Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Comparative Effectiveness of Propofol-Sufentanil vs Propofol-Fentanyl in Elderly Patients Undergoing Transurethral Resection of the Prostate
Received 24 June 2025
Accepted for publication 19 November 2025
Published 20 December 2025 Volume 2025:21 Pages 1773—1782
DOI https://doi.org/10.2147/TCRM.S549323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Faustino Ramón Pérez-López
Tong Dong,1 Song Lei,2 Genfeng Ding1
1Department of Anesthesiology and Surgery, First People’s Hospital of Yongkang City, Yongkang City, Zhejiang Province, 321300, People’s Republic of China; 2Department of Medical Oncology, First People’s Hospital of Yongkang City, Yongkang City, Zhejiang Province, 321300, People’s Republic of China
Correspondence: Tong Dong, Department of Anesthesiology and Surgery, First People’s Hospital of Yongkang City, No. 599 Jinshan West Road, Yongkang City, Zhejiang Province, 321300, People’s Republic of China, Email [email protected]
Objective: The aim of this study is to compare the anesthetic effect and cognitive function impact of propofol-sufentanil (PS) versus propofol-fentanyl (PF) in elderly patients undergoing transurethral resection of the prostate (TURP) under general anesthesia (GA).
Methods: This is a retrospective cohort study conducted in First People’s Hospital of Yongkang City. They included 98 patients aged 65 and above who underwent TURP under GA between October 2023 and March 2025. 49 patients who received PS were matched with a cohort of propofol-fentanyl (PF) in a 1:1 ratio. Compare the hemodynamic parameters (heart rate (HR) and mean arterial pressure (MAP)) of two groups at 30 minutes before anesthesia induction (T0), after anesthesia completion (T1), at the time of skin incision (T2), at the end of surgery (T3), at the postanesthesia care unit (PACU) (T4), 15 minutes after PACU arrival (T5), and 30 minutes after PACU arrival (T6). Compare two perioperative indicators (anesthesia onset time, postoperative awakening time, and extubation time). Compare the pain visual analogue scale (VAS) scores of two groups at three, 12, and 24 hours after surgery. And the Montreal Cognitive Assessment Scale (MoCA) was used to evaluate the number of patients with cognitive impairment at six, 24, and 72 hours after surgery in two groups. Compare the incidence of adverse reactions within 72 hours after surgery between two groups.
Results: Compared with the PF group, the PS group had more stable hemodynamics during T2-T5 (P< 0.05); VAS scores were lower at 12 and 24 hours postoperatively (P< 0.05); The anesthesia onset time, postoperative awakening time, and extubation time of the PS group were significantly shorter than those of the PF group (P< 0.05); The incidence of cognitive dysfunction was lower at six and 24 hours after surgery (P< 0.05). However, there was no significant difference in the incidence of various complications between the two groups (P> 0.05).
Conclusion: PS is more effective for TURP anesthesia and has a better protective effect on early postoperative cognitive function.
Keywords: anesthetic effect, cognitive function, propofol, sufentanil, transurethral resection of the prostate, fentanyl
Introduction
Benign prostatic hyperplasia (BPH) is one of the most common urinary system diseases in elderly men.1,2 The data in 2021 shows that the incidence rate of BPH is 100000 people and 5531.88 cases.2 With the intensification of social aging, the incidence rate of BPH is on the rise.1 In recent years, although there have been new alternative options available for treating BPH, such as holmium laser prostatectomy.3 However, transurethral resection of the prostate (TURP) remains the most commonly used minimally invasive surgery for treating BPH.4 The main anesthesia methods for BPH are still spinal anesthesia or general anesthesia (GA).5,6 Intraspinal anesthesia can provide good analgesic effects during surgery; But the patient is in a conscious state during the surgery and may experience tension and anxiety due to the surgical procedure.5–7 Although GA can ensure that patients are unconscious and painless during surgery; However, traditional combinations of GA drugs may lead to delayed postoperative recovery, nausea, and vomiting.5 For elderly patients aged 65 and above, the presence of multiple comorbidities and reduced tolerance to anesthesia complicates the choice of anesthesia method.6,7 GA can accurately regulate the dosage of anesthetic drugs, suppress surgical stress reactions (such as sudden blood pressure rise and arrhythmia), and reduce the risk of cardiovascular and cerebrovascular accidents.6–8 Silvani et al8 found that GA provides better outcomes in terms of perioperative bleeding and 3-month functional outcomes for TURP. However, the individual situation of elderly patients is different, and multiple factors should be considered to determine the optimal anesthesia measures.
Propofol-fentanyl (PF) is a commonly used GA regimen in TURP, with propofol providing a short-acting intravenous anesthetic with rapid onset and recovery.9–11 Fentanyl effectively enhances analgesic effects; however, its efficacy in elderly patients may be limited due to its relatively lower potency and slower onset compared to sufentanil. Sufentanil, a potent derivative of fentanyl, has an increased binding affinity for the μ-opioid receptor, resulting in stronger analgesic effects and faster onset times.10 This is particularly beneficial in elderly patients, whose pharmacokinetics are altered due to age-related changes in liver and kidney function. Studies have shown that sufentanil’s shorter half-life and faster metabolism allow for more precise control over anesthetic depth, reducing the risk of prolonged sedation and postoperative cognitive dysfunction, which is crucial for elderly patients undergoing surgery.12 Research has demonstrated that elderly patients often experience altered pharmacokinetics for opioids, including reduced clearance and prolonged half-life, which are particularly relevant when considering drugs like fentanyl and sufentanil for anesthesia.13,14 The higher potency and faster metabolism of sufentanil, compared to fentanyl, make it a more effective choice in elderly patients, offering better control over anesthetic depth and reducing the potential for prolonged sedation and postoperative cognitive dysfunction. These pharmacokinetic advantages are crucial for elderly patients, whose recovery may be impaired by the side effects of prolonged anesthetic exposure.15 However, when it comes to deep sedation, the patient’s blood pressure and heart rate fluctuate greatly, and pain control is poor.10,11 As a derivative of fentanyl, sufentanil has higher analgesic intensity and shorter onset time.9–11,16 It has been widely used in GA for various surgeries. At present, the effectiveness and safety of PS have been confirmed in orthopedic and thoracic surgeries.11,16
Although both fentanyl and sufentanil are widely used in clinical anesthesia and share similar pharmacological targets, their pharmacokinetics and potency differ significantly. Elderly patients undergoing TURP represent a high-risk population due to age-related changes in drug metabolism, increased sensitivity to opioids, and higher vulnerability to perioperative hemodynamic fluctuations and cognitive impairment. By comparing the anesthetic profiles and cognitive outcomes of these two opioids specifically in elderly TURP patients, this study seeks to provide tailored guidance for anesthetic decision-making in this vulnerable group, which is currently underrepresented in the literature.
