Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Collaborative Communication: A Qualitative Study of Roles and Emphases of Health Care Providers in Obstetrics and Gynecology
Authors Gong W ![]() , Tang J, Chen Y
, Tang J, Chen Y ![]() , Ma J
, Ma J
Received 28 December 2023
Accepted for publication 15 April 2024
Published 29 April 2024 Volume 2024:17 Pages 1913—1922
DOI https://doi.org/10.2147/JMDH.S457056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wanqi Gong,1 Jiamei Tang,1 Yang Chen,2 Jing Ma3
1School of Journalism and Communication, Guangdong University of Foreign Studies, Guangzhou, People’s Republic of China; 2Health Science Center, Jinan University, Guangzhou, People’s Republic of China; 3The First Affiliated Hospital of Guangzhou Medical University, Department of Gynecology and Obstetrics, Guangzhou, People’s Republic of China
Correspondence: Jiamei Tang, School of Journalism and Communication, Guangdong University of Foreign Studies, No. 1689 Bai Yun Avenue, Guangzhou, 510420, People’s Republic of China, Tel +86 20 39328095, Email [email protected]
Purpose: Clinical nursing in obstetrics and gynecology is a technically demanding job. Doctors and nurses have different professional backgrounds and work priorities, and there are differences in communication modes, which can easily lead to poor communication between medical staff and their patients. Therefore this study aims to examine the different communication roles and emphases of obstetrician and gynecologists, nurses and midwives in different sections of SEGUE framework, and further navigate the effectiveness and differences of offline and online provider-patient communication.
Participants and Methods: This study employs in-depth interviews to address the research questions. A total of 24 health care providers, including 8 doctors, 5 midwives and 11 nurses, were interviewed face-to-face or by telephone.
Results: Doctors pay more attention to the “giving information” stage, while nurses pay more attention to “set the stage” and “elicit information” steps. Midwives and nurses spend more time with patients before and after labor. In addition to information giving, they also accommodate the “understand the patient’s perspective” and “end the encounter” steps. Nurses and midwives would attach greater importance to “understanding of patients’ perspective”. Online medical consultation is more convenient for patients, which can be used as a follow-up complement to offline medical consultation.
Conclusion: The health care providers of different types in obstetrics and gynecology communicate collaboratively with patients, highlighting the equally important role of midwives and nurses when communicating with patients. Nurses focus on “set the stage” and “elicit information” stage. Midwife is another important information source and medical care provider, especially for pregnant women in stable conditions. Nutrition clinic of midwife could be recommended for hospitals in second- and third-tier cities, which could help to alleviate obstetricians’ workload. The provision of an online collaborative consultation could be beneficial supplement after face-to-face doctor-patient communication.
Keywords: SEGUE framework, physician-patient communication, obstetrician and gynecologist, online health consultation, midwife
Introduction
Poor health care provider-patient communication often causes unexpected hazards to the medical service sector, with more than 80% of the clinical disputes being provoked by insufficient provider-patient communication or improper communication.1,2 The culprit for clinical disputes is outright confrontation caused by insufficient provider-patient communication, and most of the time doctors serve as the principal responsible party for insufficient provider-patient communication.3 In the institutional environment of Chinese hospitals, structured conversations and doctor-led, technology-focused communication models highlight the power imbalance between doctors and patients, which eventually leads to barriers to provider-patient communication.4 Physician-patient conflicts are notably prominent in obstetrics and gynecology. Because most diseases in obstetrics and gynecology involve patient privacy, and the high risk factors associated with some critical illnesses increase the likelihood of provider-patient disputes in this field.5–9 The poor communication between health workers and patients further deteriorates the already fragile relationship, which is believed to be one of the main reasons for the obstetrics and gynecology to have an ever-increasing incidence rate of clinical disputes.9
Therefore, the communication skills possessed by medical staff are crucially important to improve the quality of provider-patient communication,10 and in turn good provider-patient communication will enhance the level of mutual understanding and respect between physicians and patients, which is an effective way to improve medical quality, reduce and prevent the occurrence of medical disputes, and improve provider-patient relationship.11–14 Among the various frameworks for teaching and assessing communication skills, SEGUE framework is designed to comprehensively understand the communication skills of medical professionals from five scenarios of a medical encounter, namely “set the stage”, “elicit information”, “give information”, “understand the patient’s perspective” and “end the encounter”. After being put into use for many years, SEGUE framework proves to work effectively in terms of reliability and validity, and has been widely used in provider-patient communication education, assessment and research.15–19 However, the majority of studies on SEGUE concentrated on the communication skill of physicians,17–19 while neglecting other groups of health workers. Given the long-term nature of consultation and the limited time doctors have to address every patient’s needs throughout the process, nurses and midwives play crucial roles in physician-patient communication in obstetrics and gynecology.
