Back to Journals » Nature and Science of Sleep » Volume 15
Comparison of Acceptance and Commitment Therapy (ACT) and Cognitive Behavior Therapy (CBT) for Chronic Insomnia: A Pilot Randomized Controlled Trial
Authors Shin JW ![]() , Kim S, Shin YJ, Park B, Park S
, Kim S, Shin YJ, Park B, Park S
Received 24 March 2023
Accepted for publication 22 June 2023
Published 5 July 2023 Volume 2023:15 Pages 523—531
DOI https://doi.org/10.2147/NSS.S409981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Jung-Won Shin,1,* Seonyeop Kim,2,* Yoon Jung Shin,2 Bomi Park,2 Sunyoung Park2
1Department of Neurology, Memory Center, Bundang CHA Medical Center, CHA University, Seongnam-si, Gyeonggi-do, Republic of Korea; 2Graduate School of Clinical Counselling Psychology, CHA University, Seongnam-si, Gyeonggi-do, Republic of Korea
*These authors contributed equally to this work
Correspondence: Jung-Won Shin, Department of Neurology, CHA Bundang Medical Center, CHA University, 59 Yatap-Dong, Bundang-Gu, Seongnam-si, Gyeonggi-do, 463-712, Republic of Korea, Tel +82-31-780-5058, Email [email protected]
Purpose: Acceptance and Commitment Therapy (ACT) is part of the third wave of cognitive behavior therapy, and has six core components: acceptance, cognitive defusion, self as context, being present, values, and committed behavior. This study aimed to examine the efficacy of ACT for insomnia compared with cognitive behavior therapy for insomnia (CBT-I) in patients with chronic primary insomnia.
Methods: The study recruited patients with chronic primary insomnia from a university hospital between August 2020 and July 2021. Thirty patients were enrolled and randomly assigned to receive either ACT (n = 15) or CBT-I (n = 15). Interventions were performed over four weeks, with four sessions of face-to-face therapy and four sessions of online therapy. The outcomes were measured using a sleep diary and a questionnaire.
Results: Post-intervention, the ACT and CBT-I groups had significantly improved sleep quality, insomnia severity, depression, beliefs about sleep, sleep onset latency (SOL), and sleep efficacy (SE) (p < 0.05). However, anxiety was significantly reduced in the ACT group (p = 0.015), but not in the CBT-I group.
Conclusion: ACT had a significant effect on primary insomnia and secondary symptoms, especially anxiety related to insomnia. These findings suggest that ACT could be a potential intervention for individuals who do not respond to CBT-I, who have high anxiety regarding sleep problems.
Keywords: insomnia, cognitive behavior therapy, acceptance and commitment therapy
Introduction
Cognitive Behavioral Therapy for Insomnia (CBT-I) is a non-pharmacological treatment that modifies dysfunctional behaviors and cognition regarding sleep, and is traditionally suggested as the first-line of treatment in the United States and Europe.1 However, about 40% of patients show minimal improvement or experience relapse following CBT-I.2 Variables of insomnia patients that render them unsuitable for CBT-I include the severity of depression,3 comorbidity,4 and difficulties in conducting the restriction of sleep and therapy of stimulus control.5 Specifically, mood symptoms such as depression and anxiety, which are related to poor attendance in CBT-I, may also contribute to inconsistent wake times during behavior therapy within CBT-I.6,7 Sleep is an uncontrollable and involuntary process; efforts to control insomnia paradoxically can lead to increased anxiety and stress surrounding sleep, which in turn worsens the insomnia and perpetuates the cycle of sleeplessness.8 However, traditional CBT-I mainly focuses on reducing symptoms by modifying cognitive and behavioral habits, which can cause a vicious cycle of low effects and compliance in patients who have tried to control their sleep for a long time. Patients who had continued to have poor sleep that do not improve and persist during the treatment CBT-I, anxiety might increase during the process of emphasizing sleep restriction and repetitive modifications of dysfunctional beliefs in CBT-I. As a result, increased anxiety itself could hinder treatment effects of CBT-I. Therefore, it may be more effective to educate patients in taking a more receptive attitude towards the symptoms of sleep disorders.
Acceptance and Commitment Therapy (ACT) is the latest therapeutic approach in cognitive behavioral therapy, focusing on acceptance rather than modifying dysfunctional thoughts and feelings.9 Excessive control of thoughts and feelings can be related to the paradoxical effects of control, resulting in unintentionally experiencing unwanted thoughts and feelings more strongly.10 In the sleep effort model, excessive control and effort to sleep also induce a stronger awakening and prohibit the natural process of sleep.8 In the same way, it is suggested that sleep is an involuntary and automatic process, making it more difficult to reach sleep with conscious attention and control.11 The variables of ACT can improve the degree of acceptance, reducing the degree of excessive control.
