Back to Journals » Cancer Management and Research » Volume 18

Clinicopathological Features and Prognostic Differences Between Primary and Relapsed or Refractory Extramedullary Multiple Myeloma
Authors Hu X, Yang M, Qi Y, Dai X, Zhou J, Li Y, Zhao H, Li X, Jin M
Received 13 August 2025
Accepted for publication 25 January 2026
Published 5 February 2026 Volume 2026:18 552024
DOI https://doi.org/10.2147/CMAR.S552024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shari Youngblood
Xiumei Hu,1 Meng Yang,1 Yanan Qi,1 Xiangyang Dai,2 Jun Zhou,3 Yunlong Li,1 Hongying Zhao,1 Xue Li,1 Mulan Jin1
1Department of Pathology, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Pathology, Anhui Chest Hospital, Anhui, People’s Republic of China; 3Department of Pathology, Zigong Fourth People’s Hospital, Sichuan, People’s Republic of China
Correspondence: Mulan Jin, Department of Pathology, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China, Tel +86 10 8523146, Email [email protected]
Purpose: This study aims to explore the clinicopathological features related to extramedullary multiple myeloma (EMM) occurrence and evaluate prognosis differences between patients with primary EMM (PEMM) and those with relapsed or refractory EMM (R/REMM).
Patients and Methods: The laboratory test results, clinical, histopathological and immunophenotypic characteristics, cytogenetic changes and prognosis of 203 patients with MM were obtained. The patients were categorized into EMM+ and EMM- groups. Patients in the EMM+ group were further categorized into the PEMM and R/REMM groups based on the time of EMM occurrence, for further comparison.
Results: The incidence of EMM was 24.6% (50/203). Further classification of EMM showed that the incidence of PEMM was 16.3% (33/203), that of R/REMM was 8.4% (17/203).The proportion of CD20+ was significantly lower than that in the EMM- group (2.0% vs 15.0%, P =0.013).In the EMM+ group,70% (35/50) of patients had elevated levels of β 2-MG (≥ 5.5 mmol/L), and 24% (12/50) had elevated levels of serum calcium (> 2.65 mmol/L), higher than that in the EMM− group (41.2% and 12.4%, respectively), and the differences were statistically significant (P < 0.001 and P = 0.049, respectively).Patients with R/REMM were more likely to have plasma cell leukemia and lower albumin levels than those with PEMM (P = 0.021 and 0.014, respectively). The median OS of patients in the EMM- group was longer than that of patients in the EMM+ group (59.6 vs 47.0 months, P=0.197).The median OS of patients in the PEMM group was longer than that of patients in the R/REMM group and the difference was statistically significant (53.3 vs 30.5 months,P= 0.015). Univariate and multivariate survival analyses revealed that R/REMM is an independent adverse prognostic factor (P = 0.003 and P < 0.001 respectively),and PEMM was not associated with OS in patients with MM (P = 0.503 and P = 0.545, respectively).
Conclusion: R/REMM is an independent adverse prognostic factor for patients with MM. Patients with R/REMM are more likely to have plasma cell leukemia and lower albumin levels.
Keywords: extramedullary multiple myeloma, incidence rate, pathological characteristics, prognosis, overall survival
Introduction
Multiple myeloma (MM) is a malignant tumor characterized by the abnormal proliferation of clonal plasma cells in the bone marrow (BM). Its incidence ranks second among all hematological malignancies.1 It is characterized by a complex genetic background, numerous gene mutations, and significant heterogeneity in prognosis.2 Recently, proteasome inhibitors (PIs), immunomodulatory drugs (IMiDs), and autologous stem cell transplantation (ASCT) have been widely used to treat patients with MM.3,4 These treatment plans significantly prolong the overall survival (OS) and progression-free survival in patients with MM. However, certain patients do not benefit from these treatments. Therefore, accurate risk stratification and prognostic assessment are crucial for achieving personalized treatment and improving the prognosis of patients with MM.
Extramedullary MM (EMM) is an aggressive subtype, characterized by the ability of a subclone to thrive and grow independently of the BM microenvironment.5 EMM has been reported to be associated with escape from apoptosis, resistance to treatment, and poor prognosis in patients with MM.6–8Clinicopathological information, including plasma cell morphology, infiltration patterns, immunophenotypes, and cytogenetic changes, can effectively guide the selection of treatment plans and prognostic evaluations in patients with MM. Our center previously analyzed bone marrow fibrosis (BMF) in 146 patients with MM, and the results showed that the median OS of the BMF+ group (39.1 months; 95% confidence interval [CI]: 34.0–44.3) was shorter than that of the BMF- group (45.4 months; 95% CI: 39.5–51.3).9 However, the relationship between clinicopathological features and EMM remains unclear due to the lack of large-scale clinical studies.
According to the time of occurrence, EMM can be classified into primary EMM (PEMM) and recurrent/refractory EMM (R/REMM), while according to the location of occurrence, EMM can be classified into extramedullary bone related(EMB) and extramedullary extraosseous (EME).10 Previous studies have shown that median OS of EMB was longer than EME (51months vs 26 months, p = 0.0067), suggesting that EMB and EME have significantly different effects on the prognosis of patients with MM.11,12 However, there have been no large-scale studies reporting the difference between PEMM and R/REMM on the prognosis of patients with MM.
The aim of this study is to explore the clinical and pathological features associated with the occurrence of EMM, evaluate the differences in prognosis between PEMM and R/REMM patients, and provide a basis for the selection of treatment plans and prognosis evaluation for MM patients.
