Back to Journals » Risk Management and Healthcare Policy » Volume 19
Clinicians’ Personal Delivery Preference and Decision-Making for Cesarean Delivery: A Survey of Obstetricians and Midwives
Authors Aldardeir NF, Sulaimani MA, Bahowarth SY, Almanasif M, Alghamdi YS, Aseeri SS, Alsulymani B, Heggi R, Hasanain R, Alyazidi A ![]()
Received 23 August 2025
Accepted for publication 28 December 2025
Published 7 February 2026 Volume 2026:19 562709
DOI https://doi.org/10.2147/RMHP.S562709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gulsum Kaya
Nashwa Fahad Aldardeir,1 Mohammed Ahmed Sulaimani,1 Sarah Yasir Bahowarth,2 Mersal Almanasif,2 Yasmeen Saeed Alghamdi,2 Sarah Saad Aseeri,2 Badr Alsulymani,2 Rawan Heggi,1 Rayyan Hasanain,1 Anas Alyazidi2
1Department of Obstetrics and Gynecology, Faculty of Medicine, King Abdulaziz University, Jeddah, 21589, Saudi Arabia; 2Faculty of Medicine, King Abdulaziz University, Jeddah, 21589, Saudi Arabia
Correspondence: Anas Alyazidi, Faculty of Medicine, King Abdulaziz University, Jeddah, 21589, Saudi Arabia, Tel +00966-2-6401000 ext 20094-20096, Fax +ext 20127, Email [email protected]
Purpose: The increasing prevalence of cesarean delivery (CD) worldwide has raised concerns in healthcare and academic circles. This study aimed to explore the factors influencing obstetricians’ decisions regarding CD in Saudi Arabia.
Patients and Methods: A cross-sectional study was conducted involving maternity clinicians (obstetricians and midwives). Data were collected using a structured questionnaire administered to a stratified sample of obstetricians practicing in healthcare facilities across the region. The questionnaire included questions about participants’ demographics, preferences for the mode of delivery, and factors influencing decision-making. Data were analyzed using RStudio.
Results: Infant and maternal safety, pain management, and long-term health implications were the main factors guiding CD decisions. Evidence-based medicine (EBM)-aligned practitioners were significantly less likely to perform non-medically indicated CS. Gender differences were observed, with female physicians more likely to prefer vaginal delivery. Partner influence and years of professional experience showed no significant effect on delivery preferences.
Conclusion: The study highlights the importance of EBM in guiding CD decisions and the need for open communication between healthcare providers and expectant parents. Future research with larger and more diverse samples could provide further insights into obstetricians’ decision-making processes.
Keywords: cesarean delivery, vaginal delivery, obstetrics, decision-making, healthcare providers
Introduction
In recent years, the increasing prevalence of cesarean delivery (CD) on a global scale has prompted considerable unease within the healthcare community and academic circles. The global average CD rate has risen dramatically from about 7% in 1990 to over 21% today, with rates exceeding 40% in some regions, far above the 10–15% considered optimal by the World Health Organization,1,2. This surge is notably conspicuous in Middle-Eastern cultures, including Saudi Arabia, where a recent study reported a CD rate of 28.5%.3 In these settings, a blend of cultural conventions, medical practices, and patient anticipations crafts a distinct backdrop for childbirth encounters.4,5 The mounting inclination towards CD presents hurdles and prompts inquiries into the determinants affecting the choices of obstetricians and patients alike, a process often shaped by a combination of medical, social, and personal factors.6 By exploring the motivations and decision-making processes of healthcare providers in Saudi Arabia, this study aims to provide insights into the evolving landscape of childbirth and the reasons for the increasing preference for CD in the region. Additionally, legal and ethical considerations can further complicate the choices available to expectant mothers.7 By exploring the motivations behind patients’ choices and the decision-making processes of healthcare providers, this study aims to provide insights into the evolving landscape of childbirth in the Middle East. It seeks to uncover the reasons for the increasing preference for CD and to identify strategies that could support informed, safe, and culturally sensitive childbirth experiences.
Materials and Methods
Study Design and Setting
This cross-sectional study was conducted among maternity clinicians (obstetricians and midwives) practicing in the major healthcare sectors in Saudi Arabia, including government (public), private, and university-affiliated tertiary care hospitals. While the Saudi Ministry of Health provides national clinical guidelines for cesarean delivery, their adoption and implementation can vary across these different settings. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline.8 The study utilized a structured, pre-validated questionnaire to gather data from a sample of practicing clinicians from healthcare facilities across the country.9 A pilot study on 30 clinicians was conducted prior to the complete data collection; feedback and adjustments were made during the pilot study phase. In the completed study, a total of 108 obstetricians completed the questionnaire.
Population and Sampling Technique
A stratified sampling technique was utilized to ensure the representation of clinicians from diverse healthcare settings, including government, private, and university hospitals. This approach was selected to accurately capture the variation in clinical practices and preferences across these distinct sectors.
The target population was all practicing obstetricians in Saudi Arabia. The accessible population consisted of obstetricians affiliated with major hospitals and professional networks in the Western, Central, and Eastern regions. The final study sample included 108 participants.
