")
Back to Journals » Journal of Pain Research » Volume 16
Comparison of Edge of Lamina Block with Thoracic Paravertebral Block and Retrolaminar Block for Analgesic Efficacy in Adult Patients Undergoing Video-Assisted Thoracic Surgery: A Prospective Randomized Study
Authors Gao X, Chen M, Liu P, Zhou S, Kong S, Zhang J, Cao J
Received 9 March 2023
Accepted for publication 9 June 2023
Published 13 July 2023 Volume 2023:16 Pages 2375—2382
DOI https://doi.org/10.2147/JPR.S409721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ellen M Soffin
Xiaoyun Gao,* Moxi Chen,* Penghao Liu, Shenyuan Zhou, Sai Kong, Junfeng Zhang, Jun Cao
Department of Anesthesiology, Shanghai Sixth People’s Hospital, Shanghai, 200233, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Cao, Department of Anesthesiology, Shanghai Sixth People’s Hospital, No. 600, Yishan Road, Shanghai, 200233, People’s Republic of China, Tel +86 18930173661, Email [email protected]
Background: A novel ultrasound-guided paravertebral block, the edge laminar block (ELB) was reported recently. However, it was unclear how effective ELB was in comparison with traditional blocking methods. We conducted a trial to compare the analgesic efficacy of ELB with the thoracic paravertebral block (TPVB) and the retrolaminar block (RLB) in patients undergoing video-assisted thoracic surgery (VATS).
Methods: We identified 90 patients who were scheduled for VATS and randomly assigned them to three groups: ELB group (Group E), TPVB group (Group T), and RLB group (Group R). Each group underwent ELB, TPVB, and RLB, respectively, under ultrasound guidance before general anesthesia induction. All patients received post-operative routine analgesia protocol. Our primary outcome was the extent of dermatomal sensory loss on the midclavicular, midaxillary, and scapular lines, measured using a pinprick 15 minutes after the nerve block. Secondary outcomes included the intraoperative dose of sufentanil, the numerical rating scale (NRS) scores assessed in the post-anesthesia care unit (PACU) and at 6, 12, and 24 hours post-operatively, and pethidine administrated as analgesic rescue dose.
Results: The percentages of nerve block range reaching the midclavicular line, midaxillary line, and scapular line in Group E were 96.7%, 93.3%, 93.3%, and 60% in Group T and 30%, 56.7%, and 96.7% in Group R, respectively. Group E had wider dermatomal sensory loss on the midclavicular line and midaxillary line compared to Group R (P < 0.001) and had a wider range compared to Group T on the scapular line (P < 0.001). There was no significant difference in the intraoperative use of sufentanil in the three groups. Post-operative NRS scores at each time point were significantly lower in Group E than those in the other two groups (P < 0.01).
Conclusion: ELB had a wider nerve block range and applied better post-operative analgesia in comparison with TPVB and RLB.
Keywords: analgesia, retrolaminar block, thoracic paravertebral block, ultrasound guidance, video-assisted thoracic surgery
Background
Thoracic paravertebral block (TPVB) can provide effective perioperative analgesia and is currently used extensively in thoracic surgery as part of the enhanced recovery after surgery (ERAS) protocol.1,2 However, complications such as pneumothorax and nerve or vessel injury cannot be completely avoided.3 As an alternative to TPVB, interfascial plane block, including erector spinae plane block (ESPB) and RLB, has no risk of injection-induced injury and has also become commonly used analgesic method in chest surgery,4–7 but its analgesic effect is inferior to that of TPVB.4
ELB had sufficient analgesic effect in the internal fixation of rib fractures.8 As we previously reported, in the ultrasound-guided laminar block the puncture needle was advanced by in-plane approach until the needle tip touched the lateral edge of “lamina’s cliff” with some resistance. The hypoechoic local anesthetics diffused to both sides (up and down to the lamina’s cliff) around the injection point. This is the reason why this new approach is called ELB. ESPB, which is an interfascial block procedure, has the similar puncture sites with RLB. However, several studies have reported that the blocking effect of ESPB is not ideal for RLB, which has been concluded in a study that ESPB is equivalent, and not superior, to RLB for postoperative analgesia.9,10 Hence, ESPB was not considered in this trial.
To evaluate the effectiveness of ELB in video-assisted thoracic surgery, more information is needed. Besides, as a new approach to therapeutic lamina block, there is no comparative study between it and traditional blocking methods. Therefore, this study was designed to fill the gaps by comparing the ELB with TPVB and RLB for analgesic efficacy in adult patients undergoing video-assisted thoracic surgery.