Materials and Methods
Case Selection
Pathology data were obtained from the Beijing Chao-Yang Hospital, Capital Medical University, between January 2018 and August 2023. The inclusion criteria were as follows: 1. The diagnostic criteria for MM were based on the 2016 guidelines of the International Myeloma Working Group,13 2. The patients’ clinical data were complete, 3.BM aspiration biopsy was performed on all patients before treatment. This study excluded the following cases: 1) Solitary plasmacytoma. 2) Solitary plasmacytoma with minimal bone marrow infiltration. 3) Plasma cell leukemia without MM.
The baseline medical data of all patients were reviewed from their medical records. Disease parameters included M protein type, light-chain type, Durie–Salmon (D–S) stage, International Staging System (ISS) stage, β2-microglobulin (β2-MG), serum calcium, creatinine, albumin, BM plasma cell infiltration, combined plasma cell leukemia, combined amyloidosis, and proportion of tumor cells in the BM smear.
All patients received standard treatment regimens, including PIs, IMiDs, and ASCT. Patient prognosis was assessed using medical records and telephone follow-ups until December 30, 2024. OS was defined as the time from the date of MM diagnosis to the date of the last follow-up when the patient was alive.
This study was approved by the institutional review board and ethics committee of Beijing Chao-Yang Hospital and was conducted in accordance with requirements in the Declaration of Helsinki.
Hematoxylin and Eosin (H&E) and Immunohistochemical (IHC) Staining and Pathological Diagnosis
Routine pathological evaluation of the BM in patients with MM involves H&E and IHC staining. H&E-stained sections from each patient were reviewed. The diagnoses were independently confirmed by two pathologists, HXM and JML. Only the cases approved by both pathologists were included in this study.
We focused on the following features in the H&E-stained sections: First, the plasma cell morphology was assessed and classified into four types: mature, immature, polymorphic, and plasmablastic.14 Second, the plasma cell burden was assessed based on the proportion of plasma cells in the BM nucleated cells and categorized as mild increase (≤20%), moderate increase (21–50%), and significant increase (>50%). Third, according to the growth pattern of tumor plasma cells in bone marrow tissue, they are divided into interstitial type, nodular type, and diffuse type.15
IHC was performed on formalin-fixed, paraffin-embedded tissues using an UltraView Universal DAB Detection Kit (Ventana Medical Systems; Tucson, AZ, USA) and a BenchMark XT automated immunostainer (Ventana Medical Systems). Proteins CD38 (clone 38CO3), CD138 (clone MAB 0200), MUM1 (clone MX093), kappa (clone RAB-0111), lambda (clone MAB-0357), CD56 (clone ZM-0057), CD20 (clone ZM-0039), cyclin D1 (clone RMA-0541), their reagents, and their primary antibodies were purchased from Fuzhou Maixin Biotech Co. Ltd. (Fuzhou, China).Any proportion of neoplastic plasma cells expressing cyclin D1 suggested that the samples were positive for cyclin D1. CD56 and CD20 positivity was established if more than 30% of the neoplastic plasma cells demonstrated moderate-to-strong expression.
Reticular fiber staining was performed using a silver impregnation kit for reticulin (Artisan Link Pro; Agilent, Santa Clara, CA, USA; Ventana BenchMark Ultra, Ventana Medical Systems) according to the manufacturer’s instructions. Bone marrow fibrosis (BMF) assessment followed the European consensus scoring system, which includes four grades (myelofibrosis [MF]-0 to MF-3).16 This study classified MF-2 and MF-3 as the BMF+group, and MF-0 and MF-1 as the BMF - group.
Interphase Fluorescence in Situ Hybridization (iFISH) Staining
We collected the patients’ BM fluid, added heparin as an anticoagulant, and sorted the fluid using CD138 magnetic beads, followed by iFISH. Mononuclear cells were enriched by the Ficoll–gradient centrifugation (Ficoll-Paque PLUS; GE Healthcare Bio-Sciences AB, Uppsala, Sweden) and were assessed using commercially available probes for the regions containing 4p16 (FGFR3)/14q32 (IGH), 11q13 (CCND1)/14q32 (IGH), 14q32 (IGH)/16q32 (MAF), 1q21, and 17p13.1 (TP53) using Vysis IGH/FGFR3 DF FISH Probe Kit, Vysis IGH/CCND1 DF FISH Probe Kit, Vysis IGH/MAF DF FISH Probe Kit, 1q21 CKS1B Spectrum Orange/1p32CDKN2C Spectrum Green FISH Probe Kit, and Vysis TP53/CEP 17 FISH Probe Kit (Vysis/Abbott Molecular; Des Plaines, IL, USA). Slides containing cells were pretreated, denatured, and hybridized using standard laboratory procedures according to the manufacturer’s instructions (Vysis/Abbott Molecular). For each specimen, 200 interphase cells were analyzed.17 Cases with t (4; 14), t (14; 16), and 17p deletions detected by iFISH are classified as high-risk for cytogenetics.
Characterization of EMM
EMM was diagnosed by physical examination, including whole-body magnetic resonance (MR) or positron emission computed tomography (PET-CT). Biopsies were obtained whenever possible.
EMMs that occurred during the initial diagnosis or treatment course were recorded and categorized as PEMMs or R/REMMs. This study classified the cases of both PEMM and R/REMM into the PEMM category. For patients with R/REMM, we recorded the time of the first occurrence of EMM.