The statistically appropriate sample size was calculated using Raosoft software, with a 95% confidence interval (CI) and a margin of error <0.05. The applied equation was as follows:

where n = population size, p=prevalence, d = precision (desired margin of error), DEFF = design effect, and Z1−α/2 = 1.96 for a 95% confidence level.
Our inclusion criteria included practicing obstetricians, gynecologists, and certified professional midwives involved in the care of pregnant women in different gestational stages or postpartum mothers who have recently undergone childbirth. We excluded retired clinicians and those not currently providing direct patient care. After applying the inclusion criteria and removing duplicate and incomplete responses, 98% of the responses were included in the analysis. After applying the inclusion criteria and removing duplicate and incomplete responses, 98% of the responses were included in the analysis.
Data Collection
Data were collected through a 29-item self-administered online survey. The survey was emailed to the obstetricians after their Email address was collected in advance. The surveys contained multiple sections, including section 1, which obtained a consent statement explaining the nature of the study andthe targeted population. Section 2 obtained socio-demographic data of participating obstetricians including their gender, age, nationality, marital status, family status, region of work, work sector (ie private, university, public hospital), profession and postgraduate training, clinical experience in CD and forceps use, preferences for the mode of delivery, factors influencing their decision-making, perceptions of safety and risks associated with different delivery methods. Section 3 assessed factors that influence their choices to their preferred mode of delivery, including questions on patient, physician, and baby’s safety, as well as other concerns. It also assessed their perception of patients’ autonomy and their approach towards patients.
Data Analysis
Data were cleaned, managed, and coded using Microsoft Excel 2019 (Microsoft Corporation, Redmond, WA). Statistical analysis was performed using R (RStudio, version 1.4.1106; RStudio, Inc). Descriptive analysis included frequency distributions. Cross-tabulations were evaluated using the chi-square test, and odds ratios (OR) with 95% CI were calculated. For cross-tabulations where any expected cell count was less than 5, Fisher’s exact test was used instead of the chi-square test to ensure statistical accuracy. Sensitivity analysis was performed by excluding participants with no CD experience to ensure the robustness of the primary outcomes. A p-value of less than 0.05 was considered statistically significant.
Ethical Statement
This study will adhere to ethical guidelines, ensuring voluntary participation, confidentiality, and informed consent from all participants. The study was approved by the Unit of Biomedical Ethics Research Committee at the Faculty of Medicine, King Abdulaziz University (reference number: 35–24). The committee is registered at the National Committee of Bioethics (NCBE) with registration number (HA-02-J-008). Patients’ privacy and confidentiality were maintained throughout the study, and all revealing data were appropriately masked. This study followed the ethical standards of the Declaration of Helsinki and its subsequent amendments.
Results
Participants’ Characteristics
The study involved 108 participants, with the majority being Saudi nationals (79.6%) and female (75.0%). Half of the participants were aged 30–39 (50.0%), and most worked in the Western region (66.7%). Regarding the work sector, 34.3% were employed exclusively in government hospitals, and 25.0% worked in university hospitals. Experience with CD was relatively evenly distributed, with 44.4% having no experience and 41.7% having experience. Professionally, 88.9% of participants were obstetricians or gynecologists, with 75.0% practicing in obstetrics and gynecology. Among doctors, 37.0% were consultants, and 27.8% were residents (Table 1).
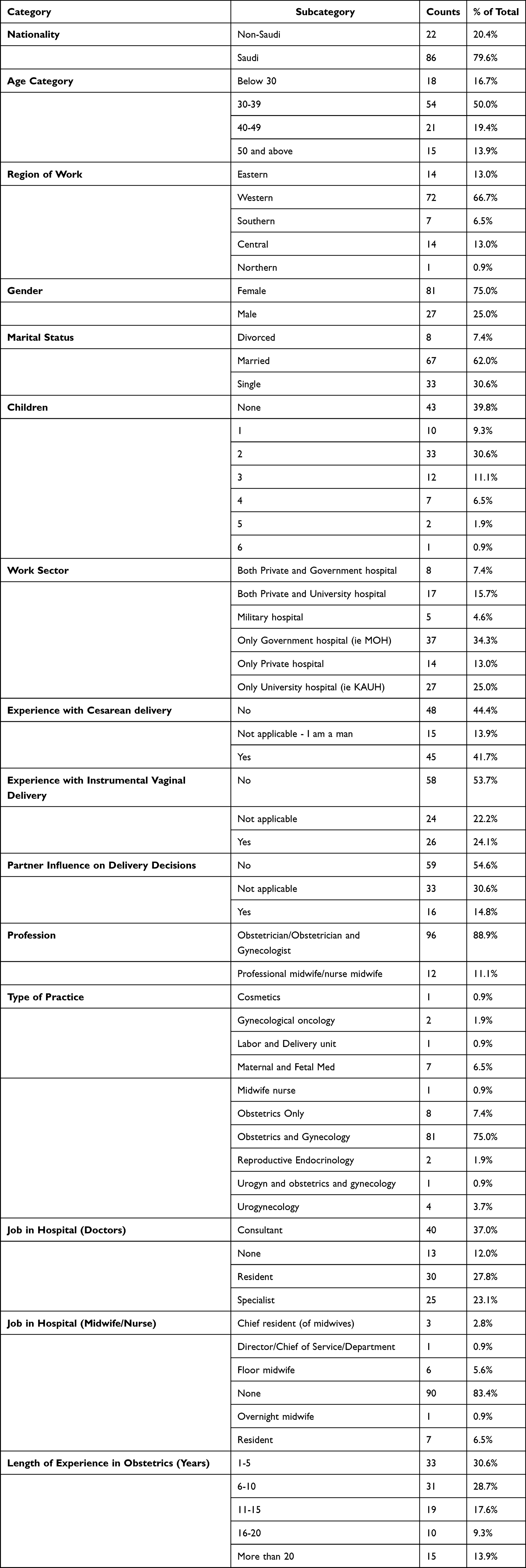 |
Table 1 Demographic and Professional Characteristics of Participating Physicians and Midwives |
Preferred Mode of Delivery
Table 2 presents participants’ characteristics and their preferred mode of delivery. A non-significant trend was observed, with female physicians more likely to prefer vaginal delivery compared to male physicians (p=0.093). Nationality, region of work, age, marital status, number of children, work sector, experience with CS, experience with instrumental vaginal delivery, partner influence, profession, type of practice, job in hospital, and length of experience in obstetrics did not significantly impact the choice of delivery method, with p-values all above 0.05. When analyzing preferences by profession, a similar proportion of physicians (88.5%, n=85/96) and midwives (100%, n=12/12) preferred vaginal delivery for themselves.
