Back to Journals » Clinical Ophthalmology » Volume 20
Comparative Outcomes of Standalone Xen63 Gel Stent and Preserflo Microshunt Implantation: A Multicenter Study
Authors De Francesco T ![]() , Zhang HA
, Zhang HA ![]() , Costa VP, Ahmed IIK
, Costa VP, Ahmed IIK ![]()
Received 15 February 2026
Accepted for publication 27 April 2026
Published 12 June 2026 Volume 2026:20 603751
DOI https://doi.org/10.2147/OPTH.S603751
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Ticiana De Francesco,1– 4 Huixin Anna Zhang,5– 7 Vital P Costa,2 Iqbal Ike K Ahmed1,5,8
1John A. Moran Eye Center, University of Utah, Salt Lake City, UT, USA; 2Department of Ophthalmology and Otorhinolaryngology, University of Campinas, Campinas, Sao Paulo, Brazil; 3Clinica de Olhos De Francesco, Fortaleza, Ceara, Brazil; 4Hospital de Olhos Leiria de Andrade, Fortaleza, Ceara, Brazil; 5Prism Eye Institute, Mississauga, ON, Canada; 6Department of Ophthalmology and Otolaryngology, Laval University, Quebec City, QC, Canada; 7Ophthalmology University Center, Saint-Sacrement Hospital, CHU de Québec, Quebec City, QC, Canada; 8Department of Ophthalmology and Vision Sciences, University of Toronto, Toronto, ON, Canada
Correspondence: Ticiana De Francesco, John A. Moran Eye Center, University of Utah, 65 Mario Capecchi Dr, Salt Lake City, UT, 84132, USA, Tel +1 801 581 2352, Email [email protected]
Purpose: To evaluate the intraocular pressure (IOP)-lowering efficacy and adverse event profile of Xen63 gel stent compared to the Preserflo microshunt.
Methods: Retrospective, multicenter, two-arm cohort study comparing 65 eyes undergoing standalone Xen63 implantation and 75 eyes undergoing standalone Preserflo implantation, all with intraoperative mitomycin C (MMC). Primary outcome was complete success, defined as all of the followings: 1) no two consecutive IOP readings > 17mmHg, 2) ≥ 20% IOP reduction from baseline; 3) no clinical hypotony (IOP < 6 mmHg associated with loss of ≥ 2 lines of vision); and 4) no use of glaucoma medications. Secondary outcomes included success at different IOP cut offs, qualified success (allowing medications), change in IOP, medications, complications, interventions, and re-operations.
Results: At 12 months, complete success was achieved in 61.5% of eyes in the Xen63 group and 73.9% in the Preserflo group (p = 0.13). Postoperative complications were more frequent in the Xen63 group compared with the Preserflo group (61.5% vs. 29.3%, p = 0.0002). Postoperative interventions were required at similar rates between groups (Xen63 30.8% vs. Preserflo 28.0%, p = 0.85); however, reoperations were performed more frequently in the Xen63 group (16.9% vs. 4.0%, p = 0.01). Non-Caucasian ethnicity was associated with an increased risk of surgical failure (HR 2.57; 95% CI, 1.26– 5.23).
Conclusion: Both devices achieved comparable success rates, median IOP reduction, and postoperative medication burden; however, the Xen63 group experienced a higher rate of complications and reoperations.
Keywords: glaucoma, SIBS microshunt, gelatin microstent, filtering surgery
Introduction
Microinvasive glaucoma surgery (MIGS) comprises a group of surgical procedures developed to reduce intraocular pressure (IOP) through minimally traumatic and physiologic mechanisms.1 As an extension of this concept, microinvasive bleb surgery (MIBS) was introduced to provide greater IOP reduction than MIGS while creating a controlled subconjunctival filtration pathway with a lower risk of hypotony compared with conventional filtering surgery.2–4 These devices are microlumen implants designed according to the Hagen–Poiseuille equation, enabling IOP reduction approaching that of trabeculectomy while mitigating hypotony-related complications.5,6 In addition to limiting hypotony, MIBS devices aim to simplify and standardize surgical techniques, thereby reducing postoperative complication rates and increasing predictability.
Currently, two MIBS devices are widely available: the Preserflo Microshunt and the Xen Gel Stent. The Preserflo Microshunt (Santen Pharmaceutical Co., Osaka, Japan) is an ab externo, bleb-forming device composed of poly(styrene-block-isobutylene-block-styrene) (SIBS), a highly biocompatible polymer associated with minimal inflammation and fibrosis.7 The device is 8.5mm in length, has a 70-µm lumen, and diverts aqueous humor directly to the subconjunctival space, thereby bypassing the conventional outflow pathways.8
The Xen Gel Stent (AbbVie, North Chicago, IL) is a 6 mm-long device designed to be implanted via an ab interno approach and that also facilitates subconjunctival filtration. It consists of a hydrophilic, porcine-derived gelatin tube cross-linked with glutaraldehyde, providing structural stability, biocompatibility, and minimal tissue reaction.9 Two models are commercially available: the Xen45, with a 45-µm lumen, and the Xen63, with a larger 63-µm lumen.10 The Xen45 has been globally available for over a decade, whereas the XEN63 was introduced more recently within the last 5 years.
Previous studies have demonstrated favorable IOP-lowering outcomes for both devices.11–15 Small retrospective comparisons between Preserflo and Xen45 have reported greater IOP reduction with Preserflo and some reported lower rates of hypotony-related complications with Xen45, although many were underpowered to demonstrate statistically significant differences.16–19 Additionally, comparative studies between Xen45 and Xen63 have reported superior IOP reduction and higher surgical success rates with the Xen63, albeit with a higher incidence of hypotony-related complications.10,20
Given the similar theoretical outflow resistance between Xen63 and Preserflo, these devices may represent more physiologically comparable subconjunctival filtration systems than Xen45.21 This raises a clinically relevant question as to whether comparable efficacy can be achieved, and whether differences in design and implantation approach influence the balance between IOP reduction and safety.
Although studies have compared Xen45 and Preserflo,16–19 and only limited data exist comparing Xen63 and PreserFlo,22 direct comparative evidence remains scarce, with existing studies often restricted by small sample sizes, single-center design, and the inclusion of both standalone and combined procedures.
The present study addresses this gap by reporting the largest multicenter comparison to date of standalone Preserflo Microshunt and Xen63 Gel Stent implantation. The primary objective was to compare the surgical success and adverse event profile of the Xen63 gel stent versus Preserflo microshunt implantation at 12 months.
Materials and Methods
This investigator-initiated, multicenter, retrospective, interventional cohort study evaluated consecutive patients undergoing standalone Preserflo Microshunt or Xen63 Gel Stent implantation with intraoperative mitomycin C (MMC). Surgeries were performed between 2015 and 2024 at academic ophthalmology centers in Canada, Italy, Austria, the Netherlands, Belgium, Singapore, and the Dominican Republic. The study adhered to the tenets of the Declaration of Helsinki. Institutional review board approval was obtained from University of Toronto (#48676), and all local regulatory requirements were met. All patients provided written informed consent for surgical intervention.
Inclusion and Exclusion Criteria
Consecutive glaucomatous eyes were included if they demonstrated IOP above target and/or documented disease progression despite maximally tolerated medical therapy (MTMT) and underwent a standalone Xen63 Gel Stent or Preserflo Microshunt implantation. Eyes were excluded if they had undergone prior filtering glaucoma surgery, if the procedure was combined with phacoemulsification, or if follow-up was less than 1 month.
Baseline demographic data collected included age, sex, eye laterality, ethnicity, and diabetes status. Baseline ocular characteristics included best-corrected visual acuity, decision IOP (defined as the IOP at which surgical intervention was elected), number of glaucoma medications, glaucoma diagnosis and severity, cup-to-disc ratio, visual field mean deviation, prior cataract surgery, prior ocular surgery, and history of laser trabeculoplasty.
Surgical Procedure
Xen63 Gel Stent
The Gel Stent was implanted using an ab interno approach, performed either with a closed- or open-conjunctiva technique, at the discretion of the surgeon. For the closed-conjunctiva ab interno approach, the injector was introduced into the anterior chamber (AC) through a clear corneal incision and directed toward the superonasal quadrant just anterior to the pigmented trabecular meshwork. The needle was advanced through the sclera to create a scleral tunnel with the distal end exiting into the sub-Tenon’s space approximately 2.0–2.5 mm posterior to the limbus. An intra-Tenon injection of 0.1 mL MMC was used. Primary needling was done at the surgeon’s discretion.