Materials and Methods
Study Participants
This double-blinded, prospective, randomized controlled trial was approved by the Ethics Committee of Shanghai Sixth People’s Hospital (2021–005) and registered at www.chictr.org.cn (ChiCTR2000040053). Written informed consent was obtained from each participant. Meanwhile, this study had been conducted in compliance with the current version of the Declaration of Helsinki. The trial began on February 5, 2021, and ended on October 29, 2021. We enrolled 90 patients who underwent VATS, aged 18–80 years, with American Society of Anesthesiologists (ASA) physical status I and II. The exclusion criteria were as follows: 1. Presence of local infection, 2. Neuropathy of spinal cord or trunk nerve, 3. Coagulation dysfunction, 4. Allergy to anesthetic drugs. Patients shifted to open thoracic surgery were also excluded.
Procedures
We randomly assigned each individual to Group E, Group T, or Group R in a 1:1:1 ratio, and the assigned group was concealed in an opaque, sealed envelope. Each envelope was opened only by the medical personnel who performed the nerve block procedure. All patients, operating room anesthetists, staff who did the postoperative NRS follow-up, and statisticians were blinded to the group allocation.
After the patients were admitted into an operating room, upper-limb blood pressure, pulse oxygen saturation, and electrocardiography were regularly monitored.
All three nerve blockades were performed using the S-Nerve™ Ultrasound System (Fujifilm SonoSite Inc. Bothell, WA, USA) with a convex-array probe (5–2 MHz; C60x; Fujifilm SonoSite Inc. Bothell, WA, USA). The patients were asked to lie in a lateral decubitus position (with the affected side up). Each patient was injected with 20 mL of 0.375% ropivacaine after negative aspiration using in-plane approach. In Group E, the low-frequency convex transducer was placed in a transverse position at the sixth vertebral level, ensuring that the spinous process, vertebral lamina (VL), and transverse process (TP) were visible on one screen. We rotated the probe 30–45 degrees, keeping VL and TP of the sixth thoracic vertebral in view, and moved the probe caudally until the hyperechoic line of TP diminished. Thus, the lateral edge of the laminar arcus was silhouetted.8 Local analgesic (LA) was injected at the edge of the lamina. In Group T, we injected the LA into the sixth thoracic paravertebral space (TPVS) through the paralaminar in-plane approach described by Taketa.11 In Group R, the LA was injected on the surface of the sixth thoracic lamina through the RLB approach. The ultrasound images and demonstration figure were showed in Figure 1.
 |
Figure 1 Ultrasound-guided images and demonstration figure. (A) The image of TPVB. (B) The image of RLB. (C) The image of ELB. (D) The demonstration figure. Triangles indicate the needle; Arrow (black and white) and cross signs indicate the injection sites. Abbreviations: PP, Parietal Pleura; VL, Vertebral Lamina; TP, Transverse Process; SP, Spinae Process; IIM-SCTL, Internal Intercostal Membrane, and Superior Costotransverse Ligament. |
The patients remained resting for 15 min after the nerve block procedure and were sent into the operating room. Each patient’s loss of pinprick sensation was evaluated by an anesthesiologist in the room. The dermatomal sensory loss on the midclavicular line, midaxillary line, and scapular line were recorded.
Anesthesia was induced with intravenous injection of 2 mg/kg propofol, 0.4 μg/kg sufentanil, 0.6 mg/kg rocuronium, and maintained with sevoflurane at 0.7–1.2 age-adjusted minimum alveolar concentration (MAC). Sufentanil administered intermittently maintained the blood pressure within 20% of the baseline value. At the end of the surgery, sevoflurane inhalation was withdrawn and 50 mg of flurbiprofen was administered. All patients received a controlled intravenous analgesia pump (PCA, 100 mL, infusion rate 2 mL/h) consisting of tramadol 500 mg + lornoxicam 16 mg with no initial infusion dose. A dosage of 50 mg of flurbiprofen was infused twice a day. If the patient’s NRS was more than 4, an additional intramuscular injection of 50 mg pethidine was given as an analgesic rescue.
Outcomes and Data Collection
Primary outcomes
The dermatomal sensory loss on the midclavicular line, midaxillary line, and scapular line were measured with a pinprick.
Secondary outcomes included:
- Dosages of sufentanil.
- NRS pain scores assessed at PACU (T0), 6 (T1), 12 (T2), and 24 (T3) hours after surgery.
