Back to Journals » Clinical Ophthalmology » Volume 20
Comparison of Refractive Outcomes and Visual Quality Between Topography-Guided LASIK and Small Incision Lenticule Extraction: A 6-Month Prospective Study
Authors Wei S ![]() , Wang Y, Fu C, Zhang L, Hu Y, Dong Y, Ma D, Zhai C, Zheng Y
, Wang Y, Fu C, Zhang L, Hu Y, Dong Y, Ma D, Zhai C, Zheng Y
Received 10 February 2026
Accepted for publication 16 April 2026
Published 27 April 2026 Volume 2026:20 597116
DOI https://doi.org/10.2147/OPTH.S597116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
Shanshan Wei,* Yue Wang,* Caiyun Fu, Li Zhang, Yabin Hu, Yiran Dong, Dongyue Ma, Changbin Zhai, Yan Zheng
Beijing Institute of Ophthalmology, Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University, Beijing Ophthalmology & Visual Sciences Key Laboratory, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Changbin Zhai, Email [email protected] Yan Zheng, Email [email protected]
Purpose: To compare the postoperative refractive outcomes and visual quality between topography-guided laser in situ keratomileusis (TG-LASIK) and small incision lenticule extraction (SMILE) over a 6-month follow-up.
Patients and Methods: This study included 100 eyes of 50 patients, 50 eyes received TG-LASIK and 50 underwent SMILE. The outcomes measured included uncorrected distance visual acuity (UDVA), spherical equivalent (SEQ), cylinder, contrast sensitivity, and objective visual quality including objective scattering index (OSI), modulation transfer function (MTF) cutoff and Strehl Ratio (SR).
Results: Baseline characteristics differed between groups, with the SMILE group being younger and demonstrating better preoperative UDVA and lower cylinder. At 6 months, 98% of TG-LASIK eyes and 100% of SMILE eyes achieved UDVA of 0.0 logMAR or better, with no significant difference between groups (P = 0.315). A significantly higher percentage of eyes in the TG-LASIK group achieved SEQ within ± 0.25 D (58% vs 36%, P = 0.028) and ± 0.50 D (88% vs 64%, P = 0.01). Despite treating significantly higher preoperative astigmatism, TG-LASIK achieved comparable correction accuracy to SMILE. Objective visual quality was similar between groups at 3 and 6 months; SMILE showed higher MTF cutoff at 1 month (P = 0.027). TG-LASIK demonstrated significantly higher contrast sensitivity at 6.0 c/d (P < 0.001) and 18.0 c/d (P < 0.001) at 6 months.
Conclusion: Both TG-LASIK and SMILE are effective and safe for myopia and astigmatism correction. TG-LASIK demonstrated higher refractive precision and better contrast sensitivity at higher spatial frequencies compared to SMILE.
Plain Language Summary: Conventional FS-LASIK and SMILE have been widely compared in previous studies. However, TG-LASIK differs from both procedures by using individualized corneal topography to guide customized ablation and is often applied in eyes with higher astigmatism or greater refractive complexity in routine practice.
Whether this customized approach provides meaningful clinical advantages over SMILE under real-world conditions remains unclear.
Both TG-LASIK and SMILE provided comparable visual acuity outcomes at 6 months after surgery. TG-LASIK achieved higher refractive precision, with a greater proportion of eyes reaching the intended spherical equivalent target. Although objective visual quality parameters were largely similar between the two groups, TG-LASIK was associated with better contrast sensitivity at higher spatial frequencies.
Keywords: topography-guided LASIK, small incision lenticule extraction, Myopia, astigmatism, contrast sensitivity, visual quality
Introduction
Over the past few decades, small incision lenticule extraction (SMILE) and femtosecond laser in situ keratomileusis (FS-LASIK) have both emerged as effective and safe procedures for the correction of refractive errors such as myopia and astigmatism.1–3 SMILE is a flapless, minimally invasive procedure that creates a lenticule within the corneal stroma, which is then removed through a small incision. FS-LASIK, one of the most widely performed refractive surgeries, uses a femtosecond laser to create a corneal flap, followed by reshaping of the cornea with excimer laser ablation.4–7
Topography-guided LASIK (TG-LASIK) is a more recent advancement in refractive surgery, utilizing detailed corneal topographic data to customize the ablation pattern. It stands out by utilizing topographical data to direct laser reshaping of the cornea. Its principle relies on the corneal shape, as optical quality is closely linked to corneal topography. This method offers the advantage of reducing the induction of higher-order aberrations (HOAs) and improving contrast sensitivity, particularly in patients with irregular corneas or pre-existing aberrations.8–11 TG-LASIK has demonstrated consistent and stable visual outcomes, making it a valuable option for personalized refractive surgery.12 Large-scale studies, such as that by Wallerstein et al involving more than 25,000 TG-LASIK eyes, have further confirmed the safety, accuracy, and refractive predictability of this platform across a wide range of myopic and astigmatic corrections.13
While previous studies have compared TG-LASIK and SMILE,2,3,14–17 most of these have focused primarily on visual acuity and refractive outcomes, with limited attention to objective optical quality measures. Contrast sensitivity, which reflects functional vision more closely than visual acuity alone, has also been inconsistently reported across studies and rarely evaluated across multiple spatial frequencies over time. Therefore, a comparative study incorporating both objective visual quality and contrast sensitivity, conducted in a Chinese population, may provide additional clinical insights. The present study aimed to compare the efficacy and safety of TG-LASIK and SMILE, including refractive outcomes, objective visual quality, and contrast sensitivity between TG-LASIK and SMILE over a 6-month follow-up period.
