Back to Journals » Drug Design, Development and Therapy » Volume 20
Co-Administration of MPC Polymer Enhances the Ocular Absorption and Intraocular Pressure-Lowering Effect of Timolol Maleate
Authors Otake H, Ogata F, Kawasaki N ![]() , Sasaki A, Gotanda R, Matsuoka Y, Nagai N
, Sasaki A, Gotanda R, Matsuoka Y, Nagai N ![]()
Received 16 January 2026
Accepted for publication 13 May 2026
Published 22 May 2026 Volume 2026:20 596715
DOI https://doi.org/10.2147/DDDT.S596715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leonidas Panos
Hiroko Otake,1 Fumihiko Ogata,1 Naohito Kawasaki,1 Ayano Sasaki,2 Ryuya Gotanda,2 Yosuke Matsuoka,2 Noriaki Nagai1
1Faculty of Pharmacy, Kindai University, Higashi-Osaka, Osaka, 577-8502, Japan; 2Life Science Division, NOF CORPORATION, Shibuya-ku, Tokyo, 150-6012, Japan
Correspondence: Noriaki Nagai, Faculty of Pharmacy, Kindai University, 3-4-1 Kowakae, Higashi-Osaka, Osaka, 577-8502, Japan, Tel +81 6 4307 3638, Fax +81 6 6730 1394, Email [email protected]
Purpose: We previously developed a novel 2-methacryloyloxyethyl phosphorylcholine-based polymer (MPCP) containing a zwitterionic stearyl methacrylate moiety and an acrylic functional group, which significantly improved moisture retention on the ocular surface. In this study, we investigated whether incorporating 0.1% MPCP into 0.25% or 0.5% timolol maleate (TM) ophthalmic formulations could enhance the ocular surface retention, corneal permeability, and intraocular pressure (IOP)-lowering efficacy of TM.
Methods: Male Wistar rats (7 weeks old) and male adult rabbits (body weight: 2.39 ± 0.71 kg) were used to evaluate ocular surface retention and corneal permeability of TM. IOP-lowering efficacy of TM was evaluated using a rabbit treated with 5% glucose solution (high IOP model).
Results: The TM ophthalmic formulations with MPCP (TM@MPCP-OF) were transparent, with MPCP nanoparticles (mean particle size 80.7 nm) dispersed in the formulation, and exhibited stable viscosity, regardless of the presence of MPCP (approximately 0.95– 1.1 mPa∙s). The addition of MPCP reduced cytotoxicity in human corneal epithelial cells (HCE-T) and caused no damage after repeated instillation in rats. Moreover, the combination with MPCP improved TM retention on the ocular surface and increased the corneal TM concentration and aqueous humor penetration after the instillation of TM@MPCP-OF. In addition, the corneal permeability-enhancing effect of MPCP on the TM was more pronounced with TM@MPCP-OF containing 0.5% TM than with TM@MPCP-OF containing 0.25% TM. Furthermore, compared with the TM ophthalmic formulation alone, MPCP co-administration significantly prolonged the duration and magnitude of the IOP-lowering effect of TM in a rabbit model of acute ocular hypertension.
Conclusion: These findings indicate that MPCP is a safe and biocompatible additive that enhances the pharmacological performance of ophthalmic formulations and may contribute to the development of improved and longer-acting antiglaucoma medications. On the left, Timolol is shown with arrows indicating high ocular surface retention, middle corneal permeability and low intraocular-lowering effect. On the right, combination of Timolole and MPCP is depicted with arrows showing middle ocular surface retention, low corneal permeability and high intraocular-lowering effect. The legend at the top explains the arrow types: solid for high, dashed for middle, dotted for low and dash-dotted for minimum. The illustration highlights differences in drug effects on eye physiology.Diagram: Timolol vs. MPCP on eye surface retention, corneal permeability and eye pressure.
Keywords: MPC polymer, timolol maleate, intraocular pressure, ocular drug delivery, glaucoma
Introduction
Glaucoma is a chronic ocular disorder with elevated intraocular pressure (IOP) characterized by an imbalance between the production and drainage of aqueous humor within the eye. High IOP is a primary risk factor contributing to the onset and progression of this disease, ultimately leading to the degeneration of retinal ganglion cells and subsequent visual impairment.1 Glaucoma is an irreversible and progressive optic neuropathy that remains a major cause of permanent visual field loss and blindness worldwide.2,3
Extensive research has confirmed that therapeutic strategies to effectively lower IOP play a critical role in preserving visual function in patients with glaucoma.2,4,5 Current pharmacological management predominantly depends on topical ophthalmic formulations containing IOP-lowering agents, including β-adrenergic blockers, cholinergic agonists, carbonic anhydrase inhibitors, and prostaglandin analogs.6–8 Among these, timolol maleate (TM), a non-selective β-blocker, is one of the most widely prescribed medications for glaucoma treatment.9 TM exerts its pharmacological effects by inhibiting sympathetic activity in the ciliary epithelium, thereby suppressing the secretion of the aqueous humor. Because TM functions through a mechanism distinct from those of miotics, carbonic anhydrase inhibitors, and prostaglandin analogs, it is often used in combination therapy to enhance clinical efficacy.10 Consequently, TM is expected to remain the cornerstone of glaucoma management in the near future. However, less than 5% of TM administered via conventional eye drops penetrates the intraocular tissues because of the efficient protective barriers of the eye. This limited absorption is largely attributed to precorneal loss mechanisms such as rapid tear turnover, poor corneal permeability, brief residence in the conjunctival sac, and nonspecific absorption.10 The short retention time allows the drug to be washed away through tear drainage, leading not only to reduced therapeutic efficacy but also to systemic side effects, such as bradycardia, hypotension, and bronchospasm, as well as local irritation, dryness, and redness.11 Although eye drops constitute approximately 90% of all topically administered ophthalmic preparations and are generally favored for their ease of use, nearly 95% of the applied drugs are lost via conjunctival absorption or nasolacrimal drainage. Therefore, recent formulation research has focused on enhancing ocular drug bioavailability by improving retention and mucoadhesive properties.