- Pethidine dose administrated as analgesic rescue.
- Complications related to the nerve block procedure such as nerve or vessel injuries.
Sample Size
The sample size was calculated based on the ratio of blockade range at the midclavicular line with PASS 11.0 (NCSS, LLC, Kaysville, USA). According to our pilot study, the ratios were 80%, 80%, and 40% in ELB, TPVB, and RLB, respectively. A total of 23 cases in each group were required to achieve 80% power with an α-value of 0.05. Taking into consideration a potential dropout rate of 15%, we aimed to enroll 30 patients in each group in this trial.
Statistical Analysis
We used the Shapiro–Wilk test to check for data normality and Levene’s test to verify the homogeneity of variance. Normally distributed data were expressed as mean ± standard deviation. Student’s t-test was used for intergroup comparisons, and data in multiple groups were compared with analysis of variance (ANOVA). Non-normally distributed data were represented as median (interquartile range), and comparisons between groups were assessed by the Mann-Whitney U-test or Kruskal–Wallis H-test. Categorical variables were described as numbers (%) and analyzed using the Chi-square test or Fisher’s exact test. P < 0.05 was considered as the significance level. All statistical analyses were performed using SPSS 26.0 software.
Results
A total of 90 patients were enrolled in this study. As no one was shifted to open thoracic surgery, all patients were included in the final study and there were 30 patients in each of the groups E, T, and R. A flow chart of patient recruitment is shown in Figure 2. Patient characteristics are listed in Table 1. No significant differences were found between the three groups.
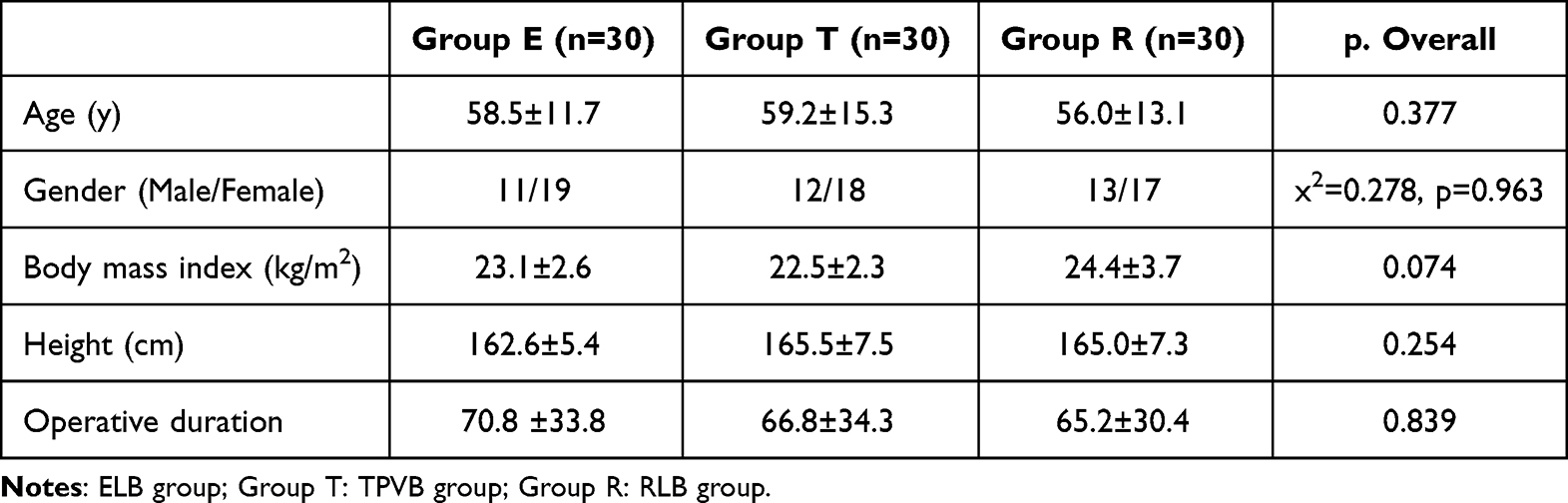 |
Table 1 Demographic and Clinical Characteristics of the Patients |
 |
Figure 2 Flow diagram of the study. |
The dermatomal sensory loss on the midclavicular line, midaxillary line, and scapular line of all groups are presented in Table 2. In order to better reflect the effects of the three blocking methods on the skin segment, we presented the case results of the three observation lines with blocking effects separately. We also measured the effective ratio of patients who achieved a blocking effect on one observation line in a group. Group E had wider dermatomal sensory loss on the midclavicular and midaxillary line compared to Group R and had a wider range on the scapular line compared to Group T (P < 0.001), regardless of whether non-effective dermatomes were included (Table 2). Meanwhile, in Group E, T, and R, the percentages of analgesic effect on the three observation lines were 93.3% (28/30 cases), 60% (18/30 cases) and 26.7% (8/30 cases), respectively. This suggested that ELB was able to block the region of the three lines simultaneously when compared with the other two nerve block techniques (x2 = 27.778, P < 0.001). Compared with the values in Group R, Group T had wider dermatomal sensory loss on the midclavicular line and midaxillary line (P < 0.001), but the range on the scapular line was narrower (P < 0.01). In addition, bilateral blockade occurred in two patients in Group E. They both had 9 hypoesthesia dermatomes (T4–T12).