Nurses and midwives of obstetrics are deeply involved in communications with patients, and many information briefing, examinations, nursing and treatment need to be completed by nurses and midwives, and they are also involved in outpatient clinics, responsible for consultation and various interpretations.20 Clinical nursing in obstetrics and gynecology is a technically demanding job. Doctors and nurses have different professional backgrounds and work priorities, and there are differences in communication modes, which can easily lead to poor communication between medical staff and their patients.21 It has been discovered that 80% of the medical disputes between nursing staff and patients are caused by communication problems, and this problem is particularly serious within the obstetrics and gynecology.22 An Irani study focuses on midwives’ significant role by pointing out professional ethics and personal character influence midwife-patient communication.23 As nurses play a crucial role in communicating with patients, caring communication models featured with strong empathy would relieve patients’ intense pressure.24 Trust-building through communication entails the patient’s acceptance of vulnerability, information disclosure, relinquishing control, conceding to health workers’ expertise, and feeling heard. Systematic communication skills training is vital for enhancing this trust in obstetrics and gynecology.25 Therefore it is essential to explore the different roles and characteristics of doctors, nurses and midwives when trying to improve the provider-patient communication within the obstetrics and gynecology.
Since the outbreak of the COVID-19 pandemic in 2020, patients of the obstetrics and gynecology have begun to access medical consultation remotely through Internet hospitals and other online diagnosis and treatment platforms, and consequently online medical service sees a rapid growth.26,27 The Internet medical service has succeeded to some extent in enhancing the satisfaction rate of obstetrics and gynecology patients and improving the provider-patient relationship.28 Obstetrics and gynecology patients and doctors are gradually adapting to the online-and-offline mixed medication and communication mode.29 The development of online health consultation further highlights the importance of online provider-patient communication. However, the quality assessment of Internet provider-patient functional communication has shown that the current Internet medical and health management platform model in China is not standardized, and the quality of online provider-patient functional communication is relatively low.30 The SEGUE framework, while comprehensive in its approach to assessing provider-patient communication, may exhibit limitations in adequately accommodating the requirements inherent to online health consultation context.
In view of this online-offline mixed communication context, this study tries to conduct targeted research on the health workers patient communication in the obstetrics and gynecology based on SEGUE framework, examine the different communication characteristics and emphases of obstetrician and gynecologists, nurses and midwives in different steps of SEGUE, and provide empirical evidence on the communication key points of different types of obstetrics and gynecology medical staff. The study also further navigates the effectiveness and differences of offline and online provider-patient communication, therefore to provide an empirical basis and make an empirical contribution for improving the teaching and assessing framework for communication skills for health workers. In addition, through the comparison of online and offline communication experiences in the post-epidemic era, this study is also designed to explore effective online health communication to achieve efficient with limited medical resources, improve the efficient use of medical resources and maximize the therapeutic effect on patients.
Materials and Methods
Ethical Approval
The procedures of this study were reviewed and approved by Human Subjects Ethics Sub-Committee of City University of Hong Kong (No. H002708). The participations were voluntary; the informed consent, including the permission to publish the results of the research and anonymized responses, was obtained.
Participants and Procedure
This study employs in-depth interview with healthcare providers of varying roles within the field of obstetrics and gynecology to address the research questions. Purposive sampling was utilized to ensure a diverse representation of participants based on gender, age, professional designation (doctor, nurse, or midwife), title, and experience levels. The initial target was to include thirty interviewees, comprising 8 doctors, 14 nurses, and 8 midwives, according to the approximate composing proportion of health workers in obstetrics and gynecology. However, six declined participation citing time constraints. Subsequently, a total of 24 healthcare providers, comprising 8 doctors, 5 midwives, and 11 nurses, were interviewed either face-to-face or via telephone. Notably, midwives play a distinctive role, as they are actively engaged not only in the care continuum throughout pregnancy and delivery but also in the specialized domain of midwifery during the final stages of labor.
