Back to Journals » Journal of Pain Research » Volume 18
Comparative Analysis of Paraspinal Muscle Fat Infiltration and Clinical Efficacy Following Single-Level UBD-TLIF versus MIS-TLIF: A Retrospective MRI-Based Study
Authors Yan J, Tian M, Wu M, Yuan Z, Fan Y, Wu X, Ni H ![]() , Zhao Y, Yu S, He S
, Zhao Y, Yu S, He S ![]()
Received 7 December 2024
Accepted for publication 29 September 2025
Published 30 October 2025 Volume 2025:18 Pages 5673—5680
DOI https://doi.org/10.2147/JPR.S507695
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Jiajun Yan,1,2,* Muhang Tian,1,2,* Min Wu,1,2,* Zhixin Yuan,1,2 Yunshan Fan,1,2 Xinbo Wu,1,2 Haijian Ni,1,2 Yingchuan Zhao,1,2 Shunzhi Yu,1,2 Shisheng He3
1Department of Orthopaedics, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 2Spinal Pain Research Institute, Tongji University School of Medicine, Shanghai, People’s Republic of China; 3Department of Orthopaedics, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shisheng He, Department of Orthopaedics, Shanghai East Hospital, School of Medicine, Tongji University, 150 Jimo Road, Shanghai, 20092, People’s Republic of China, Email [email protected] Shunzhi Yu, Orthopedic Department, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, 301 Yanchang Road, Shanghai, 200072, People’s Republic of China, Email [email protected]
Purpose: The paraspinal muscles, particularly the multifidus and erector spinae, are essential for supporting physiological loads, coordinating functional movements, and ensuring lumbar segment stability. This study aims to evaluate the effectiveness of Uni-Portal Bi-Channel Dual-Media Transforaminal Lumbar Interbody Fusion (UBD-TLIF) versus Minimally Invasive Transforaminal Lumbar Interbody Fusion (MIS-TLIF) in minimizing paraspinal muscle damage during lumbar surgeries.
Methods: This retrospective study analyzed patients who underwent single-level UBD-TLIF or MIS-TLIF from January 2020 to December 2022. Key outcomes measured included preoperative and postoperative Visual Analog Scale (VAS) scores for back and leg pain, Oswestry Disability Index (ODI) scores, radiological changes in paravertebral muscle integrity via MRI, operative time, estimated blood loss, and length of hospital stay.
Results: Among 103 patients (51 cases in UBD-TLIF group), no significant baseline differences were observed. Although UBD-TLIF takes longer operative time (210.80± 71.86 min vs 181.12± 36.74 min, P=0.002), UBD-TLIF group showed a significant less reduction in fat infiltration with a mean change of 7.29± 2.46 versus 10.51± 3.72 for MF (P< 0.001) and 4.63± 1.98 versus 7.62± 2.83 for ES (P< 0.001). Earlier recovery was noted in UBD-TLIF group, with Day 3 postoperative VAS scores for back pain significantly lower (2.12± 0.84) compared to MIS-TLIF (3.48± 1.08, P< 0.001), also shorter length of hospital stay (7.02± 1.75 vs 8.38± 1.33, P< 0.001). Additionally, UBD-TLIF group showed less estimated blood loss (155.69± 93.41mL vs 230.96± 102.18 mL, P< 0.001).
Conclusion: UBD-TLIF offers clinical outcomes comparable to MIS-TLIF for single-level lumbar interbody fusion surgery while providing enhanced muscle preservation and faster postoperative recovery. Additionally, the use of T2-weighted MRI and ImageJ software for measuring fat infiltration rates proves to be a reliable method.
Keywords: UBD-TLIF, MIS-TLIF, magnetic resonance imaging, fat infiltration, paraspinal muscle
Corrigendum for this paper has been published.
Introduction
Transforaminal lumbar interbody fusion (TLIF) has traditionally been a standard approach in lumbar fusion surgeries. However, the development of minimally invasive spinal techniques has positioned Minimally Invasive Transforaminal Lumbar Interbody Fusion (MIS-TLIF) as a preferred method for treating various spinal regenerative diseases.1,2 This technique utilizes tubular retractors to access the facet joint and employs paramedian incisions with microscopic or endoscopic assistance, facilitating a muscle-splitting approach that aims to reduce soft tissue damage and postoperative complications, while achieving clinical and radiographic outcomes comparable to open surgeries. Despite its advantages, MIS-TLIF presents challenges such as a steep learning curve, potentially longer operative times, increased intraoperative radiation exposure, and risks related to cage and pedicle screw positioning and migration.1,2
Endoscopic-assisted TLIF allows direct decompression of the neural structure and complete lumbar interbody fusion with minor injury.3 Our previous studies introduced a Uni-Portal Bi-Channel Dual-Media (UBD) spinal endoscope system, also known as the V-Shape Bi-Channel Endoscopy (VBE), as an innovative approach to spinal surgery.3–6 Unlike traditional single-port, single-channel coaxial endoscopes or unilateral bi-portal endoscopes, the UBD system features a non-coaxial architecture with dual-working channels. This design not only provides a larger operative field but also maintains a fixed spatial relationship between the working and endoscopic channels, closely aligning with traditional endoscopic spinal surgery practices and allowing continuous real-time visualization during surgery.