 |
Table 2 Dermatomes and Ratios of Sensory Loss on Midclavicular Line, Midaxillary Line, and Scapular Line of Three Groups |
There was no significant difference in the intraoperative sufentanil dosage in the three groups. Post-operative NRS scores at each time point were significantly lower in Group E than in the other two groups (P < 0.05). There was no statistical difference in NRS scores between Group T and Group R at each time point (Table 3). Patients in Group E received less pethidine rescue compared to the other two groups (P = 0.006).
 |
Table 3 Intraoperative Consumption of Sufentanil, Postoperative Pethidine Rescue, and NRS Scores in Three Groups |
Perioperative nerve block-related complications were not observed in any of them.
Discussion
Although the safety and effectiveness of TPVB have been acknowledged,12 the outcome depends to some extent on the skill of the operator on account of the anatomy of TPVS. Previous studies reported that the continuous RLB shows effective surgical analgesia and satisfactory postoperative pain control in PCNL surgery,13 breast cancer surgery by landmark technique14 and rib fracture.15 These studies indicated that RLB could be developed as an alternative to TPVB due to its easier and safer properties. However, its analgesic effect is inferior to that of TPVB.4 We developed the ELB based on RLB. There were no major vessels, nerves, or pleura in the needle pathway, which was confirmed with ultrasonography. The operator could easily advance the needle to the point of injection without worrying about the risk of TPVB.
In this study, we found that group T had wider dermatomal sensory loss on the midclavicular line and midaxillary line than Group R, but the blocking effect of Group R on the scapular line was superior to that of Group T. This is consistent with the conclusion of Sabouri.16 These results indicated that the injection sites of the two groups could be related to these results. Although TPVS is connected with the intervertebral foramen, the injection point is at a certain distance from the intervertebral foramen. Therefore, the TPVB local anesthetics mainly infiltrate the anterior thoracic nerve. However, the anesthetics for RLB were injected in the space between the erector spinae and the lamina that was close to the posterior branch. Although previous cadaver studies have demonstrated that LA of the RLB may penetrate the superior costal transverse ligament and the posterior ramus of the spinal nerve to the TPVS, its blocking effect is still inferior to that of the TPVB.16
The injection site of ELB which Shu8 introduced is at the edge of the lamina near the inferior articular process of the vertebra and is closer to the zygapophyseal than RLB. In this study, the analgesic dermatomal along the three lines in Group E were more than those of the other two groups, irrespective of whether the patients who did not experience the blocking effect were excluded or not. In addition, we found that ELB blocked anterior branches more effectively than RLB and blocked posterior branches more effectively than TPVB. A relatively wider range of blocks enabled Group E to experience better post-operative analgesia. Also, in Group E, the ratio of sensory loss on the midclavicular line, midaxillary line, and scapular line was 96.7% (29/30 cases). The percentage of patients who acquired anterior and posterior branch blockade simultaneously in Group E was 93.3% (28/30 cases), which was significantly higher than that in groups T and R (60% (18/30 cases), 26.7% (8/30 cases)), respectively. The above findings may be due to more anesthetics being diffused into the TPVS near the foraminal outlet as it spreads along the lamina, so the anterior and posterior branches of the thoracic nerve could be effectively blocked.
