Back to Journals » Risk Management and Healthcare Policy » Volume 16
Perceived Relationship Between Horizontal Violence and Patient Safety Culture Among Nurses
Authors Jaber HJ, Abu Shosha GM, Al-Kalaldeh MT, Oweidat IA, Al-Mugheed K ![]() , Alsenany SA, Farghaly Abdelaliem SM
, Alsenany SA, Farghaly Abdelaliem SM ![]()
Received 29 April 2023
Accepted for publication 4 August 2023
Published 14 August 2023 Volume 2023:16 Pages 1545—1553
DOI https://doi.org/10.2147/RMHP.S419309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Huda Jalal Jaber,1 Ghada Mohammad Abu Shosha,1 Mahmoud Taher Al-Kalaldeh,2 Islam Ali Oweidat,1 Khalid Al-Mugheed,3 Samira Ahmed Alsenany,4 Sally Mohammed Farghaly Abdelaliem5
1Faculty of Nursing, Zarqa University, Zarqa, Jordan; 2Faculty of Nursing, the University of Jordan, Aqaba, Jordan; 3Faculty of Nursing, Riyadh Elm University, Riyadh, Saudi Arabia; 4Department of Community Health Nursing, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia; 5Department of Nursing Management and Education, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Correspondence: Islam Ali Oweidat, Faculty of Nursing, Zarqa University, P.O. Box 132222, Zarqa, 13132, Jordan, Email [email protected]
Objective: Despite the value of undertaking patient safety culture, its association with horizontal violence in nursing workplace is still understudied. This study aimed to investigate the association between the perceived patient safety culture and its relationship with horizontal violence among nurses working in Jordan.
Methods: A cross-sectional correlational design was used. Nurses working in major governmental hospitals in Jordan were conveniently recruited to complete an online self-administered questionnaire, which included the following tools: Hospital Survey on Patient Safety Culture and Negative Behaviours in Healthcare (NBHC) Survey. The survey was designed to measure attitudes and perceptions on patient safety culture at multiple levels of a healthcare organization with ten dimensions. The Negative Behaviours in Healthcare (NBHC) survey was developed as an adaptation of the Lateral Violence in Nursing Survey (LVNS) with 25 items and two open-ended questions.
Results: A total of 330 nurses responded to the questionnaire. Nurses moderately perceived patient safety culture (HSOPS mean = 3.5, SD = 1.1). Low incidence of horizontal violence was claimed (mean = 2.1, SD = 1.1). However, it was associated with moderate negative correlation with patient safety culture (r = − 0.53, p < 0.001). Regression model revealed that patient safety culture explained an additional 53% of the variance of horizontal violence after controlling the effects of age and length of clinical experience (R-square change: 0.560, SE: 19.7, P: 0.001, CI: 1.21– 1.57).
Conclusion: Despite its low incidence, patient safety culture was found influential to the horizontal violence based on the perspectives of nurses in Jordan. Patient safety culture can be incorporated with other factors that contribute to the development of horizontal violence in nursing workplace.
Keywords: patient safety culture, hospital, horizontal violence, nurses, safety
A Letter to the Editor has been published for this article.
Background
Safety has been identified as one of the essential components of quality nursing care.1 In the past, safe nursing practice has been defined within the constraints of activities that prevent the occurrence of harm from errors and adverse events in health care.2,3 This definition has now been expanded to include the critical contribution of nurses in the collaboration and integration of activities to ensure safer and standardized practice.4
The traditional perspective that delimits the concept of safety in healthcare has extended to include a healthy work environment without fear of harm, discrimination, or prejudice.5,6 A patient safety culture demonstrates the efforts to initiate, implement, and sustain interventions despite increasing risks from medical errors, incorrect technology utilization, staff shortage, and improper or outdated facilities.7,8 Healthcare organizations that demonstrate positive patient safety culture possess the critical components of teamwork, reporting and learning from errors, communication, and leadership support.4
Despite the recognition of the significance of patient safety culture, little is known about its association with the precluding horizontal violence (HV).9,10 HV is a phenomenon that can negatively impact staff physical, mental, and occupational health.11,12 HV in nursing is defined as
Hostile, aggressive, and harmful behaviour by a nurse or a group of nurses toward a co-worker or group of nurses via attitudes, actions, words, and/or other behaviours.13
Studies have documented many forms of HV such as bullying, incivility, and hazing, mobbing, and relational aggression. Gaudine et al suggested that HV occurs between individuals who have unequal power, for example, between senior nurses and novice nurses.14 The predominant viewpoint is that HV is only an individual or, at most, an interpersonal issue, and occurrences that are underreported by nurses and studies suggest that nurses may have difficulty in recognizing the existence of the phenomenon.15,16 A number of studies performed in Jordan have reported the prevalence of HV in health care system.17 Thus, understanding the link between patient safety culture and HV can provide insight about this association and possible implications to policymakers. This study aimed to investigate the association between the perceived patient safety culture and its relationship with horizontal violence among nurses working in Jordan.
Methodology
Design
The study utilized a descriptive, cross-sectional, and correlational study design. The design allowed the researcher to investigate whether any significant relationship exists between the two variables of interest which are patient safety culture and HV.
