Back to Journals » Clinical Epidemiology » Volume 15
Cohort Profile: Better Health in Late Life
Authors Sørensen HT ![]() , Christensen T
, Christensen T ![]() , Bøtker HE
, Bøtker HE ![]() , Christiansen CF
, Christiansen CF ![]() , Fuglsang CH
, Fuglsang CH ![]() , Gribsholt SB, Kristensen FPB
, Gribsholt SB, Kristensen FPB ![]() , Laugesen K
, Laugesen K ![]() , Laursen ASD, Nørgaard M
, Laursen ASD, Nørgaard M ![]() , Schmidt M
, Schmidt M ![]() , Skajaa N
, Skajaa N ![]() , Troelsen FS
, Troelsen FS ![]() , Pedersen L
, Pedersen L
Received 12 September 2023
Accepted for publication 5 December 2023
Published 20 December 2023 Volume 2023:15 Pages 1227—1239
DOI https://doi.org/10.2147/CLEP.S436617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Laura Horsfall
Henrik Toft Sørensen,1 Tina Christensen,1 Hans Erik Bøtker,2 Christian Fynbo Christiansen,1 Cecilia H Fuglsang,1 Sigrid B Gribsholt,1 Frederik Pagh Bredahl Kristensen,1 Kristina Laugesen,1 Anne Sofie D Laursen,1 Mette Nørgaard,1 Morten Schmidt,1 Nils Skajaa,1 Frederikke S Troelsen,1 Lars Pedersen1
1Department of Clinical Epidemiology, Aarhus University Hospital and Aarhus University, Aarhus, Denmark; 2Department of Clinical Medicine, Aarhus University, Aarhus, Denmark
Correspondence: Henrik Toft Sørensen, Department of Clinical Epidemiology, Aarhus University Hospital and Aarhus University, Olof Palmes Allé 43-45, Aarhus, 8200, Denmark, Tel +45 87 16 82 15, Email [email protected]
Purpose: Humans are living longer and may develop multiple chronic diseases in later life. The Better Health in Late Life cohort study aims to improve our understanding of the risks and outcomes of multimorbidity in the Danish population.
Methods: A randomly-selected sample of Danish residents who were 50– 65 years of age received a questionnaire and an invitation to participate in this study. Respondents completed an online survey between October 2021 and January 2022 which addressed topics that included self-assessed health, mental health, sleep, specific medical conditions, use of painkillers, diet, alcohol consumption, smoking, physical activity, and body composition. This information was linked to the Danish health and social registries (some established in 1943 and onwards) that maintain data on filled prescriptions, hospital records, socioeconomic status, and health care utilization.
Results: Responses were received from 115,431 of the 301,244 residents invited to participate (38%). We excluded respondents who answered none of the questions as well as those who provided no information on sex or indicated an age other than 50– 65 years. Of the 114,283 eligible respondents, 54.8% were female, 30.3% were overweight, and 16.7% were obese. Most participants reported a weekly alcohol consumption of less than seven units and 13.3% were current smokers; 5.2% had a history of hospitalization for solid cancer, and 3.0%, 2.3%, 2.0%, and 0.9% reported chronic pulmonary disease, diabetes, stroke, and myocardial infarction, respectively. The most frequently filled prescriptions were for medications used to treat the nervous system and cardiovascular diseases (38.1% and 37.4%, respectively).
Keywords: aging, epidemiology, health registries, life course epidemiology, multimorbidity, prospective cohort
Introduction
During the past 200 years, the average human life expectancy in many developed countries has doubled.1 Better health experienced by people of all ages is largely the result of public health measures, including improved standards of living, the availability of vaccinations, and improved medical care.1–3 One immediate challenge facing health care systems in countries such as Denmark is the need to care for an aging population while under significant pressure to encompass costs. The proportion of people aged 65 years or more in Europe is expected to increase from 16% in 2012 to 27% by the year 2050.4 Given the recent improvements in the diagnosis and treatment of chronic disease, the threshold for initiating preventive treatment of asymptomatic conditions has been reduced. However, as per the World Health Organization, the five-year increase in life expectancy among those who were 65 years of age or older between 2000 and 2015 included only 4.6 years of healthy life.5 In other words, 16–20% of one’s later life may be spent coping with disease.6
Population aging is transforming clinical medicine in several ways. The observed demographic transformation has been accompanied by an epidemiological transition. Chronic diseases, such as cardiovascular disease, cancer, chronic pulmonary disease, diabetes, and mental disorders are now among the major causes of death and contributors to disease and disability in later life.7 Age is a strong predictor of developing these chronic diseases, and a substantial fraction of the population may ultimately develop multiple chronic diseases. Such multimorbidity has been defined as the coexistence of two or more chronic conditions in a single individual.8 Multimorbidity is associated with poor physical and psychological outcomes and impaired quality of life9–14 and thus poses a critical challenge for those providing medical care and the health care system as a whole.8 As we prepare for the future, we will need to have a much better understanding of the interactions and relationships among these chronic diseases. Of note, patients presenting with multimorbidity are often excluded from randomized clinical trials and epidemiological studies, because most studies seek to maximize their internal validity.15 Moreover, polypharmacy is prevalent among patients who have been diagnosed with chronic diseases. Some reports have estimated that polypharmacy may be responsible for as many as 30% of hospital admissions among older patients.16–18
Multimorbidity and polypharmacy are therefore among the greatest challenges to health in older age and the modern health care system as a whole.19 Importantly, multimorbidity has been associated with socioeconomic deprivation because many of these patients develop contemporary difficulties with both physical and psychological health. Most clinical guidelines focus on treatments against single conditions and only rarely consider the impact of multimorbidity in their decision pathways.20,21
Denmark maintains an extensive network of health and social registries which together represent one of the best sources of population-based data available for global aging research.22 However, at this time, these registries do not provide data on disease symptoms nor any insight into lifestyle factors such as smoking, diet, or exercise. To address this issue, the “Better Health in Late Life” cohort was created to add self-reported data that focuses on such factors and combine questionnaire-based information with information already available from Danish population-based registries. These registries maintain information on birth, employment, other social factors, health, morbidity, and mortality among residents of Denmark for the past 50 years.23–25 This cohort aims to improve our understanding of the risks and outcomes of multimorbidity in the Danish population among those currently at 50–65 years of age.
Because the majority of risk factors that account for approximately 37 million annual deaths worldwide from the most common chronic diseases, ie cardiovascular disease, cancer, chronic pulmonary disease, diabetes, and mental disorders, are potentially modifiable, an improved understanding of the interaction between risk factors, multimorbidity and polypharmacy has a huge potential for preventive medicine.26 The aim of this publication is to provide the background and the approach for establishing The Better Health in Late Life cohort study and to present the cohort characteristics so that it can be a vital reference for researchers accessing the cohort to improve our understanding of the risks and outcomes of multimorbidity in the Danish population. In this paper, we thus describe how the cohort was assembled, present baseline data, and outline the potential for future research.