For the open-conjunctiva ab interno approach, a superior fornix-based conjunctival peritomy was created, and Tenon’s capsule was bluntly dissected from the sclera. MMC-soaked sponges were placed in the sub-Tenon’s space for 2 minutes. The XEN63 was then implanted ab interno using the same technique described above. The AC was pressurized with BSS to confirm flow through the implant. Tenon’s capsule and conjunctiva were closed, and a watertight bleb was confirmed.
Preserflo Microshunt
The Preserflo Microshunt was implanted using a standardized ab externo approach. A 6-mm fornix-based conjunctival peritomy with blunt dissection of Tenon’s capsule was performed. MMC-soaked Merocel sponges were applied beneath Tenon’s capsule for 2 minutes. A scleral mark was placed approximately 3 mm posterior to the limbus, and a 1-mm-wide scleral tunnel was created with a microknife, entering the AC at the level of the trabecular meshwork. The SIBS microshunt was inserted into the tunnel. Flow through the distal end of the device was verified by pressurizing the AC with BSS. Tenon’s capsule and conjunctiva were closed, and bleb formation was confirmed.
Mitomycin C Use
Mitomycin C dosing for both procedures was determined at the discretion of the surgeon and varied between 0.1 and 0.4 mg/mL.
Postoperative Management
Postoperatively, all glaucoma medications were discontinued. Patients were prescribed topical steroids every 2 hours during the first postoperative week, followed by a gradual taper over 8 to 10 weeks. Topical antibiotics were administered for 1 week. Follow-up visits occurred on postoperative day 1, postoperative day 3 or 4, and subsequently at the discretion of the treating surgeon. Postoperative management, including reintroduction of glaucoma medications, needling procedures, digital ocular compression, anterior chamber reformation, surgical revisions, or reoperations, was performed at the surgeon’s discretion.
Primary Outcome
The primary outcome measure was surgical success at 12 months. Complete success criteria are in line with the World Glaucoma Association Guidelines on Design and Reporting of Glaucoma Surgical Trials,23 defined as: (1) absence of two consecutive IOP measurements >17 mmHg; (2) at least a 20% reduction from decision IOP; (3) no clinical hypotony, defined as IOP <6 mmHg associated with a loss of ≥2 lines of visual acuity from baseline; and (4) no use of glaucoma medications. Qualified success met the same criteria but allowed the use of glaucoma medications. Surgical revision, reoperation, or loss of light perception vision were considered immediate failures. Out-of-range IOP values or medication use during the first postoperative month were not classified as failures, nor were in-clinic interventions such as needling.
Secondary Outcomes
Secondary outcomes included complete and qualified success using alternative upper IOP thresholds of 14 mmHg and 21 mmHg while maintaining a minimum 20% IOP reduction from baseline. Additional secondary outcomes included adjusted hazard rations (HR) for surgical failure of Xen63 relative to Preserflo at all IOP cut offs, median IOP and medication burden, time to failure and best-corrected visual acuity (BCVA) in logarithm of the minimum angle of resolution units at last follow-up or at the time of reoperation. Exploratory analyses were conducted to identify potential risk factors for surgical failure, including age, sex, ethnicity, glaucoma severity, decision IOP, preoperative BCVA, type of device, diabetes status, and MMC dose. Safety outcomes included postoperative interventions, complications such as wound leak or dehiscence, hyphema, vitreous hemorrhage, choroidal detachment, macular folds, prolonged inflammation, corneal decompensation, macular edema, diplopia, iris incarceration, or device obstruction or exposure, as well as serious adverse events including angle closure, retinal detachment, suprachoroidal hemorrhage, malignant glaucoma, blebitis, endophthalmitis, loss of light perception vision, and reoperations.
Statistical Analysis
All statistical analyses were performed using Python version 3.12.5 (Python Software Foundation). Figures were generated using Python or GraphPad Prism version 10.6.1 (GraphPad Software, LLC, San Diego, CA). Categorical variables were summarized as frequencies (percentages) and compared using the Fisher exact test. Continuous variables were reported as means ± standard deviations for normally distributed data or medians [interquartile range (IQR)] for non-normally distributed data. Results were compared using 2-sided Student t tests or Wilcoxon rank-sum tests, as appropriate. Snellen visual acuity measurements were converted to logarithm of the minimum angle of resolution (logMAR) units.
Time-to-event success outcomes were analyzed using survival analysis to account for censoring and variable follow-up duration, using Python lifelines version 0.30.0. Kaplan–Meier survival curves were generated using Python matplotlib version 3.9.2. Survival analyses were stratified according to implant device and compared using a Log rank test with administrative censoring at 12 months. Median time-to-event values were reported only for eyes experiencing the event of interest during the study period.
Cox proportional hazards regression models were used to identify risk factors for surgical failure. Variables were selected a priori based on clinical relevance and their potential to predict treatment failure or confound the relationship between intervention and outcome. Age, sex, MIBS implant type, ethnicity, diabetes status, disease severity, decision IOP, preoperative vision, and MMC concentration were evaluated using univariable (crude) and multivariable (adjusted) models. Tied event times were handled using the Efron approximation. Collinearity among covariates was assessed using condition indices, with values greater than 30 considered indicative of significant collinearity. Competing risks were assumed to be absent with respect to censoring. The proportional hazards assumption was evaluated for each covariate using Schoenfeld residuals. Variables that violated the proportional hazards assumption were addressed by either including a time-dependent interaction term or by stratifying the Cox model by the non-proportional variable. Time-dependent interaction terms accounting for less than 1% of the change in hazard over time were excluded from the final model.
Because some patients contributed data from both eyes, intracluster correlation was accounted for using a shared frailty model based on the approach described by Lee, Wei, and Amato (1992).24 Regression coefficients were estimated using partial likelihood under an independent working assumption and a robust sandwich variance estimator was applied. All statistical tests were 2-sided, and a P value < 0.05 was considered statistically significant.
Results
Study Population and Baseline Characteristics
A total of 65 and 75 consecutive nonrefractory eyes that underwent standalone Xen63 Gel Stent and Preserflo Microshunt implantation with at least 1 month follow-up, respectively, were included. In the Xen63 group, implantation was performed via an open-conjunctiva approach in 18.4% of cases. Two patients in the Xen63 group and three patients in the Preserflo group had both eyes included in the study. Twelve-month follow-up was available for 84.6% of Xen63 eyes and 88.0% of Preserflo eyes (p=0.62).
Baseline demographic and ocular characteristics are summarized in Table 1. Overall, the two groups were comparable with respect to key baseline characteristics. Most patients were white, had primary open-angle glaucoma (POAG), and presented with advanced disease at the time of surgery. Compared with the Preserflo group, patients in the Xen63 group were older, more frequently female, and more likely to have undergone prior selective laser trabeculoplasty (SLT) and cataract surgery. In contrast, a higher proportion of eyes in the Preserflo group had pseudoexfoliative glaucoma. Most eyes in both groups received higher concentrations of MMC (0.4mg/mL).
