Back to Journals » Infection and Drug Resistance » Volume 19
Colistin Therapy for Urinary Tract Infections Due to Multidrug-Resistant Bacteria: Experience at a Tertiary Academic Medical Center
Authors Aldairem A ![]() , Alowais SA
, Alowais SA ![]() , Alshaya AI
, Alshaya AI ![]() , Alrashed M, Alqahtani T, Alharbi L, Alshehri R, Al Dughaish ST, Alenazi A, Bin Saleh K
, Alrashed M, Alqahtani T, Alharbi L, Alshehri R, Al Dughaish ST, Alenazi A, Bin Saleh K
Received 12 March 2026
Accepted for publication 15 May 2026
Published 25 May 2026 Volume 2026:19 608721
DOI https://doi.org/10.2147/IDR.S608721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Atheer Aldairem,1– 3 Shuroug A Alowais,1– 3 Abdulrahman I Alshaya,1,3,4 Mohammed Alrashed,1– 3 Tariq Alqahtani,2,5,6 Lina Alharbi,7 Rawan Alshehri,3 Sarah Turki Al Dughaish,8 Arwa Alenazi,7 Khalid Bin Saleh1– 3
1Department of Pharmacy Practice, College of Pharmacy, King Saud Bin Abdulaziz University for Health Sciences (KSAU-HS), Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center (KAIMRC), Riyadh, Saudi Arabia; 3Department of Pharmaceutical Care, King Abdulaziz Medical City (KAMC), Ministry of National Guard–Health Affairs, Riyadh, Saudi Arabia; 4Collaboration and Partnerships Department, King Abdullah International Medical Research Center (KAIMRC), Riyadh, Saudi Arabia; 5College of Pharmacy, Department of Pharmaceutical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 6Department of Preclinical Studies, Benefit and Risk Assessment Executive Directorate, Drug Sector, Saudi Food and Drug Authority (SFDA), Riyadh, Saudi Arabia; 7College of Pharmacy, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 8Clinical Pharmacy Department, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia
Correspondence: Atheer Aldairem, Email [email protected]
Background: Urinary tract infections (UTIs) caused by multidrug-resistant Gram-negative bacteria (MDR-GNB) present increasing therapeutic challenges, especially in regions with limited access to novel β-lactam/β-lactamase inhibitors. Colistin remains a salvage therapy in such cases; however, data describing its real-world efficacy and nephrotoxicity in urinary infections are limited.
Methods: We conducted a retrospective cohort study of adult patients who received intravenous colistin (colistimethate sodium) for culture-confirmed UTIs at a tertiary academic medical center in Riyadh, Saudi Arabia. The primary outcome was colistin-induced acute kidney injury (AKI), defined as an increase in serum creatinine of ≥ 26 μmol/L from baseline per the AKIN creatinine criterion. Secondary outcomes included microbiologic failure, clinical failure, and in-hospital mortality. Multivariable logistic regression was used to identify independent predictors of AKI.
Results: Among 102 patients, the median age was 80 years (IQR, 72– 84), and 46% were male. Klebsiella pneumoniae (44.9%) and Pseudomonas aeruginosa (20.4%) were the most common pathogens. Over half (52%) were exposed to concomitant nephrotoxic agents. Colistin-induced AKI occurred in 15 patients (14.7%). Chronic kidney disease was more frequent among those who developed AKI (73% vs. 26%, p< 0.001); however, no independent predictors were identified in multivariable analysis. In a sensitivity analysis using CKD as a binary covariate, CKD was independently associated with AKI (adjusted OR 19.17; 95% CI, 3.03– 121.30; p=0.002). Clinical failure occurred in 12.7% and microbiologic failure in 2.9% of patients.
Conclusion: In this cohort of patients with MDR-GNB UTIs, intravenous colistin was associated with favorable clinical and microbiological outcomes. The observed incidence of AKI was lower than previously reported in the literature, though this should be interpreted cautiously given the small number of events and the high prevalence of baseline renal impairment and nephrotoxic co-exposures. The infographic is divided into three sections: study population, treatment and outcomes. The study population section describes patients with multidrug-resistant gram-negative urinary tract infections, totaling 102 individuals. The median age is 80 years, with 33.3 percent having chronic kidney disease and 52.0 percent exposed to nephrotoxic agents. The treatment section details intravenous colistin, specifically colistimethate sodium (CMS). The median duration of treatment is 10 days, with a median loading dose of 4 mg per kg (range 2.5 to 5) and a median maintenance dose of 2.9 mg per kg per day (range 1.95 to 4.35). The outcomes section lists clinical failure at 12.7 percent, microbiological failure at 2.9 percent, culture negative results in 5 days, afebrile status in 1 day and colistin-induced acute kidney injury at 14.7 percent.Infographic on study population, treatment and outcomes of intravenous colistin for urinary tract infections.
