Back to Journals » International Journal of Women's Health » Volume 18
Association Between Mode of Delivery and Levator Ani Muscle Abnormalities on 4D Transperineal Ultrasound at 6 Weeks Postpartum
Authors Yi J, Tang Z, Wang L, Zhang B, Chen X, Liu X
Received 23 February 2026
Accepted for publication 1 May 2026
Published 8 June 2026 Volume 2026:18 601021
DOI https://doi.org/10.2147/IJWH.S601021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jiao Yi,1 Zhiguo Tang,2 Leilei Wang,3 Bin Zhang,4 Xianxia Chen,1 Xiaoying Liu5
1Department of Obstetrics and Gynecology, Maternal and Child Medical Centre Affiliated with Anhui Medical University, Hefei Maternal and Child Health Care Hospital, Hefei, People’s Republic of China; 2Department of Urology, Maternal and Child Medical Centre affiliated with Anhui Medical University, Hefei Maternal and Child health care Hospital, Hefei, People’s Republic of China; 3Department of Postpartum Rehabilitation, Maternal and Child Medical Centre affiliated with Anhui Medical University, Hefei Maternal and Child health care Hospital, Hefei, People’s Republic of China; 4Department of Science and Education, Maternal and Child Medical Centre affiliated with Anhui Medical University, Hefei Maternal and Child health care Hospital, Hefei, People’s Republic of China; 5Department of Ultrasound, Maternal and Child Medical Centre Affiliated with Anhui Medical University, Hefei Maternal and Child Health Care Hospital, Hefei, People’s Republic of China
Correspondence: Jiao Yi, Department of Obstetrics and Gynecology, Maternal and Child Medical Centre affiliated with Anhui Medical University, Hefei Maternal and Child health care Hospital, No. 15 Yimin Street, Hefei, 230000, People’s Republic of China, Tel +86 13866728121, Email [email protected]
Purpose: It is well established that vaginal delivery is the main risk factor for the development of pelvic floor disorders, which is mainly mediated by structural alterations in the levator ani muscle. However, there are no robust data on the magnitude of cesarean section correlated with the morphological changes of the levator ani muscle based on ultrasound anatomical markers, which is an interesting topic to focus on in this article.
Materials and Methods: This retrospective study included 1930 women who delivered at our center between February 2024 and March 2025. The two groups were divided according to the mode of delivery (vaginal delivery and cesarean section), and analysis included baseline characteristics, pregnancy parameters, delivery details, and ultrasonic findings in the levator ani muscle and levator hiatus 6 weeks postpartum.
Results: In the vaginal delivery group, 45 cases (3.7%) have levator ani muscles avulsion, while 887 cases (72.5%) with enlarged levator hiatus, the corresponding figures of cesarean section group were 2 cases (0.3%) and 295 cases (41.8%), respectively. On univariate analysis, we found significant differences in the baseline characteristics, obstetrical details, levator ani muscle avulsion and hiatal enlargement when comparing participants with vaginal deliveries versus women who underwent cesarean sections. After adjustment for confounding factors, multivariate logistic regression analysis shows women who delivered vaginally had a 6.58-times and 4.31-times odds of levator ani muscle avulsion as well as hiatal enlargement compared to women who underwent cesarean sections, respectively (OR = 6.58, 95% CI = 1.55– 27.87, P = 0.011; OR = 4.31, 95% CI = 3.30– 5.61, P < 0.001, respectively). Based on the dimensional evaluation for pelvic floor structures using 4D ultrasound, no association was noted between the levator avulsion as well as levator hiatus over-distension and cesarean section regardless of surgical indications (P = 0.162 and P = 0.313, respectively).
Conclusions: As a reliable, easily accessible and cost-effective methods, 4D ultrasonography has now become standard in recent years for the assessment of pelvic floor trauma. Therefore, our findings which are based on 4D ultrasound imply that vaginal delivery is an independent risk factor for levator ani muscle injury and over distension of the genital hiatus 6 weeks after childbirth.