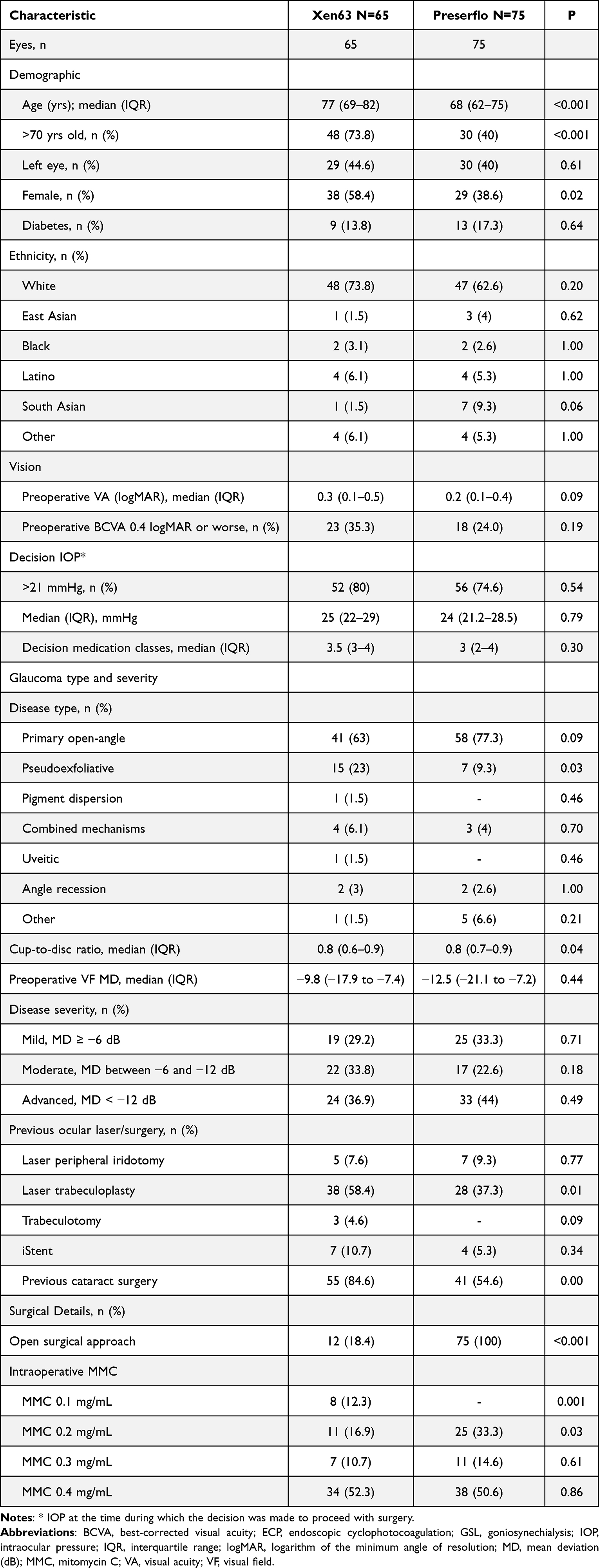 |
Table 1 Baseline Characteristics |
Complete and Qualified Surgical Success
At the primary IOP threshold of 6–17 mmHg, complete surgical success was achieved in 61.5% (95% CI, 47.9–72.6%) of eyes in the Xen63 group and 73.9% (95% CI, 62.2–82.5%) of eyes in the Preserflo Microshunt group (p = 0.13). Qualified success rates increased to 81.8% (95% CI, 69.6–89.6%) in the Xen63 group and 90.2% (95% CI, 80.6–95.2%) in the Preserflo group (p = 0.13). For complete success at this threshold, the median (IQR) time to failure was 6.0 (2.4–9.5) months in the Xen63 and 5.9 (3.3–9.1) months in the Preserflo (p = 0.91) group.
Using a more stringent upper IOP threshold of 14 mmHg, complete success was achieved in 54.6% (95% CI, 41.1–66.3%) of the eyes in the Xen63 group and 62.8% (95% CI, 50.6–72.8%) of the eyes in the Preserflo Microshunt group (p = 0.39). Qualified success at the same IOP cut-off was 76.6% (95% CI, 63.7–85.5%) and 87.4% (95% CI, 77.2–93.3%) in the Xen63 and Preserflo groups, respectively (p = 0.09). At the less stringent upper IOP threshold of 21 mmHg, complete success was observed in 63.3% (95% CI, 49.7–74.1%) of the eyes in the Xen63 group and 75% (95% CI, 63.2–83.4%) of the eyes in the Preserflo group (p = 0.13), with qualified success rates of 81.9% (95% CI, 69.6–89.5%) and 91.6% (95% CI, 82.3–96.2%), respectively (p = 0.08). Kaplan–Meier survival curves for complete and qualified success at IOP thresholds of 6 to 14 mmHg, 6 to 17 mmHg, and 6 to 21 mmHg are shown in Figures 1A–F. The crude and adjusted hazard ratio for surgical failure of Xen63 relative to the Preserflo Microshunt at all IOP cut offs at 12 months are summarized in Table 2. Clinical hypotony accounted for one failure in each group. Reasons for treatment failure for the primary complete success outcome are detailed in Supplemental Table 1.
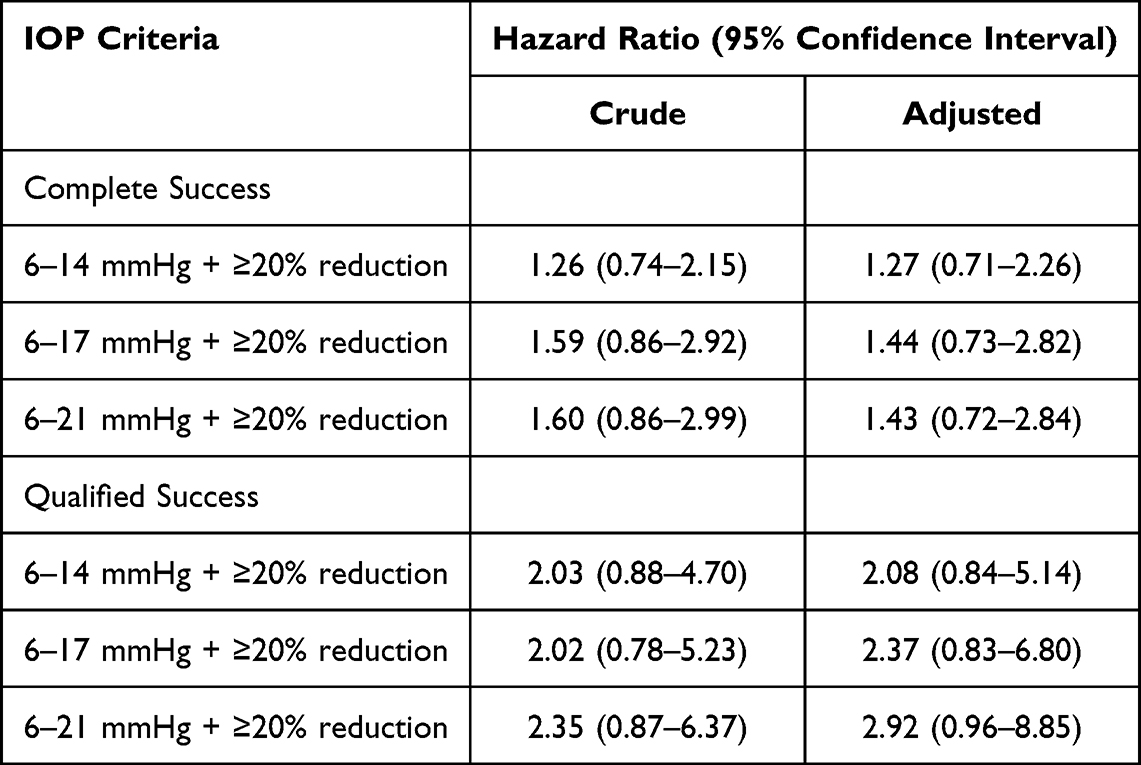 |
Table 2 Crude and Adjusted Hazard Ratios for Failure in Xen63 Relative to Preserflo Eyes |
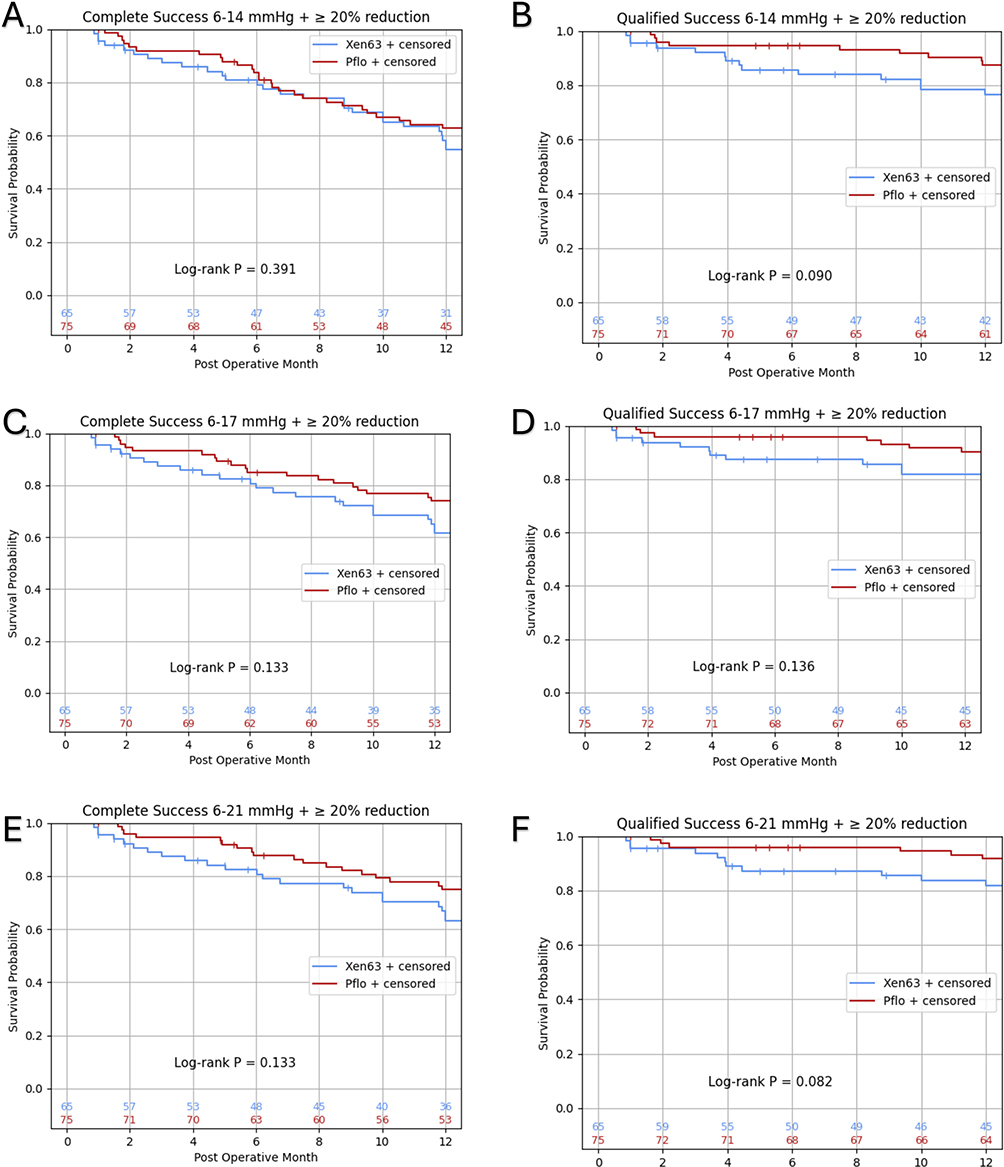 |
Figure 1 Kaplan-Meier survival curves, with number of eyes at risk, for complete and qualified success at various IOP thresholds plus at least 20% IOP reduction from baseline in 63-µm gelatin microstent and Preserflo eyes over 12 months of follow-up. Complete success with IOP thresholds at (A), 6 mmHg to 14 mmHg, (B), 6 mmHg to 17 mmHg, (C), 6 mmHg to 21 mmHg. Qualified success with IOP thresholds of (D), 6 mmHg to 14 mmHg, (E), 6 mmHg to 17 mmHg, (F), 6 mmHg to 21 mmHg. Abbreviation: IOP, intraocular pressure. |
