Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Combined Auricular Acupoint Pressing and Intradermal Acupuncture for Insomnia and Glycemic Control in Elderly Patients with Type 2 Diabetes: A Retrospective Study
Received 9 June 2025
Accepted for publication 21 October 2025
Published 22 November 2025 Volume 2025:18 Pages 7647—7657
DOI https://doi.org/10.2147/JMDH.S538807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Ling Zhang,1 Yuanyuan Liu2
1Department of Traditional Chinese Medicine, First People’s Hospital, Hefei City, Anhui Province, 230001, People’s Republic of China; 2Department of Endocrinology, First People’s Hospital, Hefei City, Anhui Province, 230001, People’s Republic of China
Correspondence: Yuanyuan Liu, Department of Traditional Chinese Medicine, First People’s Hospital, No. 390 Huaihe Road, Luyang District, Hefei, Anhui, People’s Republic of China, Email [email protected]
Objective: To investigate the clinical efficacy of combined auricular acupoint pressing and intradermal acupuncture in elderly patients with type 2 diabetes mellitus and insomnia.
Methods: A retrospective study selected 122 such patients, divided into a control group (60 patients with basic diabetes treatment) and an observation group (62 patients with basic treatment plus auricular acupoint pressing and intradermal acupuncture). Pittsburgh Sleep Quality Index (PSQI), quality of life assessment, blood glucose, glycated hemoglobin, and serum indicators including 5-hydroxytryptamine (5-HT), brain-derived neurotrophic factor (BDNF), and norepinephrine (NE) were measured. Statistical analysis was done using SPSS 26.0.
Results: In the control group, pre - treatment blood glucose of 7.84± 1.89 mmol/L decreased to 7.78± 1.76 mmol/L post - treatment (P< 0.05). PSQI score dropped from 11.69± 2.74 to 8.07± 2.86 (P< 0.05), with a 75.00% effective rate. In the observation group (n=62), blood glucose decreased from 8.43± 2.17 to 6.96± 1.68 mmol/L (P< 0.05). PSQI score declined from 11.63± 2.16 to 6.38± 2.32 (P< 0.05), and the effective rate was 90.32% (P< 0.05 vs control group).
Conclusion: The combined treatment of auricular acupoint pressing and intradermal acupuncture has potential in treating these patients. But due to the retrospective nature of the study, well - designed RCTs and in - depth mechanistic studies are needed to confirm its efficacy and clarify the mechanisms.
Keywords: type 2 diabetes, auricular acupoint pressing, intradermal acupuncture, insomnia, elderly patients
Introduction
In recent years, with the rapid economic development in China, the prevalence of high - fat and high - carbohydrate diets has increased. Currently, China has the largest number of diabetes patients globally.1 Type 2 diabetes is a escalating global public health issue. Cases are projected to surge from 536.6 million adults in 2021 to 783.2 million by 2045,2 fueled by economic development, lifestyle shifts, and aging. In the elderly population, due to the slowdown of basal metabolism, the decline of physiological functions, and changes in sleep structure, the overall sleep quality is relatively poor. Sleep disorders are one of the common syndromes among elderly diabetes patients, with an incidence rate ranging from 40% to 70%.3 The control of diabetes can easily lead to the generation of negative emotions, which in turn affect sleep quality. The combination of diabetes and insomnia seriously impacts people’s normal lives and work, imposing a continuous and significant economic and social burden.4 Thus, it is crucial to strengthen the attention and intervention regarding the sleep of elderly diabetes patients with insomnia.
Insomnia is a prevalent sleep disorder in elderly patients with type 2 diabetes mellitus, related to multiple factors. The aging process reduces the production of 5 - hydroxytryptamine (5 - HT or serotonin), crucial for sleep regulation. Diabetes - related complications can cause pain and disrupt sleep.5 Brain - derived neurotrophic factor (BDNF) levels may be disrupted in insomnia, impairing neuron function in sleep regulation.6 Noradrenaline (NE) imbalance, due to stress and sleep deprivation, can lead to increased arousal and abnormal stress responses, affecting sleep quality.7 Thus, the imbalance of 5 - HT, BDNF, and NE levels is closely linked to insomnia in this patient group, and understanding this is key for treatment development.
The current treatment for diabetes - related insomnia in the elderly mainly includes Western medicine and traditional Chinese medicine. Western medicine often uses sedative - hypnotic drugs, but long - term use may lead to drug dependence, withdrawal reactions, and side effects such as drowsiness, dizziness, and memory impairment.8 Traditional Chinese medicine, on the other hand, offers alternative approaches. Auricular acupoint pressing and intradermal acupuncture are two common traditional Chinese medicine techniques that have shown potential in treating insomnia.9
Auricular acupoint pressing is based on the theory that the ear is connected to the body’s internal organs and meridians. By applying pressure to specific auricular acupoints, it can regulate the functions of the corresponding organs and meridians, thereby improving sleep quality.10 Previous studies suggest that stimulation of auricular acupoints such as Shenmen and Endocrine may help improve sleep quality by modulating neuroendocrine activity and calming the nervous system.11,12 Intradermal acupuncture, a method of inserting needles into the skin for a relatively long - time, can also stimulate specific acupoints continuously.13 It has been reported to have a positive impact on sleep by regulating the body’s qi and blood circulation and adjusting the function of the nervous system.14
Building upon the individual benefits of these therapies, their combination offers a synergistic approach grounded in complementary mechanisms. From a TCM perspective, auricular therapy primarily regulates zang-fu organs and calms the mind through meridian connections,15 while intradermal acupuncture facilitates qi and blood circulation,16 resolves stagnation, and harmonizes yin and yang. Energetically, the integrated application enhances the regulation of common patterns underlying diabetic insomnia, such as heart-kidney imbalance and liver qi stagnation. From a biomedical standpoint, auricular stimulation is thought to modulate autonomic nervous system activity and promote serotonin release,17 whereas intradermal acupuncture may contribute to BDNF expression and reduce sympathetic dominance.18 For instance, TCM-defined liver qi stagnation—often presenting as irritability and sleep disruption—may correspond to dysregulated HPA axis function and elevated cortisol levels,19 while heart-kidney imbalance may reflect broader neuroendocrine disturbances.20 Together, these therapies work synergistically through both physiological and energetic pathways to restore neuroendocrine balance and improve sleep outcomes.