Therefore, enhancing the ocular bioavailability of TM ophthalmic formulations (OF) is crucial for effective management of glaucoma. Developing formulations that maintain therapeutic efficacy with fewer daily instillations and improved therapeutic indices remains challenging. Sustained-release systems, in particular, continue to represent an unmet need in ophthalmic drug delivery. The use of ocular biomaterials capable of prolonging drug residence and maintaining sustained-release profiles has emerged as a promising strategy to overcome these limitations.12,13 Different formulation approaches have been explored to enhance the therapeutic efficiency and ocular availability of topically applied drugs by extending their precorneal retention and promoting corneal permeability. These include hydrogel-based systems, in situ gelling matrices, microparticles, colloidal carriers, nanovesicular gels, nanoparticles, liposomes, and nanogels.14–20
The polymer 2-methacryloyloxyethyl phosphorylcholine (MPC) is a multifunctional molecule with antiadhesive, antithrombogenic, and highly hydrophilic characteristics.21,22 Owing to its structural similarity to cell membrane phospholipids, MPC can form biocompatible hydrogel coatings that minimize tissue irritation by reducing the friction between the biological surface and the applied material. MPC has been incorporated into more than 2000 products, including cosmetics, disinfectants, and medical devices, such as artificial blood vessels, artificial hearts, and hemodialysis systems, owing to its excellent hemocompatibility and anti-inflammatory behavior.23–25 In ophthalmology, MPC has been used as a component of contact lens solutions and materials,26,27 as a coating for intraocular lenses,28 and as a corneal substitute.29 The high biocompatibility and low cytotoxicity of MPC-based polymers suggest that they are suitable for ocular applications. However, reduced tolerability has occasionally been observed when MPC is combined with sodium hyaluronate or preservative.30,31 In our previous study, we developed a novel MPC-based polymer via radical polymerization of MPC stearyl methacrylate/N,N-dimethylacrylamide (MPCP). In addition, we previously demonstrated that instillation of 0.1% MPCP significantly improved moisture retention on the ocular surface, indicating its potential to prevent dry-eye symptoms.32 Collectively, these results suggest that MPCP is a safe and biocompatible material suitable for OF and may help maintain ocular surface homeostasis of hydrophilic drugs. In the present study, we examined whether incorporating MPCP into TM ophthalmic formulations (TM@MPCP-OF) could enhance the ocular surface retention and intraocular permeation of TM. Furthermore, we used a rabbit model of acute ocular hypertension to evaluate the effect of MPCP co-administration on the IOP-lowering efficacy of TM.
Materials and Methods
Animals
In this study, to eliminate the influence of hormonal balance, evaluations were conducted using subjects of the same sex (male). The male Wistar rats (7 weeks old) were procured from Kiwa Laboratory Animals Co., Ltd. (Wakayama, Japan), and male adult rabbits (body weight: 2.39 ± 0.71 kg) were obtained from Shimizu Laboratory Supplies Co., Ltd. (Kyoto, Japan). All animals were housed under controlled environmental conditions at 25°C with free access to tap water and a standard laboratory diet (CE-2 for rats and CR-3M for rabbits; Clea Japan Inc., Tokyo, Japan). In the instillation experiment, eye drops were administered to only one eye. All animal experiments were performed in accordance with the ethical standards of Kindai University, the Japanese Pharmacological Society, and the U.S. National Institutes of Health (NIH) Guidelines for the Care and Use of Laboratory Animals. The experimental protocol was reviewed and approved by the Institutional Animal Care and Use Committee of Kindai University on April 1, 2024 (approval no. KAPS-2024-008 and KAPS-2024-009). All procedures complied with the ARRIVE and 2020 AVMA Guidelines for the Euthanasia of Animals. Euthanasia was performed by intraperitoneal administration of 200 mg/kg pentobarbital sodium.
Chemicals
All reagents and chemicals used in this study were of the highest commercially available grade. A 5% glucose solution was obtained from Otsuka Pharmaceutical Co., Ltd. (Tokyo, Japan). TM and 0.4% benoxil were obtained from Sigma-Aldrich (Osaka, Japan) and Santen Pharmaceutical Co., Ltd. (Osaka, Japan), respectively. Benzalkonium chloride (BAC) was purchased from Kanto Chemical Co., Inc. (Tokyo, Japan). Pentobarbital was supplied by the Tokyo Chemical Industry Co., Ltd. (Tokyo, Japan). Dulbecco’s Modified Eagle’s medium/Ham’s F-12 (DMEM/F-12), penicillin, streptomycin, and fetal bovine serum (FBS) were purchased from GIBCO (Tokyo, Japan). The Cell Counting Reagent SF was obtained from Nacalai Tesque, Inc. (Kyoto, Japan).
Preparation of MPCP and TM@MPCP-OF
MPCP was synthesized by the radical polymerization of 2-methacryloyloxyethyl phosphorylcholine, stearyl methacrylate, and N,N-dimethylacrylamide at a molar ratio of 50:5:45, followed by purification via dialysis.32 Next, the residual monomer content was analyzed, and the conversion rate for each monomer exceeded 99%, confirming the successful synthesis of the target polymer.32 For the present experiments, MPCP ophthalmic formulation (MPCP-OF) was prepared as a 0.1% (w/v) aqueous solution in saline. The concentration of MPCP in the solution was determined by calculating the weight of dried MPCP (residue) contained in a fixed volume of solvent (weight/volume). The TM ophthalmic formulations (TM-OF) were prepared by dissolving TM (0.25% or 0.5%) and BAC (0.005%) in physiological saline. TM@MPCP-OF was prepared by incorporating 0.1% MPCP into TM-OF.