Statistical Analysis
Continuous variables are expressed as medians and ranges, and categorical variables are expressed as absolute frequencies and percentages. IBM SPSS 29.0 (IBM SPSS Inc., Armonk, NY, USA) and GraphPad Prism 9.4 were used for statistical analyses. Chi-square test with Fisher’s exact test, as appropriate, was used to examine the relationships between categorical variables. Univariate and multivariate Cox regression analyses were used to determine the association between clinicopathological characteristics and OS, and Kaplan–Meier survival curves were used to determine the median OS stratified by the presence of EMM. Differences were evaluated using Log rank tests. Statistical significance was set at P < 0.05.
Results
Clinical and Morphological Features
In total, 203 patients with MM were diagnosed and treated in our institution between January 2018 and August 2023. The median age at MM diagnosis was 62 years (range: 29–84 years), and the female/male sex ratio was 1.4:1. Of these, 15 patients were diagnosed with amyloidosis and 13 with plasma cell leukemia.Of the 203 patients, 194 received induction chemotherapy with a combination regimen based on new agents, including PIs and IMiDs; 23 were treated with a PI-based regimen, 2 were treated with an IMiD-based regimen, and 169 were treated with a combination of a PI and an IMiD-based regimen. Among 203 MM patients, 68 underwent ASCT.Follow-up was performed in 165 of 203 patients, of whom 114 survived and 51 died, with a survival period of 1–81 months and a median survival time of 30 months.
The clinicopathological characteristics of 203 patients with MM are shown in Supplementary Table 1. Among these patients, 31 (15.3%) had elevated serum calcium levels (≥ 2.65 mmol/L), and 98 (48.3%) had elevated serum β2-MG levels (≥ 5.5 mmol/L).Cases with DS stage III accounted for 86.2% (175/203), ISS stage III accounted for 62.1% (126/203).
Moreover, 203 patients with MM were classified according to the morphology of tumorigenic plasma cells into mature (41.8%,85/203), immature (42.3%,86/203), polymorphic (1.4%,3/203), and plasmablastic (14.2%,29/203) types. The predominant growth pattern of the tumor cells was diffuse (58.1%,118/203). The positivity rates for CD20, cyclin D1, and CD56 were 11.8% (24/203), 23.1% (47/203), and 46.3% (94/203), respectively, and the incidence rate of BMF was 59.1% (120/203). Figure 1 shows typical pathological morphologies and immunophenotypes of patients with MM.
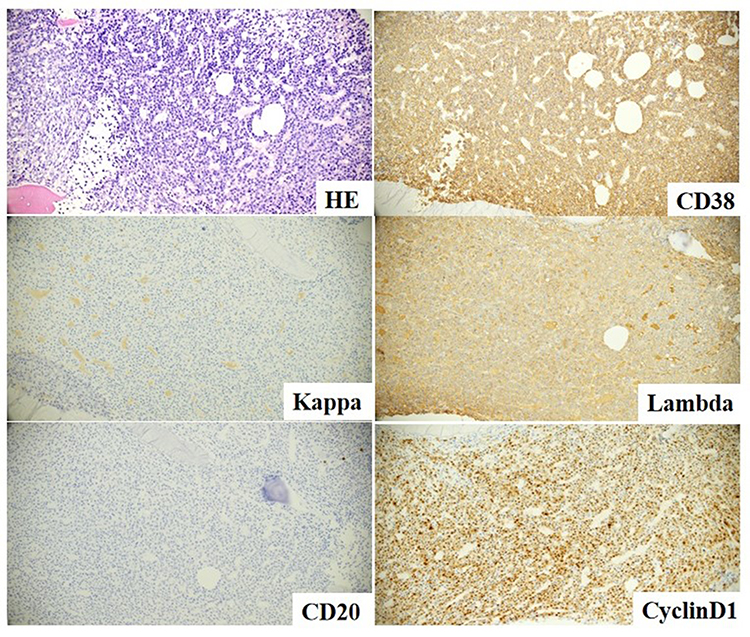 |
Figure 1 Hematoxylin & eosin (H&E) and immunohistochemical (IHC) staining in bone marrow (BM) biopsy samples of patients with multiple myeloma (MM). H&E and IHC staining, ×200. |
iFISH was performed in 163 of 203 patients. The prevalence of 4p16 (FGFR3)/14q32 (IGH), 11q13 (CCND1)/14q32 (IGH), 14q32 (IGH)/16q32 (MAF), 1q21, and 17p13.1 (TP53) mutations was 40.5% (66/163), 42.9% (70/163), 31.9% (52/163), 61.3% (100/163), and 20.9% (34/163), respectively. The high-risk cytogenetic group represented 63.8% (104/163) cases. The iFISH results for 163 patients with MM are shown in Supplementary Table 2. Figure 2 shows representative images of iFISH detection of 11q13 (CCND1)/14q32 (IGH) translocations.
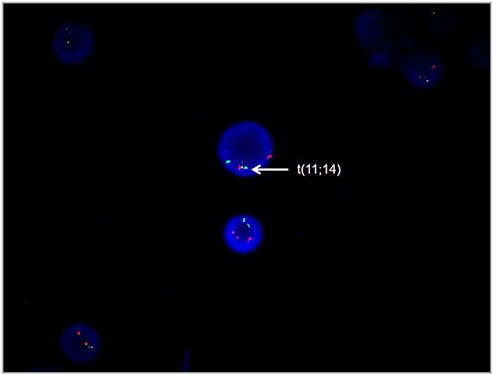 |
Figure 2 Representative images of interphase fluorescence in situ hybridization (iFISH) detection of 11q13 (CCND1)/14q32 (IGH) translocations. The cell shows two red, one green, and one fusion signal patterns indicative of t(11;14). iFISH, ×1000. |
Characteristics of EMM
The diagnosis of EMM was based on imaging findings. The incidence of EMM was 24.6% (50/203). Further classification of EMM showed that the incidence of PEMM was 16.3% (33/203), and the incidence of R/REMM was 8.4% (17/203). Three patients with both PEMM and R/REMM were classified under the PEMM group. All 50 patients with EMM were diagnosed using MR, and 34 of them underwent PET-CT based on MR examination. In patients with R/REMM, the mean interval from the diagnosis of MM to the diagnosis of EMM was 24.4 months (range: 8.5–101.1 months). Of the 33 patients with PEMM, 29 had parapapillary soft tissue invasion and 7 had hematogenous dissemination. Of the 17 patients with R/REMM, 16 had parapapillary soft tissue invasion and 2 had hematogenous dissemination. Figure 3 shows MR images of patients with EMM.