The paraspinal muscles, particularly the multifidus and erector spinae, are essential for supporting physiological loads, coordinating functional movements, and ensuring lumbar segment stability.6–8 Compared to traditional open surgery, MIS-TLIF is effective in reducing muscle atrophy, alleviating low back pain, and decreasing the incidence of failed back surgery syndrome by significantly minimizing traumatic dissection and soft tissue damage.9 UBD-TLIF, as an innovative minimally invasive approach for lumbar interbody fusion, aims to further reduce muscle injuries compared to conventional minimally invasive endoscopic spinal procedures. Our previous research demonstrated a reduction in postoperative back pain and inflammatory markers following UBD-TLIF.5 Yet, there remains an absence of studies directly comparing the postoperative paravertebral muscle changes between UBD-TLIF and MIS-TLIF, specifically regarding muscle cross-sectional area (CSA) and fat infiltration (FI). This study aims to assess these muscular alterations one year after surgery using Magnetic Resonance Imaging (MRI), and to explore the impact of these changes on surgical outcomes.
Materials and Methods
Participants and Clinical Data Collection
This retrospective study adhered to the Declaration of Helsinki, written informed consent was obtained from each patient. And, it was approved by the Institutional Review Boards of Shanghai Tenth People’s Hospital. From January 2020 to December 2022, consecutive patients who underwent single-level MIS-TLIF or UBD-TLIF were enrolled, the exclusion criteria included: 1) severe scoliosis deformity or lumbar spondylolisthesis; 2) spinal infections or tumors; 3) severe osteoporosis or back muscle atrophy; 4) severe stenosis that requires bilateral decompression; 5) obesity with a BMI over 30; 6) history of lumbar surgery; 7) lack of MRI or clinical data. This retrospective cohort study was approved by the Institutional Review Boards of our hospital. Demographic parameters and clinical data were collected from hospital electronic records.
Clinical Evaluation
Primary surgical outcomes included Visual Analog Scale (VAS) scores for back and leg pain, Oswestry Disability Index (ODI) scores and the change in FI of the multifidus(MF) and erector spinae(ES) muscles. Secondary outcomes included operative time, blood loss, hospital stay, complications, and global outcome based on the Macnab outcome criteria. VAS scores for back and leg pain were collected preoperatively, as well as 3 days, 3 months, and 12 months postoperatively. ODI version 2.0 was used to assess the impact of the patient’s back and leg condition on daily life, measured preoperatively, 3 months, and 12 months postoperatively. Global outcomes were categorized as excellent, good, fair, or poor based on Macnab criteria at 12 months postoperatively, with favorable outcomes defined as excellent or good.10
Surgical Procedures
The surgeries were performed by a team of three experienced surgeons. For MIS-TLIF, a single 2.5 cm paramedian skin incision was made at the decompression site, followed by blunt dissection through the multifidus and longissimus muscles to expose the lamina and facet joint. A tubular retractor system was used for muscle retraction, and procedures including facet joint removal, posterior soft tissue decompression, disc removal, and interbody fusion were performed. Bilateral percutaneous vertebral body screw fixation was completed under C-arm fluoroscopy guidance. UBD-TLIF was performed as previously described, with percutaneous pedicle screws placed first, followed by guided puncture needle positioning and the establishment of the working channel under fluoroscopy. Specialized tools were used for bone block removal, nucleus pulposus extraction, intervertebral space expansion, bone grafting, and fusion cage implantation. Decompression and percutaneous pedicle screw fixation were then finalized.
Radiological Quantification
Radiographic parameters were independently measured by two physicians to evaluate the extent of paravertebral muscle damage in both groups. A functional cross-sectional area (FCSA) approach was employed to assess this damage (Figure 1).11 The FCSA measurement was obtained by selecting a threshold signal within the total muscle CSA to include only pixels within the lean muscle tissue range.12 Preoperative and approximately one-year postoperative lumbar MRI scans were obtained using a 1.5-Tesla model (Signa; General Electric Medical Systems, Milwaukee, WI, USA) to minimize susceptibility artifacts near metallic implants. Axial images at intervertebral disc levels from L2–3 to L5–S1 were acquired on T2-weighted images, aligned horizontally to the vertebral endplates.