Characteristics in TM@MPCP-OF
The particle size distribution and concentration of MPCP were analyzed using a NanoSight LM10 system (Quantum Design Japan; Tokyo, Japan) equipped with a 405 nm laser, and measurements were conducted over a 60s acquisition period. Atomic force microscopy (AFM) was performed using a scanning probe microscope (SPM)-9700 (Shimadzu Corp., Kyoto, Japan), and final AFM images were generated by merging the phase and height data. The viscosity of OF was determined using a rotational viscometer (model SV-1A, A&D Company, Ltd., Tokyo, Japan) at 25°C. Osmotic pressure was measured using a freezing point osmometer (OM807, VOGEL MedTec, Germany).33
Measurement of TM
The concentration of TM was quantified by high-performance liquid chromatography (HPLC) using an LC-20AT system (Shimadzu Corp., Kyoto, Japan) equipped with a UV detector set at 294 nm. The mobile phase consisted of 25 mM phosphate buffer, methanol, and acetonitrile (60:30:10, v/v, pH 7.0). Analytical conditions were as follows: internal standard, 10 µg/mL propyl p-hydroxybenzoate; analytical column, Mightysil RP-18 (3 µm; Kanto Chemical Co., Inc., Tokyo, Japan); column temperature, 35°C; and mobile phase flow rate, 0.2 mL/min.34
Evaluation of in vitro Corneal Toxicity of TM@MPCP-OF Using HCE-T Cells
The human corneal epithelial (HCE-T) cell line was established by Araki-Sasaki et al35 were donated from RIKEN BRC CELL BANK (Ibaraki, Japan). HCE-T cells were maintained in Dulbecco’s Modified Eagle’s medium/Ham’s F-12 medium supplemented with 5% heat-inactivated fetal bovine serum, penicillin (1000 IU/mL), and streptomycin (0.1 mg/mL). Next, we conducted an in vitro corneal cytotoxicity assay, for which HCE-T cells (1 × 104 cells/well) were seeded in 96-well microplates (IWAKI, Chiba, Japan) and exposed to 0.1% MPCP-OF or 0.5% TM-OF, with or without 0.1% MPCP, for 120 s. After exposure, Cell Count Reagent SF was added, and the absorbance at 490 nm was measured using a microplate reader. Cell viability was determined according to the manufacturer’s protocol, and is expressed in Eq. (1):

Evaluation of in vivo Corneal Toxicity of TM@MPCP-OF Using Rat Eye
To assess the corneal toxicity of this formulation, we conducted toxicity evaluations under more stringent conditions than usual, using an instillation frequency of five times per day. Briefly, thirty microliters of saline, 0.1% MPCP-OF, 0.5% TM-OF, or 0.5% TM@MPCP-OF were instilled into the eyes of the rats five times daily (at 9:00, 12:00, 15:00, 18:00, and 21:00) for 14 consecutive days. Following treatment, the corneal wound areas were assessed by staining with 1% fluorescein and imaging using a TRC-50X fundus camera equipped with a digital camera (Topcon; Tokyo, Japan).33
Ocular Surface Retention of TM@MPCP-OF
Rabbits were randomly divided into three groups (n = 7 per group), and 30 µL of TM-OF and TM@MPCP-OF were instilled into the eyes. Tear fluid was collected using Schirmer test strips at 15 and 60 min after instillation, and the TM concentration in the tear samples was quantified by HPLC, as described above. In addition, the 30 µL of TM-OF and TM@MPCP-OF were instilled into the rat eyes, and the animals were euthanized by intraperitoneal administration of pentobarbital (200 mg/kg) at 15 and 60 min after instillation. The TM content in the isolated corneal tissues was measured by HPLC as described above.
In vitro Transcorneal Penetration of TM@MPCP-OF
The corneas were excised from 7-week-old Wistar rats (n = 14) that were randomly assigned to two groups (n = 7 per group). The animals were euthanized by intraperitoneal administration of pentobarbital (200 mg/kg), and the isolated corneal tissues were mounted onto Franz diffusion cells. The receptor compartment (12.2 mL) was filled with 0.2 mM phosphate buffer (pH 7.2) and maintained at 37°C. The TM-OF, with or without MPCP, was uniformly applied to the corneal surface. At predetermined time points, 100 µL aliquots were withdrawn from the receptor chamber for HPLC analysis described above. The cumulative transcorneal drug absorption, expressed as the area under the concentration–time curve from 0 to 90 min (AUCpenetration), was calculated using the trapezoidal integration method.33,34
In vivo Transcorneal Penetration of TM-OF with or without MPCP
The rabbits were randomly assigned to four groups (n = 7 per group). Thirty microliters of 0.25% or 0.5% TM-OF, with or without MPCP, were instilled into the eyes, and 5 µL samples of aqueous humor were collected at designated time points over 90 min. The concentrations of TM were measured by HPLC as described above. The area under the concentration–time curve from 0 to 90 min (AUCAH) was calculated using the trapezoidal integration method.33,34
IOP in Rabbits Instilled with TM-OF with or without MPCP
Rabbit models were used to evaluate the effects of the formulations on IOP. An elevated IOP was induced by rapid intravenous infusion of a 5% glucose solution via the marginal ear vein (15 mL/kg body weight).36 All infusions were completed within 20s. IOP measurements were performed under topical anesthesia with 0.4% benoxil using TonoPen XL (Medtronic SOLAN, FL, USA). Following instillation of 30 µL of the OF containing TM, IOP was recorded at 5–20 min intervals over a 90-min period. The change in intraocular pressure (ΔIOP) was calculated as the difference between the measured IOP and baseline IOP at the start of the experiment. The area under the ΔIOP–time curve from 0 to 90 min (AUCΔIOP) was calculated using the trapezoidal integration method.33,34
Statistical Analysis
All data are presented as the mean ± standard error (S.E). The sample size (n) represents the number of independent biological samples (eg., different formulations, cell-culture wells, or animals), as indicated in each figure legend. To further assess the adequacy of the analyses, effect sizes (Cohen’s d) were calculated from the obtained data. For datasets subjected to statistical analyses, the results indicated that the statistical power exceeded 0.8. Statistical analyses were performed using the JMP software version 5.1 (SAS Institute, Cary, NC, USA). Differences between the two groups were assessed using Student’s t-test, whereas comparisons among multiple groups were analyzed by one-way analysis of variance (ANOVA) followed by the Tukey–Kramer post-hoc test. Homogeneity of variance was evaluated using an F-test for two-group comparisons and Levene’s test for multiple-group comparisons. A value of P < 0.05 was considered statistically significant. Normality was assessed using graphical methods (Q–Q plots), which were visually inspected. The results indicated no substantial deviation from normality, supporting the use of subsequent parametric analyses.
Results
Effect of MPCP Combination on Characteristics and Ophthalmic Safety of TM-OF
TM is widely used as an antiglaucoma agent clinically. In this study, we investigated the potential benefits of incorporating MPCP into a TM-OF. Figure 1A shows the chemical structure of the MPCP, and Figures 1B–F physicochemical properties of the TM@MPCP-OF. Visual inspection revealed that the MPCP aqueous solution was clear, and no precipitation or turbidity was observed in TM@MPCP-OF (Figure 1B). On the other hand, the MPCP alone formed colloidal particles with an average size of 80.7 nm (Figure 1C). The particle size distribution and morphology of these colloidal particles were altered by TM incorporation, and the particle size increased (mean particle size: 159.0 nm, Figure 1D and E). The viscosities of TM and MPCP alone were 1.06 mPa∙s and 0.95 mPa∙s, respectively, and these values remained unchanged in the TM@MPCP-OF formulation (Figure 1F). Ensuring ocular surface safety is critical for the development of OF. In this case, the osmotic pressure was isotonic in all formulations (TM@MPCP-OF 295 ± 9 mOsm). Therefore, we evaluated the cytotoxicity of HCE-T cells (Figure 2A) and corneal damage (Figure 2B) following repeated instillation in rats (Figure 2). Treatment with TM-OFs alone induced cell death in HCE-T cells, whereas treatment with MPCP-OFs alone demonstrated no cytotoxicity (Figure 2A). Furthermore, the incorporation of MPCP into TM mitigated TM-induced cytotoxicity (Figure 2A). In addition, repetitive instillation (five times/day) for 1 week in rats caused no detectable corneal damage to any of the formulations tested (Figure 2B). These findings demonstrate that TM@MPCP-OF ensures ocular safety and suggest its potential application as an OF.