ACT does not encourage patients to avoid thoughts, feelings, or physical sensations but allows patients to experience them as they are.12 The acceptance of insomnia reduces the severity of the patient’s symptoms and, paradoxically, can lead to a higher level of sleepiness.13 These processes are dependent on the patient being willing to experience anxiety and physical discomfort, which can prevent a vicious cycle of insomnia and also increase the therapeutic effects.13 In addition, acceptance rather than excessive control of emotions such as depression and anxiety can help patients who have high degree of emotional symptoms caused by insomnia.
A recent study has shown that applying ACT to chronic insomnia reduces the severity of insomnia and improves sleep quality compared with controls.14,15 Therefore, the objective of this study was to develop an insomnia program utilizing Acceptance and Commitment Therapy and to evaluate the effectiveness of ACT techniques in addressing the limitations of Cognitive Behavioral Therapy for Insomnia (CBT-I). Our hypothesis was that ACT would be more effective than traditional CBT in improving mood symptoms, including depression and anxiety about sleep, which can reduce the effectiveness of CBT-I.
Methods
Participants
This was a single-site trial conducted at a University Medical Center, where participants were recruited between August 2020 and July 2021, and they were admitted to outpatient sleep clinics in the Medical Center due to symptoms of insomnia. The study recruited adults aged 19 years or older who met the research diagnostic criteria for chronic insomnia as defined by the International Classification of Sleep Disorders-3,16 and participants were diagnosed after face-to-face interviews and structured questionnaires with a neurologist (JWS) in the outpatient sleep clinic at their first visit. The following exclusion criteria were applied: (1) uncontrolled psychiatric conditions requiring immediate treatment outside the scope of the study, including an ongoing major depressive episode; (2) uncontrolled medical conditions suspected to affect sleep or requiring immediate treatment outside the scope of the study; (3) previous diagnosis or evidence of specific sleep disorders, such as restless legs syndrome, obstructive sleep apnea, or circadian rhythm sleep disorders (screened using clinical interviews and sleep questionnaires, including Sleep-50);17 (4) use of any sedating drugs or hypnotics for improving symptoms of insomnia; or (5) insufficient Korean language proficiency hindered their ability to complete the protocol. Written informed consent was obtained from all participants and the study received approval from the institutional review board of CHA University Medical Center (IRB approval No.: 2020–06-028). This trial has been registered with the Clinical Research Information Service (CRIS), Republic of Korea (KCT0008296). The study followed the principles of the Declaration of Helsinki.
Study Procedure
Randomization was accomplished using randomization.com to create a list of 30 participants before the start of the trial in blocks of two conditions (1:1 CBT-I to ACT) with no stratification. A neurologist (JWS) who was not involved in the study managed all assignments.
Participants receiving ACT or CBT-I attended four weekly individual face-to-face treatment sessions, each lasting approximately one hour. In addition, participants underwent assessments of their sleep schedule and sleep hygiene and received treatment-related images and videos via an online chat consultation (Kakao channel, Seoul, Korea) once a week at midday (Supplementary Figure 1), for a total of four weeks. The CBT-I program included a manualized multicomponent approach,18 that include education of sleep hygiene,19 muscle relaxation techniques, sleep restriction,5 stimulus control20 and cognitive therapy.21
The program in this study combined ACT elements with insomnia, and was reconstructed by referring to existing ACT programs for insomnia.13,22,23 The ACT program included the following components: sleep hygiene, cognitive defusion, willingness to experience problems related to sleep without controlling them, staying in the present with mindfulness, clarifying the value of life, and activating committed behavior.
The treatment protocols used in the CBT-I and ACT condition to address insomnia are outlined in Supplementary Table 1. While CBT-I is focused on modifying thoughts related to insomnia, ACT is focused on the present moments and value of life by non-judgmentally accepting thoughts and emotions caused by insomnia. Details are given in the session of Supplementary Table 1. The therapy sessions were led by two clinical psychologists, YJS and SYK, both of whom hold Ph.D. degrees and were trained in both ACT and CBT-I. Additionally, the formalized program curriculum was delivered to participants by a supervised clinical psychologist (SYP) with over 10 years of CBT practice and certification by the Korean Psychological Association. The therapist manual was used to secure the integrity and minimize the risk of contamination. The manual consisted of treatment protocols for CBT-I and ACT and how to handle potential questions related to treatment integrity. Principal Investigator (JWS) checked that each group’s participants received the same material in the online chat consultation. The two therapists were assigned to participants in alternating fashion. After treatment had been initiated, all therapists were allowed supervision on a need-to basis.
Failure to participate in the research was defined as dropout if the session or pre-post-sleep questionnaire were not completed, and the dropout data were excluded from the analysis of the research results.
