")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Level of Patient Safety Culture Awareness Among Healthcare Workers
Authors Albaalharith T , A'aqoulah A
Received 11 June 2022
Accepted for publication 19 August 2022
Published 2 February 2023 Volume 2023:16 Pages 321—332
DOI https://doi.org/10.2147/JMDH.S376623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Taghreed Albaalharith,1 Ashraf A’aqoulah1,2
1Department of Health Systems Management, College of Public Health and Health Informatics, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Centre, Riyadh, Saudi Arabia
Correspondence: Ashraf A’aqoulah, Department of Health Systems Management, College of Public Health and Health Informatics, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia, Tel +966 11 4295415, Email [email protected]
Background: Patient safety is a major concern at all levels of the healthcare system, with the primary objective of reducing patient hazards when providing care. The Kingdom of Saudi Arabia has made great progress in improving the health of its citizens over the last few decades, particularly in terms of patient safety. Currently, many health-care institutions throughout the world are interested in implementing a safety culture to lower the risk of harm and the number of accidents associated with routine treatment.
Purpose: This study aims to assess the level of awareness concerning patient safety culture among health-care providers in hospitals in Riyadh, Saudi Arabia.
Methods: This is a descriptive cross-sectional quantitative study that used the Agency for Healthcare Research and Quality’s patient safety culture questionnaire. The survey was conducted online and was completed by 204 health-care employees from three distinct hospital settings in Riyadh, Saudi Arabia: government, quasi-government, and private hospitals.
Results: The results showed a low level of patient safety culture awareness among health-care workers in the 10 dimensions of patient safety. The mean score was 2.24 out of 5 and the standard deviation was 0.50. Participants assigned the highest mean scores to Organisational Learning and Continuous Improvement (Mean: 2.48, Standard deviation: 0.66), Communication About Error (Mean: 2.44, Standard deviation: 0.70), and Teamwork (Mean: 2.40, Standard deviation: 0.64). Interestingly, the scores for hospital supervisor and managerial positions are significant compared to other clinical positions (p-value = 0.047). Moreover, the patient safety rating and the number of reported events were significantly related to the overall level of awareness (p-value < 0.001), (p-value = 0.042), respectively.
Conclusion: In Riyadh hospitals, overall patient safety awareness is low, necessitating adequate attention and effective solutions such as encouraging reporting errors, implementing safety huddles and leadership walkarounds, and establishing a patient safety culture. Health-care executives and managers are encouraged to develop safety cultures that promote trust and justice, allowing employees to be candid about their mistakes and failings without retaliation. Moreover, this safety culture should be defined by the following qualities: a just culture, a learning culture, and a reporting culture.
Keywords: patient safety culture, awareness among healthcare, hospital, Saudi Arabia
Introduction
Patient safety is a worldwide concern at all levels of the healthcare system, with the primary goal of lowering patient risks when providing health-care services. To this end, the World Health Organization (WHO) has advised its member countries to implement systematic changes in order to promote safety and improve the quality of health care.1 In 1999, the Institute of Medicine (IOM) issued the “To Err is Human” report, which emphasised the importance of patient safety. Additionally, it stressed that the prevention of error is a process that requires significant system-wide adjustments centred on avoiding, recognising, and minimising hazardous behaviours in hospitalised patients that could lead to high morbidity and mortality rates. This IOM report was supported by a 2016 report from Johns Hopkins University School of Medicine, whose findings reveal that more than 250,000 people in the US die every year because of medical mistakes, which makes it the third-leading cause of death after heart disease and cancer.2–5 Therefore, health-care organisations (HCOs) should focus on promoting patient safety as practiced by various health-care workers (HCWs) linked with patient safety culture, such as physicians, nurses, pharmacists, and nutritionists.4
Unsafe medical care places a major burden on people’s lives. Every year, over 134 million adverse events occur in health facilities in poor and middle-income nations, resulting in 2.6 million fatalities from hazardous care. In an Eastern Mediterranean and African study, nearly a third of patients who had a harmful episode died, 14% had permanent disability, 16% had moderate disability, 30% had minor disability, and 8% of the patients’ harm could not be determined.6 In Saudi Arabia, patient safety and medical errors have become a major national issue in the last decade, with the media focusing on them. However, only a few studies on the subject have been conducted.7 A combination of negative factors such as staff shortages, insufficient buildings and overcrowded facilities, deficiencies in health-care supplies, lack of basic equipment, and poor cleanliness and sanitation contribute to the lack of safety in patient care in low- and middle-income countries (LMICs). Moreover, other factors that can worsen patient care include insufficient capability of health-care systems and institutions (including a lack of a strong safety and quality culture), defective care processes, and leadership indifference. Consequently, it is the responsibility of health-care institutions to ensure that people receive safe health care.8 Promoting this concept among health-care practitioners and maintaining this perception in hospital systems require establishing a strong patient safety culture that cannot be achieved without the support of policymakers, health-care practitioners, and managers. A healthy and positive patient safety culture is essential to making the patient safety culture a top priority.9
In recent years, patient safety in health care has become a major global issue. Despite the fact that health systems vary by country, many patient safety concerns have similar causes and can often be addressed in similar ways. For that reason, the global ministerial summits on patient safety were launched in 2015. The first two summits took place in March 2016 in London and March 2017 in Bonn. The main goal was to promote and support the worldwide movement for patient safety and narrow the safety gap by bringing together international experts and political decision makers. In Tokyo 2018, the third global ministerial conference took place, reaffirming the worldwide commitment to patient safety. Additionally, Saudi Arabia hosted the fourth Global Ministerial Summit on Patient Safety in 2019. The conference centred on improving patient safety in low- and middle-income nations, which account for two-thirds of worldwide patient damage. During the summit, the Jeddah Declaration on Patient Safety was produced, which includes crucial suggestions for continuing to advance the global patient safety movement, particularly in low- and middle-income countries. Despite this momentum, the fifth global summit, which was scheduled to be hosted by the Swiss government in 2020, was postponed due to the Covid-19 pandemic.10
Over the last few decades, Saudi Arabia has achieved significant progress in improving the health of its people—particularly in the area of patient safety. The new model of care (MOC) highlights the best practices for persons and population groups in terms of care and services. It additionally aims to guarantee that patients obtain the appropriate care at the appropriate time from the appropriate team in the appropriate setting.11 This model consists of six systems of treatment that focus on the many types of care that the health system would provide: preventive, planned, maternity and child, urgent, chronic, and palliative. It also offers six levels of services, ranging from individual empowerment through primary care and specialist health services. Each system of care has its own set of paths for individuals to follow in order to receive the treatment they need, as well as its own set of success metrics.12
Aim of the Study
The present study focuses on assessing the level of awareness concerning patient safety culture among health-care providers in hospitals in Riyadh, Saudi Arabia.