Keywords: colistin, urinary tract infection, multidrug-resistant bacteria, acute kidney injury, nephrotoxicity
Introduction
Urinary tract infections (UTIs) remain among the most common bacterial infections worldwide, representing a substantial source of morbidity and healthcare costs, particularly in hospitalized and immunocompromised patients.1,2 In Saudi Arabia, Escherichia coli and Klebsiella pneumoniae continue to dominate as uropathogens, but the increasing prevalence of extended-spectrum β-lactamase (ESBL)-producing and carbapenem-resistant strains has rendered many first-line antibiotics ineffective.3,4
Recent surveillance data across the Kingdom have reported ESBL-producing E. coli in over one-third of urinary isolates, with an alarming rise in resistance to fluoroquinolones and cephalosporins.5 In addition, the global spread of multidrug-resistant (MDR) and carbapenem-resistant Enterobacterales (CRE), as well as Acinetobacter baumannii and Pseudomonas aeruginosa, has led to a critical shortage of effective therapeutic options, a challenge that is particularly pronounced in Saudi hospitals.6,7
In this context, colistin a polymyxin antibiotic discovered in the 1940s, has been reintroduced as one of the few remaining active agents against MDR Gram-negative pathogens.8 However, clinical data specifically addressing the use of colistin for urinary tract infections remain limited, as most evidence comes from studies on ventilator-associated pneumonia or bloodstream infections.9 Moreover, variations in colistin formulations, dosing strategies, and resistance mechanisms (including plasmid-mediated mcr genes) further complicate its clinical use and outcomes.10
Acute kidney injury (AKI) is the most clinically significant adverse effect of colistin therapy, with reported rates typically ranging from 30% to 70%.11–14 Although nephrotoxicity is often reversible, it is associated with prolonged hospitalization, increased need for renal replacement therapy, and limited future antibiotic options. However, most existing data are derived from mixed infection cohorts, and few studies have evaluated AKI specifically in patients treated for urinary tract infections, where lower systemic exposure may theoretically be sufficient.
In Saudi Arabia, colistin resistance among gram-negative organisms has been documented, yet data on treatment outcomes for colistin therapy in MDR UTIs remain scarce.15
Therefore, this study aims to describe the clinical outcomes, microbiological response, and nephrotoxicity associated with intravenous colistin therapy in patients with UTIs due to MDR gram-negative bacteria at a tertiary academic medical center in Riyadh, Saudi Arabia.
Methods
This single-center retrospective cohort study was conducted at King Abdulaziz Medical City, a 1501-bed tertiary academic medical center in Riyadh, Saudi Arabia. Adult patients aged ≥18 years who received at least two doses of intravenous colistin for the treatment of culture-confirmed urinary tract infections (UTIs) were included. UTIs were identified based on positive urine cultures with compatible clinical findings as documented by the treating physician. UTIs were classified as complicated cystitis, pyelonephritis, or uncomplicated cystitis based on documented clinical and microbiological criteria. Patients were excluded if colistin was prescribed for indications other than UTI, if medical records were incomplete, or if patients were discharged or died within 48 hours of initiating colistin therapy.
Data were extracted from the electronic medical record system and included patient demographics (age, sex, body weight, and body mass index), comorbid conditions including chronic kidney disease and baseline dialysis status, infection characteristics (UTI type and presence of bacteremia), and markers of illness severity such as septic shock, ICU admission, and mechanical ventilation at diagnosis. Baseline renal function was assessed using serum creatinine measured at the time of colistin initiation. The formulation used at our institution throughout the study period was sodium CMS, the inactive prodrug of colistin, which is converted in vivo to the active compound. At our institution, colistin dosing follows the standardized Ministry of National Guard Health Affairs (MNGHA) institutional guidelines (Supplementary Table S1). Colistin-related variables included receipt of a loading dose, loading and maintenance dosing expressed as mg/kg, and duration of therapy. Exposure to concomitant nephrotoxic agents during colistin therapy was also recorded, including furosemide, vancomycin, aminoglycosides, amphotericin B, and trimethoprim/sulfamethoxazole.
The primary outcome was colistin-induced AKI, defined as a new onset or worsening of renal dysfunction occurring during colistin therapy or by the end of treatment. AKI was defined as an increase in serum creatinine of ≥26 µmol/L from baseline, in accordance with the Acute Kidney Injury Network (AKIN) criteria, based on documented laboratory values and clinical assessment.16
Secondary outcomes included microbiological failure, clinical failure, and in-hospital mortality. Clinical failure was defined as persistence or worsening of presenting signs and symptoms, or death occurring during colistin therapy or within 4 days of treatment initiation. Microbiological failure was defined as persistent positive urine cultures for the same pathogen despite intravenous colistin therapy.
Statistical Analysis
Continuous variables were assessed for normality and are presented as median with interquartile range (IQR). Comparisons between patients with and without colistin-induced AKI were performed using the Wilcoxon rank-sum test for continuous variables and Fisher’s exact test for categorical variables.
Multivariable logistic regression was used to identify factors associated with colistin-induced AKI. Variables included in the multivariable model were selected a priori based on clinical relevance and included age, baseline serum creatinine, ICU admission, and colistin daily dose. Body weight was not included in the multivariable model due to its collinearity with weight-based colistin dosing. Similarly, chronic kidney disease was not included as a separate covariate, as baseline serum creatinine incorporated instead. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) are reported. A sensitivity analysis was performed excluding patients receiving dialysis to evaluate the robustness of the main findings. Missing data were handled by complete-case analysis. A two-sided p-value <0.05 was considered statistically significant. All analyses were performed using RStudio (version 2026.01.0, Build 392; Posit Software, PBC) with R statistical software version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline Characteristics
Baseline demographic and clinical characteristics are summarized in Table 1. A total of 102 adult patients who received intravenous colistin for culture-confirmed UTIs were included. The median age was 80 years (IQR, 72–84), and 47 patients (46.1%) were male. The median body weight was 65.3 kg (IQR, 48.9–75.8), with a median body mass index of 25.3 kg/m2 (IQR, 19.2–31.9). Baseline serum creatinine was 121 µmol/L (IQR, 58–195.5); chronic kidney disease was present in 34 patients (33.3%), including 9 patients (8.8%) receiving maintenance hemodialysis at baseline. Prior to colistin initiation, AKI was documented in 33 patients (32.4%) (Supplementary Table S1).