Materials and Methods
Setting
The Better Health in Late Life population cohort was developed from respondents to an online questionnaire survey that was conducted in Denmark in late 2021 through early 2022. At that time, the total population in Denmark was 5.6 million residents, of whom 1.2 million (21%) were 50–65 years of age. The National Health Service in Denmark provides tax-supported health care to all residents.25 All residents are assigned a unique 10-digit civil registration (CPR) number by the Danish Civil Registration System.27 The CPR number is used across all registries and facilitates unambiguous linkage of individual-level data both to and between all social and health registries. The Danish Civil Registration System is updated daily and includes nationwide data on address of residence, mortality, and migration for all Danish residents since 1968.27
The Questionnaire
Developing the Questionnaire
We developed a comprehensive online questionnaire focused on lifestyle, health, and well-being that could be completed using any type of electronic device (ie, desktop or laptop computers, tablets, or mobile phones). The main topics in the questionnaire focused on self-assessed health, mental health, sleep, specific medical conditions, use of painkillers, diet, alcohol consumption, smoking, physical activity, and body composition (Table 1). Some topics were addressed using previously validated questionnaires (Supplementary Table 1). For example, self-assessed health was evaluated using the 12-item short-form health survey known as SF12v2 (Quality Metric Incorporated, license no. QM053156). We used the Major Depression Inventory28 and the Perceived Stress Scale29 to measure depression and stress, respectively.
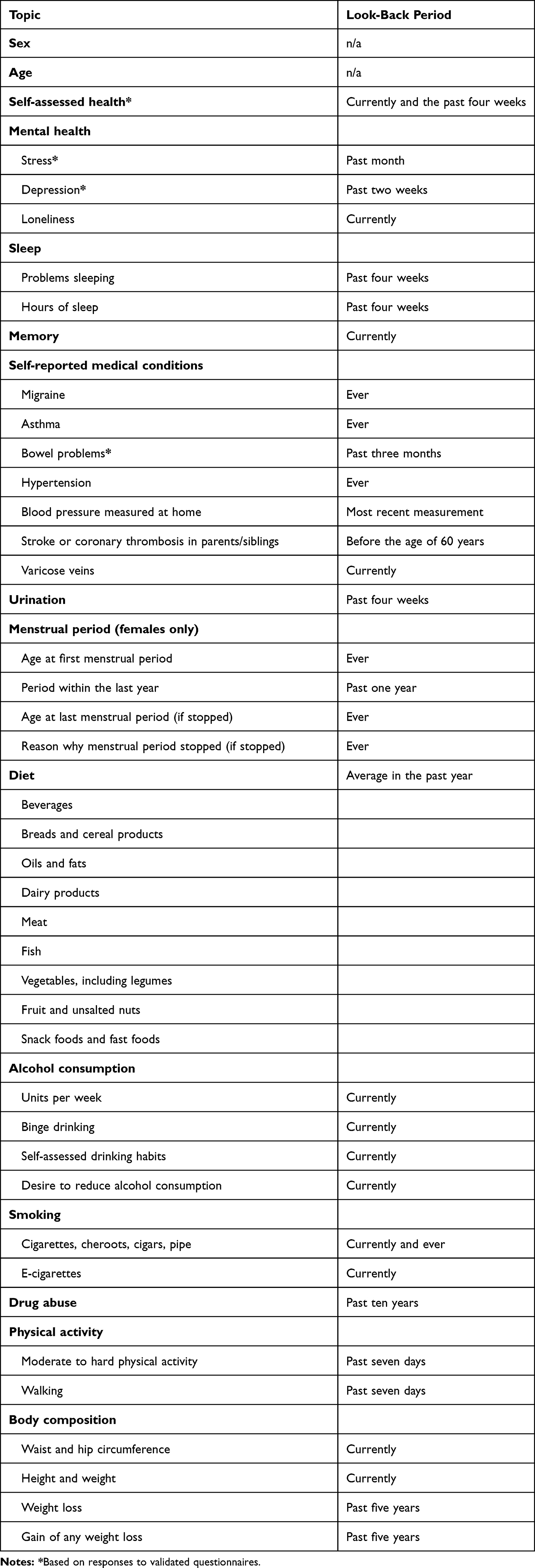 |
Table 1 Contents of the Better Health in Late Life Questionnaire |
Pilot Test of the Questionnaire
The questionnaire was initially pilot-tested among 1000 people who were 50–65 years of age. The pilot test included a qualitative follow-up that analyzed both written comments provided by respondents and telephone interviews with 14 of the participants who completed the entire questionnaire, seven respondents who completed only part of the questionnaire, and nine non-respondents. The questionnaire was subsequently modified and the number of questions was reduced.
Recruitment and Data Collection
Data were collected by DST Survey, Statistics Denmark, on behalf of Aarhus University from October 2021 through January 2022. An invitation to fill out the questionnaire was sent to 301,244 randomly selected Danish residents who were 50–65 years of age, which corresponds to 25% of the total target population of 1,222,220 Danish residents within this age group at that time. Invitations were sent through e-Boks, which is a secure digital mailing system introduced by the Danish Government in 2014 to enhance communication between public institutions and residents. All residents aged 15 years or older are required to use e-Boks, unless granted an exemption, which identifies individuals by their CPR number.30 The invitation letter included a hyperlink to the online survey as well as a unique log-in code that was linked to the individual’s CPR number. A hyperlink to a website with more information about the project was also provided.31
To submit the questionnaire, the participant had to click through to the last page and either check “No further comments” or write some text in the box provided. Apart from that, the questionnaire included no mandatory questions. Reminders were sent two and four weeks after the initial invitation to those who had not yet responded. Individuals who began the questionnaire but had not submitted it received as many as three reminders encouraging them to log in and complete the questionnaire.
The participants provided informed consent through Statistics Denmark by accepting the following:
We treat your answers confidentially and use results in a way that no one can see the replies of individual participants. Your answers cannot be linked to you and the collected data will be used for statistical and scientific purposes only. Participation is voluntary, but the study will be better, if many people participate. Your link to participation should not be handed to someone else. If you have any questions, please contact Statistics Denmark by email […] or phone. […]
Record Linkage to the Danish Health and Social Registries
Using their CPR numbers, we linked individual respondents in this cohort to information in several health and social registries. This facilitates the use of cohort data in studies designed to improve our understanding of the impact of lifestyle on health and multimorbidity. The cohort dataset was linked to the Danish National Patient Registry (DNPR), which contains records of all inpatient hospitalizations since 1978 and all outpatient clinic and emergency room visits since 1995.24 Each record contains the CPR number, one primary and up to 19 secondary diagnoses, procedures, and selected treatments, and date and type of contact (ie, inpatient, outpatient, emergency room visit). Diagnoses were recorded according to the World Health Organization’s International Classification of Diseases, Eighth Revision, until 1994 and according to the Tenth Revision (ICD-10) thereafter.24 We also linked the cohort to the Danish National Prescription Database (DNPD), which lists medications sold at pharmacies and in retail stores as well as medications sold to Danish hospitals.32 The DNPD was established in 1994 and is considered complete from 1997 onwards.32 Individual prescriptions issued by general practitioners, private practicing specialists, and hospital outpatient clinics were recorded, although not medications used to treat hospitalized patients.33 In addition to the DNPR and the DNPD, the cohort was linked to the Danish Cancer Registry,34 the Laboratory Information Systems,35 the Psychiatric Central Research Registry,36 the Educational Attainment Register,37 the Integrated Database for Labor Market Research,38 the National Health Insurance Service Registry,39 the National Pathology Registry,40 and the Registry of Causes of Death41 (Figure 1). A description of each of these registries is available in Supplementary Table 2. Data are stored on a secure server maintained by Statistics Denmark and all personal information in the survey has been de-identified.