Outcome Measures
Self-assessments were conducted both before treatment and 2 weeks after treatment, with a 6-week interval between the two assessments. The primary outcome measures were the Korean version of the Pittsburgh Sleep Quality Index (PSQI),24 Insomnia Severity Scale (ISI),25 Dysfunctional Beliefs and Attitudes about Sleep Scale (DBAS-16),26 and Glasgow Sleep Effort Scale (GSES)27 to evaluate sleep quality, dysfunctional beliefs and attitudes about sleep-related symptoms of insomnia. To determine treatment response, participants were assessed based on their change score on the ISI (Insomnia Severity Index) compared to their baseline score. Participants with a change score greater than 7 were considered treatment responders. Additionally, participants with an absolute ISI score of less than 8 were considered treatment remitters. Secondary outcome measures were the Korean versions of the Patient Health Questionnaire (PHQ-9)28 and General Anxiety Disorder (GAD-7)29 to evaluate insomnia-related psychiatric symptoms, including depression and anxiety.
A 7-day sleep diary was used to assess nighttime symptoms.18,30 The diary assessed bedtime, lights out time, rise time and wake time after sleep onset (WASO) with sleep onset latency (SOL). Data for four weeks treatment periods were calculated as weekly means of WASO, SOL, total sleep time (TST = total time spent in bed – (SOL+WASO)), and sleep efficiency (SE, sleep efficacy (%) = total sleep time/total time spent in bed × 100).
Statistical Analysis
For the data analysis of this study, we used SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Per-protocol (patients compliant to treatment a final follow-up) analysis is presented. Categorical data were analyzed using the χ2 test and Fisher’s exact test. Continuous variables were reported as mean ± standard deviation (SD), and independent t-tests were utilized for comparisons between the two groups. To evaluate the treatment effects, a repeated-measures ANOVA was conducted, with the factors of “Group” (CBT-I vs ACT) and “Time” (pre-treatment vs post-treatment). A p-value of less than 0.05 was considered statistically significant for all analyses.
Results
Participants and Baseline Characteristics
The participant flow through enrollment, randomization, and analysis is shown in Figure 1 for this pilot study. Forty-three individuals were assessed for eligibility. Thirty participants were randomized to ACT and CBT-I treatment groups, and 26 completed the treatment with the two week – posttreatment follow-up assessment. Three CBT-I and one ACT participant(s) dropped out, and one participant did not attend the majority of dropouts were between baseline and Session 1 for both groups. Three of them expressed difficulty in participating due to their personal schedules, and one participant did not participate after agreeing at baseline. Table 1 provides a summary of the descriptive statistics for the study groups at baseline. There were no significant differences in any of the baseline variables between the two groups, with p-values greater than 0.05 for all variables. At baseline, the mean ± SD age of participants was 58.7 years ± 9.4 and 66.7% were female. The mean ± SD of ISI was 21.3 ± 4.2, indicating at least moderate insomnia in all participants. Participants had a high level of intrusive thoughts whilst trying to sleep and had a tendency to worry about their problems regarding sleep status, with mild to moderate depressive mood (PHQ-9 mean ± SD: 9.2 ± 5.4) and anxiety (GAD-9 mean SD: 6.7 ± 4.4).
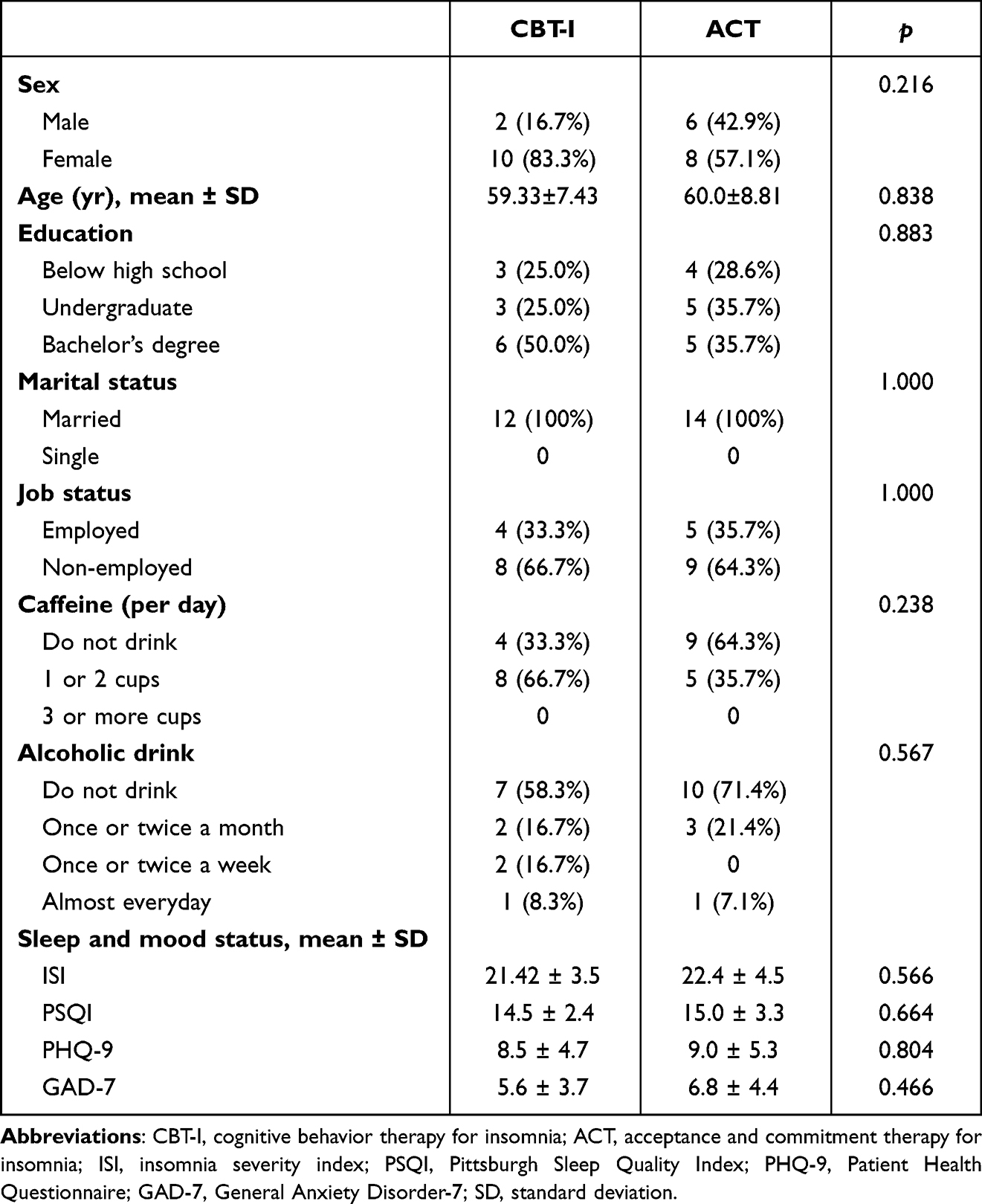 |
Table 1 Clinical Characteristics and Baseline Sleep and Mood Status |
 |
Figure 1 Study Flow Diagram. |