Objectives
The main objectives of the research are as follows:
- To assess the level of PSC awareness among health-care workers
- To identify the main domain of PSC that impede the implementation of patient safety
- To identify the major challenges within the domains that impede the implementation of patient safety in hospitals in Riyadh, Saudi Arabia
- To determine the impact of demographic variables (gender, age, level of education, position in hospital, work area, and hospital type) on the awareness of PSC
Literature Review
A Patient Safety Culture (PSC) has been well-defined as the organisation’s shared attitudes and beliefs about safety.13 It includes a safety climate, which is the organisation’s perceived value of safety. Patient safety was initially revised in response to health and climate reports, but the current review focuses on safety culture. Although the perspectives of organisations may vary, a positive PSC should imply that people are safe whenever they enter the healthcare system.13 A culture of this type recognises the inevitability of error and tends to focus on proactively addressing latent threats while trying to incorporate non-punitive practices for reporting errors and analysing possible adverse events. The situation of cultural safety in Saudi is similar to the concepts mentioned above.14 According to the cross-sectional study that was conducted in Saudi Arabia, three dimensions were recommended to influence patient safety climate: support from the management, a proper reporting system, and the availability of adequate resources.15
Patient safety is a critical part of providing high-quality healthcare, which is why there is a growing safety culture around the world. Cultivating a safety culture, however, requires a thorough grasp of a society’s cultural ideas, values, and standards in terms of population health. Such knowledge allows health-care administrators to identify behaviours and attitudes that should be encouraged, rewarded, or anticipated. For example, a critical examination of many health systems has demonstrated the importance of emphasising organisational elements such as patient safety rather than individual failings.16 Dealing with patient safety issues from a culture change approach has been shown to produce the most positive impact on increasing the safety and quality of healthcare. Instead of blaming individual culprits, health systems are recommended to consider mistakes as opportunities for safety and quality improvements.17
Patient safety in healthcare refers to the protection of both patients and health-care workers (HCWs), and patient safety cultures have evolved to promote health-care procedures and serve as a benchmark for future progress.3 Furthermore, research has shown that health-care facilities all across the world are concerned about patient safety. In 2010 and 2013, studies conducted in Taiwan and China, respectively, revealed similar results. There was a positive attitude towards PSC among health-care workers in these countries;18,19 conversely, a study conducted in Iran measuring the culture of patient safety showed moderate and weak levels of PSC.20 A similar study in Iran also showed that the level of PSC is low.21 Moreover, another study conducted in 2017 in Peru testing PSC in two different health sectors (public and private) showed a low-grade result.22 Therefore, attention should be directed to this issue by managers, professionals, and policymakers.
A growing number of health-care organisations throughout the world are interested in the safety culture idea as a way to reduce the risk for injury and the number of accidents related to everyday treatment.23 However, patient safety culture still needs to be emphasised more strongly in Arab countries. All stakeholders—including legislators, health professionals, medical educators—should be involved in the journey towards improvement.24
According to patient safety studies, there are still areas for improvement in the patient safety culture at hospitals in Riyadh, Saudi Arabia.25 As such, health-care institutions should develop a blame free culture boosting communication and leadership capability, learning from errors and incorporating patient insights into safety programs.24 A study conducted in Palestinian public hospitals highlighted that punitive and blame cultures, under-reporting of occurrences, lack of open communication, and insufficient managerial support are all major obstacles to patient safety in hospitals.26 Nonetheless, previous research in Arab nations has found a typically expected low standard of positive patient safety culture among pharmacists as well as less development in the provision of safe health care.26,27 This implies that a patient safety problem exists in Saudi Arabia, and that health-care staff continue to face obstacles in maintaining patient safety in hospitals in accordance with patient safety guidelines.3
In Saudi Arabia, access to healthcare has increased dramatically during the last three decades.28 Furthermore, quality improvement and safety methods have been addressed to overcome challenges of accessing care. These methods are aligning organisational procedures with pressure from outside sources; prioritising quality over quantity; establishing quality-improvement mechanisms that are beneficial to the entire organisation; launching departmental duties and team expertise; creating care pathways that are based on evidence of high-quality and safety actions; setting up information systems with a pathway focus; assessing and offering comments on a regular basis.10
Still, merely having access to health care is not enough. Patients entering the healthcare system, whether in a clinic, hospital, or another setting, need to know that they will receive care that is safe, effective, and based on the most recent clinical evidence. This is especially crucial in hospitals, where patients are often desperately ill. Because of this, ensuring quality is a crucial component of a high-performing system.29 Accreditation programs such as the Joint Commission International Accreditation (JCIA) and the Central Board Accreditation of Health Institutions (CBAHI) have been shown to improve patient safety and reduce the chance of near misses, poor outcomes, and medical mistakes.30 In a study conducted at King Abdul-Aziz University Hospital to assess the impact of accreditation on the PSC, the result showed that accreditation has significantly improved the perception of nurses on the awareness of patient safety.31 Furthermore, success in patient safety requires the creation of a PSC that supports health-care facilities.32 Despite the fact that PSC is becoming more widespread within every health-care institution, more efforts, such as investing in health-care provider education, are needed to progress and eventually champion its values. Thus, the current study aims to assess the level of awareness of health-care providers toward patient safety culture in Riyadh hospitals in the Kingdom of Saudi Arabia.
Materials and Methods
Study Design and Setting
A descriptive cross-sectional quantitative study targeting all health-care workers across the central region of the Kingdom of Saudi Arabia, in Riyadh. The study was conducted at three different hospital settings: governmental, quasi, and private hospitals in Riyadh, Saudi Arabia.
Study Subjects and Sample Size
All health-care workers in Riyadh hospitals—whether clinicians, non-clinicians with direct contact with patients such as doctors and staff nurses, and workers without direct contact such as support services, administrators, managers, supervisors or contractors, were eligible and invited to participate in this study. Health-care workers outside Riyadh were excluded from this study. The data were collected in April and May 2021. The sample size was 204 participants completed the survey.
Sampling Method
The probability-sample technique was utilised in this study. The hospital survey on patient safety culture (HSOPSC) questionnaire was administered online to the target population as a Google Form through several social media applications including Telegram, Twitter, WhatsApp, as well as via email. The questionnaire consisted of 14 sections, and it varied between requiring short answers and five-point Likert scale responses. All questions were marked as obligatory to ensure that none was left unanswered. Participants were moved automatically to the next section once all the questions were answered.