Additional Surgical Success Analysis
Because the Xen63 group included eyes undergoing gel stent implantation using either an open- or closed-conjunctiva approach, a subgroup analysis was performed. At the IOP threshold of 6–17 mmHg, complete surgical success at 12 months was achieved in 69.8% of eyes in the open-conjunctiva subgroup (n=12) and 60.4% of eyes in the closed-conjunctiva subgroup (n=53, p = 0.81). No statistically significant differences in complete or qualified surgical success were observed at any IOP threshold between the two approaches.
Characteristics Associated with Surgical Failure
Cox proportional hazards regression was performed to identify factors associated with surgical failure using the IOP threshold of 6–17 mmHg (Figure 2). In the multivariable analysis, non-Caucasian ethnicity was independently associated with an increased risk of surgical failure (hazard ratio [HR], 2.57; 95% CI, 1.26–5.23; p = 0.009), an association that remained significant in the frailty model (HR, 2.57; 95% CI, 1.30–5.09; p = 0.006). No other baseline demographic or clinical variable was significantly associated with an increased risk of surgical failure.
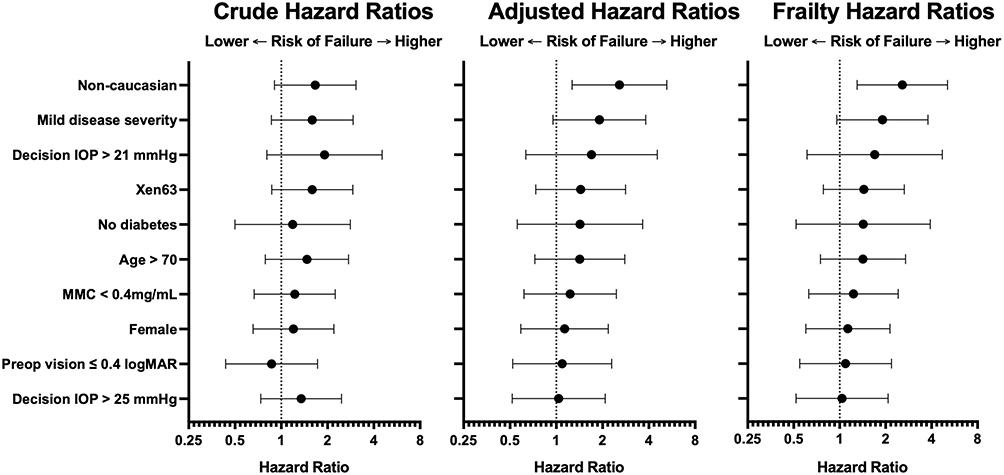 |
Figure 2 Crude and adjusted hazard ratios for surgical failure at 12-month follow-up. Shown are crude (Left), adjusted (Middle), and frailty model (Right) hazard ratios for the indicated risk factors, with 95% confidence intervals. |
Intraocular Pressure, Medication Use, and Best-Corrected Visual Acuity
At baseline, median IOP was 25 mmHg (22–29) and 24 mmHg (21.2–28.5) in the Xen63 and the Preserflo Microshunt groups respectively (p = 0.79). The median number of glaucoma medications was 3.5 (3–4) in the Xen63 group and 3.0 (2–4) in the Preserflo group (p = 0.30). At 12 months, median IOP was 13 mmHg (10–18) in the Xen63 group and 14 mmHg (11–16) in the Preserflo group (p = 0.67), with a median of 0 (IQR, 0–1) glaucoma medications in both groups (p = 0.75). No statistically significant differences were observed between groups in median IOP or medication burden at any postoperative time point. The longitudinal course of median IOP and glaucoma medication use over the follow-up period is shown in Figure 3. At the end of follow-up, 70.9% of the patients in the Xen 63 group and 71.4% of the patients in the Preserflo group were medication-free (p=1.00).