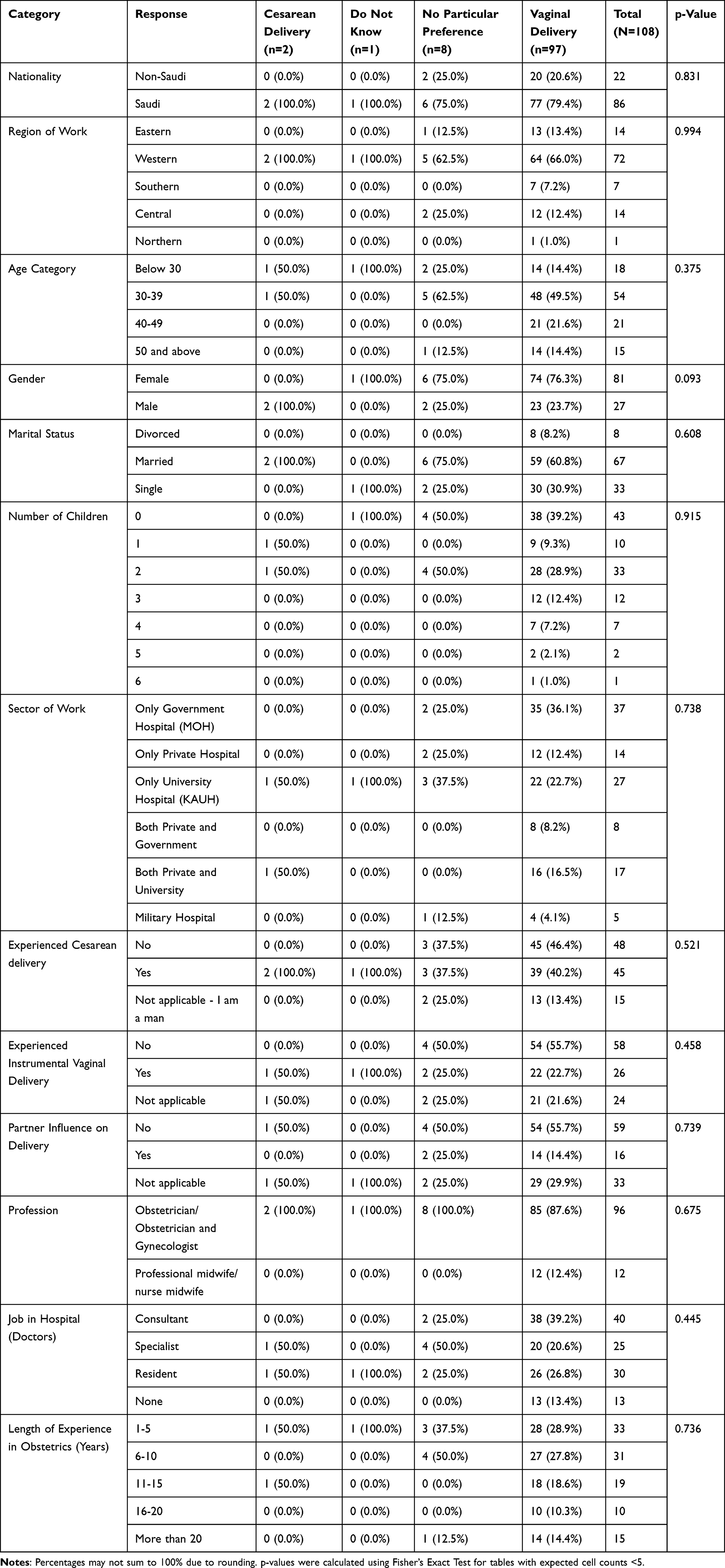 |
Table 2 Participants’ Characteristics and Their Preferred Mode of Delivery |
Reasons Influencing the Decision
Figure 1 shows the key reasons for choosing a CD for oneself or a partner. The most cited reason was the baby’s safety, mentioned by 46.3% (n=50). This was followed by the mother’s safety, cited by 31.5% (n=34), and the desire to decrease pain and increase comfort, cited by 29.6% (n=32). Uro-gynecological reasons and advanced maternal age were each mentioned by 25.9% (n=28). Reducing figure trauma was a factor for 22.2% (n=24), while minimizing effects on sexual function influenced 18.5% (n=20). Other considerations included the desire for fewer children, mentioned by 17.6% (n=19), and fear of fetal death, cited by 16.7% (n=18). Reducing pelvic organ prolapse, mentioned by 12.0% (n=13), preventing postpartum bleeding, cited by 6.5% (n=7), and lowering the risk of infection, noted by 5.6% (n=6).