 |
Figure 3 Magnetic resonance (MR) images of samples from patients with extramedullary multiple myeloma (EMM). MM can be observed on the right scapula, and irregular elongated tumors with a diameter of approximately 4.4 cm can be observed in the soft tissue adjacent to the bone, indicating the occurrence of EMM. |
Analysis of EMM-Associated Clinicopathological Features
Based on the presence or absence of EMM, the enrolled patients were categorized into EMM+ and EMM− groups, and the differences in the clinicopathological features between the two groups were compared (Supplementary Table 1). The proportion of CD20+ in the EMM+ group was significantly lower than that in the EMM- group (2.0% and 15.0%, respectively), and the difference was statistically significant (P =0.013). Approximately 70% (35/50) of patients with EMM+ had elevated levels of β2-MG (≥ 5.5 mmol/L), and 24% (12/50) had elevated levels of serum calcium (> 2.65 mmol/L), which were higher than the levels in the EMM− group (41.2% and 12.4%, respectively), and the differences were statistically significant (P < 0.001 and P = 0.049, respectively).
We further compared the differences in clinicopathological features between 33 patients with PEMM and 17 patients with R/REMM (Supplementary Table 3). Patients with R/REMM were more likely to have plasma cell leukemia (14/17, 82.4%) and lower albumin levels (11/17, 64.7%) than those with PEMM (30.3% and 0%, respectively); these differences were statistically significant (P = 0.021 and P = 0.049, respectively). Supplementary Table 3 shows the clinicopathological characteristics of 50 patients with EMM.
Relationship Between EMM and Median OS
The median OS of patients in the EMM- group (59.6 months; 95% CI: 53.7–65.6) was longer than that of patients in the EMM+ group (47.0 months; 95% CI: 39.1–54.8); however, no significant difference was noted between the two groups (P = 0.197).The median OS of patients in the PEMM group (53.3 months; 95% CI: 43.8–62.8) was longer than that of patients in the R/REMM group (30.5 months; 95% CI: 22.0–39.0), and the difference was statistically significant (P = 0.015). Figure 4 shows the Kaplan–Meier cumulative OS analysis of patients in the EMM+ and EMM− groups. Figure 5 shows the Kaplan–Meier cumulative OS analysis of patients in the PEMM and R/REMM groups.
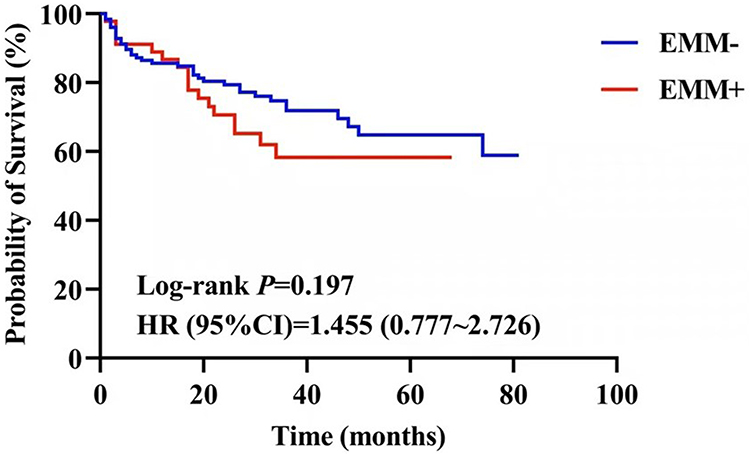 |
Figure 4 Kaplan–Meier cumulative overall survival (OS) analysis of patients in the EMM+ and EMM− groups. |
 |
Figure 5 Kaplan–Meier cumulative OS analysis of patients in the primary extramedullary multiple myeloma (PEMM) and relapsed or refractory EMM (R/REMM) groups. |
Univariate and Multivariate Analyses for Prognostic Factors
We further constructed Cox proportional hazard models to evaluate prognostic factors in patients with MM. Univariate analysis of OS revealed that the presence of R/REMM (HR=2.744, P=0.003), age ≥ 60 years (HR=1.974, P=0.024), high ISS stage (HR=3.270, P<0.001), serum calcium levels ≥ 2.65 mmol/L (HR=2.330, P=0.007), IgH/MAF+ (HR=2.078, P=0.027), and high β2-MG levels (≥ 5.50 mmol/L) (HR=2.120, P=0.011),combined with amyloidosis (HR=2.667, P=0.011) and CD56− (HR=0.552, P=0.046) were associated with poor survival in patients with MM.
Based on the results of univariate survival analysis, we included R/REMM, PEMM, age, ISS staging, serum calcium levels and IgH/MAF for multivariate survival analysis to validate the prognostic value of these parameters. The results showed that R/REMM (HR=3.253, P<0.001),age ≥ 60 years (HR=2.207, P =0.015),high ISS stage (HR=2.831, P =0.004) and serum calcium levels ≥ 2.65 mmol/L (HR=2.554, P=0.008) are independent adverse prognostic factors for MM patients. Univariate and multivariate survival analyses revealed that PEMM was not associated with OS in patients with MM (P = 0.503 and P = 0.571, respectively).