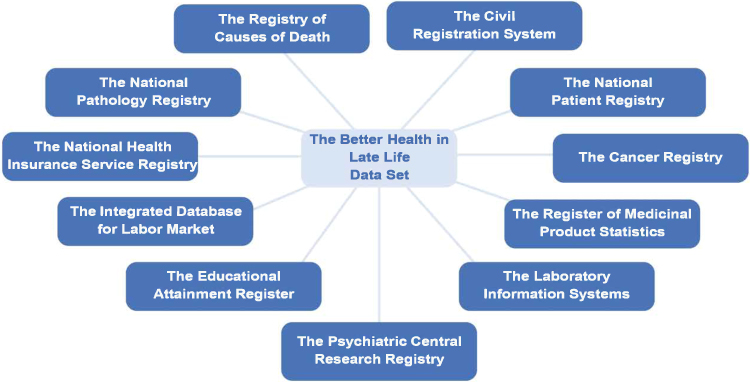 |
Figure 1 The cohort and linked registries. |
Results
Cohort Characteristics
Of the original 301,244 individuals who were invited to participate, 115,431 responded, yielding a response rate of 38.3%. Some respondents were identified as “straightliners”; these were individuals who logged in, clicked through the entire questionnaire, and then clicked “No comments” or wrote a comment at the end to submit the questionnaire, but without answering any questions. These individuals were excluded (n=876). We also excluded respondents who stated that they were less than 50 or more than 65 years of age (n=205) as well as those who did not respond to the question on sex (n=67). Thus, our final study cohort included 114,283 eligible respondents (Figure 2). Among respondents, 96,423 answered all questions (32.0% of those invited). These individuals spent an average of 33 minutes on this task.
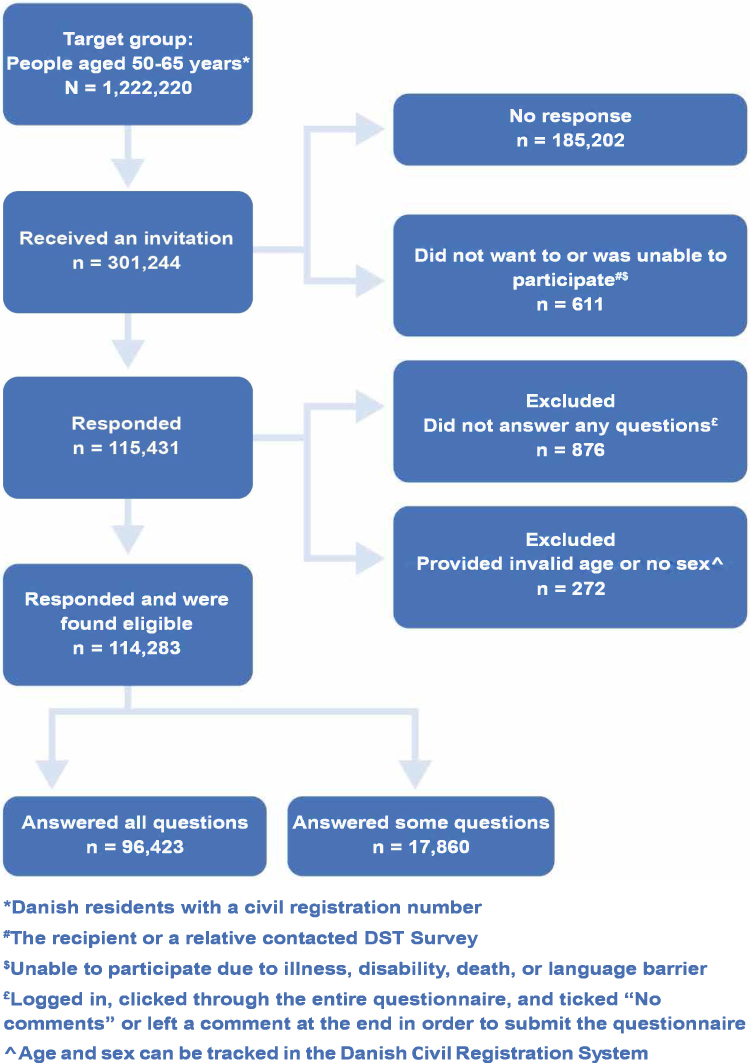 |
Figure 2 Flowchart. |
Demographics
We divided the respondents into four age categories and found that the likelihood of filling out the questionnaire was associated with age. The response rates for individuals who were 50–53, 54–57, 58–61, and 62–65 years of age were 27.0%, 30.2%, 33.9%, and 38.0%, respectively (Supplementary Table 3). As expected, a larger proportion of the invitees who reported higher education (41.3%) responded compared to those who reported that their highest level of education was primary school (20.3%). Likewise, women, persons without children, Danish as ethnic origin and high income were overrepresented in the survey. We identified no variation in the response rates across regions of residence (Supplementary Table 3).
Lifestyle and Health-Related Factors
Self-reported BMI data revealed that 0.7% of respondents were underweight (BMI <18.5 kg/m2), 30.9% were normal weight (BMI from 18.5 to <25 kg/m2), 30.3% were overweight (BMI from 25 to <30 kg/m2), and 16.7% were obese (BMI ≥30 kg/m2) (Table 2).
