Back to Journals » Advances in Medical Education and Practice » Volume 13
Comparison Between Students Admitted Through Regular Path and Affirmative Action Systems in a Brazilian Public Medical School
Authors Biazotto MLSH, Bittencourt FV, de Araújo GR, Fernandes SES, Göttems LBD, Rodrigues CML ![]() , Neves FAR
, Neves FAR ![]() , Amorim FF
, Amorim FF ![]()
Received 3 November 2021
Accepted for publication 1 March 2022
Published 14 March 2022 Volume 2022:13 Pages 251—263
DOI https://doi.org/10.2147/AMEP.S347387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Marize Lima de Sousa Holanda Biazotto,1,2 Fernanda Viana Bittencourt,3 Gilson Roberto de Araújo,2 Sérgio Eduardo Soares Fernandes,1 Leila Bernarda Donato Göttems,1 Carlos Manoel Lopes Rodrigues,4 Francisco de Assis Rocha Neves,2 Fábio Ferreira Amorim1,2
1School of Medicine, School of Health Sciences (ESCS), Brasília, Federal District, Brazil; 2Graduation Program in Health Sciences, University of Brasília (UnB), Brasília, Federal District, Brazil; 3Education and Research Foundation of Health Sciences (FEPECS), Brasília, Federal District, Brazil; 4School of Psychology, Centro Universitário de Brasília (UniCEUB), Brasília, Federal District, Brazil
Correspondence: Fábio Ferreira Amorim, School of Medicine, School of Health Sciences (ESCS), UNIDADE I - SMHN Quadra 03, Conjunto A, Bloco 1 - Edifício FEPECS, Brasília, Federal District, Brazil, Tel +55 61 999773516, Email [email protected]
Purpose: Affirmative action policies to provide access to higher education for socially vulnerable students have been implemented in several countries and have faced many questions nowadays. The aim of the study was to compare the socioeconomic background and performance during and after completing the undergraduate course of students admitted through the regular path and social quota systems in a public medical school in Brazil.
Methods: A retrospective cohort study including students admitted to a medical school within the School of Health Sciences (ESCS), in Brazil, between 2005 and 2012, and followed until May 2020. In the first phase, data collection was performed by analyzing documents from the ESCS academic management system and Brazilian government agencies. In the second phase, a survey with 12 questions was sent to the medical school alumni. The social quota system criteria were the public school attendance in all primary and secondary education levels.
Results: Among 707 students, 204 (28.9%) were from the social quota and 503 (78.5%) from the regular path system. The place of residence of social quota students had a lower Human Development Index (p < 0.001) and per capita income (p < 0.001) when compared to regular path students. Regular path students were associated with the highest dropout from medical school (OR: 50.552, 95% CI: 12.438– 205.453, p < 0.001). There was no difference between regular path and social quota students attending medical residency programs (OR: 1.780, 95% CI: 0.957– 3.309, p = 0.069). Out of the 308 alumni who completed the survey, regular path students had more family members who were health professionals than social quota students (p < 0.001). There were no significant differences regarding monthly income, job satisfaction, employment, or management activities.
Conclusion: Affirmative action targeted students with a disadvantaged socioeconomic background. Regular path students had a higher dropout rate than social quota students.
Keywords: medical school, medical education, affirmative action, public policy, social mobility, social marginalization
Introduction
The main reason for implementing affirmative action policies in higher education in several countries is to promote equality. Such policies are an instrument to provide access for students with a social vulnerability profile and promote social mobility.1–5 Especially since the 2000s, Brazilian public universities have implemented affirmative action policies to reduce inequality in higher education access, mainly through social and racial quotas.6–8 Social quotas are reserved for candidates with social vulnerability profiles due to low family income to promote equal opportunities. In contrast, racial quotas are reserved for racial groups. Both social and racial quotas have the same principle: eliminating unjust inequalities and unfair advantages.9
Notably, public universities are usually more prestigious in Brazil and have better scientific production than private universities. Indeed, Brazilian public universities have been regarded better in all national and international rankings than private universities; thus, undergraduate courses at public universities, which are also tuition-free, are in higher demand among students.1,8,10 In contrast to what is observed at the university level, at the primary and secondary education levels, Brazilian private schools display higher-quality education programs than public schools.1,8,10 Traditionally, Federal and state public universities use a regular path system based only on test scores to admit new students. Therefore, there is a higher approval rate for students from private schools, who tend to have better test scores.1,8,10
The under-representation of the less privileged classes is even more prominent for highly prestigious, public medical schools, which require students to have the highest entrance exam scores to be accepted.11 In Brazil, the medical schools traditionally followed the European structure, based on the six-year curriculum regulated by the Brazilian National Education Council. Until 2006, the Brazilian medical education system was mainly public, and the student selection process was based only on an admission test score, called vestibular. This system was replaced by the Brazilian Unified Selection System for Higher Education Institutions (SISU) and is based on students’ scores on the Brazilian National High School Exam (ENEM) in most Brazilian public universities nowadays. The ENEM is a national exam designed to assess students’ readiness for undergraduate courses, similar to the Scholastic Aptitude Test (SAT) in the United States. Additionally, in recent years, there has been a rapid increase in medical schools, primarily private, motivated by the Brazilian government to answer the societal needs of physicians. That led to a shift of public-based medical schools to predominately private ones from multinational private educational groups. The accessibility of payment usually prevails in the admission process in most private schools, further compromising the equity in access to the medical profession.12,13
Regardless of the possible benefits to socially advance historically disadvantaged minorities, the current affirmative action faces several issues related to whether the affirmative action policies in higher education have achieved their objectives (targeting), whether the affirmative action students can catch up the progress of knowledge of regular path students during the medical school, regardless of the initial gap between two groups, or they fall behind them when undergraduate (catch up), and whether academic damage is incurred due to the admission of less competitive students that are unprepared for the academic environment (minority mismatch hypothesis).8,12–18
In India, where the admissions had strict and binding quotas favoring scheduled castes and tribes rather than on income, affirmative action in higher education is similar to the racial quota system in Brazil.2,4,16,19,20 There is a serious concern whether these admission preferences displace poor students from the non-minorities groups or did not effectively target the highest disadvantaged students.16,19,20 In this respect, studies performed in Indian engineering schools showed that, even though caste-based targeting did not benefit the poorest students from the caste, the admissions were successfully reallocated for students from richer to poorer households.16,19
Out of all issues against the affirmative action policies, one of the most mentioned arguments is the minority mismatch hypothesis that defends affirmative action systems violate the merit principle. Hence, students admitted through affirmative action systems do not deserve a place in public higher education and cannot succeed in a competitive environment since they are not qualified for the undergraduate course. As evidenced by their entrance scores being lower than regular path students, this hypothesis is called minority mismatch.8,14–18 For those who defend this hypothesis, students admitted through affirmative action systems are likely to perform less well in undergraduate courses, take longer to finish their degree, and have a greater chance of dropping out. In addition, their deficits will affect their future professional performance.8,14–18
In the United States, Hinrichs showed that the removal of affirmative action students did not significantly impact overall graduation rates.21 A similar study in the United States by Alon and Tienda did not find evidence to support the minority mismatch hypothesis.22 A study conducted in India found that alumni from engineering schools admitted through a social quota system for underrepresented castes presented substantial benefits in the labor market after eight to ten years, despite their lower entrance exam scores.19 However, a study including students from an Indian prestigious engineering institution found that affirmative action students from scheduled caste and tribes had lower-income jobs than regular path students.16 As well as, a Malaysian study showed that affirmative action alumni experienced difficulty finding employment after graduation.23 In the context of this debate, mainly in the United States, universities have had to face extensive questions and legal battles, leading some institutions to ban race-conscious affirmative action policies.24–28
In medical schools, the arguments for and against affirmative action also have been the subject of vigorous debate, with studies showing contradictory results.29,30 Those who defend affirmative action policies argue that they may also positively promote student diversity since a lack of it may affect medical education. Some reports have shown that a racially and socioeconomically diverse student body in medical schools leads to doctors who are more conscious of and integrated with their patients’ desires and communities’ needs.24,31–33 A study carried out in a Brazilian medical school showed that candidates from affirmative action programs performed slightly better in medical school compared to other students.30 In contrast, another Brazilian study observed that affirmative action students achieved results modestly lower than regular path students in eight out of ten undergraduate courses, including medical school.29 Beyond the contradictory results, these studies did not evaluate the labor market outcomes between affirmative action and regular path students after medical school. Besides, most of them were performed in universities that adopted racial quota systems, not social quota systems.