Data Collection Tool
The validated and reliable HSOPSC tool, adopted from the Agency for Healthcare Research and Quality, was used to collect the data.33 The survey tool was developed to assess the awareness of hospital staff in regard with patient safety issues, medical errors, and event reporting. It contains 34 items that measure 12 dimensions of PSC, including the following: teamwork (3 items); staffing and work pace (4 items); organisational learning and continuous improvement (3 items); non-punitive response to error (4 items); supervisor, manager, clinical leader support (3 items); feedback and communication about error (3 items); communication openness (4 items); reporting patient safety events (2 items); hospital management support (3 items); hands off and information exchange (3 items). The first 10 dimensions use a five-point Likert scale of agreement (ranging from 1, “Strongly disagree”, to 5, “Strongly agree”) or frequency (from 1, “Never”, to 5, “Always’). An answer choice for ‘Does not apply’ or ‘I don’t know” was also included. Moreover, the survey contained two outcome questions that assessed how respondents rated overall patient safety in their hospital and how many events they had reported in the previous 12 months.
Data Analysis
Statistical Package for the Social Sciences (IBM SPSS version 25.0) was used to conduct the statistical analysis and calculate the overall mean score of all dimensions. A higher score indicates better PSC. Skewness and kurtosis criteria were used to test normality; therefore, the results showed that all dimensions were normally distributed. Thus, t-tests and one-way ANOVA were used. In all analyses, a p value <0.05 was considered statistically significant. Number and percentage were used to describe the sociodemographics of the study population.
An independent t-test was used to assess the statistical significance in mean scores between genders. One-way analysis of variance (ANOVA) was used to determine possible differences among other independent variables. Furthermore, ANOVA was utilised to test statistically significant differences between the number of reported events and total level of awareness (total mean score) as well as patient safety rating and total level of awareness (total mean score). When ANOVAs were significant, Tukey post-hoc tests were used to detect the differences.
Results
Demographics
Table 1 shows number and percentage of demographic data. A total of 204 employees working in different hospitals in Riyadh completed the PSC survey. More than half of the participants were male n = 105 (51.5%). Participants between the ages of 31 and 40 (n = 90), constituted 44.1% of the sample size. Participants holding a bachelor’s degree (n = 100) were almost half of the sample size (49%). Nurses were the highest participating group (n = 62, 30.4%), followed by physicians (n = 43, 21.1%). The participation of employees working in in-patient units (n = 55) and out-patient clinics (n = 51) were 27% and 25%, respectively. However, 60 participants were working in managerial and administrative positions (29.4%). Regarding hospital types, governmental hospitals (n = 76) constituted 37.3% of the sample, and quasi hospital n = 66 constituted 32.4%.
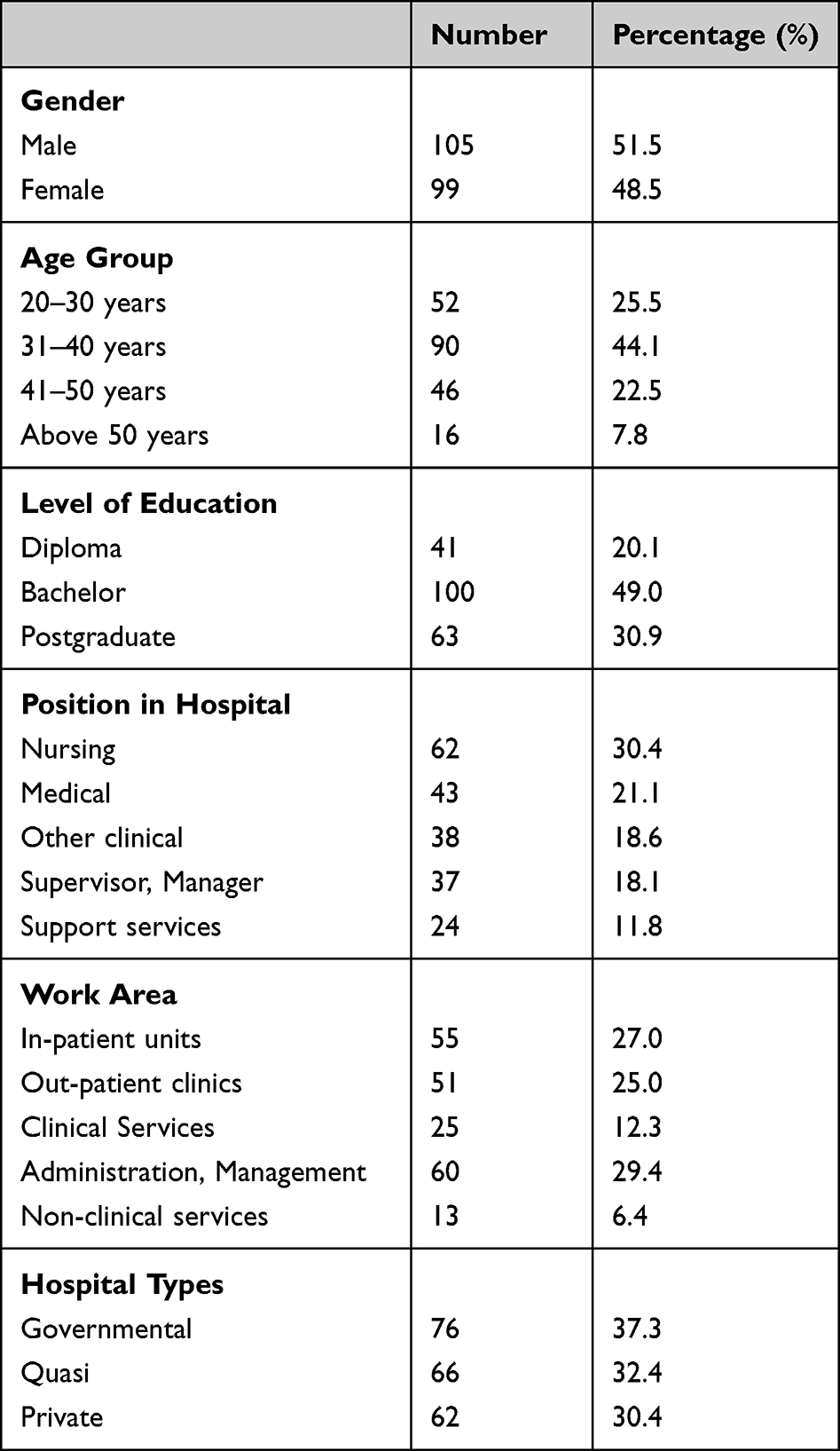 |
Table 1 Number and Percentage of Demographic Data |
Participants’ Level of Awareness on PSC Dimensions
Table 2 shows level of awareness of all PSC dimensions. The mean score of all domains together was low: 2.24 with standard deviation 0.50. In all dimensions, the level of awareness among health-care providers was low except for the following three dimensions, where the level of awareness was moderate: Team Work (M = 2.40, SD = 0.64), Organisational Learning - Continuous Improvement (M = 2.48, SD = 0.66), and Communication about Error (M = 2.44, SD = 0.70).