Settings
The study was performed in three multi-specialty government hospitals in the central region of Jordan namely (1) Al Bashir Hospital, the largest government hospital in Jordan with more than 1700 beds and 1200 nurses, (2) Prince Hamza Hospital, the second largest government hospital in Jordan with 700 beds and 600 nurses, and (3) Zarqa Hospital with 500 beds and 600 nurses.18
Sampling
Convenience sampling was utilized to recruit nurses to participate in the study. Jordanian participants who have at least bachelor’s degree and permanently employed by the research settings were included in the study. The calculated sample size was 330 nurses.
Instruments
Nurses were asked to fill-out survey forms which were distributed online via WhatsApp link. The study utilized three instruments in data collection namely:
- Participants’ demographics: The participant information sheet asked for the demographic characteristics of the nurses who agreed to join the study such as age, gender, place of work, length of years as a nurse, and length of years employed in the hospital.
- Hospital Survey on Patient Safety Culture Version 2.0 (HSOPS Ver 2.0) which was developed by the Agency for Healthcare Research and Quality (AHRQ). The survey was designed to measure attitudes and perceptions on patient safety culture at multiple levels of a healthcare organization.19 It consists of 40 items on a 6-point Likert scale indicating either agreement (from “strongly agree” to “strongly disagree”) or frequency (“never” to “always”), with a “don’t know” or “does not apply” option to choose from. Ten dimensions HSOPS investigate as follows: (1) communication about error, (2) communication openness, (3) handoffs and information exchange, (4) hospital management support for patient safety, (5) organizational learning – continuous improvement, (6) reporting patient safety events, (7) response to error, (8) staffing and workplace, (9) supervisor, manager or clinical leader support for patient safety, and (10) teamwork. Psychometric testing of the tool was tested previously and showed higher internal consistency (Cronbach’s alpha > 0.7) and factor loadings of each item via confirmatory factor analysis of more than 0.4.20
- Negative Behaviours in Healthcare (NBHC) Survey.
The Negative Behaviours in Healthcare (NBHC) survey was developed as an adaptation of the Lateral Violence in Nursing Survey (LVNS).21 The survey tool is composed of 25 items and two open-ended questions. Factors contributed to negative behaviour were measured using 9 items (ie rude behavior, major personality clashes, power and control issues, inadequate staffing and resources, job stress leading to loss of control over behavior, misunderstandings related to cultural differences, targeted person not willing to stand up to perpetrator, leaders not willing to intervene, and peers not willing to intervene), and 3 items measuring fear of retaliation using a four-point Likert-type response scale varying from “agree strongly” to “disagree strongly”. The frequency of lateral aggression between peers is measured by 3 items, while 4 items measure the frequency of vertical aggression using a five-point Likert-type response scale ranging from “daily” to “never”. Finally, 6 items measure the seriousness of lateral/vertical aggression using a five-point Likert-type response scale ranging from “very serious” to “not serious”. Testing the internal consistency showed acceptable Cronbach α values of 0.64 to 0.92. Convergent and discriminant validity tests showed acceptable variance values (0.52 to 0.77).21 For the purposes of this study, items related to vertical aggression were excluded from the analysis.
Data Collection
The study obtained ethical approval from the University’s Research Ethics Board in University of Jordan and from the ethical review boards of each of the government hospitals. Data collection started with primary researcher visits to head nurses of each selected departments. The researcher explained the inclusion criteria for the head nurses and nurse managers, who in turn screened their staff for meeting the criteria. The primary researcher then met the nurses who meet the inclusion criteria and explained the purposes of the study. The researcher then asked nurses who agreed to participate in the study to provide her with their phone number. A link of the online survey was sent to 330 nurses who accepted to join the study through phone WhatsApp applications. All nurses were asked to electronically sign an informed consent form and were given the tools of the study via the link. This link allowed the participant to open a web page and to fill out the survey forms online. For data protection and confidentiality purposes, WhatsApp link was only valid to be opened by one internet browser and only for 48 hours upon opening the link. An online informed consent was sought from each participant. Nurses had the right to refuse joining the study without providing any explanation. Data collection was started on (January 16, 2021) and completed on (May 28, 2021). Another copy of the data was saved on a disc for possible damage of data. All methods were carried out in accordance with relevant guidelines and regulations of the Declaration of Helsinki.
Data Analysis
The Statistical Package for the Social Sciences (SPSS) Version 23 was used. The Kolmogorov–Smirnov normality assessment test was performed to confirm whether data were normally distributed or not. Frequency, percentage, means and standard deviations were calculated to describe the demographic characteristics of the participants and the value of each composites and dimensions related to HSOPS and NBHC tools. Pearson’s r was calculated to determine any relationship between HSOPS and NBHC. The Hierarchical Multiple Regression was used to assess factors affecting HV after controlling potential variations across demographic characteristics. The P value was set at 0.05, and 95% Confidence Interval (CI) was reported in the final regression model.