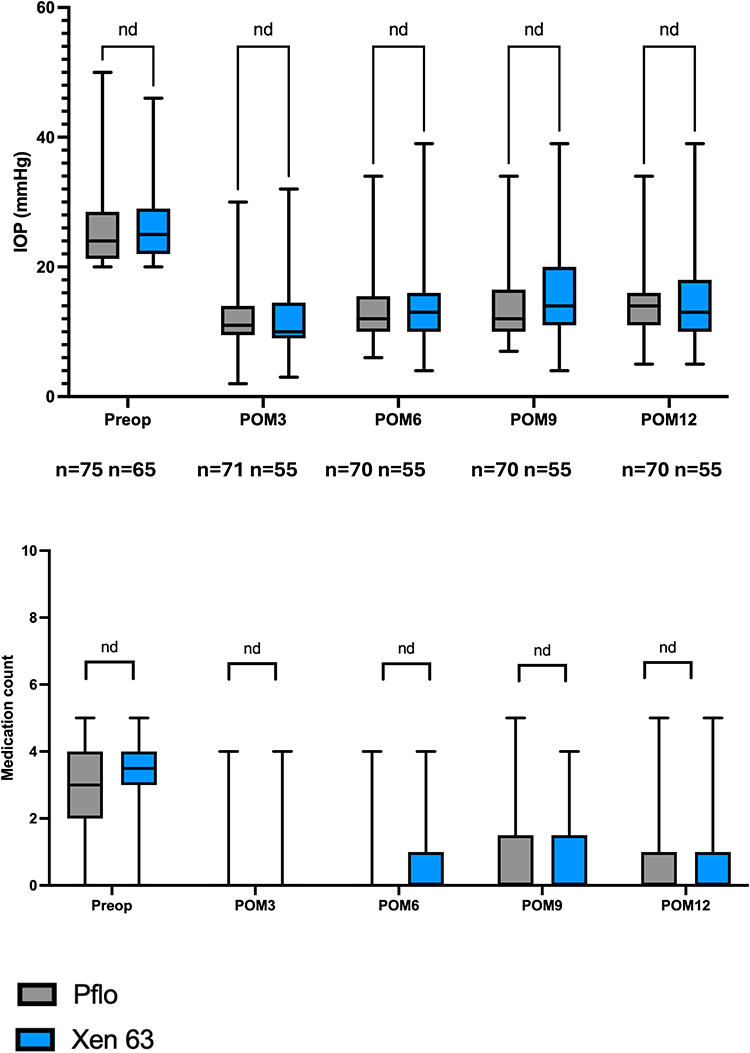 |
Figure 3 Box and whisker plot of intraocular pressure and medications over the course of 12 months. The horizontal central lines of each box indicate the median; the lower and upper ends of boxes indicate the lower and upper quartiles. Whiskers represent minimal and maximal values. Nd = indicates no statistical difference in IOP lowering or medications between Xen63 and Pflo eyes, with a p value > 0.05. Abbreviations: Preop, preoperative; POM, postoperative month. |
Median (IQR) BCVA was 0.30 (0.17–0.49) in the Xen63 group and 0.17 (0.09–0.39) in the Preserflo group at baseline (p=0.09) and remained stable at 12 months (0.30 [0.09–0.60] vs 0.17 [0.09–0.39]), with no significant difference in visual outcomes between groups (p = 0.23).
Complications
Early and late postoperative complications occurring within the 12-month follow-up period are summarized in Table 3. Overall, complications were more frequent in the Xen63 group, with 40 eyes (61.5%) experiencing at least one complication, compared with 22 eyes (29.3%) in the Preserflo Microshunt group (p = 0.0002).
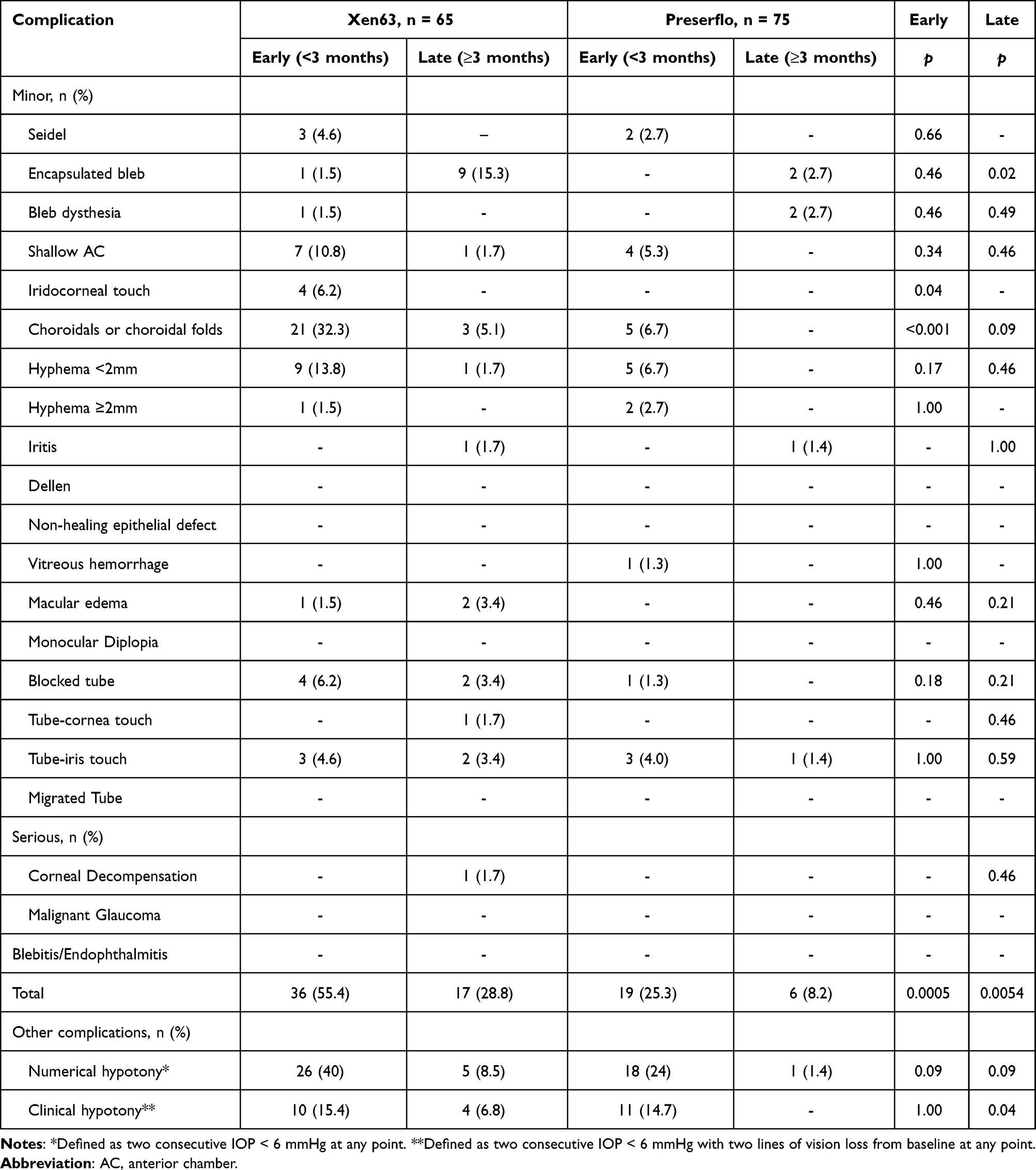 |
Table 3 Early and Late Postoperative Complications up to 12 Months of Follow-Up |
The most common early postoperative complication (<3 months) was choroidal folds or choroidal detachment, which occurred in 21 eyes (32.3%) in the Xen63 group and 5 eyes (6.7%) in the Preserflo group (p=0.0001). One eye in each group required anterior chamber reformation with OVD, with subsequent resolution. Numerical hypotony occurred more frequently in the Xen63 group compared with the Preserflo group (44.6% vs 25.3%, p = 0.02), predominantly during the early postoperative period. Rates of clinical hypotony (2 consecutive IOP <6 with ≥ 2 lines of VA loss) were similar between groups (Xen63 20.0% vs Preserflo 14.7%, p = 0.50), but, when considering only late (≥3 months) clinical hypotony, it happened more frequently in the Xen63 group (6.8% vs 0%, p=0.04).
Encapsulated bleb formation occurred more frequently in the Xen63 group (15.4% vs 2.7%, p = 0.01), with most cases presenting during the late postoperative period.
Regarding serious complications, one eye in the Xen63 group developed corneal decompensation. This eye had a history of Descemet membrane endothelial keratoplasty (DMEK) performed 1 year before Xen63 implantation and mild preoperative corneal edema. Although the device was well positioned in the iris plane and not in proximity to the cornea, progressive corneal edema developed at 6 months postoperatively, ultimately requiring a Descemet stripping automated endothelial keratoplasty (DSAEK). Loss of more than two lines of visual acuity occurred in 25.9% in the Xen63 group and in 12.9% in the Preserflo group (p=0.10).
Postoperative Interventions
Postoperative interventions were required in 20 eyes (30.8%) in the Xen63 group and 21 eyes (28%) in the Preserflo Microshunt group (p=0.85). The most frequent intervention was bleb needling, with similar rates between groups (Xen63 18.5% vs Preserflo 20%; p = 0.83). Laser treatment to the tube was performed more frequently in the Xen63 group compared with the Preserflo group (6.2% vs 0%; p = 0.04). Postoperative interventions are summarized in Table 4.