Keywords: levator ani muscle avulsion, levator hiatus, mode of delivery, vaginal delivery, cesarean section
Background
Pelvic floor disorders (PFD), a highly prevalent gynecological condition in women that may occur throughout life, are characterized by a wide range of disorders with the most common clinical presentations being pelvic organ prolapse and urinary incontinence.1 Notably, approximately one-third of adult women worldwide develop varying degrees of PFD.2 Epidemiological studies have revealed that the prevalence of PFD is 25% among Chinese women, with pelvic organ prolapses affecting up to 9.6% of this population.3 Although not life-threatening, PFD is an under-reported problem that has a significant negative impact on women’s quality of life.4,5 Unfortunately, the current management of PFD is based on expert opinion,6 and the rate of repeated surgical procedures is as high as 30%.7 Therefore, early identification of women at risk of PFD to reduce the probability of developing more severe pelvic organ prolapse is of clinical significance worldwide.8
Emerging evidence has highlighted that vaginal delivery is the most important risk factor for the developing of PFD,9,10 making it a primary concern for postpartum women. During vaginal delivery, fetal head compression leads to widespread mechanical injury to the pelvic floor tissue, which is one of the main causes of anatomical and functional alterations in the pelvic floor muscles, which are mainly composed of the levator ani muscles (LAM). It was found that the phase of delivery that caused overstretching in the LAM area was when the fetal head reaches the 4th plane of Hodge,11 at which point the LAM injury occurred,10 known as LAM avulsion. The association between LAM injury and PFD occurrence has been widely described in the literature.10,12 Moreover, the injury was present in 55% of women with pelvic organ prolapse later in life, with an odds ratio of 7.3 compared with women with normal support.10 Besides, the levator hiatus, which was found to be the missing link between LAM avulsion and pelvic organ prolapse,13 was also the principal etiological factor in the development of PFD.14 Collectively, these findings establish the importance of vaginal birth in the occurrence of PDF.
As mentioned above, the question remains: What is the association between LAM defects and changes in levator hiatus area to cesarean section? Despite numerous focusing on postpartum pelvic floor injury in women after vaginal delivery, the impact of cesarean section on pelvic floor dysfunction after childbirth is unclear. Furthermore, a few similar studies have concentrated on comparisons between both modes of delivery by combining elective and emergency cesarean sections. More importantly, in the era of personalized medicine, a better understanding of why an injury occurs is necessary to improve preventative strategies.15,16 Thus, the primary endpoint of this study was to conduct a comparison between individuals with a vaginal birth and women who underwent a cesarean section based on the use of four-dimensional transperineal ultrasound to assess the structural alterations in LAM shape and levator hiatus configuration 6 week postpartum. According to the literature, the recovery of levator hiatus in Asian primipara began at 2 weeks,17 furthermore, a prospective observational cohort study with 362 women reported that LAM trauma can reliably be diagnosed during 6–10 weeks.18 As previously described, we chose 6 weeks postpartum as the endpoint, which is the time for postpartum women to return to the hospital for follow-up examinations. The secondary endpoint was to establish whether cesarean section with different surgical indications was highly correlated with LAM avulsion and dimensional changes of levator hiatus during early postpartum.
Materials and Methods
Study Design
This retrospective cohort study was performed in seven obstetrics departments affiliated with the Hefei Maternal and Child Health Care Hospital, Hefei, China, between February 2024 and March 2025, which is the largest tertiary obstetrics and gynecology hospital in Anhui Province. In addition, all variables were collected retrospectively in the database. Owing to the retrospective design of the study, the need to obtain informed consent from eligible women was waived by the institutional ethics committee of the Hefei Maternal and Child Health Care Hospital. This retrospective study was approved by the Institutional Ethics Committee of Hefei Maternal and Child Health Care Hospital (The ethical approval numbers were YYLL20250521-AHMH-HYLL-03-1.0) and conducted in accordance with the Declaration of Helsinki.
