as biomarkers of intra-amniotic infection and chorioamnionitis. Cytokine. 2015;76(2):236–243. doi:10.1016/j.cyto.2015.04.014
34. Sawyer RG, Claridge JA, Nathens AB, et al. Trial of short-course antimicrobial therapy for intraabdominal infection. N Engl J Med. 2015;372(21):1996–2005. doi:10.1056/NEJMoa1411162
35. Chauhan N, Tiwari S, Jain U. Potential biomarkers for effective screening of neonatal sepsis infections: an overview. Microb Pathog. 2017;107:234–242. doi:10.1016/j.micpath.2017.03.042
36. Riedel S, Carroll KC. Laboratory detection of sepsis: biomarkers and molecular approaches. Clin Lab Med. 2013;33(3):413–437. doi:10.1016/j.cll.2013.03.006
37. Schietroma M, Rossi M, Fraioli F, et al. Inflammatory markers after laparoscopy versus laparotomy cholecystectomy. Ann Ital Chir. 2001;72:477–482.
38. Rettig TC, Verwijmeren L, Dijkstra IM, Boerma D, van de Garde EM, Noordzij PG. Postoperative interleukin-6 level and early detection of complications after elective major abdominal surgery. Ann Surg. 2016;263(6):1207–1212. doi:10.1097/SLA.0000000000001342
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.