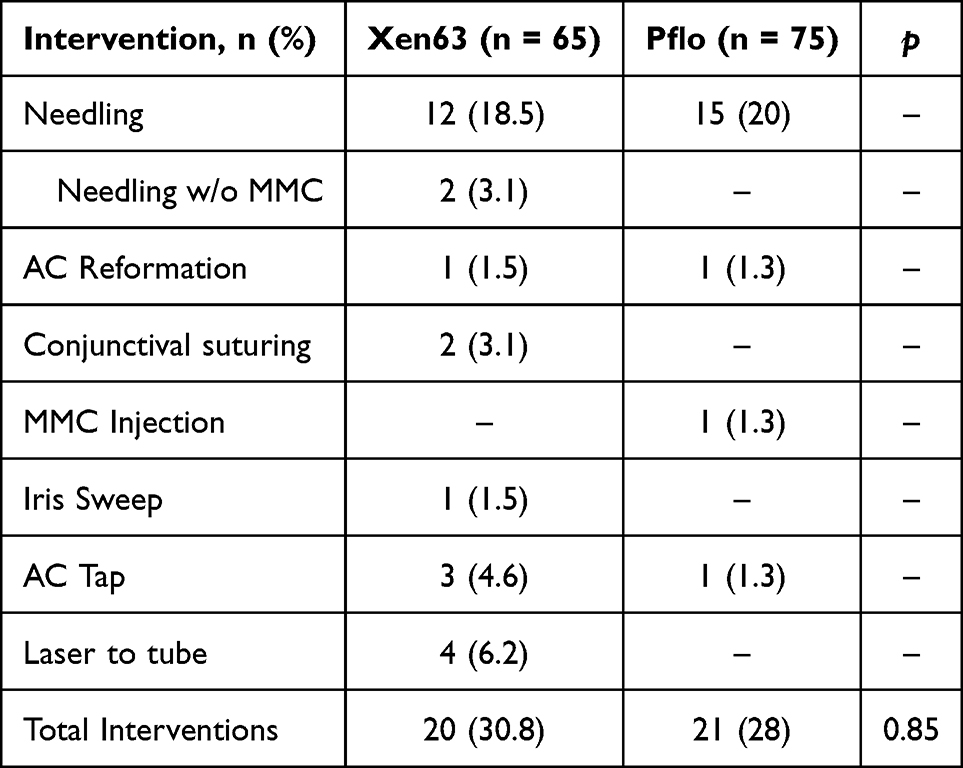 |
Table 4 Postoperative Interventions Up to 12 Months of Follow-Up |
Revisions and Reoperations
Revisions, including bleb revision or tube repositioning, were required at similar frequencies in both groups (Xen63, 6.2% vs. Preserflo, 6.7%, p= 1.00). However, reoperations were performed more often in the Xen63 group (16.9% vs 4%, p= 0.01). The most common reoperation in the Xen63 group was subsequent Preserflo implantation, which accounted for 7.7% of eyes in this cohort. Revisions and reoperations are summarized in Table 5.
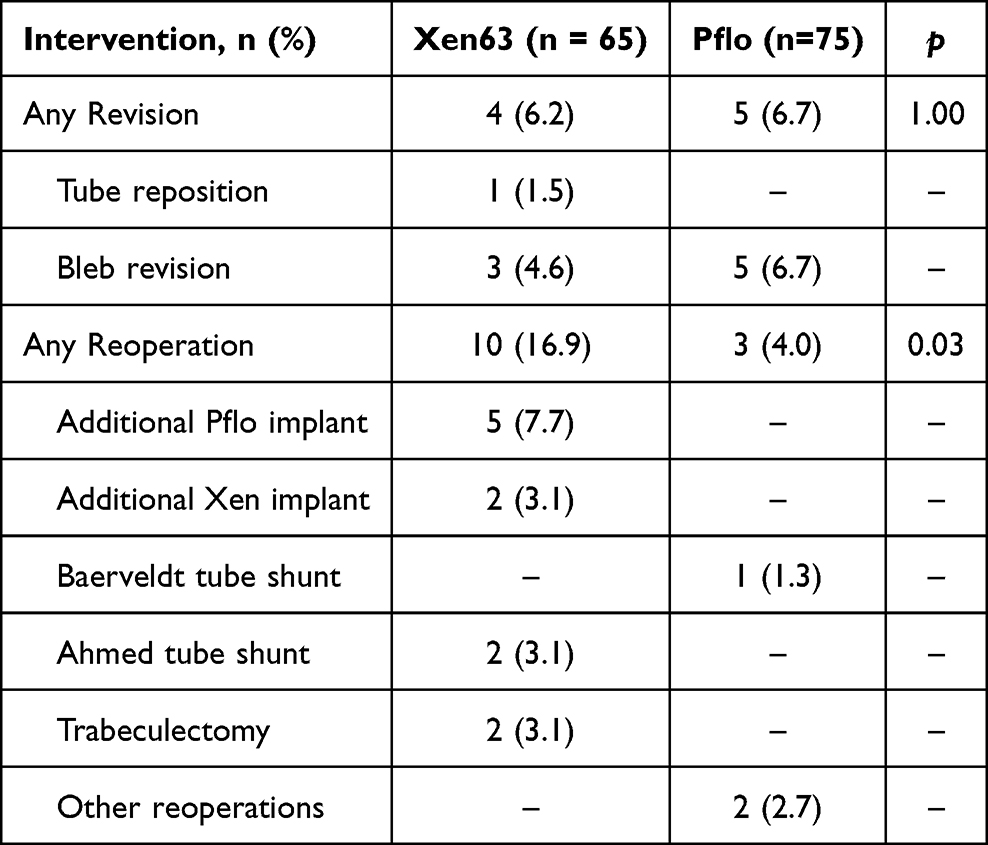 |
Table 5 Postoperative Revisions and Reoperations in Xen63 and Preserflo Eyes Up to 1 Year |
Discussion
To our knowledge, this study represents the largest evaluation to date comparing the IOP-lowering efficacy and adverse event profile of standalone Xen63 Gel Stent and Preserflo Microshunt implantation. At 12 months, both complete and qualified success were similar between groups at all IOP cut-offs.
Median IOP at 12 months was comparable between groups (13 mmHg and 14 mmHg), with both cohorts achieving a median reduction of three glaucoma medication classes and approximately 70% of eyes in both groups being medication free. Despite similar efficacy outcomes, eyes in the Xen63 group experienced a higher frequency of postoperative complications and required more reoperations compared with those undergoing Preserflo implantation.
Most prior comparative studies between Xen and Preserflo have focused on the earlier Xen45 device. Across these studies, Preserflo generally demonstrated numerically higher success rates, although differences were often not statistically significant and safety profiles were largely comparable.16–19 More recent comparisons between Xen45 and the larger-lumen Xen63 have reported superior IOP reduction and higher surgical success with Xen63, tempered by a higher incidence of hypotony-related complications.10,20 These findings have been attributed to the larger lumen of the Xen63, which is approximately 1.4 times wider than that of the Xen45 and results in an estimated 3.8 times reduction in intrinsic resistance to flow based on the Hagen–Poiseuille equation.25,26
Direct comparisons between Xen63 and Preserflo are scarce. A prior single-center retrospective study22 with 30 eyes and limited reporting, found no significant differences in surgical success, with comparable outcomes using both less stringent (IOP <21 mmHg) and more stringent (IOP ≤15 mmHg) criteria. Similarly, in the present multicenter cohort, no statistically significant differences in complete or qualified success were observed between devices at any IOP threshold. The Hagen–Poiseuille equation provides a useful framework for interpreting these findings. Resistance to flow through a shunt is proportional to tube length and inversely proportional to the fourth power of the lumen radius. Although Preserflo is longer (8.5 mm) with a larger lumen (70 µm) and Xen63 is shorter (6 mm) with a slightly smaller lumen (63 µm), their theoretical resistances to flow are remarkably similar. In vitro studies have estimated the outflow resistance at approximately 5.35 mmHg/µL/min for Xen45 and 1.3 mmHg/µL/min for Preserflo; applying the same principles, Xen63 is estimated to have a resistance of approximately 1.4 mmHg/µL/min.21 This similarity in intrinsic outflow resistance likely contributes to the comparable surgical success observed with Xen63 and Preserflo.