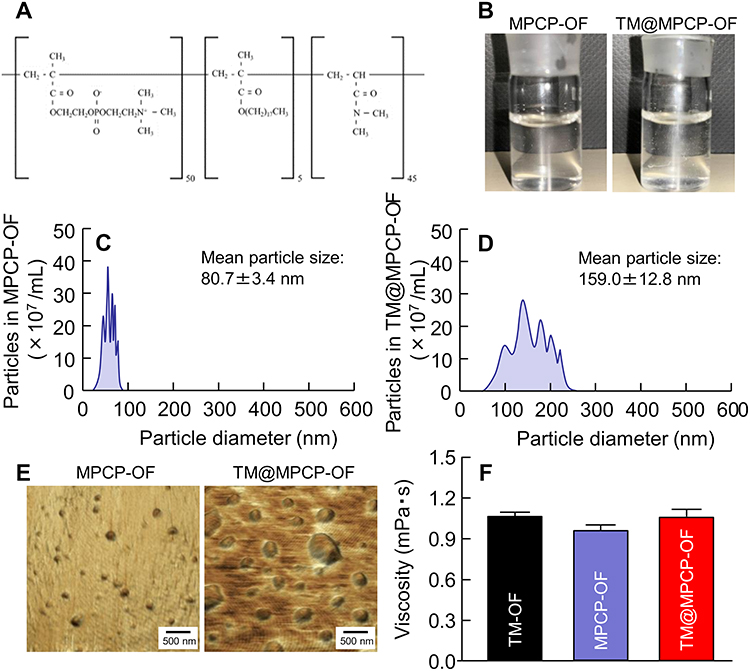 |
Figure 1 Physicochemical properties of MPCP and TM@MPCP-OF. (A) Structure of the formulated MPCP. (B) Digital image of MPCP-OF and TM@MPCP-OF. (C and D) Particle distribution of MPCP-OF (C) and TM@MPCP-OF (D). (E) SPM image of MPCP-OF and TM@MPCP-OF. (F) Viscosity of TM-OF, MPCP-OF, and TM@MPCP-OF. n = 5, *P < 0.05 vs. TM-OF for each category. The TM-OF containing MPCP was transparent. The MPCP particles in TM@MPCP were higher than those of MPCP-OP without TM, and the particle size was 50 to 250 nm. The viscosity remained constant regardless of the presence or absence of MPCP. |
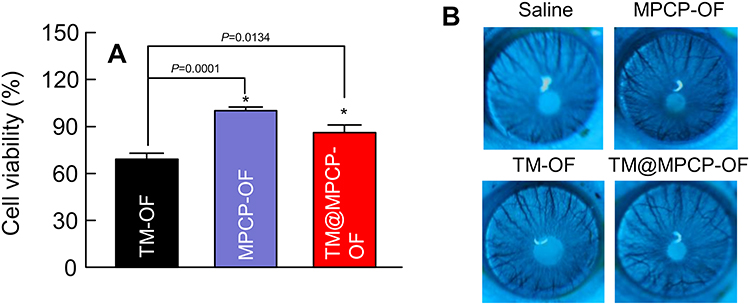 |
Figure 2 Ocular toxicity of MPCP-OF and TM@MPCP-OF. (A) Cytotoxicity in HCE-T cells treated with MPCP-OF, TM-OF, and TM@MPCP-OF. (B) Corneal damage in rats following five-daily instillation for 1 week. n = 7, *P < 0.05 vs. TM-OF for each category (Tukey–Kramer post-hoc test). The combination of MPCP reduced the corneal cytotoxicity of the TM-OF. Moreover, no corneal damage was observed following repeated instillation of TM@MPCP-OF. |
Ocular Absorption of TM in the Instillation of TM-OF with or without MPCP
The antiglaucoma drug TM must remain on the ocular surface within the tear fluid after instillation, penetrate the cornea, and subsequently reach the aqueous humor to exert its IOP-lowering effect. Figure 3 shows the evaluation of ocular surface retention in rabbits (Figure 3A) and corneal drug uptake in rats (Figure 3B). The results demonstrated that the ocular surface concentration and corneal drug content of TM@MPCP-OF at 15 min after instillation were 3.93- and 1.23-fold higher, respectively, than those of TM-OF. These findings indicate that the incorporation of MPCP not only enhanced the ocular surface retention of TM-OF (Figure 3A) but also significantly increased corneal uptake (Figure 3B). Figure 4 presents the corneal permeability of the TM-OF with and without MPCP using excised rat corneas. During the first hour of the experiment, the corneal permeability of TM-OF was comparable between the two formulations; however, after that point, TM@MPCP-OFs exhibited markedly higher permeability (Figure 4A). The AUCpenetration value of TM@MPCP-OF was two-fold greater than that of TM-OF (Figure 4B). Figure 5 shows the intraocular penetration of TM when administered at two different concentrations [0.25% (Figure 5A) and 0.5% (Figure 5B)] with or without MPCP. Increasing the TM concentration from 0.25% (AUCpenetration 342.3 µM/min) to 0.5% (AUCpenetration 365.8 µM/min) caused no substantial change in intraocular penetration (Figure 5A–C). In contrast, the incorporation of MPCP significantly enhanced intraocular penetration, which is consistent with the findings of ocular surface retention, corneal concentration, and corneal permeability. The AUCAH increased 1.4-fold upon MPCP addition in 0.25% TM-OF, whereas the AUCAH increased 1.9-fold in 0.5% TM-OF, indicating that the effect of MPCP was more pronounced at higher TM concentrations (Figure 5C).
