Back to Journals » Clinical Epidemiology » Volume 14
Patients with Chronic Diseases Who Travel: Need for Global Access to Timely Health Care Data
Authors Sørensen HT ![]()
Received 8 February 2022
Accepted for publication 18 April 2022
Published 26 April 2022 Volume 2022:14 Pages 513—519
DOI https://doi.org/10.2147/CLEP.S360699
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eyal Cohen
Henrik Toft Sørensen1,2
1Department of Clinical Epidemiology, Aarhus University Hospital and Aarhus University, Aarhus N, DK-8200, Denmark; 2Clinical Excellence Research Center, Stanford University, Palo Alto, CA, USA
Correspondence: Henrik Toft Sørensen, Department of Clinical Epidemiology, Aarhus University, Olof Palmes Allé 43-45, Aarhus N, DK-8200, Denmark, Email [email protected]
Abstract: Despite the Covid-19 pandemic, international travel is expected to increase in the future. Before the pandemic, the United Nations World Tourism Organization estimated that by 2030 nearly 2 billion people would travel internationally each year. This raises the risk of unavailable medical record information if a complication or an emergency occurs in another country (particularly problematic for the growing numbers of older travelers with multimorbidity). We propose that an international medical record containing current health information be developed to allay this additional risk of traveling.
Keywords: e-health, epidemiology, global health, medical records, travel medicine
Introduction
Travel creates health risks for the individual traveler, as well as host and home countries,1,2 as illustrated by the global spread of Covid-19.1,2 The risk can be infectious or non-infectious, sometimes destination-specific and at times globally distributed.2 It is well established that the health risk of travel varies according to the location, duration, and purpose of a trip, planned activities, season, living standards, risk behavior, and a traveler’s health status.3–14
International travel includes business and pleasure activities, as well as visits to relatives and friends and medical tourism. For example, immigrants in the United States, who represent 10% of the national population, frequently visit their homeland to maintain family ties.15,16 Medical tourism is a relatively new but growing practice of traveling outside one’s home country for the primary purpose of receiving medical care. The most common categories of care are dentistry, cosmetic surgery, reproductive procedures, bariatric surgery, orthopedic surgery, and cardiac surgery.17–24 Although medical travelers hope to obtain less expensive care whose quality is similar to that available in their home country, few outcome data exist20,25–27 Postoperative complications are common following a major surgical procedure,27 and lack of documentation from the foreign health care provider may complicate follow-up at home.
Although rigorous epidemiological evidence is scarce, it is commonly known that health problems occur frequently among travelers. Available studies have estimated that between 10% and 42% of travelers to any destination and 15% to 70% of travelers to tropical settings experience illness, either during their travels or upon return to their home country.28–34
Infections, including diarrhea, occur frequently among travelers.34,35 A survey conducted by the GeoSentinel Surveillance Network found that infections and dermatological diseases (skin infections, rash, stings, and bites) account for more than 75% of illnesses necessitating post-travel medical care.36 As well, patients with chronic diseases are at increased risk of new illness or complications of existing illness.10,35,37,38 Fatal events while traveling are estimated to occur in 1 in 100,000 travelers.39,40 Cardiovascular diseases account for more than 50% of deaths documented during commercial air travel, and are the second most frequent reason for medical evacuation.37,38 Motor vehicle injuries and drowning are major causes of preventable death in travelers, whereas malaria remains the most common travel-related cause of infectious disease death.
In-flight medical emergencies (IMEs) represent a special area within travel medicine. During IMEs, traveling physicians and other health care professionals may render medical assistance. In a plane cruising at 10 km with little medical equipment, often far from the closest airport and hospital, provision of care is difficult.41 Lack of access to data on the patient’s underlying morbidities increases the challenges for health professionals who step in to help.41 The reduced pressure of oxygen may exacerbate existing medical conditions. The rate of IMEs is estimated to be 1 in every 604 flights.42 This is based on 11,920 requested ground consultations by five large domestic and international airlines during 2008–2010.42 It is likely an underestimate because minor incidents do not result in ground consultations. In addition, cruise ship travel is associated with an increased risk of severe infections.43–45
Travelers with Multimorbidity
Despite the huge number of international travelers, little research exists on improving clinical care among travelers. The need for better travel medicine is particularly urgent for the rapidly growing elderly population. People are living longer with chronic diseases and undergoing advanced treatments involving many health care providers, often resulting in fragmented health care. The global population aged ≥60 years in Western Europe and North America is expected to more than triple by 2050, reaching 2 billion people.46 By 2050, 44% of the world’s population will live in countries with at least 20% of inhabitants aged ≥60 years. This growing elderly population will require more health care services and health care coordination in general, as well as during travel.