In an era where diversity and equity in access to higher education are highly demanded and given all the questions regarding affirmative action policies, the success of these policies can be evaluated by several factors. Among them is the quality of performance of beneficiaries in the institutions to which they gain preferential access and in the labor market.16 Thus, the aim of the study was to compare students admitted through the regular path and social quota systems based on the “students” attendance in all primary and secondary education levels in the Federal District’s public education system, a surrogate of socioeconomic status, in a public medical school in Brazil regarding their academic trajectory (dropout rate and participation in an undergraduate scientific research program) and professional trajectory (admission in a medical residency program, job satisfaction, and monthly income after medical school). We also compared the socioeconomic background based on the place of residence at medical school admission (Human Development Index – HDI, per capita income and average household income) between the regular path and social quota students to evaluate whether the social quota system using the type of school effectively provides access for candidates with social vulnerability profiles. These results may clarify the contradictory results of previous studies and assess differences in the trajectories of regular path and social quota students even after medical school completion. It is essential to note that our study evaluated a social quota system in a Brazilian medical school that aims to promote the admission of students with vulnerability profiles due to low family income regardless of ethnicity and race.
Materials and Methods
Study Design and Participants
This transversal study included all students admitted to a medical school within the School of Health Sciences (ESCS), in Brazil, between 2005 and 2012, followed as a cohort until May 2020. ESCS is a public, higher education institution created in 2001 through the initiative of the State Department of Health of the Federal District, Brazil, that is structured based on the principles of the Brazilian Unified Health System (SUS), which offers medical and nursing tuition-free undergraduate courses. In all Brazilian medical schools, including ESCS, students need six years to complete, with a maximum of nine years. The curriculum is standard for all students and based on active teaching and learning methodologies with the activities developed in the Federal District’s public health system (a system-based curriculum).34–36
The student selection process occurs once a year through the SISU and is only based on “students” scores on the ENEM. The social quota system criterion is the attendance in all primary and secondary education levels in the Federal District’s public education system, a proxy for socioeconomic status, aiming to surpass the limited participation of minorities in the medical school. Each year, 80 students are admitted to the medical school within ESCS, 48 places for students admitted according to the best scores on the ENEM (regular path system) and 32 places reserved for students who completed all primary and secondary education levels in the Federal District’s public education system (social quota system) - also based only on these students’ scores on the ENEM (affirmative action system). It is essential to point out that the minimum score to be admitted in the regular path system is higher than the social quota system. Thus, all students who meet the criteria for the social quota system applied to it. This aspect is also observed in other public universities that adopt affirmative policies.14
The inclusion criterion was a student admitted to the medical school within ESCS between 2005 and 2012. The exclusion criteria were (1) students who were still attending medical school by the end of the follow-up period (May 2020) or (2) students admitted by mandatory transfer from other higher education institutions as determined by law (relatives of Brazilian public and military officials). Out of 712 students enrolled between the evaluated period, four were excluded because of mandatory transfer admission (0.4%), and one (from the regular path system) was excluded for not completing the course by the end of the follow-up period (0.1%); therefore, the study included 707 students. All students included in the study were followed up until May 2020.
Data Collection
In the first phase, data collection was carried out through analysis of documents from the ESCS academic management system, the Brazilian “researchers” curriculum directory on the Lattes Platform - Brazilian National Council for Scientific and Technological Development (CNPq - http://buscatextual.cnpq.br/buscatextual/busca.do), the medical residency academic management system of the National Medical Residency Commission System of the Brazilian Ministry of Health (SisCNRM - http://siscnrm.mec.gov.br/login/login#), publications in the Official Gazette of the Government of Federal District, Brazil (DODF - https://www.dodf.df.gov.br/), the Brazilian Institute of Geography and Statistics (https://www.ibge.gov.br/), and the register of the Brazilian Federal Medical Council (CFM - https://portal.cfm.org.br/index.php?option=com_medicos) the CFM registration is mandatory to work as a physician in Brazil.
In the research phase, the variables collected were sociodemographic characteristics, HDI in the place of residence at the time of medical school admission, per capita income and average household income at the time of medical school admission, admission system (regular path or affirmative action system), entrance examination scores, high school completion date, medical school start and completion dates, participation in an undergraduate scientific research program, whether dropped out before finishing the course, graduate from medical school at any institution (which includes the total number of students who graduated in Medicine at ESCS or other institution after transference), CFM registration, and admission to a medical residency program according to SisCNRM.
In the second phase, a survey with 12 questions was sent to the alumni from the medical school within ESCS, and 308 former students responded (43.6%). The minimum sample size for at least a 95% confidence interval and a 5% margin of error was 251 alumni. The variables collected were health professionals in the family, feeling fit to work at the end of medical school, whether received a scholarship for students experiencing social vulnerability during medical school, medical residency program admission exams taken, whether entered public service through a government job competition process, employment in the private health sector, management activity in the public or private health sector, monthly income, remuneration per hour worked, and job satisfaction degree (from 0 to 5 on a Likert scale).