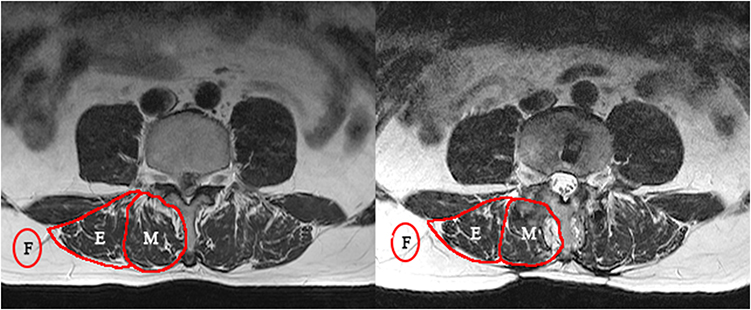 |
Figure 1 Schematic representation of Fatty Infiltration (F) measurement pre- and post-surgery. The left side illustrates the preoperative state, while the right side depicts the postoperative condition. The images display the measurement of Fatty Infiltration in the fusion side of the Multifidus (M) and Erector Spinae (E) muscles using Magnetic Resonance Imaging (MRI). The Fatty Infiltration is quantified by comparing the Total Muscle Cross-Sectional Area (TCSA) and the Functional Cross-Sectional Area (FCSA), indicating the degree of muscle composition replacement by fat. |
After scanning, the DICOM files were archived in a standard Picture Archiving and Communication System (PACS) and subsequently analyzed using the ImageJ software. In detail, first the total cross-sectional area (CSA) of each muscle was defined by outlining the innermost fascial border surrounding the muscle, including all fat within the fascial border. Fat located between the multifidus and the vertebral plate or spinous process is contained in the multifidus CSA, and fat located between the multifidus and erector spinae is contained in the erector spinae CSA. Next create a grayscale range for the lean muscle tissue on each scanned section, with 4–6 regions of interest (ROIs) taken from the areas of lean muscle tissue visible on each section (multifidus and erector spinae). The maximum value obtained from the sample ROIs is used as the highest threshold for distinguishing muscle tissue from fat. The substitution of lean muscle by fat is a marker of reduced muscle contractile tissue and the onset of muscle steatosis. Fatty Infiltration (FI) was used as a metric to quantify muscle FI on T2-weighted axial images, defined as the ratio of (TCSA - FCSA) to TCSA. Following the measurement of TCSA and FCSA, the change in FI was calculated as postoperative FI minus preoperative FI. Comparisons between the two groups were made to discern differences before and after surgery.
Statistical Analysis
Statistical analyses were performed using SPSS version 22.0 (SPSS, USA). The Intraclass Correlation Coefficient (ICC) was utilized to assess intra-rater and inter-rater reliability, demonstrating high reliability with values exceeding 89%. Frequency analysis and Chi-square tests were employed for categorical variables to assess group differences, while continuous data were expressed as mean ± standard deviation (SD). Normality of data was tested using the Shapiro–Wilk test. Depending on data normality and variance homogeneity, independent t-tests, Welch’s t-tests, or Mann–Whitney tests were applied. A P-value of <0.05 was considered statistically significant.
Results
The basic clinical characteristics of the study population are presented in Table 1. The study included 51 patients in the UBD-TLIF group and 52 in the MIS-TLIF group. There were no significant differences between groups in baseline characteristics such as gender distribution, age, or surgical segments involved. Preoperatively, VAS scores for back pain were 6.27 ± 1.08 in the UBD-TLIF group and 6.04 ± 1.25 in the MIS-TLIF group, while VAS scores for leg pain were 6.20 ± 1.25 and 5.83 ± 1.20, respectively. The ODI scores were 58.43 ± 5.63 in the UBD-TLIF group and 59.16 ± 6.06 in the MIS-TLIF group, with no significant baseline differences between the two groups (Table 2). On postoperative day 3, VAS scores for back pain were 3.48 ± 1.08 for the MIS-TLIF group and 2.12 ± 0.84 for the UBD-TLIF group (P < 0.001). However, no significant differences in VAS and ODI scores were observed between groups at other postoperative time points.
