Back to Journals » Infection and Drug Resistance » Volume 16
Comparison of Pegylated Interferon Alfa Therapy in Combination with Tenofovir Alafenamide Fumarate or Tenofovir Disoproxil Fumarate for Treatment of Chronic Hepatitis B Patients
Authors He J ![]() , Guo Y, Zhang Y, Han J, Chen J, Jia Y, Ma Z, Wu J, Zhang S, Li F, Mao R, Zhang J
, Guo Y, Zhang Y, Han J, Chen J, Jia Y, Ma Z, Wu J, Zhang S, Li F, Mao R, Zhang J
Received 6 March 2023
Accepted for publication 2 June 2023
Published 20 June 2023 Volume 2023:16 Pages 3929—3941
DOI https://doi.org/10.2147/IDR.S411183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jingjing He, Yifei Guo, Yao Zhang, Jiajia Han, Jingwen Chen, Yidi Jia, Zhenxuan Ma, Jingwen Wu, Shenyan Zhang, Fahong Li, Richeng Mao, Jiming Zhang
Department of Infectious Diseases, Shanghai Key Laboratory of Infectious Diseases and Biosafety Emergency Response, Shanghai Institute of Infectious Diseases and Biosecurity, National Medical Center for Infectious Diseases, Huashan Hospital, Fudan University, Shanghai, People’s Republic of China
Correspondence: Jiming Zhang; Richeng Mao, Department of Infectious Diseases, Shanghai Key Laboratory of Infectious Diseases and Biosafety Emergency Response, Shanghai Institute of Infectious Diseases and Biosecurity, National Medical Center for Infectious Diseases, Huashan Hospital, Fudan University, Room 510, Building 5, 12 Middle Wulumuqi Road, Shanghai, People’s Republic of China, Email [email protected]; [email protected]
Purpose: The study aims to evaluate the effectiveness of a tenofovir alafenamide fumarate (TAF) and pegylated interferon alfa (PegIFN-α) regimen compared to a tenofovir disoproxil fumarate (TDF) and PegIFN-α therapy in patients with chronic hepatitis B (CHB).
Patients and Methods: Patients who were treated with PegIFN-α in combination with TAF or TDF were retrospectively enrolled. The primary outcome measured was the HBsAg loss rate. The rates of virological response, serological response for HBeAg, and normalization of alanine aminotransferase (ALT) were also calculated. The cumulative incidences of response rates were compared between the two groups using Kaplan–Meier analysis.
Results: A total of 114 patients were retrospectively enrolled in the study, with 33 receiving TAF plus PegIFN-α treatment and 81 receiving TDF plus PegIFN-α treatment. The HBsAg loss rate for the TAF plus PegIFN-α group was 15.2% at 24 weeks and 21.2% at 48 weeks, while the TDF plus PegIFN-α group had rates of 7.4% at 24 weeks and 12.3% at 48 weeks (P=0.204 at 24 weeks, P=0.228 at 48 weeks). In subgroup analysis of HBeAg positive patients, the TAF group had a higher HBsAg loss rate of 25% at week 48, compared to 3.8% in the TDF group (P=0.033). According to Kaplan–Meier analysis, the TAF plus PegIFN-α group achieved virological response more quickly than the TDF plus PegIFN-α group (p=0.013). There was no statistical difference in HBeAg serological rate or ALT normalization rate.
Conclusion: There was no significant difference in the HBsAg loss between the two groups. However, subgroup analysis revealed that TAF plus PegIFN-α treatment had a higher HBsAg loss rate than TDF plus PegIFN-α treatment in HBeAg-positive patients. Additionally, TAF plus PegIFN-α treatment demonstrated better virological suppression for CHB patients. Therefore, TAF plus PegIFN-α treatment regimen is recommended for CHB patients who aim to achieve functional cure.
Keywords: hepatitis B virus infection, tenofovir alafenamide fumarate, tenofovir disoproxil fumarate, interferon, functional cure, combination therapy
Introduction
One of the leading causes of hepatocellular carcinoma (HCC) is chronic hepatitis B virus infection (CHB), with approximately 292 million people worldwide estimated by the World Health Organization to be affected by this condition.1 In cases where patients meet the specified criteria, prompt treatment is necessary. Currently, two classes of antiviral therapies have been approved for the treatment of chronic HBV infection: nucleos(t)ide analogues (NAs) and pegylated interferons alfa (PegIFN-α).2 Prompt and effective antivirus treatment can reduce liver-related complications such as fibrosis, hepatic decompensation, HCC, and decrease mortality related to HBV.3,4
Both NAs and PegIFN-α have limitations. Studies have shown that long-term NAs treatment cannot completely eradicate the virus as covalently closed circular DNA (cccDNA) remains latent in the nucleus. Moreover, it is challenging to achieve sero-clearance of Hepatitis B surface antigen (HBsAg) with NA treatment.2 On the other hand, PegIFN-α treatment has a higher chance of HBsAg clearance and has been proven to reduce intrahepatic cccDNA.5–7 However, it has high variability of response and some negative side-effects.
A combined approach of NA and PegIFN-α may offer advantages by combining the antiviral powerful effects of NA plus the immune modulation of IFN. Combination therapy has shown to have a higher rate of serological response and induce long-term immunological control with a finite duration treatment.8,9 Recent studies have explored various combinations treatment regimens and shown good therapeutic effects.9–11 Evidence suggests that tenofovir disoproxil fumarate (TDF) combining with PegIFN-α is more effective in clearing HBsAg than monotherapies and is widely used in China.8,9
NAs treatment with high barriers against HBV resistance includes entecavir (ETV), TDF, and tenofovir alafenamide (TAF). ETV has high resistance in patients previously exposed to lamivudine,12 while TDF is widely used in antiretroviral therapy but has concerns over long-term nephrotoxicity and bone impairments.13 TAF, a prodrug of TDF, a newer alternative, has shown better renal outcomes, good tolerability, and a high resistance barrier in real-world and Phase 3 studies.14–17 It has also shown better HBsAg reduction compared to ETV.18 Despite its high price, TAF is gradually being promoted in China as a first-line treatment due to its inclusion in the national insurance and future price reduction.19 However, the efficacy and safety of TAF combined with pegylated interferon alpha (PegIFN-α) treatment has not been reported. To address this, we conducted a retrospective study to compare the efficacy and safety of TAF combined with PegIFN-α therapy to the widely adopted TDF combined with PegIFN-α therapy in the treatment of chronic hepatitis B (CHB).