The present study is the first to report complications in a large cohort directly comparing Xen63 and Preserflo. Despite similar IOP-lowering efficacy, hypotony-related complications—including choroidal effusions and numerical hypotony—were more frequent in the Xen63 group. Prior studies reported higher hypotony rates with Preserflo compared with Xen45,17,18 whereas studies comparing Xen45 with Xen63 consistently showed increased complications with the larger-lumen Xen63.10,20 Both Xen63 and Preserflo provide similar theoretical resistance, yet one possible explanation for the higher rate of early hypotony-related events is transient peritubular flow around the Xen63 implant. Although the Xen63 is inserted through a 27-gauge needle tract, the gelatin implant expands after deployment and relies primarily on tissue apposition rather than a mechanical anchor. In contrast, the Preserflo Microshunt incorporates a fin designed to provide greater stability within the scleral tunnel and may reduce peritubular flow. It is therefore possible that transient leakage around the Xen implant could occur in the early postoperative period before tissue apposition is fully established. This remains a hypothesis and other factors, including surgical technique and wound-healing responses, may also contribute to the observed differences. Nonetheless, it is consistent with the predominantly early and self-limited hypotony-related complications observed in our cohort, most of which were managed conservatively. While not statistically significant, a greater proportion of eyes in the Xen63 group lost >2 lines of visual acuity compared with the Preserflo group (25.9% vs 12.9%), which may be related to the higher rates of hypotony and choroidal complications observed in this group.
While the Preserflo is only performed with an open-conjunctival ab-externo approach, we included both open and closed conjunctiva ab-interno approaches in the Xen63 group. Although this introduces some variability and a potential confounder, the vast majority of Xen63 (82%) were performed with a closed conjunctival approach. Furthermore, a subgroup analysis of Xen63 eyes did not identify statistically significant differences in success rate between the two approaches, although this analysis may be underpowered given the small proportion of open-conjunctiva cases.This contrasts with prior Xen45 data favoring open-conjunctiva implantation and may reflect our limited statistical power to detect a difference due to the small proportion of open-conjunctiva cases, the larger lumen of Xen63 reducing the impact of conjunctival approach, and frequent use of primary needling in our closed-conjunctiva technique.27,28 It would be interesting to study only open Xen63 versus Preserflo, which may lead to different results.
The need for postoperative interventions was similar between groups, with needling being the most common intervention in both cohorts. However, reoperations were significantly more frequently required in the Xen63 group. Although reoperation remains a common outcome following filtering procedures, as demonstrated by the Primary Tube Versus Trabeculectomy (PTVT) study,29 which reported reoperation rates of 6.6% in the tube group and 3.5% in the trabeculectomy group (P = 0.14) at 12-months, minimizing the need for additional surgery remains a key goal in glaucoma management.
These findings have practical implications for surgical planning. While both devices achieve similar IOP control, the higher complication and reoperation rates with Xen63 may influence device selection, particularly in patients where minimizing postoperative morbidity is prioritized. Conversely, the closed conjunctival approach of Xen63 may remain preferable in eyes where preserving conjunctiva, surgical efficiency, and postoperative patient comfort are considerations.
Some potential limitations and how we addressed them are worth mentioning. Baseline characteristics were largely comparable between groups, although patients in the Xen63 group were older, more frequently female, and more likely to have pseudoexfoliative glaucoma. None of these variables were associated with surgical failure in multivariable Cox regression. Non-White ethnicity was the only factor independently associated with an increased risk of failure, consistent with prior reports.30,31
The retrospective design is subject to unmeasured confounding; however, the inclusion of consecutive cases, use of multivariable regression, and high 12-month follow-up rates help mitigate this limitation. Surgical technique, perioperative decision-making, and postoperative management were not standardized and were left to the discretion of individual surgeons across centers. While this reflects real-world clinical practice, it introduces heterogeneity that may have led to bias and limits direct comparability between groups; therefore, our findings should be interpreted with caution.MMC dosing was not standardized, and lower concentrations differed between groups, which may have introduced bias. Although most eyes in both groups received 0.4 mg/mL and MMC dose was not identified as a significant predictor of surgical failure in our Cox regression analysis, the study may be underpowered to detect such an effect, and residual confounding cannot be excluded.Finally, although complete and qualified success rates were not statistically significant between groups, eyes that underwent Preserflo implantation consistently demonstrated numerically higher success rates, with an 8–12% difference that may be clinically relevant. Importantly, the absence of statistical significance should not automatically be interpreted as equivalence between procedures. A larger sample size may have allowed detection of a statistically significant difference favoring the Preserflo group. However, we also reported adjusted hazard ratios, which showed no statistically significant difference, with a reasonable confidence interval comparable to those reported in other well-established trials.2,28 Unlike prospective randomized trials, retrospective cohort studies cannot predefine sample size calculations; therefore, the precision of effect estimates is best assessed by the width of the confidence intervals rather than by post-hoc power calculations. Accordingly, reporting confidence intervals is considered a more appropriate approach for interpreting the robustness and clinical relevance of findings in retrospective studies. These findings highlight the need for larger, robust studies, including randomized controlled trials, to further evaluate and confirm this observed trend.
Despite these limitations, the strengths of this study include its multicenter design and the inclusion of only standalone procedures, which avoids confounding from combined cataract surgery seen in prior studies evaluating MIBS devices. Although the size of the cohort remains modest, to our knowledge this represents the largest retrospective comparison of standalone Xen63 Gel Stent and Preserflo implantation to date. We employed more robust reporting and statistical modeling, including a frailty model to account for intracluster correlation and multivariable regression analyses to adjust for potential confounders. The inclusion of multiple international centers enhances external validity and reflects real-world surgical practice.
Conclusions
Xen63 and Preserflo achieved comparable surgical success rates, median IOP reduction, and postoperative medication burden. The Xen63 group experienced a higher rate of complications, predominantly hypotony-related events, which were largely self-limited. Rates of postoperative interventions and revisions were similar between groups, but reoperations were more frequently required in the Xen63 group.
Funding
IIKA: Supported in part by an Unrestricted Grant from Research to Prevent Blindness, New York, NY, to the Department of Ophthalmology & Visual Sciences, University of Utah. The sponsor or funding organization had no role in the design or conduct of this research.
Disclosure
TDF: Alcon (consultant [C]), Abbvie (C, speaker [S]), Bausch and lomb (C), Carl Zeiss (C), Elios (C), EyeD Pharma (C), Iantrek (C), Glaukos (C, S), Iantrek (C), Myra Vision (C), MM instrumentos S.A.C (writing support [W]), NovaEye Medical (C,S), Sight Sciences (C), Vialase (C), Zeiss (C, S). VPC: Ache (C,S), Alcon (C, H), Abbvie (C, R), Genon (C, S) Iridex (R), Carl Zeiss (H, R), Glaukos (C, R, H). IIKA: AbbVie (C, R), Ace Vision (C), Alcon (C, R), Aliph Medical (C), AmarosEngine (C), Apellis Pharmaceutical (C), Aquea Health, Inc (C), ArcScan (C), Avellino Lab USA, Inc (C), Avisi (C), Balance Ophthalmics (C), Bausch and Lomb (C), Beaver Visitec (C), Belkin Vision (C), Bionode (C), Carl Zeiss (C), Centricity Vision, Inc (C), Ciliatech (C), CorNeat Vision (C,R), Custom Surgical (C), Dragonfleye Therapeutics Corp (C), Elios Vision (C, R), ElutiMed (C), Emmes Biopharma Services, LLC (C), eyeFlow, Inc (C), Eye to Eye TeleHealth (C), EyeMed (C), EyeQ Technologies (C), EyeX Solutions (C), Exhaura Limited (C), Glaukos (C,R), Gore (C, R), Hexiris Pharma (C), Iantrek (C,R), Implandata (C), InjectSense (C), Iridex (C), iCare USA (C, R), iStar (C, R), Johnson & Johnson Vision (C, R), LayerBio (C), Liqid Medical (C), Long Bridge Medical, Inc (C), Medicontur (C), MST Surgical (C), Myra Vision (C, R), New World Medical (C, R), Nova Eye (C,R), Noxelis (C), Ocular Instruments (C), Ocular Therapeutix (C), Oculus Surgical (C), OcuSciences (C), Omega Ophthalmics (C), Ophthalmic Therapeutic Innovations, LLC (C), OrbitaU (C), Perfuse Therapeutics, Inc (C), Peripherex (C), PolyActiva (C), PulseMedica (C), Qlaris Bio (C), Radiance Therapeutics, Inc (C), Radius XR (C), Regeneron Pharmaceuticals, Inc (C), Rheon Medical SA (C), Ripple Therapeutics (C), Sanoculis (C), Santen (C, R), SeonixBio (C), Sierra Clinical Services LLC (C), Singapore Biodesign (C), Shifamed, LLC (C), Shockwave Medical (C), Sight Sciences (C), Smartlens, Inc (C), Stroma (C), Tavo BioTherapeutics, Inc (C), SpyGlass Pharma (C), Thea Pharma (C), TFS Health Science (C), ViaLase (C), Visci Ltd (C), Visus Therapeutics (C), Vizzario (C), WL Gore (C), Zilia, Inc (C). The authors report no other conflicts of interest in this work.