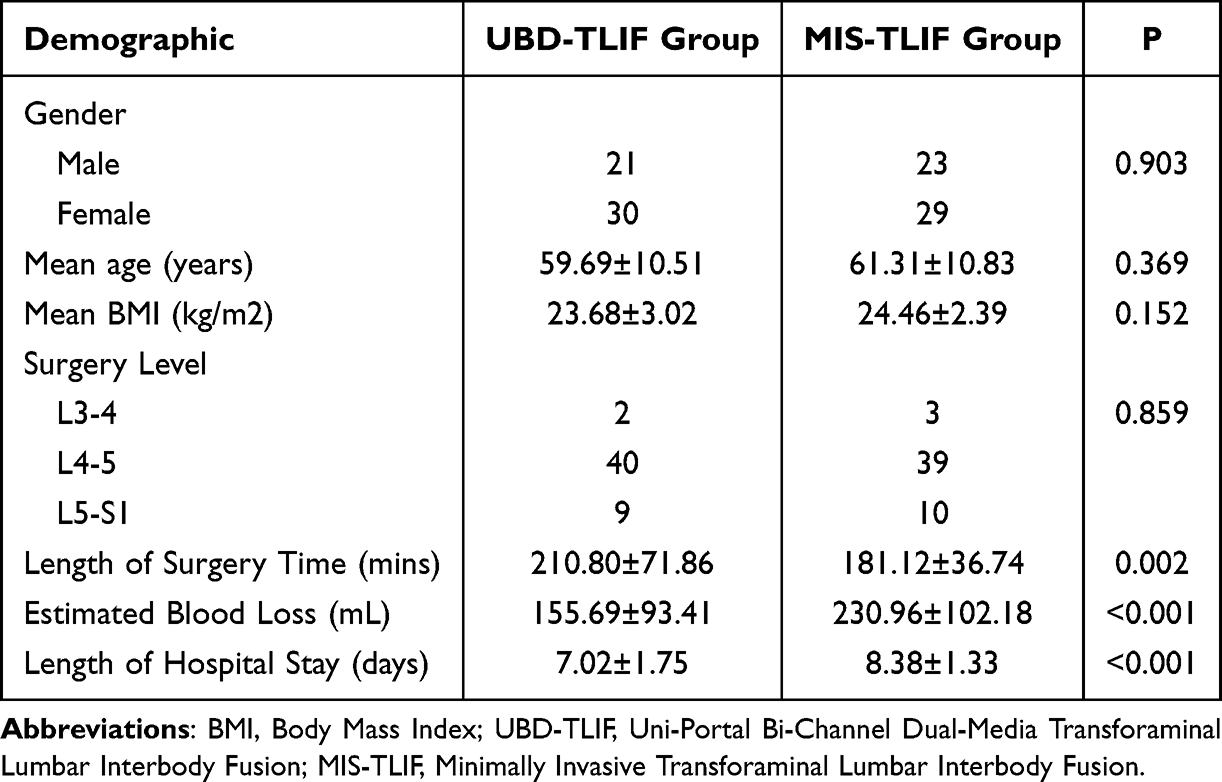 |
Table 1 Demographic and Clinical Characteristics of Patients Undergoing UBD-TLIF and MIS-TLIF |
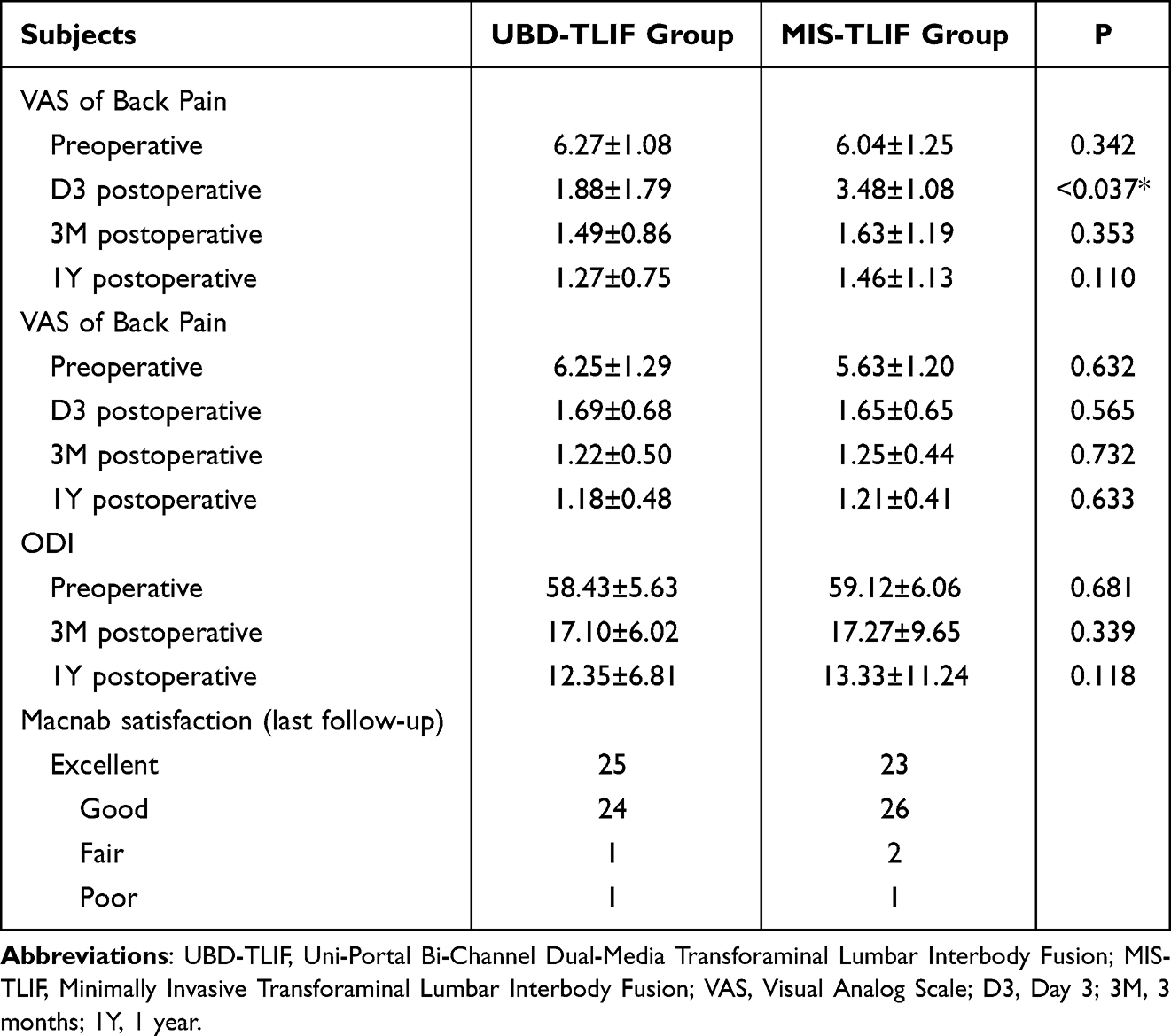 |
Table 2 Comparative Analysis of Patient-Reported Outcomes Measures Following UBD-TLIF and MIS-TLIF |
The ICC demonstrated excellent reliability in repeated measurements (Table 3). Postoperatively, the mean FI change of the multifidus muscle was 7.29 ± 2.46 in the UBD-TLIF group and 10.51 ± 3.72 in the MIS-TLIF group (P < 0.001), while the FI change of the erector spinae muscle was 4.63 ± 1.98 and 7.62 ± 2.83, respectively (P < 0.001). In addition, the FCSA change of the multifidus muscle was 1.32 ± 0.26 in the UBD-TLIF group and 1.98 ± 0.22 in the MIS-TLIF group (P = 0.042), while the FCSA change of the erector spinae muscle was 2.51 ± 0.58 and 2.96 ± 0.63, respectively (P = 0.036). There was also a statistically significant difference (P<0.001) in the postoperative gray values between the two groups. The average gray value of MF in the UBD-TLIF group (10.04 ± 2.40) compared to the MIS-TLIF group (7.67 ± 2.35, P < 0.001) and ES in the UBD-TLIF group (10.84 ± 2.37) compared to the MIS-TLIF group (8.79 ± 2.34, P < 0.001) (Figure 2).
 |
Table 3 Intra-Rater and Inter-Rater Reliability of Cross-Sectional Area Measurements in Paraspinal Muscle |