Materials and Methods
Study Population
This study is a retrospective observational cohort study that enrolled CHB patients who voluntarily started taking PegIFN-α (180ug, subcutaneous injection, once weekly) plus TAF (25mg per day) or TDF (300mg per day) between June 2016 and October 2021 at the Infection Disease Department. The patients were diagnosed with CHB and treated according to the guidelines of prevention and treatment for chronic hepatitis B.20 The admission criteria include patients who were between the ages of 18 and 75, had not received treatment with PegIFN-α in the past year, had no evidence of HCC, liver decompensation, or other severe comorbidities, and did not have co-infections with hepatitis C virus, hepatitis D virus, or human immunodeficiency virus. Patients who did not meet these criteria were excluded. Once a month, patients were admitted to the hospital for a comprehensive examination, including tests for HBV markers and biochemical parameters. For the remaining three weeks, patients self-administered subcutaneous injections at home. The combination treatment was to continue for one year. This study was approved by the Institutional Review Board or Independent Ethics Committee of Huashan Hospital and all patients provided written informed contest. The PegIFN-α that patients used in the study was neither PegIFN-α-2a (Pegasys; Roche, Shanghai, China) nor PegIFN-α-2b (PegBeron; Y shape, 40 kD, China).
Data Collection
During treatment, laboratory tests were assessed every four weeks, including quantitative HBsAg, HBeAg, anti-HBs, anti-HBe, HBV DNA, hematology, clinical chemistries, and routine blood tests. The HBV DNA levels were quantified by the real-time polymerase-chain reaction assay (TaqMan HBV assay, Roche Diagnostics; lower detection limit of 50 IU/mL and higher detection limit of 3×10^8 IU/mL). The serological markers of HBV were detected with enzyme-linked immune-sorbent assay kits (ARCHITECT I 2000; Abbott Architect, USA). The biological parameters were measured using a biochemistry analyzer (7600 Series; Hitachi, Tokyo, Japan). Adverse events (AEs) are continuously monitored.
Definition
Serological responses for HBsAg represented HBsAg loss and were defined as undetectable level (lower limit: 0.05 IU/mL) in serum. This research focused on HBsAg loss rate at 24 weeks and 48 weeks. HBeAg serological responses, indicating HBeAg loss (lower limit: 1.00 s/co), were also evaluated only in HBeAg-positive patients. Virological response was defined as undetectable HBV DNA (lower limit: 50 IU/mL). Biochemical responses were evaluated through the normalization of ALT levels, which were considered normal if within the range of 9–50 U/L for men and 7–40 U/L for women. Non-invasive biomarkers for fibrosis, such as the aspartate aminotransferase-to-platelet ratio index (APRI) and FIB-4 index were also included.
Statistical Analyses
The summary of the baseline variables of patients was done using frequencies and percentages for categorical variables and medians with interquartile ranges or mean values with standard deviations for continuous variables. The statistical analysis showed that baseline characteristics of the two groups were similar, so the follow-up analysis was conducted directly between them without propensity score matching. The rates of clinical outcomes were calculated and analyzed using the Chi-squared-test and Yates’ correction for continuity for categorical data, and the t-test for continuous variances. The Kaplan–Meier survival curves were used to determine the cumulative incidence for HBsAg loss, virological response, HBeAg loss, and ALT normalization. The Cox regression was used to examine the relationship between baseline characteristics and incidence rates of HBsAg loss, with results expressed as Hazard rate (HR), corresponding 95% confidence intervals and p values. P values were 2-sides, and the type I error was 5%. The statistical analysis and graphical display were performed using STATA software (release 7.0, Stata Corporation, College Station, TX) and R software (version 3.3.1; R Foundation for Statistical Computing, Vienna, Austria), with the packages “survminer”, “survival”, and “ggpubr” for calculating and plotting.
Results
Baseline Demographics and Clinical Characteristics
Two hundred eighty-seven patients received treatment with PegIFN-α between October 2016 and October 2021. After reviewing clinical records, 12 patients with HCC before were excluded. Among those patients, 119 patients received either PegIFN-α with TDF or TAF. After selection, five patients who did not finish 48 weeks of treatment were excluded, leaving 114 patients left (Supplementary Figure 1). Of the 114 patients, 33 patients (75.8% male, n=25) received 180ug PegIFN-α weekly with TAF 25mg daily, and 81 patients (79% male, n=64) received 180ug PegIFN-α weekly with TDF 300mg daily. The average age of patients in the TAF group was 39.15±9.00 years, while in the TDF group, it was 37.53±7.81 years. A 48.5% (16/33) patients in TAF plus PegIFN-α and 65.4% (53/81) patients in TDF plus PegIFN-α were HBeAg positive. Mean HBsAg was 2.59±1.30 log10 IU/mL in TAF group and 2.91±1.02 log10 IU/mL in the TDF group. Mean HBeAg for TAF and TDF group were 0.50±1.19 log10 s/co and 0.78±1.20 log10 s/co. HBV DNA was 1.58±2.3 log10 copies/mL in the TAF group and 1.19±2.55 log10 copies/mL in the TDF group. Baseline ALT was 53.48±51.99 U/L in TAF group and 68.22±85.74 U/L in TDF group. Baseline aspartate transaminase (AST) was 30.64±15.00 U/L in TAF group and 39.07±33.19 U/L in TDF group. There are 24 patients in the TAF group (72.7%) and 58 in the TDF group (71.6%) had received NA treatment before combination treatment. One patient in the TAF group (3.03%) and two patients in the TDF group (2.47%) had received Peg-IFNα-2b. The average time of NAs treatment before receiving combination treatment was 6.13±5.42 years in the TAF group and 5.34±3.79 years in the TDF group (p=0.45) (Table 1).