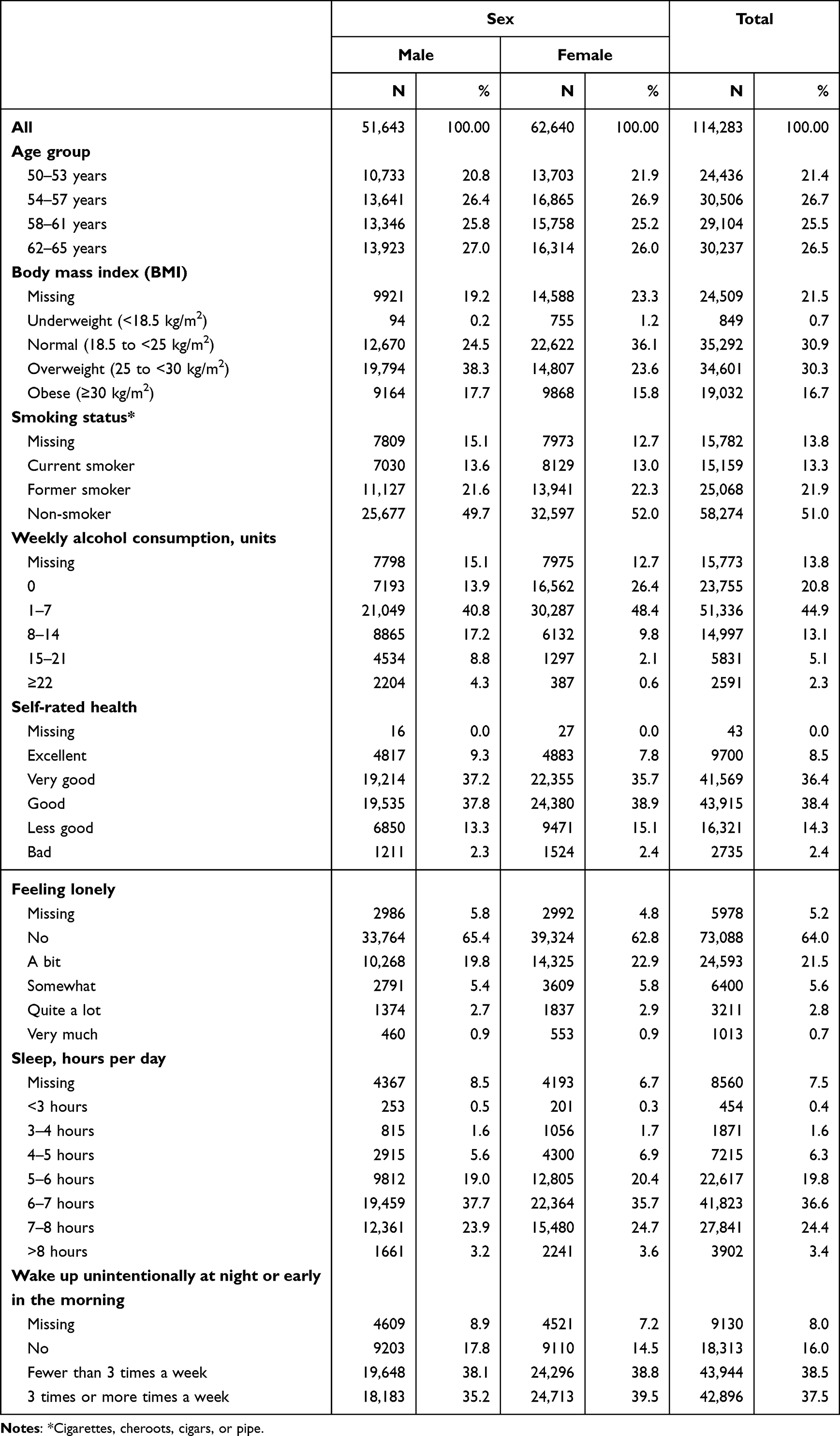 |
Table 2 Distribution of the Respondents by Age, Lifestyle Factors, and Health-Related Factors |
Thirteen percent of the respondents reported that they currently smoked cigarettes, cigars, cheroots, or pipes; 21.9% were former smokers and 51.0% reported that they never smoked. The distribution did not vary substantially between males and females (Table 2).
At the time of the survey, the Danish health authorities recommended that females should consume a maximum of seven units and males a maximum of 14 units of alcohol per week. Among male respondents, 71.9% reported an average weekly intake of 14 units of alcohol or fewer. Similarly, 74.8% of the females stated that they consumed 7 units or fewer per week (Table 2).
Based on the SF-12v2, 8.5% of the respondents provided excellent health self-ratings, with 36.4% and 38.4% reporting very good and good health, respectively. Another 14.3% described their current state of health as fair, while 2.4% reported poor health (Table 2). Similarly, 64.0% of respondents reported that they did not feel lonely at all, while 21.5% and 5.6% stated that they felt a bit or somewhat lonely, respectively. Only 2.8% reported that they felt lonely “a lot” and slightly less than 0.7% felt lonely “very much” (Table 2).
With respect to the average duration of sleep, 19.8% of the respondents reported that they slept for 5–6 hours each night during the past four weeks. By contrast, 36.6% reported that they slept for 6–7 hours while 24.4% slept for 7–8 hours per night during this interval. While 38.5% of the respondents reported that they had awakened unintentionally at night or early in the morning fewer than three times per week in the past four weeks, 37.5% reported that they had awakened unintentionally three or more times each week and 16.0% stated that they had not awakened unintentionally at all during the past four weeks (Table 2).
Among the missing values for the lifestyle and health-related factors, at the lowermost end, we identified <0.1% among the questions that addressed self-rated health, reaching a maximum of 21.5% for BMI (Table 2). The distribution of demographic, lifestyle, and health-related factors in the respondent cohort are described in Table 3.
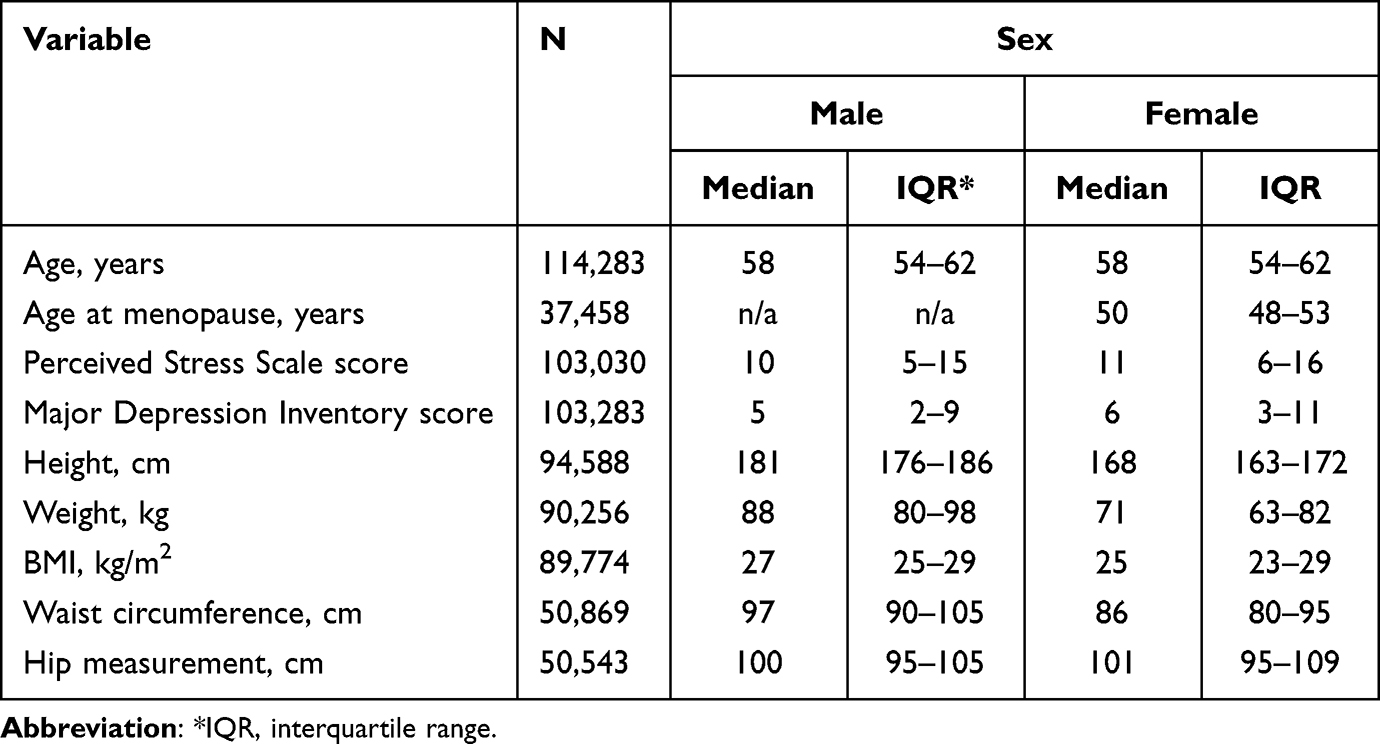 |
Table 3 Distribution of demographics, Lifestyle Factors, and Health-Related Factors |
Morbidity
We retrieved individual diagnosis codes assigned to each respondent that were registered in the DNPR for the five years immediately preceding their responses to the Better Health in Late Life questionnaire. Based on the ICD-10 codes of the 19 conditions included in the Charlson Comorbidity Index, we identified the somatic diseases that were the most prevalent in our cohort. The category “Solid cancer” ranked highest, at 5.2% (6.2% of female and 3.9% of male respondents). This was followed by “Chronic pulmonary disease” at 3.0% (3.2% of female and 2.7% of male respondents), and “Diabetes type I/II” at 2.3% (1.8% of female and 2.9% of male respondents) (Table 4).