Primary and Secondary Outcomes
The proportions of treatment responders (66.7% in the CBT-I group and 85.7% in the ACT group; p = 0.250) and treatment remitters (33.4% in the CBT-I group and 28.6% in the ACT group; p = 0.793) were not significantly different between the CBT-I and ACT groups. The results of the sleep questionnaire indicated significant effect and group × time interactions (Table 2). Post-treatment, insomnia severity significantly decreased in both the CBT-I and ACT groups, and both programs also resulted in reduced intrusive thoughts, dysfunctional beliefs about sleep, and improved sleep quality (p < 0.05). Regarding sleep-related psychiatric symptoms, PHQ-9 scores showed significant improvement in both groups. However, the GAD-7 scores in the interaction of group with time (F = 5.183, p = 0.032) showed improvement only in the ACT group and not in the CBT-I group.
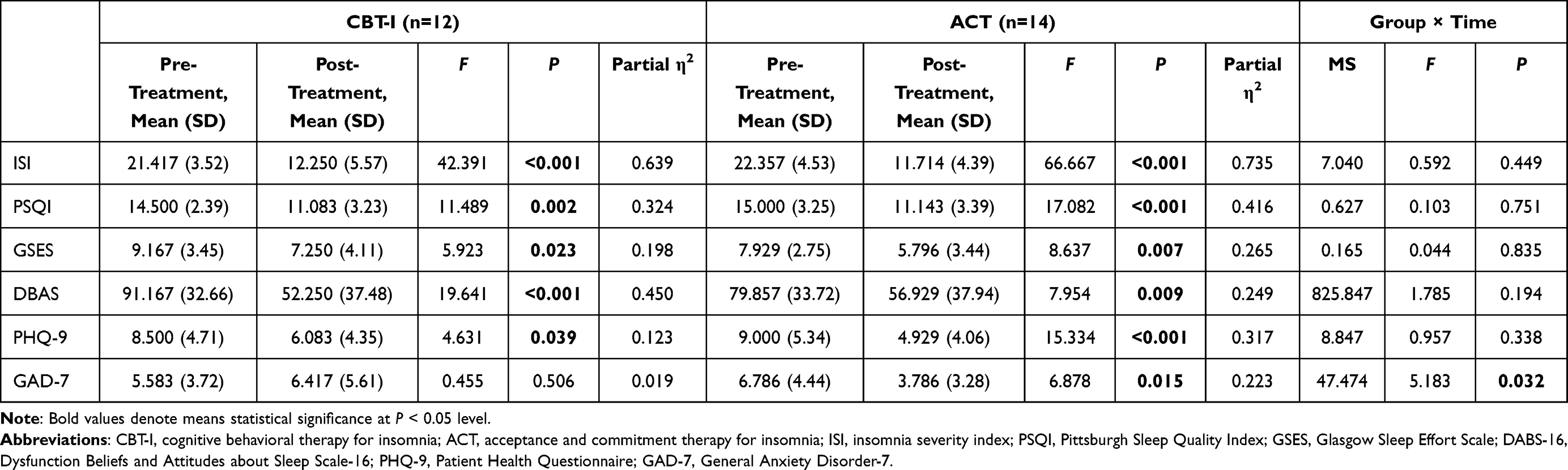 |
Table 2 Primary and Secondary Outcome Measures |
In the sleep diary, two participants in the CBT-I group and three in the ACT group did not complete the weekly sleep diary during the intervention period. Therefore, data from 10 CBT-I and 11 ACT sleep diaries were analyzed. As shown in Supplementary Figure 2 and Supplementary Table 2, while participants in the ACT group showed a significant, steady improvement in SE and reduction in SOL during intervention, participants in the CBT-I group showed a significantly reduced SOL during the second and third sessions compared with the first session. In the ACT group, TST showed a steady increase and WASO showed a decreasing trend; however, these findings were not statistically significant. For the noninferiority analysis, the data from the sleep diaries were analyzed using the interaction of group with time. As the interactions of group with time in SOL (F = 0.376, p = 0.771), SE (F = 0.652, p = 0.586), TST (F = 0.413, p = 0.530), and WASO (F = 0.618, p = 0.607) were not statistically significant, the ACT program was determined to be noninferior to CBT-I.
Discussion
This study verifies the effect of ACT in insomnia treatment. We confirmed that ACT is an effective alternative to CBT-I for insomnia treatment. This result is same as recent RCT study that showed insomnia severity was improved in both ACT and CBT-I groups.31 In our study, CBT-I and ACT were both effective in improving the primary symptoms of insomnia, including sleep quality and depression symptoms. This study is the first study that compares the effects of ACT and CBT-I on insomnia as well as mood symptoms associated with sleep disturbance. The results of this study are in line with previous research indicating that ACT is effective in enhancing emotional regulation and sleep quality in individuals with chronic insomnia. Additionally, studies suggest that insomnia treatment utilizing ACT is associated with significant reductions in insomnia, fatigue, depression, and anxiety.9,32–35
In this study, depression was significantly reduced in both groups; however, anxiety was significantly reduced in the ACT group only. Similarly, a systematic review showed that ACT can help reduce anxiety.36 Lundh and Broman suggested maintaining a focus on the cognitive processes of insomnia have two processes that are the sleep-interpreting processes and sleep-interfering processes, which consist of worries, negative emotions, and thoughts related to stressful events that lead to arousal and thus interfere with sleep.37 Sleep-interfering process including depressive and anxiety mood affect treatment response of CBT-I outcomes. Our previous study, daytime dysfunction and moods symptoms (PHQ-9 and GAD-7) were predictors for treatment outcome of CBT-I.38 Therefore, mental