The first round of interviews took place from December 2021 to March 2022, involving 16 participants. The second round occurred from June to September 2023, with 8 participants interviewed. The ongoing COVID-19 pandemic posed significant challenges, as the hospital enforced strict protocols prohibiting non-medical staff from entering the wards and medical staff from leaving, resulting in an interruption to the interview process. Consequently, the interviews were temporarily halted until the outbreak restrictions were lifted. Given the predominantly open-ended nature of the research questions, researchers employed a responsive approach, probing for additional details based on the interviewees’ responses. As a result, the duration of each interview with healthcare providers ranged from 30 to 55 minutes, ensuring thorough exploration of the topics under investigation. Two authors (YC and JM) conducted the interview. Since both of them have worked in the hospital. The information of the interviewees is as follows (Table 1):
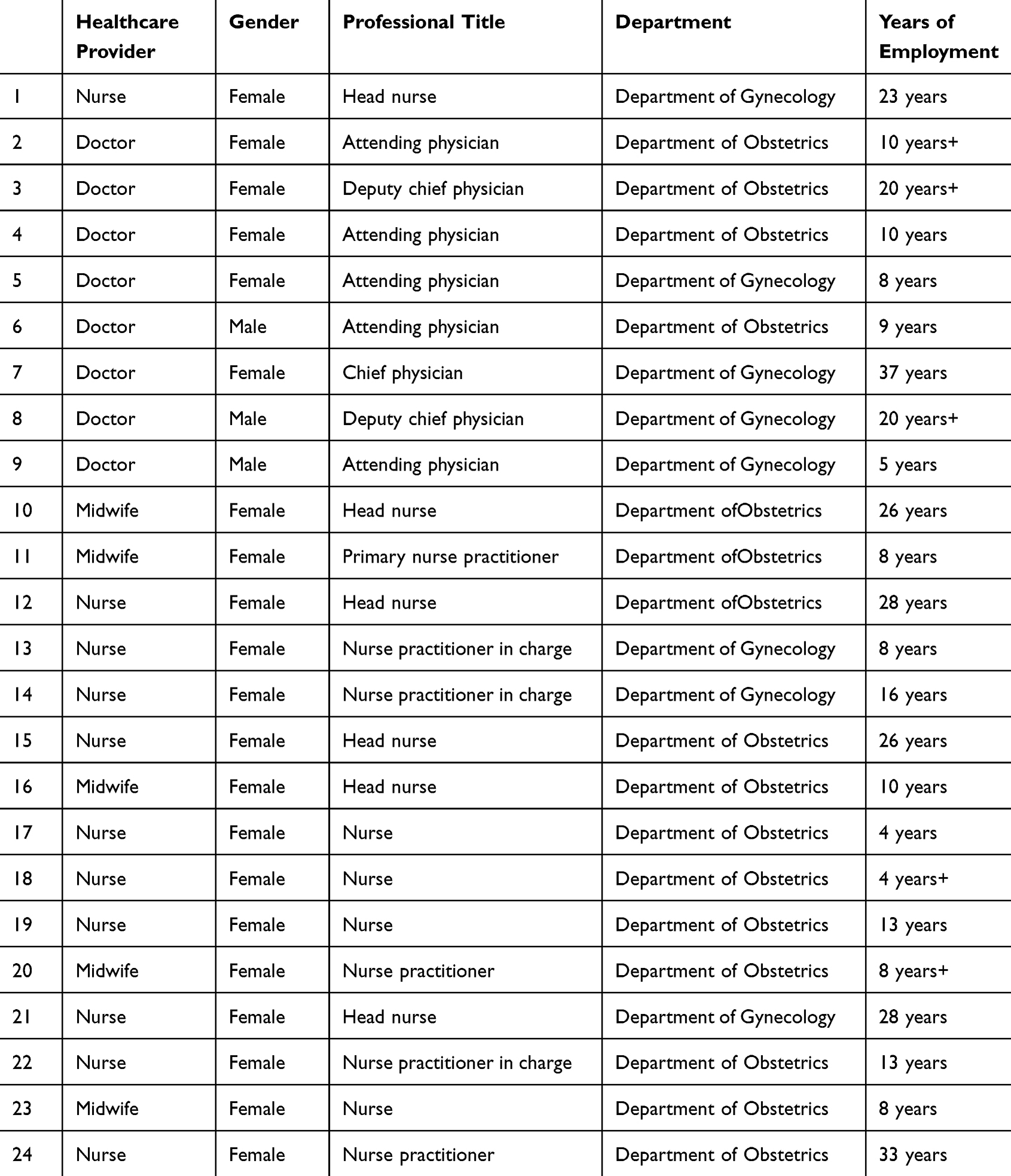 |
Table 1 Respondents’ Information |
The interview outline is mainly based on SEGUE framework, inquiring the interviewees about the preparation before communication with patients, the gathering and giving of information, the understanding of patients’ perspective, the end encounter stage, and the impact of communication on patients’ compliance and follow-up treatment (Appendix A). Furthermore, within the context of increasing online consultations because of COVID-19 pandemic, we also inquired the interviewees’ opinions on online consultation. Appendix A shows the interview outline. All interviews were audio recorded and transcribed. Interviewers also recorded field notes during interviews to aid transcript analysis.