TPVB and RLB have been widely used for post-operative analgesia in VATS.17–20 Wang19 and Sandeep20 noted that TPVB was superior to RLB, while in our study, there was no significant difference in NRS scores between our T and R groups. This may be related to the routine daily intravenous infusion of flurbiprofen in our trial. It is worth noting that the post-operative NRS scores in our Group E were significantly lower than those in the other two groups at each time point (P < 0.05). There was no statistical difference in the intraoperative usage of sufentanil among the three groups, whether in the analysis of total amount or unit dosage. Meanwhile, the frequency of pethidine rescue in Group E was also significantly lower than those in the other two groups. It is assumed that the decrease in post-operative NRS might be attributed to ELB. Satisfactory post-operative analgesia depends on effective analgesia in the anterior, middle, and posterior areas of the chest wall, namely successful blockade at the anterior and posterior branches.
There were several limitations in this study. Firstly, there was no cadaver study, and we could not confirm whether the LA of the ELB was mainly diffused to the TPVS adjacent to the foramina. Even if this was the case, it is still not known whether the solution similarly infiltrates into the TPVS as it does in RLB. In addition, there were two patients with bilateral blocks in Group E. How the solution enters the vertebral canal can perhaps only be understood in a cadaver study. Secondly, only NRS scale was used to find the efficacy, other pain score assessment scales should be used to conclude this result. Finally, all the three nerve blocks in the study belong to the paravertebral block. Theoretically, LA spreads in different ways and ranges due to different doses. In a study with pig carcasses, Damjanovska21 found that LA of 10 mL could spread to the posterior branch of the spinal nerve, but could not spread to the TPVS when RLB was done. Nonetheless, LA was found in the TPVS when 30 mL dose was given. We do not know whether using higher doses in our study would have resulted in different results, and this needs to be addressed in further clinical studies.
Conclusion
In conclusion, ELB was effective in achieving block of the anterior and posterior branches of the thoracic nerve simultaneously, and had a wider nerve block range and better post-operative analgesia in comparison with TPVB and RLB. It has the potential to be a better alternative to TPVB in thoracic surgery.
Data Sharing Statement
The datasets used and analyzed during the current study had been submitted to publicly available repository https://pan.baidu.com/s/1FXkjstyAJ0XZuU_MpsyV_A, and the accession code is available from the corresponding author on reasonable request.
Ethics Approval
This trial had been approved by the Ethics Committee of Shanghai Sixth People’s Hospital (2021–005). This study was conducted in accordance with the declaration of Helsinki.
Consent to Participate
Written informed consents were obtained from all patients.
Consent for Publication
All authors read and approved the final manuscript and were in agreement with the content of the manuscript.
Code Availability
The sample size was calculated with PASS 11.0, and the statistical analyses were performed using SPSS 26.0 software.
Acknowledgments
We appreciate the supports from the cardiothoracic surgeons and nursing teams of Shanghai Sixth People’s Hospital.
Funding
This work was supported by grant from the Scientific research fund of Shanghai Sixth People’s Hospital to M.X.C. (YNTS202005).
Disclosure
The authors report no conflicts of interest in this work.
References
1. El Mourad MB, Amer AF. Effects of adding dexamethasone or ketamine to bupivacaine for ultrasound-guided thoracic paravertebral block in patients undergoing modified radical mastectomy: a prospective randomized controlled study. Indian J Anaesth. 2018;62(4):285–291. PMID: 29720754; PMCID: PMC5907434. doi:10.4103/ija.IJA_791_17
2. Ding W, Chen Y, Li D, et al. Investigation of single-dose thoracic paravertebral analgesia for postoperative pain control after thoracoscopic lobectomy - a randomized controlled trial. Int J Surg. 2018;57:8–14. PMID: 30056127. doi:10.1016/j.ijsu.2018.07.006