Results
Sociodemographic Characteristics of the Participants
A total of 330 nurses participated in the study. As shown in Table 1, the mean of participants’ age was 36.9 years old. The majority of the participants were females (90.9%). Almost half of the participants worked in inpatient wards (46.7%) followed by the emergency department (17.9%). In terms of the length of time working as a registered nurse, the majority of the participants practiced nursing for 6–10 years (34.2%) and had a clinical experience between 1 and 5 years in the current clinical area (40.9%). Table 1 shows the demographic characteristics of the participants (Table 1).
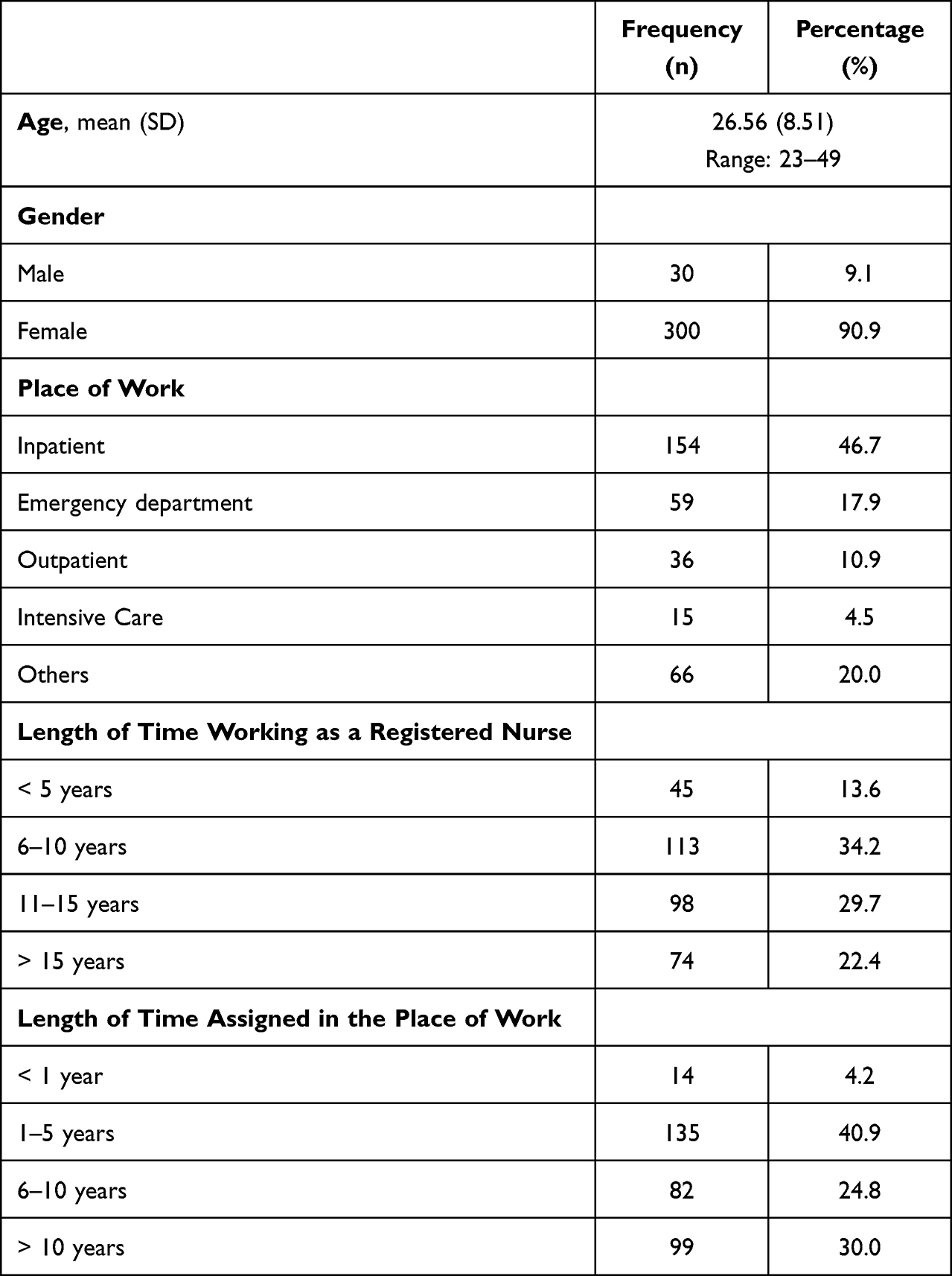 |
Table 1 Participants’ Demographics (N = 330) |
Nurses’ Perception of Patient Safety Culture
Participants had a moderate level of patient safety culture (mean = 3.5, SD = 1.1). Among the composite measures, participants scored the highest in communication about error and reporting patient safety events (means = 4.1 and 3.9, respectively). The lowest scored composite were on organizational learning and continuous improvement and response to error (means = 3.0 and 2.9, respectively). Table 2 shows the scores for each composite measure and overall rating for patient safety culture.