Data Analysis
The interview material was analyzed through inductive thematic approach. Coding was carried out by two researchers (WQG and YC). Both coders independently coded all transcripts to ensure reliability and consistency. Themes were developed via SEGUE five steps, online and offline context and comparison of communication experiences across participants. The codebook underwent iterative refinement as the researchers independently double-coded all remaining transcripts. They convened periodically to review the application of coding and to address any discrepancies through consensus discussions.
Results
Different Healthcare Professionals Place Emphasis on Different Communication Stages
In Obstetrics and gynecology, nurses primarily focus on “set the stage and elicit information” stage, while doctors concentrate more on information giving stage. Nurses and midwives take more responsibility for routine information communication with general patients. They entail supporting physicians in the initial stages of patient interaction, including setting the communicative context and gathering preliminary information from patients before consulting with the physician.
Nurse 14:We usually have to record patients data. Most of them are personal information, such as ID, phone number, education level. And we will ask her history of disease and pregnancy. Because some patients may take some short-acting contraceptives orally, and some may have malignant tumors.
Midwife 16:We will ask the medical history. If she is a multipara, we will ask: ”How much is the Birth weight of your first child? Did you have a side cut? Is there any postpartum bleeding? Was your first labor fast or slow?” In fact, we just want to assess if she can have a natural birth or not.
The midwives take part in whole process, from nutritional and psychological assessment to prenatal guidance, as well as the final stage of labor. The midwives, after doctors, would communicate with pregnant women in their late pregnancy. In addition to information giving, they also accommodate the “understand the patient’s perspective” and “end the encounter” steps.
Midwife 10:Doctors mainly prescribes medical examination or medicine to patients according to their medical condition, and then tell the patients about their health condition according to their examination reports. However the follow-up details, such as how to use the drugs, are done by nurses and us. We actually help doctors to do so because doctors do not have much time.
Midwife 11:The pregnant women will be transferred to the midwifery clinic in the later stages of pregnancy. We will tell them what preparations should be made when they come to hospital for full-term labor. If there is any abnormality, we will tell them to take the medical report to the doctors, who will make an overall assessment of their conditions and further consider whether they should choose natural labor or Caesarean section.
Doctors lead the “information giving stage” through rational communication, which embodies the authority status in the communication process. Then doctors can take the details collected by the nurses and use their expertise to explain diagnoses, treatment plans, and other vital health-related information in a comparatively brief consultation. However, in light of the substantial volume of patient consultations every day, doctors only pay more attention to patients under severe conditions.
Doctor 2:I often tell my patients the pros and cons of having medical examinations, so that they could make a well-informed decision. We should give them an in-depth analysis, instead of merely offering emotional support.
Doctor 4:For those major surgeries involving critically ill patients, I will communicate fully with the patients. I will tell them if the risks of having surgeries outweigh the risks of not having surgeries, and I will let them know that best possible efforts will be made to reduce surgery risks. We will assess and decide whether we should choose surgeries or not.
Nurses and Midwives Attach Greater Importance to “Understanding of Patients’ Perspective”
Pregnant women’s emotional well-being hold significant influence over both maternal health and fetal development. Nevertheless, doctors have limited time to provide extensive emotional support. The nurses will keep a close eye on patients’ emotions and observe patients’ family relationship before the formal provider-patient communication begins.
Head Nurse 15:The doctors’ communication will focus more on pregnant women’s physical condition. While for our nurses, we put more emphasis on their feelings or mood, or the way these women react to their pregnancies. Apart from providing medical treatment and maternal care, we provide mental care to them, such as many details in relation to their social network, family or daily life.
Head Nurse 1:The jobs in the department of gynecology are particularly sensitive. First of all, women are sensitive creatures. Secondly, some diseases are sensitive. We need to find out the relationships between our patients and their family first. Some people are difficult to communicate with, and some professions are very sensitive. When we are making an evaluation, we need to bear in mind many important factors.
Nurse 14:Many young women come here by themselves. When giving them medical advice, we need to address their psychological needs and other personal concerns. We first soothe the patients’ nerve, then we may tell them safe contraception methods and effective ways to look after themselves.
Midwives and nurses spend more time than doctors with patients before and after labor. Due to hormonal fluctuations, the physical pain associated with childbirth, and the apprehension regarding the newborn, parturient often exhibit heightened emotional sensitivity. Therefore the understanding of patient from healthcare providers assumes significance during this juncture. However, physicians may encounter constraints in allocating sufficient time to address patient emotions. Hence, the role of nurses and midwives becomes particularly crucial in conveying compassion, empathy, and elucidating the entire childbirth process to expectant mothers during this critical period.
Nurse 18:When women give births, some of them are anxious and nervous. So mainly of my work is to accompany her, to listen to her needs, to consider her feelings, and to give her more encouragement and help.