Materials and Methods
Subjects
This prospective, observational study was carried out at Beijing Tongren Hospital from June 2021 to May 2022. A total of 50 patients (100 eyes) were enrolled, including 25 patients (50 eyes) in the TG-LASIK group and 25 patients (50 eyes) in the SMILE group. Both eyes of each patient were included when eligible. The inclusion criteria were as follows: (1) patients aged 18 to 40 years with surgical expectations to be glasses-free; (2) spherical refractions ranging from −0.75 to −10.00 diopters (D), with or without cylinder up to −4.0D; (3) stable refraction for more than 1 year; (4) corrected distance visual acuity (CDVA) of both eyes reaching a 0.1 logarithm of the minimum angle of resolution (logMAR); (5) cessation of wearing soft contact lenses for 1 week or rigid contact lenses for 3 weeks. Exclusion criteria included (1) a residual stromal bed less than 280μm; (2) suspicion of keratoconus on corneal topography; (3) previous ocular surgery or history of herpes viral infection, uncontrolled diabetic mellitus, systemic immune diseases, pregnancy or under lactation.
The study adhered to the tenets of the Declaration of Helsinki and was approved by the Medical Ethics Committee of Beijing Tongren Hospital, Capital Medical University (No. TERC2024-KY166). A written informed consent was obtained from each patient prior to the surgical procedure.
The primary endpoint of this study was refractive outcomes at 6 months postoperatively, including uncorrected distance visual acuity (UDVA) and spherical equivalent (SEQ). Secondary endpoints included astigmatic correction accuracy assessed by vector analysis, objective visual quality, and contrast sensitivity across five spatial frequencies at each follow-up visit. Objective visual quality was measured by Optical Quality Analysis System (OQAS, Visiometrics, Terrassa, Spain) and included the objective scattering index (OSI), modulation transfer function (MTF) cutoff, and Strehl ratio (SR).
Preoperative Assessment and Surgical Technique
All patients underwent preoperative assessment including UDVA, CDVA and manifest refraction, the slit-lamp bio-microscopy, funduscopic examinations, the Topographic Modeling System (TMS-4, Tomey Corporation, Nagoya, Aichi, Japan), a reference biometer (Lenstar LS 900, HAAG-STREIT AG, Switzerland) and corneal topography (VARIO Topolyzer, WaveLight, Alcon Laboratories, Inc., Fort Worth, TX, United States). The surgery was performed by the same experienced surgeon to ensure consistency. TG-LASIK was performed using the WaveLight FS200 femtosecond laser (Alcon Vision, LLC, Fort Worth, TX, USA) to create the corneal flap (thickness 110 μm, diameter 8.5 mm, side-cut angle 90°, hinge angle 50°). The Wavelight EX500 excimer (Alcon Vision, LLC, Fort Worth, TX, USA) was used for ablation with an optical zone of 6–6.5mm.
Corneal topography data were acquired with the Topolyzer VARIO system; a minimum of 8 high-quality scans were captured, and only scans meeting manufacturer quality standards (no missing data, consistent axis alignment, and minimal eyelid interference) were accepted. Ablation planning followed the Topography-Modified Refraction (TMR) protocol, which integrates manifest refraction with topography-measured astigmatism and axis to optimize alignment. Iris registration and cyclotorsion compensation were applied to ensure accurate ablation.
SMILE was performed using the VisuMax femtosecond laser system (Carl Zeiss Meditec, Oberkochen, Germany). A stromal lenticule was created with a cap thickness of 110 μm and a cap diameter of 7.0–7.5 mm. The lenticule diameter ranged from 6.0 to 6.5 mm. The laser spot and track spacing were both set to 4.5 μm, and a 2.0 mm side incision was placed at the 120° meridian for lenticule extraction.
Postoperative Care and Follow-up
Postoperative care was identical for both groups. All patients were treated with topical 0.3% levofloxacin four times daily for 2 weeks. Topical 0.1% fluorometholone was prescribed with a tapering regimen from four times daily to once daily over 30 days. In addition, 0.3% sodium hyaluronate was administered four times daily for 3 months.
Follow-up visits were scheduled at 1 day, 1 week, 1 month, 3 months, and 6 months postoperatively. During each visit, patients underwent UDVA, manifest refraction, slit-lamp examination. Contrast sensitivity and objective visual quality were assessed at 1, 3, and 6 months postoperatively. Contrast sensitivity was measured using the Functional Vision Analyzer (Vision Tester, Stereo Optical Company Inc., Chicago, IL, United States) under mesopic conditions at a calibrated target luminance of 3.0 cd/m2, with undilated pupils. The spatial frequencies of the stimuli were 1.5, 3.0, 6.0, 12.0, and 18.0 cycles per degree (c/d). Objective visual quality was measured by OQAS, a double-pass retinal imaging instrument that quantifies intraocular scattering and optical quality. Measurements were performed under undilated pupils. Three consecutive readings were obtained for each eye, and the mean value was used for analysis. All measurements were performed by the same experienced examiner. The MTF cutoff reflects the resolving capacity of the optical system, with higher values indicating better optical quality. The SR represents optical performance relative to an ideal system, ranging from 0 to 1, with higher values indicating better optical quality. The OSI quantifies intraocular light scatter, with lower values indicating better optical quality. Values below approximately 2.0 are generally considered within the normal range, higher values indicate increased scattering, which may be associated with corneal haze, interface irregularity, or early lens changes, and correlates with symptoms such as glare and reduced contrast sensitivity. These parameters provide complementary, instrument-based assessments of retinal image quality that are independent of subjective patient responses.