Although prior studies have explored these interventions separately for sleep or metabolic disorders, their combined effect on elderly patients with type 2 diabetes mellitus and comorbid insomnia remains under-investigated. Given the limitations of pharmacological treatments in this age group and the high prevalence of sleep disturbances among diabetic individuals, evaluating this integrative, non-pharmacologic approach could provide a safer and more effective alternative. Therefore, this study aimed to assess the clinical efficacy of combining auricular acupoint pressing with intradermal acupuncture in improving glycemic control, sleep quality, and quality of life.
Method
Patient Data
In this retrospective study, 122 elderly patients with type 2 diabetes mellitus complicated by insomnia were selected from those who sought treatment at the Endocrinology Department and Traditional Chinese Medicine Department of First People’s Hospital of Hefei between January 2024 and December 2024. These patients were allocated into two groups according to different intervention methods: the control group consisted of 60 patients, and the observation group included 62 patients. A post-hoc power analysis, based on an assumed medium effect size (d≈0.50) for the primary outcome (PSQI score reduction), indicated that the sample of 122 patients (60 vs 62) provided >80% power at α=0.05 to detect between-group differences of approximately 0.45–0.50 standard deviations.21 This study was approved by the Medical Ethics Committee of the First People’s Hospital of Hefei, Anhui Province (No. 20250217). The Committee waived the requirement for obtaining patient consent to review medical records, as the study was retrospective in design and used de-identified clinical data that posed no risk of identifying individual patients. All methods were carried out in accordance with the Declaration of Helsinki, and strict measures were implemented to ensure the confidentiality of patient data throughout the research process.
Patients were assigned to groups according to the treatments they received in routine clinical practice, with allocation guided by both patient preference and clinician judgment. All interventions were delivered by nationally certified TCM practitioners, each with over 5 years of acupuncture experience and specific protocol training to ensure consistency. Laboratory assays were performed in the hospital’s central laboratory following standardized protocols and routine quality control procedures. Clinical data were retrieved from the electronic medical record system and independently cross-verified by two investigators. Missing information was rare (<0.2%) and addressed according to predefined criteria.
Diagnostic Criteria
The diagnostic criteria for diabetes adhered to the 1999 World Health Organization (WHO) standards.22 Firstly, for patients presenting with typical symptoms such as polyuria, polydipsia, polyphagia, and unexplained weight loss, a fasting blood glucose level of ≥7.0 mmol/L or a post - prandial blood glucose level of ≥11.1 mmol/L was diagnostic of diabetes. Secondly, in the absence of these typical symptoms, if a patient’s fasting blood glucose was ≥7.0 mmol/L or post - prandial blood glucose was ≥11.1 mmol/L, the test should be repeated. A confirmed diagnosis could be made if the repeated results still met the above - mentioned values. Thirdly, when typical symptoms were lacking, a 2 - hour oral glucose tolerance test with a blood glucose level of ≥11.1 mmol/L was also considered diagnostic of diabetes.
The diagnostic criteria for insomnia were based on the “Diagnostic and Therapeutic Criteria for TCM Diseases and Syndromes” in the Chinese medicine industry standard of the People’s Republic of China.23 For mild cases, patients experienced difficulty falling asleep or woke up easily and had trouble falling back asleep. Severe cases were characterized by complete sleeplessness throughout the night. Insomnia was usually accompanied by symptoms such as headache, dizziness, palpitations, forgetfulness, fatigue, restlessness, and excessive dreaming. After comprehensive laboratory tests of various systems, no other organic diseases that could interfere with sleep were detected.
Inclusion and Exclusion Criteria
Inclusion Criteria
- Patients aged 60 years or older.
- Met the diagnostic criteria for type 2 diabetes mellitus (WHO 1999) and insomnia (Chinese medicine industry standard).
- Had stable diet, exercise, lifestyle, and hypoglycemic regimens, with fasting blood glucose coefficient of variation < 16% in the 3 - day pre - treatment period and on the treatment day.
- Aged 20–80 years, regardless of gender.
- No severe liver/kidney damage, cardiovascular/cerebrovascular diseases, or acute complications like diabetic ketoacidosis.
- Insomnia lasting 6 months or more.
- Did not take any insomnia medications in the 2 weeks before the visit.
- Pittsburgh Sleep Quality Index (PSQI) total score ≤ 15 points.
Exclusion Criteria
- Excessive blood glucose fluctuations.
- Severe liver/kidney damage, cardiovascular/cerebrovascular diseases, or ketoacidosis.
- Obstructive sleep apnea syndrome.
- Outer ear ulcers, eczema, or breakages.
- Pregnant or lactating women.
- Severe complications in respiratory, circulatory, digestive, urinary, or hematological systems, or severe mental/psychological disorders.
Intervention Information
The control group received basic treatment, which included diabetes education, a low - sugar diet, exercise guidance, and administration of oral hypoglycemic medications or insulin injections. For oral hypoglycemic medications, the selection was based on the patients’ specific conditions, such as metformin for improving insulin sensitivity in patients with insulin resistance, or sulfonylureas for enhancing insulin secretion in those with relatively insufficient insulin production. Insulin injections were adjusted according to the patients’ blood glucose levels, with short - acting insulin used to control post - meal blood glucose spikes and long - acting insulin to maintain basal blood glucose levels.
The observation group, on the basis of the basic treatment, underwent auricular acupoint pressing combined with intradermal acupuncture.