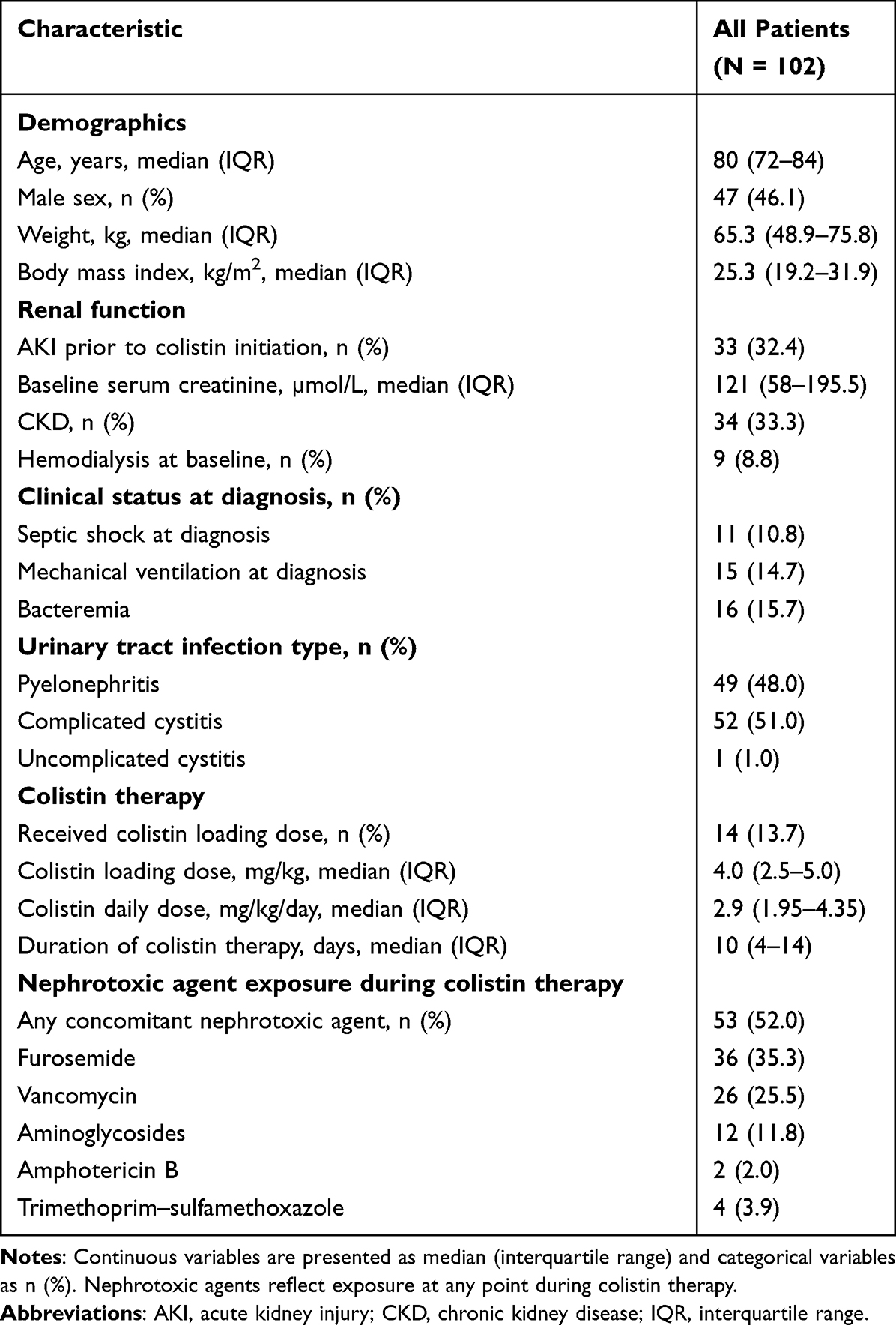 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients Treated with Colistin for Urinary Tract Infections |
Complicated cystitis (51.0%) and pyelonephritis (48.0%) were the most common UTI syndromes; only one patient (1.0%) had uncomplicated cystitis (Table 1). Bacteremia was documented in 16 patients (15.7%). Septic shock and mechanical ventilation at diagnosis were present in 11 (10.8%) and 15 (14.7%) patients, respectively. The median duration of colistin therapy was 10 days (IQR, 4–14). A loading dose was administered in 14 patients (13.7%), with a median loading dose of 4.0 mg/kg (IQR, 2.5–5.0) and a median daily dose of 2.9 mg/kg/day (IQR, 1.95–4.35). Prior to colistin initiation, 53 patients (52.0%) had received at least one systemic antibacterial agent, most commonly carbapenems (35.3%) and piperacillin–tazobactam (12.7%), while 49 patients (48.0%) had not received prior antibacterial therapy for the index infection. Concomitant nephrotoxic agents were used in 52.0% of patients, most commonly furosemide and vancomycin (Supplementary Table S2).
Clinical and Microbiologic Outcomes
Colistin-associated acute kidney injury occurred in 15 patients (14.7%) by the end of therapy. Clinical failure was observed in 13 patients (12.7%), while microbiological failure occurred in 3 patients (2.9%). In-hospital mortality was 13.7% (Table 2). Clinical response was generally rapid, with a median time to defervescence of 1 day (IQR, 1–2) and a median time to documented culture negativity of 5 days (IQR, 4–8). The median hospital length of stay was 19 days (IQR, 12–25).