health status should be considered as factors that play an important role in treatment of insomnia patients. For patients with obsessive tendencies and high anxiety regarding their sleep, the level of anxiety can increase during the process of emphasizing sleep hygiene and repetitive modifications of dysfunctional beliefs in CBT-I. In contrast, in ACT, patients’ inner experiences, such as thoughts and emotions, are not objectives that need to be modified. Through the acceptance of anxiety-inducing thoughts, it lessens the paradoxical effect on insomnia. Patients who participate in ACT learn how to stop struggling the discomfort brought on by their anxiety.39 ACT as well as Mindfulness-based interventions (MBIs) is a shift from an outcome-oriented thinking (eg, actions to relieve stress) to a process-oriented approach (eg, observing that one is stressed). This metacognitive shift is posited to reduce emotional distress by changing the relationship with stress rather than changing the environment or source of stress.40 Also, ACT/MBIs deal with commitment to the value of well-being in whom the patients with chronic insomnia may lose sight of some of their life values as their focus becomes more directed toward control of sleeplessness. A measure that can capture shifts from a narrow focus on sleep related issues to a more broad focus on values and life issues would be important when assessing changes in metacognition.37 This principle of ACT/MBI seems to have reduced anxiety, making the treatment more comfortable for patients. The degree of anxiety reduction in the ACT group showed a large effect size (partial η2 = 0.223). For patients with anxiety, adhering to some of the behavioral components of CBT-I may be challenging, but ACT played a role in facilitating the treatment process by assisting participants in accepting feelings of discomfort, such as fatigue, that may arise during sleep restriction and stimulus control. A pilot study conducted previously demonstrated a substantial enhancement in sleep-related quality of life and subjective sleep quality in individuals with chronic primary insomnia who did not respond to CBT-I, immediately after completing six weekly outpatient sessions of ACT and at the 3-month follow-up.22 In a recent study, treating Mindfulness-based therapy for insomnia to patients who did not resolve insomnia symptoms after CBT-I and/or pharmacotherapy was effective to reduced ISI and had also acute large effect of acute reductions in depression and cognitive arousal.41 Also, a meta-analysis showed CBT-I had small and non-reliable effects on rumination that is crucial maintaining factor of insomnia and strong predictor of anxiety and depression, and moderate but not significant on anxiety. Interestingly, they found that studies including “boosted” CBT-I protocols, with the integration of specific techniques targeting worry (mindfulness, meta-cognitive therapy, constructive worry) within the CBT-I protocol, appeared to have a larger impact on general worry compared to those including standard CBT-I techniques only.42 In our study, CBT-I showed a greater effect size in reducing dysfunctional beliefs about sleep (partial η2 = 0.450) compared with ACT (partial η2 = 0.249), while ACT showed a greater effect size in reducing depression (partial η2 = 0.317) and anxiety (partial η2 = 0.223) compared with CBT-I (depression: partial η2 = 0.123; anxiety: partial η2 = 0.019, ns). Therefore, novel treatments using mindfulness and acceptance-based approaches may hold promise as an effective intervention for individuals who do not respond to CBT-I, particularly for patients with anxiety that is related to prominent worry and rumination at night.