Auricular Acupoint Pressing: On one side of the ear, acupoints including Chuiqian, Zhen, Yuanzhong, Neifenmi (Endocrine), Qiunao (Thalamus), Yidan (Pancreas - Gallbladder), Gan (Liver), Shen (Kidney), Shenmen, and Erzhong were selected. The operator gently massaged the patient’s bilateral ears from bottom to top and from inside to outside until they became warm and red. After that, the auricles were disinfected with 75% ethanol - soaked cotton balls. Then, a probe was used to find sensitive points within the corresponding auricular acupoint areas of both ears. Adhesive tapes with Vaccaria seeds were placed on these sensitive points and firmly adhered to the acupoints. The patient used the index finger and thumb to apply pressure on the front and back of the auricle to stimulate the area where the seeds were placed. The pressure was gradually increased from light to heavy, and the optimal effect was achieved when the patient felt local numbness, soreness, distension, or a slight pain, along with a warm sensation in the auricle. The patient was instructed to press the acupoints daily, with the intensity of pressure being appropriate when a distending pain was felt and the auricle became warm. Each acupoint was pressed for 30 seconds, 5 times a day, for 3 consecutive days. The auricular stickers were replaced every 3 days, and 5 such cycles constituted one treatment course. The treatment lasted for 5 consecutive courses.
Intradermal Acupuncture Therapy: On the other side of the ear, acupoints such as Zhen, Shenmen, Xin (Heart), Pizixia (Subcortex), Sanjiao, Neifenmi (Endocrine), Yuanzhong, Tangniaobingdian (Diabetes Point), and Erzhong were selected. The skin at the selected acupoint areas was routinely disinfected with 1% Anerdian disinfectant. A acupuncture needle was held and inserted into the skin at an angle of less than 15° along the intradermal layer in the corresponding acupoint area. The needle body was kept within the skin, and it was fixed with adhesive tape for 4 hours. This acupuncture was performed once every 3 days, and 5 times made up one treatment course. The treatment was continuously carried out for 5 courses.
Observation Indicators
- Pittsburgh Sleep Quality Index (PSQI):24 The PSQI is composed of 24 items across 7 dimensions, namely sleep quality, sleep latency, sleep duration, etc. The total score ranges from 0 to 21 points, and a lower score indicates better sleep quality, showing a negative correlation between the score and sleep quality.
- Quality of Life Assessment: The World Health Organization Quality of Life - Brief Version (WHOQOL - BREF)25 was employed. This scale encompasses 4 domains: physical health, psychological state, environment, and social relationships, with a total of 26 items. The overall score ranges from 0 to 100 points, and a higher score is positively associated with a better quality of life.
- Fasting Blood Glucose and Glycated Hemoglobin: These two indicators were used to evaluate the patients’ recent blood glucose levels.
- Serum Indicators Before and After Treatment in Both Groups: Venous blood samples (5 mL) were collected from the patients’ fasting outer elbow veins at 8:00 am on the day before treatment and the day after 5 treatment courses. The samples were centrifuged at 3000 revolutions per minute (r/min) with a radius of 15 cm for 10 minutes. Then, the enzyme - linked immunosorbent assay (ELISA) was utilized to measure the levels of 5 - hydroxytryptamine (5 - HT), brain - derived neurotrophic factor (BDNF), and norepinephrine (NE).
- Effective Rate: The reduction rate was calculated based on the PSQI scores. The formula for calculating the curative effect reduction rate is: Curative Effect Reduction Rate = [(Total Score Before Treatment - Total Score After Treatment) / Total Score Before Treatment] × 100%. Clinical cure was defined as a reduction rate of ≥ 75%; marked effect was a reduction rate of ≥ 50% and < 75%; effective was a reduction rate of ≥ 25% and < 50%; and ineffective was a reduction rate of < 25%.26
Statistical Analysis
Statistical analysis was carried out using SPSS 26.0 software. In this study, measurement data were assessed for normality using the Shapiro–Wilk test and for homogeneity of variance with Levene’s test. Data that conformed to a normal distribution and had homogeneous variances were expressed as mean ± standard deviation. For between - group comparisons, independent - sample t - tests were utilized, and paired - sample t - tests were employed for within - group comparisons. Enumeration data were presented as frequencies and percentages, and the chi - square (χ2) test was applied for between - group comparisons. A significance level of P<0.05 was set to indicate statistically significant differences.
Result
General Information of Patients in the Two Groups
This study involved 60 patients in the control group and 62 in the observation group (Table 1). When comparing their baseline characteristics, no significant differences were found. The P - values for gender, age, disease duration, presence of peripheral neuropathy, hypertension, coronary heart disease, diabetic nephropathy, retinopathy, BMI, and basic hypoglycemic drug use were 0.674, 0.357, 0.178, 0.225, 0.563, 0.866, 0.445, 0.628, 0.240, and 0.725 respectively. Since all these values were greater than 0.05, the two groups were comparable at the start of the study.