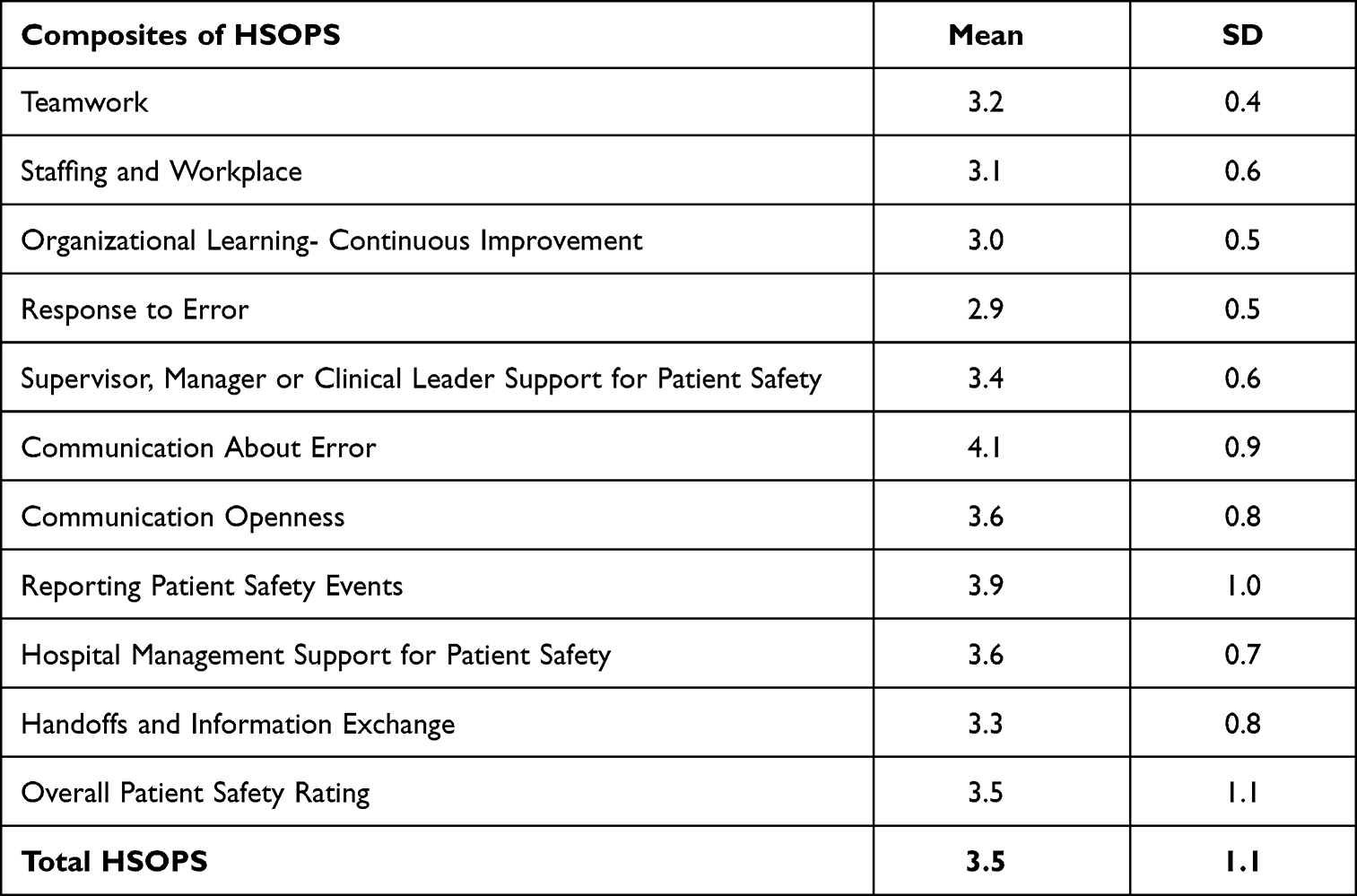 |
Table 2 Nurses’ Perception of Patient Safety Culture (HSOPS) and Its Correlation with HV (N = 330) |
Nurses’ Perception of Horizontal Violence
Based on the data presented in Table 3, participants demonstrated moderate levels of agreement that contributing factors to HV existed within their hospitals (mean = 2.8 out of 4). However, participants responded that incidents of HV were low (mean = 2.1 out of 5). When asked about the seriousness of incidents of HV, participants scored a moderate level of severity (mean = 2.5 out of 4). Lastly, participants claimed a moderate level of fear of retaliation when they reported an incident of HV (mean = 2.8 out of 4) (Table 3).
 |
Table 3 Nurses’ Perception of Negative Behaviors in Healthcare (NBHC) and Its Correlation with Patient Safety Culture (N = 330) |
Correlation Between Patient Safety Culture and Horizontal Violence
The results of Pearson’s r showed in Table 3 were based on the correlation between total HSOPS score and each NBHC Dimension. Based on the correlation coefficient r, a weak negative correlation was scored between HV Contributing Factors and total HSOPS (r = −0.291, p < 0.001) means that the higher the perception of nurses that contributing factors to HV existed in their hospitals, the lower were their levels of patient safety culture. Also, Pearson’s r showed a significant moderate negative relationship between frequency of aggression and patient safety culture (r = −0.532, p < 0.001) which means that the more frequent nurses experienced episodes of HV, the lower were their levels of patient safety culture. Moreover, Pearson’s r showed a weak negative but significant relationship was found between seriousness of aggression and patient safety culture (r = −0.311, p< 0.001) which means that the more serious the incidents of HV nurses experienced, the lower were their levels of patient safety culture. However, Pearson’s r showed that no significant relationship was found between the fear of retaliation and patient safety culture (p = 0.156).