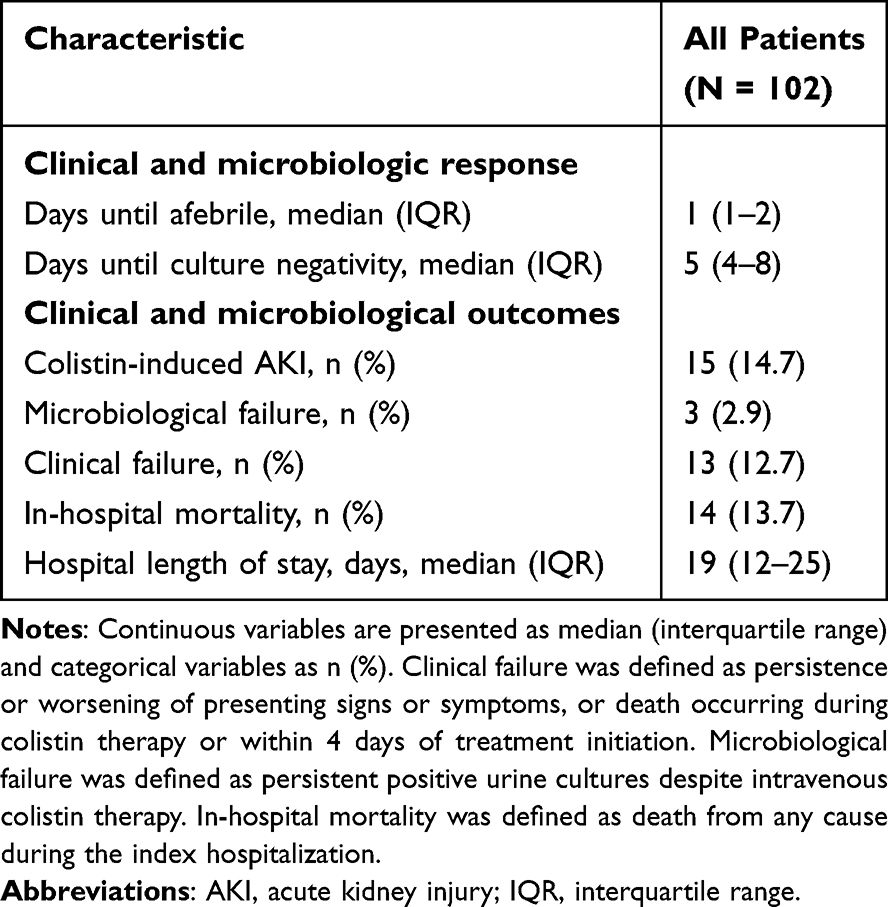 |
Table 2 Clinical Course and Outcomes Among Patients Treated with Colistin for Urinary Tract Infections |
Microbiology
Among the 98 urinary isolates identified, Klebsiella pneumoniae was the most frequently identified organism, accounting for 44.9% of isolates, followed by Pseudomonas aeruginosa (20.4%), Acinetobacter baumannii (13.3%), and Escherichia coli (10.2%). Other organisms were less common and were grouped as “Other” (Figure 1).
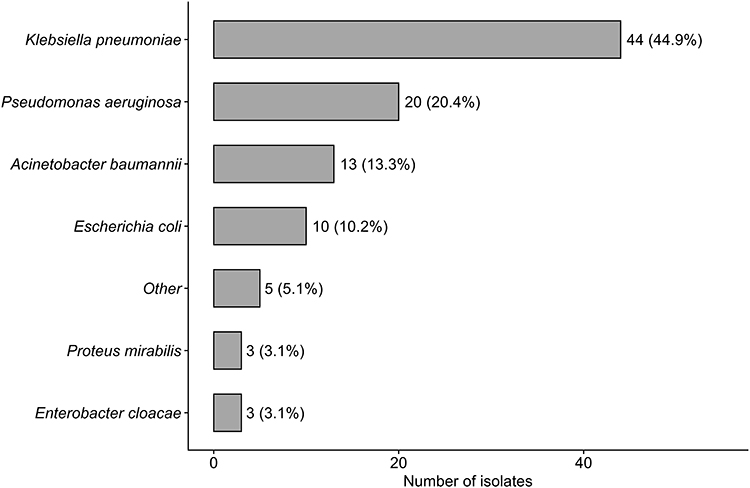 |
Figure 1 Distribution of organisms isolated from urine cultures among patients treated with colistin. Bars represent the number of isolates, with percentages shown in parentheses. Rare organisms were grouped as “Other”. |
Univariate Analysis of Factors Associated with Colistin-Induced AKI
In univariate analyses comparing patients with and without colistin-induced AKI (Table 3), patients who developed AKI had significantly higher body weight compared with those without AKI (median 74.8 kg vs 63.2 kg, p = 0.012). Chronic kidney disease was also significantly more frequent among patients who developed AKI (73% vs 26%, p < 0.001).