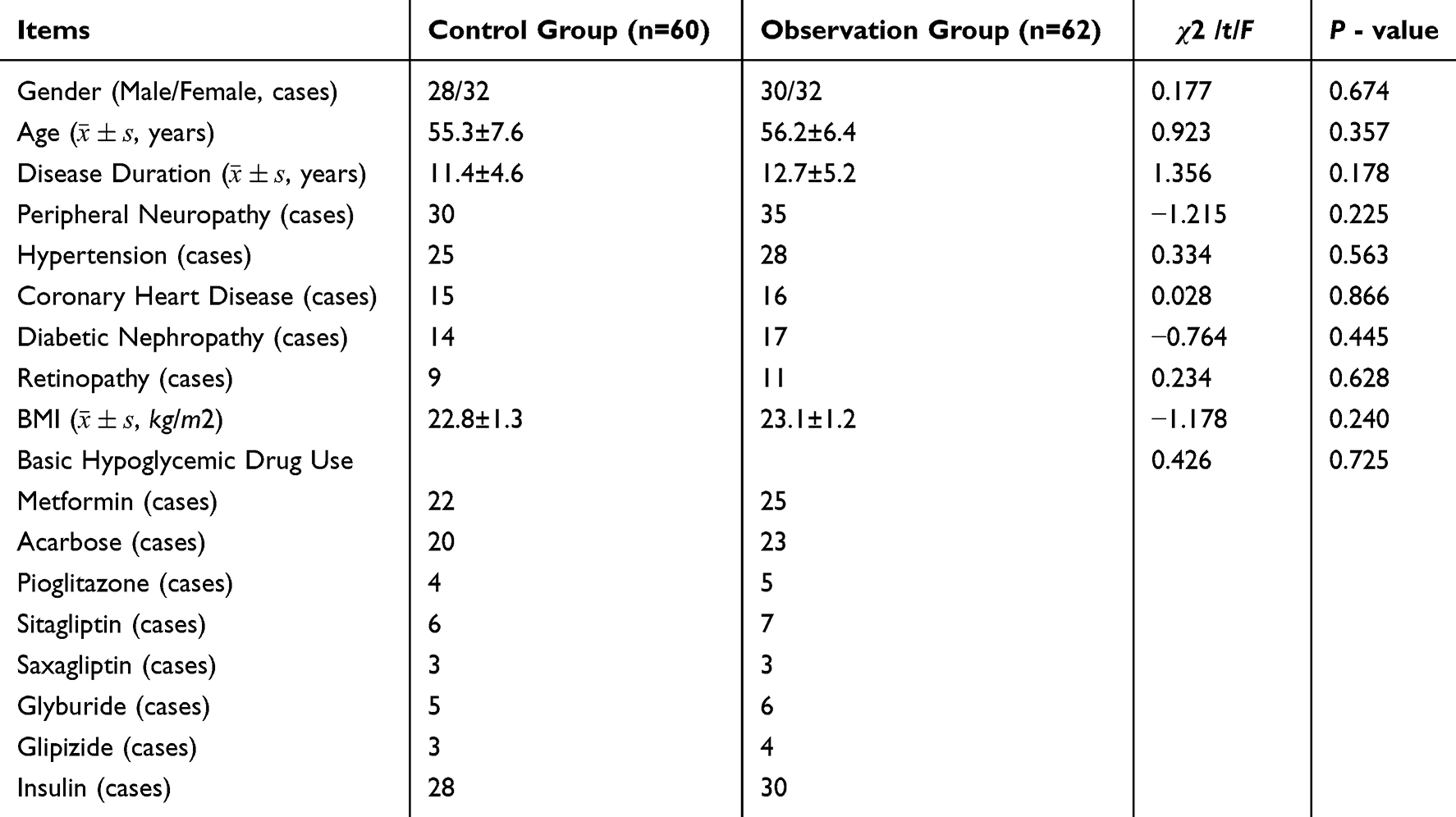 |
Table 1 Baseline Information of the Two Groups |
Blood Glucose Control in the Two Groups
We evaluated blood glucose control in 60 control - group and 62 observation - group patients (Table 2).
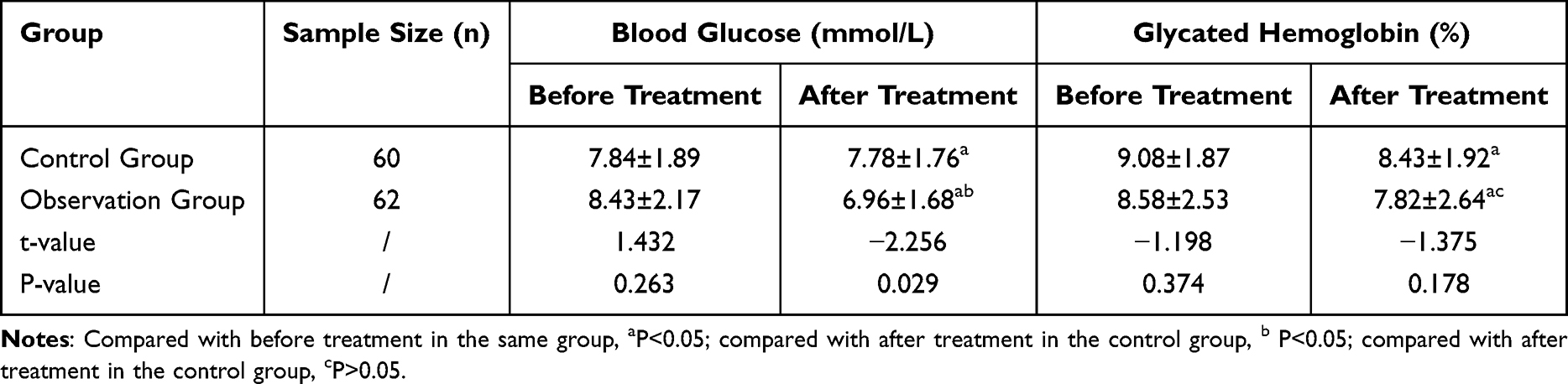 |
Table 2 Results of Blood Glucose Control in the Two Groups ( |

For blood glucose, the control group’s pre - treatment mean was 7.84±1.89 mmol/L, dropping to 7.78±1.76 mmol/L post - treatment (P<0.05). The observation group started at 8.43±2.17 mmol/L and decreased to 6.96±1.68 mmol/L (P<0.05 compared to pre - treatment and P<0.05 compared to the control group post - treatment). The pre - treatment P value between groups was 0.263, showing no baseline difference.
For glycated hemoglobin, the control group had 9.08±1.87% pre - treatment, reducing to 8.43±1.92% post - treatment (P<0.05). The observation group started at 8.58±2.53% and decreased to 7.82±2.64% (P<0.05 compared to pre - treatment). The post - treatment P value between groups was 0.178, with no significant difference, and the pre - treatment P value was 0.374, indicating no baseline difference.
Sleep Improvement in the Two Groups
Sleep improvement was examined in 60 patients in the control group and 62 in the observation group (Table 3).