Statistical Analysis
Visual acuity values assessed were converted to the logarithm of the minimum angle of resolution (logMAR). The Shapiro–Wilk test was used for confirming normality of data. Comparisons of normally distributed variables were performed using the paired t-test, whereas the Wilcoxon signed-rank test was applied for variables without a normal distribution. To analyze intragroup differences during the follow-up period, repeated measures ANOVA was applied for the normally distributed data and the Friedman test was employed on the non-normally distributed data. The intergroup comparison of categorical variables was conducted using the chi-squared test. Vector analysis of astigmatism was performed according to the Alpins method, calculating Target Induced Astigmatism (TIA), Surgically Induced Astigmatism (SIA), Difference Vector (DV), Correction Index (CI = SIA/TIA), Index of Success (IOS = DV/TIA) and Angle of Error (AE).18,19 Data analysis was conducted using SPSS 23.0 (IBM Corp., Armonk, NY, USA) and graphs were generated using GraphPad Prism 9.4.0 (GraphPad Software, San Diego, CA, USA). A P value < 0.05 was considered statistically significant. When multiple comparisons were performed, a Bonferroni-adjusted significance level of α = 0.01 was applied.
Results
Baseline Patient Data
The study enrolled 50 patients (100 eyes), comprising 25 patients (50 eyes) in the TG-LASIK group and 25 patients (50 eyes) in the SMILE group. Baseline characteristics are summarized in Table 1.
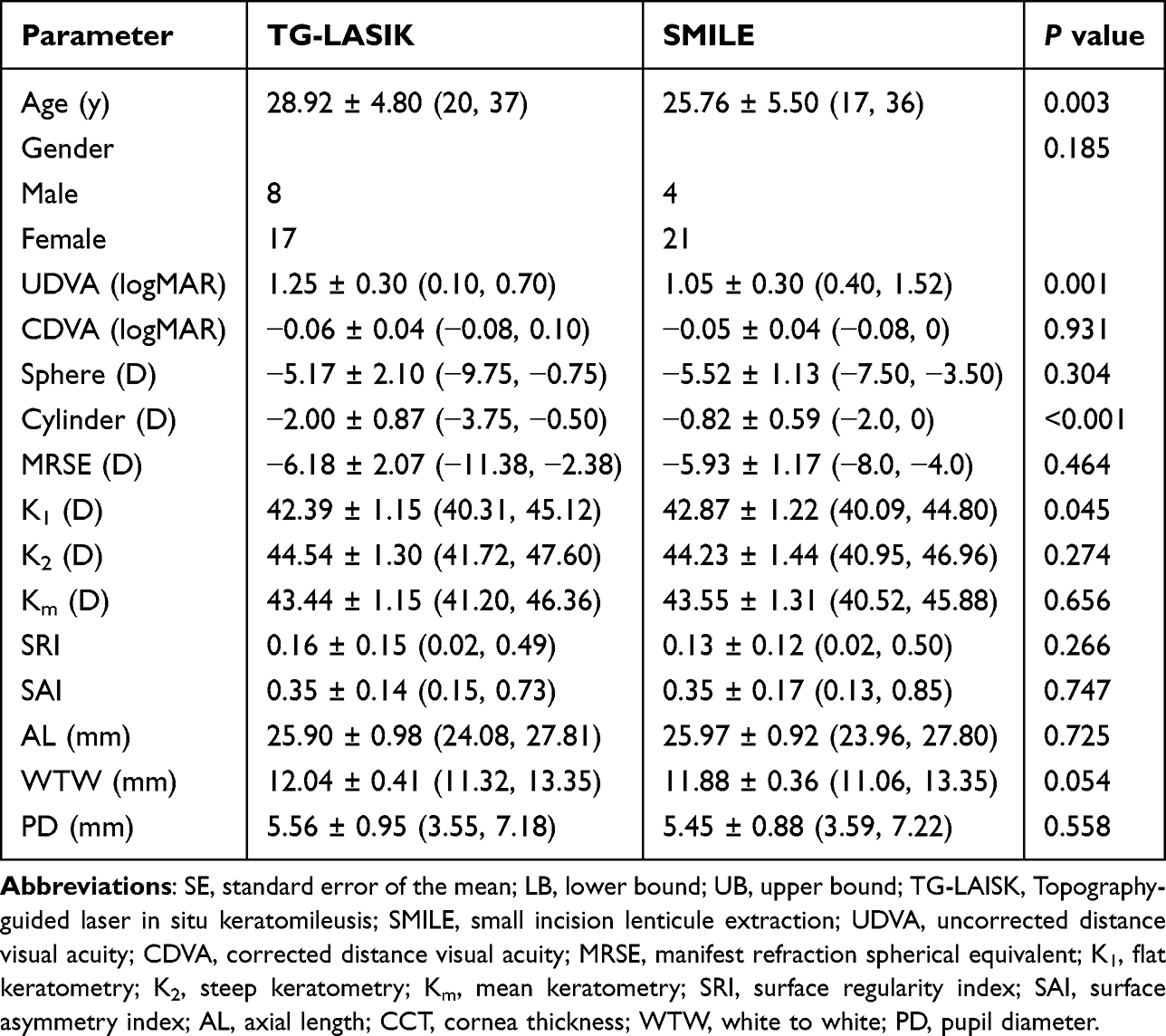 |
Table 1 Baseline Clinical Data in the Two Groups Mean ± SD (LB, UB) |
The mean age was significantly higher in the TG-LASIK group compared to the SMILE group (P = 0.003). There were no significant differences in gender distribution between the two groups. The SMILE group demonstrated better preoperative UDVA (P = 0.001). Importantly, the preoperative cylinder was significantly higher in the TG-LASIK group than in the SMILE group (P < 0.001).