Women who delivered in the obstetrical department and underwent pelvic floor ultrasound examination at the postpartum rehabilitation clinic at 6 weeks postpartum were included. At this visit, all women underwent an identical assessment, including a standardized interview, history, and clinical examination, and completed a validated pelvic floor system assessment.
The exclusion criteria were delivery in our maternity ward with placenta previa, multiple gestations, history of pre-existing pelvic floor disorders (such as chronic pelvic pain, pelvic organ prolapse, urinary or fecal incontinence), and history of pelvic floor treatment or surgery.
Basic demographic, obstetric, and delivery data were extracted from hospital databases and patient records, including maternal age, pre-pregnancy body mass index (BMI), pregnancy BMI, gravidity, parity, gestational weeks at delivery, weight gain during pregnancy, complications of pregnancy-induced hypertension or gestational diabetes mellitus, and neonatal weight.
Ultrasound parameters of the pelvic floor structures, including the LH and LAM ultrasound measurements, were obtained from the institutional ultrasonic database.
The primary outcomes focused on the association between delivery route and LAM avulsion, as well as levator hiatus size diagnosed on 4D transperineal ultrasound. In addition, subgroup analysis was performed to differentiate the shape and dimensional changes of the LAM and levator hiatus between different surgical indications.
Sonographic Procedures
In our hospital, all pelvic floor ultrasound examinations were performed by two certified sonographers, each with over five years of experience in ultrasound technology. Both operators adhered to a standardized scanning protocol. Additionally, during the image analysis phase, the two sonographers were blinded to the delivery mode of the patients. Regarding quality control, all acquired ultrasound images were systematically reviewed by a second senior sonographer who was not the initial operator, to confirm adequate image quality and clear visualization of key anatomical structures.
Four-dimensional transperineal sonography was performed to assess pelvic floor anatomy, including imaging of the LAM and levator hiatus. The woman was placed in the lithotomy position with an empty bladder using a 4D pelvic ultrasound (GE Voluson E8, USA) with a RAB6-D curved array volume transducer with minimum pressure. Volume acquisition was performed using the maximum Valsalva maneuver to valuation of levator hiatus dimensions and maximum pelvic floor muscle contraction for the diagnosis of levator avulsion.
Generally, the initial plane is the mid-sagittal plane, which is needed to display structures such as the pubic symphysis, urethra, vagina, anal canal, and levator ani muscle. The 4D scanning mode was activated to obtain pelvic floor volume data, displaying an axial plane at 2.5-mm slice intervals. The LAM was imaged from 5 to 12.5 mm above the plane with minimal dimensions. Minimal dimensions were defined as the minimal distance between the posterior aspect of the symphysis pubis and the anterior border of the levator ani muscle posterior to the anorectal muscle. LAM avulsion was diagnosed if all three central images corresponding to the plane of minimal hiatal dimensions, 2.5 mm and 5 mm above this plane of reference, showed a separation of the muscle from the inferior pubic ramus. The LAM defect was evaluated on pelvic floor muscle contraction.
The hiatal area was acquired at the maximum Valsalva. Initially, the plane of minimal hiatal dimensions was identified in the mid-sagittal plane, and a rendered volume in the axial plane of 1–2 cm thickness was generated to allow hiatus measurements. Under normal circumstances, the hiatus area is ≤20 cm2 during the maximum Valsalva maneuver in Chinese women.
Definition
Pregnancy-induced hypertension was defined as a systolic blood pressure ≥140 mmHg and/or diastolic BP ≥ 90 mmHg occurring at or after 20 gestational weeks without significant proteinuria.
Gestational diabetes mellitus refers to abnormal glucose intolerance of varying degrees, which is first diagnosed in the second or third trimester of pregnancy.