Statistical Analysis
The variables’ distribution and their normality were checked using histograms, dispersion diagrams, and Kolmogorov–Smirnov and Shapiro–Wilk tests. Quantitative data are expressed as mean ± standard deviation (SD) or median and interquartile range (25–75%). Categorical variables are expressed as a percentage (%). The Student’s t-test or the Mann–Whitney test compared quantitative variables as appropriate. Contingency tables were used for categorical variables, and Pearson’s chi-square test (χ2) or Fisher’s exact tests were used as necessary. Binary logistic regression analysis with the enter method was performed to evaluate the variables that determine graduation and after graduation performance. In addition, the following binary dependent variables (coded as 0 or 1) were considered: (i) Dropout from medical school within ESCS; (ii) Non-graduation from medical school at any institution; and (iii) Admission to a medical residency program. Non-collinearity was accepted when the tolerance was higher than 0.10 and the variance inflation factor (VIF) was lower than 10.0. The independent variables included in the logit regression models were admission system, age, gender, marital status, time between high school completion and medical school admission, and entrance examination score. A p-value of < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS program, IBM version 23.0 for Mac.
Ethical Approval and Consent Form
The study was approved by the Ethics Committee of the Education and Research Foundation of Health Sciences (FEPECS), Brasília, Federal District, Brazil under the number 21324719.1.3001.5553. For the study’s first phase, the ethics committee waived the requirement for an informed consent form due to the retrospective study design. As for the second phase, all alumni have provided a written informed consent form. This study complies with the Declaration of Helsinki.
Results
The study included 707 students, 28.9% (204/707) from the social quota system and 71.1% (503/707) from the regular path system. The median age at the time of medical school admission was 19.0 years (IQ25–75%: 18.0–21.0 years), 52.3% (370/707) were female, and 2.4% (17/707) were married. Out of all students admitted during the study period, 13.7% (97/707) dropped out from medical school within ESCS, 8.6% (61/707) were transferred to another institution, and 0.4% (3/707) died. Thirty-six students did not complete medical school at any institution (5.1%). The median time to complete medical school was 6.0 years (IQ25–75%: 6.0–6.0 years). After medical school, 42.0% (256/610) of alumni attended a medical residency program (Table 1).
 |
Table 1 Baseline Data and Academic Trajectory During and After Medical School of Students Admitted to a Medical School Within the School of Health Sciences (ESCS), in Brazil, Between 2005 and 2012 |
Table 2 compares the students admitted from the regular path and social quota systems. In the univariate analysis, students from the social quota system were older at the time of medical school admission (p < 0.001), majority of them were married (p = 0.006) and had lower entrance examination scores than the students admitted from the regular path system (p < 0.001). The place of residence of social quota students at the time of medical school admission had lower HDI (p < 0.001), per capita income (p < 0.001), and average household income (p < 0.001) compared to regular path students. Social quota students had a longer delay between high school completion and medical school admission than regular path students (p < 0.001). More students from the regular path system (17.9%) dropped out from medical school within ESCS than students from the social quota system (3.4%, p < 0.001). Among the students who complete the medical school within ESCS, an increased percentage of regular path students attended a medical residency program (p = 0.001), and the time needed to complete medical school was higher in social quota students compared to regular path students (p < 0.001).
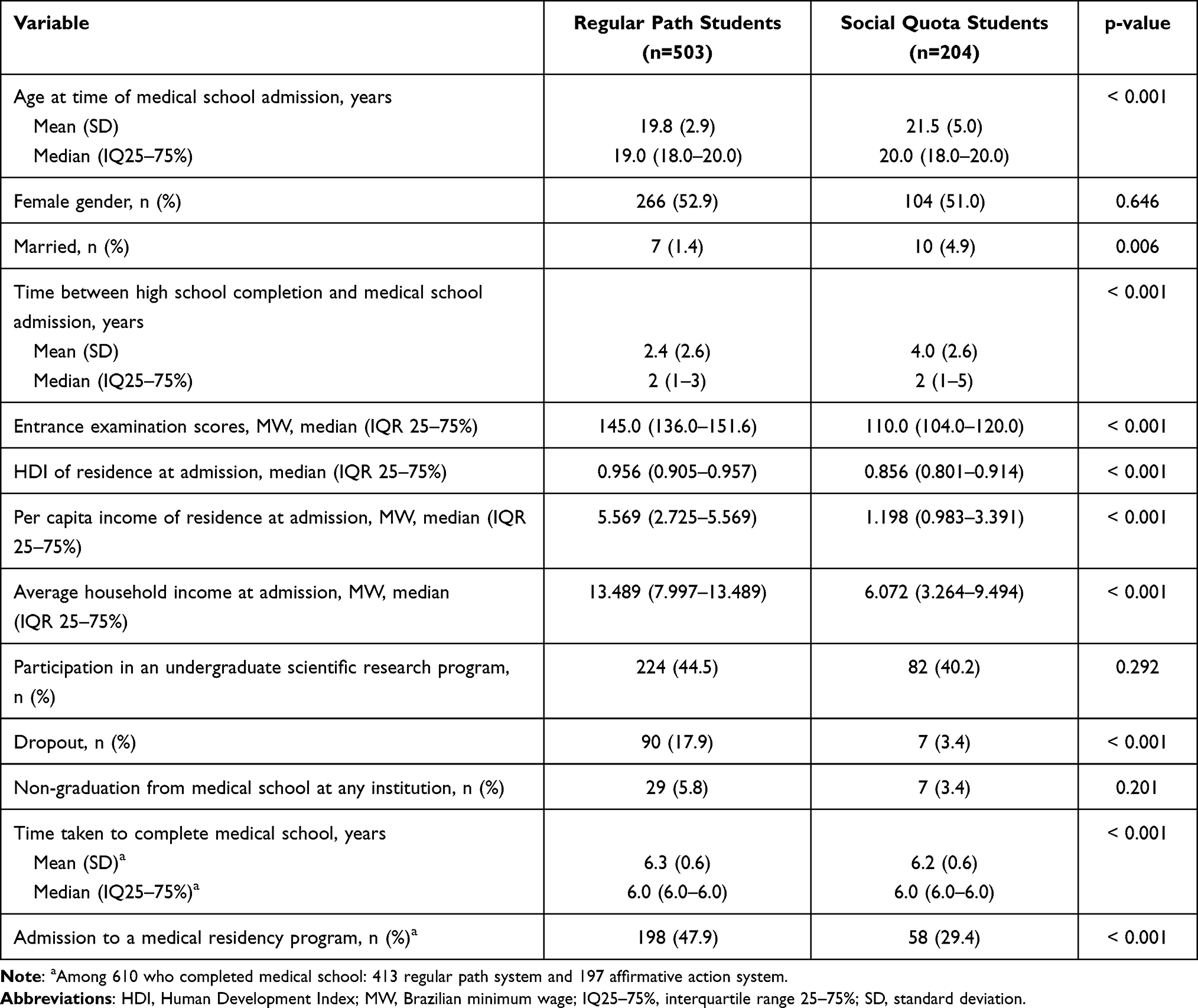 |
Table 2 Univariate Analysis Comparing Students Admitted to a Medical School Within the School of Health Sciences (ESCS) in Brazil, Between 2005 and 2012 Through Affirmative Action and Regular Path Systems |
Among the 604 regular path students, 202 students (30.4%) resided in towns outside the Federal District at the time of medical school admission.