Visual and Refractive Outcomes
Figures 1 and 2 collectively summarize postoperative refractive outcomes using standardized refractive surgery outcome graphs that demonstrate surgical efficacy, safety, predictability, stability, and astigmatic correction at 6 months postoperatively.
 |
Figure 1 Standard refractive surgery outcome graphs for TG-LASIK at 6 months postoperatively (A) Cumulative uncorrected distance visual acuity (UDVA) (Snellen 20/x or better). (B) Difference between uncorrected and corrected distance visual acuity (UDVA vs CDVA). (C) Attempted versus achieved spherical equivalent refraction (SEQ). (D) Distribution of postoperative SEQ (refractive accuracy). (E) Distribution of refractive astigmatism (D). (F) Stability of SEQ over time. (G) Correlation between target-induced astigmatism (TIA) and surgically induced astigmatism (SIA). (H) Scatter plot of magnitude of error. (I) Histogram of astigmatism angle of error. |
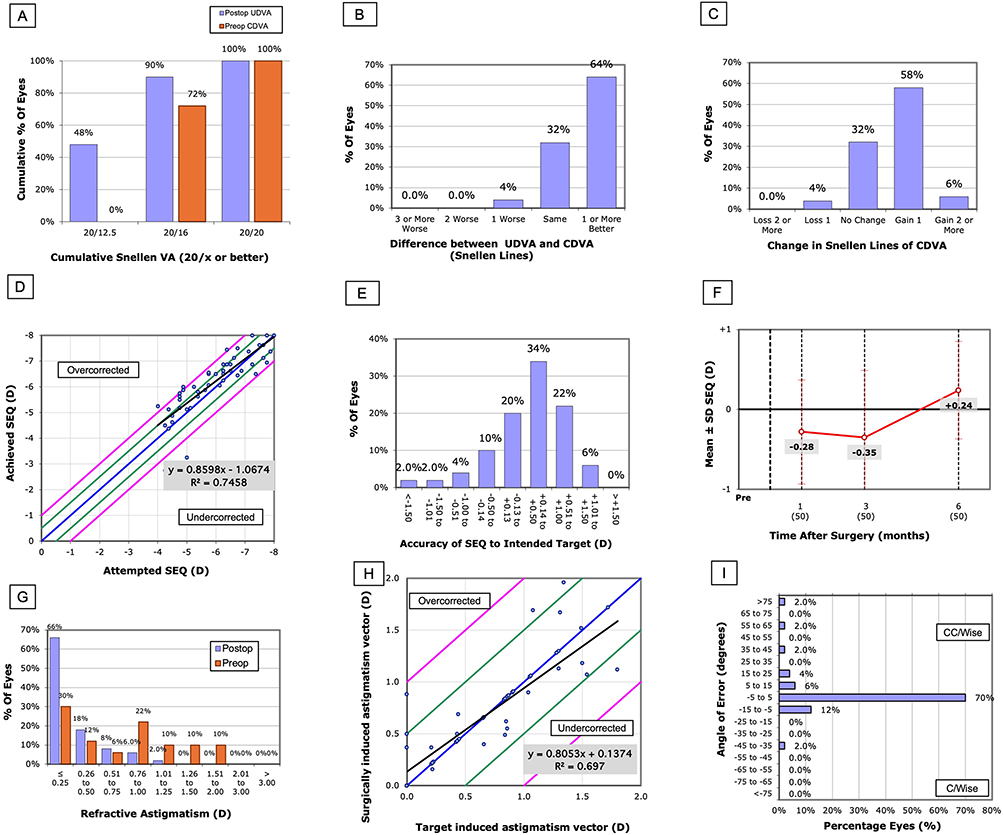 |
Figure 2 Standard refractive surgery outcome graphs for SMILE at 6 months postoperatively (A) Cumulative uncorrected distance visual acuity (UDVA) (Snellen 20/x or better). (B) Difference between uncorrected and corrected distance visual acuity (UDVA vs CDVA). (C) Attempted versus achieved spherical equivalent refraction (SEQ). (D) Distribution of postoperative SEQ (refractive accuracy). (E) Distribution of refractive astigmatism (D). (F) Stability of SEQ over time. (G) Correlation between target-induced astigmatism (TIA) and surgically induced astigmatism (SIA). (H) Scatter plot of magnitude of error. (I) Histogram of astigmatism angle of error. Visual acuity is presented in Snellen notation, with statistical analyses using logMAR values. |
UDVA and CDVA: Both groups achieved excellent postoperative UDVA. At 6 months, 98% of TG-LASIK eyes and 100% of SMILE eyes achieved UDVA of 0.0 logMAR or better, with no significant difference between groups (P = 0.315). 88% of TG-LASIK and 96% of SMILE eyes saw the same number of lines or better of UDVA compared to preoperative CDVA. (Figures 1A, B and 2A, B). 2% of eyes in the TG-LASIK group and no eyes in the SMILE group lost two or more lines of CDVA (Figures 1C and 2C).
SEQ: Linear regression analysis of attempted versus achieved SEQ showed slops of 1.06x + 0.55 D (R2 = 0.97) for TG-LASIK and 0.86x - 1.07 D (R2 = 0.75) for SMILE (Figures 1D and 2D).TG-LASIK demonstrated superior refractive precision, with significantly more eyes achieving SEQ within ±0.50 D (88% vs 64%, P = 0.01) at 6 months (Figure 1E and 2E). Both groups showed significant changes in SEQ over time (TG-LASIK: P = 0.001; SMILE: P < 0.001). At 1 month, the TG-LASIK group had a mean SEQ of 0.02 ± 0.43 D, while the SMILE group showed −0.28 ± 0.65 D (P = 0.007). At 6 months, TG-LASIK maintained stable refraction at −0.15 ± 0.41 D, while SMILE demonstrated a hyperopic shift to +0.24 ± 0.61 D (P < 0.001; Figures 1F and 2F).