Materials and Methods
Patients
This is a retrospective cohort study conducted in First people’s Hospital of Yongkang City. They included 98 patients aged 65 and above who completed TURP under GA between October 2023 and March 2025. 49 patients who received PS were matched with a cohort of PF in a 1:1 ratio. The matching criteria are age, BMI, American Society of Anesthesiologists (ASA) classification, and comorbidities. Ethical approval for this retrospective cohort study was obtained from the Ethics Committee of the First People’s Hospital of Yongkang City (Approval No. EC2025-LW-017-01(K)). The study was conducted in accordance with relevant guidelines and regulations. Informed consent was waived due to the retrospective design and use of anonymized data. The results of this study were reported in accordance with the STROBE guidelines.
Inclusion Criteria
- Age 65 and above;
- Meets the diagnostic criteria for BHP;
- ASA I–III level;
- Complete TURP under GA;
- Using a PS or PF drugs;
- Anesthesia recording and clinical data are complete.
Exclusion Criteria
- Patients with acute myocardial infarction, end-stage liver disease, uremia requiring dialysis, etc;
- Patients who had a history of taking psychoactive medications, including but not limited to selective serotonin reuptake inhibitors (SSRIs), benzodiazepines, tricyclic antidepressants, antipsychotics, or mood stabilizers, were excluded due to the potential influence of these drugs on cognitive function and anesthetic response;
- Patients with malignant tumors;
- Patients with anemia or thrombocytopenia;
- Patients who enter the ICU after surgery.
Anesthesia Method
Two groups of patients underwent routine fasting and water deprivation before surgery. After entering the room, venous access was opened to monitor electrocardiogram (ECG), heart rate (HR), mean arterial pressure (MAP), and pulse oxygen saturation (SpO2). The anesthesia induction of PS group was performed using propofol (Beijing Fresenius Kirby Pharmaceutical Co., Ltd. China) 1.5–2.5 mg/kg, sufentanil (Yichang Renfu Pharmaceutical Co., Ltd. China) 0.1–0.2 μg/kg, and cisatracurium (Hangzhou Aoya Biotechnology Co., Ltd. China) 0.15 mg/kg; The anesthesia induction of PF group was performed using propofol 1.5–2.5 mg/kg, fentanyl (Yichang Renfu Pharmaceutical Co., Ltd. China) 3–5 μg/kg, and cisatracurium (Jiangsu Hengrui Pharmaceutical Co., Ltd. China) 0.15 mg/kg. Although cisatracurium was sourced from two different manufacturers, we confirmed that the batches met the same standard specifications and there were no significant differences in quality. The dosages and handling procedures were identical in both groups, and it is generally accepted that opioids and muscle relaxants from different manufacturers within the same class do not result in clinically significant differences in anesthetic outcomes when used within the recommended dosage range. After endotracheal intubation, mechanical ventilation is performed to maintain the end expiratory partial pressure of carbon dioxide (PETCO2) at 35–45 mmHg. Anesthesia maintenance: The PS group received propofol TCI target concentration of 2–4 μg/mL, and sufentanil was intermittently administered at 0.005–0.01 μg/(kg · min); The PF group received propofol TCI target concentration of 2–4 μg/mL and fentanyl 0.05–0.1 μg/(kg · min) intermittent injection. Adjust the drug dosage during surgery based on the intensity of surgical stimulation and changes in hemodynamics. Stop administering sufentanil or fentanyl 10 minutes before the end of the surgery, and stop administering propofol at the end of the surgery. Send the tube into PACU. Then wait for the patient to recover spontaneous breathing, regain consciousness, swallow and cough reflexes before extubating.