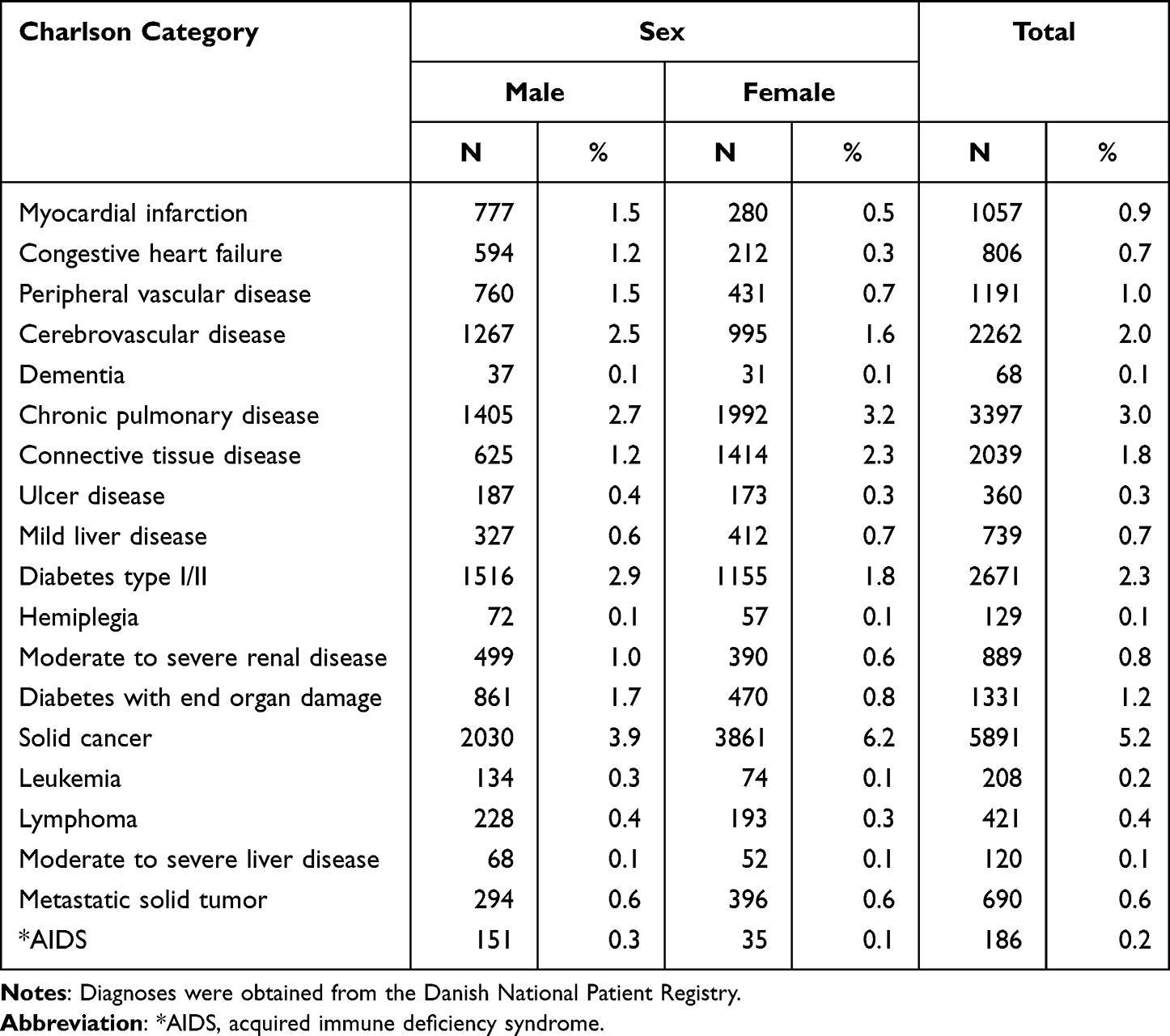 |
Table 4 Hospital Diagnoses Among 114,283 Respondents (Grouped According to the Charlson Comorbidity Index) Recorded Up to Five Years Before the Date of the Questionnaire |
Medication Use
Medication use is another factor that can help us to map the health profile of the population under study. Using the DNPD, we identified prescriptions filled by respondents within the year immediately preceding their responses to the questionnaire. 38.1% (43.5% of female and 31.7% of male respondents) filled prescriptions for medications used to treat nervous system disorders, while 37.4% (35.6% of female and 39.6% of male respondents) filled prescriptions for medications for cardiovascular disease (Table 5). The 10 most commonly dispensed prescription medications recorded up to one year before each individual completed the questionnaire are reported in Table 6.