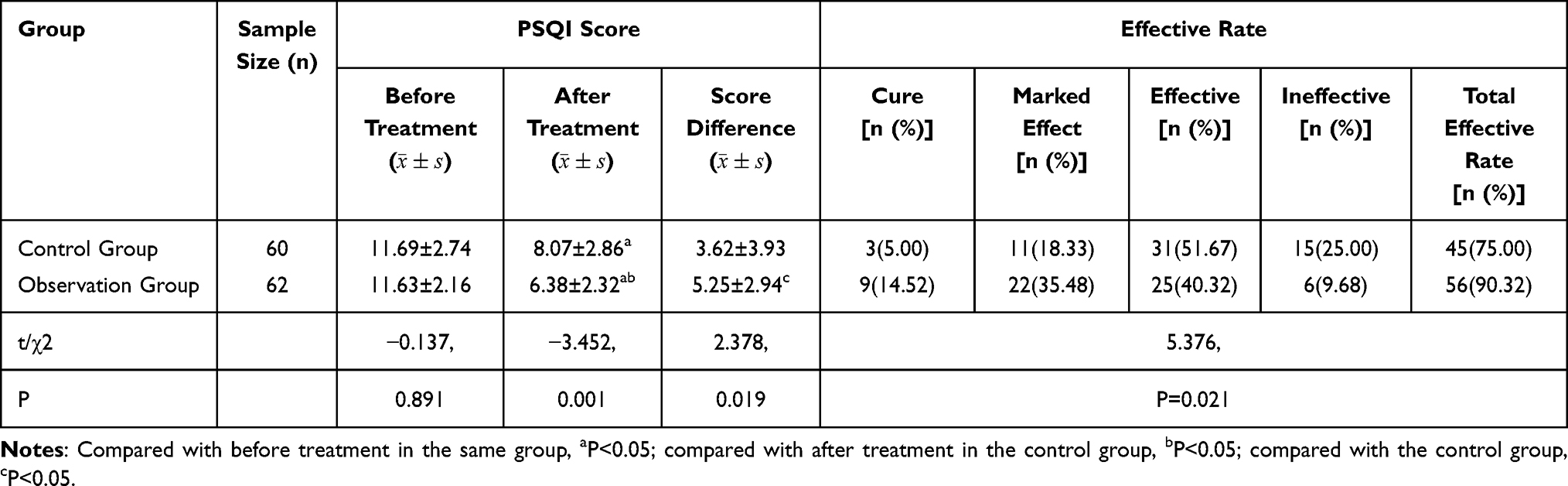 |
Table 3 Results of PSQI Scores and Efficacy Evaluation of Patients in the Two Groups |
For PSQI scores, in the control group, the mean score before treatment was 11.69 ± 2.74, which decreased to 8.07 ± 2.86 after treatment (P < 0.05 compared to before treatment). In the observation group, the initial mean score was 11.63 ± 2.16, dropping to 6.38 ± 2.32 after treatment (P < 0.05 compared to before treatment and P < 0.05 compared to the control group after treatment). The P - value for the pre - treatment comparison between groups was 0.891, indicating no significant difference at baseline. The difference in score change between the two groups also showed significance with a P - value of 0.019.
Regarding the effective rate, the total effective rate in the control group was 75.00% (45 out of 60 patients), while in the observation group it was 90.32% (56 out of 62 patients). The difference in total effective rates between the two groups was significant with a P - value of 0.021. The observation group had a higher proportion of patients with cure and marked effect compared to the control group.
Comparison of Serum Indicators Between the Two Groups Before and After Treatment
Serum indicators were compared in 60 control - group and 62 observation - group patients before and after treatment (Table 4).
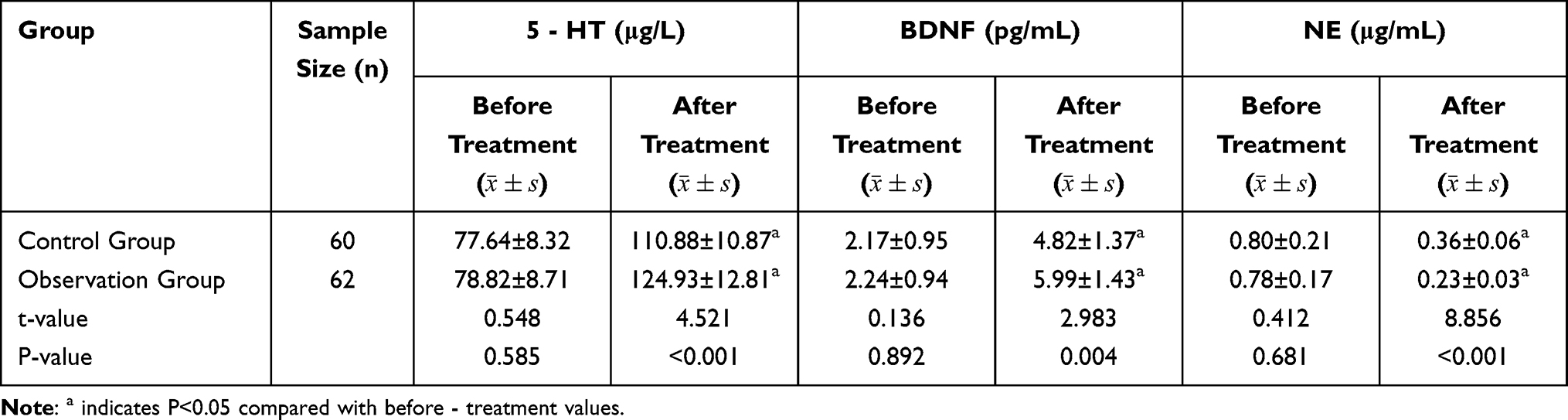 |
Table 4 Results of Two Groups of Serum Indicators |
For 5 - HT, both groups had significant post - treatment increases (P < 0.05). The pre - treatment levels were similar (P = 0.585), but post - treatment, the observation group had a significantly higher level (P < 0.001). Regarding BDNF, levels increased significantly after treatment in both groups (P < 0.05). There was no pre - treatment difference (P = 0.892), yet the post - treatment value was higher in the observation group (P = 0.004). For NE, both groups showed significant post - treatment decreases (P < 0.05). Pre - treatment levels were comparable (P = 0.681), and post - treatment, the observation group had a significantly lower level (P < 0.001).