Aging is strongly related to multimorbidity - broadly defined as the co-occurrence of two or more diseases or conditions in the same individual.47 Multimorbidity negatively influences a range of outcomes, including utilization, quality, and cost of health care, quality of life, and morbidity.48–50 In the US, patients with chronic conditions account for approximately 80% of medical care spending,51 and the cost increases exponentially as the number of chronic diseases increases.52 Multimorbidity is strongly associated with polypharmacy. While there is no clear definition of polypharmacy, it often includes prescriptions for more than five drugs. Polypharmacy is increasingly common due to the greater availability of effective drugs, guideline-recommended treatments for many chronic conditions, and changes in patients’ expectations.53,54 It comes at the risk of adverse drug effects and interactions.
Travel medicine is a long-standing branch of medicine dealing with the prevention and treatment of health problems in international travelers. A key necessity for reducing travelers’ health-related risks is to make information on their health conditions timely and accessible to medical professionals.1 However, when travel by persons with chronic diseases occurs across borders, it is difficult to coordinate clinical care and prepare international guidelines.55
The clinical process for travel and medicine can be divided into 1) pre-travel 2) travel itself, and 3) post-travel. A pre-travel evaluation should ideally take place 4–6 weeks before departure and include a risk assessment based on itinerary, type and duration of travel, prevention strategies, self-treatment instructions for anticipated complications, and special guidance on health treatment abroad (eg, instructions on how to access medical care at the destination).56,57 Several websites provide information on physicians abroad, as shown in Box 1. In low-income countries, options for obtaining medical care may be limited, with no guaranteed access to urgent medical care.
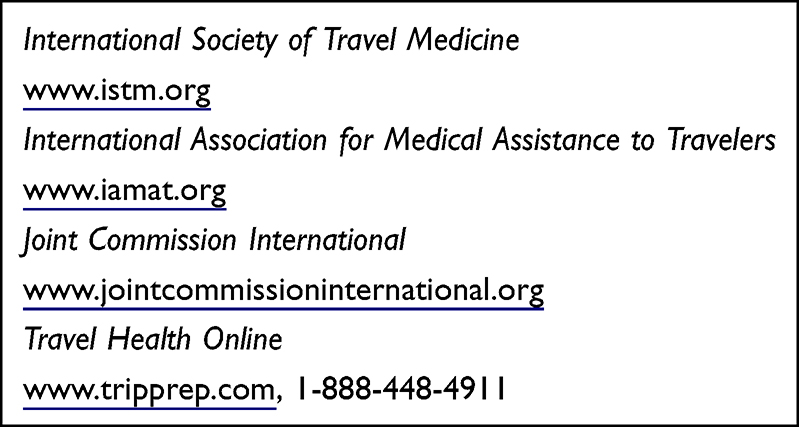 |
Box 1 Resources for Obtaining Medical Care During International Travel |
Need for a Globally Accessible and Timely Medical Travel Record
Accurate, accessible, and up-to-date medical record information is a prerequisite for all good health care, enabling immediate treatment and preventing overtreatment, undertreatment, or inappropriate treatment. According to informal international guidelines, travelers should carry certifications of vaccinations, travel insurance cards, medical reports, a list of allergies, blood type, name, as well as the address and phone number of the personal physician, hospital, and family members. However, it is uncommon for travelers to carry such information. Although it is recommended that persons with complex medical problems bring their medical records in paper form or on a portable USB drive, it rarely happens.56,58
The main challenge for travel medicine is to provide key information for medical professionals to access in order to help stricken travelers. In an acute situation, such information is rarely available and difficult to obtain due to logistic and linguistic barriers. As well, in many health care systems, such data are often scattered on many platforms (depending on the structure of the health care system). If accessible, it is relatively easy to translate data on prescriptions and vaccinations into English or another common language. For example, the Anatomical Therapeutic Chemical Classification System is used in many countries in Europe for prescriptions and can easily be translated. The same applies to the International Classification of Diseases classification. However, many other medical records are unstructured. Patients with multiple chronic diseases will have a substantial list of diagnoses possibly generated over decades. Some are relevant for treatment outside the home country, but many would create unnecessary “noise” and uncertainty, and cause a delay for the treating physician.