Table 1 shows the univariate and multivariate analyses results for OS in 203 patients with MM.
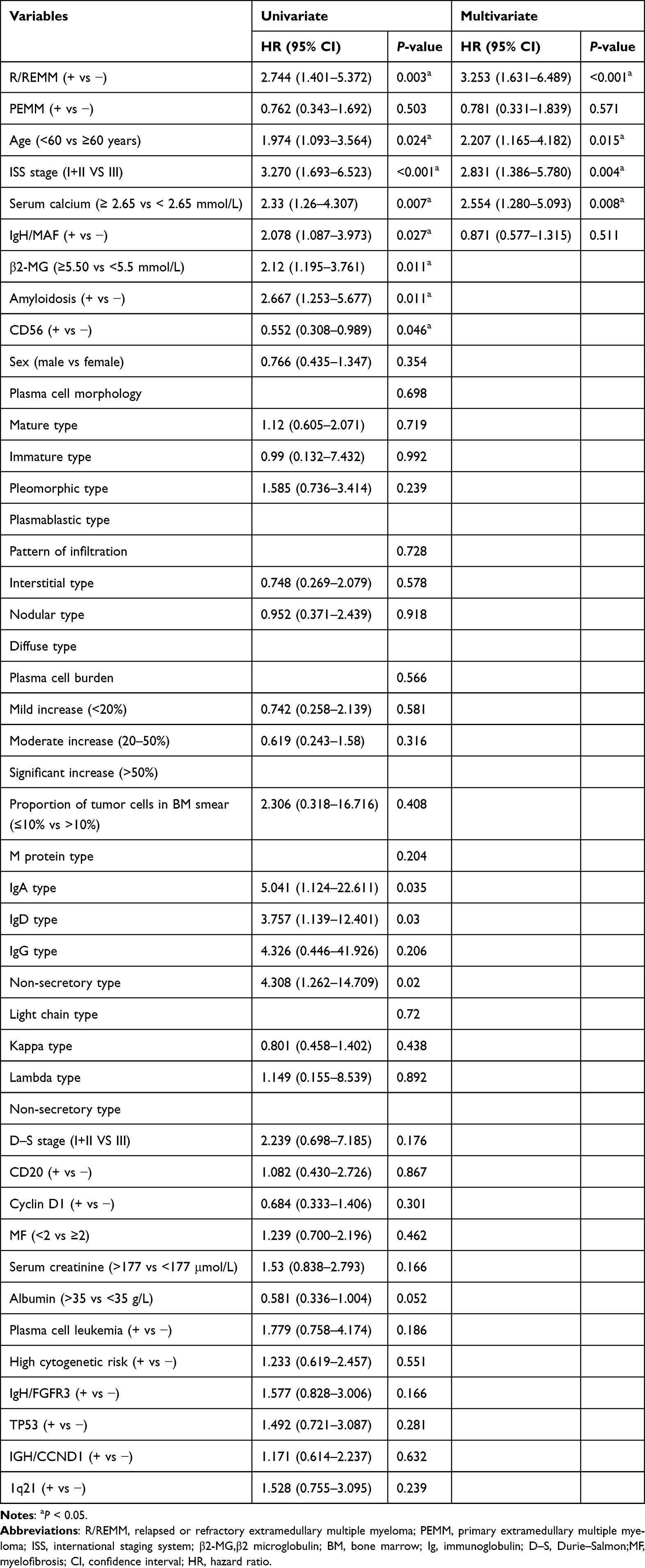 |
Table 1 Univariate and Multivariate Analyses for OS of 203 Patients with MM |
Discussion
EMM is a rare subtype of MM characterized by the infiltration of neoplastic plasma cells into other parts or organs away from the BM. It has been recognized as an aggressive subtype, even in the era of new drugs.18 We retrospectively analyzed 203 patients with MM and used imaging methods to screen for EMM during diagnosis and treatment. The incidence of PEMM was 16.3% (33/203), that of R/REMM was 8.4% (17/203). In a series study evaluating 3744 patients with MM from a European registry, which is the largest study to date, the overall incidence of EMM was 18.2% (682/3744).19 Deng et al20 assessed EMM in 834 consecutive patients with MM from a single center in China and reported incidence rates of 4.8% and 3.4% in patients with newly diagnosed multiple myeloma (NDMM) and R/REMM, respectively. Similarly, Rasche et al21 screened 357 patients with MM and reported an incidence of R/REMM of 6.7% (24/357). The incidence rates of PEMM and R/REMM in this study were slightly higher than those reported in previous studies. This is probably due to the use of highly sensitive imaging techniques, prolonged survival, and increased clinician attention to EMM. Therefore, the current incidence of EMM at diagnosis may have been underestimated in other studies.
This study further investigates the clinical and pathological features associated with the occurrence of EMM.Our results suggest that the proportion of CD20 + in the EMM + group was significantly lower than that in the EMM-group, indicating that the incidence of EMM is low in MM cases with abnormal expression of CD20. CD20 is not expressed in normal plasma cells, and approximately 5–20% of patients with MM may be CD20+.22 A previous study analyzed the immunophenotypes of myeloma cells in the BM using flow cytometry in 80 patients with MM. The results demonstrated that CD20 tended to have lower expression in the EMM+ group than in the EMM− group (5.0% vs 11.8%, P = 0.098).23 This is consistent with the results of this study.The prognostic value of CD20+ in MM varies among different subtypes of MM.Jian et al compared the relationship between CD20 expression and prognosis in 211 MM patients with t (11; 14), and the results showed that CD20+ patients had a longer tendency of PFS (59.0 vs 29.0 months, P =0.163) and significantly longer OS (99.0 vs.56.0 months, P=0.003) than CD20- patients.CD20+ plasma cells are more likely to proliferate in bone marrow tissue, and are less prone to EMM. The detailed mechanism is not clear. This phenomenon may provide a basis for better prognosis of CD20 + patients with MM.