 |
Table 1 Demographic and Clinical Characteristics of the 114 Subjects at Baseline |
HBsAg Loss
Patients who received a combination of PegIFN-α and TAF had an HBsAg loss rate of 15.2% (5/33) at week 24 and 21.2% (7/33) at week 48 which was numerically higher compared to patients who received TDF and PegIFN-α with a rate of 7.4% (6/81) at week 24 and 12.3% (10/81) at week 48. However, this difference was not statistically significant (p=0.204 at week 24 and p=0.228 at week 48) (Figure 1A). In a subgroup analysis of HBeAg positive patients, the response rate was higher in the TAF group at 48 weeks with 18.8% (3/16) at 24 weeks and 25% (4/16) at 48 weeks, compared to 1.9% (1/53) at 24 weeks and 3.8% (2/53) at 48 weeks in the TDF group. The p-value at 24 weeks was 0.055, while p-value at 48 weeks was 0.033, which was significant (p<0.05) (Figure 1B). In the HBeAg-negative subgroup, the response rate was 11.8% (2/17) at 24 weeks and 17.6% (3/17) at 48 weeks in the TAF group, compared to 17.9% (5/28) at 24 weeks and 28.6% (8/28) at 48 weeks in the TDF group. The p-values were not significant at 24 weeks (0.902) and 48 weeks (0.639) (Figure 1C). The results showed a difference in response rate between the two subgroups, as shown in the forest (Supplementary Figure 2).
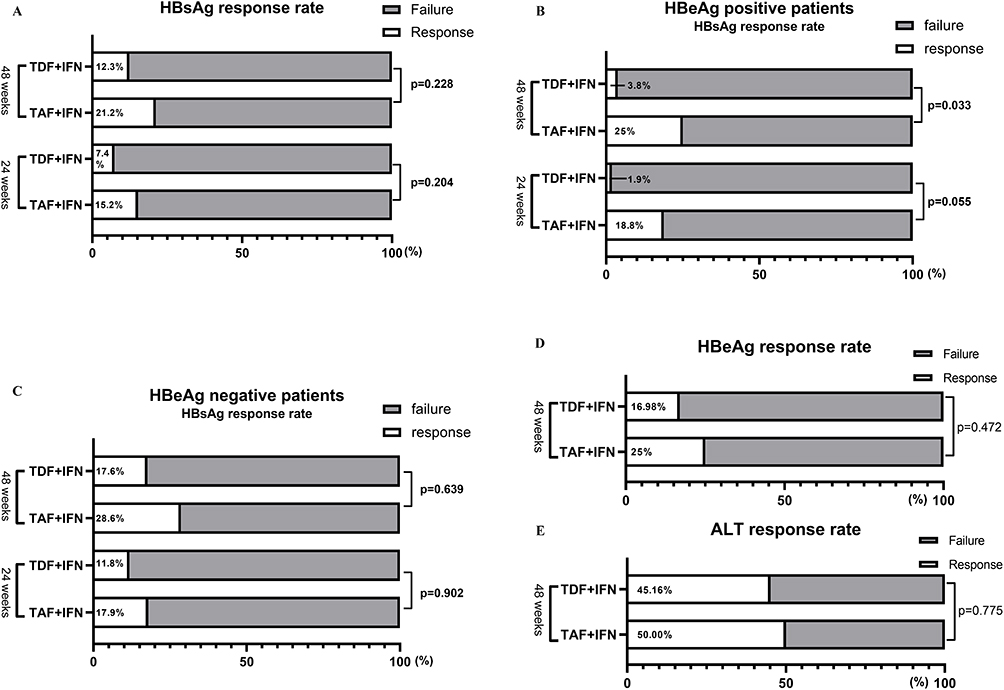 |
Figure 1 Comparison of response rates of PegIFN-α therapy combining in combination with TDF or TAF in chronic hepatitis B patients. (A) The HBsAg loss rate was 15.2% at week 24 and 21.2% at week 48 in TAF plus IFN group, compared to 7.4% at week 24 and 12.3% at week 48 in TDF plus IFN group (p=0.204 at week 24 and p=0.228 at week 48). (B) In HBeAg positive patients, the HBsAg loss rate was 18.8% at 24 weeks and 25% at 48 weeks in TAF group, compared to 1.9% at 24 weeks and 3.8% at 48 weeks in the TDF group (p=0.055 at week 24 and p=0.033 at week 48). (C) In HBeAg negative patients, the HBsAg loss rate was 11.8% at 24 weeks and 17.6% at 48 weeks in the TAF group, compared to 17.9% at 24 weeks and 28.6% at 48 weeks in the TDF group (p=0.902 at week 24 and p=0.639 at week 48). (D) The HBeAg loss rate in the TAF group was 25.00%, while it was 16.98% in the TDF group at 48 weeks (p = 0.472). (E) The ALT normalization rate at week 48 was 50% in the TAF group and 45.16% in the TDF group (p=0.775). |
Average HBsAg decline at week 48 was 0.83±1.31 log10 IU/mL for the TAF group and 1.00±1.38 log10 IU/mL for the TDF group (p=0.54) (Figure 2) (HBsAg reaching 0 were treated as 0.01 for logarithmic transformation). The average HBsAg decline at 24 week was 0.58±1.07 log10 IU/mL for the TAF group and 0.66±1.03 log10 IU/mL for the TDF group with no significant difference (p=0.69) (Table 2). The average HBsAg loss times was 23.43±9.07 weeks for the TAF plus PegIFN-α group and 24.8±11.12 weeks for the TDF plus PegIFN-α group with no significant difference (p= 0.79). The cumulative incidence of HBsAg loss calculated from Kaplan–Meier curves showed no difference between the two groups (p=0.22) (Figure 3B). A total of 10 patients in the TDF group and 6 in the TAF group who had achieved HBsAg loss were treated with NA before combination therapy. The average duration of NA treatment was 3.6±0.82 years for the TDF group and 5.43±2.0 years for the TAF group (p=0.36).