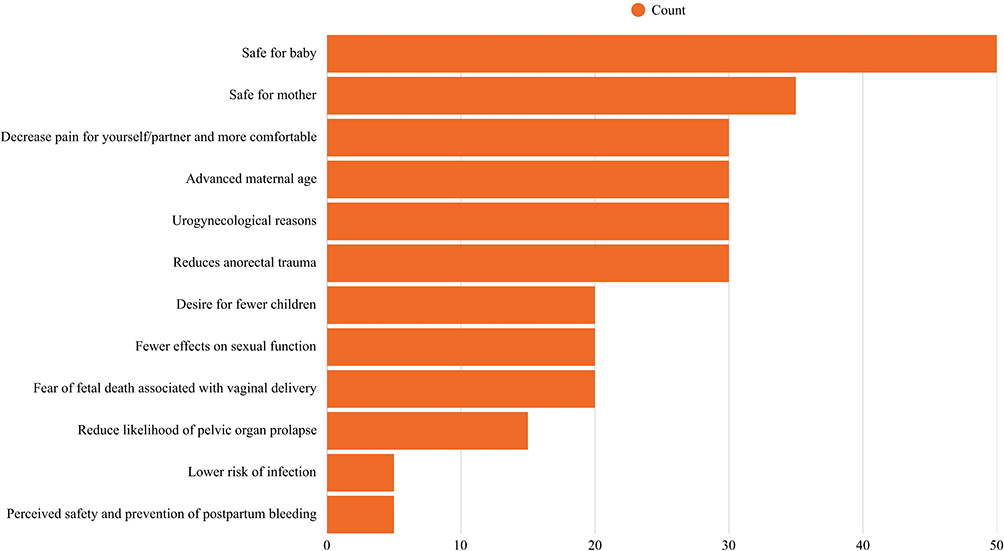 |
Figure 1 Most frequent reasons for choosing a caesarean section for oneself or a partner. |
Table 3 demonstrates that vaginal delivery is the preferred method among physicians, especially those in government hospitals (p=0.738). While the perceived patient preference for vaginal delivery was also highest among government hospital employees, no significant differences were found across sectors (p=0.656). Support for a woman’s right to choose her delivery method was widespread, particularly in government hospitals, though not statistically significant (p=0.239). The willingness to perform a CD without a medical indication varied slightly across groups but was insignificant (p=0.314). Evidence-based medicine (EBM) was the main factor influencing CD decisions across all sectors (p=0.749). Even after counseling on CD risks, many physicians were willing to perform the procedure if requested, with no significant differences across sectors (p=0.069).
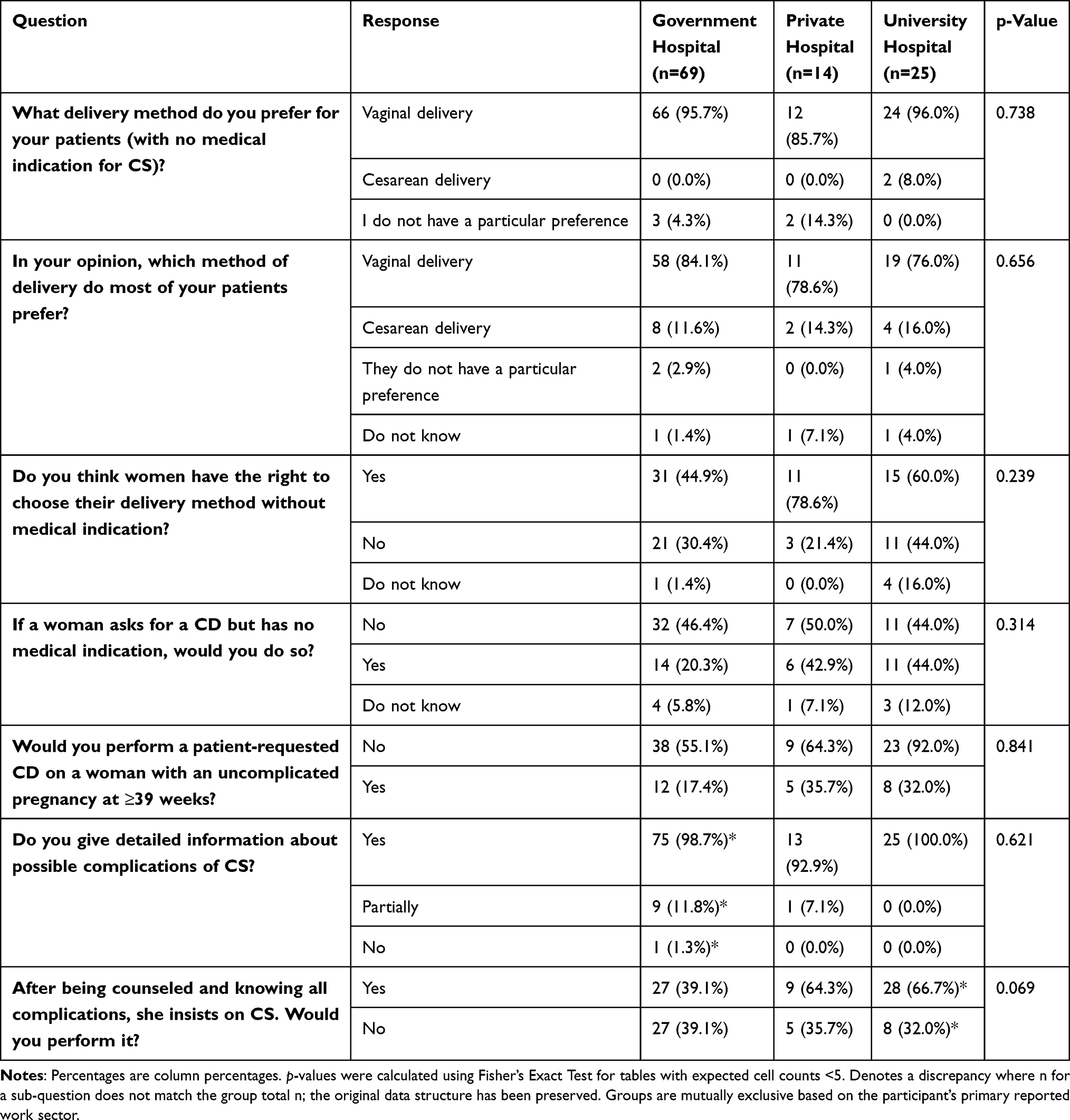 |
Table 3 Variables Affecting the Mode of Delivery Based on the Type of Practice |
The Influence of EBM on Practitioners
Table 4 highlights key differences between physicians who adhere to EBM and those who do not exclusively rely on it. The provision of detailed information about CD complications was standard across both groups, with no significant difference (p=0.241). However, a near-significant trend indicated that EBM practitioners were more likely to support a woman’s right to choose her delivery method without medical indication (p=0.053). Importantly, EBM practitioners were significantly less likely to perform a patient-requested CD in an uncomplicated pregnancy at 39 weeks (p=0.004) and were more likely to refuse to perform a CD without medical indication (p=0.005). These findings underscore the more conservative approach of EBM practitioners in decisions related to CS.
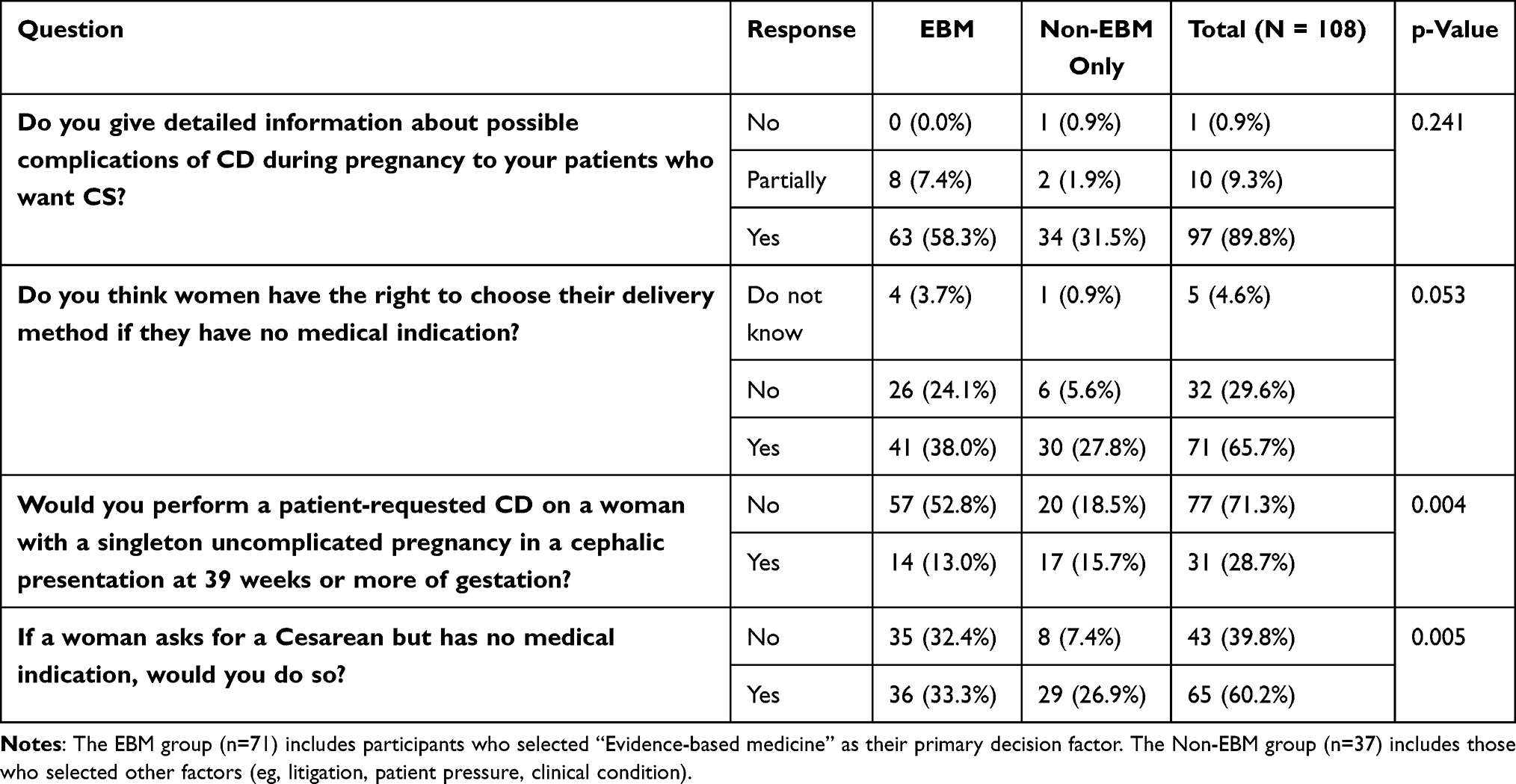 |
Table 4 Participants Affected by EBM and Others |
Discussion