In the sleep diaries of our study, SOL improved in both groups, and SE only improved in ACT. Although there was no statistical significance, TST tended to increase and WASO tended to decrease in the ACT group. In the CBT-I group, TST tended to shorten after post-treatment Session 2, which may be due to the behavioral therapy of sleep restriction and stimulus control; WASO decreased significantly. However, our sleep diary data are limited in interpretation. The number of participants was small and assessed only during the treatment period.
Our study had some limitations. First, this study is a pilot RCT study with a limited sample size, requiring caution in interpretation. Additionally, as this study examined the effects over a short period of six weeks, it is necessary to investigate through long-term follow-up assessments whether the effects of CBT-I and ACT persist even after the completion of treatment and if so, in which variables they manifest. Through this, we can examine the strengths of each program in influencing factors of insomnia and apply tailored treatments for insomnia patients. Second, our study excluded patients with severe medical or psychiatric conditions, and had a relatively high proportion of female participants with a higher level of education and married status in the clinical population. In actual clinical practice, individuals with insomnia often have serious comorbid medical or psychiatric conditions and are socioeconomically unstable. Therefore, further ongoing research is needed to determine if ACT has sufficient therapeutic effects for patients with these clinical characteristics.
Nevertheless, this study suggests that the application of alternative insomnia programs for the chronic insomnia by considering the characteristics of individual patients who have poor mental health status related to insomnia, which have been difficult to deal with using CBT-I should be necessary. ACT has an effect on the primary symptoms of insomnia similar to CBT-I; while CBT-I has greater strength in modifying dysfunctional beliefs, ACT seems to have more strength in dealing with anxiety and depressive mood. In particular, because traditional CBT-I has focused on modifying dysfunctional beliefs about sleep and changing dysfunctional sleep behavior or habits, it is meaningful that ACT has presented an alternative way that can be effective for patients with insomnia who are not effectively treated with traditional CBT-I, by introducing a new context of treatment such as acceptance and defusion rather than change. Novel therapies including mindfulness and acceptance-commitment approaches help patients accept thoughts and emotions caused by insomnia non-judgmentally, alleviating mood-related symptoms and cognitive arousal. As sleep is an involuntary and natural process, a treatment that focus on a new context of acceptance without resistance, not change or correction, can be a useful alternative approach that compensates for the limitations of CBT-I. It is also expected to improve the patient’s quality of life by clarifying the value of life and activating behavior that focuses on this, rather than focusing on the symptoms of insomnia.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (Jung-Won Shin) upon reasonable request. Individual deidentified participant data are available after contacting the corresponding author via email. The data will be available immediately after publication without an end date.
Funding
This study was supported by a research grant from the Korean Sleep Research Society in 2020, and the National Research Foundation of Korea, South Korea (NRF) grant funded by the Korean government (No. NRF- 2020R1F1A1067882).
Disclosure
Jung-Won Shin and Seonyeop Kim are co-first authors. The authors report no conflicts of interest in this work.