 |
Table 2 Clinical Treatment Outcomes of Two Groups |
 |
Figure 2 HBsAg decline changes between two groups. (A) The average HBsAg decline at 24 week was 0.58±1.07 log10 IU/mL for the TAF group and 0.66±1.03 log10 IU/mL for the TDF group (p=0.69). (B) Average HBsAg decline at week 48 were 0.83±1.31 log10 IU/mL for the TAF group and 1.00±1.38 log10 IU/mL for the TDF group (p=0.54). |
 |
Figure 3 Kaplan–Meier analysis comparing the cumulative incidence of response rates between two groups. (A) The cumulative incidence of HBV DNA loss, calculated from Kaplan Meier curves, showed p value of 0.013 between the two groups. (B) The cumulative incidence of HBsAg loss, calculated from Kaplan Meier curves, showed p value of 0.22 between the two groups. (C) The cumulative incidence of HBeAg loss, calculated from Kaplan Meier curves, showed p value of 0.41 between the two groups. (D) The cumulative incidence of ALT normalization, calculated from Kaplan Meier curves, showed p value of 0.55 between the two groups. |
Virological Response
Initially, 28 patients had HBV DNA above the detection threshold (12 in TAF plus PegIFN-α group and 16 in TDF plus PegIFN-α group). At baseline, the DNA level of those patients was 1.58±2.3 log10 copies/mL for the TAF group and 1.19±2.55 log10 copies/mL for the TDF group (P=0.451) (Table 2). After 48 weeks of treatment, all serum HBV DNA of those patients became undetectable. The average time for patients in the TAF group to achieve virological response was 9 ± 8.16 weeks, which is less than the time for patients in the TDF group: 18.13 ± 11.71 (p=0.0293 < 0.05). Kaplan–Meier analysis indicated that the cumulative incidence rates of DNA loss were different between the two groups. Patients in TAF group achieved virological response easier than in the TDF group (p=0.013) (Figure 3A).
HBeAg Serological Response
A total of 69 patients were HBeAg positive in two groups (16 in TAF plus PegIFN-α group and 53 in TDF plus PegIFN-α group). The HBeAg serological response rate in the TAF group was 25.00% (4/16), while in the TDF group it was 16.98% (9/53). There was no statistically significant difference between the two groups (p = 0.472) (Figure 1D). The average HBeAg decline in week 48 was 112.60±179.99 s/co for TAF group and 232.06±445.56 s/co for TDF group (p=0.30). HBeAg serological response time in TAF group was 15.00±8.25 weeks and 28.44±14.48 weeks in TDF group (p=0.12) (Table 2). Kaplan–Meier analysis indicated no statistical difference in the cumulative incidence rate of HBeAg serological response between the two groups (p=0.41) (Figure 3C).
Biochemical Response
Out of the total number of patients, 43 had initially ALT levels above the upper limit (12 in the TAF plus PegIFN-α group and 31 in the TDF plus PegIFN-α group). The ALT normalization rate at week 48 was 50% (6/12) in the TAF group and 45.16% (14/31) in the TDF group. However, the rate was not statistically significant (p=0.775) (Figure 1E). The average ALT normalization time was 13.33±13.78 weeks for the TAF group and 25.71±13.74 weeks for the TDF group (Table 2). The P-value of normalization time was 0.082. However, the one-tailed P-value was 0.041< 0.05. Kaplan–Meier analysis indicated no statistical difference in the cumulative incidence rate of HBeAg serological response between the two groups (p=0.55) (Figure 3D).
Cox Regression Analysis
When considering factors such as sex, age, drug, HBsAg, HBeAg positive, HBeAg level, DNA, ALT level, AST level, NA treatment before, and IFN treatment before, univariate Cox regression analysis showed that HBeAg positive (p-value=0.028) and HBsAg level (p-value=0.001) before treatment were associated with HBsAg loss. The results are shown in Table 3. In multivariable Cox regression, which take sex, age, HBeAg positive and HBsAg into account, it was revealed that age and HBsAg level before treatment were associated with HBsAg response. The P-value was 0.02 for age and 00.001 for HBsAg. In multivariable Cox regression, HR was 0.996 (95% CI: 0.994 0.998) for HBsAg level before treatment.