Our study aimed to delve into crucial epidemiological data by examining the personal delivery preferences of maternity clinicians and the factors that influence their attitudes toward performing CS. The future of women’s reproductive health hinges significantly on their experience during their first childbirth.12 One of the contentious issues in obstetrics is the rising trend of performing CD solely based on maternal request,13 presenting obstetricians with numerous challenges. Studies have identified factors such as personal beliefs, preferences, and risk perceptions among obstetricians as major influencers in this decision-making process.14,15 Beyond clinical considerations, factors like the fear of legal consequences and litigation have been found to significantly impact the decision to perform CS.15,16 In our study, fear of litigation was ranked as a primary factor influencing the decision to perform a CD by only a small minority of respondents (see Table 3), suggesting that while it may be a consideration for some, it was not the dominant driver in this cohort.
Our study observed that a higher proportion of female physicians preferred vaginal delivery for themselves compared to male physicians; however, this association was not statistically significant (p=0.093). This finding is consistent with the general trend observed in other studies, where vaginal delivery is also the predominant personal preference among healthcare professionals. For instance, a study in Egypt reported a high preference for vaginal delivery at 78.0% among its participants, which is a similar direction of preference, though the specific proportion differs from our cohort.17 Female physicians within the medical field displayed a lower preference for CD (17.1%) compared to those in other professions (27.0%).17 Similarly, a study in the United Kingdom found that men were more likely to opt for CD (13.0%) than women (9.0%).18 These findings resonate with a long-standing trend observed since 1996, where obstetricians’ personal preferences have shown reluctance towards elective CD in the absence of clinical indications.19
While many studies support the association between gender and delivery preferences, some reports suggest a negative correlation, hinting at the presence of additional influencing factors.20 Consequently, our study delved into other factors, including the influence of family members, such as partners and friends, in the decision-making process, as proposed by existing literature.21 Surprisingly, our