References
1. Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison. Arch Intern Med. 2004;164(17):1888–1896. doi:10.1001/archinte.164.17.1888
2. Castronovo V, Galbiati A, Sforza M, et al. Long-term clinical effect of group cognitive behavioral therapy for insomnia: a case series study. Sleep Med. 2018;47:54–59. doi:10.1016/j.sleep.2018.03.017
3. Ong JC, Kuo TF, Manber R. Who is at risk for dropout from group cognitive-behavior therapy for insomnia? J Psychosom Res. 2008;64(4):419–425. doi:10.1016/j.jpsychores.2007.10.009
4. Cui R, Fiske A. Predictors of treatment attendance and adherence to treatment recommendations among individuals receiving cognitive behavioral therapy for insomnia. Cog Behav Ther. 2020;49(2):113–119. doi:10.1080/16506073.2019.1586992
5. Spielman AJ, Saskin P, Thorpy MJ. Treatment of chronic insomnia by restriction of time in bed. Sleep. 1987;10(1):45–56.
6. Riedel BW, Lichstein KL. Strategies for evaluating adherence to sleep restriction treatment for insomnia. Behav Res Ther. 2001;39(2):201–212. doi:10.1016/S0005-7967(00)00002-4
7. Galbiati A, Sforza M, Fasiello E, Castronovo V, Ferini-Strambi L. Impact of phenotypic heterogeneity of insomnia on the patients’ response to cognitive-behavioral therapy for insomnia: current perspectives. Nat Sci Sleep. 2019;11:367–376. doi:10.2147/NSS.S198812
8. Broomfield NM, Espie CA. Towards a valid, reliable measure of sleep effort. J Sleep Res. 2005;14(4):401–407. doi:10.1111/j.1365-2869.2005.00481.x
9. Salari N, Khazaie H, Hosseinian-Far A, et al. The effect of acceptance and commitment therapy on insomnia and sleep quality: a systematic review. BMC Neurol. 2020;20(1):1–18. doi:10.1186/s12883-020-01883-1
10. Wegner DM, Schneider DJ, Carter SR, White TL. Paradoxical effects of thought suppression. J Pers Soc Psychol. 1987;53(1):5. doi:10.1037/0022-3514.53.1.5
11. Espie CA, Broomfield NM, MacMahon KM, Macphee LM, Taylor LM. The attention–intention–effort pathway in the development of psychophysiologic insomnia: a theoretical review. Sleep Med Rev. 2006;10(4):215–245. doi:10.1016/j.smrv.2006.03.002
12. Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. 2006;44(1):1–25. doi:10.1016/j.brat.2005.06.006
13. Dalrymple KL, Fiorentino L, Politi MC, Posner D. Incorporating principles from acceptance and commitment therapy into cognitive-behavioral therapy for insomnia: a case example. J Contemp Psychother. 2010;40(4):209–217. doi:10.1007/s10879-010-9145-1
14. Zakiei A, Khazaie H, Rostampour M, et al. Acceptance and Commitment Therapy (ACT) improves sleep quality, experiential avoidance, and emotion regulation in individuals with insomnia—results from a randomized interventional study. Life. 2021;11(2):133. doi:10.3390/life11020133
15. Chapoutot M, Peter‐Derex L, Schoendorff B, Faivre T, Bastuji H, Putois B. Telehealth‐delivered CBT‐I programme enhanced by acceptance and commitment therapy for insomnia and hypnotic dependence: a pilot randomized controlled trial. J Sleep Res. 2021;30(1):e13199. doi:10.1111/jsr.13199
16. Sateia MJ. International classification of sleep disorders. Chest. 2014;146(5):1387–1394. doi:10.1378/chest.14-0970
17. Spoormaker VI, Verbeek I, van den Bout J, Klip EC. Initial validation of the SLEEP-50 questionnaire. Behav Sleep Med. 2005;3(4):227–246. doi:10.1207/s15402010bsm0304_4
18. Lundh L-G. Morin, cm: insomnia: psychological assessment and management. Scand J Behav Ther. 1994;23:62.
19. Morgan K, Thompson J, Dixon S, Tomeny M, Mathers N. Predicting longer-term outcomes following psychological treatment for hypnotic-dependent chronic insomnia. J Psychosom Res. 2003;54(1):21–29. doi:10.1016/S0022-3999(02)00569-X
20. Bootzin R, Nicassio P, Hersen M, Eisler R, Miller P. Progress in Behavior Modification. Vol. 6. New York, NY: Academic Press; 1978.
21. Beck AT. Cognitive Therapy and the Emotional Disorders. Penguin; 1979.
22. Hertenstein E, Thiel N, Lüking M, et al. Quality of life improvements after acceptance and commitment therapy in nonresponders to cognitive behavioral therapy for primary insomnia. Psychother Psychosom. 2014;83(6):371–373. doi:10.1159/000365173
23. Meadows G. Acceptance and Commitment Therapy for Insomnia (ACT-I) by Dr Guy Meadows. Available from: https://contextualscience.org/acceptance_and_commitment_therapy_for_insomnia_act#.