Data Collection
Collect the following information from anesthesia records and medical records database. Collect patients’ age, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, and comorbidities from medical records. Obtain the following information from anesthesia records: 1) HR and MAP at 30 minutes before anesthesia induction (T0), after anesthesia completion (T1), at the time of skin incision (T2), at the end of surgery (T3), at the time of arrival at PACU (T4), 15 minutes after arrival at PACU (T5), and 30 minutes after arrival at PACU (T6). 2) Anesthesia effect, onset time of anesthesia, postoperative wake-up time, extubation time. 3) Pain levels at three hours, 12 hours, and 24 hours after surgery. Use the Visual Analog Scale (VAS) to assess postoperative pain levels; The total score is 0–10 points. The higher the score, the greater the degree of pain. 4) Cognitive function status at six, 24, and 72 hours postoperatively; Evaluate using the Montreal Cognitive Assessment Scale (MoCA); A MoCA score of less than 26 is considered cognitive impairment. 5) The incidence of bradycardia, hypotension, postoperative nausea and vomiting (PONV), urinary retention, respiratory depression and other adverse reactions within 72 hours after surgery were recorded. Definitions of outcome indicators were as follows: Hemodynamic stability was defined as maintaining heart rate (HR) and mean arterial pressure (MAP) within 20% of baseline values during surgery and early recovery, consistent with previous literature.17,18 Cognitive impairment was assessed using the Montreal Cognitive Assessment (MoCA), with a score <26 indicating mild cognitive dysfunction, as commonly used in geriatric anesthesia research.19 Adverse reactions were defined according to established perioperative criteria, including bradycardia (HR <50 bpm), hypotension (MAP <60 mmHg or >30% drop from baseline), PONV, urinary retention, and respiratory depression (SpO2 <90% or requiring assisted ventilation).20
Statistical Analysis
This study used SPSS 27.0 statistical software (IBM Corp, NY, USA) to analyze the collected data. Use Python 3.11.1 for propensity score matching. Count data is presented in the form of n (%), and inter group differences are measured using chi square test or Fisher’s exact probability method. Measurement data that conforms to a normal distribution are expressed in the form of mean ± standard deviation (SD). Use independent sample t-test to determine the difference between the two groups. Non normally distributed data are represented by median and interquartile range (IQR), and Mann Whitney U-test is used for inter group comparison. Use Shapiro–Wilk test to evaluate the normality of the evaluation data. P<0.05 indicates a significant difference. PRISM 9.0 software (GraphPad, San Diego, USA) is used to prepare charts. To address potential baseline imbalances, we employed two propensity score–based weighting techniques: stabilized inverse probability of treatment weighting (IPTW) and overlap weighting (OW). Propensity scores were estimated using logistic regression including the following covariates: age, body mass index (BMI), ASA classification, hypertension, diabetes, coronary heart disease, chronic obstructive pulmonary disease (COPD), and cerebrovascular disease. Initial attempts at 1:1 nearest neighbor matching with caliper (0.2 × SD of logit of PS) resulted in substantial sample loss. Therefore, we used weighting methods to retain statistical power. Overlap weighting was selected as the primary adjustment method due to its stability in small samples and ability to target the population with sufficient overlap between treatment groups. Covariate balance was assessed using standardized mean differences (SMDs), with values <0.1 considered acceptable Distribution of PS and covariate balance before and after weighting were illustrated in Supplementary eTable 1–2 and eFigure 1–3.
Results
This study included a total of 98 elderly male BPH patients, who were matched in a 1:1 ratio as either the PF group (n=49) or the PS group (n=49). There was no significant difference in demographic data between the two groups (P>0.05) (Table 1). Before weighting, several baseline variables demonstrated imbalance between groups, with absolute standardized mean differences (SMDs) exceeding 0.1 (Supplementary eTable 1). Propensity score distributions showed adequate overlap between the groups (Supplementary eFigure 1), supporting the use of weighting methods. After applying overlap weighting, all covariates achieved excellent balance (SMDs <0.05), as shown in Supplementary eTable 2. These improvements were visualized using Love plots for both IPTW and OW (Supplementary eFigure 2 and eFigure 3, respectively).
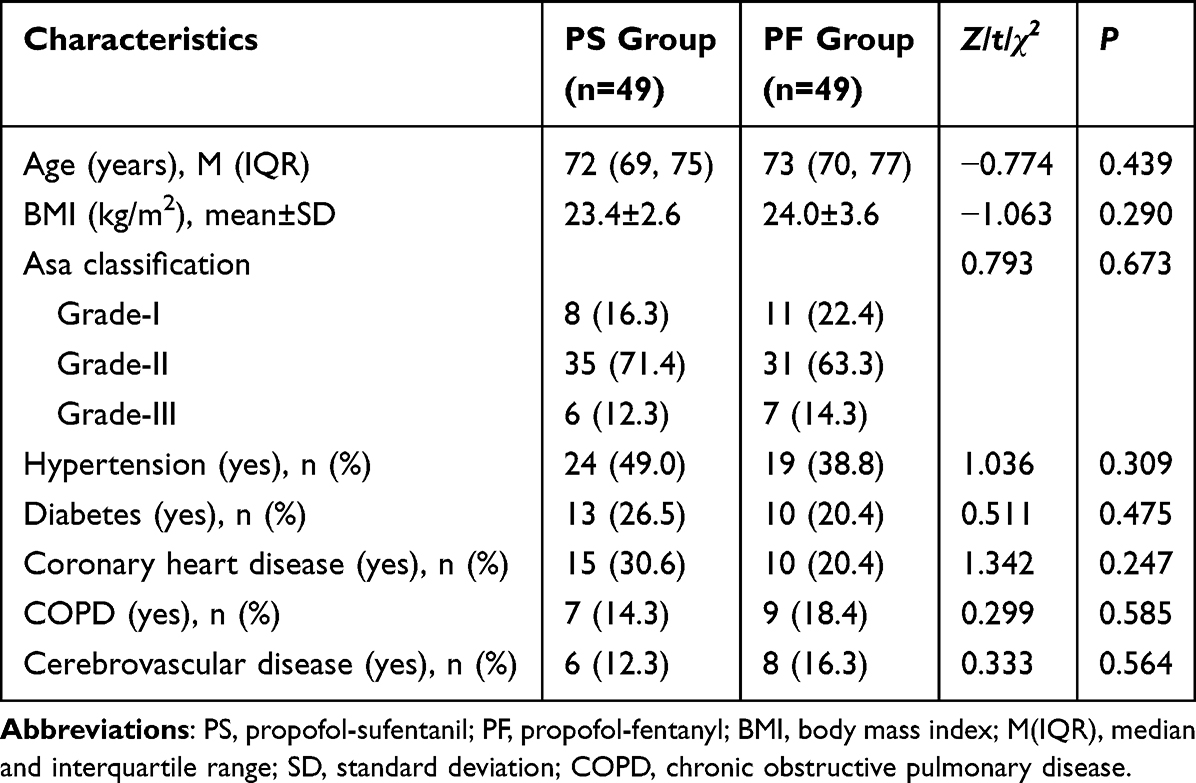 |
Table 1 Comparison of Population Characteristics Data Between Two Groups |
There were no statistically significant difference in HR and MAP between the two groups of patients at T0, T1, and T6 (P>0.05). The HR and MAP of the PS group were lower than those of the PF group at T2, T3, T4, and T5 (P<0.05) (Figure 1).