In addition, our study suggests that certain indicators reflecting high tumor burden in MM, such as elevated levels of serum β2-MG and calcium, are significantly correlated with EMM occurrence (P < 0.001, P = 0.049, respectively). Besides,the results of this study indicate that the proportion of D–S III in the EMM+ group was higher than that in the EMM− group (90.0% vs.85.0%, P=0.370). These results suggest that the occurrence of EMM is associated with high tumor burden.A previous study has demonstrated that cells in EMM are characterized by immature and plasmablastic cell types.24 However, the results of our study indicate that plasma cell morphology is not associated with EMM occurrence (P = 0.144). This could be because of the low proportion of the plasmablastic type (14.3%) in this study.
Based on the time of EMM occurrence, EMM was further categorized into PEMM and R/REMM, and the differences in clinicopathological features between the two groups were discussed. Plasma cell leukemia and lower albumin levels significantly correlated with the occurrence of R/REMM (P = 0.021 and P = 0.014, respectively).Plasma cell leukemia is associated with the occurrence of R/REMM, suggesting that the two diseases may have the same mechanism of extramedullary migration. In addition, the proportion of diffuse growth mode of tumor cells in the R/REMM group was higher than that in the PEMM group (70.6% vs 57.6%). Diffuse growth is considered a more invasive growth mode, suggesting that R/REMM may exhibit more invasive biological behavior than PEMM.
Several genetic features have been linked to EMM.25 These include 17p deletion,26 nuclear expression of p53,27 a higher incidence of t(4;14),28 and overexpression of the MAFB (MAF BZIP transcription factor B) gene.29 These high-risk genetic features promote overexpression of oncogenes and genomic instability, leading to malignant cells to escape from the BM microenvironment and leading to the development of EMM.30 In this study, iFISH was performed in 163 out of 203 patients with MM, and the prevalence of 4p16 (FGFR3)/14q32 (IGH), 11q13 (CCND1)/14q32 (IGH), 14q32 (IGH)/16q32 (MAF), 1q21, and 17p13.1 (TP53) mutations was 40.5% (66/163), 42.9% (70/163), 31.9% (52/163), 61.3% (100/163), and 20.9% (34/163), respectively. Our results indicated no significant differences in the above cytogenetic changes between the EMM+ and EMM− groups or between the PEMM and R/REMM groups (P > 0.05).
Besides,we used iFISH to detect and demonstrate that the positivity rate for IgH/CCND1 in the R/REMM group was significantly higher than that in the PEMM group (9/14, 64.3% vs 13/30, 43.3%), however, a minor difference was noted between the EMM+ and EMM− groups (34.1% vs 46.2%). Therefore, IgH/CCND1 is closely associated with the occurrence of R/REMM. In MM, t(11; 14) and IgH-CCND1 fusion gene formation are common changes, with a reported incidence of approximately 20%.31 Currently, the Mayo Medical Center in the United States classifies NDMM with t(11; 14) as a standard risk group, indicating that CCND1 positivity has no clear prognostic value.32 The results of this study show that IgH/CCND1 is associated with the occurrence of R/REMM, which may indicate that IgH/CCND1 has a poor prognosis of MM. Further studies are needed to explore the mechanisms underlying the occurrence and development of EMM.
A previous study has discussed the impact of EMM on the prognosis of patients with MM, demonstrating that the OS period of patients with PEMM is 19.2–63.5 months and that of patients with R/REMM is 7–28.8 months.33 The results of our study indicate that the median OS of patients in the EMM+ group was lower than in the EMM− group (47.0 months vs 59.6 months, P = 0.197). Further categorization of EMM revealed that the OS of patients in the R/REMM group was shorter than that of patients in the PEMM group (30.5 months vs 53.3 months, P = 0.015). Further univariate and multivariate survival analyses revealed that R/REMM was an independent risk factor for MM,PEMM was not associated with OS in patients with MM.The OS in this study was slightly higher than that reported in previous studies, possibly because of the application of new treatment options, including PIs, IMiDS, and ASCT.This study showed that the median OS of the PEMM group was slightly shorter than that of the EMM-group, but the difference was not statistically significant.R/REMM is an independent poor prognostic factor for MM patients,suggesting that we should pay more attention to this group of diseases and provide personalized treatment to improve the quality of life and prognosis of patients.
The mechanisms related to EMM occurrence remain unclear, and the possible mechanisms are as follows: 1) Changes in the levels of different cytokines and chemokines promote the growth of tumor cells that no longer need to depend on the BM microenvironment, thus causing EMM.34 2) Genome structural mutations: MAPK pathway mutations occur in 80% of patients with EMM; high-frequency mutations exist in 20% of patients, of which 40% are deletions of TP53; secondary MYC/FGFR3/CCND2 translocations are obtained, and these molecular changes promote EMM occurrence.35 3) Stromal cells in the BM microenvironment interact with myeloma cells, increasing their migration ability and cytokine signaling, thereby promoting EMM occurrence.36
This study had the following characteristics: 1. It provides a comprehensive report on the laboratory test results, clinical, histological, and immunophenotypic features, cytogenetic changes,and prognosis of 203 patients with MM and explores the association of these factors with EMM. 2. This study is the first to classify cases according to the time of EMM occurrence and analyze the differences between the PEMM and R/REMM groups.