Table 3 shows the multivariate analysis comparing students admitted through the regular path and affirmative action systems adjusted to gender, age, marital status, entrance examination scores, time between high school completion and medical school admission regarding the dropout rate from medical school within ESCS, non-completion students at any institution, participation in an undergraduate scientific research program, and the alumni admitted to a medical residency program. Admission from the regular path system was independently and positively associated with dropping out from medical school within ESCS (OR: 50.552, 95% CI: 12.438–205.453, p < 0.001), non-completion at any institution (OR: 111.533, 95% CI: 24.102–516.117, p < 0.001). Among the students who completed the medical school within ESCS, the type of admission system was not independently associated with attendance at a medical residency program (OR: 1.780, 95% CI: 0.957–3.309, p = 0.069).
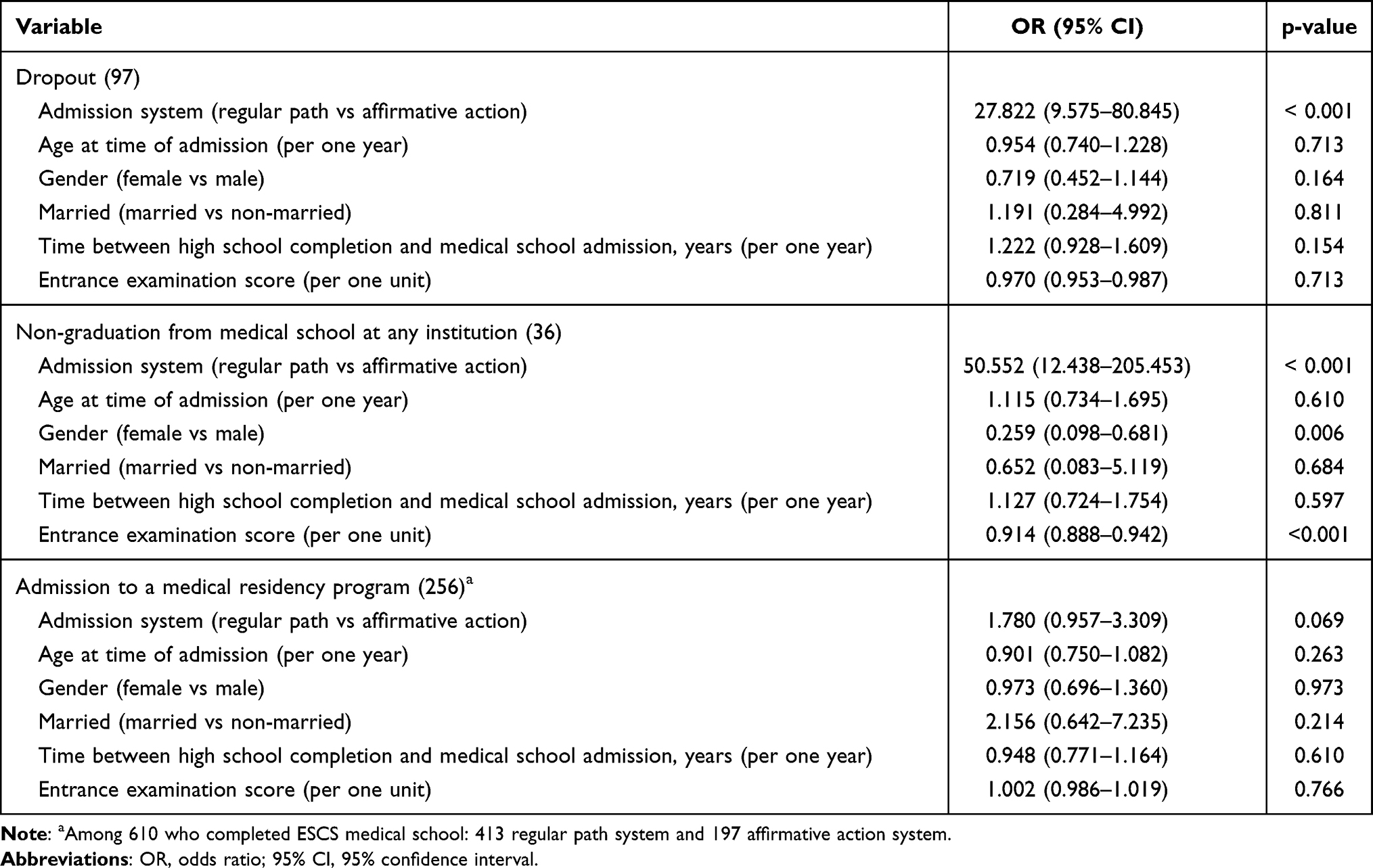 |
Table 3 Multivariate Analysis Regarding the Dropout Rate from a Medical School Within the School of Health Sciences (ESCS), Non-Graduation from Medical School at Any Institution, and Alumni Admission to a Medical Residency Program Among Students Admitted to a Medical School Within ESCS in Brazil, Between 2005 and 2012 |
Table 4 compares the responses to the survey given, and students from the regular path system had more family members who were health professionals (p < 0.001) and took more medical residency program admission exams (p < 0.001) than social quota students. Students experiencing social vulnerability from the affirmative action system received more scholarships than regular path students (p = 0.001). There were no statistically significant differences for the other items, such as job activities and satisfaction, monthly income, or feeling fit to work at SUS after finishing medical school.