Astigmatism Correction: At 1, 3, and 6 months postoperatively, both groups showed significant improvement in cylinder compared to baseline (TG-LASIK: P = 0.003; SMILE: P = 0.024). At 6 months, 72% of TG-LASIK eyes and 84% of SMILE eyes achieved residual cylinder ≤0.50 D, with no significant difference between groups (P = 0.148; Figures 1G and 2G). There were no significant differences when comparing the two groups at each follow-up point. Linear regression analysis of TIA showed a mean regression value of 1.04x - 0.04 D (R2 = 0.85) for TG-LASIK and 0.81x + 0.14 D (R2 = 0.697) for SMILE (Figures 1H and 2H). The mean DV was 0.04 D × 40° in the TG-LASIK group and 0.09 D × 16° in the SMILE group. Vector analysis showed comparable correction accuracy between groups, with CI values close to 1.0 (1.03 vs 0.97, P = 0.361) (Figures 3 and 4). IOS was numerically lower in TG-LASIK (0.22 compared to 0.32, P = 0.248), as was AE (1.11° compared to 3.37°, P = 0.433, Figures 1I and 2I).
 |
Figure 3 Vector analysis for TG-LASIK at 6 months postoperatively. |
 |
Figure 4 Vector analysis for SMILE at 6 months postoperatively. |
Objective Visual Quality
As shown in Table 2, OSI showed no difference within or between the TG-LASIK and SMILE group at 1, 3, 6 months after the surgery. OSI remained stable in both groups. For MTF cutoff, SMILE demonstrated significantly higher values than TG-LASIK at 1 month (P = 0.027), but this difference was not present at 3 or 6 months, with both groups showing stable values throughout follow-up. SR showed no significant between-group difference at any time point. Within both groups, SR remained stable over the 6-month period.
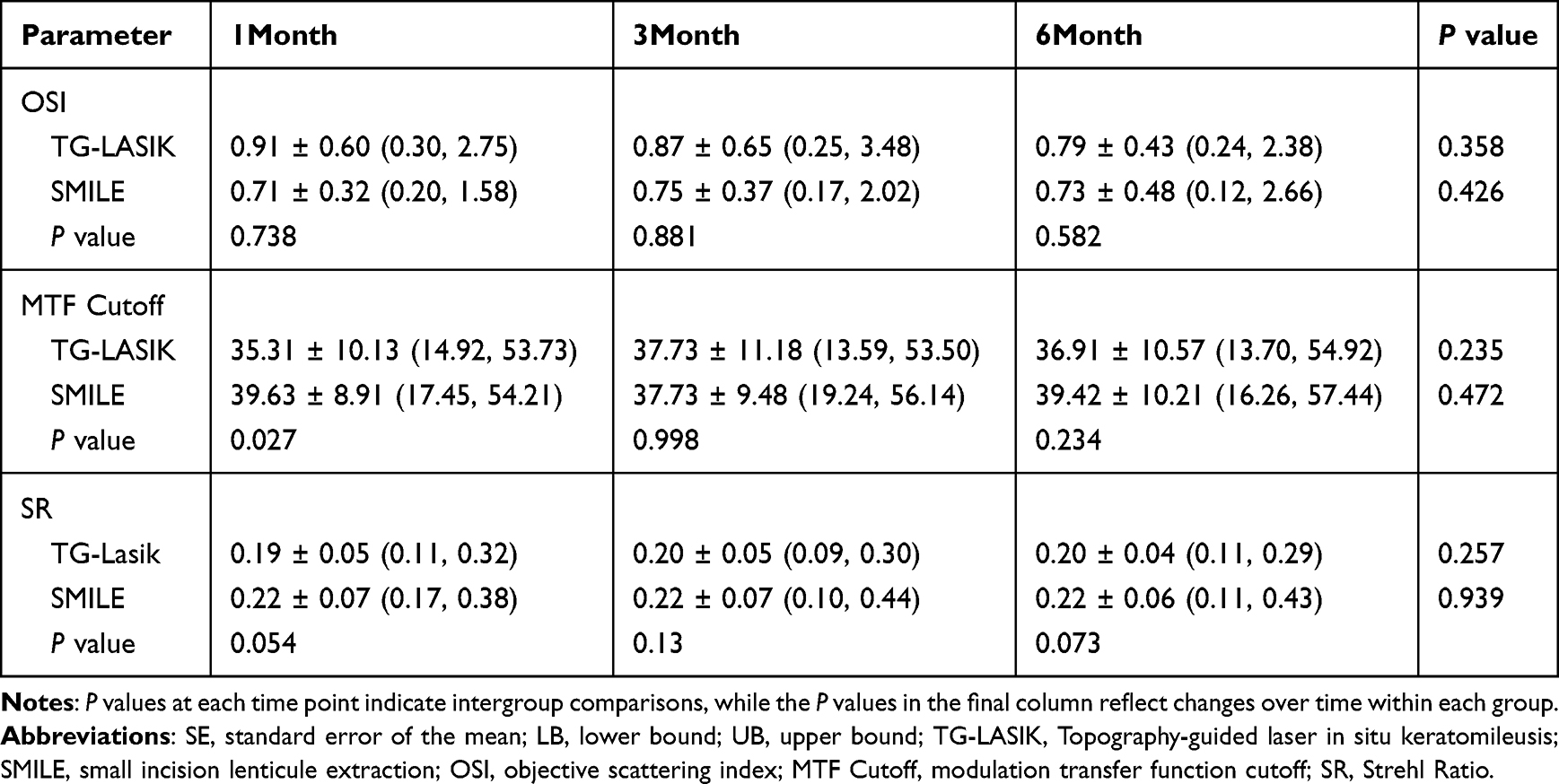 |
Table 2 Postoperative Objective Visual Quality Mean ± SD (LB, UB) |
Contrast Sensitivity
At the lower spatial frequency of 1.5 c/d (Figure 5A), the TG-LASIK group showed lower contrast sensitivity at baseline compared to the SMILE group. However, contrast sensitivity improved over time in the TG-LASIK group, and no significant differences were observed between the two groups at postoperative time points.
 |
Figure 5 The Log values of contrast sensitivity at different frequencies (A) 1.5 c/d; (B) 3.0 c/d; (C) 6.0 c/d; (D) 12.0 c/d; (E) 18.0 c/d. *P < 0.01 indicates statistical significance. |
For 3.0 c/d (Figure 5B) and 12.0 c/d (Figure 5D), both groups exhibited an increase in contrast sensitivity postoperatively. The contrast sensitivity was similar between the TG-LASIK and SMILE groups across all time points, with no statistically significant differences observed.