results indicated that partner influence and professional experience did not significantly impact the choice of delivery method. This shift in perception regarding risks among eastern cultures, which historically exhibit a more defensive approach towards uncertainties, including health matters, was notable.22 However, a recent study in India revealed a weak correlation between the decision on delivery mode and partner influence and pressure,23 underscoring the complex interplay of cultural and individual factors in decision-making processes.
Our findings highlight that obstetricians’ decisions are primarily guided by clinical factors, with infant safety (46.3%), maternal safety (31.5%), and pain management (29.6%) being the most cited reasons for considering a CS. This clinical focus is further reinforced by the central role of Evidence-Based Medicine. The significant reluctance of EBM-aligned practitioners to perform non-medically indicated CS, even after patient counseling, demonstrates a commitment to clinical guidelines over patient convenience or non-clinical requests. Therefore, the crucial “open communication” between provider and patient should be framed as evidence-based counseling, where the physician’s role is to educate patients on the risks and benefits, aligning patient expectations with medical best practices to reduce unnecessary interventions. Furthermore, while our sample included different clinician types, the core findings on EBM were consistent, suggesting that adherence to clinical guidelines is a universal factor that transcends specific professional roles in this setting.
Regarding EBM variables, our study revealed that practitioners who adhered to EBM were significantly less likely to perform a patient-requested CD in uncomplicated pregnancies at 39 weeks or later with cephalic presentation (p=0.004). While the practitioners’ work sector did not significantly influence their decisions, in contrast to another study, where the private sector exhibited a higher likelihood of elective CD under similar circumstances.20 This shift reflects the growing impact of EBM on clinical decision-making across healthcare settings in Saudi Arabia, emphasizing patient safety and ethical considerations related to cesarean deliveries.