Table 4 shows the correlation coefficient by Pearson’s r statistic test to determine the relationships existed between composite measures of patient safety culture and dimensions of HV. The table demonstrates a number of positive and negative significant correlations, ranged from weak–moderate strength correlations (Table 4). It can be concluded from the table that nurses who had higher perceptions of the existence of contributing factors to HV in their workplace, had scored less in the majority of composite measures of patient safety culture. Similarly, nurses who perceived more incidents of HV had scored less in the majority of composite measures of patient safety culture. In terms of seriousness of aggression, nurses who experienced more severe incident of HV had low scores in the majority of composite measures of patient safety culture. Lastly, nurses who experienced fear of retaliation of HV were associated with minimal relationship with most patient safety culture dimensions.
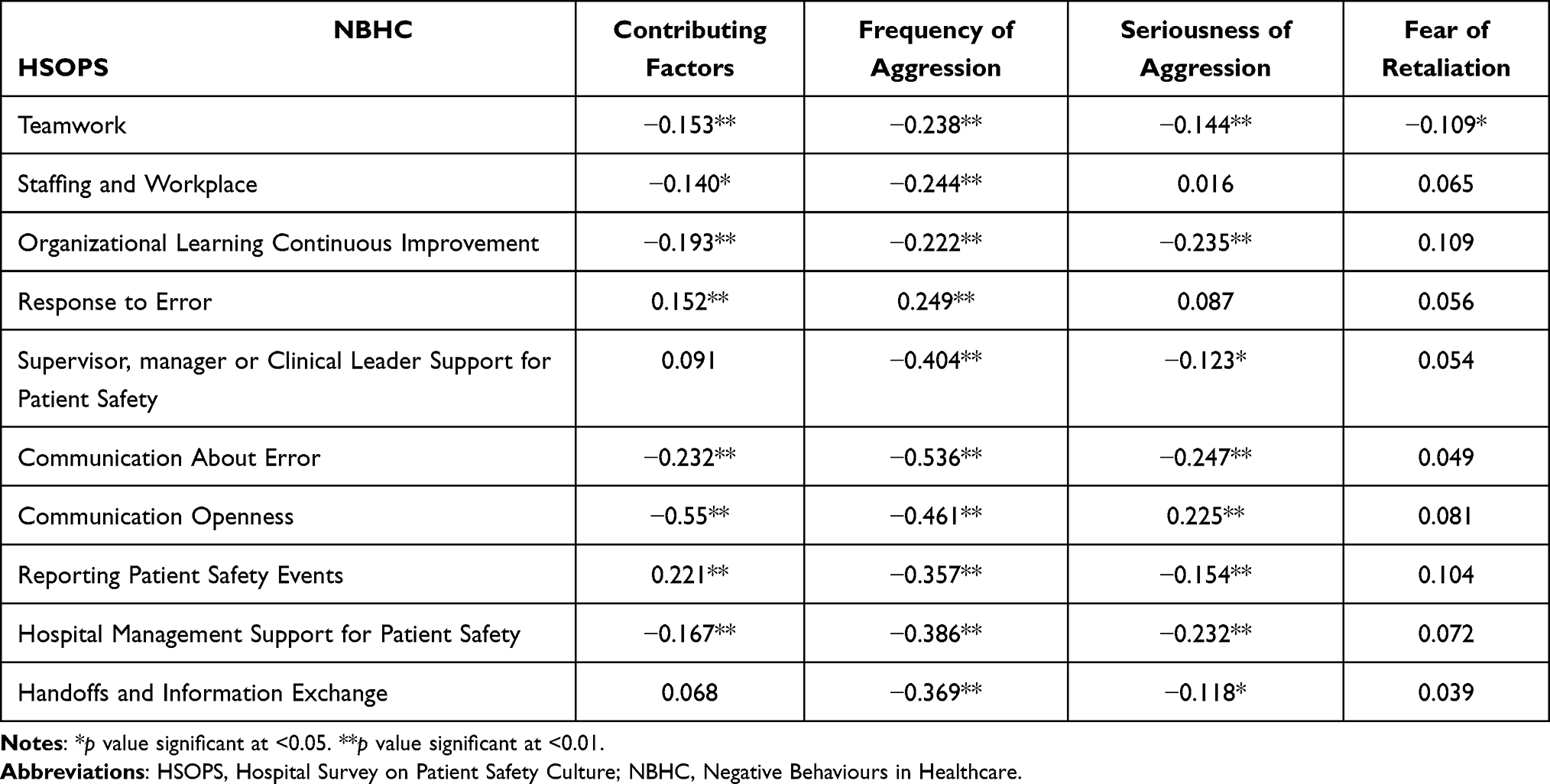 |
Table 4 Inter-Correlations Matrix Between Dimensions of Patient Safety Culture and Horizontal Violence |
Based on the correlation coefficient and mean differences across demographic variables, two main demographic variables showed significant correlation/variations with patient’s safety culture and HV which were age and length of experience as RN. Thus, Hierarchical Multiple Regression was conducted to assess the effect of patient’s safety culture on the HV frequency of aggression (Dependent variable), which was found the highly correlated variable, after eliminating the impact of the above demographic variables. As shown in Table 5, the results of this regression model indicated that patient’s safety culture explained an additional 53% of the variance in HV after controlling the effects of age and length of experience. This means that patients’ safety culture is considered a robust factor contributing to the incidence of HV.