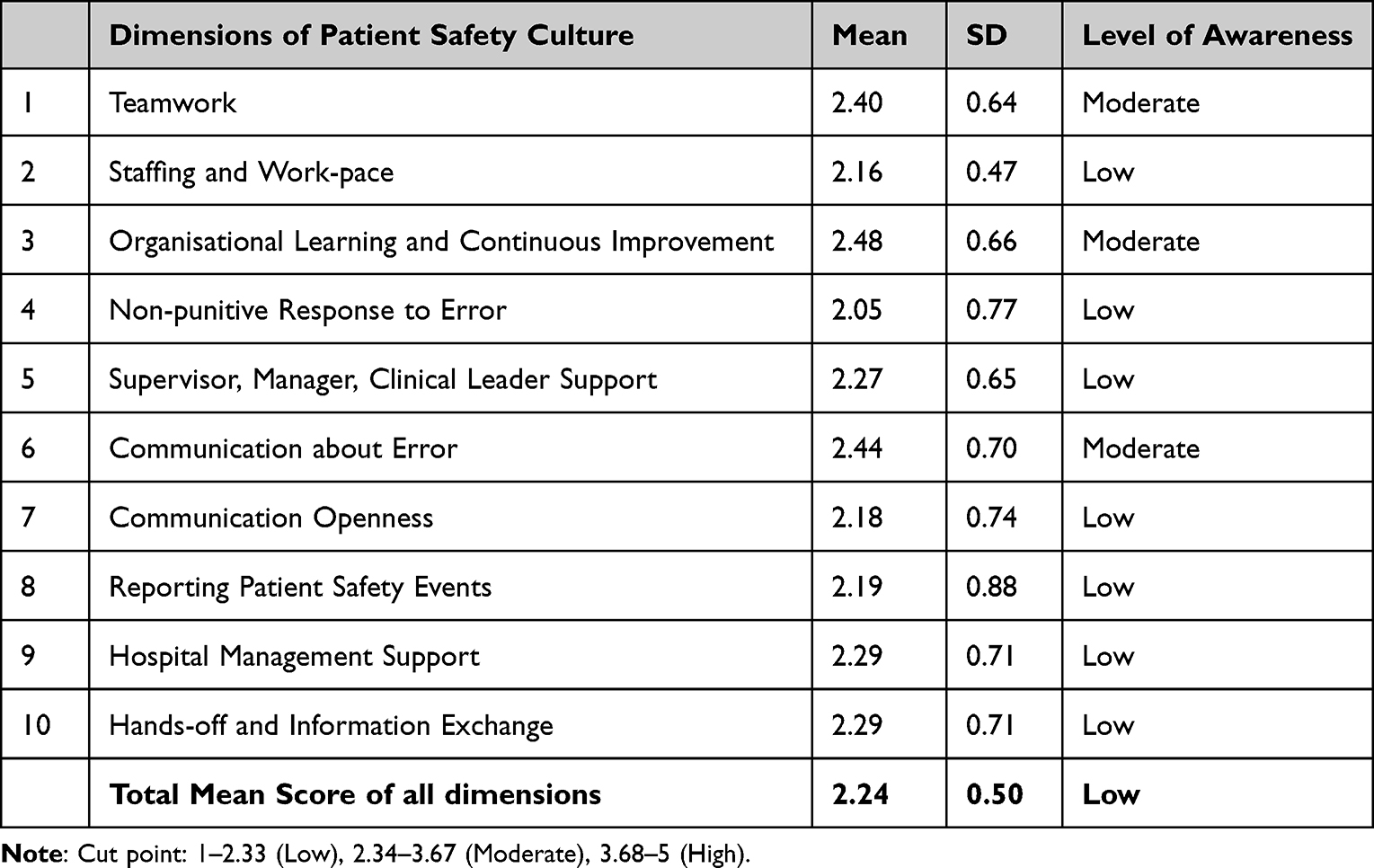 |
Table 2 Level of Awareness of All PSC Dimensions |
Determining the Factors of Significance Influence by Using t-test or ANOVA
A t-test was used to determine whether there was a statistically significant difference in the mean between male and female. The results showed that there is no significant difference between genders (p-value = 0.53). One-way ANOVA was used to determine the possible differences among other independent variables. The result revealed that there is no significant difference between and within the groups in all variables which are age group (p-value: 0.69); education level (p-value: 0.13); work area (p-value: 0.67); and hospital type (p-value: 0.87), except in position in hospital variable.
Table 3 shows association between position in hospital variable and level of awareness.
 |
Table 3 Association Between Position in Hospital Variable and Level of Awareness |
The result revealed that there is significant association between position in hospital variable and level of awareness (p-value = 0.038).
Table 4 shows difference between positions in hospital groups. To investigate this significant difference between groups, the Tukey HSD post hoc was used. The analysis revealed that there is a statistically significant difference in “supervisor, management position” (Mean: 2.43, Standard Deviation: 0.50) compared to other clinical positions (Mean: 2.11, Standard Deviation: 0.37) in hospital (p-value = 0.047).