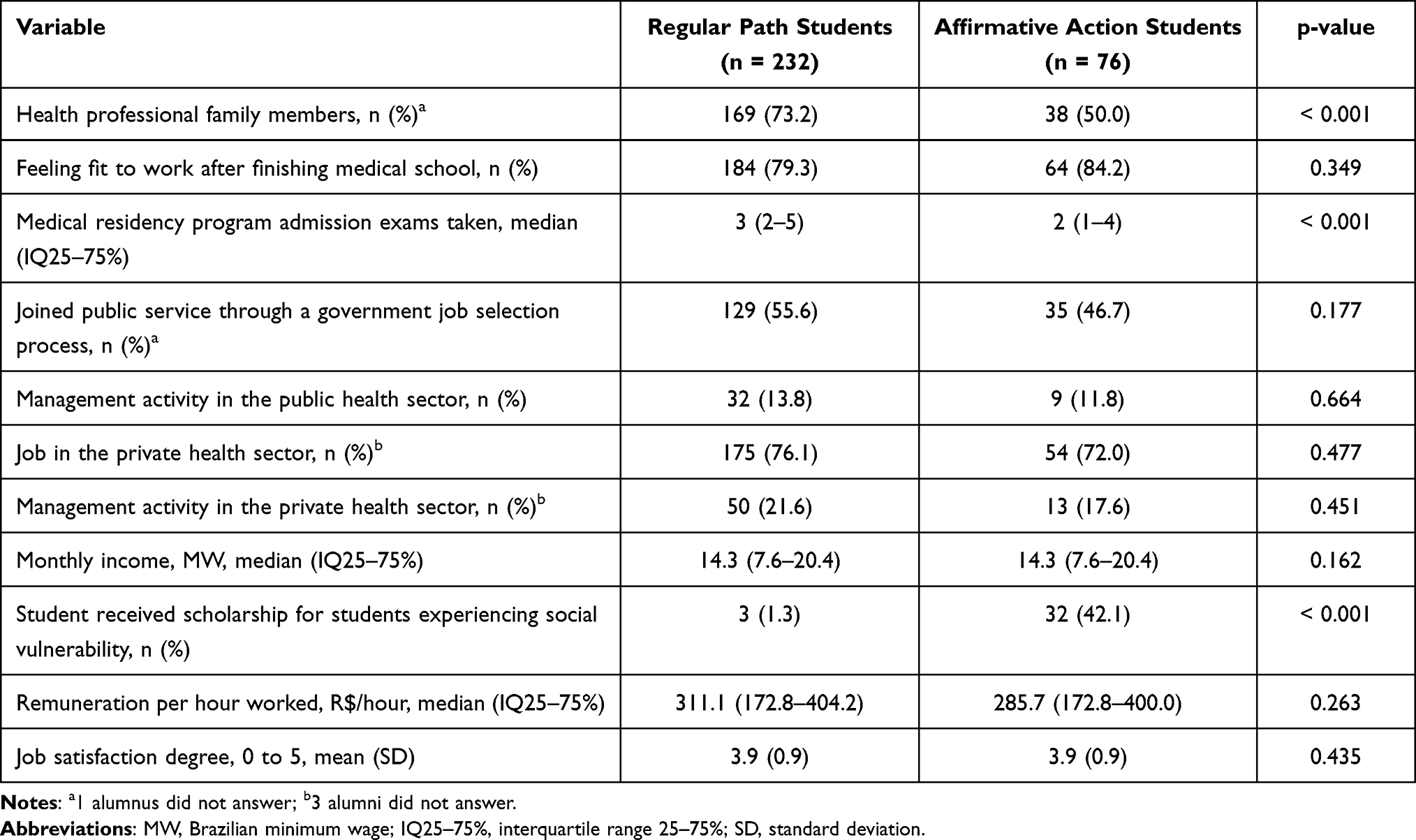 |
Table 4 Univariate Analysis Comparing the Survey Responses of Students Admitted from the Regular Path and Affirmative Action Systems |
Discussion
Affirmative action policies to provide access to higher education for students with a social vulnerability profile have been implemented in several countries to promote equal opportunities and social inclusion.1–5,37–39 Although about one-quarter of nations worldwide adopted some form of affirmative action police into higher education,37 these policies have faced many questions regarding the students’ performance when admitted to universities through this path and whether these policies effectively target genuinely disadvantaged students.8,14–18,29,40 The social quota system was able to target students who had disadvantaged socioeconomic status. In our study, the students evaluated were from a social quota system from a public medical school, based on the students’ attendance in all primary and secondary education levels in the public education system. In this case, social quota students showed lower HDI, per capita income, and average household income than regular path ones considering the place of residence at medical school admission.
Moreover, 42.1% of social quota students received a scholarship for students experiencing social vulnerability, a grant to support retaining and assisting students with monthly household income up to two Brazilian minimum wages. Conflicting with the minority mismatch hypothesis arguments that affirmative action students are less qualified, perform less well at university and in their future professional life, and to achieve high levels of excellence in higher education,8,14–18,29,40 our study observed a lower dropout rate from the medical school within ESCS for affirmative action students than regular path students. Even considering that students may have left the ESCS medical school due to transfer to other universities, regular path admission had a positive and independent association with non-graduation from medical school at any institution. Furthermore, there were no differences between alumni from these systems regarding job placement, management activities in the Brazilian public and private health sectors, and attendance to a medical residency program. Both groups earned similar monthly incomes. Despite social quota students showing a higher time to complete medical school than regular path students, the mean difference in time taken to undergraduate between these students was very close (about 0.1 years). It may also be influenced by a possible higher dropout rate of regular path students who had difficulty progressing in medical school.
A study carried out at the University of the State of Rio de Janeiro (UERJ), a public university in Brazil, showed similar results regarding the performance of affirmative action students in undergraduate courses. This study evaluated 49 undergraduate courses, and the affirmative action students had similar performance to the other students and showed lower dropout rates.40 Another Brazilian study analyzed the performance of affirmative action and regular students on the National Students Performance Exam (ENADE), which evaluates medical schools in Brazil. This study showed that affirmative action students perform similarly to regular path students in Brazilian public universities. In contrast, students admitted through affirmative action in Brazilian private universities perform slightly better than students admitted through the regular path.9 Another study at the public University of Campinas (Unicamp), in the State of São Paulo, Brazil, uses a system that adds points to admission test scores for students from public schools instead of reserving a specific percentage of admissions slots. The results showed that candidates from the affirmative action program performed slightly better in medical school than other students.30 In contrast, a study from the University of Brasília (UnB), Brazil, showed that affirmative action students had slightly lower academic performance than regular path students in eight out of ten highly selective undergraduate courses, including medical school.29
Indeed, one of the central aspects in evaluating the success or failure of an affirmative action policy and any other policy in higher education is the relationship between the number of students from eligible groups who complete and those who do not complete their education.16,20 Thus, in addition to providing access to higher education, it is crucial to guarantee the students’ permanence until they complete the course. This aspect has been an important issue in Brazil and other countries such as Argentina, with high dropout rates among university students.41 In this respect, our study showed higher medical school graduation from affirmative action students than regular path students, even considering that students may have left the medical school within ESCS due to transfer to other universities. Supporting our results, previous Brazilian studies performed at Rio de Janeiro State University40 and the University of Brasília29 also showed that regular path students had higher dropout rates than affirmative action students. A similar finding was observed in a study performed in the United States, where students who benefited from affirmative action policies left school at lower rates than others.4 An explanation for this finding was not examined in the present study. It is conceivable that regular path students had more opportunities to transfer to other federal public universities, usually ones with a better rating among higher education institutions in Brazil, and feel safer searching for a new career.