Statistical Analysis
Statistical analyses were performed using SPSS (version 13.0; SPSS Inc., Chicago, IL, USA). The counting variables were expressed as percentages. Continuous variables are expressed as mean and standard deviation (SD). The continuous variables all followed a normal distribution; therefore, comparisons between groups were performed using the T test for continuous variables and the chi-square test for categorical variables. Multivariate analysis was performed using a logistic regression model to identify the association between the different delivery modes and the risk of LAM avulsions and hiatal enlargement. Odds ratios (OR) and 95% confidence intervals (CI) were used to quantify this association. Women were categorized into three groups according to the primary recorded indication for cesarean delivery: 1. Primary cesarean section group: Cesarean section performed for non-laboring indications; 2. Intrapartum cesarean section group: Cesarean section performed after the onset of labor; 3. Selective cesarean section group: Cesarean section due to a history of cesarean section. Multivariate logistic regression analysis was used to quantify the association between different surgical indications and the risk for the levator hiatus overstretching. Regarding the LAM avulsion, due to the low incidence rate in cesarean section subgroup, therefore, it was difficult to analyze different surgical indications and association with LAM avulsion by multivariate logistic regression analysis. Odds ratios (OR) and 95% confidence intervals (CI) were used to quantify this association. Statistical significance was set at P < 0.05.
Results
During the study period, there was a total of 3837 subjects delivering in our institution, among which 2800 underwent pelvic floor ultrasound examination. Finally, 1930 cases met the study inclusion criteria. The two groups were categorized according to the mode of delivery: Group 1 (vaginal delivery group, 1224 cases) and Group 2 (cesarean section group, 706 cases).