3. Pace MM, Sharma B, Anderson-Dam J, Fleischmann K, Warren L, Stefanovich P. Ultrasound-guided thoracic paravertebral blockade: a retrospective study of the incidence of complications. Anesth Analg. 2016;122(4):1186–1191. PMID: 26756911. doi:10.1213/ANE.0000000000001117
4. Murouchi T, Yamakage M. Retrolaminar block: analgesic efficacy and safety evaluation. J Anesth. 2016;30(6):1003–1007. PMID: 27518726. doi:10.1007/s00540-016-2230-1
5. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41:621–627. doi:10.1097/AAP.0000000000000451
6. Gurkan Y, Aksu C, Kus A, Yorukoglu UH, Kilic CT. Ultrasound guided erector spinae plane block reduces postoperative opioid consumption following breast surgery: a randomized controlled study. J Clin Anesth. 2018;50:65–68. doi:10.1016/j.jclinane.2018.06.033
7. Yao Y, Li H, He Q, Chen T, Wang Y, Zheng X. Efficacy of ultrasound-guided erector spinae plane block on postoperative quality of recovery and analgesia after modified radical mastectomy: randomized controlled trial. Reg Anesth Pain Med. 2020;45:5–9. doi:10.1136/rapm-2019-100983
8. Shu Z, Zhang J, Cao J. A novel approach of ultrasound-guided laminar block for rib fracture surgery. J Clin Anesth. 2021;70:110191. PMID: 33561706. doi:10.1016/j.jclinane.2021.110191
9. Sotome S, Sawada A, Wada A, Shima H, Kutomi G, Yamakage M. Erector spinae plane block versus retrolaminar block for postoperative analgesia after breast surgery: a randomized controlled trial. J Anesth. 2021;35(1):27–34. doi:10.1007/s00540-020-02855-y
10. Tao T, Zhou Q. 竖脊肌平面阻滞与后路椎板阻滞对后路腰椎手术术后镇痛效果的比较 [Efficacy of erector spinae block versus retrolaminar block for postoperative analgesia following posterior lumbar surgery]. Nan Fang Yi Ke Da Xue Xue Bao. 2019;39(6):736–739. Chinese. doi:10.12122/j.issn.1673-4254.2019.06.17
11. Taketa Y, Fujitani T. A novel paralaminar in-plane approach for ultrasound-guided continuous thoracic paravertebral block using microconvex array transducer. Reg Anesth Pain Med. 2015;40(4):390. PMID: 26079356. doi:10.1097/AAP.0000000000000259
12. Schnabel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery: a meta-analysis of randomized controlled trials. Br J Anaesth. 2010;105(6):842–852. Erratum in: Br J Anaesth. 2013;111(3):522. PMID: 20947592. doi:10.1093/bja/aeq265
13. Kumari P, Kumar A, Sinha C, Kumar A, Kumari A. Continuous retrolaminar block in percutaneous nephrolithotomy surgery. Saudi J Anaesth. 2023;17(1):132–133. doi:10.4103/sja.sja_486_22
14. Jüttner T, Werdehausen R, Hermanns H, et al. The paravertebral lamina technique: a new regional anesthesia approach for breast surgery. J Clin Anesth. 2011;23:443–450. doi:10.1016/j.jclinane.2010.12.015
15. Voscopoulos C, Palaniappan D, Zeballos J, Ko H, Janfaza D, Vlassakov K. The ultrasound-guided retrolaminar block. Can J Anesth. 2013;60:888–895. doi:10.1007/s12630-013-9983-x
16. Sabouri AS, Crawford L, Bick SK, Nozari A, Anderson TA. Is a retrolaminar approach to the thoracic paravertebral space possible?: A human cadaveric study. Reg Anesth Pain Med. 2018;43(8):864–868. PMID: 29923954. doi:10.1097/AAP.0000000000000828
17. Taketa Y, Irisawa Y, Fujitani T. Comparison of analgesic efficacy between two approaches of paravertebral block for thoracotomy: a randomised trial. Acta Anaesthesiol Scand. 2018;62(9):1274–1279. PMID: 30047132. doi:10.1111/aas.13216
18. Nobukuni K, Hatta M, Nakagaki T, Yoshino J, Obuchi T, Fujimura N. Retrolaminar versus epidural block for postoperative analgesia after minor video-assisted thoracic surgery: a retrospective, matched, non-inferiority study. J Thorac Dis. 2021;13(5):2758–2767. PMID: 34164168; PMCID: PMC8182553. doi:10.21037/jtd-21-238
19. Wang Q, Wei S, Li S, et al. Comparison of the analgesic effect of ultrasound-guided paravertebral block and ultrasound-guided retrolaminar block in uniportal video-assisted thoracoscopic surgery: a prospective, randomized study. BMC Cancer. 2021;21(1):1229. PMID: 34784889; PMCID: PMC8594110. doi:10.1186/s12885-021-08938-7
20. Sandeep B, Huang X, Li Y, Xiong D, Zhu B, Xiao Z. A comparison of regional anesthesia techniques in patients undergoing video-assisted thoracic surgery: a network meta-analysis. Int J Surg. 2022;105:106840. PMID: 36030040. doi:10.1016/j.ijsu.2022.106840
21. Damjanovska M, Stopar Pintaric T, Cvetko E, Vlassakov K. The ultrasound-guided retrolaminar block: volume-dependent injectate distribution. J Pain Res. 2018;11:293–299. PMID: 29445296; PMCID: PMC5808708. doi:10.2147/JPR.S153660
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.