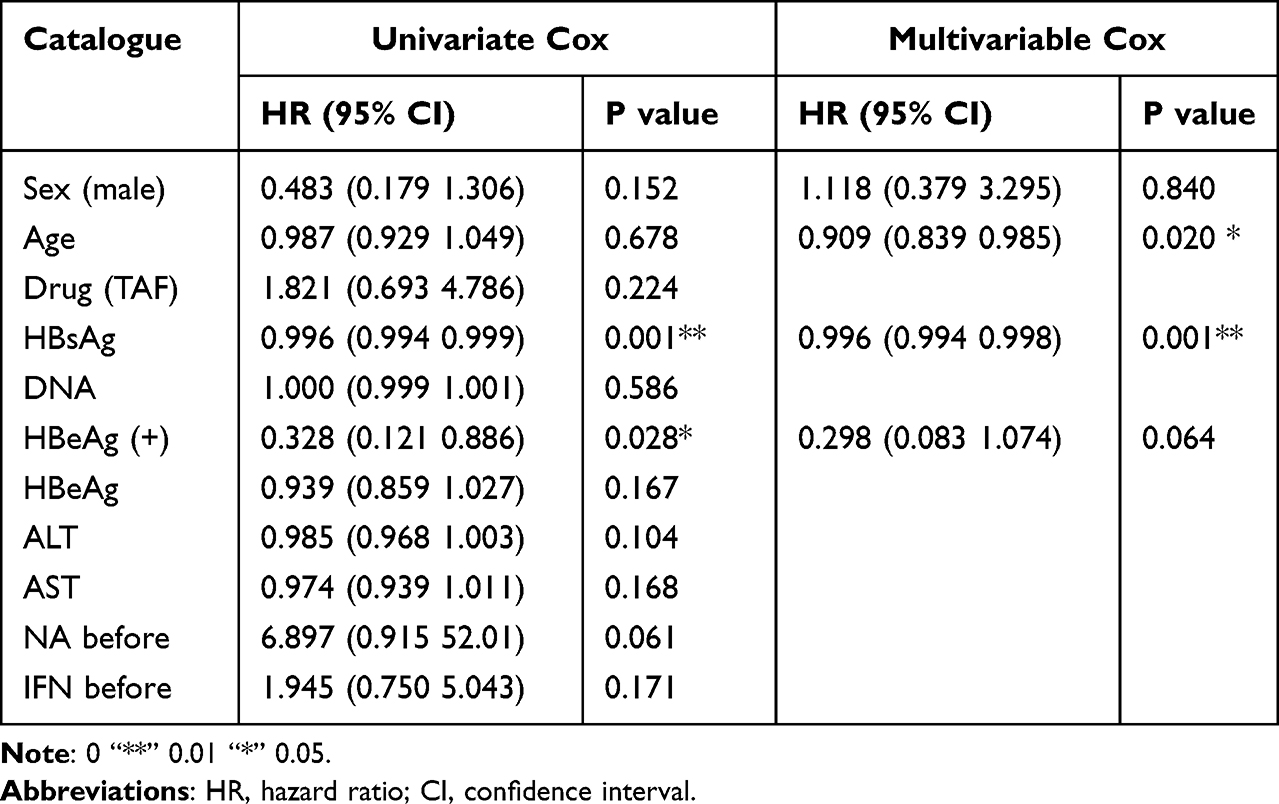 |
Table 3 Univariate and Stepwise Multivariable Cox Hazard Analysis |
Adverse Events and Changes in Renal Function
The changes in serum levels of AST, ALT, ALP, γ-GGT, RBC, WBC, PLT, NEU%, APRI, and FIB4 are demonstrated in Figure 4 and Supplementary Figure 3. There were no statistical differences between the two groups (Supplementary Table 1). Throughout the treatment, no patients in either group experienced thrombocytopenia (<50E+09/L), but two patients in TDF group suffered from neutropenia (<1.0E+06/L). The majority of patients experienced reductions in the number of neutrophils and platelet cells. Flu-like syndrome (48.5% vs 50.6%), myalgia (30.3% vs 28.4%), headache (36.4% vs 37.0%), fatigue (33.3% vs 39.5%), rash (3.0% vs 3.7%) weight loss (18.2% vs 14.8%) and local reactions at the site of injection (9.1% vs 8.6%) were the most frequently reported side effects. However, the rates showed no statistical difference between the two groups. None of the groups had any evidence of hepatic decompensation or a severe acute exacerbation of chronic HBV infection characterized by ALT levels of >10×ULN or total bilirubin levels of >51 μmol/L. All symptoms were effectively managed with temporary dose reduction.
 |
Figure 4 Liver function changes during treatment. (A) The changes in serum levels of ALT between two groups. (B) The changes in serum levels of AST between two groups. (C) The changes in serum levels of ALP between two groups. (D) The changes in serum levels of γ-GGT between two groups. (E) The changes in serum levels of APRI between two groups. (F) The changes in serum levels of FIB4 between two groups. |
No difference was observed in the changes of creatinine, urea, and eGFR levels between the two groups after 48 weeks of treatment (Table 3). Compared with patients receiving TDF plus IFN treatment, patients who had TAF plus IFN treatment showed a numerical decline in serum creatinine (−6.00±6.87 vs −2.58±8.96 μmol/L), a decline in serum urea level instead of an increase (−0.06±1.068 vs 0.07±0.95 mmol/L), and a minor eGFR increase (10.64±15.02 vs 13.46±15.96 mL/min) after 48 weeks treatment (Figure 5). A one-tailed P-value of the hypothesis that the decline in creatinine in the TAF group was more than in the TDF group was 0.034< 0.05.