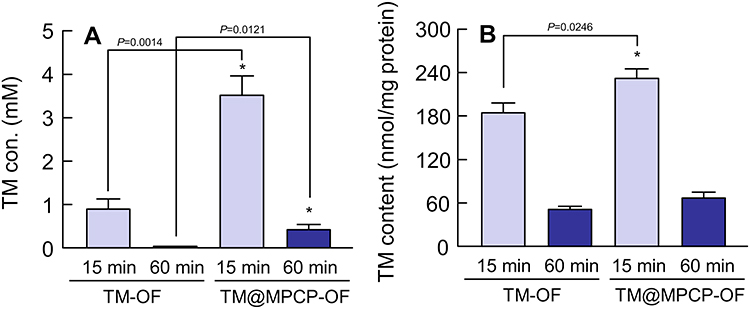 |
Figure 3 Ocular surface retention of TM-OF and TM@MPCP-OF. (A) Changes in TM concentrations in the tear fluid of the rabbit at 15 min and 60 min after instillation of TM-OF and TM@MPCP-OF. (B) Changes in TM levels in rat cornea at 15 min and 60 min after the instillation of TM-OF and TM@MPCP-OF. n = 7, *P < 0.05 vs. TM-OF for each category (Tukey–Kramer post-hoc test). The incorporation of MPCP enhanced the ocular surface retention of TM. Moreover, the corneal TM content at 15 min after instillation was increased by the combination of MPCP. |
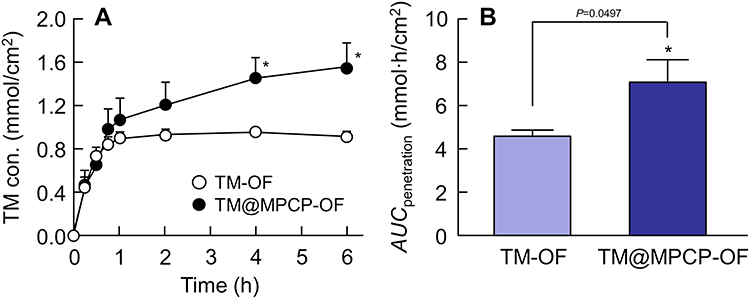 |
Figure 4 In vitro corneal permeability of TM-OF and TM@MPCP-OF in rats. (A and B) Changes in permeation behavior (A) and AUCpenetration (B) after TM-OF and TM@MPCP-OF treatments. n = 7, *P < 0.05 vs. TM-OF for each category (Figure 4A; Tukey–Kramer post-hoc test, Figure 4B; Student’s t-test). No difference in corneal permeability was observed between the formulations with and without MPCP up to 60 min after the start of the experiment; however, a significant increase in corneal permeability was observed in the TM@MPCP-OF group than in the TM-OF group. |
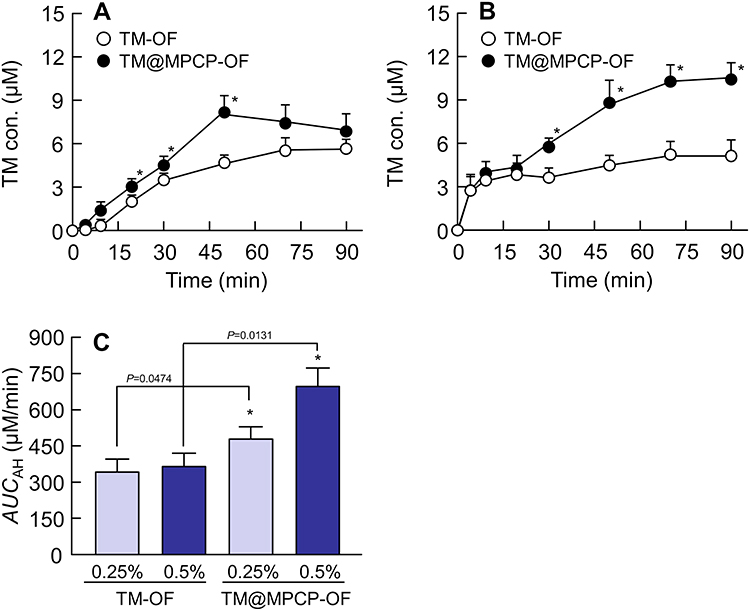 |
Figure 5 Changes in TM concentration in rabbit aqueous humor after instillation of TM-OF and TM@MPCP-OF. (A and B) TM concentration profiles in rabbit aqueous humor after instillation of 0.25% (A) and 0.5% (B) TM-OF and TM@MPCP-OFs. (C) AUCAH values after the instillation of 0.25% and 0.5% TM-OF and TM@MPCP-OF, n = 7, *P < 0.05 vs. TM-OF for each category (Tukey–Kramer post-hoc test). No significant difference in drug penetration into the aqueous humor was observed during the early phase after instillation; however, from 20 min onward, the amount of TM transferred into the aqueous humor significantly increased with the addition of MPCP. The enhancing effect of MPCP on the corneal permeability of the TM was more pronounced in the 0.5% TM-OF group than in the 0.25% TM-OF group. |
Effect of TM-OF with or without MPCP on IOP in the High-IOP Rabbit Model Induced by the Rapid Infusion of a 5% Glucose Solution
As the incorporation of MPCP enhanced the intraocular penetration of TM-OF, we evaluated the IOP-lowering effect of TM using a high-IOP rabbit model induced by rapid infusion of a 5% glucose solution. Figure 6A and B show the results obtained when 5% glucose solution was administered immediately after instillation. TM-OF significantly inhibited IOP elevation induced by a 5% glucose solution (Figure 6A). In addition, TM@MPCP-OF exhibited a strong IOP-lowering effect; however, its AUCΔIOP was comparable to that of TM-OF without MPCP (Figure 6B). To further evaluate the sustained effect of MPCP incorporation, we examined the results when a 5% glucose solution was administered 2 h after instillation (Figure 6C and D). IOP gradually increased in the TM-OF-treated group following the administration of the 5% glucose solution (Figure 6C), and its AUCΔIOP was 611 mmHg∙min (Figure 6D). In contrast, TM@MPCP-OF maintained a significant IOP-lowering effect 2 h after instillation (Figure 6C), and the AUCΔIOP of TM@MPCP-OF was 39.0% that of TM-OF without MPCP (Figure 6D).
 |
Figure 6 Effect of TM-OF and TM@MPCP-OF instillation on IOP in rabbits with acute ocular hypertension. High IOP model of rabbits was induced by rapid intravenous infusion of a 5% glucose solution (Control). (A–D) The ΔIOP (A and C) and AUCΔIOP (B and D) of TM-OF and TM@MPCP-OF immediately after instillation (A and B) and 2 h after instillation (C and D), n = 7, *P < 0.05 vs. control for each category, #P < 0.05 vs. TM-OF for each category (Figure 6A–C; Tukey-Kramer post-hoc test, Figure 6D; Student’s t-test). The combination with MPCP prolonged the duration of the IOP-lowering effects of TM-OF. The AUCΔIOP in the high IOP model induced by glucose loading 2 h after TM@MPCP-OF instillation was 39.0% of that of the TM-OP without MPCP. |
Discussion
We previously designed MPCP, a polymer containing both a zwitterionic group derived from stearyl methacrylate and an acrylic group, and found that it exhibited a high affinity for water and enhanced moisture retention on the ocular surface.32 Furthermore, we demonstrated that the topical application of MPCP has potential as an effective treatment for dry eye disease. In the present study, we revealed that the co-administration of this MPCP with the antiglaucoma drug TM enhanced the ocular surface residence time, corneal permeability, and pharmacological efficacy (ie., IOP-lowering effect) of TM.