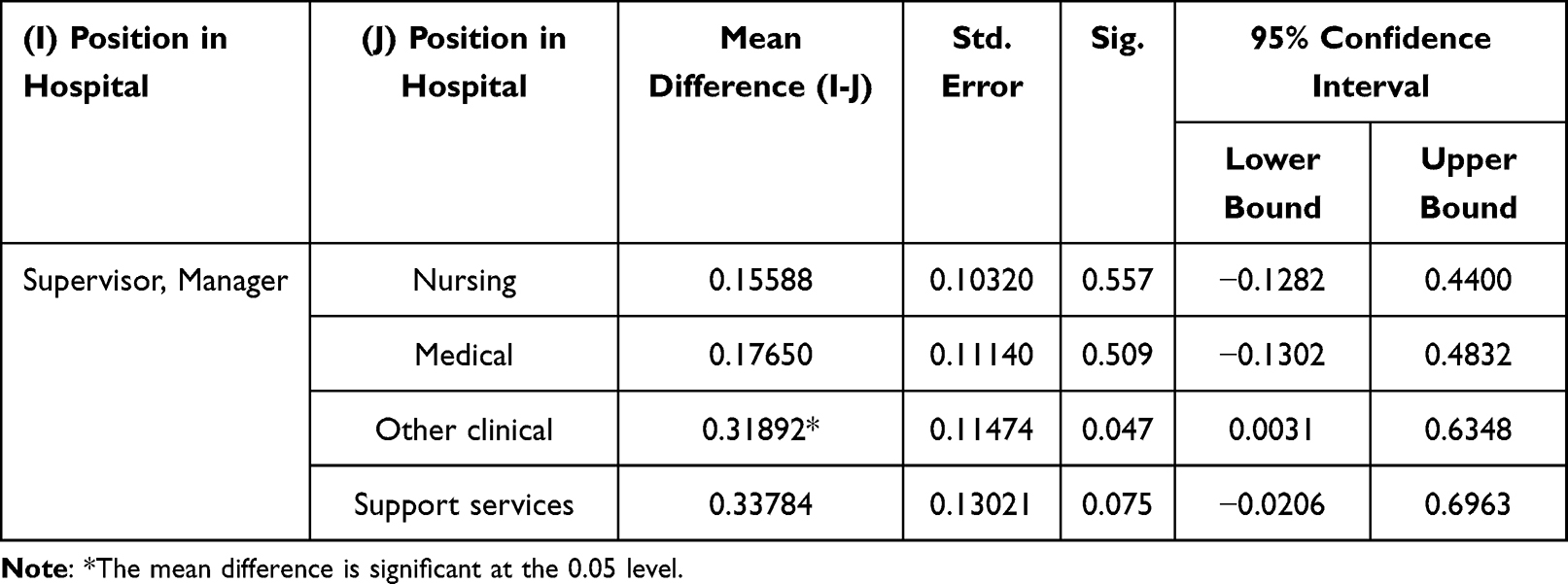 |
Table 4 Difference Between Positions in Hospital Groups |
Discussion
The present study used the HSOPSC tool to assess the level of PSC awareness among health-care workers in Riyadh hospitals. Findings of this study identified that PSC awareness is generally low, particularly in the following dimensions: staffing and work-pace; non-punitive response to error; communication openness; supervisor, manager, clinical leader support; reporting patient safety events; hospital management support for patient safety; and hands-off and information exchange. These areas, in particular, require improvement. By contrast, the dimensions of teamwork, feedback and communication about error, and organisational learning and continuous improvement had a moderate score. In 2017, the Saudi Patient Safety Centre sponsored a nationwide hospital assessment on PSC. Both cycles’ findings revealed the same areas of improvements, such as staffing, communication openness and non-punitive response to error.34
In this study, the overall level of PSC awareness was low, which is similar to the finding of the cross-sectional research conducted at a teaching hospital in Ghana. This indicates that the situation is serious. To completely comprehend and alter the PSC in healthcare, professionals must be trained in patient safety.35 Specifically, the seven areas that need urgent improvement are nonpunitive response to error, staffing and work-pace, communication about error, communication openness, hospital management support, reporting patient safety events, and hands-off and information exchange. The remaining three dimensions—organisational learning and continuous improvement, teamwork, and a nonpunitive response to errors—must be preserved and enhanced, as this is the core of maintaining and improving patient safety.
Research conducted in a large teaching hospital in Riyadh showed that the areas of strengths were teamwork and organisational learning and continuous improvement. In contrast, staffing, non-punitive response to error, and communication openness were the areas that need to be improved. Our findings are aligned with the strengths and weaknesses of this study. Regarding the barriers of communication openness and response to errors, these can be linked to participants’ responses to the question about how often they report an incident; this indicates a fear of reporting, and this can be linked to some participants’ view that their mistakes would be used against them when they report an incident. Fear of reporting can be a barrier to developing a healthy PSC. Fear, guilt, and the presence of a punitive response to error are all reasons given in the literature for not reporting errors. There is a need to motivate health-care workers, especially nurses, who made up around 30% of sampled respondents, to report events because of their positive influence on patient safety.9
Further, a study conducted in Primary Health Centres (PHCs) in Kuwait found that effective communication methods could be institutionalised to promote communication openness. Moreover, poor communication is associated with unsafe worker behaviours such as policy and procedure infractions and inadequate event reporting. Establishing an open communication system can lead to improvement in patient safety outcomes.36 The results of this study are in line with others conducted in Sweden and Tunisia, both of which revealed the existence of a punitive culture.37 Because of the fear of punishment, a punitive culture may leave essential patient safety issues unresolved. Multiple interventions and ongoing efforts are required to create a non-punitive culture. Furthermore, cultural transformation is a lengthy process. Safety culture should be monitored on a regular basis, areas of improvement should be identified, and steps should be established to strengthen the culture even more.38
Staffing proved to be an issue for respondents in this study, as they explicitly noted working longer hours than is optimum for patient safety and trying to accomplish too much too fast in crisis mode. Given the enormous body of research relating the availability of health-care workers to population health outcomes, this conclusion is critical.39 Major patient-related crises have occurred in organisations with an insufficient number of staff.24 In circumstances when the number of employees is fewer than optimal for providing patient care, most professionals are overworked, burned out, suffer from stress, and lack sleep which can lead to failures in performance that influence the quality and patient outcomes.36 Several researchers found that work environment problems such as feeling overworked, staff shortages, lack of time and equipment, and workload are barriers to patient centred care.40 Improvement efforts concentrating on staffing, work pace as well as work pressure may lead to better safety culture.41
Moreover, many respondents also stated that they require further help from their bosses and leaders. More effective governance and leadership might help with this. Front-line employees should feel heard and appreciated when they communicate with management.42 Leadership is critical to fostering an open and encouraging environment for the reporting of patient safety hazards.43 Closing the loop or giving feedback fosters trust and openness, both of which are crucial characteristics of a good patient safety culture.42 A systematic review study undertaken in Saudi Arabia found that “blame culture” and communication challenges were major issues confronting health-care systems in several Arab nations. Consequently, it is possible to argue that in the health-care systems in Arab nations, especially in Saudi Arabia, a blaming culture prevails. This might be attributed to weak leadership and a lack of legislation to ensure patient safety.24 Through leadership acts of facilitation and elaboration, hospital administrators and managers play a critical role in establishing a safety culture that emphasises patient safety in health-care institutions.44
Respondents also voice concern about “hands off and Information exchange”. Our result is similar to the study conducted in a public hospital in Yemen.45 According to a study conducted in 2010, staff perceptions of the behavioural characteristics of handoffs impact their judgement of the hospital’s level of patient safety.46 The AHRQ and the Accreditation Council for Graduate Medical Education (ACGME) have made improving patient handoffs a priority in order to improve patient safety.47 Building the capacity of the medical staff through handoff processes and established protocols may help to boost a hospital’s PSC.48 Mentoring and leading by example, with a clear focus on transitions of care, are also important components of building a safety program in a healthcare company.49 Additionally, hospitals may create a strong culture of cooperation across units to assist health-care workers to manage the trade-off between efficiency and thoroughness, while also adopting other organisational development activities to link its employees to a similar vision and mental model. According to the theory of planned behaviour, attitude is a critical aspect that may be modified via training and education. Teaching and training clinical staff in handoff processes and protocols can potentially be utilised to affect the PSC of a health-care institution.48