Thus it is necessary to start developing a global medical record system based on algorithms to ensure an appropriate balance between the specificity and sensitivity of diagnostic and treatment information.59 Using the patient’s cell phone, global access to validated medical data via secured platforms would improve clinical care and allow direct communication between physicians and hospitals. If physicians in the home country could access updated information on medical episodes occurring during post-travel, medical care also would be improved.
The Covid-19 epidemic has shown that it is possible to make individual health care data globally available. For example the Danish Health Data Authorities have created vaccinations and immunization records for the entire Danish population (5.8m) available on cell phones in the languages Danish, English and French (Figure 1). Similar initiatives have been developed in other countries, but the initiatives have been restricted to Covid-19-related medical information. Ongoing feasibility studies aim to extend the health care information available on the phones to describe the actual clinical status of the patients. A huge amount of health care information is available for many patients with chronic diseases, often accumulated over many years. It requires development of advanced algorithms to reduce the huge amount of data to describe the actual clinical status of the patient, but feasibility studies have indicated that this aim can be reached with a reasonable accuracy of the algorithms. Cell phones have become a world source for both clinical care and travel medicine epidemiology.60,61
 |
Figure 1 Example of a Danish Covid-19 Record in French available on all Danes’ cell phones. |
An informal survey in Denmark of patients with chronic diseases and their physicians depicts the situation as follows: 72% of the physicians said that there are no Danish guidelines for ensuring that medical information follows patients with chronic diseases when they travel abroad. However, 94% of the physicians reported that in some cases they write unstructured medical summaries in Danish or English for traveling patients. The majority of physicians (84%) responded that patients with chronic diseases, such as cancer and cardiovascular disease, would likely receive safer and better treatment abroad if treating physicians had access to updated medical information. Very few patients reported that they bring their own medical information on their travels, although 92% believed that quality of care would improve if doctors abroad had access to their medical data. An American study conducted at Boston Logan International Airport reported that 46% of travelers to low- or low-middle income countries did not seek health advice prior to their trip, largely due to lack of concern about travel-related health issues. Among travelers who sought medical advice, the internet and primary care providers were the most common sources of information.62
In Conclusion
Travelers with health issues require: a) updated information on health status, diagnoses, treatments, and vaccinations; b) access to this updated information by health care providers at the destination - ideally through cell phones, c) secure handling of information on treatments abroad and the availability of this information in the patient’s home country to permit continuity of medical care. Importantly, any provided information needs to be in a relevant language because many health care providers primarily speak only their mother tongue. Creating a global electronic medical record system is possible, but complex - with multiple stakeholders, legal requirements, and need for rigorous IT security.63
Given the logistical challenges of setting up an international medical record system, it is important that efforts start now. Such information may make life-saving treatment possible, especially in settings with language differences.60,61 Boxes 1 and 2 below provide an overview of key information that should be included in global medical records.1 Box 2 is based on interviews with several Danish physicians.