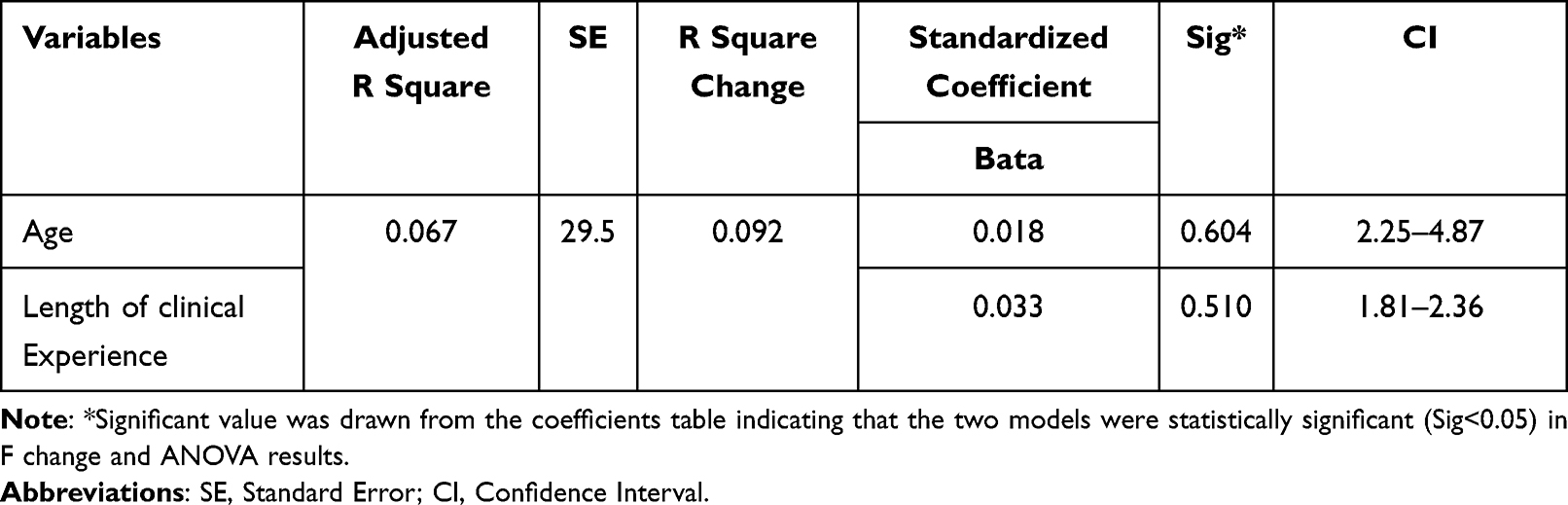 |
Table 5 Regression Model of Factors Influencing the Perception of Horizontal Violence |
Discussion
The results of the study showed that participants demonstrated a moderate level of patient safety culture which was not significantly different to the findings of other studies performed in Jordan.22–25 The moderate level of patient safety culture, while far from the ideal high levels that are being advocated for healthcare organizations worldwide, implies a room for improvement among hospitals that participated in this study. In addition, the study recognizes that there are certain weak components such as response to error, organizational learning – continuous improvement, and staffing and workplace (which are composite measures of patient safety culture where participants had the lowest scores) that can be targeted by innovative and evidence-based interventions and strategies. With the current healthcare climate around the world, coupled with pressures from managing the consequences of COVID-19 pandemic, problems of inadequate staffing, unavailable resources and supplies, inadequate time for nurse managers to fairly and judiciously respond to incidents of errors in patient care, and issues with cascading and disseminating learning points from patient safety incidents continue to plague healthcare organizations. Therefore, making it unsurprising that participants in the study found the same issues that could jeopardize patient safety within their hospitals.26,27 On the other hand, higher scores on communication about error and reporting of patient safety events indicated the strengths of the hospitals which should be fostered and promoted, especially since the results demonstrated that nurses frequently reported both errors that were caught prior to reaching the patient and errors that could have harmed the patient, and that nurses were made aware once errors were committed and discussions were held on how to prevent the reoccurrence of those errors.28,29 While it is recognized that committing errors in the delivery of patient care is ultimately inevitable since nurses and other healthcare professionals are not perfect and are only humans, the significant component of patient safety culture is the reporting of such errors when they occur and finding effective strategies in mitigating the risks of those errors from ever happening again.4 However, the low scores of participants on response to error indicated that nurse managers and hospital administrators had less than satisfactory performance when it comes to dealing with incidents of errors in patient care, with nurses citing mistakes being held personally against them, nurses being targeted instead of the root cause of why the error occurred in the first place, and the lack of support provided to nurses who committed errors and mistakes.