Despite the findings described above, other dimensions including teamwork, feedback and communication about error, and organisational learning and continuous improvement were scored in the moderate level. This conclusion is consistent with other studies.9,37,50–52 This consistency could be due to proper utilisation of the SBAR tool (Situation, Background, Assessment, Recommendation), which has been found to reduce adverse occurrences in hospitals, enhance communication among health-care workers, and improve patient safety.53 Additionally, the hospital staff are supportive of one another and treat others with respect when it comes to teamwork.35 Current literature has demonstrated a strategy— team huddles or daily briefings—to enhance communication, teamwork, and patient safety and care.42
Regarding the influence of demographic characteristics on PSC awareness, our findings demonstrated that there was no linkage between gender and overall mean score. The finding is in line with research conducted at a Turkish primary health-care institution. There was no association between gender and total mean score.50 Moreover, our result showed that there was no relationship between the level of education and patient safety. The lack of this relationship was highlighted by an integrative review done in 2008.54 Despite this deficiency, the Council of the European Union and the Helsinki Declaration have supported patient safety training and education at all levels of the health system. Leaders of health-care institutions, consequently, must strive to promote continual learning and education for their workers, which will improve their safety performance.55,56 Another finding revealed in the present study is that there were no statistically significant differences in the level of awareness of PSC among health-care workers in the various work areas or among the three types of hospitals (governmental, quasi-governmental, and private). This finding demonstrated that safety culture is not comprehensively established in these hospitals, which mirrors the study carried out in Brazil in 2016 and Iran in 2019.57,58
Interestingly, the current research identified an association between the position held in the hospital and the total level of awareness; this is particularly true of the supervisor and management positions as compared to other clinical positions. Researchers found similar results in a study conducted in hospitals in Palestine, Virginia, and Japan.59–61 This outcome may be due to the fact that leaders and managers have a proper and accurate understanding of the present state of patient safety issues, which allows them to create an action plan when needed. Additionally, managers and leaders must always be aware of patient safety issues and must have a stronger influence on hospital safety culture formation than other clinicians or non-managers. From this perspective, hospital leaders must emphasise the need of developing a culture of safety while taking into consideration the diverse levels of health-care workers. They must work diligently and effectively to reduce any potential risk to the quality and safety of patient care.60,61
Limitation of the Study
There are a few limitations in this study. First, the study was conducted in a single location in Saudi Arabia, Riyadh may not reflect the country’s overall trend. Another limitation is that all respondents came from the same city in Riyadh, thus limiting the generalisability of the findings. Furthermore, online data collection usually involves some unique challenges, such as low response rates, inability to reach older age groups, uneven participant distribution, recall bias, and participant fraud. Finally, despite the fact that Arabic is the official language in Saudi Arabia, only the English version of the questionnaire was disseminated, which may have limited the ability of some employees to fully comprehend it.
Conclusion
The current study uses one of the most widely used tools, HSOPSC, to assess patient safety culture awareness among health-care workers in Riyadh hospitals. Despite the fact that the majority of respondents reported significant weaknesses in areas such as staffing and work-pace; non-punitive response to errors; supervisor, manager, and clinical leader support; communication openness; reporting patient safety events; hospital management support; and hands-off and information exchange. They also reported moderate mean scores in some HSOPSC domains, primarily in teamwork, organisational learning and continuous improvement, and communication about errors.
It is critical for Riyadh hospitals to invest in training that would improve patient safety. There is a need to incorporate safety training into hospital learning programs, with a focus on the need to build a safety culture. Continuous training is required, as is the implementation of policies, governance, and an open reporting system. Leaders and managers are also encouraged to create a blame-free environment for health-care professionals to report incidents, as well as to implement structures and processes that prioritise psychological safety alongside physical safety, and to use the Just Culture Algorithm to respectfully respond to a crisis.
The findings of this study provide significant insight into the issues that Riyadh hospitals face in Saudi Arabia. The findings may pave the way for legislative reforms targeted at enhancing hospital safety. To begin implementing safety improvements, hospitals must mobilise resources to increase the number of staff, set rules that encourage non-punitive reporting, and establish effective communication channels to improve communication and teamwork, as well as to simplify the transition process.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (IRB) at King Abdullah International Medical Research Centre (KAIMRC). The study approval number is SP21R/157/04. Written informed consent was obtained from all participants.
Funding
No funding was obtained to conduct this research.
Disclosure
There were no conflicts of interest revealed by the authors.