On the other hand, considering that affirmative action students have fewer opportunities than regular students, it is possible that they feel insecure about discontinuing the medical course. Our study demonstrated that affirmative action students were more experienced, admitted at an older age, and had a longer gap between high school and higher education. A higher proportion of them had already completed other undergraduate courses. Together with the prospect of improved socioeconomic status after graduation, these factors may explain affirmative action students’ greater resilience when facing the difficulties of medical school, resulting in a lower dropout rate. Nevertheless, new studies are necessary to address these hypotheses. Another consideration is that affirmative action students have more difficulty performing academic activities than regular path students, such as writing reports and scientific research. In our study, there were no significant differences between the social and regular path students’ participation in an undergraduate scientific research program, a voluntary extracurricular activity that aims to develop students’ scientific critical analysis and technological knowledge,42 which contradicts the argument that affirmative action students poorly performed in academic activities.
An important issue and common aspect in Latin American countries is the unequal admission in higher education that prevents social mobility, with a concentration of students from high-income families including an intergenerational context.14,38,39,41,43 In our study, regular path students had more family members who were health professionals than social quota studies. Brazilian medical schools are traditionally attended by whites and students with higher family income and whose parents have a college degree,9 as seen in other countries like the United States and Latin America.33,38,39,41,44,45 Commonly, most medical students have physician relatives, mostly parents,46,47 and tend to maintain the same social groups in medical school. This indicates the difficulty of being admitted to medical school that students from the most vulnerable social classes face without affirmative action policies.
Moreover, affirmative action students are usually the first in their families to attend a university, showing the importance of affirmative action as a social mobility tool in many cases. Indeed, a study carried out in a Brazilian medical school showed that more black students had parents with a low level of schooling than white students (54.5% of black students had no parent with a higher education degree, compared with 16.1% of white students).9 Several Latin American countries proposed reforms in their national higher education systems last decades to overcome this context, aiming to promote access and equity in higher education. Among these initiatives, there are affirmative action policies that aim to increase enrolment in universities among low-income groups and racial and cultural minorities rolled out in Argentina, Bolivia, Brazil, Chile, Colombia, Peru, the Dominican Republic, and Venezuela. However, most governments use financial instruments, such as scholarships and students loans, rather than direct interferes in the university admission system.8,39,48 Argentina has quite open and unrestricted access to higher education, but with a high dropout rate. So, in Argentina, affirmative action policies should focus on increasing student retention in universities rather than providing admission in universities, which is the focus of the social quota system.41 On the other hand, in Bolivia, the affirmative action policy to promote access to minorities in higher education is not based on quotas but on implementing specific institutions for indigenous populations. For example, the Intercultural Community Indigenous Universities offer undergraduate programs in fields considered relevant to the indigenous communities. Although the first universities started in 2009, the indigenous participation among the Bolivian students attended universities was only about 0.5% in 2013, showing that the policy still had not yet achieved a significant impact on the Bolivian higher education system.39,48
An important issue of the social quota admission system is to assess the ability to promote the inclusion of students from minorities groups, that is, the target question. Regarding the student’s socioeconomic background, the social quota students lived in places with lower HDI, average household income, and per capita income than regular path students at medical school admission. Furthermore, 32 of 76 social quota students received a scholarship for students experiencing social vulnerability in the survey sample. The role of the social quota system as an instrument to surpass the socioeconomic status boundaries in access to medical education was also demonstrated by the higher age of the affirmative action students compared to regular path students at attendance, as well as the increased duration between completing high school and attending medical school. In the Federal District, Brazil, only two among six medical schools are public (ESCS and the University of Brasília). These few vacancies available in the public education system make it difficult for students from less privileged social classes to access medical schools and explain why the quota students were older than non-quota students in the present study. This fact is even worse due to the impossibility of these students carrying out admission exams in other towns due to the lack of financial support and, even, to the competition with students from towns outside the Federal District in the regular path system. In this aspect, it is essential to note that 30.4% of regular path students resided in towns outside the Federal District at the medical school admission in our study. Indeed, the capability of affirmative action to promote equality in higher education by redistributing university admission slots for the most vulnerable students has been illustrated in different studies, whether by racial or social quota.14,16,19,20 In a study conducted at the University of Brasília, Brazil, black students from the racial quota system reported lower family incomes, parenteral educational levels, and higher attendance at a public secondary school than students from the regular admission system.14 In India, studies analyzing the quota system for underrepresented castes in engineering schools observed that affirmative action policies significantly improve the admission of the poorest students.16,19
In our study, although regular path students had increased admission to a medical residency program in the univariate analysis, there was no significant difference between regular path and social quota students regarding attendance to the medical residency program in the multivariate analysis. At first glance, it was expected that affirmative action students had a lower attendance at medical residency programs since there is high competitiveness of medical residency program admission exams due to the low number of vacancies in Brazilian medical residency programs in relation to the number of newly graduated physicians each year.12,49,50 These aspect leads medical students to seek high-cost private preparatory courses. These courses are fairly expensive, and they cost approximately twice the value of the annual minimum wage income, which corresponds to approximately US $197.00.49 This cost is relatively high for students who come from less privileged classes, the case of most students who have accessed the university through an affirmative action system.
Additionally, in Brazil, there is no national residency exam, so the tests are carried out and located in different towns in which the programs are developed, and those who have less financial support do not have the opportunity to take multiple tests.50 Indeed, in our study, the number of medical residency admission exams was lower among the affirmative action students. Besides, only 42.0% of medical school students attended a medical residency program. It is important to note that medical residency is not mandatory to work as a physician in Brazil. There are other ways to obtain a degree in a medical specialty, such as exams carried out by specialist societies.12,51 Indeed, approximately 30% to 40% of physicians in Brazil do not have a medical specialty.12,51 The high demand for physicians in the health services and the certification exams of specialist societies may lead to physicians without medical residency training having similar job opportunities as those who attend a medical residency program.51 In addition, the grants of medical residents are less generous than the wages offered to recent medical graduate students in the health care system for jobs that do not require medical residency.52 The opportunity includes military service as a physician, which does not require specialization. These employment opportunities may help students look for a faster way to improve their financial situation.