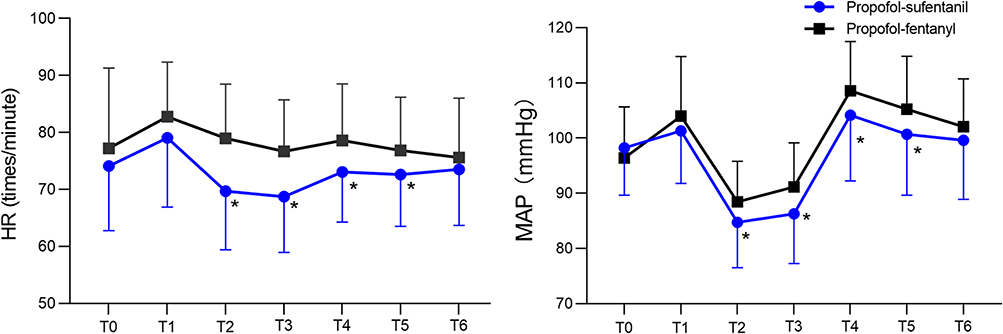 |
Figure 1 The hemodynamic changes during the perioperative period in two groups. HR (left); MAP (right). Compared with the PF group, *P<0.05. 30 minutes before anesthesia induction (T0); After anesthesia is completed (T1); During skin cutting (T2); At the end of the surgery (T3); Upon arrival at PACU (T4); 15 minutes after arriving at PACU (T5); 30 minutes after arrival at PACU (T6). |
The onset time of anesthesia, postoperative awakening time, and extubation time in the PS group were shorter than those in the PF group (P<0.05) (Table 2). After adjustment using overlap weighting, the PS group showed significantly shorter onset time of anesthesia (median 14 vs 16 minutes, difference: −2.34 [95% CI: −3.89 to −0.78], p=0.003), shorter postoperative awakening time (median 12 vs 15 minutes, difference: −2.62 [95% CI: −4.17 to −1.06], p=0.001), and shorter extubation time (median 15 vs 20 minutes, difference: −4.74 [95% CI: −6.65 to −2.83], p<0.001) compared to the PF group (Supplementary eTable 3).
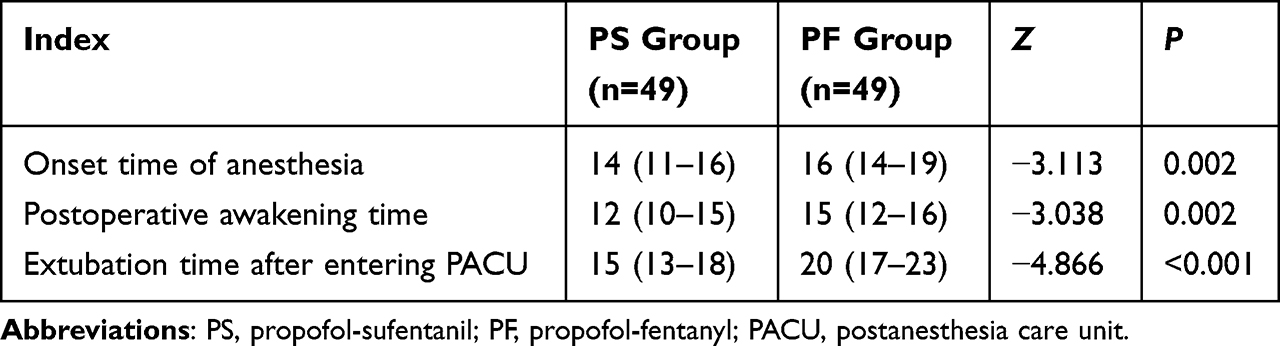 |
Table 2 Comparison of Anesthesia Onset Time, Postoperative Awakening Time, and Extubation Time Between Two Groups |
The pain VAS scores in the PS group were lower than those in the PF group at 12 and 24 hours after surgery (P<0.05) (Figure 2).
 |
Figure 2 Changes in pain levels within 24 hours after surgery in both groups. Compared with the PF group, *P<0.05. |
The number of patients with cognitive impairment at 6 and 24 hours after surgery in the PS group was lower than that in the PF group (P<0.05); However, there was no statistically significant difference in the number of patients with cognitive impairment 72 hours after surgery (P>0.05) (Table 3). Following overlap weighting adjustment, the PS group had lower incidence of postoperative cognitive dysfunction at 6 hours (14.3% vs 32.7%, OR: 0.173 [95% CI: 0.033–0.913], p=0.125) and 24 hours (6.1% vs 20.4%, OR: 0.433 [95% CI: 0.059–3.197], p=0.412), although these differences did not reach statistical significance. No meaningful difference was found at 72 hours postoperatively (Supplementary eTable 4).