At 6.0 c/d (Figure 5C), a significant difference between the two groups was observed at the 6 months after the surgery (P < 0.001). TG-LASIK significantly improved from baseline by the 6-month postoperative period. The SMILE group also showed a slight increase in contrast sensitivity.
At the highest spatial frequency at 18.0 c/d (Figure 5E), the TG-LASIK group exhibited a gradual improvement in contrast sensitivity over time. The SMILE group, however, showed more variable results, with an initial improvement at 1 month followed by a slight decrease by 6 months. At 6 months after surgery, TG-LASIK and SMILE showed a significant difference in contrast sensitivity at the spatial frequency of 18 c/d (TG-LASIK: 0.81 ± 0.48, SMILE: 0.33 ± 0.27, P < 0.001). No significant differences were found at 1.5, 3.0, or 12.0 c/d at any follow-up time point. Detailed contrast sensitivity values at each spatial frequency and time point are provided in Table 3.
 |
Table 3 Postoperative Contrast Sensitivity Mean ± SD (LB, UB) |
Discussion
This study aimed to evaluate the outcomes of TG-LASIK and SMILE surgeries in terms of visual acuity and refractive results over a 6-month postoperative period, comparing the efficacy, safety, and stability of both procedures.
It is demonstrated that both the TG-LASIK and SMILE groups achieved satisfactory visual outcomes at 6 months, with no significant differences in UDVA, which is consistent with the finding of previous studies.3,14–16,20,21 Zhang et al found that there were no significant differences in UDVA between the TG-LASIK and SMILE eyes and postoperative SEQ was similar between the groups at the 6-month follow-up3 Similarly, Sitto et al similarly reported comparable UDVA between TG-LASIK and SMILE at 12 months in a prospective contralateral-eye design.14 Our results align with this in terms of UDVA, where both groups in our study achieved similar percentages of eyes with UDVA better than or equal to −0.1 logMAR and 0.0 logMAR.3 These findings suggest that both TG-LASIK and SMILE provide satisfactory visual acuity outcomes at 6 months.
Regarding refractive outcomes, our study found that a significantly higher percentage of eyes in the TG-LASIK group achieved an SEQ within 0.25 D and 0.50 D compared to the SMILE group. The findings match those observed in Hidenaga Kobashi’s study. In his study, 95.5% of the LASIK group achieved SEQ within ±0.50 D, compared to 77.3% of the SMILE group (P < 0.05).20 Our results also demonstrated a similar trend, with 88% of TG-LASIK eyes achieving SEQ within ±0.50 D, compared to 64% in the SMILE group, suggesting the greater refractive precision of TG-LASIK.
In terms of astigmatism correction, our study found no significant differences between TG-LASIK and SMILE in the percentage of eyes achieving cylinder ≤0.25 D or ≤0.50 D postoperatively. Vector analysis revealed that the TG-LASIK group treated significantly higher preoperative astigmatism, reflecting the clinical practice of using TG-LASIK for moderate to high astigmatism. Despite the baseline difference, both groups demonstrated comparable correction accuracy, with CI values close to 1.0 and low DV. The TG-LASIK showed numerically lower IOS and AE, suggesting a trend toward improved precision in astigmatism correction and axis alignment. Sitto et al also noted residual astigmatism as a limitation in their SMILE group, attributing it partly to the absence of automated cyclotorsion compensation.14 This may partly explain the comparable correction accuracy observed between the two groups despite the higher preoperative astigmatism in the TG-LASIK group.
No significant differences in OSI and MTF Cutoff between TG-LASIK and SMILE group suggests that both surgeries provide comparable objective visual quality. The significant differences in MTF cutoff at 1 month indicate that SMILE may initially provide slightly better optical performance compared to TG-LASIK. However, this difference was no longer present at 3 and 6 months, indicating comparable optical quality between the two procedures at longer follow-up. This is partially consistent with previous findings showing that MTF cutoff is higher after SMILE than FS-LASIK in the early postoperative period.22 The convergence of outcomes by 3 months in our study may be attributed to the individualized topography-guided ablation profile of TG-LASIK, which optimizes corneal optical quality and may offset the early advantage in the SMILE group. A recent prospective contralateral study reported better subjective visual quality in the TG-LASIK group compared to SMILE.23 These findings may indicate a potential advantage of TG-LASIK in visual quality–related outcomes. However, these results were primarily based on subjective assessments, highlighting the need for further validation using objective optical quality parameters.