Studies evaluating alumni from affirmative action tracks in education are still scarce, especially those concerning employment after graduation. In the survey in our study, although there was a higher enrolment rate in medical residency programs favoring regular path students, there was no difference between a social quota and non-quota students regarding monthly income, job satisfaction, employment, and management activities in the Brazilian public and private health sector. As mentioned above, physicians without residency training have similar job opportunities as those who do a medical residency. Several issues may contribute to these results. The demand for physicians in Brazil is extremely high.12,52–54 For example, the More Doctors Programme encourages foreign physicians to come to Brazil, mainly Cuba, to enhance healthcare access for the population in regions with shortages, particularly small and distant-from-state-capital municipalities.12,52–54 Nevertheless, we do not know whether the similarities between the two groups will remain in the long term, and it is plausible that differences will emerge.
In Malaysia, a study showed that most graduates of public higher education institutions who benefitted from affirmative action policies experienced difficulties in being employed in occupations that match their qualifications, even within affirmative action in public sector employment.23 However, unlike in Malaysia, Brazilian public schools have the most prestige.1,8,10 Furthermore, the evaluated undergraduate course in our study is a medical school, which presents high social prestige, making it easy to get a job.
Among the limitations, our study evaluated students from only one medical school in Brazil, so further studies performed in other medical institutions are needed to confirm our results. As documentary data were used in the first phase, some relevant variables for evaluating affirmative action and regular path students could not be obtained. The convenience sample in the second phase may selectively include a higher proportion of students interested in the study topic. Our study results should be interpreted in the context of medical education and a Brazilian public education institution with its specificities and characteristics, such as the high prestige accorded to public universities in Brazil. Beyond these limitations, our results may clarify the contradictory results of previous studies that evaluated affirmative action policies in medical education, assessing the differences in trajectories of the students from the regular path and social quota systems even after completing the undergraduate course. Besides, most of the studies did not evaluate the labor market outcomes between affirmative action and regular path students, especially after medical school, and majority of them were performed in universities that adopted racial quota systems.
Conclusion
In our study, affirmative action targeted students with a disadvantaged socioeconomic background with reduced HDI, per capita income, and average household income at medical school admission. There was a higher dropout and non-graduation from medical school at any institution among regular path action students. In the short term, after graduation, there were no significant differences between the regular path and affirmative action alumni regarding attendance at medical residency programs, monthly income, job satisfaction, employment, and management activities in the Brazilian public and private health sectors. These results contradict the minority mismatch hypothesis and support affirmative action as an instrument to promote diversity and equity in access to higher education, especially a highly demanded undergraduate course, such as Medical School.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Schwartzman LF, Paiva AR. Not just racial quotas: affirmative action in Brazilian higher education 10 years later. Br J Sociol Educ. 2014;37(4):548–566. doi:10.1080/01425692.2014.973015
2. Jenkins LD. Identity and Identification in India: Defining the Disadvantaged. London: Routledge; 2003.
3. Kahlenberg RD. America’s Untapped Resource: Low-Income Students in Higher Education. New York: The Century Foundation Press; 2004.
4. de Zwart F. The logic of affirmative action: caste, class and quotas in India. Acta Sociol. 2016;43(3):235–249. doi:10.1177/000169930004300304
5. Lee PR, Franks PE. Diversity in US Medical Schools: Revitalizing Efforts to Increase Diversity in a Changing Context, 1960s–2000s. San Francisco: Institute for Health Policy Studies; 2010.
6. McCowan T. Expansion without equity: an analysis of current policy on access to higher education in Brazil. High Educ. 2007;53(5):579–598. doi:10.1007/s10734-005-0097-4
7. Marteleto LJ. Educational inequality by race in Brazil, 1982–2007: structural changes and shifts in racial classification. Demography. 2012;49(1):337–358. doi:10.1007/s13524-011-0084-6
8. De Oliveira CT, Haddad EJ, Dias ACG, et al. Closing the gap: affirmative action and college adjustment in Brazilian undergraduate universities. J Coll Stud Dev. 2018;59(3):347–358. doi:10.1353/csd.2018.0031
9. Valente RR, Berry BJL. Performance of students admitted through affirmative action in Brazil. Lat Am Res Rev. 2017;52(1):18–34. doi:10.25222/larr.50
10. Lee JH. Policy and ideology collide: an examination of affirmative action for students of Brazilian public higher education. Race Ethn Educ. 2020;24(1):39–55. doi:10.1080/13613324.2020.1753673
11. Souza PGA, Pôrto ACCA, Souza A, et al. Socio-economic and racial profile of medical students from a public university in Rio de Janeiro, Brazil. Rev Bras Educ Méd. 2020;44:e090.
12. Scheffer MC, Pastor-Valero M, Cassenote AJF, Compan Rosique AF. How many and which physicians? A comparative study of the evolution of the supply of physicians and specialist training in Brazil and Spain. Hum Resour Health. 2020;18(1):30. doi:10.1186/s12960-020-00472-0
13. Dos santos RA, Nunes MDPT. Medical education in Brazil. Med Teach. 2019;41(10):1106–1111. doi:10.1080/0142159X.2019.1636955
14. Francis AM, Tannuri-Pianto M. The redistributive equity of affirmative action: exploring the role of race, socioeconomic status, and gender in college admissions. Econ Educ Rev. 2012;31(1):45–55. doi:10.1016/j.econedurev.2011.08.005
15. Aberson CL. Diversity experiences predict changes in attitudes toward affirmative action. Cultur Divers Ethnic Minor Psychol. 2007;13(4):285–294. doi:10.1037/1099-9809.13.4.285
16. Frisancho V, Krishna K. Affirmative action in higher education in India: targeting, catch up, and mismatch. High Educ. 2016;71(5):611–649. doi:10.1007/s10734-015-9927-1
17. Tierney WG. Merit and affirmative action in education. Urban Educ. 2016;42(5):385–402. doi:10.1177/0042085907304911
18. Heriot G. Just say no to affirmative action. Acad Quest. 2011;24(4):449–466. doi:10.1007/s12129-011-9257-4
19. Bertrand M, Rema H, Sendhil M. Affirmative action in education: evidence from engineering college admissions in India. J Public Econ. 2010;94(1–2):16–29. doi:10.1016/j.jpubeco.2009.11.003