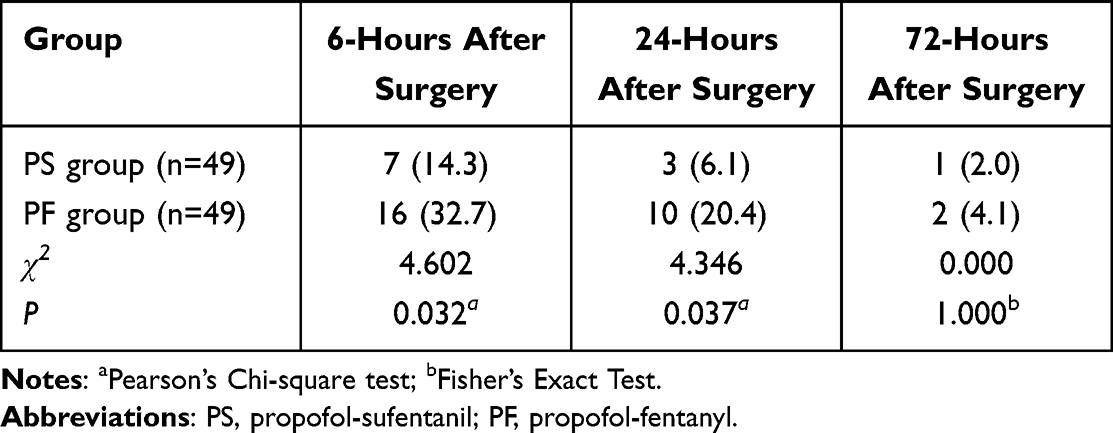 |
Table 3 Comparison of Postoperative Cognitive Dysfunction Between Two Groups |
There was no statistically significant difference between the two groups in the incidence of bradycardia, hypotension, PONV, urinary retention, respiratory depression and other adverse reactions within 72 hours after surgery (P>0.05) (Table 4). The weighted analysis showed no statistically significant differences in the incidence of bradycardia, hypotension, postoperative nausea and vomiting (PONV), urinary retention, or respiratory depression between the PS and PF groups (all p>0.05, Supplementary eTable 5).
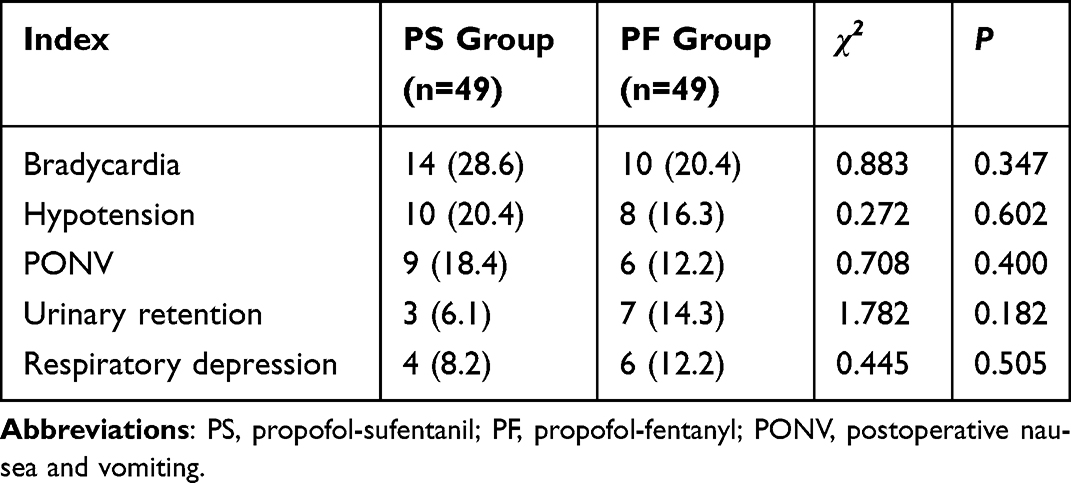 |
Table 4 Comparison of Incidence of Complications Within 72 Hours After Surgery Between Two Groups |
Discussion
In this study, we compared the effects of PF or sufentanil on anesthesia efficacy and postoperative cognitive function in elderly patients undergoing TURP. The results indicate that in elderly TURP, the PS has higher benefits in maintaining perioperative hemodynamic stability, anesthesia efficacy, postoperative pain control, protecting early postoperative cognitive function and complications.
In this study, we defined hemodynamic stability as the maintenance of HR and MAP within ±20% of baseline levels, in line with previous anesthesia literature.17,18 The PS group showed more consistent values during T2–T5, suggesting reduced intraoperative stress and better circulatory control. Elderly patients, especially those with cardiovascular comorbidities, are more vulnerable to perioperative fluctuations, and ensuring hemodynamic stability is critical to avoid postoperative complications including delirium and organ hypoperfusion.19,20 A randomized controlled trial (RCT) result showed a significant correlation between perioperative hemodynamics and postoperative cognitive function.21 The results of this study showed that the PS group exhibited lower heart rate (HR) and mean arterial pressure (MAP) at T2 to T5 compared to the PF group, with smaller deviations from baseline values. These findings suggest that PS was associated with reduced hemodynamic fluctuations during surgery and early recovery, which may contribute to improved circulatory control and anesthetic tolerance in elderly patients. Similarly, Ren et al11 also found that PS can provide more stable hemodynamics and reduce cognitive impairment in patients undergoing intertrochanteric fracture surgery. In addition, Qu et al22 also found that the PS had a smaller effect on the hemodynamics of radical mastectomy. We believe that this may be because the binding affinity between sufentanil and the μ receptor is 7–10 times stronger than that of fentanyl. By long-term inhibition of central pain sensitization pathways such as locus coeruleus, the secretion of adrenal medullary hormones and stress response are reduced. Thus, the impact of trauma on hemodynamics was reduced.23,24 Although the receptor affinity and analgesic potency of sufentanil are 7–10 times higher than those of fentanyl, the dosage used in our study did not strictly follow this ratio. The sufentanil dose was 0.1–0.2 μg/kg, while the fentanyl dose was 3–5 μg/kg during induction. This corresponds to approximately a 1:20–1:30 ratio. However, considering the differences in pharmacokinetics and clinical potency between the two drugs, such as sufentanil’s higher lipophilicity, faster onset, shorter context-sensitive half-life, and more stable hemodynamic profile, the selected dosing was designed to achieve clinical equivalence rather than strict numerical potency matching. Additionally, anesthesiologists dynamically adjusted intraoperative doses based on vital signs to ensure anesthetic depth and safety. Therefore, the efficacy differences observed in this study are less likely to be attributed to underdosing or overdosing and more likely reflect true pharmacodynamic advantages of sufentanil.