In addition, when participants in the cesarean section group were stratified according to surgical indications, three subgroups were allocated, including 193 women who underwent cesarean sections due to a history of cesarean surgery (scarred uterus group), 432 women with primary cesarean section because of fetal malpresentation, fetal distress, and maternal request (primary cesarean section group), and 81 who underwent intrapartum cesarean sections (intrapartum cesarean section group).
The baseline information of the vaginal delivery and cesarean section groups are shown in Table 1. Statistically significant differences were found in terms of the maternal age, gestational age at birth, pre-pregnancy BMI, pregnancy BMI, weight gain during pregnancy, percentages of cesarean sections due to scarred uterus and intrapartum cesarean sections, infant birth weight, gravidity, parity, and complicated with pregnancy induced hypertension (P < 0.001, < 0.001, < 0.001, < 0.001, < 0.001, < 0.001, < 0.001, < 0.001, < 0.05, < 0.05, and < 0.05, respectively). Conversely, no statistically significant differences were observed regarding gestational diabetes complications (P > 0.05).
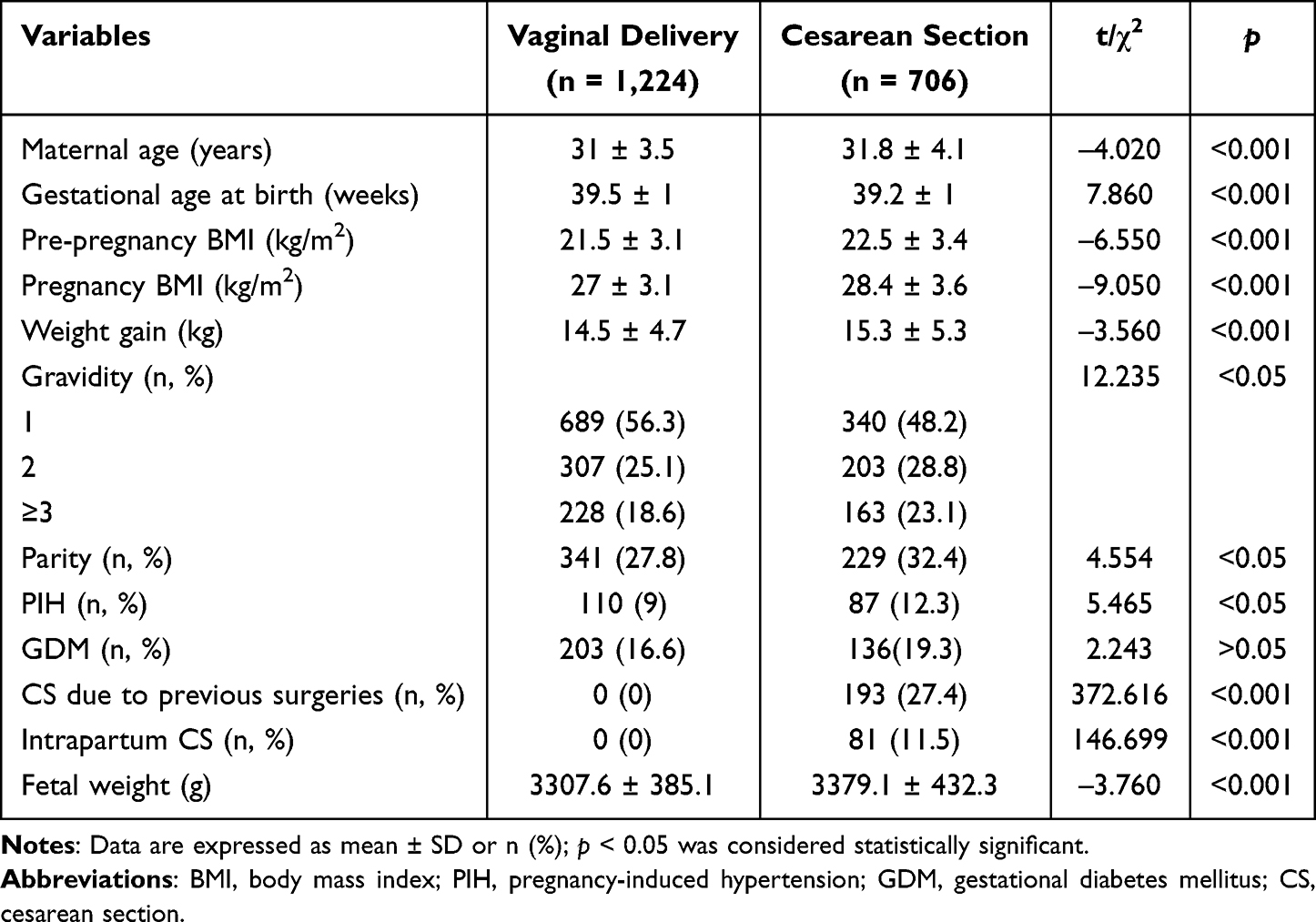 |
Table 1 Comparison of Baseline Characteristics Between Vaginal Delivery Group and Cesarean Section Group |
Table 2 shows the incidence of LAM avulsion and levator hiatus overdistension between vaginal delivery group and cesarean section group. Clinically significant differences were observed regarding the rates of levator avulsion (3.7% VS 0.3%) as well as levator hiatus overdistension (72.5% VS 41.8%) and mode of delivery (both P < 0.001).