When it comes to HV, results showed that nurses had moderate levels of agreement that contributing factors to HV existed within their healthcare organizations, and that nurses experienced moderate levels of seriousness of aggression and fear of retaliation. While to the knowledge of the researcher and as per the review of literature, this study is the first to utilize the Negative Behaviors in Healthcare Survey among nurses in Jordan. The results of the study matched with Jordanian nurses at some point in their careers experienced one form or another of HV.25,30 Even if participants reported a low frequency of the occurrence of HV in their workplaces, the fact remains that nurses experienced aggression towards them that was perpetrated by their colleagues. Literature is clear that HV, regardless of the frequency of occurrence, can negatively impact job performance, job satisfaction, mental health and well-being, and staff retention.31,32 Therefore, every effort to lessen and prevent the occurrence of HV should be prioritized by nurse managers and hospital administrators.
The key limitation of this study is the cross-sectional nature of the study which was performed at the same time as the COVID-19 pandemic, which meant that significantly added stress and pressures arising from this disease might have contributed to lower levels of patient safety culture and observed higher incidences of HV.
Conclusions
Patient safety culture is a relevant component of safer and quality healthcare delivery system. However, HV can negatively affect the well-being of nurses and the attainment of patient-sensitive outcomes. The study results showed that nurses had a moderate level of patient safety culture while at the same time had moderate levels of agreement that HV is existing within their workplaces. Patient safety culture is considered an influential factor that affects the development and occurrence of HV in nursing workplace.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgment
The authors extend their appreciation to Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R279), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Funding
The research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R279), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sim J, Joyce-McCoach J, Gordon R, Kobel C. Development of a data registry to evaluate the quality and safety of nursing practice. J Adv Nurs. 2019;75:1877–1888.
2. Kim MJ, Jang SG, Kim IS, Lee W. A study on the status and contributory factors of adverse events due to negligence in nursing care. J Patient Saf. 2020;17:e904–e910. doi:10.1097/PTS.0000000000000791
3. Chapuis C, Chanoine S, Colombet L, Calvino-Gunther S, Tournegros C, Schwebel C. Interprofessional safety reporting and review of adverse events and medication errors in critical care. Ther Clin Risk Manag. 2019;15:549–556. doi:10.2147/TCRM.S188185
4. Agency for Healthcare Research and Quality. Advancing patient safety; 2020. Available from: https://www.ahrq.gov/patient-safety/resources/advancing.html.
5. Connor JA, Ziniel SI, Porter C, Doherty D, Moonan M, Hickey PA. Interprofessional use and validation of the AACN healthy work environment assessment tool. Am J Crit Care. 2018;27:363–371. doi:10.4037/ajcc2018179
6. Raso R, Fitzpatrick JJ, Masick K. Clinical nurses’ perceptions of authentic nurse leadership and health work environment. J Nurs Adm. 2020;50:489–494. doi:10.1097/NNA.0000000000000921
7. Smith JG. The nurse work environment: current and future challenges. J Appl Biobehav Res. 2018;23(1):e12126. doi:10.1111/jabr.12126
8. Nouri A, Sanagoo A, Jouybari L, Taleghani F. Challenges of respect as promoting healthy work environment in nursing: a qualitative study. J Educ Health Promot. 2019;8:261. doi:10.4103/jehp.jehp_125_19
9. Rainford WC, Wood S, McMullen PC, Philipsen N. The disruptive force of lateral violence in the health care setting. J Nurse Pract. 2015;11:157–164. doi:10.1016/j.nurpra.2014.10.010
10. Nemeth LS, Stanley KM, Martin MM, Mueller M, Layne D, Wallston KA. Lateral violence in nursing survey: instrument development and validation. Healthcare. 2017;5(3):33. doi:10.3390/healthcare5030033
11. Taylor RA. Nurses’ perceptions of horizontal violence. Glob Qual Nurs Res. 2016;3:1.
12. Wei H, Sewell KA, Woody G, Rose MA. The state of the science of nurse work environments in the United States: a systematic review. Int J Nurs Sci. 2018;5:287–300. doi:10.1016/j.ijnss.2018.04.010
13. Taylor RA, Taylor SS. Reframing and addressing horizontal violence as a workplace quality improvement concern. Nurs Forum. 2018;53:459–465. doi:10.1111/nuf.12273
14. Gaudine A, Patrick L, Busby L. Nurse leaders’ experiences of upwards violence in the workplace: a systematic review protocol. JBI Database Syst Rev Implement Rep. 2019;17:627–632. doi:10.11124/JBISRIR-2017-003765
15. Blackstock S, Salami B, Cummings GG. Organizational antecedents, policy and horizontal violence among nurses: an integrative review. J Nurs Manag. 2018;26(8):972–991. doi:10.1111/jonm.12623
16. Layne DM, Nemeth LS, Mueller M, Schaffner MJ, Stanley KM, Wallston KA. Negative behaviours in health care: prevalence and strategies. J Nurs Manag. 2018;27(3):154–160. doi:10.1111/jonm.12660
17. El-Hneiti M, Shaheen AM, Salameh AB, Al-dweeri RM, Al-Hussami M, Ahmad M. An explorative study of workplace violence against nurses who care for older people. Nurs Open. 2019;7:1.