In terms of perioperative indicators, the PS group had shorter onset time of anesthesia, postoperative awakening time, and extubation time. This is consistent with the research results of Zhang et al25 and Chen et al.26 This is mainly because sufentanil has a stronger affinity for the μ receptor than fentanyl, making it easier to quickly cross the blood-brain barrier and occupy the central analgesic site.25–27 Meanwhile, because the half-life of sufentanil is shorter than fentanyl, it is metabolized and cleared faster in the body, and the central inhibitory effect subsides rapidly, resulting in faster postoperative recovery.27,28 Yu et al29 found in a study involving 182 patients that the average recovery time of PS was 12.3 ± 3.7 minutes. This is similar to the recovery time (M (IQR): 12 (10–15) minutes) of the PS group in this study.
In terms of postoperative pain control, the VAS scores of the PS group were lower than those of the PF group at 12 and 24 hours after surgery. This is consistent with previous research results.22,30 Sufentanil, with its high lipophilicity and high affinity for μ receptors, can continue to exert potent analgesic effects after surgery, significantly reducing patients’ pain perception.27,30 Xu et al31 also found that sufentanil can exert greater analgesic effects for a longer period of time and reduce the incidence of respiratory depression and adverse events. It can be seen that the long-acting analgesic properties of sufentanil can reduce the need for postoperative salvage analgesia.30,31 However, at three hours postoperatively, there was no significant difference in VAS scores between the two groups. We believe that it may be due to the use of equivalent doses in our surgery, the large distribution volume of fentanyl, and the continuous release of drugs from adipose tissue into the bloodstream after discontinuation, forming a “secondary peak”.29–31
Postoperative cognitive impairment (POCD) remains a major challenge that worsens the prognosis of elderly surgical patients.32 This study found that PS significantly reduced the number of patients with cognitive impairment at six and 24 hours after surgery compared to PF. This is mainly due to the short acting and fast metabolism characteristics of sufentanil, which makes its impact on the central nervous system relatively small.30–32 The pharmacokinetic characteristics of propofol, such as short half-life and rapid clearance, together reduce the accumulation of anesthetic drugs in the brain and decrease neurotoxicity.31,32 Zeng et al32 found in a meta-analysis of 34 studies that the incidence of POCD with sufentanil was 6.3%, significantly lower than fentanyl’s 23.9%. This is consistent with the results of this study, confirming that sufentanil is more effective in protecting nerve cells in elderly surgical patients.
Elderly surgical patients have a higher incidence of postoperative complications due to their complex physical conditions.32,33 In this study, the main complications were bradycardia (24.5%, 24/98), hypotension (18.4%, 18/98), PONV (15.3%, 15/98), urinary retention and respiratory depression (10.2%, 10/98). However, there was no significant difference in the incidence of various complications between the two groups. For bradycardia, we use anticholinergic drugs such as atropine; Treating hypotension by adjusting blood volume and vasoactive drugs; Using 5-hydroxytryptamine receptor antagonists to prevent PONV; For urinary retention, we can first take induced micturition or catheterization, and if there is no improvement, we can take bladder function training combined with drug intervention (such as alpha receptor blocker). Respiratory depression requires high flow mask oxygen (6–10 L/min) to maintain SpO2 > 95%. If heart rate is less than 50 beats per minute, intravenous injection of atropine 0.5 mg is necessary. In addition, intravenous infusion of 0.1 mg of nalmefene 30 minutes before the end of surgery can prevent postoperative respiratory depression.25–30
While both fentanyl and sufentanil are approved and effective agents, our findings suggest that sufentanil may offer additional advantages in elderly patients, particularly in reducing cognitive dysfunction and enhancing perioperative recovery. These observations may help refine anesthetic protocols for TURP in older adults, who often require more individualized approaches due to their physiological vulnerabilities. To our knowledge, this is the first study comparing the anesthetic efficacy and postoperative cognitive function effects of PF or sufentanil in elderly patients undergoing TURP. The results showed that PS has a series of advantages. However, Yu et al16 found that using a dose of 0.2 μg/kg sufentanil can reduce the consumption of propofol, but the incidence of respiratory depression in patients is significantly higher than that of 0.1 μg/kg. Akarsu Ayazoglu et al34 also found that the incidence of complications with sufentanil 0.5 μg/kg was significantly higher than that with sufentanil 0.25 μg/kg. However, in our study, the specific dosage of PS was not provided. Therefore, in future research, it is necessary to further explore the optimal dosage of PS for different subgroups of populations.
To enhance the internal validity of our findings, we applied two propensity score-based weighting techniques (IPTW and overlap weighting) to adjust for baseline imbalances between the PS and PF groups. Despite initial differences in covariates, overlap weighting achieved excellent covariate balance, as demonstrated by standardized mean differences close to zero. Importantly, the key findings—including shorter perioperative recovery times and lower incidence of early cognitive dysfunction in the PS group—remained consistent after adjustment. These results support the robustness of our conclusions and suggest that the observed effects are unlikely to be explained by confounding bias.
This study still has certain limitations: firstly, it is a retrospective study with a relatively limited sample size, only including patients aged 65 and above, and cannot represent the entire population. Secondly, the postoperative cognitive function assessment only evaluated the incidence within 72 hours after surgery, lacking continuous tracking of long-term cognitive function changes. Thirdly, we excluded patients who underwent ICU after surgery, which resulted in incomplete statistics of postoperative complications. Fourthly, different dosage combinations have varying effects on anesthesia efficacy and cognitive function, and further exploration is needed to determine the optimal dosage for different subgroups of the population; Finally, without comparison with other analgesic drug combinations or anesthesia methods, it is difficult to fully highlight the advantages of PS.