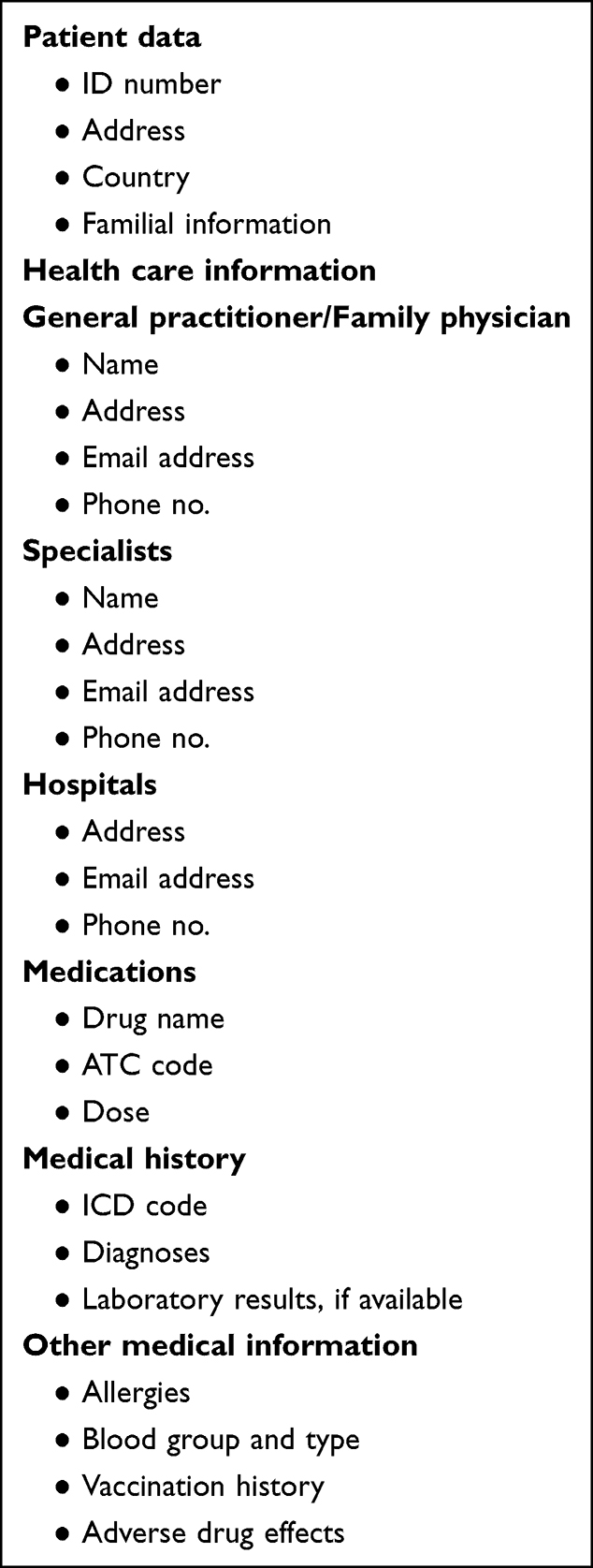 |
Box 2 Basic Structure of a Global Electronic Medical Record |
Acknowledgments
The author thanks Professors Jan P. Vandenbroucke and Niels Obel for their valuable review of this commentary.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Li YC, Detmer DE, Shabbir SA, et al. A global travelers’ electronic health record template standard for personal health records. J Am Med Inform Assoc. 2012;19(1):134–136. doi:10.1136/amiajnl-2011-000323
2. LaRocque RC, Jentes ES. Health recommendations for international travel: a review of the evidence base of travel medicine. Curr Opin Infect Dis. 2011;24(5):403–409. doi:10.1097/QCO.0b013e32834a1aef
3. Steffen R, deBernardis C, Baños A. Travel epidemiology–a global perspective. Int J Antimicrob Agents. 2003;21(2):89–95. doi:10.1016/S0924-8579(02)00293-5
4. Hatz C, Chen LH. Pre-travel consultation. In: Keystone JS, Freedman DO, Kozarsky PE, Connor BA, Nothdurft HD, editors. Travel Medicine.