MPCP was prepared as described in our previous report using 2-methacryloyloxyethyl phosphorylcholine, stearyl methacrylate, and N,N-dimethylacrylamide, followed by purification via dialysis. Nanoparticles larger than 30 nm, which were not detected in the conventional MPCP-BMA,32 were observed in this MPCP preparation. As previously reported, the MPCP contained micelle-like monomeric structures (polymer nanospherules) with particle sizes ranging from 50 to 250 nm.32 These nanoparticles were also detected in MPCP when TM was incorporated, although the particle size increased with the addition of TM (Figures 1C–E). The viscosity and osmotic pressure of MPCP were 0.96 mPa·s and remained constant regardless of the presence or absence of TM (Figure 1F). In addition, the osmotic pressure of TM-OF, MPCP-OF, and TM@MPCP-OF were 293 ± 9 mOsm/L, 288 ± 5 mOsm/L, and 295 ± 9 mOsm/L, respectively. The increase in the MDPI particle size may be attributed to the encapsulation of TM. Further studies are required to confirm this hypothesis.
Ensuring the safety of OFs is crucial for their clinical application. Therefore, the ocular toxicity was evaluated both in vitro using HCE-T cells and in vivo through direct instillation into rat eyes (Figure 2). Treatment with TM-OF reduced the viability of HCE-T cells by 69.1%. Because TM-OF typically contain 0.005% BAC as a preservative, and BAC is known to exert cytotoxic effects, it is likely that BAC strongly contributed to the observed toxicity in HCE-T cells (cell viability of BAC, 73.4 ± 4.9%, mean ± S.E., n = 6). In contrast, MPCP-OFs alone exhibited almost no cytotoxicity toward HCE-T cells. Furthermore, the combination of MPCP and TM significantly reduced the cytotoxicity induced by TM-OF. Because of their biocompatibility, MPCP should exhibit low toxicity. MPCP exerts a protective effect on the cell membrane and reduces the cytotoxicity of BAC.30 Thus, tolerability may be attenuated when a combination of MPCP and a preservative is used. Furthermore, in vitro studies using cultured cells and in vivo experiments using rats were conducted to evaluate the ocular toxicity when MPCP was co-administered with TM. As shown in Figure 2B, no corneal damage was observed even after frequent instillation. These results indicate that the incorporation of MPCP into TM-OF poses no safety concerns.
Next, we investigated the effects of MPCP incorporation on the ocular pharmacokinetics of TM-OF after instillation, focusing on the ocular surface, cornea, and aqueous humor. A prolonged drug retention on the ocular surface was observed in the TM@MPCP-OF group than in the TM-OF alone group (Figure 3A). Moreover, TM levels within the cornea and the amount of TM that penetrated the aqueous humor were significantly increased by the addition of MPCP (Figure 4). In a previous study using rebamipide, MPCP maintained a micellar-like structure in aqueous environments, thereby enhancing its ocular surface retention.32 Consistent with this finding, the present results demonstrated improved retention of TM-OF on the ocular surface, suggesting that this effect contributes to the enhanced penetration of TM into the aqueous humor observed in the in vivo rabbit model.
Therefore, we examined whether the incorporation of MPCP enhanced the pharmacological effects of TM-OF, namely, its IOP-lowering activity after instillation. The selection of an appropriate animal model is crucial for evaluating IOP-lowering effects. The intravenous administration of an isotonic glucose solution is a simple and highly reproducible method for screening antiglaucoma agents.37 Therefore, the IOP-lowering effect of the TM@MPCP-OF was evaluated using an experimental glaucoma model (Figure 6). When a 5% glucose solution was administered intravenously, the IOP of the rabbits rapidly increased, reaching a peak 20 min after injection and then gradually declined. This convenient and reproducible method can be used to screen antiglaucoma agents.37 The mechanism of IOP elevation in this model has been reported to involve the rapid infusion of an isotonic glucose solution, which decreases blood osmotic pressure and induces fluid movement into the eye. The rapid production of aqueous humor consequently increases IOP.38 Because TM reduces IOP by suppressing aqueous humor production, the IOP elevation model is often used to evaluate TM efficacy. Topical instillation of TM@MPCP-OF, similar to TM-OF, significantly suppressed the glucose-induced increase in IOP compared to that in the control group; however, no significant difference was noted between OF with and without MPCP (Figure 6A and B). These findings indicate that the acute glaucoma rabbit model is simple and useful for screening purposes, but also suggest that under such conditions, the effect of MPCP cannot be properly evaluated. Therefore, TM-OF, with or without MPCP, was administered 120 min before intravenous injection of the isotonic glucose solution to assess the effect of MPCP under more appropriate conditions, and changes in IOP were monitored. The AUCΔIOP value of TM@MPCP-OF was significantly higher than that of TM-OF without MPCP (Figure 6C and D). These results may demonstrate that under properly optimized experimental conditions, the retention properties of the formulations can be evaluated. Moreover, the co-administration of MPCP enhanced the effect of TM in the animal model (Figure 6C), and the 2.56-fold increase in AUCΔIOP value (Figure 6D) is considered meaningful not only in terms of statistical significance but also in terms of biological relevance. Furthermore, consistent with the results for TM concentrations in the aqueous humor (Figure 5), these results suggested that the inclusion of MPCP enhanced the pharmacological efficacy of TM. It is possible that this study suggests that topical administration of TM@MPCP-OF could serve as an effective therapeutic for patients with glaucoma. It is important to clarify the mechanism for enhancement of retention and permeability by MPCP combination. The corneal epithelium, which constitutes the outermost surface of the cornea, is hydrophobic and acts as a barrier to drug permeation. In addition, after instillation, drugs are rapidly washed away from the ocular surface by tear fluid, resulting in only limited retention on the corneal epithelium. In contrast, MPCP is amphiphilic and is therefore likely to adhere to the corneal epithelium, while also exhibiting affinity for the hydrophilic drug used in this study. Accordingly, the observed increases in ocular surface retention and corneal permeability of TM upon the addition of MPCP may be attributed, at least in part, to an indirect enhancement of the affinity between the drug and the corneal epithelium mediated by MPCP. However, further studies are required to elucidate the precise mechanism by which co-administration of MPCP enhances the corneal permeability of TM-OF. In addition, this study has several limitations, including the validity of the animal model, the short study duration, and the presence of benzalkonium chloride. Especially, the short-term experimental timeframe is suitable for initial pharmacokinetic and pharmacodynamic assessment but limits conclusions regarding long-term efficacy. To address this, we investigated the effects of MPCP on the tight junctions of corneal epithelial cells using histological approaches. In addition, ongoing studies have examined the influence of MPCP-containing TM-OF on aqueous humor production and outflow during the circadian cycle.39,40
Conclusion
The use of MPCP as an ophthalmic additive enhanced the ocular surface retention and corneal permeability of 0.5% TM-OF, thereby prolonging the duration of their IOP-lowering effect in a rabbit model. Furthermore, topical application of MPCP demonstrated minimal toxicity to the ocular surface. These findings provide valuable insights for the future design and development of improved formulations of antiglaucoma medications. In the present study, TM was used as a model drug; however, we plan to investigate other anti-glaucoma agents in future studies. If similar results are obtained with these formulations, it may become possible to reduce the dosing frequency of glaucoma medications to once daily, thereby improving patient compliance and adherence. On the other hand, as the present findings are still at the animal experimental stage, further investigation is required.