18. Ministry of Health. Health statistics and indicators; 2020. Available from: https://www.moh.gov.jo/EN/Pages/Health_Statistics_and_Indicators.
19. Giai J, Boussat B, Occelli P, et al. Hospital survey on patient safety culture (HSOPS): variability of scoring strategies. Int J Qual Health Care. 2017;29:685–692. doi:10.1093/intqhc/mzx086
20. Sorra J. AHRQ surveys on patient safety culture TM hospital survey version 2.0; 2021. Available from https://www.ahrq.gov/sites/default/files/wysiwyg/sops/surveys/3-sorra-sopshospital-survey-2-0-webcast.pdf.
21. Layne DM, Nemeth LS, Mueller M, Martin M. Negative behaviors among healthcare professionals: relationship with patient safety culture. Healthcare. 2019;7:23. doi:10.3390/healthcare7010023
22. Abu AlRub RF, Alhijaa EH. The impact of educational interventions on enhancing perceptions of patient safety culture among Jordanian senior nurses. Nurs Forum. 2014;49(2):139–150. doi:10.1111/nuf.12067
23. Khater WA, Akhu-Zaheya LM, Al-Mahasneh SI, Khater R. Nurses’ perception of patient safety culture in Jordanian hospitals. Int Nurs Rev. 2014;62:82–91. doi:10.1111/inr.12155
24. Saleh AM, Darawad MW, Al-Hussami M. The Perception of Hospital Safety Culture and Selected Outcomes among Nurses: an Exploratory Study. Nurs Health Sci. 2015;17:339–346. doi:10.1111/nhs.12196
25. Obeidat RF, Qan’ir Y, Turaani H. The relationship between perceived competence and perceived workplace bullying among registered nurses: a cross-sectional study. Int J Nurs Stud. 2018;88:71–78. doi:10.1016/j.ijnurstu.2018.08.012
26. Al-Mugheed K, Bayraktar N, Al-Bsheish M, et al. Patient safety attitudes among doctors and nurses: associations with workload, adverse events, experience. Healthcare. 2022;10(4):631. doi:10.3390/healthcare10040631
27. Al‐Mugheed K, Bayraktar N. Patient safety attitudes among critical care nurses: a case study in North Cyprus. Int J Health Plan Manag. 2020;35(4):910–921. doi:10.1002/hpm.2976
28. Alzoubi MM, Al-Mahasneh A, Al-Mugheed K, Al Barmawi M, Alsenany SA, Farghaly Abdelaliem SM. Medication administration error perceptions among critical care nurses: a cross-sectional, descriptive study. J Multidiscip Healthc. 2023;31:1503–1512. doi:10.2147/JMDH.S411840
29. Oweidat I, Al-Mugheed K, Alsenany SA, Abdelaliem SM, Alzoubi MM. Awareness of reporting practices and barriers to incident reporting among nurses. BMC Nurs. 2023;22(1):1. doi:10.1186/s12912-023-01376-9
30. Al-Sagarat A, Qan’ir Y, Al-Azzam M, Obeidat H, Khalifeh A. Assessing the impact of workplace bullying on nursing competencies among registered nurses in Jordanian public hospitals. Nurs Forum. 2018;53:304–313. doi:10.1111/nuf.12253
31. Brooks AM, Polis N, Philips E. The new healthcare landscape: disruptive behaviors influence work environment, safety and clinical outcomes. Nurse Leader. 2014;12:39–44. doi:10.1016/j.mnl.2013.11.006
32. Al-Shaban ZR, Al-Otaibi ST, Alqahtani HA. Occupational violence and staff safety in health-care: a cross-sectional study in a large public hospital. Risk Manag Healthc Policy. 2021;20:1649–1657. doi:10.2147/RMHP.S305217
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Perceptions About Patient Safety Culture Between Physicians and Nurses in Public Hospitals in Vietnam
Tran TNH, Pham QT, Tran LH, Vu TA, Nguyen MT, Pham HT, Le TT, Bui TTH
Risk Management and Healthcare Policy 2022, 15:1695-1704
Published Date: 6 September 2022
Level of Patient Safety Culture Awareness Among Healthcare Workers
Albaalharith T, A'aqoulah A
Journal of Multidisciplinary Healthcare 2023, 16:321-332
Published Date: 2 February 2023
Impact of Educational Intervention on Compliance of Health Care Workers Towards Chemotherapy Handling Guidelines
Alaraidh S, Alnaim LS, Almazrou SH
Journal of Multidisciplinary Healthcare 2023, 16:3035-3042
Published Date: 16 October 2023
Factors Associated with Work Life Balance Among Nurses in Hospitals: A Socio-Ecological Scoping Review
Widayana IGAA, Agustina HR, Mediawati AS
Journal of Multidisciplinary Healthcare 2025, 18:4511-4521
Published Date: 31 July 2025