24. Sohn SI, Kim DH, Lee MY, Cho YW. The reliability and validity of the Korean version of the Pittsburgh Sleep Quality Index. Sleep Breath. 2012;16(3):803–812. doi:10.1007/s11325-011-0579-9
25. Cho YW, Song ML, Morin CM. Validation of a Korean version of the insomnia severity index. J Clin Neurol. 2014;10(3):210–215. doi:10.3988/jcn.2014.10.3.210
26. Yu E, Ko Y, Sung G, Kwon J. Validation of the Korean version of dysfunctional beliefs and attitudes about sleep (K-DBAS-16). Korean J Clin Psychol. 2009;28(1):309–320. doi:10.15842/kjcp.2009.28.1.018
27. Kim M, Kwon J, Koo H, Han J. Validation of Korean version of Glasgow sleep effort scale (GSES). Cogn Behav Ther Kor. 2014;14:319–337.
28. Han C, Jo SA, Kwak J-H, et al. Validation of the patient health questionnaire-9 Korean version in the elderly population: the Ansan Geriatric study. Compr Psychiatry. 2008;49(2):218–223. doi:10.1016/j.comppsych.2007.08.006
29. Lee SH, Shin C, Kim H, et al. Validation of the Korean version of the generalized anxiety disorder 7 self‐rating scale. Asia Pac Psychiatry. 2020;14:e12421. doi:10.1111/appy.12421
30. Carney CE, Buysse DJ, Ancoli-Israel S, et al. The consensus sleep diary: standardizing prospective sleep self-monitoring. Sleep. 2012;35(2):287–302. doi:10.5665/sleep.1642
31. El Rafihi-Ferreira R, Morin CM, Hasan R, Brasil IS, Zago Ribeiro JHJ, Cecilia Toscanini A. A Pilot Randomized Controlled Trial (RCT) of acceptance and commitment therapy versus cognitive behavioral therapy for chronic insomnia. Behav Sleep Med. 2023;21(2):193–207. doi:10.1080/15402002.2022.2071272
32. Kallestad H, Jacobsen HB, Landrø NI, Borchgrevink PC, Stiles TC. The role of insomnia in the treatment of chronic fatigue. J Psychosom Res. 2015;78(5):427–432. doi:10.1016/j.jpsychores.2014.11.022
33. Jacobsen HB, Kallestad H, Landrø NI, Borchgrevink PC, Stiles TC. Processes in acceptance and commitment therapy and the rehabilitation of chronic fatigue. Scand J Psychol. 2017;58(3):211–220. doi:10.1111/sjop.12363
34. Lang AJ, Schnurr PP, Jain S, et al. Randomized controlled trial of acceptance and commitment therapy for distress and impairment in OEF/OIF/OND veterans. Psychol Trauma. 2017;9(S1):74. doi:10.1037/tra0000127
35. Craner JR, Lake ES, Bancroft KA, George LL. Treatment outcomes and mechanisms for an ACT‐based 10‐week interdisciplinary chronic pain rehabilitation program. Pain Pract. 2020;20(1):44–54. doi:10.1111/papr.12824
36. Swain J, Hancock K, Hainsworth C, Bowman J. Acceptance and commitment therapy in the treatment of anxiety: a systematic review. Clin Psychol Rev. 2013;33(8):965–978. doi:10.1016/j.cpr.2013.07.002
37. Ong JC, Ulmer CS, Manber R. Improving sleep with mindfulness and acceptance: a metacognitive model of insomnia. Behav Res Ther. 2012;50(11):651–660. doi:10.1016/j.brat.2012.08.001
38. Shin JW, Kim S, Park B, Shin YJ, Park S. Improving mental health and daytime function in adult insomnia patients predict cognitive behavioral therapy for insomnia effectiveness: a case-control study. Sleep Med X. 2023;5:100071. doi:10.1016/j.sleepx.2023.100071
39. Chapoutot M, Peter-Derex L, Bastuji H, et al. Cognitive behavioral therapy and acceptance and commitment therapy for the discontinuation of long-term benzodiazepine use in insomnia and anxiety disorders. Int J Environ Res Public Health. 2021;18(19):10222. doi:10.3390/ijerph181910222
40. Ong JC, Kalmbach DA. Mindfulness as an adjunct or alternative to CBT-I. Sleep Med Clin. 2023;18(1):59–71. doi:10.1016/j.jsmc.2022.09.002
41. Kalmbach DA, Cheng P, Ong JC, et al. Mindfulness-based therapy for insomnia alleviates insomnia, depression, and cognitive arousal in treatment-resistant insomnia: a single-arm telemedicine trial. Front Sleep. 2023;2:8. doi:10.3389/frsle.2023.1072752
42. Ballesio A, Bacaro V, Vacca M, et al. Does cognitive behaviour therapy for insomnia reduce repetitive negative thinking and sleep-related worry beliefs? A systematic review and meta-analysis. Sleep Med Rev. 2021;55:101378. doi:10.1016/j.smrv.2020.101378
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.