This retrospective study has several limitations. First, all patients were Chinese and from a single center; the sample size was relatively small, and the follow-up time was relatively short. Therefore, studies involving multiple centers and large sample sizes are required to generalize our findings. Second, pathological biopsy is not mandatory for the diagnosis of EMM. The diagnosis of EMM in this study was based on imaging examinations, and intramedullary and extramedullary lesions could not be compared. Finally, the treatment regimens varied among patients, potentially influencing the prognostic outcomes. Therefore, future studies with larger sample sizes and more rigorous methodologies must provide comprehensive information on prognostic outcomes.
Take-Home Point
R/REMM is an independent adverse prognostic factor for patients with MM. Patients with R/REMM are more likely to have plasma cell leukemia and lower albumin levels.
Abbreviations
β2-MG, β2 microglobulin; ASCT, Autologous stem cell transplantation; BM, Bone marrow; BMF, Bone marrow fibrosis; CT, Computed tomography; D–S, Durie–Salmon (referring to the Durie–Salmon staging system); EME, Extramedullary extraosseous; EMM, Extramedullary multiple myeloma; H&E, Hematoxylin and eosin; HRMM, High-risk multiple myeloma; iFISH, Interphase fluorescence in situ hybridization; Ig, Immunoglobulin; IHC, Immunohistochemical; IMiDs, Immunomodulatory drugs; ISS, International staging system; MAFB, MAF BZIP transcription factor B; MF, Myelofibrosis (in the context of grading bone marrow fibrosis); MM, Multiple myeloma; MR, Magnetic resonance; NDMM, Newly diagnosed multiple myeloma; OS, Overall survival; PEMM, Primary EMM; PET-CT, Positron emission computed tomography; PIs, Proteasome inhibitors; R/REMM, Relapsed or refractory EMM.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available because of privacy and ethical restrictions but are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the institutional review board and ethics committee of Beijing Chao-Yang Hospital and was conducted in accordance with requirements in the Declaration of Helsinki. The studies involving human participants were reviewed and approved by Ethics Committee of Beijing Chaoyang Hospital.
Consent for Publication
The patients provided their written informed consent to participate in this study.
Acknowledgments
This paper has been uploaded to Social Science Research Network as a preprint: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5286469.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Rajkumar SV, Kumar S. Multiple myeloma current treatment algorithms. Blood Cancer J. 2020;10(9):94. doi:10.1038/s41408-020-00359-2
2. van de Donk NWCJ, Pawlyn C, Yong KL. Multiple myeloma. Lancet. 2021;397(10272):410–12. doi:10.1016/S0140-6736(21)00135-5
3. Bertamini L, Bonello F, Boccadoro M, Bringhen S. New drugs in early development for treating multiple myeloma: all that glitters is not gold. Expert Opin Investig Drugs. 2020;29(9):989–1004. doi:10.1080/13543784.2020.1772753
4. Soekojo CY, Chng WJ. Treatment horizon in multiple myeloma. Eur J Haematol. 2022;109(5):425–440. doi:10.1111/ejh.13840
5. Bhutani M, Foureau DM, Atrash S, Voorhees PM, Usmani SZ. Extramedullary multiple myeloma. Leukemia. 2020;34(1):1–20. doi:10.1038/s41375-019-0660-0
6. Bladé J, Fernández de Larrea C, Rosiñol L, Cibeira MT, Jiménez R, Powles R. Soft-tissue plasmacytomas in multiple myeloma: incidence, mechanisms of extramedullary spread, and treatment approach. J Clin Oncol. 2011;29(28):3805–3812. doi:10.1200/JCO.2011.34.9290
7. Liu Y, Jelloul F, Zhang Y, et al. Genetic basis of extramedullary plasmablastic transformation of multiple myeloma. Am J Surg Pathol. 2020;44(6):838–848. doi:10.1097/PAS.0000000000001459
8. Narita T, Inagaki A, Kobayashi T, et al. t(14;16)-positive multiple myeloma shows negativity for CD56 expression and unfavorable outcome even in the era of novel drugs. Blood Cancer J. 2015;5(2):e285. doi:10.1038/bcj.2015.6
9. Hu X, Dai X, Guo X, et al. Bone marrow fibrosis in newly diagnosed multiple myeloma and its correlation with clinicopathological factors. Diagn Pathol. 2024;19(1):99. doi:10.1186/s13000-024-01516-y
10. Plasma Cell Disease Group, Chinese Society of Hematology, Chinese Medical Association, Chinese Myeloma Committee-Chinese Hematology Association. Consensus for the diagnosis and management of extramedullary plasmacytoma in China (2024). Zhonghua Xue Ye Xue Za Zhi. 2024;45(1):8–17. doi:10.3760/cma.j.cn121090-20231107-00253
11. Gao S, Li Q, Dong F, et al. Clinical characteristics and survival outcomes of newly diagnosed multiple myeloma patients presenting with extramedullary disease: a retrospective study. Leuk Res. 2022;115:106793. doi:10.1016/j.leukres.2022.106793
12. He J, Yue X, He D, et al. Multiple extramedullary-bone related and/or extramedullary extraosseous are independent poor prognostic factors in patients with newly diagnosed multiple myeloma. Front Oncol. 2021;11:668099. doi:10.3389/fonc.2021.668099
13. Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328–e346. doi:10.1016/S1470-2045(16)30206-6
14. Fujino M. The histopathology of myeloma in the bone marrow. J Clin Exp Hematop. 2018;58(2):61–67. doi:10.3960/jslrt.18014
15. Pich A, Chiusa L, Marmont F, Navone R. Risk groups of myeloma patients by histologic pattern and proliferative activity. Am J Surg Pathol. 1997;21(3):339–347. doi:10.1097/00000478-199703000-00011
16. Thiele J, Kvasnicka HM, Facchetti F, Franco V, van der Walt J, Orazi A. European consensus on grading bone marrow fibrosis and assessment of cellularity. Haematologica. 2005;90(8):1128–1132.