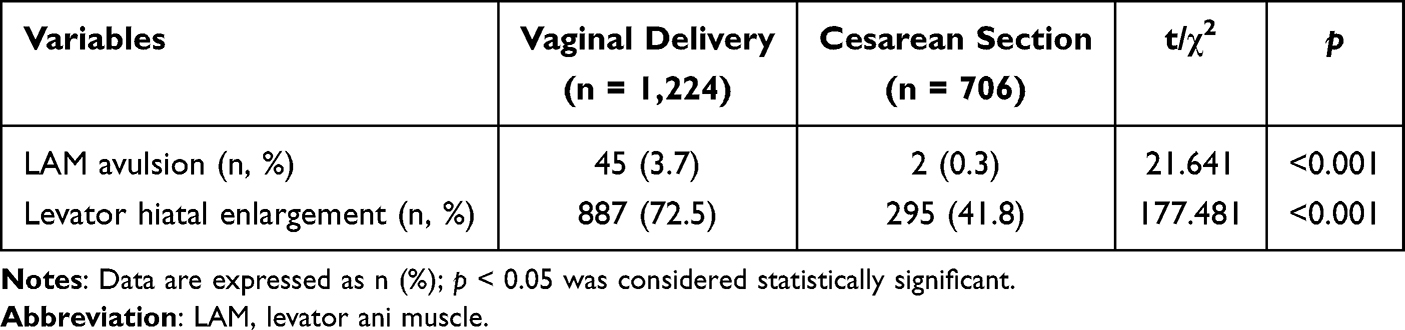 |
Table 2 Comparison of LAM Avulsion and Levator Hiatus Overdistension Between the Vaginal Delivery Group and Cesarean Section Group |
Table 3 describes the results of the multivariate logistic analysis of the association between LAM avulsion, levator hiatus overdistension, and different delivery modes. After adjusting for confounders, including maternal age, gestational age at birth, pre-pregnancy BMI, pregnancy BMI, weight gain during pregnancy, infant birth weight, gravidity, parity, and complications of pregnancy-induced hypertension or gestational diabetes mellitus, we found that only vaginal delivery was associated with LAM avulsion and levator hiatus overdistension (OR = 6.58, 95% CI = 1.55–27.87, P < 0.05; OR = 4.31, 95% CI = 3.30–5.61, P < 0.001, respectively).
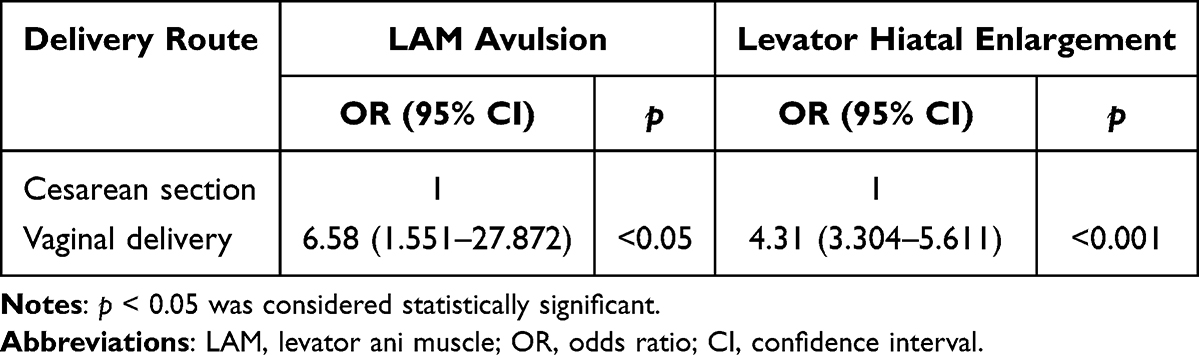 |
Table 3 Multivariate Logistic Regression Analysis of the Association Between LAM Avulsion/Levator Hiatus Overdistension and Delivery Route |
Table 4 lists the results of the multivariate logistic analysis of the association between excessive distension of the levator hiatus and cesarean section according to different surgical indications. After controlling for the confounding factors, no significant association was observed between levator hiatus overdistension and the three surgical indication groups (P = 0.162 and P = 0.313, respectively).