Abbreviations
AFM, atomic force microscopy; AUCAH, the area under the timolol maleate concentration–time curve in aqueous humor; AUCΔIOP, the area under the Δintraocular pressure–time curve; AUCpenetration, the area under the concentration–time curve for cornea-penetrated timolol maleate; BAC, benzalkonium chloride; HCE-T, human corneal epithelial cell line; HPLC, high-performance liquid chromatography; IOP, intraocular pressure; MPC, 2-methacryloyloxyethyl phosphorylcholine; MPCP, 2-methacryloyloxyethyl phosphorylcholine-based polymer incorporating a zwitterionic; OF, ophthalmic formulation; SE, standard error; SPM, scanning probe microscope; TM, timolol maleate; TM@MPCP, ophthalmic formulations incorporating MPCP and benzalkonium chloride into TM solution.
Data Sharing Statement
The data generated in the present study may be requested from the corresponding author.
Ethics Approval
All animal experiments were performed in accordance with the guidelines of Kindai University, the Japanese Pharmacological Society, and the National Institutes of Health (NIH). The experimental protocols were approved on April 1, 2024, by the Kindai University under project identification codes KAPS-2024-008 and KAPS-2024-009, and the study was conducted in compliance with the ARRIVE and AVMA euthanasia guidelines, 2020.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
Author Ayano Sasaki, Ryuya Gotanda and Yosuke Matsuoka are affiliated with a company NOF CORPORATION but has no potential interest relationship. The authors report no other conflicts of interest in this work.
References
1. Kumara BN, Shambhu R, Prasad KS. Why chitosan could be apt candidate for glaucoma drug delivery - an overview. Int J Biol Macromol. 2021;176:47–12. doi:10.1016/j.ijbiomac.2021.02.057
2. The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7. the relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130(4):429–440. doi:10.1016/S0002-9394(00)00538-9
3. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–267. doi:10.1136/bjo.2005.081224
4. Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Arch Ophthalmol. 2002;120(10):1268–1279. doi:10.1001/archopht.120.10.1268
5. Kass MA, Heuer DK, Higginbotham EJ, et al. The ocular hypertension treatment study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):701–713. doi:10.1001/archopht.120.6.701
6. Lee DA, Higginbotham EJ. Glaucoma and its treatment: a review. Am J Health Syst Pharm. 2005;62(7):691–699. doi:10.1093/ajhp/62.7.691
7. Gupta B, Mishra V, Gharat S, Momin M, Omri A. Cellulosic polymers for enhancing drug bioavailability in ocular drug delivery systems. Pharmaceuticals. 2021;14(11):1201. doi:10.3390/ph14111201
8. Costagliola C, dell’Omo R, Romano MR, Rinaldi M, Zeppa L, Parmeggiani F. Pharmacotherapy of intraocular pressure – part II. carbonic anhydrase inhibitors, prostaglandin analogues and prostamides. Expert Opin Pharmacother. 2009;10(17):2859–2870. doi:10.1517/14656560903300129
9. Stamper RL, Wigginton SA, Higginbotham EJ. Primary drug treatment for glaucoma: beta-blockers versus other medications. Surv Ophthalmol. 2002;47(1):63–73. doi:10.1016/S0039-6257(01)00286-7
10. Sah AK, Suresh PK. Medical management of glaucoma: focus on ophthalmologic drug delivery systems of timolol maleate. Artif Cells Nanomed Biotechnol. 2017;45(3):448–459. doi:10.3109/21691401.2016.1160917
11. Cuggino JC, Tártara LI, Gugliotta LM, Palma SD, Alvarez Igarzabal CI. Mucoadhesive and responsive nanogels as carriers for sustainable delivery of timolol for glaucoma therapy. Mater Sci Eng C Mater Biol Appl. 2021;118:111383. doi:10.1016/j.msec.2020.111383
12. Singh A, Dogra TS, Mandal UK, Narang RK. Novel approaches for ocular drug delivery: a review. Int J Bio-Pharma Res. 2019;8(7):2722–2732.
13. Pontillo ARN, Detsi A. Nanoparticles for ocular drug delivery: modified and nonmodified chitosan as a promising biocompatible carrier. Nanomedicine. 2019;14(14):1889–1909. doi:10.2217/nnm-2019-0040
14. Yadav M, Guzman-Aranguez A, Perez de Lara MJ, Singh M, Singh J, Kaur IP. Bimatoprost loaded nanovesicular long-acting sub-conjunctival in-situ gelling implant: in vitro and in vivo evaluation. Mater Sci Eng C Mater Biol Appl. 2019;103:109730. doi:10.1016/j.msec.2019.05.015
15. Ahmad I, Pandit J, Sultana Y, Mishra AK, Hazari PP, Aqil M. Optimization by design of etoposide loaded solid lipid nanoparticles for ocular delivery: characterization, pharmacokinetic and deposition study. Mater Sci Eng C Mater Biopl Appl. 2019;100:959–970. doi:10.1016/j.msec.2019.03.060
16. Shokry M, Hathout RM, Mansour S. Exploring gelatin nanoparticles as novel nanocarriers for timolol maleate: augmented in-vivo efficacy and safe histological profile. Int J Pharm. 2018;545(1–2):229–239. doi:10.1016/j.ijpharm.2018.04.059
17. Bhattacharjee A, Das PJ, Adhikari P, et al. Novel drug delivery systems for ocular therapy: with special reference to liposomal ocular delivery. Eur J Ophthalmol. 2018;29(1):113–126. doi:10.1177/1120672118769776
18. Tan G, Yu S, Pan H, et al. Bioadhesive chitosan-loaded liposomes: a more efficient and higher permeable ocular delivery platform for timolol maleate. Int J Biol Macromol. 2017;94(Pt A):355–363. doi:10.1016/j.ijbiomac.2016.10.035
19. Ilka R, Mohseni M, Kianirad M, Naseripour M, Ashtari K, Mehravi B. Nanogel-based natural polymers as smart carriers for the controlled delivery of timolol male ate through the cornea for glaucoma. Int J Biol Macromol. 2018;109:955–962. doi:10.1016/j.ijbiomac.2017.11.090
20. Almeida H, Amaral MH, Lobão P, Silva AC, Loboa JMS. Applications of polymeric and lipid nanoparticles in ophthalmic pharmaceutical formulations: present and future considerations. J Pharm Sci. 2014;17(3):278–293.