5. Fink D, Wani RS, Johnston V. Fever in the returning traveller. BMJ. 2018;360:j5773. doi:10.1136/bmj.j5773
6. Piché-Renaud PP, Hoang Nguyen J, Pell LG, et al. Underestimation of travel-associated risks by adult and paediatric travellers compared to expert assessment: a cross-sectional study at a hospital-based family pre-travel clinic. Travel Med Infect Dis. 2022;47:102315. doi:10.1016/j.tmaid.2022.102315
7. Zhong L, Deng B, Morrison AM, Coca-Stefaniak JA, Yang L. Medical health and wellness tourism research-a review of the literature (1970–2020) and research Agenda. Int J Environ Res Public Health. 2021;18:20. doi:10.3390/ijerph182010875
8. Lopez-Gigosos RM, Segura M, Mariscal-Lopez E, Gutierrez-Bedmar M, Mariscal A. Prevalence of chronic diseases among international travelers seeking pretravel medical advice in 2018 at Malaga, Spain. Am J Trop Med Hyg. 2020;102(3):684–688. doi:10.4269/ajtmh.19-0702
9. Gudmundsson A, Stevenson TJ, Petrovice M, et al. Challenges and risks for older travellers with multimorbidity: focus on pharmacotherapy. Eur Geriatric Med. 2016;7(5):407–410. doi:10.1016/j.eurger.2016.03.005
10. Hochberg NS, Barnett ED, Chen LH, et al. International travel by persons with medical comorbidities: understanding risks and providing advice. Mayo Clinic Proceedings. 2013;88(11):1231–1240. doi:10.1016/j.mayocp.2013.07.018
11. Askling HH, Dalm VA. The medically immunocompromised adult traveler and pre-travel counseling: status quo 2014. Travel Med Infect Dis. 2014;12(3):219–228. doi:10.1016/j.tmaid.2014.04.009
12. Steffen R, Wilson ME. Fifty years of travel medicine epidemiology: what have we learnt? Int Health. 2015;7(6):375–376. doi:10.1093/inthealth/ihv035
13. Freedman DO, Weld LH, Kozarsky PE, et al. Spectrum of disease and relation to place of exposure among ill returned travelers. N Engl J Med. 2006;354(2):119–130. doi:10.1056/NEJMoa051331
14. Steffen R. Epidemiology of travellers’ diarrhea. J Travel Med. 2017;24(suppl_1):S2–S5. doi:10.1093/jtm/taw072
15. Bacaner N, Stauffer B, Boulware DR, Walker PF, Keystone JS. Travel medicine considerations for North American immigrants visiting friends and relatives. JAMA. 2004;291(23):2856–2864. doi:10.1001/jama.291.23.2856
16. Angelo KM, Haulman NJ, Terry AC, et al. Illness among US resident student travellers after return to the USA: a GeoSentinel analysis, 2007–17. J Travel Med. 2018;25(1). doi:10.1093/jtm/tay074
17. Connell J. Medical tourism: sea, sun, sand and surgery. Tourism Manage. 2006;27(6):1093–1100. doi:10.1016/j.tourman.2005.11.005
18. Reed CM. Medical tourism. Med Clin North Am. 2008;92(6):1433–1446. doi:10.1016/j.mcna.2008.08.001
19. Huntington MK. The expanding scope of medical travel. Am Fam Physician. 2011;84(8):863–864.
20. Alleman BW, Luger T, Reisinger HS, Martin R, Horowitz MD, Cram P. Medical tourism services available to residents of the United States. J Gen Intern Med. 2011;26(5):492–497. doi:10.1007/s11606-010-1582-8
21. Hudson N, Culley L, Blyth E, Norton W, Rapport F, Pacey A. Cross-border reproductive care: a review of the literature. Reprod Biomed Online. 2011;22(7):673–685. doi:10.1016/j.rbmo.2011.03.010
22. Birch DW, Vu L, Karmali S, Stoklossa CJ, Sharma AM. Medical tourism in bariatric surgery. Am J Surg. 2010;199(5):604–608. doi:10.1016/j.amjsurg.2010.01.002
23. Klímová B, Kuča K. Medical tourism: its research and implications for public health. Cent Eur J Public Health. 2020;28(3):226–229. doi:10.21101/cejph.a5744
24. Kumar S, Breuing R, Chahal R. Globalization of health care delivery in the United States through medical tourism. J Health Commun. 2012;17(2):177–198. doi:10.1080/10810730.2011.585699