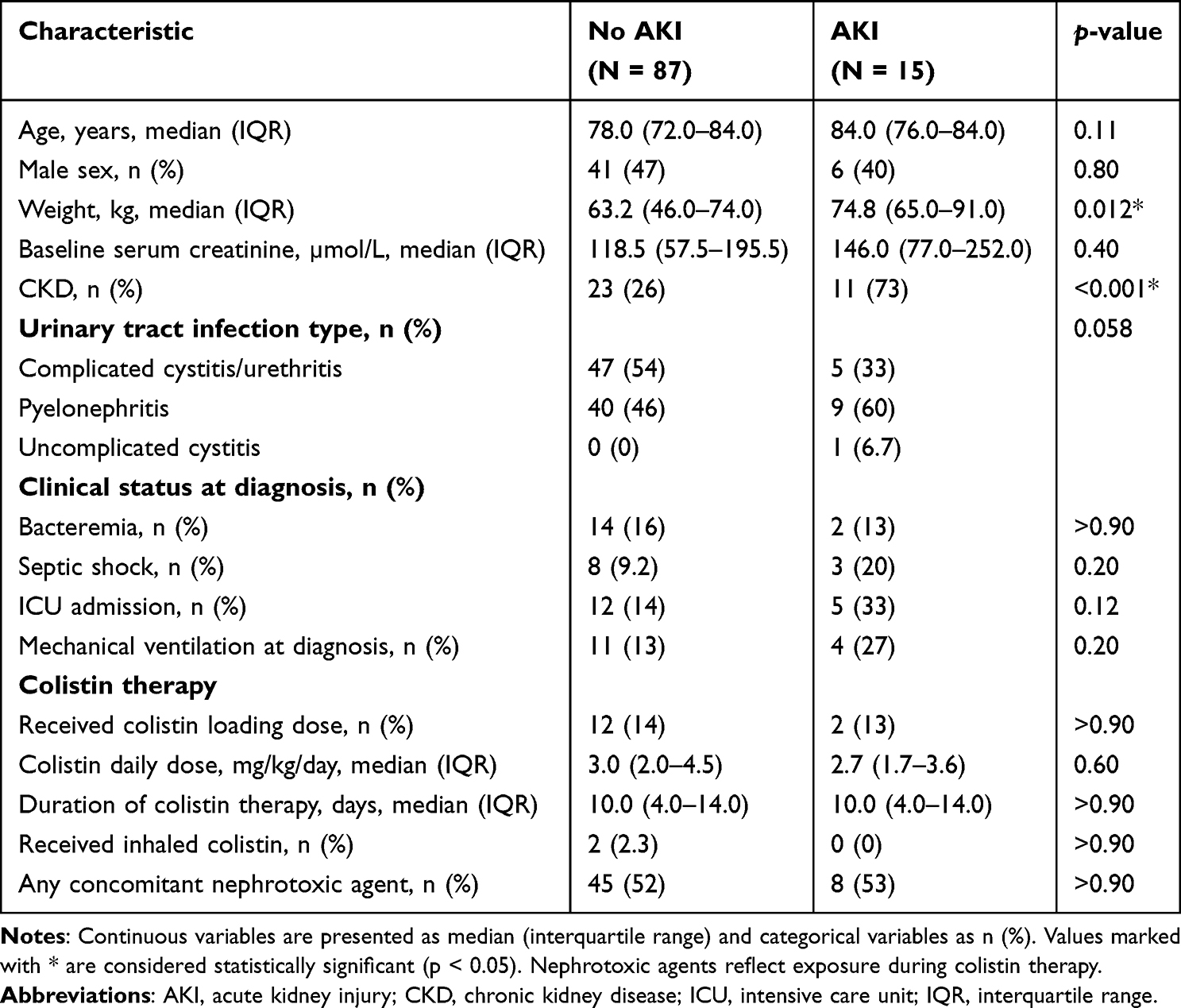 |
Table 3 Univariate Comparison of Patients with and without Colistin-Induced Acute Kidney Injury |
No statistically significant differences were observed between groups regarding other variables. A higher proportion of patients with AKI had pyelonephritis compared with those without AKI; however, this difference did not reach statistical significance (p = 0.058).
Multivariable Analysis
In multivariable logistic regression analysis adjusting for age, baseline serum creatinine, ICU admission, and colistin daily dose, no variable was independently associated with colistin-induced AKI (Supplementary Table S3). ICU admission showed a non-significant trend toward increased risk of AKI (adjusted OR 3.60; 95% CI, 0.93–13.37; p = 0.054), while colistin daily dose was not associated with AKI risk.
In a sensitivity analysis excluding patients receiving dialysis (n = 93), predictors of AKI remained consistent with the main model. ICU admission showed a trend toward higher AKI risk (OR 3.54, 95% CI 0.95–13.13, p = 0.06), while age, baseline creatinine, and daily colistin dose were not significantly associated with AKI (Supplementary Table S4). In a second sensitivity analysis substituting CKD as a binary covariate for baseline serum creatinine, CKD was independently associated with colistin-induced AKI (adjusted OR 19.17; 95% CI, 3.03–121.30; p=0.002), while ICU admission showed a similar non-significant trend (adjusted OR 4.18; 95% CI, 0.95–18.35; p=0.058) (Supplementary Table S5).
Discussion
In this single-center retrospective cohort of patients treated with intravenous colistin for culture-confirmed UTIs, most infections presented as pyelonephritis or complicated cystitis and were caused by MDR gram-negative bacteria, primarily K. pneumoniae. Most patients were on a relatively low maintenance dose of CMS. However, despite the high prevalence of baseline renal dysfunction in this population, the incidence of colistin-associated AKI was relatively low, at approximately 15%.
The observed AKI incidence in our study was notably lower than the 30–70% range commonly reported in the literature. However, most existing data are derived from critically ill populations treated for pneumonia or bloodstream infections, where higher colistin doses, greater illness severity, and longer treatment durations likely contribute to higher nephrotoxicity rate.11,12,14,17 For instance, Hartzell et al reported a 45% incidence among patients receiving colistimethate sodium,11 while AKI occurred in 53–60% of critically ill patients.12 The rate reached as high as 70% in the Paraguayan cohort.17 Even in studies using optimized dosing strategies, nephrotoxicity was reported in over 50% of ICU patients.14
Colistin-associated nephrotoxicity is well described and is primarily attributed to its direct tubular toxicity, leading to acute tubular necrosis and subsequent rise in serum creatinine and reduction in creatinine clearance. The risk of nephrotoxicity is influenced by colistin exposure, concomitant nephrotoxic agents, and patient related factors such as advanced age, hypoalbuminemia, hyperbilirubinemia, and illness severity.18 In the present study, ICU admission demonstrated a trend toward increased risk of AKI, suggesting that critical illness and hemodynamic instability may play a more prominent role than colistin exposure alone.