Despite the majority of EBM-aligned practitioners acknowledging women’s right to choose their delivery method in the absence of medical indications, they tended to adopt a conservative approach, being less inclined to perform non-medically indicated CD (p=0.005).20,24–29 The conservatism seen in our study is consistent with Saudi Arabian practitioners’ emphasis on evidence-based practices, which are prioritized in all sectors—private, public, and even educational—because they can more effectively handle the complexity of patients’ requests for CD and, in the long run, eventually result in safer outcomes and well-informed decisions.
Limitations
The study’s sample size may pose limitations on the generalizability of the findings. A larger and more diverse sample could provide a broader understanding of obstetricians’ decision-making processes regarding CS. Another statistical limitation of this study was the small cell sizes in some subgroup analyses, which necessitated the use of Fisher’s exact test. This may affect the power to detect significant associations for some variables. A potential skewed result due to selection bias might be a limitation in addition to recall bias whereas obstetricians may have difficulty accurately recalling past experiences or factors influencing their decision-making process. Furthermore, self-report bias and the single-country focus can potentially limit our findings.
Conclusion
This study provides a critical exploration of the personal preferences and decision-making paradigms of maternity clinicians in Saudi Arabia regarding cesarean delivery. The most salient finding is the significant association between adherence to EBM and a more conservative approach to CS. Clinicians who primarily relied on EBM were markedly less likely to perform non-medically indicated CS, underscoring EBM’s role as a pivotal moderating factor against the trend of cesarean delivery on maternal request. This highlights the paramount importance of reinforcing evidence-based guidelines and ethical decision-making in clinical practice to ensure that maternal and neonatal safety remains the central tenet of obstetric care. While a preference for vaginal delivery was predominant overall, our analysis suggests that clinician gender may be a factor worthy of further investigation, as a greater proportion of female clinicians preferred this mode for themselves. The primary motivations driving considerations for CD were squarely focused on clinical concerns, namely infant and maternal safety. For clinical practice, these findings emphasize the necessity of integrating structured, evidence-based counseling into patient interactions. Such an approach can effectively address misconceptions, align patient expectations with clinical best practices, and potentially reduce unnecessary cesarean deliveries. Future research should aim to validate these findings with larger, nationally representative samples and incorporate qualitative methods to gain a deeper understanding of the complex motivations behind clinicians’ personal and professional choices. This will be essential for developing targeted, multi-faceted interventions aimed at optimizing childbirth outcomes in the region.
Abbreviations
CD, cesarean delivery; DEFF, design effect; EBM, evidence-based medicine; NCBE, National Committee of Bioethics; OR, odds ratio; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; WA, Washington.
Acknowledgments
The authors acknowledge with thanks WAQF and the Deanship of Scientific Research (DSR) for their support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Angolile CM, Max BL, Mushemba J, Mashauri HL. Global increased cesarean section rates and public health implications: a call to action. Health Sci Rep. 2023;6(5):e1274. doi:10.1002/hsr2.1274
2. Betrán AP, Ye J, Moller AB, Zhang J, Gülmezoglu AM, Torloni MR. The increasing trend in caesarean section rates: global, regional and national estimates: 1990–2014. PLoS One. 2016;11:e0148343. doi:10.1371/journal.pone.0148343
3. Alsulami SM, Ashmawi MT, Jarwan RO, Malli IA, Albar SK, Al-Jifree HM. The rates of cesarean section deliveries according to Robson classification system during the year of 2018 among patients in King Abdulaziz Medical City, Jeddah, Saudi Arabia. Cureus. 2020;12:e11529. doi:10.7759/cureus.11529
4. Alzubaidi H, Samorinha C, Saidawi W, Hussein A, Saddik B, Scholl I. Preference for shared decision-making among Arabic-speaking people with chronic diseases: a cross-sectional study. BMJ Open. 2022;12:e058084. doi:10.1136/bmjopen-2021-058084
5. Roudsari RL, Zakerihamidi M, Khoei EM. Socio-cultural beliefs, values and traditions regarding women’s preferred mode of birth in the north of Iran. Int J Community Based Nurs Midwifery. 2015;3:165–13.