20. Weisskopf TE. Affirmative Action in the United States and India: A Comparative Perspective. London: Routledge; 2004.
21. Hinrichs P. Affirmative action bans and college graduation rates. Econ Educ Rev. 2014;42:43–52. doi:10.1016/j.econedurev.2014.06.005
22. Alon S, Tienda M. Assessing the “mismatch” hypothesis: differences in college graduation rates by institutional selectivity. Sociol Educ. 2016;78(4):294–315. doi:10.1177/003804070507800402
23. Hwok-Lee A. Affirmative action in Malaysia: education and employment outcomes since the 1990s. J Contemp Asia. 2012;42(2):230–254. doi:10.1080/09500782.2012.668350
24. Cohen JJ. The consequences of premature abandonment of affirmative action in medical school admissions. JAMA. 2003;289(9):1143–1149. doi:10.1001/jama.289.9.1143
25. Mickey-Pabello D, Garces LM. Addressing racial health inequities: understanding the impact of affirmative action bans on applications and admissions in medical schools. Am J Educ. 2018;125(1):79–108. doi:10.1086/699813
26. Garces LM, Mickey-Pabello D. Racial diversity in the medical profession: the impact of affirmative action bans on underrepresented student of color matriculation in medical schools. J Higher Educ. 2015;86(2):264–294. doi:10.1353/jhe.2015.0009
27. Kaufmann SW. The history and impact of state initiatives to eliminate affirmative action. New Dir Teach Learn. 2007;2007(111):3–9. doi:10.1002/tl.280
28. Sterrett WM. Current issues involving affirmative action and higher education. J Coll Admission. 2005;187:22–28.
29. Velloso J. Quota and non-quota system: performance of students at university of Brasília. Cad Pesqui. 2009;39(137):621–644. doi:10.1590/S0100-15742009000200014
30. Childs P, Stromquist NP. Academic and diversity consequences of affirmative action in Brazil. Int J Comp Educ Dev. 2014;45:792–813.
31. Guiton G, Chang MJ, Wilkerson L. Student body diversity: relationship to medical students’ experiences and attitudes. Acad Med. 2007;82:S85–S88. doi:10.1097/ACM.0b013e31813ffe1e
32. Saha S, Guiton G, Wimmers PF, Wilkerson L. Student body racial and ethnic composition and diversity-related outcomes in US medical schools. JAMA. 2008;300(10):1135–1145. doi:10.1001/jama.300.10.1135
33. Bollinger LC. The need for diversity in higher education. Acad Med. 2003;78(5):431–436. doi:10.1097/00001888-200305000-00002
34. Amorim FF, Santana LA, Gottems LBD. Stricto sensu postgraduate education in the Brazilian Federal District: the experience of the higher school of health sciences (ESCS). Cien Saude Colet. 2019;24(6):2203–2210. doi:10.1590/1413-81232018246.08422019
35. Göttems LBD, Almeida MO, Raggio AMB, Bittencourt RJ. The unified health system in the federal district, Brazil (1960 to 2018): revisiting history to plan the future. Cien Saude Colet. 2019;24(6):1997–2008. doi:10.1590/1413-81232018246.08522019
36. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–1958. doi:10.1016/S0140-6736(10)61854-5
37. Jenkins LD, Moses MS. Affirmative Action Initiatives Around the World. Int High Educ. 2014;77(77):5–6. doi:10.6017/ihe.2014.77.5672
38. Bernasconi A, Celis S. Higher education reforms: Latin America in comparative perspective. Educ Policy Anal Arch. 2017;25:67. doi:10.14507/epaa.25.3240
39. Villalobos C, Treviño E, Wyman I, Scheele J. Social justice debate and college access in Latin America: merit or Need? The role of educational institutions and states in broadening access to higher education in the region. Educ Policy Anal Arch. 2017;25:73. doi:10.14507/epaa.25.2879
40. Cicaló GA. What do we know about quotas? Data and considerations about the implementation of the quota system in the state university of Rio de Janeiro (UERJ). Univ Humanist. 2008;65:262–280.
41. Vargas HM, Heringer R. Student retention policies in public higher education in comparative perspective: Argentina, Brazil and Chile. Educ Policy Anal Arch. 2017;25:72. doi:10.14507/epaa.25.2799
42. Amorim FF, Santana LA, Toledo IL, et al. Undergraduate research in medical education. Rev Assoc Med Bras. 2017;63(12):1017–1018. doi:10.1590/1806-9282.63.12.1017
43. Gomes MR, da Cunha MS, De souza SCI, Mourão PJR. About sad legacies: a study of the intergenerational occupational legacy in Brazil. Int J Manpow. 2021;42(4):702–731. doi:10.1108/IJM-04-2020-0156
44. Thernstrom S. Farewell to preferences? Public Interest. 1998;130:34–49.
45. Carnevale AP, Rose SJ. Socioeconomic Status, Race/Ethnicity and Selective College Admissions. New York: The Century Foundation Press; 2003.
46. Filho WRC, Ribeiro VMB. Premature choice of speciality by medicine students: a challenge for medical education. Rev Bras Educ Méd. 2004;28:133–144.
47. Filisbino MA, Moraes VA. Undergraduate medical education and professional practice from a student’s perspective. Rev Bras Educ Méd. 2013;37(4):540–548. doi:10.1590/S0100-55022013000400009
48. Brunner JJ, Villalobos C. Políticas de educación superior en Iberoamérica [Higher education policies in Iberoamerica], 2009–2013. Santiago: Universidad Diego Portales; 2014.
49. Hamamoto Filho PT, Zeferino AMB. Preparatory courses for medical residency: reflections on possible causes and consequences. Rev Bras Educ Méd. 2011;35(4):550–556. doi:10.1590/S0100-55022011000400015
50. Chaves HL, Borges LB, Guimarães DC, Cavalcanti LPG. Medical residency vacancies in Brazil: where to apply and what is assessed. Rev Bras Educ Méd. 2013;37(4):557–565. doi:10.1590/S0100-55022013000400011
51. Feuerwerker L. Mudanças na educação médica e residência médica no Brasil [Changes in medical education and medical residency in Brazil]. Interface. 1998;2(3):51–71. doi:10.1590/S1414-32831998000200005
52. da Silva EN, Ramos MC, Santos W, et al. Cost of providing doctors in remote and vulnerable areas: programa Mais Medicos in Brazil. Rev Panam Salud Publica. 2018;42:e11. doi:10.26633/RPSP.2018.11
53. Santos LM, Oliveira A, Trindade JS, et al. Implementation research: towards universal health coverage with more doctors in Brazil. Bull World Health Organ. 2017;95(2):103–112. doi:10.2471/BLT.16.178236
54. Maffioli EM, Hernandes Rocha TA, Vivas G, et al. Addressing inequalities in medical workforce distribution: evidence from a quasi-experimental study in Brazil. BMJ Glob Health. 2019;4(6):e001827. doi:10.1136/bmjgh-2019-001827
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.