17. Ross FM, Avet-Loiseau H, Ameye G, et al. Report from the European Myeloma Network on interphase FISH in multiple myeloma and related disorders. Haematologica. 2012;97(8):1272–1277. doi:10.3324/haematol.2011.056176
18. Li G, Song YP, Lv Y, Li ZZ, Zheng YH. Clinical characteristics and prognostic analysis of multiple myeloma with extramedullary disease: a SEER-based study. J Oncol. 2021;2021:6681521. doi:10.1155/2021/6681521
19. Gagelmann N, Eikema DJ, Iacobelli S, et al. Impact of extramedullary disease in patients with newly diagnosed multiple myeloma undergoing autologous stem cell transplantation: a study from the Chronic Malignancies Working Party of the EBMT. Haematologica. 2018;103(5):890–897. doi:10.3324/haematol.2017.178434
20. Deng S, Xu Y, An G, et al. Features of extramedullary disease of multiple myeloma: high frequency of p53 deletion and poor survival: a retrospective single-center study of 834 cases. Clin Lymphoma Myeloma Leuk. 2015;15(5):286–291. doi:10.1016/j.clml.2014.12.013
21. Rasche L, Bernard C, Topp MS, et al. Features of extramedullary myeloma relapse: high proliferation, minimal marrow involvement, adverse cytogenetics: a retrospective single-center study of 24 cases. Ann Hematol. 2012;91(7):1031–1037. doi:10.1007/s00277-012-1414-5
22. Robillard N, Avet-Loiseau H, Garand R, et al. CD20 is associated with a small mature plasma cell morphology and t(11;14) in multiple myeloma. Blood. 2003;102(3):1070–1071. doi:10.1182/blood-2002-11-3333
23. Wang Y, Liu A, Xu T, Yin J, Chen W. Bone-related extramedullary disease in newly diagnosed myeloma patients is an independent poor prognostic predictor. Clin Med Insights Oncol. 2022;16:11795549221109500. doi:10.1177/11795549221109500
24. Cerny J, Fadare O, Hutchinson L, Wang SA. Clinicopathological features of extramedullary recurrence/relapse of multiple myeloma. Eur J Haematol. 2008;81(1):65–69. doi:10.1111/j.1600-0609.2008.01087.x
25. Bladé J, Beksac M, Caers J, et al. Extramedullary disease in multiple myeloma: a systematic literature review. Blood Cancer J. 2022;12(3):45. doi:10.1038/s41408-022-00643-3
26. López-Anglada L, Gutiérrez NC, García JL, Mateos MV, Flores T, San Miguel JF. P53 deletion may drive the clinical evolution and treatment response in multiple myeloma. Eur J Haematol. 2010;84(4):359–361. doi:10.1111/j.1600-0609.2009.01399.x
27. Sheth N, Yeung J, Chang H. p53 nuclear accumulation is associated with extramedullary progression of multiple myeloma. Leuk Res. 2009;33(10):1357–1360. doi:10.1016/j.leukres.2009.01.010
28. Besse L, Sedlarikova L, Greslikova H, et al. Cytogenetics in multiple myeloma patients progressing into extramedullary disease. Eur J Haematol. 2016;97(1):93–100. doi:10.1111/ejh.12688
29. Usmani SZ, Heuck C, Mitchell A, et al. Extramedullary disease portends poor prognosis in multiple myeloma and is over-represented in high-risk disease even in the era of novel agents. Haematologica. 2012;97(11):1761–1767. doi:10.3324/haematol.2012.065698
30. Pawlyn C, Morgan GJ. Evolutionary biology of high-risk multiple myeloma. Nat Rev Cancer. 2017;17(9):543–556. doi:10.1038/nrc.2017.63
31. Avet-Loiseau H, Attal M, Moreau P, et al. Genetic abnormalities and survival in multiple myeloma: the experience of the Intergroupe Francophone du Myelome. Blood. 2007;109(8):3489–3495. doi:10.1182/blood-2006-08-040410
32. Rajkumar SV. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am J Hematol. 2022;97(8):1086–1107. doi:10.1002/ajh.26590
33. Rosiñol L, Beksac M, Zamagni E, et al. Expert review on soft-tissue plasmacytomas in multiple myeloma: definition, disease assessment and treatment considerations. Br J Haematol. 2021;194(3):496–507. doi:10.1111/bjh.17338
34. Bansal R, Rakshit S, Kumar S. Extramedullary disease in multiple myeloma. Blood Cancer J. 2021;11(9):161. doi:10.1038/s41408-021-00527-y
35. Rasche L, Schinke C, Maura F, et al. The spatio-temporal evolution of multiple myeloma from baseline to relapse-refractory states. Nat Commun. 2022;13(1):4517. doi:10.1038/s41467-022-32145-y
36. Binder M, Szalat RE, Talluri S, et al. Bone marrow stromal cells induce chromatin remodeling in multiple myeloma cells leading to transcriptional changes. Nat Commun. 2024;15(1):4139. doi:10.1038/s41467-024-47793-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.