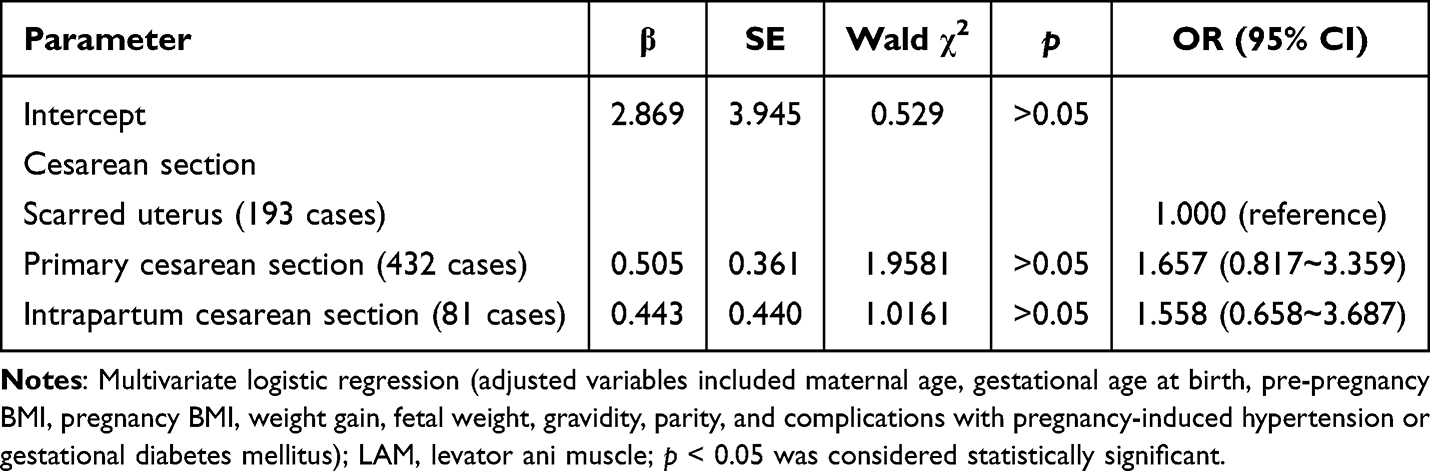 |
Table 4 Multivariate Logistic Regression Analysis of Association Between Cesarean Section Indications and Levator Hiatus Overdistension |
Discussion
In our study cohort, vaginal delivery was an independent risk factor for the development of LAM avulsion and larger levator hiatus area 6 weeks of delivery. Additionally, compared with women who underwent cesarean section, those with vaginal delivery were 6.58 times more likely to have LAM avulsion and 4.31 times more likely to experience a larger levator hiatus dimensions at 6 weeks after birth. Furthermore, a relationship between an enlarged hiatus and cesarean section based on different surgical indications has not yet been established.
During childbirth, the LAM undergoes a series of changes that can lead to the loss of morphological and/or functional integrity,19 resulting in the subsequent occurrence of PFD.10 One study highlighted a strong relationship between vaginal birth and LAM avulsion.20 Additionally, LAM avulsion during vaginal delivery was reported to occur in nearly one in every five deliveries.21 Specifically, compared to cesarean section, vaginal deliveries were associated with an odds ratio of 11 for LAM avulsion.22 In contrast, this condition was not observed in women after cesarean section.23,24 Our findings were similar to those studies, and we did not find an association between LAM avulsion and cesarean delivery. However, the populations in the abovementioned studies differed completely from ours and were a selected cohort of women studied 5–10 years after their first childbirth. Conversely, our findings were based on a larger sample, and only participants at 6 weeks postpartum were recruited, providing reliable results on this issue. Furthermore, we quantified the association between LAM avulsion and different delivery methods, finding that women with vaginal deliveries had a 6.58-fold increased risk of developing LAM avulsion. Hence, our results are valuable in clinical practice for educating patients and healthcare providers on the implications of delivery routes to the pelvic floor muscle during early postpartum.
Regarding the levator hiatus area, which was found to increase by 29% from the first to the third trimester, in preparation for childbirth.25 Hence, an enlarged hiatus during pregnancy can be interpreted as a preparation for uncomplicated delivery. After vaginal delivery, nearly 70% of women had a natural “recovery” of the levator hiatus dimensions.26 Specifically, in Asian primipara, the levator hiatus muscle began to recover within the first 2 weeks postpartum.17 Consequently, the parameters of the levator ani hiatus had a significant association with different types of PFD.27 Therefore, we designed this retrospective study of a large dataset of several thousand women to determine the levator hiatus region based on different delivery routes after 6 weeks postpartum. Our research specifically sought out adjustment of known confounding factors and quantification of the association between delivery method and levator hiatus overdistension. According to our results, we demonstrated that vaginal delivery was a predisposing factor for hiatal hiatus overdistension after delivery; women with vaginal birth had a 4.31 fold higher risk of hiatal hiatus overdistension compared to those who underwent cesarean section. Therefore, in light of the present data, we believe that the delivery mode is the etiological factor in the development of levator hiatal overstretching, mediated by mechanical trauma that occurs during the delivery process.