Midwives play an important role between doctors and nurses, so midwives’ communication should be flexible. They accompany parturient throughout the entirety of the childbirth process, thereby necessitating their provision of not only accurate obstetric knowledge but also emotional support from the patient’s perspective.
Midwife 20:In the delivery room, we focus on the labor process, such as how she performed and how she felt, especially in terms of pain. (Before and after labor) In the ward, we will also pay attention to her life aspects, giving her some long-term health education, teaching her how to prevent falls, etc.
Experience Enhancing Communication Skills
Doctors, midwives and nurses with richer experience or honorary professional titles are more likely to care for the feelings of patients than younger ones. Their advanced proficiency in communicating with patients during the information-giving stage is notably refined, reflecting more mature skill in navigating delicate medical discussions with empathy and clarity.
Head Nurse 12:Some individual (patients) have demanding requirements. When she comes to give birth to a baby in our hospital, what she hopes most is to deliver smoothly. I will communicate with her from this aspect, and she will feel safe and pleased that she has been looked after with good care.
Doctor 3:The (understanding of patients) requires accumulation of experience, which cannot be done when you are young. When you are young, you may be irritable But when you become mature and professionally competent, you will grow your confidence, and your patients will trust you as a good doctor. Communication is a kind of art. I also feel that it has something to do with our personality and professional training process.
Differences Between Online and Offline Health Consultation
Online medical consultation is more convenient, which can be used as a follow-up complement to offline medical consultation. Online communication tools, such as WeChat groups, facilitate more convenient daily interactions between healthcare providers and patients. Social media platforms also offer additional channels for disseminating health knowledge and public education. The online consultation concentrates on the “elicit information” and “give information” stage, since it typically occurs during healthcare providers’ off-duty hours. Additionally, due to patients’ concerns regarding privacy, individuals often refrain from divulging excessive personal emotions or information during the online communication.
Doctor 5:Now we will leave the patient a QR code in outpatient service, which will enable the patient to ask further questions online. The online medical consultation is definitely more convenient, since sometimes we are really too busy in seeing outpatients. Sometimes I may forget mentioning follow-up treatment to my patients. Later, it will be better to have a feedback online.
Doctor 2:Our department has our own official WeChat account to popularize medical science, such as some basic knowledge during pregnancy. We will post the information to the group, and pregnant mothers can also discuss them in the group.
Nurse 15:We have set up some Wechat groups, which can reduce patients’ anxiety about their disease, especially when patients were anxious……In general, it helps patients. But from the experts of online nursing care. I think it mainly gives patients some suggestions about how to do or how to understand rather than diagnostic or therapeutic content.
However, due to the inability to conduct face-to-face examinations, online consultations may not be suitable for managing patients with serious or complex medical conditions that require thorough physical assessments and diagnostic tests.
Nurse 19:Some patients, for example, she said “I had a fever or my baby had a fever”, but I cannot see whether it was true or not. The truth maybe is different from what she describes, so there are pros and cons about online medical consultation.
Midwife 16:Most of the Wechat friend I accepted were postpartum patients. I would give them some information about breast feeding, wound care and rehabilitation guidance. …… I did not give them treatment suggestion, because it’s out of my hands.
Mutual Trust Building
Different roles of health workers consistently identify the cultivation of mutual trust as the foremost challenge encountered during patient communication, a notion that aligns with the outcome through SEGUE training. The establishment of trust emerges as a pivotal aspect of effective healthcare communication, serving as a cornerstone for fostering meaningful patient-provider relationships and optimizing patient outcomes.
Midwife 11:The biggest difficulty and obstacle is that your patients do not trust you. When a pregnant woman and her families communicate with us, we must let them feel safe and trust us in the first place. Only in this way she will be highly cooperative.
Doctor 4:I think the most important thing is to build trust. Actually, patients do not know much about medical treatment, but will demonstrate a high level of compliance if there is such a trust.
Midwife 16:We need empathy. Sometimes the pain makes parturient lose her temper. If you have a bad attitude, it’s useless for changing her bad mood, and sometimes you’ll get complain. So even when I was busy, I will make priority, and do the important thing first. You should not leave her alone without any explain.
Discussion
Based on the SEGUE framework, this study explores the communication between patients and health professions in obstetrics and gynecology, and compares the provider-patient communication emphasis of health care providers of different types, especially the role of midwives and nurses. The findings reveal the overall communication process between the health workers of obstetrics and gynecology department and their patients. What’s more, within the context of COVID-19 pandemic, online medical consultation becomes increasingly popular. The results also show how online and offline medical services are integrated and applied to serve the patients.