References
1. Saheb H, Ahmed II. Microinvasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23(2):96–16. doi:10.1097/ICU.0b013e32834ff1e7
2. Sheybani A, Vera V, Grover DS, et al. Gel stent versus trabeculectomy: the randomized multicenter Gold-Standard Pathway Study at 12 months. Am J Ophthalmol. 2023;252:306–325. doi:10.1016/j.ajo.2023.03.026
3. Panarelli JF, Moster MR, Garcia-Feijoo J, et al. Ab externo MicroShunt versus trabeculectomy in primary open-angle glaucoma: 2-year results. Ophthalmology. 2024;131(3):266–276. doi:10.1016/j.ophtha.2023.09.023
4. Schlenker MB, Gulamhusein H, Conrad-Hengerer I, et al. Standalone ab interno gelatin stent versus trabeculectomy. Ophthalmol Glaucoma. 2018;1(3):189–196. doi:10.1016/j.ogla.2018.10.003
5. Sheybani A, Reitsamer H, Ahmed II. Fluid dynamics of a novel microfistula implant. Invest Ophthalmol Vis Sci. 2015;56(8):4789–4795. doi:10.1167/iovs.15-16625
6. Do AT, Parikh H, Panarelli JF. Subconjunctival microinvasive glaucoma surgeries: an update. Curr Opin Ophthalmol. 2020;31(2):132–138. doi:10.1097/ICU.0000000000000643
7. Acosta AC, Espana EM, Yamamoto H, et al. A newly designed glaucoma drainage implant. Arch Ophthalmol. 2006;124(12):1742–1749. doi:10.1001/archopht.124.12.1742
8. Pinchuk L, Riss I, Batlle JF, et al. Development of a micro-shunt made from SIBS. J Biomed Mater Res B Appl Biomater. 2017;105(1):211–221. doi:10.1002/jbm.b.33525
9. Lewis RA. Ab interno approach to the subconjunctival space using a collagen glaucoma stent. J Cataract Refract Surg. 2014;40(8):1301–1306. doi:10.1016/j.jcrs.2014.01.032
10. Hussein IM, De Francesco T, Ahmed IIK. Intermediate outcomes of the novel 63-μm gelatin microstent versus the 45-μm microstent. Ophthalmol Glaucoma. 2023;6(6):580–591. doi:10.1016/j.ogla.2023.05.001
11. Armstrong JJ, De Francesco T, Ma J, et al. Ab externo SIBS MicroShunt with MMC: 3-year results. Ophthalmol Glaucoma. 2023;6(5):480–492. doi:10.1016/j.ogla.2023.04.002
12. Schlenker MB, Armstrong JJ, De Francesco T, et al. All consecutive ab externo SIBS MicroShunt implantations. Am J Ophthalmol. 2023;255:125–140. doi:10.1016/j.ajo.2023.06.009
13. De Francesco T, Armstrong JJ, Hussein IM, et al. Mitomycin C 0.2 vs 0.4 mg/mL during MicroShunt implantation. Ophthalmol Glaucoma. 2024;7(5):454–465. doi:10.1016/j.ogla.2024.06.001
14. Fea AM, Bron AM, Economou MA, et al. European study of a cross-linked gel stent. J Cataract Refract Surg. 2020;46(3):441–450. doi:10.1097/j.jcrs.0000000000000065
15. Armstrong JJ, De Francesco T, Beckers HJ, et al. Glaucoma surgery comparison study. Am J Ophthalmol. 2025;277:169–183. doi:10.1016/j.ajo.2025.05.011
16. Nobl M, Freissinger S, Rudolph K, et al. Long-term outcomes of PreserFlo vs XEN45. Klin Monbl Augenheilkd. 2024;241(7):805–812. doi:10.1055/a-2152-8455
17. Lüke JN, Dietlein TS, Widder RA, et al. Matched case-control comparison of XEN45 and PRESERFLO. Clin Exp Ophthalmol. 2024;52(7):732–739. doi:10.1111/ceo.14407
18. Scheres LMJ, Kujovic-Aleksov S, Ramdas WD, et al. XEN Gel Stent vs PRESERFLO: 2-year results. Acta Ophthalmol. 2021;99(3):e433–e440. doi:10.1111/aos.14602
19. Giansanti F, Quaranta G, Serino F, et al. Comparison of XEN and PreserFlo: a monocentric experience. J Clin Exp Ophthalmol. 2023;14:953.
20. Evers C, Böhringer D, Kallee S, et al. XEN63 compared to XEN45. J Clin Med. 2023;12(15):5043. doi:10.3390/jcm12155043
21. Ibarz Barberá M, Hernández-Verdejo JL, Bragard J, et al. Ultrastructural and flow properties of PRESERFLO. Transl Vis Sci Technol. 2021;10(13):26. doi:10.1167/tvst.10.13.26
22. Martínez-de-la-Casa JM, Pascual-Santiago A, Morales-Fernandez L, et al. Xen63 versus PreserFlo. Sci Rep. 2025;15:1634. doi:10.1038/s41598-024-81616-3
23. World Glaucoma Association. Guidelines on Design & Reporting Glaucoma Trials. World Glaucoma Association; 2018. Available from: https://wga.one/wpfd_file/guidelines-on-design-reporting-glaucoma-trials/.
24. Lee EW, Wei LJ, Amato DA, Leurgans S. Cox-type regression analysis. In: Klein JP, Goel PK, editors. Survival Analysis: State of the Art. Kluwer Academic Publishers; 1992:237–247.
25. Fea AM, Menchini M, Rossi A, et al. Early experience with XEN63. J Clin Med. 2021;10(8):1628. doi:10.3390/jcm10081628
26. Lavin-Dapena C, Cordero-Ros R, D’Anna O, Mogollón I. XEN63 gel stent: 5-year follow-up. Eur J Ophthalmol. 2021;31(4):1829–1835. doi:10.1177/1120672120952033
27. McGlumphy EJ, Do A, Du A, et al. Open vs closed conjunctival XEN45. Ophthalmol Glaucoma. 2024;7(2):116–122. doi:10.1016/j.ogla.2023.09.001
28. El Helwe H, Ingram Z, Neeson CE, et al. Ab interno vs ab externo XEN approaches. J Glaucoma. 2024;33(2):116–125. doi:10.1097/IJG.0000000000002320
29. Gedde SJ, Feuer WJ, Shi W, et al. Treatment outcomes in the primary tube versus trabeculectomy study. Ophthalmology. 2018;125(5):650–663. doi:10.1016/j.ophtha.2018.02.003
30. Nguyen AH, Fatehi N, Romero P, et al. Trabeculectomy outcomes by ancestry. JAMA Ophthalmol. 2018;136(10):1106–1113. doi:10.1001/jamaophthalmol.2018.2897
31. Borisuth NS, Phillips B, Krupin T. Risk profile of glaucoma filtration surgery. Curr Opin Ophthalmol. 1999;10(2):112–116. doi:10.1097/00055735-199904000-00006
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Trabeculectomy Vs Non‐penetrating Deep Sclerectomy for the Surgical Treatment of Open-Angle Glaucoma: A Long-Term Report of 201 Eyes
Correia Barbosa R, Gonçalves R, Bastos R, Alves Pereira S, Basto R, Viana AR, Tenedório P
Clinical Ophthalmology 2023, 17:1619-1627
Published Date: 6 June 2023