Conclusion
The anesthesia effect of PS for elderly TURP is superior to PF. It can effectively maintain stable perioperative hemodynamics, reduce postoperative pain, shorten perioperative time, protect early postoperative cognitive function, and has good safety. In the future, it is necessary to expand the sample size, extend the follow-up period, and compare with different analgesics or anesthesia methods to find better anesthesia measures for elderly TURP patients.
Abbreviations
PS, propofol-sufentanil; TURP, transurethral resection of the prostate; GA, general anesthesia; PF, propofol-fentanyl; HR, heart rate; MAP, mean arterial pressure; VAS, visual analogue scale; PACU, postanesthesia care unit; MoCA, Montreal Cognitive Assessment Scale; BMI, body mass index; SD, standard deviation; IQR, interquartile range; BPH, benign prostatic hyperplasia; POCD, postoperative cognitive impairment; ASA, American Society of Anesthesiologists; ECG, electrocardiogram; PONV, postoperative nausea and vomiting.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All procedures performed in the study involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee(s) and the Helsinki Declaration (revised in 2013). The requirement for informed consent was waived by the ethics committee because of the observational and retrospective nature of the study. This study was approved by the Ethics Committee of the First People’s Hospital of Yongkang City, with the approval number EC2025-LW-017-01(K), issued on July 22, 2025. All procedures were carried out in accordance with institutional guidelines, the Declaration of Helsinki (2013 revision), and Good Clinical Practice (GCP) principles. The requirement for informed consent was waived by the ethics committee due to the retrospective nature of the study and anonymized data processing. All data were stored securely and confidentiality was maintained throughout the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Launer BM, McVary KT, Ricke WA, Lloyd GL. The rising worldwide impact of benign prostatic hyperplasia. BJU Int. 2021;127(6):722–728. doi:10.1111/bju.15286
2. Zi H, Liu MY, Luo LS, et al. Global burden of benign prostatic hyperplasia, urinary tract infections, urolithiasis, bladder cancer, kidney cancer, and prostate cancer from 1990 to 2021. Mil Med Res. 2024;11(1):64. doi:10.1186/s40779-024-00569-w
3. Shvero A, Calio B, Humphreys MR, Das AK. HoLEP: the new gold standard for surgical treatment of benign prostatic hyperplasia. Can J Urol. 2021;28(S2):6–10.
4. Ottaiano N, Shelton T, Sanekommu G, Benson CR. Surgical complications in the management of benign prostatic hyperplasia treatment. Curr Urol Rep. 2022;23(5):83–92. doi:10.1007/s11934-022-01091-z
5. Feng F, Chen Z, Cromer J, et al. Anesthetic concerns for patients undergoing a transurethral resection of the prostate (TURP). Urol Nurs. 2016;36(2):75–81. PMID: 27281864.
6. Darwish OM, Lutnick E, Dalimov Z, et al. Neuraxial vs general anesthesia: 30-day mortality outcomes following transurethral resection of prostate. Urology. 2021;157:274–279. doi:10.1016/j.urology.2021.06.034
7. Longo MA, Cavalheiro BT, de Oliveira Filho GR. Laparoscopic cholecystectomy under neuraxial anesthesia compared with general anesthesia: systematic review and meta-analyses. J Clin Anesth. 2017;41:48–54. doi:10.1016/j.jclinane.2017.06.005
8. Silvani C, Lucignani G, Bebi C, et al. General anesthesia is associated with lower perioperative bleeding and better functional outcomes than spinal anesthesia for endoscopic enucleation of the prostate: a single-center experience. World J Urol. 2024;42(1):569. doi:10.1007/s00345-024-05271-z
9. Becerra Á, Valencia L, Saavedra P, Rodríguez-Pérez A, Villar J. Effect of prewarming on body temperature in short-term bladder or prostatic transurethral resection under general anesthesia: a randomized, double-blind, controlled trial. Sci Rep. 2021;11(1):20762. doi:10.1038/s41598-021-00350-2
10. Wang LL, Guan ZY, Wang CM, Zhang YW, Zhang J, Zhao P. A comparative study on the efficacy and safety of propofol combined with different doses of alfentanil in gastroscopy: a randomized controlled trial. J Anesth. 2023;37(2):201–209. doi:10.1007/s00540-022-03145-5
11. Ren J, Wang L, Sun X. The effect of propofol combined with sufentanil on anesthetic effect, cognitive function, and hemodynamics in patients undergoing intertrochanteric fracture surgery evaluated by propensity score matching. Am J Transl Res. 2023;15(5):3607–3615.