25. Weiss EM, Spataro PF, Kodner IJ, Keune JD. Banding in Bangkok, CABG in Calcutta: the United States physician and the growing field of medical tourism. Surgery. 2010;148(3):597–601. doi:10.1016/j.surg.2010.06.012
26. Hod K, Bronstein Y, Chodick G, Shpilberg O. Hemato-oncology tourism in Israel: a retrospective review. JCO Glob Oncol. 2020;6(6):1314–1320. doi:10.1200/GO.20.00098
27. Pavli A, Maltezou HC. Infectious complications related to medical tourism. J Travel Med. 2021;28(1):taaa210. doi:10.1093/jtm/taaa210
28. Reed JM, McIntosh IB, Powers K. Travel illness and the family practitioner: a retrospective assessment of travel-induced illness in general practice and the effect of a travel illness clinic. J Travel Med. 1994;1(4):192–198. doi:10.1111/j.1708-8305.1994.tb00594.x
29. Fleck S, Jäger H, Zeeb H. Travel and health status: a survey follow-up study. Eur J Public Health. 2006;16(1):96–100. doi:10.1093/eurpub/cki144
30. Steffen R, Rickenbach M, Wilhelm U, Helminger A, Schär M. Health problems after travel to developing countries. J Infect Dis. 1987;156(1):84–91. doi:10.1093/infdis/156.1.84
31. Bruni M, Steffen R. Impact of travel-related health impairments. J Travel Med. 1997;4(2):61–64. doi:10.1111/j.1708-8305.1997.tb00781.x
32. Winer L, Alkan M. Incidence and precipitating factors of morbidity among Israeli travelers abroad. J Travel Med. 2002;9(5):227–232. doi:10.2310/7060.2002.24202
33. Hill DR. Health problems in a large cohort of Americans traveling to developing countries. J Travel Med. 2000;7(5):259–266. doi:10.2310/7060.2000.00075
34. Wilson ME, Weld LH, Boggild A, et al. Fever in returned travelers: results from the geosentinel surveillance network. Clin Infect Dis. 2007;44(12):1560–1568. doi:10.1086/518173
35. Steffen R, Hill DR, DuPont HL. Traveler’s diarrhea: a clinical review. JAMA. 2015;313(1):71–80. doi:10.1001/jama.2014.17006
36. Leder K, Torresi J, Libman MD, et al. GeoSentinel surveillance of illness in returned travelers, 2007–2011. Ann Intern Med. 2013;158(6):456–468. doi:10.7326/0003-4819-158-6-201303190-00005
37. Tonellato DJ, Guse CE, Hargarten SW. Injury deaths of US citizens abroad: new data source, old travel problem. J Travel Med. 2009;16(5):304–310. doi:10.1111/j.1708-8305.2009.00318.x
38. McCarthy AE, Burchard GD. The travelers with pre-existing disease. In: Keystone JS, Freedman DO, Kozarsky PE, Connor BA, Nothdurft HD, editors. Travel Medicine.
39. Steffen R, Grieve S. Epidemiology: morbidity and mortality in travelers. In: Keystone JS, Freedman DO, Kozarsky PE, Connor BA, Nothdurft HD, editors. Travel Medicine.
40. Windsor JS, Firth PG, Grocott MP, Rodway GW, Montgomery HE. Mountain mortality: a review of deaths that occur during recreational activities in the mountains. Postgrad Med J. 2009;85(1004):316–321. doi:10.1136/pgmj.2009.078824
41. Martin-Gill C, Doyle TJ, Yealy DM. In-flight medical emergencies: a review. JAMA. 2018;320(24):2580–2590. doi:10.1001/jama.2018.19842
42. Peterson DC, Martin-Gill C, Guyette FX, et al. Outcomes of medical emergencies on commercial airline flights. N Engl J Med. 2013;368(22):2075–2083. doi:10.1056/NEJMoa1212052
43. Freeland AL, Vaughan GH
44. Marshall CA, Morris E, Unwin N. An epidemiological study of rates of illness in passengers and crew at a busy Caribbean cruise port. BMC Public Health. 2016;16(1):314. doi:10.1186/s12889-016-2991-3
45. Mouchtouri VA, Rudge JW. Legionnaires’ disease in hotels and passenger ships: a systematic review of evidence, sources, and contributing factors. J Travel Med. 2015;22(5):325–337. doi:10.1111/jtm.12225
46. United Nations World Tourism Organization. Annual report, united nations world tourism organization. United Nations World Tourism Organization; 2017. Available from: https://www.e-unwto.org/doi/book/10.18111/9789284419807.