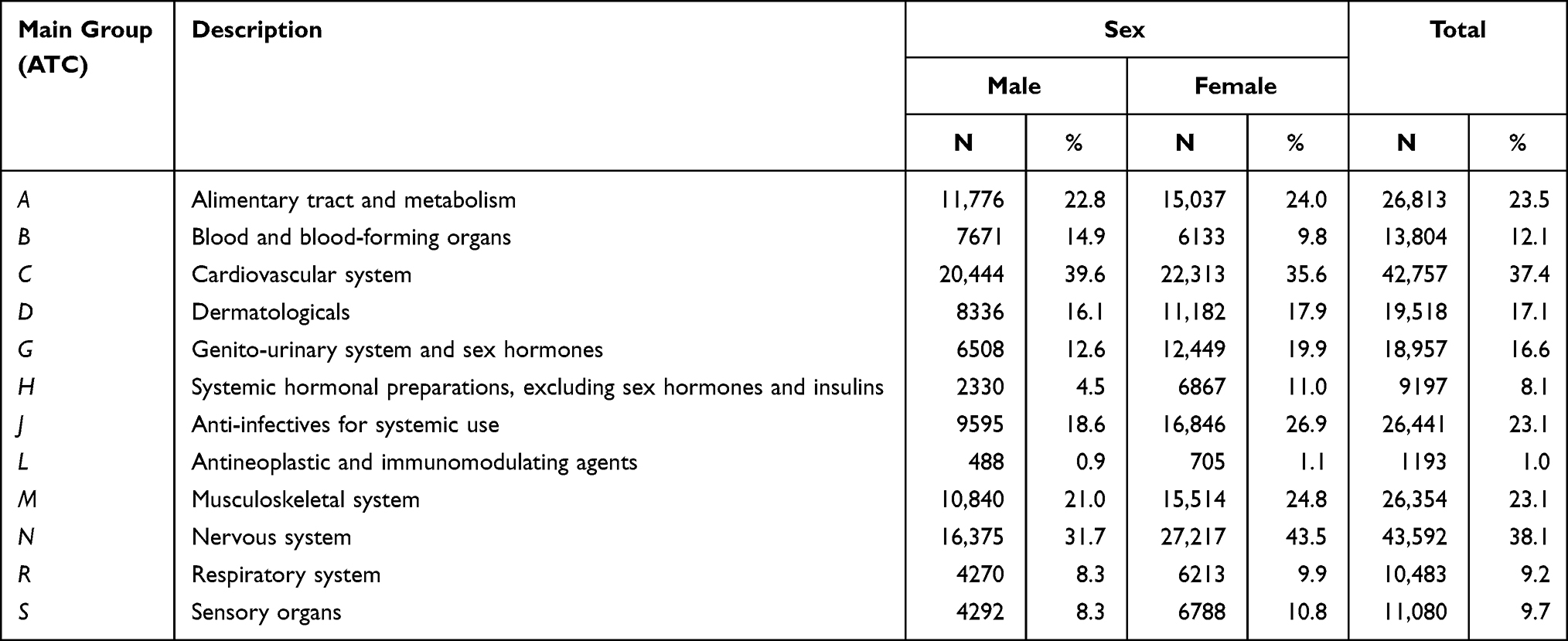 |
Table 5 Distribution of Dispensed Prescription Medication Among 114,283 Respondents According to the 12 Main Anatomical, Therapeutic, Chemical (ATC) Classification Groups Recorded Up to One Year Before the Date of the Questionnaire |
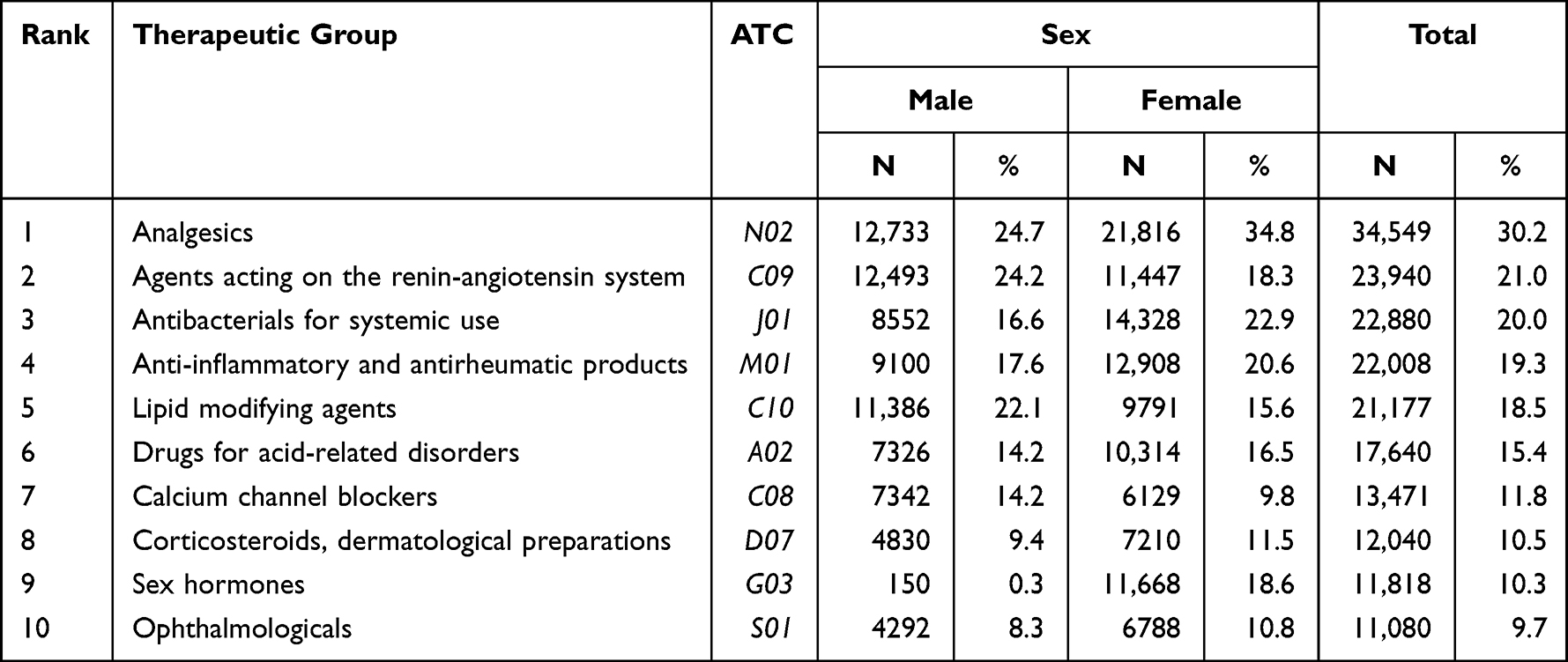 |
Table 6 ATC Codes of the 10 Most Commonly Dispensed Prescription Medications Among 114,283 Respondents Recorded Up to One Year Before the Date of the Questionnaire |
Discussion
The Better Health in Late Life cohort is one of the largest and most comprehensive sources of information that can be used to address late-life morbidity. While the opportunity to live a long and healthy life is universally valued, important inequalities exist. It will be important to know how to predict the number of years of disability-free life that might remain for those currently at 65 years of age.42 The relation between multimorbidity and mortality depends not only on the number of diseases but also their severity and potential responses to treatment combined with lifestyle and associated social factors, as well as other exposures. A life-course approach as a means to understand determinants of health in later life may provide us with the critical insight needed in our attempt to minimize the number of years lived with a physical or psychological disability. Findings from the Better Health in Late Life cohort offers the possibility of elucidating and evaluating the impact of these determinants, as supplementing the registries with self-reported data increases the value of the health registries as a research tool, in particular with respect to multimorbidities.
We chose to focus on the age group 50–65 years due to the challenges of global aging. The United Nations’ Population Division predicts that the number of individuals aged 60+ will more than double from about 900 million in 2015 (~12% of the world’s population) to 2.1 billion by 2050 (21.5%).43 The population changes and the burden of non-communicable diseases have raised concern about a surge in health expenditure, reduced labor force participation, and lack of social security.