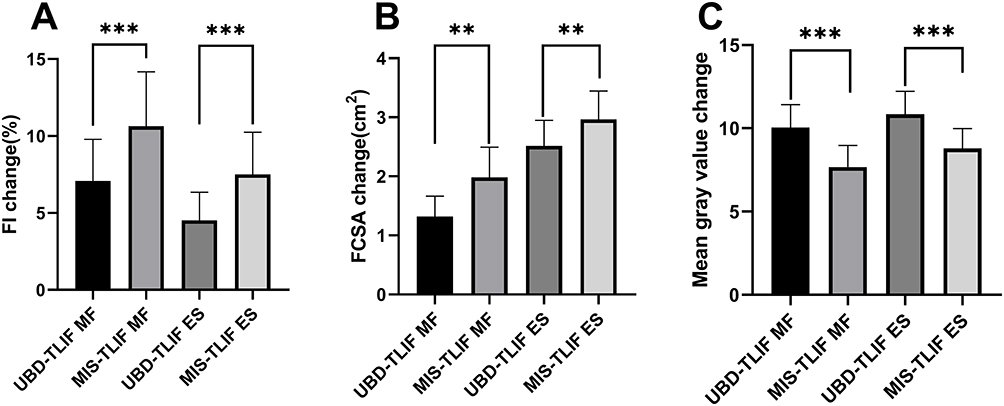 |
Figure 2 Comparative analysis of muscle characteristics changes in the Multifidus (MF) and Erector Spinae (ES) muscles following Uni-Portal Bi-Channel Dual-Media Transforaminal Lumbar Interbody Fusion (UBD-TLIF) and Minimally Invasive Transforaminal Lumbar Interbody Fusion (MIS-TLIF) procedures. (A) Comparative analysis of Fatty Infiltration (FI) in the MF and ES; (B) Comparative analysis of Functional cross-sectional area (FCSA) in the MF and ES; (C) Comparative analysis of mean gray value in the MF and ES. ***P<0.001; **P<0.05. |
In terms of operative time, the UBD-TLIF group had an average duration of 210.80 ± 71.86 minutes, compared to 181.12 ± 36.74 minutes for the MIS-TLIF group (P = 0.002), indicating shorter surgery times for the latter. The average estimated blood loss was significantly less in the UBD-TLIF group (155.69 ± 93.41 mL) compared to the MIS-TLIF group (230.96 ± 102.18 mL, P < 0.001). Additionally, the UBD-TLIF group experienced a shorter length of hospital stay (7.02 ± 1.75 days) compared to the MIS-TLIF group (8.38 ± 1.33 days, P < 0.001). According to the Macnab criteria, global satisfaction rates were 96.1% for the UBD-TLIF group and 94.2% for the MIS-TLIF group.