 |
Figure 5 Baseline renal function and changes in two groups (A) Serum levels of creatinine, urea, and eGFR at 24 and 48 weeks in TAF and TDF groups. (B) Changes of serum levels of creatinine, urea, and eGFR between TAF and TDF groups. |
Discussion
Most patients infected with hepatitis B virus require lifelong therapy, which can be a significant burden both financially and in their daily lives. Combining NAs with IFN therapy may be a better treatment option for HBeAg positive and negative patients with a higher rate of HBsAg, HBeAg loss, and virological response compared to NAs or IFN monotherapy.21,22 In previous studies, the HBsAg loss rate was reported to be 6.5–13% in patients receiving NAs combined with PegIFN-α therapy.8,10,23 However, selecting which NA to use in clinical practice can be confusing. TAF and TDF are both initially metabolized to TFV in the plasma, which is metabolized in target viral-infected cells to the active metabolite tenofovir-diphosphate (TFV-DP).24 In monotherapy, TAF was found to be non-inferior to TDF for the primary outcome (HBsAg loss) in treatment of CHB and had better renal and bone profiles for patients.14,25 Whether combining TAF with PegIFN-α can lead to better immune modulation is still under investigation. In our study, the TAF plus PegIFN-α group had an HBsAg loss of 15.2% in 24 weeks and 21.1% at 48 weeks, while the TDF plus PegIFN-α group had rates of 7.4% at 24 weeks and 12.3% at 48 weeks. Although the result was numerically higher in the TAF plus PegIFN-α group, there was no statistical difference (p=0.204 at 24 weeks, p=0.228 at 48 weeks). In HBeAg-positive patients, the HBsAg loss rate was 25% at 48 weeks in the TAF combining PegIFN-α group, while it was only 3.8% in the TDF plus PegIFN-α group (P=0.033), indicating that TAF plus IFN treatment may be a better treatment option for HBeAg-positive patients than TDF plus IFN treatment. This rate is also higher than that of IFN monotherapy for HBeAg-positive patients reported before.26 However, as this is a subgroup analysis, which is typically usually used to assess internal trial consistency or to make exploratory distinctions for unusual or unexpected outcomes, this conclusion is not enough convincing. Subgroup forest plot showed that HBeAg negative and positive patients showed different treatment outcomes. Independent studies are needed to assess the treatment efficacy of TAF plus IFN on HBeAg positive patients. Four HBeAg-positive patients achieved HBsAg loss in TAF plus PegIFN-α group, but two of them did not achieve HBeAg loss (1 achieved HBeAb seroconversion). This phenomenon is also reported in other studies investigating the efficacy of IFN on HBeAg-positive patients.27,28 HBeAg positivity/HBsAg negativity in the serological profile compresses an atypical pattern, which may be due to changes in the tertiary structure of determinant “a” of HBsAg, making the binding of neutralizing antibodies targeted to the wild-type virus and detection of HBsAg for diagnosis difficult.29 Further testing using highly sensitive HBV DNA assays may be required to investigate the possibility of low-level virus replication in these patients. Another possible explanation may be the integration of HBV DNA into the liver genome.30 The decline in HBsAg was numerically lower in TAF plus PegIFN-α group compared to TDF plus PegIFN-α group. This is consistent with 96 weeks’ treatment outcomes of TAF monotherapy compared to TDF monotherapy, which showed a numerically higher HBsAg seroconversion rate and lower HBsAg changes.14 Our study found quicker virological response in TAF combining the PegIFN-α group, possibly due to a longer plasma half-life of TAF and its ability to efficiently be introduced to hepatocytes and peripheral blood mononuclear cells, leading to consistent virus restriction.31 Additionally, PegIFN-α may have a better immune modulation function.32 Sustained virological response after PegIFN-α is typically associated with remission of the liver disease,4 which make the TAF plus PegIFN-α a regimen potentially beneficial for patients with liver fibrosis. HBeAg serological response rates were similar between the two groups. ALT normalization rate also showed no statistical difference. However, PegIFN-α treatment is commonly associated with ALT flare, which may diminish the positive role of TAF.
PegIFN-α therapy is associated with considerable side effects. In our study, no patients in either group reported severe side effects. During patient enrollment, those who did not complete 48 weeks of treatment were excluded. They were likely to withdraw from treatment due to unwillingness to tolerate side effects. Most patients’ side effects would mitigate after reducing the dose of PegIFN-α, so timely close observation in the hospital and dose adjustment is necessary. Patients who wish to undergo domestic PegIFN-α therapy in other studies should pay close attention to side effects and undergo regular laboratory testing in the hospital. The renal function between the two groups showed no statistical difference. However, our observation time was only 48 weeks, which may not be long enough to observe renal function differences. Unfortunately, we were unable to conduct a bone marrow analysis in our study.
Our study had several limitations. Firstly, the small sample size reduced the power of our research. In China, TAF was significantly more expensive than TDF, resulting in fewer patients choosing TAF as their primary NA treatment option. Consequently, we were unable to achieve a 1:1 ratio between the TAF and TDF groups during retrospective data collection. Secondly, our study was retrospective in nature, which meant that we were unable to follow the principles of randomized control principle. The mixing of confounding factors at baseline further complicated our results and made them less straightforward and persuasive. As a result, the credibility of our study was statistically lower than that of prospective randomized controlled trials. Thirdly, many patients in our study had received NA treatment before enrollment, making combination treatment more like an add-on therapy. However, with declining treatment standards and the wider availability of vaccines, fewer patients will be treated for the first time. Nonetheless, add-on therapy has shown promising results in significantly reducing HBV DNA and HBsAg levels.33 Despite these limitations, our study is the first to report the effectiveness and safety of TAF combined with PegIFN-αa therapy for CHB patients compared to the widely adopted TDF combined with PegIFN-α therapy in China. Our results indicate that TAF combined with IFN therapy is effective and can lead to serological cure in some CHB patients.
There are still several unresolved issues regarding the use of PegIFN-α in combination with NAs for treating CHB. The first issue is which treatment to choose. In addition to simple combination treatment, “add-on” or the “switch” to PegIFN-α in patients on long-term NA treatment also showed improved HBsAg kinetics in CHB patients34 Secondly, more biological and clinical markers need to be studied to select the patients who would benefit most from NAs plus PegIFN-α therapy.35–37 According to COX regression analysis, those with low HBsAg would benefit most from the NAs plus PegIFN-α treatment. Thirdly, most CHB patients in Europe and America belong to gene types A and D, while most CHB patients in Asia belong to gene types B and C. Whether there could be differences in treatment efficacy remains unknown.38,39 Further prospective double-blinded studies, long-term and real-world studies are needed to gain a comprehensive understanding of the effects of TAF-combined PegIFN-α treatment for both HBeAg positive and negative CHB patients.