Strengths and Weaknesses
We developed the Better Health in Late Life cohort as a data source that contains comprehensive life course information focusing on lifestyle and self-rated health. We have linked the data collected from this cohort to both health and social registries which provided us with the opportunity to obtain additional information on morbidity, prescriptions that have been filled, educational level, income, and health care utilization at an individual level. These registries also provide a virtually complete follow-up of all individuals within this prospective cohort. Of note, the study sample was drawn at random from all residents of Denmark who were 50–65 years of age at that time. Thus, the cohort has the potential to represent individuals from a variety of different sociodemographic segments and all regions of Denmark. Nonetheless, certain limitations need to be considered. We were unable to ensure that the person to whom the invitation was directed was the one who actually filled out the questionnaire. The first questions asked the respondents to state their sex and age. We excluded those who reported an age outside that of the target group (50–65 years) and those who did not answer the question on sex. It is also critical to note that the questionnaire responses were not validated. The participants may have underreported certain behaviors such as alcohol consumption and smoking that have known detrimental effects. However, we assume that these are self-reported data that are independent of later disease outcome. Such non-differential misclassification tends to produce conservative estimates closer to the null or no effect value than the real effect. If there is no real effect, there will be no bias.44,45
Likewise, the questionnaire required the participant to have a clear recollection of symptoms and lifestyle behaviors. Questions that focus on longer recall periods may ultimately have more inaccurate responses. However, the recall period was relatively short for many of the questions (typically 2–4 weeks). Finally, although the invitation was sent out to a random sample of the population, our analysis of the cohort characteristics revealed that persons who were older and reported higher educational backgrounds may be overrepresented in this sample.
The response rate of 38% may be associated with bias of absolute risk estimates if the study participation only reach a selected subgroup of the target population.46 The most important issues for etiological studies is to get a sufficient number of exposed individuals in each category. Our large cohort size seems to have sufficient variance and therefore, the generalization of associations between risk factors and outcomes is most likely assured.47 For example, the UK Biobank has an analytic sample of 499,701 persons based on a response rate as low as 5.5%. A comprehensive analysis showed similar risk factor associations in the UK Biobank as in other large cohorts with a much higher response rate.48
Perspectives
Humans are living longer and experiencing a higher prevalence of late-in-life illnesses. Thus, many key issues confronting clinical medicine and health policies related to this concern might be best investigated using longitudinal data from large, population-based cohorts. The Better Health in Late Life cohort was developed to address this need and will build on an important array of existing health-related social resources in Denmark. The Better Health in Late Life cohort will provide Denmark with an outstanding database and infrastructure for conducting clinical research at the highest level and has the potential to follow medical events on an individual and population basis from a lifelong perspective. This will not be possible in most other countries. Of particular interest, many people experience little illness throughout life and into old age. This trait might be identified, evaluated, and explored over a much larger proportion of the population.
Non-communicable diseases, including mental disorders, are largely preventable The disease burden and the associated economic burden can therefore be effectively reduced in many countries by implementing strategies to reduce risk factors, improve health care, and strengthen surveillance and monitoring.26,49
Data Sharing Statement
The data collection has been supported by a personal grant to Henrik Toft Sørensen from the Novo Nordisk Foundation (the Hagedorn Award). A steering committee, chaired by Professor Henrik Toft Sørensen, Principal Investigator and initiator of the study, was appointed by Aarhus University. Interested scientists can apply for access to the data presented in this manuscript by contacting the chair of the committee via e-mail ([email protected] or [email protected]).
Consent Statements
The study was reported to the Danish Data Protection Agency (record number 2016-051-000001) by Aarhus University. According to Danish legislation, informed consent and approval from an ethics committee are not required for registry-based studies, but the participants provided informed consent through Statistics Denmark by accepting a statement.
Acknowledgments
We thank Professor Jes Olesen, MD, DMSc, for sharing his expertise regarding the migraine questions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Oeppen J, Vaupel JW. Demography. Broken limits to life expectancy. Science. 2002;296(5570):1029–1031. doi:10.1126/science.1069675
2. Vaupel JW, Carey JR, Christensen K, et al. Biodemographic trajectories of longevity. Science. 1998;280(5365):855–860. doi:10.1126/science.280.5365.855
3. Partridge L, Deelen J, Slagboom PE. Facing up to the global challenges of ageing. Nature. 2018;561(7721):45–56. doi:10.1038/s41586-018-0457-8
4. Pew Research Center. Americans are aging, but not as fast as people in Germany, Italy and Japan; 2015. Available from: www.pewresearch.org/short-reads/2015/05/21/americans-are-aging-but-not-as-fast-as-people-in-germany-italy-and-japan/.
5. World Health Organization. European observatory health policy series; 2014. Available from: https://www.who.int/data/gho.
6. Jagger C, Gillies C, Moscone F, et al. Inequalities in healthy life years in the 25 countries of the European Union in 2005: a cross-national meta-regression analysis. Lancet. 2008;372(9656):2124–2131. doi:10.1016/S0140-6736(08)61594-9
7. Temesgen A, Murray C. Transitions in global disease burden. In: Boulton ML, Wallace RB, editors. Public Health and Preventive Medicine.
8. Academy of Medical Sciences. Multimorbidity: a priority for global health research. Available from: https://acmedsci.ac.uk/file-download/82222577.
9. Palladino R, Tayu Lee J, Ashworth M, Triassi M, Millett C. Associations between multimorbidity, healthcare utilisation and health status: evidence from 16 European countries. Age Ageing. 2016;45(3):431–435. doi:10.1093/ageing/afw044
10. Garin N, Koyanagi A, Chatterji S, et al. Global multimorbidity patterns: a cross-sectional, population-based, multi-country study. J Gerontol a Biol Sci Med Sci. 2016;71(2):205–214. doi:10.1093/gerona/glv128
11. Marengoni A, Angleman S, Melis R, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. 2011;10(4):430–439. doi:10.1016/j.arr.2011.03.003
12. Forjaz MJ, Rodriguez-Blazquez C, Ayala A, et al. Chronic conditions, disability, and quality of life in older adults with multimorbidity in Spain. Eur J Intern Med. 2015;26(3):176–181. doi:10.1016/j.ejim.2015.02.016
13. Pati S, Agrawal S, Swain S, et al. Non communicable disease multimorbidity and associated health care utilization and expenditures in India: cross-sectional study. BMC Health Serv Res. 2014;14:451. doi:10.1186/1472-6963-14-451
14. Palladino R, Pennino F, Finbarr M, Millett C, Triassi M. Multimorbidity and health outcomes in older adults in ten European health systems, 2006-15. Health Aff (Millwood). 2019;38(4):613–623. doi:10.1377/hlthaff.2018.05273
15. Sørensen HT, Lash TL, Rothman KJ. Beyond randomized controlled trials: a critical comparison of trials with nonrandomized studies. Hepatology. 2006;44(5):1075–1082. doi:10.1002/hep.21404
16. Bushardt RL, Massey EB, Simpson TW, Ariail JC, Simpson KN. Polypharmacy: misleading, but manageable. Clin Interv Aging. 2008;3(2):383–389. doi:10.2147/CIA.S2468
17. Baré M, Herranz S, Roso-Llorach A, et al. Multimorbidity patterns of chronic conditions and geriatric syndromes in older patients from the MoPIM multicentre cohort study. BMJ Open. 2021;11(11):e049334. doi:10.1136/bmjopen-2021-049334
18. Violan C, Foguet-Boreu Q, Flores-Mateo G, et al. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS One. 2014;9(7):e102149. doi:10.1371/journal.pone.0102149
19. Pearson-Stuttard J, Ezzati M, Gregg EW. Multimorbidity-a defining challenge for health systems. Lancet Public Health. 2019;4(12):e599–e600. doi:10.1016/S2468-2667(19)30222-1
20. Guthrie B, Payne K, Alderson P, McMurdo ME, Mercer SW. Adapting clinical guidelines to take account of multimorbidity. BMJ. 2012;345:e6341. doi:10.1136/bmj.e6341
21. Gryglewska B, Piotrowicz K, Grodzicki T. Ageing, multimorbidity, and daily functioning. In: Oxford Textbook of Geriatric Medicine. Oxford: Oxford University Press.; 2018.