Physicians Provide Medical Diagnoses, While Nurses Prioritize Emotional Support
Physicians lead the “information giving” stage. Due to the busy outpatient in China, physicians are often constrained by limited time and can only prioritize the provision of medical information to patients, particularly those with severe conditions. This involves explaining the necessity of diagnostic tests, interpreting test data, and outlining subsequent treatment plans. As a result, doctors may find it challenging to adequately address the emotional needs of their patients.
Therefore, nurses play important roles in the steps of “set the stage” and “elicit information”, they would express their understanding and conciliation for patients according to their backgrounds and emotional states, and communication with their families. Nurses will try to address patients’ psychological needs and soothe the patients’ anxieties prior to the patient-doctor encounter. This preparatory work is vital in laying the groundwork for a productive and therapeutic interaction between the patient and their healthcare providers.
Midwife is a unique specialty within obstetrics and gynecology. During face-to-face communication between midwives and pregnant women in the nutrition clinical (often more than 20 minutes for every pregnant woman), midwives can better understand the feelings and concerns of these pregnant women. Midwives play the major roles in “understanding the patient’s perspective”, and “end the encounter” steps. They collect detailed information about the pregnant women so that doctors can make more comprehensive evaluations in the follow-up communication process. Midwives will continue to monitor and care for the nutritional status, physical recovery, and mental wellbeing of mothers postpartum. They provide explanations about subsequent examination plans, ensuring that mothers are well-informed and at ease. Their understanding will effectively alleviate feelings of helplessness and depression that may arise postpartum.
Nurse and Midwives are Irreplaceable Information Sources in Obstetrics and Gynecology
Although midwives and nurses are not the main roles in information giving step, remains indispensable as valuable sources of information for patients throughout the provider-patient communication process. Nurse is the first point of contact for patients seeking medical attention and the ones who spend much time with them, offering care and support, thus bridging the gap between medical professionals and their patients. Nurses will focus on “set the stage” and “elicit information”. They would address concerns or anxieties the patient may have, providing a welcoming and supportive environment, and collecting pertinent details about the patients.
Midwives are another important information source and medical care provider, especially for pregnant women in stable conditions. Midwives have their own nutrition clinical with pregnant women. They will engage expectant mothers in detailed discussions regarding dietary requirements, nutritional supplements, and healthy eating habits essential for the well-being of both mother and baby. By offering these comprehensive services, midwives play a crucial role in promoting the health and well-being of expectant mothers and their unborn children.
Dynamic Integration of Online and Offline Consultation
Due to the COVID-19 pandemic, it is much harder to make offline medical appointments, and patients are in fear of risks of being infected when seeing doctors offline, therefore online diagnosis and treatment activities have seen a significant increase. Online medical platforms in China have registered a record high number of medical consultations compared to that before the COVID-19 pandemic. More and more Chinese hospitals have also launched online diagnosis and treatment services. Previous studies tend to focus more on online doctor-patient communication mode and effectiveness,31,32 while the in-depth interviews of this study provide a new pattern for the combination of online and offline health consultations. Patients consult doctors face-to-face at first, doctors then provide a way of continuing online communications (such as QR code for follow-up online consultants). Doctors and patients can communicate online subsequently, if there are any doubts that require further consultations or daily inquires. Besides online diagnosis platform, healthcare workers also use online chatting group to communicate with regular patients.
This can save patients’ time and efforts to make health appointments and go to hospitals, and the medical inquiries are not restricted by time and place. In addition, obstetricians and gynecologists are able to offer better consultation service based on their preliminary offline inquires about patients’ basic conditions and physical examination results, thereby the efficiency of diagnosis and treatment would be greatly improved. It is of great significance for this pattern to be further promoted for the treatment of obstetrical diseases and other chronic diseases during pandemics, as the communications between health care providers and patients of those diseases alike would last longer period of time and need a greater number of hospital visits.
Practical Implication
The main respondents in this study are from obstetrics and gynecology departments in 3A hospitals in a major Chinese city. Some measures in their responses could provide enlightenment for future practices, such as the nutrition clinic of midwives. It is discovered that these practices are popularly accepted by patients. So these measures can be introduced to obstetrics and gynecology practices in other regions or applied to medical services for chronic diseases with similar demands, for example, diabetes. In addition, the provision of online collaborative consultations after face-to-face communication is also worth recommending. Obstetrician and Gynecologist could provide subsequent diagnosis and treatment then can be proceed based on better mutual understanding, in the end contributing to lowering the online misdiagnosis rate. Nurses and midwives could make daily nutrition notes and health information for pregnant women on online patient group. The combination of online and offline health consultations not only reduce burdens of Chinese hospitals, but also improve the efficiency and effectiveness of online health service, both of which have been urgently needed since the outbreak of COVID-19 pandemic.