References
1. Kang S, Ho TTT, Lee NJ. Comparative studies on patient safety culture to strengthen health systems among southeast asian countries. Front Public Heal. 2021;8(January). doi:10.3389/fpubh.2020.600216
2. Makary MA, Daniel M. Medical error-the third leading cause of death in the US. BMJ. 2016;353:1–5. doi:10.1136/bmj.i2139
3. Alshammari F, Pasay-an E, Alboliteeh M, Alshammari MH, Susanto T, Villareal S. A survey of hospital healthcare professionals’ perceptions toward patient safety culture in Saudi Arabia. Int J Africa Nurs Sci. 2019;11:100149. doi:10.1016/j.ijans.2019.100149
4. Koushal VK, Goyal V. Patient safety is the need of the hour: a study in nursing department of a tertiary care teaching hospital. Int J Res Found Hosp Healthc Adm. 2017;5(2):55–59. doi:10.5005/jp-journals-10035-1076
5. Aburayya A, Alshurideh M, Albqaeen A, Alawadhi D, Al A’yadeh I. An investigation of factors affecting patients waiting time in primary health care centers: an assessment study in Dubai. Manag Sci Lett. 2020;10(6):1265–1276. doi:10.5267/j.msl.2019.11.031
6. Mohammed F, Taddele M, Gualu T. Patient safety culture and associated factors among health care professionals at public hospitals in Dessie town, north east Ethiopia, 2019. PLoS One. 2021;16:1–9. doi:10.1371/journal.pone.0245966
7. Al-Khaldi Y. Attitude of primary care physicians toward patient safety in Aseer region, Saudi Arabia. J Fam Community Med. 2013;20(3):153. doi:10.4103/2230-8229.121976
8. World Health Organization. WHO/HIS/SDS/2017.11.2017; 2017. Available from: http://apps.who.int/bookorders.
9. El-Jardali F, Sheikh F, Garcia NA, Jamal D, Abdo A. Patient safety culture in a large teaching hospital in Riyadh: baseline assessment, comparative analysis and opportunities for improvement. BMC Health Serv Res. 2014;14. doi:10.1186/1472-6963-14-122
10. Global Ministerial Summit on Patient Safety. Jeddah declaration on patient safety. Minist Heal MOH. 2019;2019:1.
11. Alomari N, Alshehry B, Alenazi A, et al. Model of care knowledge among Riyadh first health cluster staff at the ministry of health, Saudi Arabia. J Fam Med Prim Care. 2021;10(8):3094. doi:10.4103/jfmpc.jfmpc_405_21
12. Chowdhury S, Mok D, Leenen L. Transformation of health care and the new model of care in Saudi Arabia: kingdom’s vision 2030. J Med Life. 2021;14(3):347–354. doi:10.25122/jml-2021-0070
13. Willmott J, Mould J. Health professionals’ perception of patient safety culture in acute hospitals: an integrative review. Aust Heal Rev. 2018;42(4):387–394. doi:10.1071/AH16274
14. Okuyama JHH, Galvão TF, Crozatti MTL, Silva MT. Health professionals’ perception of patient safety culture in a university hospital in São Paulo: a cross-sectional study applying the hospital survey on patient safety culture. Sao Paulo Med J. 2019;137(3):216–222. doi:10.1590/1516-3180.2018.0430140319
15. Walston SL, Al-Omar BA, Al-Mutari FA. Factors affecting the climate of hospital patient safety: a study of hospitals in Saudi Arabia. Int J Health Care Qual Assur. 2010;23(1):35–50. doi:10.1108/09526861011010668
16. Alonazi NA, Alonazi AA, Saeed E, Mohamed S. The perception of safety culture among nurses in a tertiary hospital in Central Saudi Arabia. Sudan J Paediatr. 2016;16(2):51–58.
17. Elmontsri M, Banarsee R, Majeed A. Improving patient safety in developing countries – moving towards an integrated approach. JRSM Open. 2018;9(11):205427041878611. doi:10.1177/2054270418786112
18. Chen IC, Li HH. Measuring patient safety culture in Taiwan using the Hospital Survey on Patient Safety Culture (HSOPSC). BMC Health Serv Res. 2010;10. doi:10.1186/1472-6963-10-152
19. Nie Y, Mao X, Cui H, He S, Li J, Zhang M. Hospital survey on patient safety culture in China. BMC Health Serv Res. 2013;13(1). doi:10.1186/1472-6963-13-228
20. Ebrahimzadeh N, Saravani S, Soltani A, Bazzi M. Hospital survey on patient safety culture in Iran. J Pharm Sci Res. 2017;9(10):1765–1767.
21. Lawati M, Dennis S, Short SD, Abdulhadi NN. Patient safety and safety culture in primary health care: a systematic review. BMC Fam Pract. 2018;19(1):1–13. doi:10.1186/s12875-018-0793-7
22. Arrieta A, Suárez G, Hakim G. Assessment of patient safety culture in private and public hospitals in Peru. Int J Qual Heal Care. 2018;30(3):186–191. doi:10.1093/intqhc/mzx165
23. Cooper MD. Towards a model of safety culture. Saf Sci. 2000;36(2):111–136.
24. Albalawi A, Kidd L, Cowey E. Factors contributing to the patient safety culture in Saudi Arabia: a systematic review. BMJ Open. 2020;10(10):1–8. doi:10.1136/bmjopen-2020-037875
25. Alswat K, Abdalla RAM, Titi MA, et al. Improving patient safety culture in Saudi Arabia (2012–2015): trending, improvement and benchmarking. BMC Health Serv Res. 2017;17(1):1–14. doi:10.1186/s12913-017-2461-3
26. Ghobashi MM, El-Ragehy HAG, Mosleh H, Al-Doseri FA. Assessment of patient safety culture in primary health care settings in Kuwait. Epidemiol Biostat Public Heal. 2014;11(3):e9101. doi:10.2427/9101
27. Alwabel AM, Bawazir AA, Al-Surimi K. Assessment of patient safety culture among pharmacists in Riyadh hospitals, Saudi Arabia. J Infect Public Health. 2015;8(4):402. doi:10.1016/j.jiph.2015.04.016
28. Aljuaid M, Mannan F, Chaudhry Z, Rawaf S, Majeed A. Quality of care in university hospitals in Saudi Arabia: a systematic review. BMJ Open. 2016;6(2):e008988. doi:10.1136/bmjopen-2015-008988
29. Joint Commission International. JCI accreditation standards for hospitals. Jt Comm Int Accredit Stand Hosp. 2015;2015:12–14.
30. Gupta S, Sahu J, Shivani Gupta C. Benefit of accreditation in hospitals. Curr Res Pharm Sci. 2013;2:39–44.
31. Al-Awa B, Al Mazrooa A, Rayes O, et al. Benchmarking the post-accreditation patient safety culture at King Abdulaziz University Hospital. Ann Saudi Med. 2012;32(2):143–150. doi:10.5144/0256-4947.2012.143
32. Stavrianopoulos T. The development of patient safety culture. Heal Sci J. 2012;6(2):201–211.
33. Sorra J, Gray L, Streagle S, Famolaro T, Yount N, Behm J. Surveys on Patient Safety Culture (SOPS) hospital survey; 2016. Available from: https://www.ahrq.gov/sops/surveys/hospital/index.html.