47. van den Akker M, Buntinx F, Knottnerus JA. Comorbidity or multimorbidity. Eur J Gen Pract. 1996;2(2):65–70. doi:10.3109/13814789609162146
48. Whitty CJM, MacEwen C, Goddard A, et al. Rising to the challenge of multimorbidity. BMJ. 2020;368:l6964. doi:10.1136/bmj.l6964
49. Rizzuto D, Melis RJF, Angleman S, Qiu C, Marengoni A. Effect of chronic diseases and multimorbidity on survival and functioning in elderly adults. J Am Geriatr Soc. 2017;65(5):1056–1060. doi:10.1111/jgs.14868
50. Lancet. Making more of multimorbidity: an emerging priority. Lancet. 2018;391(10131):1637. doi:10.1016/S0140-6736(18)30941-3
51. Anderson G. Chronic Conditions: Making the Case for Ongoing Care. Johns Hopkins Bloomberg School of Public Health: Robert Wood Johnson Foundation; 2010.
52. Frølich A, Ghith N, Schiøtz M, Jacobsen R, Stockmarr A. Multimorbidity, healthcare utilization and socioeconomic status: a register-based study in Denmark. PLoS One. 2019;14(8):e0214183. doi:10.1371/journal.pone.0214183
53. Guthrie B, Makubate B, Hernandez-Santiago V, Dreischulte T. The rising tide of polypharmacy and drug-drug interactions: population database analysis 1995–2010. BMC Med. 2015;13:74. doi:10.1186/s12916-015-0322-7
54. Bushardt RL, Massey EB, Simpson TW, Ariail JC, Simpson KN. Polypharmacy: misleading, but manageable. Clin Interv Aging. 2008;3(2):383–389. doi:10.2147/CIA.S2468
55. Schlagenhauf P, Santos-O’Connor F, Parola P. The practice of travel medicine in Europe. Clin Microbiol Infect. 2010;16(3):203–208. doi:10.1111/j.1469-0691.2009.03133.x
56. Lang WE. Healthcare Abroad. In: Keystone JS, Freedman DO, Kozarsky PE, Connor BA, Nothdurft HD, editors. Travel Medicine.
57. Gherardin T. The pre-travel consultation - an overview. Aust Fam Physician. 2007;36(5):300–303.
58. Leung DT, LaRocque RC, Ryan ET. Travel medicine. Ann Intern Med. 2018;168(1):Itc1–itc16. doi:10.7326/AITC201801020
59. Chubak J, Pocobelli G, Weiss NS. Tradeoffs between accuracy measures for electronic health care data algorithms. J Clin Epidemiol. 2012;65(3):343–349.e342. doi:10.1016/j.jclinepi.2011.09.002
60. Lai S, Farnham A, Ruktanonchai NW, Tatem AJ. Measuring mobility, disease connectivity and individual risk: a review of using mobile phone data and mHealth for travel medicine. J Travel Med. 2019;26(3). doi:10.1093/jtm/taz019
61. Farnham A, Blanke U, Stone E, Puhan MA, Hatz C. Travel medicine and mHealth technology: a study using smartphones to collect health data during travel. J Travel Med. 2016;23(6). doi:10.1093/jtm/taw056
62. LaRocque RC, Rao SR, Tsibris A, et al. Pre-travel health advice-seeking behavior among US international travelers departing from Boston Logan International Airport. J Travel Med. 2010;17(6):387–391. doi:10.1111/j.1708-8305.2010.00457.x
63. Manlapaz P, Castillejo L, Herrington S. An Electronic Medical Record System Supporting Global Health and Medical. One Petro; 2016.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cohort Profile: Better Health in Late Life
Sørensen HT, Christensen T, Bøtker HE, Christiansen CF, Fuglsang CH, Gribsholt SB, Kristensen FPB, Laugesen K, Laursen ASD, Nørgaard M, Schmidt M, Skajaa N, Troelsen FS, Pedersen L
Clinical Epidemiology 2023, 15:1227-1239
Published Date: 20 December 2023