Gender, age and experience of medical care providers tend to affect the communication effectiveness between doctors and patients in obstetrics and gynecology. Our study also finds that medical service providers who are experienced, or with higher grade of professional titles, demonstrate a higher level of patience and empathy toward patients, as well as remarkable communication skills. Medical service providers of different types all agree that appropriate communication can promote patients’ compliance so as to conduct better medical service.
Limitation
It should be noted that this study employs the method of in-depth interviews, and the samples only derive from obstetrics and gynecology departments in major cities. This consultation pattern cannot represent all obstetrics and gynecology departments in Chinese hospitals. Hence, the follow-up studies could utilize surveys, observations and field work of ethnography to further investigate the provider-patient communication in obstetrics and gynecology. Besides, this paper only discusses the research questions from health care providers’ perspective. It would provide more significant insights and practical reflections for SEGUE framework if patients’ feedbacks on the communications with doctors, midwives and nurses can be included.
Conclusion
Due to the limited available to have face-to-face communication in Chinese hospitals, it is challenging for obstetrician and gynecologist to perform all the required five communication steps as indicated in SEGUE framework. This study examines the health care provider-patient communication through in-depth interviews with doctors, nurses and midwives in obstetrics and gynecology. The health care providers of different types in obstetrics and gynecology communicate collaboratively with patients, highlighting the equally important role of midwives and nurses when communicating with patients. Online health service platforms can work as a useful supplement to face-to-face consultations. The online consultations leave a path for follow-up online diagnosis and treatment after face-to-face diagnosis between doctors and patients, which can improve the effectiveness of online diagnosis and treatment and enhance daily understanding of patients.
Funding
Funded by National Institute of Hospital Administration(NHC) Management and Evaluation Research Project (NIHA23JXH017) and National Social Science Foundation (No. 23BXW031).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Xu T, Yong B, Yin L, Mi T. Patient perception and the barriers to practicing patient-centered communication: a survey and in-depth interview of Chinese patients and physicians. Patient Educ Couns. 2016;99:
2. Zhang XQ, Sleeboom-Faulkner M. Tensions between medical professionals and patients in mainland China, camb. Q Healthc Ethics. 2011;20(3):458–465. doi:10.1017/S0963180111000144
3. Sun XY, Shi XY, Wang SW, Zhang WY. Looking for solutions of doctor-patient disputes: a study and practice based on doctors’ responsibilities. Jiang Health Manag. 2018;29:1351–1353. doi:10.3969/j.issn.1005-7803.2018.12.002
4. Tu J, Kang G, Zhong J, Cheng Y. Outpatient communication patterns in a cancer hospital in China: a qualitative study of doctor–patient encounters. Health Expect. 2019;22(3):594–603. doi:10.1111/hex.12890
5. Zhang LY. The significance of provider-patient communication in clinical obstetrics and gynecology. China Health Indus. 2018;2:195–196. doi:10.16659/j.cnki.1672-5654.2018.02.195
6. Yang X, Bai WP. The key points of provider-patient communication in clinical obstetrics and gynecology. China Psycho Health J. 2012;26. 10.3969/j.issn.1000-6729.2012.03.001.
7. Xiong W, Zhou R. The importance of provider-patient communication in clinical obstetrics and gynecology. J Prac obste gyne. 2010;26:498–499.
8. Zhang KZ. The teaching and assessment of provider-patient communication skills for obstetrics and gynecology doctors. J Trad Chinese Med Manage. 2014;22:973–974. doi:10.16690/j.cnki.1007-9203.2014.06.030
9. Hu Y, Xie B, Yu H, Yan J, Ren ML. The research of provider-patient communication skills for obstetrics and gynecology doctors. Chinese J Grad Med Educ. 2019;3:202–205.
10. Shaw J, Sethi S, Vaccaro L, et al. Is care really shared? A systematic review of collaborative care (shared care) interventions for adult cancer patients with depression. BMC Health Serv Res. 2019;19(1):1–18. doi:10.1186/s12913-019-3946-z
11. Liu SQ. Representation of doctor-patient images on Chinese newspapers: a narrative analysis of four violent clinical disputes. Contem Commun. 2016;2:40–44.
12. Griffin SJ, Kinmonth AL, Veltman M, Gillard S, Grant J, Stewart M. Effect on health-related outcomes of interventions to alter the interaction between patients and practitioners: a systematic review of trials. Ann Fam Med. 2004;2(6):595–608. doi:10.1370/afm.142
13. Stewart MA. Effective physician–patient communication and health outcomes: a review. Can Med Assoc J. 1995;152:1423–1430. doi:10.0000/PMID7728691
14. Jackson JL. Communication about symptoms in primary care: impact on patient outcomes. J Altern Complement Med. 2005;11:S51–56. doi:10.1089/acm
15. Makoul G. The SEGUE framework for teaching and assessing communication skills. Patient Educ Couns. 2001;45(1):23–34. doi:10.1016/S0738-3991(01)00136-7.