CKD was strongly associated with AKI in univariate analysis (p <0.001); however, this association did not emerge as an independent predictor in the multivariate model. This likely reflects collinearity with baseline serum creatinine, which already captures underlying renal function. To further explore this relationship, we performed a sensitivity analysis including CKD in the multivariable model. CKD was not independently associated with AKI, and its inclusion did not meaningfully change the overall findings. Furthermore, the limited number of AKI events (n=15) relative to the covariates in the model may have reduced the model’s ability to detect independent associations. These findings are consistent with prior literature suggesting that patient-related factors, particularly critical illness and concurrent nephrotoxic exposures, contribute more substantially to the development of colistin-associated nephrotoxicity than colistin dosing alone.19–22
In our study, colistin was administered as CMS, the inactive prodrug of colistin and the formulation available in our institution. Although CMS has been linked to higher risk of nephrotoxicity compared with the active colistin sulfate formulation, this risk is influenced by renal dose adjustment, cumulative exposure, and duration of therapy. In our cohort, the median daily colistin dose was 2.9 mg/kg/day and the median treatment duration was 10 days, suggesting a relatively controlled exposure. This dose was lower than those reported in several cohorts with higher nephrotoxicity rates, including DeRyke et al, in which patients received a mean daily dose of 5.1 mg/kg/day and nephrotoxicity occurred in 33% of patients,23 and Shields et al, in which the median daily dose was 3.45 mg/kg/day and doses >5 mg/kg/day were independently associated with AKI within 7 days.24 Similarly, Dalfino et al reported AKI in 44% of severely ill patients receiving a median daily CMS dose of 9 million IU.25 Careful CMS dosing according to renal function and avoidance of unnecessary prolonged exposure may help mitigate nephrotoxicity risk.26
Colistin efficacy in UTIs can be explained by its renal elimination and high urinary exposure. CMS is administered intravenously and is predominantly cleared by the kidneys, where it is converted to active colistin within the urinary tract. In UTI-specific populations, CMS undergoes extensive renal excretion and achieves urinary concentrations that far exceed plasma levels, potentially allowing for clinical efficacy at lower systemic exposures. This pharmacokinetic advantage, combined with the lower illness acuity in our UTI cohort compared with VAP or BSI populations, may partially account for the lower AKI rate.27 Nonetheless, this finding should be interpreted with caution, as over half of our patients (52%) were exposed to concomitant nephrotoxic agents and a substantial proportion had pre-existing CKD, both of which would be expected to increase AKI risk. Conservative institutional dosing practices and close renal monitoring may have further mitigated nephrotoxicity.2,19–21
Previous clinical studies evaluating CMS for UTIs have reported clinical cure rates ranging from 50% to 92%.28–30 In our cohort, clinical failure occurred in 12.9% of patients, which is lower than rates reported in earlier studies, such as Cheng et al, who observed 27% failure among patients with severe MDR infections.30 Microbiological failure was documented in only three patients (2.9%), although this likely underestimates true rates due to the absence of routine post-treatment urine cultures in some cases. The clinical success observed in our cohort demonstrates the effectiveness of colistin for severe MDR-GNB infections, including Pseudomonas aeruginosa and Klebsiella pneumoniae.30
Several new β-lactam/β-lactamase inhibitor combinations including ceftolozane-tazobactam, ceftazidime-avibactam, and cefiderocol have shown promising efficacy and better safety profiles compared to colistin.31 However, resistance to ceftolozane-tazobactam and ceftazidime-avibactam has been documented during treatment,20,32–34 indicating that polymyxins remain necessary as part of the antimicrobial options against MDR pathogens. This challenge extends beyond adult populations, as rising rates of ESBL-producing uropathogens have also been reported in pediatric and infantile UTIs, where treatment options are even more constrained.35 Overall, most patients treated with colistin for MDR-GNB UTIs achieved favorable outcomes. The high clinical response rate, combined with manageable nephrotoxicity, highlights the clinical role of colistin as a salvage therapy when newer agents are unavailable or contraindicated.
The strengths of this study include a relatively large single-center sample, which provides a valuable real-world perspective on the safety and efficacy of colistin in MDR-GNB UTIs. Despite this, several limitations must be acknowledged: its retrospective design, small number of AKI events which limits the statistical power of the multivariable analysis, lack of minimum inhibitory concentration (MIC) data, and the high prevalence of baseline renal impairment and concomitant nephrotoxic exposure which may confound the observed AKI incidence.
In conclusion, colistin therapy for MDR-GNB UTIs was associated with favorable clinical and microbiological outcomes and a lower-than-expected incidence of nephrotoxicity in our cohort. While the low AKI rate observed may reflect the pharmacokinetic advantage of colistin in the urinary tract and conservative institutional dosing, the small sample size and limited number of AKI events preclude definitive conclusions regarding optimal dosing strategies. Colistin should be used with caution, particularly in patients with chronic kidney disease or septic shock, and always with close renal monitoring. Although newer agents offer safer alternatives, colistin continues to play an important role in managing infections caused by resistant Gram-negative bacteria, especially in resource-limited settings or when novel agents fail.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. The study protocol was reviewed and approved by the Institutional Review Board of King Abdullah International Medical Research Center (KAIMRC), Riyadh, Saudi Arabia (Study Number NRC21R/071/03). All data were de-identified prior to analysis and handled in accordance with institutional ethical standards to ensure patient confidentiality. Given the retrospective nature of the study and the use of de-identified data, the requirement for informed consent was waived by the Institutional Review Board.