Discussion
This study revealed that UBD-TLIF effectively minimizes paraspinal muscle damage, including reducing the percentage of FI in the multifidus and erector spinae muscles compared to MIS-TLIF. Although no significant differences in clinical outcomes (VAS and ODI scores) were observed between the two groups one year postoperatively, the UBD-TLIF group exhibited faster recovery, evidenced by lower VAS scores for back pain on postoperative day 3 and a shorter length of hospital stay. These findings suggest that UBD-TLIF is capable of reducing paravertebral muscle damage while achieving similar clinical outcomes to MIS-TLIF.
The multifidus muscle, located deep within the lumbar spine, plays a crucial role in facilitating sagittal plane rotation, while the erector spinae, as the most extensive and robust dorsal musculature, governs spinal extension and orientation.9,13–15 These muscle groups are integral to the mobility and stability of the lumbar spine. Consequently, any impairment can significantly affect lumbar segment stability, potentially leading to lower back pain.14,16 Several factors can contribute to iatrogenic injury to the lower back paraspinal muscles during lumbar interbody fusion surgery, including prolonged traction and multiple or long incisions at the surgical site, which may cause local ischemia and denervation, leading to postoperative muscle atrophy, pain, and an increased risk of failed back surgery syndrome.8,17–19 Kim et al have shown that mini-open fusion surgery significantly reduces muscle injury and systemic inflammation, with MRI studies supporting that minimally invasive surgery causes less muscle damage and reduces FI.17 Magnetic resonance imaging study also supported that minimal invasive surgery causes less muscle damage and followed less muscle FI.9,19 Besides, Andrew J et al found that the percentage of FI but not the CSA was closely associated with low back pain. In our previous research, we documented reduced levels of inflammatory markers such as C-reactive protein (CRP), neutrophils, interleukin-6 (IL-6), and creatine phosphokinase (CPK) in the UBD-TLIF cohort.5 The current study further supports the finding that UBD-TLIF leads to diminished changes in muscle FI, suggesting that this technique is more effective in preserving muscle integrity during surgical interventions.
Despite the longer operative time observed in the UBD-TLIF group, this technique demonstrated significant advantages in terms of reduced blood loss, lower postoperative back pain VAS scores, and lesser changes in muscle FI. These benefits may be attributed to the innovative design of the UBD endoscopic system, which features two channels arranged in a “V” shape that expands the surgical field of view and enhances operability without altering conventional endoscopic practices. Both channels of the UBD system can function as working channels and are compatible with both air and water media, allowing the surgeon to perform precise surgery and stop bleeding in a clear, magnified view, and with specially designed surgical instruments such as ring drills, reamers, and spatulas, minimizing soft tissue damage and making the surgery more efficient. The longer duration of UBD-TLIF surgeries observed in this study may be due to the novelty of the technique.4 While MIS-TLIF techniques have been well-mastered by the surgeons involved, the UBD-TLIF technique is still in its learning and adaptation stages. Preliminary studies indicate that UBD-TLIF’s complication rates are not significantly different from those associated with MIS-TLIF, suggesting that UBD-TLIF maintains the conventional endoscopic operational practices, ensuring good surgical safety.3–5
Moreover, our study demonstrated that MRI is highly reproducible for measuring the infiltration rate of the multifidus and erector spinae muscles. Previous studies have used MRI or computed tomography (CT) to assess the incidence of paravertebral muscle atrophy and degeneration following various surgical approaches.7,20,21 Compared to CT, MRI provides a safer alternative for both quantitative and qualitative muscle evaluation, as it does not expose patients to ionizing radiation. T2-weighted axial images were selected for their ability to distinguish between muscle contractile components and adipose tissue, offering a clearer assessment of muscle FI.13 However, this method has certain limitations, including the need for manual polygon placement around muscle boundaries, which can be challenging in cases of severe muscle atrophy and FI.22 To address this, patients with severe baseline muscle atrophy and FI were excluded from our study. Furthermore, T2-weighted axial images used for evaluating postoperative paravertebral muscles can be affected by metal implants, potentially reducing the reliability of CSA measurements.23 In this study, MRI sections with minimal metal artifact interference were selected at the fusion segment disc level for postoperative images, and preoperative MR images were referenced accordingly to enhance the reliability of comparisons. All measurements were conducted using ImageJ software, which facilitates area and pixel value calculations for user-defined regions and intensity thresholds,14 supporting various image file formats, including DICOM files, used in this study.