22. Frank L. Epidemiology. The epidemiologist’s dream: Denmark. Science. 2003;301(5630):163. doi:10.1126/science.301.5630.163
23. Laugesen K, Ludvigsson JF, Schmidt M, et al. Nordic health registry-based research: a review of health care systems and key registries. Clin Epidemiol. 2021;13:533–554. doi:10.2147/CLEP.S314959
24. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish national patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
25. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
26. Alwan A, Collins P, Sankaranarayanan R, Saxena S. Addressing the growing burden of chronic noncommunicable diseases. In: Boulton ML, Wallace RB, editors. Maxcy-Rosenau-Last Public Health & Preventive Medicine.
27. Schmidt M, Pedersen L, Sørensen HT. The Danish civil registration system as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
28. Bech P, Rasmussen NA, Olsen LR, Noerholm V, Abildgaard W. The sensitivity and specificity of the major depression inventory, using the present state examination as the index of diagnostic validity. J Affect Disord. 2001;66(2–3):159–164. doi:10.1016/S0165-0327(00)00309-8
29. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
30. Ebert JF, Huibers L, Christensen B, Christensen MB. Paper- or web-based questionnaire invitations as a method for data collection: cross-sectional comparative study of differences in response rate, completeness of data, and financial cost. J Med Internet Res. 2018;20(1):e24. doi:10.2196/jmir.8353
31. Department of Clinical Epidemiology, Aarhus University Hospital. Bedre sundhed 50+ [Better health 50+]. Available from: https://kea.au.dk/research/bedresundhed.
32. Pottegard A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data resource profile: the Danish national prescription registry. Int J Epidemiol. 2017;46(3):798–798f. doi:10.1093/ije/dyw213
33. The register of medicinal products statistics. Available from: https://sundhedsdatastyrelsen.dk/da/registre-og-services/om-de-nationale-sundhedsregistre/sygdomme-laegemidler-og-behandlinger/laegemiddelstatistikregisteret.
34. Gjerstorff ML. The Danish cancer registry. Scand J of Public Health. 2011;39(7_suppl):42–45. doi:10.1177/1403494810393562
35. Arendt JFH, Hansen AT, Ladefoged SA, Sørensen HT, Pedersen L, Adelborg K. Existing data sources in clinical epidemiology: laboratory information system databases in Denmark. Clin Epidemiol. 2020;12:469–475. doi:10.2147/CLEP.S245060
36. Munk-Jørgensen P, Mortensen PB. The Danish psychiatric central register. Dan Med Bull. 1997;44(1):82–84.
37. Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39(7 Suppl):91–94. doi:10.1177/1403494810394715
38. Petersson F, Baadsgaard M, Thygesen LC. Danish registers on personal labour market affiliation. Scand J Public Health. 2011;39(7 Suppl):95–98. doi:10.1177/1403494811408483
39. Andersen JS, Olivarius Nde F, Krasnik A. The Danish national health service register. Scand J Public Health. 2011;39(7 Suppl):34–37. doi:10.1177/1403494810394718
40. Bjerregaard B, Larsen OB. The Danish pathology register. Scand J Public Health. 2011;39(7 Suppl):72–74. doi:10.1177/1403494810393563
41. Gjersøe P, Andersen SE, Mølbak AG, Wulff HR, Thomsen OO. Reliability of death certificates. The reproducibility of the recorded causes of death in patients admitted to departments of internal medicine. Ugeskr Laeger. 1998;160(35):5030–5034.
42. Bell R, Marmot MG. Life course approach to understanding inequalities in health in later life. In: Michel J, Beattie B, Martin F, editors. Oxford Textbook of Geriatric Medicine. Oxford: Oxford University Press; 2018:69–76.
43. United Nations, Department of Social Affairs, Population Division. World population prospects: the 2015 revision, volume II: demographic profiles; 2015.
44. Greenland S, Lash TL, Rothman KJ. Concepts of interaction. In: Rothman KJ, Greenland S, Lash TL, editors. Modern Epidemiology.
45. Rothman KJ. Epidemiology: An Introduction.
46. Eysenbach G, Wyatt J. Using the Internet for surveys and health research. J Med Internet Res. 2002;4(2):E13. doi:10.2196/jmir.4.2.e13
47. Manolio TA, Collins R. Enhancing the feasibility of large cohort studies. JAMA. 2010;304(20):2290–2291. doi:10.1001/jama.2010.1686
48. Batty GD, Gale CR, Kivimäki M, Deary IJ, Bell S. Comparison of risk factor associations in UK Biobank against representative, general population based studies with conventional response rates: prospective cohort study and individual participant meta-analysis. BMJ. 2020;368:m131. doi:10.1136/bmj.m131
49. Strandberg TE. Midlife risk factors of diseases and geriatric syndromes. In: Michel J-P, Beattie BL, Martin FC, Walston J, editors. Oxford Textbook of Geriatric Medicine. Oxford University Press; 2017.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patients with Chronic Diseases Who Travel: Need for Global Access to Timely Health Care Data
Sørensen HT
Clinical Epidemiology 2022, 14:513-519
Published Date: 26 April 2022
Spotlight on the Challenges of Depression following Retirement and Opportunities for Interventions
Dang L, Ananthasubramaniam A, Mezuk B
Clinical Interventions in Aging 2022, 17:1037-1056
Published Date: 7 July 2022
The DIAbetes MANagement and Treatment (DIAMANT) Cohort
Overbeek JA, Swart KMA, van der Pal EYM, Blom MT, Beulens JWJ, Nijpels G, Elders PJM, Herings RMC
Clinical Epidemiology 2022, 14:1453-1462
Published Date: 5 December 2022
Interaction Between Multimorbidity and Hip Fracture Surgery Leads to Excess Risk of Infection: A Danish Registry-Based Cohort Study of 92,599 Patients With Hip Fracture
Hansen CM, Gadgaard NR, Vandenbroucke-Grauls C, Hailer NP, Pedersen AB
Clinical Epidemiology 2025, 17:167-176
Published Date: 24 February 2025