Consent for Publication
Not applicable. This study did not include identifiable individual data.
Acknowledgments
This original research was accepted for presentation at the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Global Congress 2024, held in Barcelona, Spain (April 27–30, 2024). The study was presented as a Poster (Abstract P1069) titled “Unmasking colistin therapy for urinary tract infections due to MDR bacteria: experience at a tertiary academic medical center”, during the session “Community-acquired abdominal/gastrointestinal, urinary tract & genital infections (including epidemiology, clinical, imaging, treatment & prevention).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J Med. 2002;113(Suppl:1):5–10. doi:10.1016/S0002-9343(02)01054-9
2. Medina M, Castillo-Pino E. An introduction to the epidemiology and burden of urinary tract infections. Ther Adv Urol. 2019;11:1756287219832172. doi:10.1177/1756287219832172
3. Abalkhail A, AlYami AS, Alrashedi SF, et al. The prevalence of multidrug-resistant Escherichia coli producing ESBL among patients with urinary tract infections in Riyadh, Saudi Arabia. Healthcare. 2022;10(9):1778. doi:10.3390/healthcare10091778
4. Alameer KM, Abuageelah BM, Alharbi RH, et al. Retrospective analysis of antibiotic resistance patterns of uropathogenic Escherichia coli with focus on extended-spectrum β -lactamase at a tertiary Central hospital in Saudi Arabia. Health Sci Rep. 2025;8(1). doi:10.1002/hsr2.70378
5. Alzahrani M, Ali M, Anwar S. Bacteria causing urinary tract infections and its antibiotic susceptibility pattern at a tertiary hospital in Al-Baha region, Saudi Arabia. J Pharm Bioallied Sci. 2020;12(4):449–456. doi:10.4103/jpbs.jpbs_294_19
6. Raees F, Harun A, Ahmed A, Deris Z. Antibiotic resistance, genotype and clinical significance of Acinetobacter baumannii in Saudi Arabia. Bangladesh J Med Sci. 2022;21(2):233–242. doi:10.3329/bjms.v21i2.58054
7. Aldarhami A, Elrggal ME, Alzaylaee RA, et al. Patterns of resistance among critically ill patients at a tertiary hospital, Saudi Arabia: a retrospective cohort study. Medicine. 2025;104(41):e45159. doi:10.1097/MD.0000000000045159
8. Falagas ME, Kasiakou SK, Saravolatz LD. Colistin: the revival of polymyxins for the management of multidrug-resistant gram-negative bacterial infections. Clinl Infect Dis. 2005;40(9):1333–1341. doi:10.1086/429323
9. Almangour TA, Alenazi B, Ghonem L, Alhifany AA, Aldakheel BA, Alruwaili A. Inhaled colistin for nosocomial pneumonia due to MDR gram-negative bacteria: real-life experience in Saudi Arabia. Saudi Pharm J. 2020;28(8):1009–1013. doi:10.1016/j.jsps.2020.06.023
10. Rahimi S, Bakht M, Farshadzadeh Z, Nikkhahi F. A review of colistin-resistant Escherichia coli isolates in the Middle East. Arch Razi Inst. 2023;79:13–27. doi:10.32592/ari.2024.79.1.13
11. Hartzell JD, Neff R, Ake J, et al. Nephrotoxicity associated with intravenous colistin (Colistimethate Sodium) treatment at a tertiary care medical center. Clin Infect Dis. 2009;48(12):1724–1728. doi:10.1086/599225
12. Spapen H, Jacobs R, Van Gorp V, Troubleyn J, Honoré PM. Renal and neurological side effects of colistin in critically ill patients. Ann Intensive Care. 2011;1(1):14. doi:10.1186/2110-5820-1-14
13. Akajagbor DS, Wilson SL, Shere-Wolfe KD, Dakum P, Charurat ME, Gilliam BL. Higher incidence of acute kidney injury with intravenous colistimethate sodium compared with polymyxin B in critically Ill patients at a tertiary care medical center. Clinl Infect Dis. 2013;57(9):1300–1303. doi:10.1093/cid/cit453
14. Ozel AS, Ergönül Ö, Korten V. Colistin nephrotoxicity in critically ill patients after implementation of a new dosing strategy. J Infect Dev Ctries. 2019;13(10):877–885. doi:10.3855/jidc.11413
15. Faidah H. Colistin use and its resistance in Kingdom of Saudi Arabia: a narrative review. Adv Infect Dis. 2018;8(04):255–261. doi:10.4236/aid.2018.84021
16. Mehta RL, Kellum JA, Shah SV, et al. Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31. doi:10.1186/cc5713
17. Martínez Gómez LP, Ortega Filártiga E. Prevalence of acute renal injury in patients treated with colistin. Rev Virtual Soc Parag Med Int. 2018;5(2):45–52. doi:10.18004/rvspmi/2312-3893/2018.05(02)45-052
18. Ordooei Javan A, Shokouhi S, Sahraei Z. A review on colistin nephrotoxicity. Eur J Clin Pharmacol. 2015;71(7):801–810. doi:10.1007/s00228-015-1865-4
19. Saint S, Kowalski CP, Kaufman SR, et al. Preventing hospital-acquired urinary tract infection in the United States: a national study. Clinl Infect Dis. 2008;46(2):243–250. doi:10.1086/524662
20. Alanazi MQ, Al-Jeraisy MI, Salam M. Prevalence and predictors of antibiotic prescription errors in an emergency department, Central Saudi Arabia. Drug Healthc Patient Saf. 2015;7:103–111. doi:10.2147/DHPS.S83770
21. World Health Organization. The world health report 2007: a safer future: global public health security in the 21st century [Rapport sur la santé dans Le Monde 2007: un avenir plus sûr: la sécurité sanitaire mondiale au XXIè siècle]. 2007.