This study has several limitations. First, the sample size is relatively small, primarily due to the novelty of the UBD-TLIF technique, with cases still accumulating. Second, the inconsistency in surgeons’ proficiency with the two surgical methods may introduce bias into the study conclusions. For example, the operative time for UBD-TLIF might decrease as surgeons become more adept with the new technique.
Conclusion
UBD-TLIF achieves clinical outcomes comparable to MIS-TLIF. Although there was no statistically significant difference in ODI scores between the two groups one year postoperatively, radiological assessments indicate less change in FI for the UBD-TLIF group. Additionally, UBD-TLIF is associated with faster short-term recovery, as evidenced by lower VAS scores for back pain on postoperative day 3 and shorter hospital stays, further suggesting that UBD-TLIF results in less muscle trauma. Furthermore, the use of T2-weighted MRI and ImageJ software for measuring FI rates has been demonstrated to be a reliable method.
Data Sharing Statement
The data will not be publicly shared but can be accessed by contacting the corresponding author for permission.
Ethics Approval and Consent to Participate
This retrospective study adhered to the Declaration of Helsinki, written informed consent was obtained from each patient. And, it was approved by the Institutional Review Boards of Shanghai Tenth People’s Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by National Natural Science Fundation of China (No.82001927), Science and Technology Commission of Shanghai Municipality, (No. 22S31900100), and The Medical Discipline Construction Program of Shanghai Pudong New Area Health Commission (the Key Disciplines Program) (PWZxk2022-21).
Disclosure
The authors have declared that no competing interest exists in this work.
References
1. May AT, Farah K, Meyer M, Fuentes S. How I do it: mini invasive transforaminal lumbar interbody fusion. Acta Neurochir (Wien). 2021;163(1):289–293. doi:10.1007/s00701-020-04388-5
2. Holly LT, Schwender JD, Rouben DP, Foley KT. Minimally invasive transforaminal lumbar interbody fusion: indications, technique, and complications. Neurosurg Focus. 2006;20(3):E6. doi:10.3171/foc.2006.20.3.7
3. Gong H, Fan Y, Zhao Y, et al. Minimally invasive transforaminal lumbar interbody fusion by a novel two-medium compatible bichannel endoscopy system, technique note and preliminary clinical results. Eur Spine J. 2023;32(8):2845–2852. doi:10.1007/s00586-023-07746-w
4. Tian MH, Wu XB, Zhao YC, et al. Original Uniportal Bichannel and Dual-Media Spinal Endoscopy System Assists Elderly Patients with Thoracolumbar Kyphosis Associated with Osteoporosis: technical Note and Preliminary Clinical Results. World Neurosurg. 2025;196:123785. doi:10.1016/j.wneu.2025.123785
5. Wu X, Liu W, Xiao X, et al. Comparison of the clinical outcomes of VBE-TLIF versus MIS-TLIF for single-level degenerative lumbar diseases. Eur Spine J. 2024;33(3):1120–1128. doi:10.1007/s00586-023-08096-3
6. Zhou Z, Ni H, Hu S, et al. Original Designed Uniportal-Bichannel Spinal Endoscopic System (UBiSES) for Foraminoplasty in Percutaneous Endoscopic Transforaminal Discectomy. Orthop Surg. 2021;13(7):1987–1999. doi:10.1111/os.13050
7. Han G, Wu H, Dai J, et al. Does paraspinal muscle morphometry predict functional status and re-operation after lumbar spinal surgery? A systematic review and meta-analysis. Eur Radiol. 2023;33(8):5269–5281. doi:10.1007/s00330-023-09548-6
8. Schoennagel L, Guven AE, Camino-Willhuber G, et al. Examining the Role of Paraspinal Musculature in Postoperative Disability After Lumbar Fusion Surgery for Degenerative Spondylolisthesis. Spine. 2024;49(14):997–1003. doi:10.1097/BRS.0000000000004840