Results of Quality of Life Assessment in the Two Groups
Quality of life, as measured by the WHOQOL - BREF score, was evaluated in 60 patients of the control group and 62 of the observation group (Table 5).
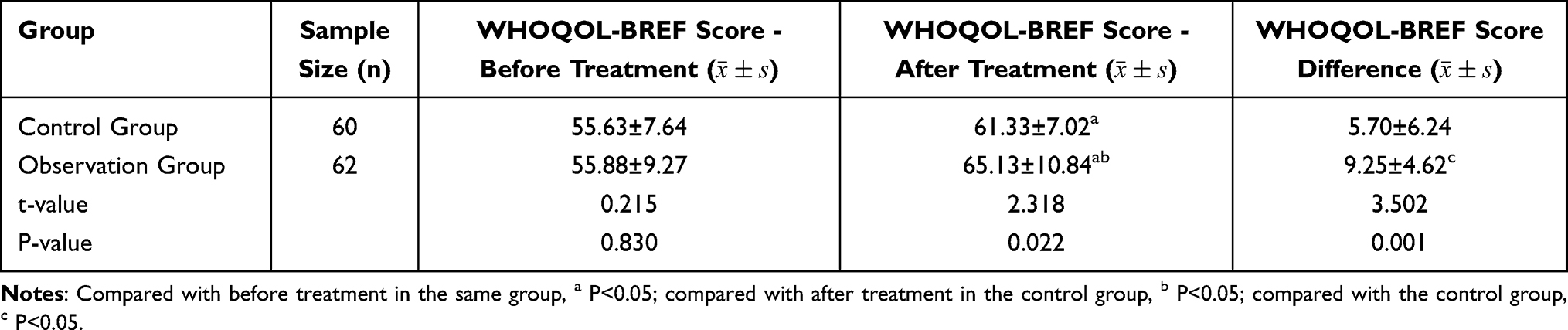 |
Table 5 Comparison of WHOQOL-BREF Score Between the Two Groups |
Before treatment, the mean WHOQOL - BREF scores in the control group were 55.63 ± 7.64 and in the observation group were 55.88 ± 9.27, with a P - value of 0.830, indicating no significant difference between the two groups at baseline. After treatment, the control group’s mean score increased to 61.33 ± 7.02 (P < 0.05 compared to before treatment), while the observation group’s mean score rose to 65.13 ± 10.84 (P < 0.05 compared to before treatment and P < 0.05 compared to the control group after treatment). The P - value for the post - treatment comparison between the two groups was 0.022. The difference in score changes between the two groups was also significant, with a P - value of 0.001, suggesting that the observation group experienced a more substantial improvement in quality of life compared to the control group.
Discussion
Insomnia, a prevalent sleep disorder, is characterized by transient or persistent difficulty in falling asleep or maintaining sleep. In elderly patients with type 2 diabetes mellitus, the co - morbidity of insomnia and diabetes exacerbates the complexity of treatment. This study explored the clinical efficacy of auricular acupoint pressing combined with intradermal acupuncture in this patient population, and the results offer profound insights.
Diabetes and insomnia are intricately linked. The circadian sleep - wake rhythm is crucial for glucose metabolism. Disruptions in this rhythm due to insomnia can lead to abnormal blood glucose regulation.27 From a traditional Chinese medicine (TCM) perspective, insomnia is often classified as “bu mei” (non - sleep), with the common pattern of liver - depression transforming into fire. The liver, in TCM theory, stores blood and houses the soul, and its proper function is crucial for emotional well - being. When the liver fails to regulate qi smoothly due to emotional stress, pathogenic invasion, or sudden shock, qi stagnation occurs, which over time transforms into fire and disturbs the mind, leading to insomnia.28 Auricular acupoint pressing and intradermal acupuncture aim to soothe the liver, regulate qi, and calm the mind, thereby restoring the body’s yin - yang balance. Research indicates that individuals with sleep - disordered breathing have a 1.33 - fold higher risk of developing diabetes compared to those without. The underlying mechanisms involve oxidative stress, hormonal imbalances, and inflammatory responses. In the elderly, the high prevalence of diabetes - related insomnia highlights the urgency of developing effective treatment strategies.29
The results of this study reveal significant improvements in blood glucose levels in both the control and observation groups post - treatment. However, the observation group, which received the combined treatment of auricular acupoint pressing and intradermal acupuncture, demonstrated a more substantial reduction. Auricular acupoint pressing, grounded in traditional Chinese medicine (TCM) meridian theory, uses Vaccaria seeds to stimulate auricular acupoints. This stimulation may modulate the body’s internal organs and qi - blood circulation, thereby influencing glucose metabolism. Intradermal acupuncture, with its non - invasive nature (the needle only penetrates the skin layer without reaching the subcutaneous tissue or cartilage), not only has high patient acceptance but may also directly regulate local nerve - endocrine function, contributing to better blood glucose control. The significant difference in post - treatment blood glucose levels between the two groups (P < 0.05) underscores the superiority of the combined TCM treatment. However, it is important to note that the short intervention period limits interpretability of long-term glycemic outcomes, as the observed changes may not fully capture sustained glycemic control.
Regarding sleep quality, as measured by the Pittsburgh Sleep Quality Index (PSQI), the improvement in the observation group was more pronounced. The PSQI score in the observation group decreased significantly after treatment, and the difference compared to the control group was also significant (P < 0.05). In TCM, insomnia is often associated with liver disharmony. The liver stores blood and houses the soul, and its malfunction can lead to emotional disorders and insomnia. Auricular acupoint pressing and intradermal acupuncture work in tandem to soothe the liver, regulate qi, and calm the mind. By stimulating specific auricular acupoints, the body’s yin - yang balance is restored, alleviating insomnia symptoms. The higher total effective rate in the observation group (90.32% vs 75.00% in the control group) further validates the effectiveness of this combined treatment.