22. Newton-Foot M, Snyman Y, Maloba MRB, Whitelaw AC. Plasmid-mediated mcr-1 colistin resistance in Escherichia coli and Klebsiella spp. clinical isolates from the Western Cape region of South Africa. Antimicrob Resist Infect Control. 2017;6(1):78. doi:10.1186/s13756-017-0234-8
23. Deryke CA, Crawford AJ, Uddin N, Wallace MR. Colistin dosing and nephrotoxicity in a large community teaching hospital. Antimicrob Agents Chemother. 2010;54(10):4503–4505. doi:10.1128/AAC.01707-09
24. Shields RK, Anand R, Clarke LG, et al. Defining the incidence and risk factors of colistin-induced acute kidney injury by KDIGO criteria. PLoS One. 2017;12(3):e0173286. doi:10.1371/journal.pone.0173286
25. Dalfino L, Puntillo F, Ondok MJM, et al. Colistin-associated acute kidney injury in severely Ill patients: a step toward a better renal care? A prospective cohort study. Clin Infect Dis. 2015;61(12):1771–1777. doi:10.1093/cid/civ717
26. Almutairy R, Aljrarri W, Noor A, et al. Impact of colistin dosing on the incidence of nephrotoxicity in a tertiary care hospital in Saudi Arabia. Antibiotics. 2020;9(8):485. doi:10.3390/antibiotics9080485
27. Luque S, Escaño C, Sorli L, et al. Urinary concentrations of colistimethate and formed colistin after intravenous administration in patients with multidrug-resistant gram-negative bacterial infections. Antimicrob Agents Chemother. 2017;61(8):e02595–16. doi:10.1128/AAC.02595-16
28. Zaidi STR, Al Omran S, Al Aithan ASM, Al Sultan M. Efficacy and safety of low-dose colistin in the treatment for infections caused by multidrug-resistant gram-negative bacteria. J Clin Pharm Ther. 2014;39(3):272–276. doi:10.1111/jcpt.12138
29. Chen -J-J, Kuo G, Hung -C-C, et al. Risk factors and prognosis assessment for acute kidney injury: the 2020 consensus of the Taiwan AKI task force. JFormos Med Assoc. 2021;120(7):1424–1433. doi:10.1016/j.jfma.2021.02.013
30. Montero M, Horcajada JP, Sorlí L, et al. Effectiveness and safety of colistin for the treatment of multidrug-resistant Pseudomonas aeruginosa infections. Infection. 2009;37(5):461–465. doi:10.1007/s15010-009-8342-x
31. Van Duin D, Lok JJ, Earley M, et al. Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clinl Infect Dis. 2018;66(2):163–171. doi:10.1093/cid/cix783
32. Haidar G, Philips NJ, Shields RK, et al. Ceftolozane-Tazobactam for the treatment of multidrug-resistant Pseudomonas aeruginosa infections: clinical effectiveness and evolution of resistance. Clinl Infect Dis. 2017;65(1):110–120. doi:10.1093/cid/cix182
33. Bassetti M, Castaldo N, Cattelan A, et al. Ceftolozane/tazobactam for the treatment of serious Pseudomonas aeruginosa infections: a multicentre nationwide clinical experience. Int J Antimicrob Agents. 2019;53(4):408–415. doi:10.1016/j.ijantimicag.2018.11.001
34. Humphries RM, Hemarajata P. Resistance to ceftazidime-avibactam in Klebsiella pneumoniae due to porin mutations and the increased expression of KPC-3. Antimicrob Agents Chemother. 2017;61(6):e00537–17. doi:10.1128/AAC.00537-17
35. Wong SW, Tullus K, Chan YHE. Controversies in treating febrile infantile urinary tract infection caused by extended-spectrum beta-lactamase producing Enterobacteriaceae: an international multi-centre survey. Pediatr Nephrol. 2025;40(7):2253–2266. doi:10.1007/s00467-025-06700-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comprehensive Assessment of Colistin Induced Nephrotoxicity: Incidence, Risk Factors and Time Course
Rabi R, Enaya A, Sweileh MW, Aiesh BM, Namrouti A, Hamdan ZI, Abugaber D, Nazzal Z
Infection and Drug Resistance 2023, 16:3007-3017
Published Date: 15 May 2023
Factors Associated with Successful Treatment of Carbapenem-Resistant Gram-Negative Bacilli Infections Using Intravenous Colistin Sulfate in China: A Real-World Retrospective Study
Gao W, Li W, Liu H, Xu D, Tian L, Zhang J, Liu D, He Y
Infection and Drug Resistance 2025, 18:2175-2185
Published Date: 30 April 2025
From Initiation to Recovery: A Longitudinal Analysis of Polymyxin B-Induced Kidney Injury in Clinical Practice
Zhang GX, Zhang MR, Qu Q, Yi SM, Zhang YT, Wang YM, Qu J
Drug Design, Development and Therapy 2026, 20:613715
Published Date: 9 July 2026