9. Fan S, Hu Z, Zhao F, Zhao X, Huang Y, Fang X. Multifidus muscle changes and clinical effects of one-level posterior lumbar interbody fusion: minimally invasive procedure versus conventional open approach. Eur Spine J. 2010;19(2):316–324. doi:10.1007/s00586-009-1191-6
10. Macnab I. Chapter 14. Pain and disability in degenerative disc disease. Clin Neurosurg. 1973;20:193–196. doi:10.1093/neurosurgery/20.CN_suppl_1.193
11. Newell E, Chorney H, Tiegs-Heiden CA, Benson JC, Ouellet J, Driscoll M. Augmentation of musculoskeletal soft tissue morphology within low back pain patients may suggest the presence of physiological stress shielding: an in vivo study. J Biomech. 2024;162:111894. doi:10.1016/j.jbiomech.2023.111894
12. Fortin M, Battie MC. Quantitative paraspinal muscle measurements: inter-software reliability and agreement using OsiriX and ImageJ. Phys Ther. 2012;92(6):853–864. doi:10.2522/ptj.20110380
13. Masi S, Rye M, Roussac A, et al. Comparison of paraspinal muscle composition measurements using IDEAL fat-water and T2-weighted MR images. BMC Med Imaging. 2023;23(1):48. doi:10.1186/s12880-023-00992-w
14. Liu S, Schmidt H, Ziegeler K, et al. Inter-software and inter-threshold reliability of quantitative paraspinal muscle segmentation. Eur Spine J. 2024;33(2):369–378. doi:10.1007/s00586-023-08050-3
15. Fu C, Chen W, Lu M, Cheng C, Niu C. Comparison of paraspinal muscle degeneration and decompression effect between conventional open and minimal invasive approaches for posterior lumbar spine surgery. Sci Rep. 2020;10(1):14635. doi:10.1038/s41598-020-71515-8
16. Chen M, Zhang P, Lai J, et al. A correlation study of preoperative lumbar paraspinal muscle quality and L5-S1 lumbar foraminal stenosis degeneration after L4-5 TLIF. J Orthop Surg Res. 2023;18(1):731. doi:10.1186/s13018-023-04196-4
17. Kim K, Lee S, Suk K, Bae S. The quantitative analysis of tissue injury markers after mini-open lumbar fusion. Spine. 2006;31(6):712–716. doi:10.1097/01.brs.0000202533.05906.ea
18. Hu Z, Fang X, Zhou Z, Wang J, Zhao F, Fan S. Effect and possible mechanism of muscle-splitting approach on multifidus muscle injury and atrophy after posterior lumbar spine surgery. J Bone Joint Surg Am. 2013;95(24):e191–e192. doi:10.2106/JBJS.L.01607
19. Min S, Kim M, Seo J, Lee J, Lee D. The quantitative analysis of back muscle degeneration after posterior lumbar fusion: comparison of minimally invasive and conventional open surgery. Asian Spine J. 2009;3(2):89–95. doi:10.4184/asj.2009.3.2.89
20. Prasetyo M, Nindita N, Murdana IN, Prihartono J, Setiawan SI. Computed tomography evaluation of fat infiltration ratio of the multifidus muscle in chronic low back pain patients. Eur J Radiol Open. 2020;7:100293. doi:10.1016/j.ejro.2020.100293
21. Teichtahl AJ, Urquhart DM, Wang Y, et al. Fat infiltration of paraspinal muscles is associated with low back pain, disability, and structural abnormalities in community-based adults. Spine J. 2015;15(7):1593–1601. doi:10.1016/j.spinee.2015.03.039
22. Marunowski K, Swieton D, Bzyl W, et al. Reference values for MRI-derived psoas and paraspinal muscles and macroscopic fat infiltrations in paraspinal muscles in children. J Cachexia, Sarcopenia Muscle. 2022;13(5):2515–2524. doi:10.1002/jcsm.13049
23. Pai SA, Zhang H, Street J, Wilson DR, Brown SHM, Oxland TR. Preliminary investigation of spinal level and postural effects on thoracic muscle morphology with upright open MRI. JOR Spine. 2021;4(1):2.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Radiological Changes of Paraspinal Muscles: A Comparative Study of Patients with Isthmic Spondylolisthesis, Patients with Degenerative Lumbar Spondylolisthesis, and Healthy Subjects
Li C, Wang L, Wang Z, Li D, Ibrahim Y, Tian Y, Yuan S, Liu X
Journal of Pain Research 2022, 15:3563-3573
Published Date: 11 November 2022