The changes in serum biomarkers provide further evidence for the treatment’s efficacy. NE and 5 - HT are key monoamine neurotransmitters in sleep regulation, with an opposing and coordinated relationship that forms the wake - sleep cycle. BDNF, on the other hand, participates in sleep regulation by modulating neuron regeneration, apoptosis, and reconstruction through the BDNF - tyrosine kinase receptor (Trk) B signaling pathway.30,31 In this study, both groups showed significant changes in these biomarkers after treatment. However, the observation group had more favorable alterations. The more significant increase in 5 - HT and BDNF, along with a greater decrease in NE in the observation group, suggest that the combined treatment can more effectively regulate the body’s neuro-endocrine system, which may be a crucial mechanism underlying its therapeutic effects. Although the magnitude of biomarker changes—particularly BDNF and NE—over the relatively short intervention period was considerable, the post-treatment levels remain within physiologically plausible ranges reported in previous studies of elderly individuals with metabolic or sleep disorders.32,33 We acknowledge that assay variability may have influenced the results, and future studies should incorporate repeated measurements and internal quality controls to ensure reliability. Nevertheless, these findings provide preliminary evidence that neuro‑endocrine modulation may improve sleep and glycemic control, highlighting potential strategies for optimizing TCM interventions and informing future prospective studies.
The quality of life assessment using the WHOQOL - BREF score indicated an improvement in both groups after treatment. Nevertheless, the observation group experienced a more substantial increase. The pre - treatment scores of the two groups were comparable, but the post - treatment difference was significant (P < 0.05). This suggests that the combined TCM treatment not only alleviates the physical symptoms of diabetes and insomnia but also positively impacts the overall quality of life, encompassing physical health, psychological well - being, and social relationships. In modern medicine, sedative and hypnotic drugs are commonly used to treat insomnia in diabetic patients. However, these drugs are associated with issues such as patient dependence, high recurrence rates, and heavy economic and psychological burdens. In contrast, the TCM external treatment methods used in this study, auricular acupoint pressing and intradermal acupuncture, offer advantages such as simple operation, stable efficacy, and high patient acceptance. They can achieve therapeutic effects without the side - effects of drug - induced dependence, providing a safer and more sustainable treatment option for elderly patients with type 2 diabetes mellitus and insomnia. However, adverse effects were not systematically collected or reported—a notable limitation in this geriatric population—and future studies should implement standardized safety monitoring to fully evaluate the intervention’s profile.
Despite the promising results, this study has several limitations. Firstly, the retrospective design introduces potential selection bias and unmeasured confounding factors, such as variations in lifestyle, concomitant medications, or comorbidities. Secondly, the short intervention window restricts the assessment of sustained treatment effects and long-term clinical outcomes. Thirdly, the study was conducted in a single center with a specific demographic profile, which may limit the generalizability of the findings to broader populations or different clinical settings. To overcome these limitations, future research should focus on conducting well - designed, randomized controlled trials (RCTs). Another area for future research is to further explore the underlying mechanisms of auricular acupoint pressing and intradermal acupuncture. Although the current study suggests that these treatments may modulate the neuro - endocrine system and improve the body’s physiological functions, the exact molecular and cellular mechanisms remain unclear. Investigations at the genetic, epigenetic, and proteomic levels could provide a more in - depth understanding of how these treatments work, potentially leading to the development of more targeted and effective therapies.
Conclusion
In conclusion, the combined treatment of auricular acupoint pressing and intradermal acupuncture shows potential in treating elderly patients with type 2 diabetes mellitus and insomnia. However, more research is needed to confirm its efficacy and fully elucidate its mechanisms, with RCTs and in - depth mechanistic studies being crucial steps in this process.
Data Sharing Statement
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Ethics Statement
This study was approved by the Medical Ethics Committee of the First People’s Hospital of Hefei, Anhui Province (No. 20250217). The Committee waived the requirement for obtaining patient consent to review medical records, as the study was retrospective in design and used de-identified clinical data that posed no risk of identifying individual patients. All methods were carried out in accordance with the Declaration of Helsinki, and strict measures were implemented to ensure the confidentiality of patient data throughout the research process.
Consent for Publication
All the authors confirming that written informed consent was obtained from all subjects and/or their legal guardian(s).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work did not receive any funding.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Jia W, Chan JC, Wong TY, Fisher EB. Diabetes in China: epidemiology, pathophysiology and multi-omics. Nat Metab. 2025;7(1):16–34. doi:10.1038/s42255-024-01190-w
2. Yan Y, Wu T, Zhang M, Li C, Liu Q, Li F. Prevalence, awareness and control of type 2 diabetes mellitus and risk factors in Chinese elderly population. BMC Public Health. 2022;22(1):1382. doi:10.1186/s12889-022-13759-9
3. Suzuki K, Miyamoto M, Hirata K. Sleep disorders in the elderly: diagnosis and management. J General Family Med. 2017;18(2):61–71. doi:10.1002/jgf2.27
4. Darraj A. The link between sleeping and type 2 diabetes: a systematic review. Cureus. 2023;15(11):e48228. doi:10.7759/cureus.48228
5. Brewster GS, Riegel B, Gehrman PR. Insomnia in the older adult. Sleep Med Clin. 2018;13(1):13–19. doi:10.1016/j.jsmc.2017.09.002
6. Ditmer M, Gabryelska A, Turkiewicz S, Sochal M. Investigating the role of BDNF in insomnia: current insights. Nat Sci Sleep. 2023;15:1045–1060. doi:10.2147/NSS.S401271
7. Ross JA, Van Bockstaele EJ. The locus coeruleus-norepinephrine system in stress and arousal: unraveling historical, current, and future perspectives. Front Psychiatry. 2021;11:601519. doi:10.3389/fpsyt.2020.601519
8. Chandrasekhara S, Yu S-JS. Sedative, hypnotic, and anxiolytic use and use disorder among older adults. Substance Use Older Adults. 2024;213.