34. Saudi Patient Safety Center. National recommendations for hospital survey on patient safety culture; 2020:1–13. Available from: https://t.co/yxb0SeocDv?amp=1.
35. Muftawu M, Aldogan EU. Measuring patient safety culture: a study at a teaching hospital in Ghana. J Patient Saf Risk Manag. 2020;25(6):250–258. doi:10.1177/2516043520938534
36. Alfadhalah T, Mudaf A, Alghanim HA, et al. Baseline assessment of patient safety culture in primary care centres in Kuwait: a national cross-sectional study. BMC Health Serv Res. 2021;1:1–18.
37. Aboul-Fotouh AM, Ismail NA, Ez Elarab HS, Wassif GO. Assessment of patient safety culture among healthcare providers at a teaching hospital in Cairo, Egypt. East Mediterr Heal J. 2012;18(4):372–377. doi:10.26719/2012.18.4.372
38. Singer SJ, Dunham KM, Bowen JD, et al. Lessons in safety climate and safety practices from a California hospital consortium. Adv Patient Saf from Res. 2005;3:1.
39. El-Jardali F, Jamal D, Abdallah A, Kassak K. Human resources for health planning and management in the Eastern Mediterranean region: facts, gaps and forward thinking for research and policy. Hum Resour Health. 2007;5. doi:10.1186/1478-4491-5-9
40. Ree E. What is the role of transformational leadership, work environment and patient safety culture for person-centred care? A cross-sectional study in Norwegian nursing homes and home care services. Nurs Open. 2020;7(6):1988–1996. doi:10.1002/nop2.592
41. Aboneh EA, Stone JA, Lester CA, Chui MA. Evaluation of patient safety culture in community pharmacies. J Patient Saf. 2020;16(1):E18–E24. doi:10.1097/PTS.0000000000000245
42. Dingley C, Daugherty K, Derieg MK, Persing R. Improving patient safety through provider communication strategy enhancements. Adv Patient Saf New Dir Altern. 2008;3:1.
43. Mercer S, Furler J, Moffat K, Fischbacher-Smith D, Sanci L. Multimorbidity: technicalseries on safer primary care. Geneva: World Health Organization. 2016. Available from: https://apps.who.int/iris/bitstream/handle/10665/252275/9789241511650-eng.pdf.
44. Lee SE, Dahinten VS. The enabling, enacting, and elaborating factors of safety culture associated with patient safety: a multilevel analysis. J Nurs Scholarsh. 2020;52(5):544–552. doi:10.1111/jnu.12585
45. Alsabri M, Alghallabi MA, Al-Qadasi FA, et al. Patient safety culture in emergency departments of Yemeni public hospitals: a survey study. Front Emerg Med. 2021;5(2). doi:10.18502/fem.v5i2.5618
46. Vogus TJ, Sutcliffe KM, Weick KE. Doing no harm: enabling, enacting, and elaborating a culture of safety in health care. Acad Manag Perspect. 2010;24(4):60–77. doi:10.5465/amp.2010.55206385
47. McDonald KM, Schultz EM, Chang C. Evaluating the state of quality-improvement science through evidence synthesis: insights from the closing the quality gap series. Perm J. 2013;17(4):52–61. doi:10.7812/TPP/13-010
48. Lee SH, Phan PH, Dorman T, Weaver SJ, Pronovost PJ. Handoffs, safety culture, and practices: evidence from the hospital survey on patient safety culture. BMC Health Serv Res. 2016;16(1):1–8. doi:10.1186/s12913-016-1502-7
49. Beach C, Cheung DS, Apker J, et al. Improving interunit transitions of care between emergency physicians and hospital medicine physicians: a conceptual approach. Acad Emerg Med. 2012;19(10):1188–1195. doi:10.1111/j.1553-2712.2012.01448.x
50. Bodur S, Filiz E. A survey on patient safety culture in primary healthcare services in Turkey. Int J Qual Heal Care. 2009;21(5):348–355. doi:10.1093/intqhc/mzp035
51. Farzi S, Farzi S, Moladoost A, Bahrami M, Etminani R. Patient safety culture in intensive care units from the perspective of nurses: a cross-sectional study. Iran J Nurs Midwifery Res. 2017;22(5):372–376. doi:10.4103/ijnmr.IJNMR_150_16
52. Galvão TF, Lopes MCC, Oliva CCC, De Almeida MEA, Silva MT. Patient safety culture in a university hospital. Rev Lat Am Enfermagem. 2018;26. doi:10.1590/1518-8345.2257.3014
53. Alahmadi HA. Assessment of patient safety culture in Saudi Arabian hospitals. Qual Saf Heal Care. 2010;19(5):1–5. doi:10.1136/qshc.2009.033258
54. Ridley RT. The relationship between nurse education level and patient safety: an integrative review. J Nurs Educ. 2008;47(4):149–156. doi:10.3928/01484834-20080401-06
55. Rall M, Van Gessel E, Staender S. Education, teaching & training in patient safety. Best Pract Res Clin Anaesthesiol. 2011;25(2):251–262. doi:10.1016/j.bpa.2011.02.013
56. Petrini F, Solca M, De Robertis E, et al. The Helsinki declaration on patient safety in anesthesiology: a way forward with the European board and the European society of anesthesiology. Minerva Anestesiol. 2010;76(11):971–977.
57. Chegini Z, Janati A, Afkhami M, Behjat M, Shariful Islam SM. A comparative study on patient safety culture among emergency nurses in the public and private hospitals of Tabriz, Iran. Nurs Open. 2020;7(3):768–775. doi:10.1002/nop2.449
58. Macedo TR, Rocha PK, Tomazoni A, de Souza S, Anders JC, Davis K. The culture of patient safety from the perspective of the pediatric emergency nursing team. Rev da Esc Enferm. 2016;50(5):756–762. doi:10.1590/S0080-623420160000600007
59. Elsous A, Akbari Sari A, AlJeesh Y, Radwan M. Nursing perceptions of patient safety climate in the Gaza Strip, Palestine. Int Nurs Rev. 2017;64(3):446–454. doi:10.1111/inr.12351
60. Hartmann CW, Rosen AK, Meterko M, et al. An overview of patient safety climate in the VA. Health Serv Res. 2008;43(4):1263–1284. doi:10.1111/j.1475-6773.2008.00839.x
61. Kobuse H, Morishima T, Tanaka M, Murakami G, Hirose M, Imanaka Y. Visualizing variations in organizational safety culture across an inter-hospital multifaceted workforce. J Eval Clin Pract. 2014;20(3):273–280. doi:10.1111/jep.12123
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.