21. Ishihara K, Takai M. Bioinspired interface for nanobiodevices based on phospholipid polymer chemistry. J R Soc Interface. 2009;6 Suppl 3(Suppl 3):S279–291. doi:10.1098/rsif.2008.0335
22. Ishihara K, Aragaki R, Ueda T, Watenabe A, Nakabayashi N. Reduced thrombogenicity of polymers having phospholipid polar groups. J Biomed Mater Res. 1990;24(8):1069–1077. doi:10.1002/jbm.820240809
23. Iwasaki Y, Sawada S, Ishihara K, Khang G, Lee HB. Reduction of surface-induced inflammatory reaction on PLGA/MPC polymer blend. Biomaterials. 2002;23(18):3897–3903. doi:10.1016/S0142-9612(02)00135-7
24. Sawada S, Sakaki S, Iwasaki Y, Nakabayashi N, Ishihara K. Suppression of the inflammatory response from adherent cells on phospholipid polymers. J Biomed Mater Res A. 2003;64(3):411–416. doi:10.1002/jbm.a.10433
25. Ye SH, Watanabe J, Iwasaki Y, Ishihara K. Antifouling blood purification membrane composed of cellulose acetate and phospholipid polymer. Biomaterials. 2003;24(23):4143–4152. doi:10.1016/S0142-9612(03)00296-5
26. Goda T, Matsuno R, Konno T, Takai M, Ishihara K. Protein adsorption resistance and oxygen permeability of chemically crosslinked phospholipid polymer hydrogel for ophthalmologic biomaterials. J Biomed Mater Res B Appl Biomater. 2009;89(1):184–190. doi:10.1002/jbm.b.31204
27. Goda T, Ishihara K. Soft contact lens biomaterials from bioinspired phospholipid polymers. Expert Rev Med Devices. 2006;3(2):167–174. doi:10.1586/17434440.3.2.167
28. Okajima Y, Saika S, Sawa M. Effect of surface coating an acrylic intraocular lens with poly(2-methacryloyloxyethyl phosphorylcholine) polymer on lens epithelial cell line behavior. J Cataract Refract Surg. 2006;32(4):666–671. doi:10.1016/j.jcrs.2006.01.039
29. Liu W, Deng C, McLaughlin CR, et al. Collagen-phosphorylcholine interpenetrating network hydrogels as corneal substitutes. Biomaterials. 2009;30(8):1551–1559. doi:10.1016/j.biomaterials.2008.11.022
30. Minami M, Yamaguchi M, Yamazaki Y, et al. Effect of MPC polymer on corneal toxicity and corneal drug permeation of benzalkonium chloride in corneal epithelial cells. J Eye. 2020;37(10):1309–1314.
31. Ayaki M, Iwasawa A, Niwano Y. Cytotoxicity assays of new artificial tears containing 2-methacryloyloxyethyl phosphorylcholine polymer for ocular surface cells. Jpn J Ophthalmol. 2011;55(5):541–546. doi:10.1007/s10384-011-0073-8
32. Nagai N, Sakurai S, Seiriki R, et al. MPC polymer promotes recovery from dry eye via stabilization of the ocular surface. Pharmaceutics. 2021;13(2):168. doi:10.3390/pharmaceutics13020168
33. Otake H, Kobayashi K, Kadowaki R, et al. Copolymerized polymers based on cyclodextrins and cationic groups enhance therapeutic effect of rebamipide in the N-acetylcysteine-treated dry eye model. Drug Des Devel Ther. 2024;18:4345–4358. doi:10.2147/DDDT.S469445
34. Nagai N, Ogata F, Otake H, et al. Co-instillation of nano-solid magnesium hydroxide enhances corneal permeability of dissolved timolol. Exp Eye Res. 2017;165:118–124. doi:10.1016/j.exer.2017.10.002
35. Araki-Sasaki K, Ohashi Y, Sasabe T, et al. An SV40-immortalized human corneal epithelial cell line and its characterization. Invest Ophthalmol Vis Sci. 1995;36:614–621.
36. Nagai N, Yoshioka C, Mano Y, Ito Y, Okamoto N, Shimomura Y. Effect of eye drops containing disulfiram and low-substituted methylcellulose in reducing intraocular pressure in rabbit models. Curr Eye Res. 2015;40(10):990–1000. doi:10.3109/02713683.2014.971187
37. Bonomi L, Tomazzoli L, Jaria D. An improved model of experimentally induced ocular hypertension in the rabbit. Invest Ophthalmol. 1976;15(9):781–784.
38. Shah GB, Sharma S, Mehta AA, Goyal RK. Oculohypotensive effect of angiotensin-converting enzyme inhibitors in acute and chronic models of glaucoma. J Cardiovasc Pharmacol. 2000;36(2):169–175. doi:10.1097/00005344-200008000-00005
39. Kiel JW. Modulation of choroidal autoregulation in the rabbit. Exp Eye Res. 1999;69(4):413–429. doi:10.1006/exer.1999.0717
40. McLaren JW, Trocme SD, Relf S, Brubaker RF. Rate of flow of aqueous humor determined from measurements of aqueous flare. Invest Ophthalmol Vis Sci. 1990;31(2):339–346.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol in Glaucoma and Ocular Hypertension in India: A Multicenter, Open-Label, Phase 3 Study
Menon MG, Goodkin ML
Clinical Ophthalmology 2022, 16:3559-3569
Published Date: 20 October 2022
Trabeculectomy Vs Non‐penetrating Deep Sclerectomy for the Surgical Treatment of Open-Angle Glaucoma: A Long-Term Report of 201 Eyes
Correia Barbosa R, Gonçalves R, Bastos R, Alves Pereira S, Basto R, Viana AR, Tenedório P
Clinical Ophthalmology 2023, 17:1619-1627
Published Date: 6 June 2023