Regarding contrast sensitivity, our results showed improvement in both groups, with TG-LASIK achieving significantly higher values at 6.0 c/d and 18.0 c/d at 6 months (P < 0.001). This pattern is consistent with findings from two prior studies using different measurement approaches.14,15 Kanellopoulos reported numerically higher contrast sensitivity at 6 c/d in the TG-LASIK group compared to SMILE at 3 months (7.2 ± 1.01 vs 6.20 ± 1.52), though between-group statistical comparisons were not reported. Similarly, Sitto et al demonstrated that TG-LASIK showed better mesopic low-contrast visual acuity than SMILE at 1 month. This advantage may reflect the role of active centration, iris registration, and cyclotorsion compensation in TG-LASIK, which reduce induced HOAs and preserve corneal optical regularity which known to influence contrast sensitivity, particularly at higher spatial frequencies. Similarly, Jain et al found that TG-LASIK was associated with better contrast sensitivity and reduced higher-order aberrations (HOAs) This improvement in contrast sensitivity aligns with recent literature reporting enhanced outcomes following personalized LASIK techniques, supporting the notion that TG-LASIK may provide improved contrast sensitivity, particularly at higher spatial frequencies.21,24,25
Regarding safety, no eyes in the SMILE group lost two or more lines of CDVA. In the TG-LASIK group, 2% of eyes (1 eye) experienced a loss of two or more lines of CDVA. However, this was an isolated finding and did not reach statistical significance between groups. For TG-LASIK, flap-related complications such as epithelial ingrowth, flap striae, and diffuse lamellar keratitis (DLK) have been well described, although their incidence has declined substantially with modern femtosecond laser technology; no such complications were observed in our study. For SMILE, suction loss during lenticule creation and difficult lenticule dissection may affect early visual recovery and none were observed in our study. Given the 6-month follow-up, these long-term outcomes require further evaluation. Our findings suggest that TG-LASIK may be preferred in patients requiring more precise astigmatism correction or those with higher visual quality demands, given its better performance in contrast sensitivity at higher spatial frequencies.
The limitations of the present study are as follows. First, the non-randomized design may introduce potential selection bias. Second, the baseline difference existed between groups, including age, UDVA and cylinder and they may act as potential confounding factors; although covariate adjustment was not performed for all primary analyses, the comparable CDVA at baseline suggests equivalent optical potential between groups. In addition, the 6-months follow-up and limited sample size may reduce the ability to assess long-term stability and detect modest differences between groups. Furthermore, the predominance of female participants may limit the generalizability of the findings. Finally, the absence of preoperative OQAS measurements precluded within-group analysis of changes in objective optical quality from baseline, thereby limiting the ability to assess postoperative improvements.
Conclusion
In conclusion, both TG-LASIK and SMILE are highly effective in treating myopia and myopic astigmatism. The objective visual quality parameters were comparable between the two methods, suggesting that both can offer similar visual quality. However, TG-LASIK exhibited superior refractive precision and may enhance contrast sensitivity compared to SMILE, especially at higher spatial frequencies. Future research with larger sample sizes, longer follow-up periods, and more comprehensive measures of visual quality is needed to confirm these findings.
Abbreviations
TG-LASIK, Topography-guided laser in situ keratomileusis; SMILE, small incision lenticule extraction; UDVA, uncorrected distance visual acuity; SEQ, spherical equivalent; OSI, objective scattering index; MTF, modulation transfer function; SR, Strehl Ratio; HOAs, higher-order aberrations; CDVA, corrected distance visual acuity; logMAR, logarithm of the minimum angle of resolution; TIA, target induced astigmatism; SIA, surgically induced astigmatism; DV, difference vector; CI, correction index; IOS, index of success; AE, Angle of Error.
Data Sharing Statement
The datasets used in the study are available from the corresponding author, Yan Zheng, upon reasonable request due to privacy regulations.
Ethics Approval
This study was conducted following the ethical standards in the Declaration of Helsinki and the study received ethics approval from the Beijing Tongren Hospital Medical Ethics Committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding for this study, came from the following: 1) National Key Research and Development Program of China (Grant No. 2022YFC2404505); 2) Wu Jieping Medical Foundation (Grant No. 320.6750).
Disclosure
Shanshan Wei and Yue Wang are co-first authors for this study. All authors declare that they have no conflicts of interest in this work.
References
1. Sekundo W, Kunert K, Russmann C, et al. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia: six-month results. J Cataract Refract Surg. 2008;34(9):1513–13. doi:10.1016/j.jcrs.2008.05.033
2. Schallhorn JM, Seifert S, Schallhorn SC. SMILE, topography-guided LASIK, and wavefront-guided LASIK: review of clinical outcomes in premarket approval FDA studies. J Refract Surg. 2019;35(11):690–698. doi:10.3928/1081597x-20190930-02
3. Zhang Y, Sun X, Chen Y. Comparison of corneal optical quality After SMILE, wavefront-optimized LASIK and topography-guided LASIK for Myopia and Myopic astigmatism. Front Med. 2022;9:870330. doi:10.3389/fmed.2022.870330
4. Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011;95(3):335–339. doi:10.1136/bjo.2009.174284
5. Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: all-in-one femtosecond laser refractive surgery. J Cataract Refract Surg. 2011;37(1):127–137. doi:10.1016/j.jcrs.2010.07.033