12. Mercadante S. Influence of aging on opioid dosing for perioperative pain management: a focus on pharmacokinetics. J Anesth Analg Crit Care. 2024;4(1):51. doi:10.1186/s44158-024-00182-2
13. Wen Q, Sun D, Yang L, Li Y. Impact of butorphanol versus sufentanil on postoperative cognition and inflammation in elderly: a pilot study. Front Aging Neurosci. 2024;16:1395725. doi:10.3389/fnagi.2024.1395725
14. Zhao W, Hu Y, Chen H, et al. The effect and optimal dosage of dexmedetomidine plus sufentanil for postoperative analgesia in elderly patients with postoperative delirium and early postoperative cognitive dysfunction: a single-center, prospective, randomized, double-blind, controlled trial. Front Neurosci. 2020;14:549516. doi:10.3389/fnins.2020.549516
15. Al-Qurain AA, Upton R, Williams DB, et al. Population pharmacokinetic model of subcutaneous fentanyl in older acute care patients. Eur J Clin Pharmacol. 2021;77(9):1357–1368. doi:10.1007/s00228-021-03126-9
16. Yu J, Xiang B, Song Y, Chen H, Li Y, Liu C. ED50 of propofol in combination with low-dose sufentanil for intravenous anaesthesia in hysteroscopy. Basic Clin Pharmacol Toxicol. 2019;125(5):460–465. doi:10.1111/bcpt.13280
17. Varpaei HA, Farhadi K, Mohammadi M, et al. Postoperative cognitive dysfunction: a concept analysis. Aging Clin Exp Res. 2024;36(1):133. doi:10.1007/s40520-024-02779-7
18. Suraarunsumrit P, Srinonprasert V, Kongmalai T, et al. Outcomes associated with postoperative cognitive dysfunction: a systematic review and meta-analysis. Age Ageing. 2024;53(7):afae160. doi:10.1093/ageing/afae160
19. Vacas S, Cole DJ, Cannesson M. Cognitive decline associated with anesthesia and surgery in older patients. JAMA. 2021. doi:10.1001/jama.2021.4773
20. Wu H, Song J, Hu Z, et al. Basic research on postoperative cognitive dysfunction in the past decade: a bibliometric analysis. Front Aging Neurosci. 2025;17:1529860. doi:10.3389/fnagi.2025.1529860
21. Kozarek K, Sanders RD, Head D. Perioperative blood pressure in the elderly. Curr Opin Anaesthesiol. 2020;33(1). doi:10.1097/ACO.0000000000000820
22. Qu L, Wu X. Clinical value of total intravenous anesthesia with sufentanil and propofol in radical mastectomy. Dis Markers. 2022;2022:7294358. doi:10.1155/2022/7294358
23. Volpe DA, McMahon Tobin GA, Mellon RD, et al. Uniform assessment and ranking of opioid μ receptor binding constants for selected opioid drugs. Regul Toxicol Pharmacol. 2011;59(3):385–390. doi:10.1016/j.yrtph.2010.12.007
24. Zhang C, Huang D, Zeng W, et al. Effect of additional equipotent fentanyl or sufentanil administration on recovery profiles during propofol-remifentanil-based anaesthesia in patients undergoing gynaecologic laparoscopic surgery: a randomized clinical trial. BMC Anesthesiol. 2022;22(1):127. doi:10.1186/s12871-022-01671-z
25. Zhang J, Chen L, Sun Y, He W. Comparative effects of fentanyl versus sufentanil on cerebral oxygen saturation and postoperative cognitive function in elderly patients undergoing open surgery. Aging Clin Exp Res. 2019;31(12):1791–1800. doi:10.1007/s40520-019-01123-8
26. Chen W, Guoyang H, Yu H, Xu Y. Comparisons of fentanyl and sufentanil on recovery time after inguinal hernia repair in children: a randomized clinical trial. BMC Surg. 2024;24(1):55. doi:10.1186/s12893-024-02346-x
27. van de Donk T, Ward S, Langford R, Dahan A. Pharmacokinetics and pharmacodynamics of sublingual sufentanil for postoperative pain management. Anaesthesia. 2018;73(2):231–237. doi:10.1111/anae.14132
28. Pokorná P, Šíma M, Koch B, Tibboel D, Slanař O. Sufentanil disposition and pharmacokinetic model-based dosage regimen for sufentanil in ventilated full-term neonates. Pharmacology. 2021;106(7–8):384–389. doi:10.1159/000515787
29. Yu Y, Qi SL, Zhang Y. Role of combined propofol and sufentanil anesthesia in endoscopic injection sclerotherapy for esophageal varices. World J Gastroenterol. 2017;23(44):7875–7880. doi:10.3748/wjg.v23.i44.7875
30. Fu Y, Liu Q, Nie H. Efficacy of opioids for traumatic pain in the emergency department: a systematic review and Bayesian network meta-analysis. Front Pharmacol. 2023;14:1209131. doi:10.3389/fphar.2023.1209131
31. Xu N, Chen Q, Huang ST, Sun KP, Cao H. Sufentanil reduces emergence delirium in children undergoing transthoracic device closure of VSD after sevoflurane-based cardiac anesthesia. Braz J Cardiovasc Surg. 2020;35(5):660–665. doi:10.21470/1678-9741-2019-0334
32. Zeng K, Long J, Li Y, Hu J. Preventing postoperative cognitive dysfunction using anesthetic drugs in elderly patients undergoing noncardiac surgery: a systematic review and meta-analysis. Int J Surg. 2023;109(1):21–31. doi:10.1097/JS9.0000000000000001
33. Zang SS, Zhao Q, Xiao N, Liu S. Efficacy of Vitamin-D supplementation in improving the prognosis of H-type hypertension in elderly patients. Pak J Med Sci. 2024;40(10):2379–2383. doi:10.12669/pjms.40.10.8464
34. Akarsu Ayazoglu T, Uzman S. Combination of propofol and nasal sufentanil or intravenous midazolam for colonoscopy: a comparative study. Anaesthesiol Intensive Ther. 2021;53(2):146–152. doi:10.5114/ait.2021.106298
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Successful Use of Low-Dose Combination Propofol and Fentanyl in Cataract Surgery Phacoemulsification
Irawati D, Adli M, Yadi DF
Clinical Ophthalmology 2023, 17:1929-1937
Published Date: 5 July 2023
The Effect of Sevoflurane Combined with Propofol Anesthesia on Hemodynamics and Pain in Elderly Patients Undergoing Radical Surgery for Malignant Tumors
Qi L, Yi XC, Li C, Li Y
International Journal of General Medicine 2025, 18:2197-2206
Published Date: 18 April 2025
Comparison of Esketamine/Propofol and Sufentanil/Propofol on Intraoperative Hypoxemia During Bronchoscopy: A Randomized Trial
Huang X, Li X, Sun Y, Wu A, Ai P
Drug Design, Development and Therapy 2025, 19:4429-4436
Published Date: 27 May 2025