Conclusion
The combination of TAF and PegIFN-α treatment results in better HBsAg loss in HBeAg-positive patients and quicker virological response, as compared to the TDF plus PegIFN-α group. The TAF plus PegIFN-α treatment regimen is recommended for CHB patients who aim to achieve a functional cure, particularly those who are not eligible for TDF treatment.
Acknowledgments
Our study complies with the Declaration of Helsinki.
Funding
The present study was supported by grants from the National Natural Science Foundation of China (81871640, 82172255) and Shanghai Shen Kang Hospital Development Center (No. SHDC12019116), and Shanghai Key Clinical Specialty Construction Program (ZK2019B24).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Razavi-Shearer D, Gamkrelidze I, Nguyen MH, Chen D. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol. 2018;3(6):383–403. doi:10.1016/S2468-1253(18)30056-6
2. Lampertico P, Agarwal K, Berg T, et al. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–398. doi:10.1016/j.jhep.2017.03.021
3. Kim SU, Seo YS, Lee HA, et al. A multicenter study of entecavir vs. tenofovir on prognosis of treatment-naive chronic hepatitis B in South Korea. J Hepatol. 2019;71(3):456–464. doi:10.1016/J.JHEP.2019.03.028
4. Buster EHCJ, Hansen BE, Buti M, et al. Peginterferon alpha-2b is safe and effective in HBeAg-positive chronic hepatitis B patients with advanced fibrosis. Hepatology. 2007;46(2):388–394. doi:10.1002/HEP.21723
5. Wursthorn K, Lutgehetmann M, Dandri M, et al. Peginterferon alpha-2b plus Adefovir induce strong cccDNA decline and HBsAg reduction in patients with chronic hepatitis B. Hepatology. 2006:675–684. doi:10.1002/hep.21282
6. Cheng J, Wang Y, Hou J, et al. Peginterferon alfa-2b in the treatment of Chinese patients with HBeAg-positive chronic hepatitis B: a randomized trial. J Clin Virol. 2014;61(4):509–516. doi:10.1016/j.jcv.2014.08.008
7. Chon YE, Kim DJ, Kim SG, et al. An observational, multicenter, cohort study evaluating the antiviral efficacy and safety in Korean patients with chronic hepatitis B receiving pegylated interferon-Alpha 2a (Pegasys). Medicine. 2016;95(14):e3026. doi:10.1097/MD.0000000000003026
8. Zheng C, Yan H, Zeng J, Cai S, Wu X. Comparison of pegylated interferon monotherapy and de novo pegylated interferon plus tenofovir combination therapy in patients with chronic hepatitis B. Infect Drug Resist. 2019;12:845–854. doi:10.2147/IDR.S195144
9. Hu C, Song Y, Tang C, et al. Effect of pegylated interferon plus tenofovir combination on higher hepatitis B surface antigen loss in treatment-naive patients with hepatitis B e antigen -positive chronic hepatitis B: a real-world experience. Clin Ther. 2021;43(3):572–581.e3. doi:10.1016/j.clinthera.2020.12.022
10. Ahn SH, Marcellin P, Ma X, et al. Hepatitis B surface antigen loss with tenofovir disoproxil fumarate plus peginterferon Alfa-2a: week 120 analysis. Dig Dis Sci. 2018;63(12):3487–3497. doi:10.1007/s10620-018-5251-9
11. Patrick M, Sang Hoon A, Xiaoli M, et al. Combination of tenofovir disoproxil fumarate and peginterferon α-2a increases loss of hepatitis B surface antigen in patients with chronic hepatitis B. Gastroenterology. 2016;150(1):134–144.e10. doi:10.1053/j.gastro.2015.09.043
12. Tenney DJ, Rose RE, Baldick CJ, et al. Long-term monitoring shows hepatitis B virus resistance to entecavir in nucleoside-naive patients is rare through 5 years of therapy. Hepatology. 2009;49(5):1503–1514. doi:10.1002/HEP.22841
13. Tsai HJ, Chuang YW, Yang SS, Chang YZ, Chang HR, Lee TY. Evaluating the renal safety of tenofovir disoproxil fumarate in hepatitis B patients without chronic kidney disease. J Viral Hepat. 2021;28(11):1579–1586. doi:10.1111/JVH.13603
14. Agarwal K, Brunetto M, Seto WK, et al. 96 weeks treatment of tenofovir alafenamide vs. tenofovir disoproxil fumarate for hepatitis B virus infection. J Hepatol. 2018;68(4):672–681. doi:10.1016/j.jhep.2017.11.039
15. Farag MS, Fung S, Tam E, et al. Effectiveness and renal safety of tenofovir alafenamide fumarate among chronic hepatitis B patients: real-world study. J Viral Hepat. 2021;28(6):942–950. doi:10.1111/jvh.13500
16. Hamzah L, Williams D, Bailey AC, et al. Early safety of tenofovir alafenamide in patients with a history of tubulopathy on tenofovir disoproxil fumarate: a randomized controlled clinical trial. HIV Med. 2020;21(3):198–203. doi:10.1111/hiv.12819
17. Hou J, Ning Q, Duan Z, et al. 3-year treatment of tenofovir alafenamide. Tenofovir disoproxil fumarate for chronic HBV infection in China. J Clin Transl Hepatol. 2021;9(3):324–334. doi:10.14218/JCTH.2020.00145
18. Uchida Y, Nakao M, Yamada S, et al. Superiority of tenofovir alafenamide fumarate over entecavir for serum HBsAg level reduction in patients with chronic HBV infection: a 144-week outcome study after switching of the nucleos(t)ide analog. PLoS One. 2022;17(2):e0262764. doi:10.1371/journal.pone.0262764