6. Řeháková T, Veliká V, Jirásková N. Correction of myopia and myopic astigmatism by femtosecond laser in situ keratomileusis. Ceska a Slovenska Oftalmologi. 2019;75(2):65–71. doi:10.31348/2019/2/2
7. Solomon KD, Fernández de Castro LE, Sandoval HP, et al. LASIK world literature review: quality of life and patient satisfaction. Ophthalmology. 2009;116(4):691–701. doi:10.1016/j.ophtha.2008.12.037
8. Saleh S, Epp LJ, Tran EMT, Manche EE. 12-month visual and refractive outcomes of topography-guided femtosecond laser–assisted LASIK for Myopia and Myopic astigmatism. J Refract Surg. 2024;40(9):e595–e603. doi:10.3928/1081597x-20240717-01
9. Tan J, Simon D, Mrochen M, Por YM. Clinical results of topography-based customized ablations for myopia and myopic astigmatism. J Refract Surg. 2012;28(11):S829–836. doi:10.3928/1081597x-20121005-04
10. Stulting DR, Fant BS, Bond W, et al. Results of topography-guided laser in situ keratomileusis custom ablation treatment with a refractive excimer laser. J Cataract Refract Surg. 2016;42(1):11–18. doi:10.1016/j.jcrs.2015.08.016
11. Ipek ŞC, Utine CA. Topography-guided excimer laser ablation in refractive surgery. Front Ophthalmol. 2024;4:1367258. doi:10.3389/fopht.2024.1367258
12. Moshirfar M, Somani AN, Motlagh MN, et al. Comparison of FDA-reported visual and refractive outcomes of the toric ICL lens, SMILE, and topography-guided LASIK for the correction of Myopia and Myopic astigmatism. J Refract Surg. 2019;35(11):699–706. doi:10.3928/1081597x-20190930-01
13. Wallerstein A, Gauvin M, Ruyu Qi S, Cohen M. Large axis difference between topographic anterior corneal astigmatism and manifest refractive astigmatism: can topography-guided LASIK target the manifest axis? J Refract Surg. 2021;37(10):662–673. doi:10.3928/1081597x-20210712-05
14. Sitto MM, Manion GN, Moin KA, Linn SH, Hoopes PC, Moshirfar M. One-year prospective contralateral eye study: visual outcomes of topography-guided LASIK versus KLEx for Myopia and Myopic astigmatism. J Refract Surg. 2025;41(11):e1168–e1179. doi:10.3928/1081597x-20250821-02
15. Kanellopoulos AJ. Topography-guided LASIK versus small incision lenticule extraction (SMILE) for Myopia and Myopic astigmatism: a randomized, prospective, contralateral eye study. J Refract Surg. 2017;33(5):306–312. doi:10.3928/1081597x-20170221-01
16. Yang LJ, Mi S-J, Sun L, Chen M-X. Early visual function outcomes of topography-guided FS-LASIK and SMILE in treatment of myopia and myopic astigmatism. Int J Ophthalmol. 2021;14(3):423–429. doi:10.18240/ijo.2021.03.15
17. Moin KA, Manion GN, Pandiri S, Hoopes PC, Moshirfar M. Three-month comprehensive outcomes of topography-guided LASIK versus keratorefractive lenticule extraction (KLEx): a prospective contralateral study. Ophthalmol Therapy. 2024;13(8):2265–2284. doi:10.1007/s40123-024-00987-y
18. Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg. 1993;19(4):524–533. doi:10.1016/s0886-3350(13)80617-7
19. Alpins N. Astigmatism analysis by the Alpins method. J Cataract Refract Surg. 2001;27(1):31–49. doi:10.1016/s0886-3350(00)00798-7
20. Kobashi H, Kamiya K, Igarashi A, Takahashi M, Shimizu K. Two-years results of small-incision lenticule extraction and wavefront-guided laser in situ keratomileusis for Myopia. Acta Ophthalmol. 2018;96(2):e119–e126. doi:10.1111/aos.13470
21. Zhao X, Zhang L, Ma J, et al. Comparison of wavefront-guided femtosecond LASIK and optimized SMILE for correction of moderate-to-high astigmatism. J Refract Surg. 2021;37(3):166–173. doi:10.3928/1081597x-20201230-01
22. Yin Y, Lu Y, Xiang A, et al. Comparison of the optical quality after SMILE and FS-LASIK for high myopia by OQAS and iTrace analyzer: a one-year retrospective study. BMC Ophthalmol. 2021;21(1):292. doi:10.1186/s12886-021-02048-5
23. Annis TD, Evangelista CB, Rodgers SB, Bui QVV, Kohler PD, Capó-Aponte JE. Comparison of clinical outcomes of contralateral topography-guided laser in situ keratomileusis versus keratorefractive lenticule extraction: a prospective study. J Refract Surg. 2026;42(1):e18–e30. doi:10.3928/1081597x-20251124-02
24. Heralgi MM, Kavitha V, Dwivedi M, et al. Study of change in contrast sensitivity in relation to depth of ablation after wavefront optimized myopic laser-assisted in situ keratomileusis. Indian J Ophthalmol. 2020;68(12):2975–2980. doi:10.4103/ijo.IJO_1399_20
25. Yue P, Wang X, Wang Z, et al. The effect of femtosecond laser-assisted in situ keratomileusis on contrast sensitivity. Front Neurosci. 2024;18:1326572. doi:10.3389/fnins.2024.1326572
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of the EVO/EVO+ Sphere and Toric Visian ICL: Six Month Results from the United States Food and Drug Administration Clinical Trial
Packer M
Clinical Ophthalmology 2022, 16:1541-1553
Published Date: 21 May 2022
Photorefractive Keratectomy Enhancement (PRK) After Small-Incision Lenticule Extraction (SMILE)
Moshirfar M, Parsons MT, Chartrand NA, Lau CK, Stapley S, Bundogji N, Ronquillo YC, Hoopes PC
Clinical Ophthalmology 2022, 16:3033-3042
Published Date: 12 September 2022
Prospective, Randomized, Fellow Eye-Controlled Study of Postoperative Pain and Inflammation Control with an Intracanalicular Dexamethasone 0.4 mg Ophthalmic Insert Following Small Incision Lenticule Extraction
Jee KJ, Ling J, Bafna S, Chester T, Augustine J, Wiley WF
Clinical Ophthalmology 2022, 16:3895-3904
Published Date: 22 November 2022
A Comprehensive Retrospective Analysis of EVO/EVO+ Implantable Collamer Lens: Evaluating Refractive Outcomes in the Largest Single Center Study of ICL Patients in the United States
Albo C, Nasser T, Szynkarski DT, Nguyen N, Mueller B, Libfraind L, Parkhurst G
Clinical Ophthalmology 2024, 18:69-78
Published Date: 9 January 2024
Three-Month Outcomes of SMILE Pro with the VISUMAX 800 for Myopic Astigmatism in a Large Population
Cung HS, Tran LHT, Tran TN
Clinical Ophthalmology 2025, 19:417-425
Published Date: 7 February 2025