6. Felisian S, Mushy SE, Tarimo EAM, Kibusi SM. Sociocultural practices and beliefs during pregnancy, childbirth, and postpartum among indigenous pastoralist women of reproductive age in Manyara, Tanzania: a descriptive qualitative study. BMC Womens Health. 2023;23:422. doi:10.1186/s12905-023-02277-4
7. Irvine K, Brown RCH, Savulescu J. Disclosure and consent: ensuring the ethical provision of information regarding childbirth. J Med Ethics. 2023;49:1–8. doi:10.1136/jme-2022-108283
8. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335:806–808. doi:10.1136/bmj.39335.541782.AD
9. Arikan DC, Özer A, Arikan I, Coskun A, Kiran H. Turkish obstetricians’ personal preference for mode of delivery and attitude toward cesarean delivery on maternal request. Arch Gynecol Obstet. 2011;284:543–549. doi:10.1007/s00404-010-1682-z
10. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
11. Salawati E, Ghamri R, Amir A, et al. The magnitude of influence of personal and professional factors on the career choices of medical students. J Med Life. 2024;17:449–456. doi:10.25122/jml-2023-0453
12. Wiklund I, Edman G, Ryding EL, Andolf E. Expectation and experiences of childbirth in primiparae with caesarean section. BJOG. 2008;115:324–331. doi:10.1111/j.1471-0528.2007.01564.x
13. Paterson-Brown S, Amu O, Rajendran S, Bolaji II. Should doctors perform an elective caesarean section on request? BMJ. 1998;317:462–465. doi:10.1136/bmj.317.7156.462
14. Panda S, Begley C, Daly D. Clinicians’ views of factors influencing decision-making for caesarean section: a systematic review and metasynthesis. PLoS One. 2018;13:e0200941. doi:10.1371/journal.pone.0200941
15. Bam V, Lomotey AY, Kusi-Amponsah Diji A, Budu HI, Bamfo-Ennin D, Mireku G. Factors influencing decision-making to accept elective caesarean section: a descriptive cross-sectional study. Heliyon. 2021;7:e07755. doi:10.1016/j.heliyon.2021.e07755
16. Fear of litigation is a key factor in decision to perform C-sections. Trinity College Dublin News & Events. September 23, 2024. Available from: https://www.tcd.ie/news_events/articles/fear-of-litigation-is-a-key-factor-in-decision-to-perform-c-sections/.
17. Ibrahim R, Khalil R, Ehab R, Osama R, Mohammed A, Hetler W. Preference of mode of delivery among women in childbearing period in Egypt and factors affecting it. Ginekol Pol Med Project. 2021;61:1–7.
18. Lightly K, Shaw E, Dailami N, Bisson D. Personal birth preferences and actual mode of delivery outcomes of obstetricians and gynaecologists in South West England; with comparison to regional and national birth statistics. Eur J Obstet Gynecol Reprod Biol. 2014;181:95–98. doi:10.1016/j.ejogrb.2014.07.005
19. Al-Mufti R, McCarthy A, Fisk NM. Survey of obstetricians’ personal preference and discretionary practice. Eur J Obstet Gynecol Reprod Biol. 1997;73:1–4. doi:10.1016/s0301-2115(96)02692-9
20. Kosan Z, Kavuncuoglu D, Calıkoglu EO, Aras A. Delivery preferences of pregnant women: do not underestimate the effect of friends and relatives. J Gynecol Obstet Hum Reprod. 2019;48:395–400. doi:10.1016/j.jogoh.2019.03.009
21. Guo W, Chen XR, Liu HC. Decision-making under uncertainty: how Easterners and Westerners think differently. Behav Sci. 2022;12:92. doi:10.3390/bs12040092
22. Kalyan SSG, Bhardwaj G, Shafqat N, Verma M. Preferences and factors determining preferences for mode of delivery among primigravida mothers. J Fam Med Prim Care. 2024;13:1517–1523. doi:10.4103/jfmpc.jfmpc_1365_23
23. Koken G, Cosar E, Sahin FK, Arioz DT, Duman Z, Aral I. Attitudes towards mode of delivery and cesarean on demand in Turkey. Int J Gynaecol Obstet. 2007;99:233–235. doi:10.1016/j.ijgo.2007.05.031
24. Câmara R, Burlá M, Ferrari J, et al. Cesarean section by maternal request. Rev Col Bras Cir. 2016;43:301–310. doi:10.1590/0100-69912016004002
25. Bettes BA, Coleman VH, Zinberg S, et al. Cesarean delivery on maternal request: obstetrician-gynecologists’ knowledge, perception, and practice patterns. Obstet Gynecol. 2007;109:57–66. doi:10.1097/01.AOG.0000249608.11864.b6
26. Bergholt T, Østberg B, Legarth J, Weber T. Danish obstetricians’ personal preference and general attitude to elective cesarean section on maternal request: a nation-wide postal survey. Acta Obstet Gynecol Scand. 2004;83:262–266. doi:10.1111/j.0001-6349.2004.0312.x
27. Murray SF, Elston MA. The promotion of private health insurance and its implications for the public/private mix in maternity care in Chile. BMJ Open. 2013;3:e003865. doi:10.1136/bmjopen-2013-003865
28. Wax JR, Cartin A, Pinette MG, Blackstone J. Patient choice cesarean—the Maine experience. Birth. 2005;32:272–276. doi:10.1111/j.0730-7659.2005.00370.x
29. Gamble J, Creedy DK, McCourt C, Weaver J, Beake S. A critique of the literature on women’s request for cesarean section. Birth. 2007;34:331–340. doi:10.1111/j.1523-536x.2007.00193.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Insulin Resistance as a Biomarker for Pelvic Organ Prolapse in Gestational Diabetes Mellitus: Stratification by Delivery Modes
Jiao Y, Dai Y, He L, Fei Z
International Journal of General Medicine 2025, 18:6377-6385
Published Date: 21 October 2025
Association Between Mode of Delivery and Levator Ani Muscle Abnormalities on 4D Transperineal Ultrasound at 6 Weeks Postpartum
Yi J, Tang Z, Wang L, Zhang B, Chen X, Liu X
International Journal of Women's Health 2026, 18:601021
Published Date: 8 June 2026