19. Tian F, Houle SKD, Alsabbagh MW, Wong WWL. Cost-effectiveness of tenofovir alafenamide for treatment of chronic hepatitis B in Canada. Pharmacoeconomics. 2020;38(2):181–192. doi:10.1007/s40273-019-00852-y
20. Chinese Society of Infectious Diseases CMA, Chinese Society of Hepatology CMA. The guidelines of prevention and treatment for chronic hepatitis B (2019 version). Zhonghua Gan Zang Bing Za Zhi. 2019;27(12):938–961. doi:10.3760/cma.j.issn.1007-3418.2019.12.007
21. Liu J, Wang T, Zhang W, Cheng Y, He Q, Wang FS. Effect of combination treatment based on interferon and nucleos(t)ide analogues on functional cure of chronic hepatitis B: a systematic review and meta-analysis. Hepatol Int. 2020;14(6):958–972. doi:10.1007/s12072-020-10099-x
22. Wei W, Wu Q, Zhou J, Kong Y, You H. A better antiviral efficacy found in nucleos(t)ide analog (NA) combinations with interferon therapy than NA monotherapy for HBeag positive chronic hepatitis B: a meta-analysis. Int J Environ Res Public Health. 2015;12(8):10039–10055. doi:10.3390/ijerph120810039
23. Marcellin P, Ahn SH, Chuang WL, et al. Predictors of response to tenofovir disoproxil fumarate plus peginterferon alfa-2a combination therapy for chronic hepatitis B. Aliment Pharmacol Ther. 2016;44(9):957–966. doi:10.1111/apt.13779
24. Buti M, Riveiro-Barciela M, Esteban R. Tenofovir alafenamide fumarate: a new tenofovir prodrug for the treatment of chronic hepatitis B infection. J Infect Dis. 2017;216(suppl_8):S792–S796. doi:10.1093/INFDIS/JIX135
25. Byun KS, Choi J, Kim JH, et al. Tenofovir alafenamide for drug-resistant hepatitis B: a randomized trial for switching from tenofovir disoproxil fumarate. Clin Gastroenterol Hepatol. 2021;20(2):427–437.e5. doi:10.1016/j.cgh.2021.04.045
26. Li M, Zhang L, Xie S, et al. Dynamic changes of cytokine profiles and virological markers associated with HBsAg loss during peginterferon Alpha-2a treatment in HBeAg-positive chronic hepatitis B patients. Front Immunol. 2022;13:892031. doi:10.3389/fimmu.2022.892031
27. Wu FP, Wang YK, Li YP, et al. Clinical analysis of four cases of HBsAg seroconversion in patients with HBeAg-positive chronic hepatitis B after receiving interferon alpha therapy. Zhonghua Gan Zang Bing Za Zhi. 2021;29(6):580–582. doi:10.3760/cma.j.cn501113-20200318-00123
28. Rosenthal P, Ling SC, Belle SH, et al. Combination of entecavir/peginterferon Alfa-2a in children with hepatitis B e antigen-positive immune tolerant chronic hepatitis B virus infection. Hepatology. 2019;69(6):2326–2337. doi:10.1002/HEP.30312
29. Pondé RAA. Atypical serological profiles in hepatitis B virus infection. Eur J Clin Microbiol Infect Dis. 2013;32(4):461–476. doi:10.1007/s10096-012-1781-9
30. Mathkar PP, Chen X, Sulovari A, Li D. Characterization of hepatitis B virus integrations identified in hepatocellular carcinoma genomes. Viruses. 2021;13(2). doi:10.3390/v13020245
31. Podany AT, Bares SH, Havens J, et al. Plasma and intracellular pharmacokinetics of tenofovir in patients switched from tenofovir disoproxil fumarate to tenofovir alafenamide. AIDS. 2018;32(6):761–765. doi:10.1097/QAD.0000000000001744
32. Kuipery A. Immunomodulation and RNA interference alter hepatitis B virus-specific CD8 T-cell recognition of infected HepG2-NTCP. Hepatology. 2021. doi:10.1002/HEP.32230
33. Matsumoto A, Nishiguchi S, Enomoto H, et al. Pilot study of tenofovir disoproxil fumarate and pegylated interferon-alpha 2a add-on therapy in Japanese patients with chronic hepatitis B. J Gastroenterol. 2020;55(10):977–989. doi:10.1007/s00535-020-01707-6
34. Yan L, Zhu C, Li J, et al. Entecavir add-on or switch-to pegylated interferon improves HBsAg clearance in HBe antigen negative chronic hepatitis B patients. Infect Drug Resist. 2018;11:2001–2009. doi:10.2147/IDR.S175707
35. Li M, Zhang L, Lu Y, et al. Early serum HBsAg kinetics as predictor of HBsAg loss in patients with HBeAg-negative chronic hepatitis B after treatment with pegylated interferonα-2a. Virol Sin. 2021;36(2):311–320. doi:10.1007/s12250-020-00290-7
36. De Ridder F, Sonneveld MJ, Lenz O, Janssen HLA, Talloen W, Hansen BE. Mean HBsAg decline at week 24 of PEG-IFN-based treatment predicts subsequent rate of HBsAg clearance — suggesting a valuable endpoint for early development HBV trials. J Viral Hepat. 2021;28(11):1563–1569. doi:10.1111/jvh.13599
37. Hou FQ, Song LW, Yuan Q, et al. Quantitative hepatitis B core antibody level is a new predictor for treatment response in HBeAg-positive chronic hepatitis B patients receiving peginterferon. Theranostics. 2015;5(3):218–226. doi:10.7150/thno.10636
38. Masaki K, Suzuki F, Hara T, et al. Long-term effects of peginterferon alfa-2a therapy in Japanese patients with chronic hepatitis B virus infection. Virol J. 2015;12(1). doi:10.1186/s12985-015-0453-7
39. Seo Y, Yano Y. Short- and long-term outcome of interferon therapy for chronic hepatitis B infection. World J Gastroenterol. 2014;13284–13292. doi:10.3748/wjg.v20.i37.13284
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.