9. Bi L, Gao W, Zhang X, Li N, Han J, Shi M. Efficacy of traditional Chinese medicine external therapy on sleep quality in patients with cancer: a systematic review and network meta-analysis. Asia PacJ Oncol Nurs. 2023;10(11):100308. doi:10.1016/j.apjon.2023.100308
10. Guo K, Lu Y, Wang X, et al. Multi-level exploration of auricular acupuncture: from traditional Chinese medicine theory to modern medical application. Front Neurosci. 2024;18:1426618. doi:10.3389/fnins.2024.1426618
11. Wei W, Huang X, Zhu J. Effect of acupoint therapies on postoperative sleep quality: a narrative review. Med Sci Monit. 2023;29:e938920–938921. doi:10.12659/MSM.938920
12. Wu P, Cheng C, Song X, et al. Acupoint combination effect of Shenmen (HT 7) and Sanyinjiao (SP 6) in treating insomnia: study protocol for a randomized controlled trial. Trials. 2020;21(1):261. doi:10.1186/s13063-020-4170-1
13. Guo M, Wang M, Chen -L-L, et al. Effect of intradermal needle therapy at combined acupoints on patients’ gastrointestinal function following surgery for gastrointestinal tumors. World J Clin Cases. 2022;10(31):11427. doi:10.12998/wjcc.v10.i31.11427
14. Wang X-Q, Xiao L, Duan P-B, et al. The feasibility and efficacy of perioperative auricular acupuncture technique via intradermal needle buried for postoperative movement-evoked pain after open radical gastrectomy: a randomized controlled pilot trial. Explore. 2022;18(1):36–43. doi:10.1016/j.explore.2021.09.007
15. Wang SM, Kain ZN. Auricular acupuncture: a potential treatment for anxiety. Anesthesia Analg. 2001;92(2):548–553. doi:10.1213/00000539-200102000-00049
16. Kubo K, Iizuka Y, Yajima H, Takayama M, Takakura N. Acupuncture- and intermittent compression-induced changes in blood circulation of tendon. J Alternat Complement Med. 2020;26(3):231–238. doi:10.1089/acm.2019.0345
17. Knoll J, Miklya I, Knoll B, Markó R, Rácz D. Phenylethylamine and tyramine are mixed-acting sympathomimetic amines in the brain. Life Sci. 1996;58(23):2101–2114. doi:10.1016/0024-3205(96)00204-4
18. Yan LD, Zhou P, Lai MQ, et al. Effect of acupuncture combined with low frequency rTMS on comorbid mild-to-moderate depressive disorder and insomnia: a randomized controlled trial. Zhongguo Zhen Jiu. 2023;43(4):374–378.
19. Dell’Osso L, Massoni L, Battaglini S, Cremone IM, Carmassi C, Carpita B. Biological correlates of altered circadian rhythms, autonomic functions and sleep problems in autism spectrum disorder. Ann General Psychiatry. 2022;21(1):13. doi:10.1186/s12991-022-00390-6
20. Dos Santos A, Galiè S. The microbiota-gut-brain axis in metabolic syndrome and sleep disorders: a systematic review. Nutrients. 2024;16(3):390. doi:10.3390/nu16030390
21. Liu X, Xu N, Wang S, Jia Q. Efficacy of electroacupuncture for insomnia in cancer patients: a systematic review and meta-analysis. Front Neurol. 2025;16:1512052.
22. Deckers JG, Schellevis FG, Fleming DM. WHO diagnostic criteria as a validation tool for the diagnosis of diabetes mellitus: a study in five European countries. Euro J General Prac. 2006;12(3):108–113. doi:10.1080/13814780600881268
23. Poon MM, Chung KF, Yeung WF, Yau VH, Zhang SP. Classification of insomnia using the traditional Chinese medicine system: a systematic review. Evid Based Complement Alternat Med. 2012;2012:735078. doi:10.1155/2012/735078
24. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213.
25. Skevington SM, Lotfy M, O’Connell KA. The world health organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Quality Life Res. 2004;13(2):299–310. doi:10.1023/B:QURE.0000018486.91360.00
26. Wang L, Wu YX, Lin YQ, et al. Reliability and validity of the Pittsburgh sleep quality index among frontline COVID-19 health care workers using classical test theory and item response theory. J Clin Sleep Med. 2022;18(2):541–551.
27. Mason IC, Qian J, Adler GK, Scheer F. Impact of circadian disruption on glucose metabolism: implications for type 2 diabetes. Diabetologia. 2020;63(3):462–472. doi:10.1007/s00125-019-05059-6
28. Karchmer EI. The excitations and suppressions of the times: locating the emotions in the liver in modern Chinese medicine. Culture Med Psychiatry. 2013;37(1):8–29. doi:10.1007/s11013-012-9289-4
29. Ye H, Chen J, Xu G, Liu J. Standardized auricular therapy for patients with different constitutions and suboptimal health: a retrospective study. Med Acupuncture. 2019;31(2):98–102. doi:10.1089/acu.2019.1345
30. Monti JM. Serotonin control of sleep-wake behavior. Sleep Med Rev. 2011;15(4):269–281. doi:10.1016/j.smrv.2010.11.003
31. España RA, Scammell TE. Sleep neurobiology from a clinical perspective. Sleep. 2011;34(7):845–858. doi:10.5665/SLEEP.1112
32. Sánchez-García S, Moreno-Tamayo K, Ramírez-Aldana R, et al. Insomnia impairs both the pro-BDNF and the BDNF levels similarly to older adults with cognitive decline: an exploratory study. Int J Mol Sci. 2023;24(8):7387. doi:10.3390/ijms24087387
33. Morrow LA, Linares OA, Hill TJ, et al. Age differences in the plasma clearance mechanisms for epinephrine and norepinephrine in humans. J Clin Endocrinol Metab. 1987;65(3):508–511. doi:10.1210/jcem-65-3-508
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Novel Associations of Dyslipidaemia with Vitamin D and Bone Metabolism in Elderly Patients with Diabetes: A Cross-Sectional Study
Zha K, Wang N, Zhou Y, Ying R, Gu T, Zhao Y, Guo H, An Z, Lu Y
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2939-2950
Published Date: 22 September 2023