16. Zhu D, Liu D, Feng XH, et al. Analysis of the effects on residents’ medical communication skills with SEGUE framework. Chin J Clinicians. 2016;10:3678–3682,doi:CNKI:SUN:ZLYD.0.2016–23–041.
17. Burt J, Abel G, Elliott MN, et al. The evaluation of physicians’ communication skills from multiple perspectives,Ann. Fam Med. 2018;16:330–337. doi:10.1370/afm.2241
18. Assis-Hassid S, Heart T, Reychav I, Pliskin JS, Reis S. Existing instruments for assessing physician communication skills: are they valid in a computerized setting? Patient Educ Couns. 2013;93(3):363–366. doi:10.1016/j.pec.2013.03.017
19. Xiong Y, Wang D, Chen H, Wang X, Zhang X. Development and validation of online textual pediatrician-parent communication instrument based on theSEGUE framework, Biomed. Res Int. 2019;5:1–8. doi:10.1155/2019/8638174
20. Yang RZ, Li Y, Zhang CJ, Sun GH. The health education and nurse-patient communication in out-patient operation room of obstetrics and gynecology. China Prac Med. 2010;15:262–263. doi:10.14163/j.cnki.11-5547/r.2010.28.099
21. Liu L, Wang L, Zhang YL. Effect of SBAR communication mode based on humanistic care on nursing quality and patients’ satisfaction in obstetrics and gynecology. Res Pract Clini Med. 2020;33:161–163. doi:10.19347/j.cnki.2096-1413.202033060
22. Duan XL, Song YZ. The application of nurse-patient communication in nursing work of obstetrics and gynecology. Contemp Med. 2009;15:141–142. doi:10.3969/j.issn.1009-4393.2009.24.109.
23. Amiri-Farahani L, Gharacheh M, Sadeghzadeh N, et al. Iranian midwives’ lived experiences of providing continuous midwife-led intrapartum care: a qualitative study. BMC Pregnancy Childbirth. 2022;22(1):724. doi:10.1186/s12884-022-05040-z
24. Zhu WJ, Wang HY. Empathy in the communication between nurses and gynecological patients. J Nurs Sci. 2007;12:72–74.
25. Dalton ED, Pjesivac I, Eldredge S, et al. From vulnerability to disclosure: a normative approach to understanding trust in obstetric and intrapartum nurse-patient communication. Health Communication. 2021;36(5):616–629. doi:10.1080/10410236.2020.1733225
26. Mei HH, Ruan MH, Xu ZZ, Wang L, Shao XH. Investigation and analysis of the status quo of interpersonal communication ability of obstetrics and gynecology nurses. Nurs Manage. 2019;36(01):44–46. doi:10.3969/j.issn.1671-9069.2019.01.015
27. Cheng H, Zhou Q, Liu XL. The opportunity and reflection of internet + healthcare under covid-19 pandemic. China Hosl Manag. 2020;40:38–40.
28. Zhang Q, Zhu ZG, Shen NQ, Liu Y, Yan ZZ. The practice and reflection of internet + healthcare in prevention and control of covid-19 pandemic. Jiang Health Manag. 2020;31:1570–1573. doi:10.3969/j.issn.1005-7803.2020.12.010
29. Kuang FY, Huang JW, Wu MX, Hong L, Feng XJ. Research on the application of internet medical service platform in obstetrics and gynecology nursing. China Digital Medicine. 2020;15:130–132. doi:10.3969/j.issn.1673-7571.2020.07.042
30. Wang HJ, Feng YL. Effect of ” internet + healthcare” on the traditional healthcare service delivery mode and physician-patient relationship and the suggested counter-measures. Chinese General Pract. 2017;25:3191–3194. doi:10.3969/j.issn.1007-9572.2017.25.027
31. Xiong YQ, Chen HH, Liang C, et al. Comprehensive evaluation of the quality of internet doctor-patient in instrumental communication. Chinese Health Qual Manag. 2021;28:63–65. doi:10.13912/j.cnki.chqm.2021.28.6.17
32. Zhu L, Li L, Lang J. The attitudes towards defensive medicine among physicians of obstetrics and gynaecology in China: a questionnaire survey in a national congress. BMJ Open. 2018;8(2):e019752. doi:10.1136/bmjopen-2017-019752.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.