Currently, limited data are available regarding the association between cesarean section and changes in pelvic floor biometry. A study conducted in Black South African women showed significant alterations in postpartum levator hiatal distensibility, with more pronounced effects in women after vaginal delivery,28 whereas cesarean section was found to be protective.29 Similar results were observed in a prospective observational study, demonstrating that differences existed at 6 weeks postpartum between the vaginal and cesarean delivery groups considering the measurement of levator hiatus.30 Notably, none of these studies investigated the distinctive contribution of cesarean section deliveries due to the different surgical indications for levator trauma and an enlarged hiatus. Our analysis specifically aimed to identify the association between different surgical indications and the magnitude of pelvic floor injury 6 weeks after birth, a worthwhile and interesting evaluation that is lacking in the current literature. In the present study, the three surgical indications represented different stages of labor. An elective cesarean section (scarred uterus group and primary cesarean section group, including maternal request, non-reassuring fetal heart rate patterns, abnormal fetal position) was performed without labor, whereas the intrapartum cesarean section group served as one before full cervical dilation or one in full dilatation conditions and before fetal extraction. After statistical analysis, it can be noted that neither surgical indication was a significant risk factor contributing to an enlarged hiatus in our population. Therefore, our results do add credence to the idea that a major increase in the levator hiatus area is at the moment of crowning of the fetal head.
The main limitation of our study is its retrospective nature, thus, potential selection bias from women attending the postpartum clinic cannot be ruled out. Second, the study only demonstrated an association with early postpartum ultrasound abnormalities, while long-term clinical outcomes were absent, making it important to study separately. However, this study also included a number of strengths. A strength of our study was that it was conducted in different maternal fetal centers belong to the same hospital with unified training of operating standards, as it lowers the risk of differences in protocols for care during labor and delivery, such as labor management during delivery, episiotomy rates, and standard perineal protection procedures, which may potentially affect the incidence of pelvic floor damage. In addition, our sample size was sufficient to perform a reliable multivariate analysis to evaluate the association between different delivery routes and pelvic floor morphological changes.
In conclusion, the current major knowledge gap is the absence of reliable means to rapidly identify individuals with an elevated risk of LAM damage so that we can find interventions to better prevent this damage, thereby reducing the risk of PFD later in life. In the present study, we provided original data on the assessment of the morphological structure of the pelvic floor during early postpartum, based on simple 4D ultrasound. Our findings imply that the delivery mode may contribute to changes to the pelvic floor structures, and women with vaginal delivery were strongly associated with LAM avulsion and hiatal enlargement. In addition, the rates of excessive hiatal distensibility at 6 weeks postpartum were comparable between the different surgical indication groups. Therefore, we believe that our findings might be of general value, as early diagnosis and intervention are fundamental concepts in the treatment of musculoskeletal trauma, and this investigation is informative to clinicians to improve patient care and decision management. Furthermore, ongoing prospective longitudinal research is vital to reveal the persistence of these abnormalities and their relationship to symptomatic pelvic floor disorders.
Patient Data Confidentiality
To ensure patient data confidentiality, all personal identifiers (such as names, identification numbers, dates of birth, and contact information) were removed from the dataset immediately after collection. Each participant was assigned a unique study code. The anonymized data were stored on a password-protected and encrypted institutional server, with access restricted to authorized research personnel only. All analyses were performed on this de-identified dataset.
Abbreviations
LAM, Levator ani muscle; BMI, Body mass index; SD, Standard deviation; OR, Odds ratios; CI, Confidence intervals.
Data Sharing Statement
The datasets analyzed in this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This retrospective study was approved by the Hefei Maternal and Child Health Care Hospital and was conducted in accordance with the Declaration of Helsinki. The requirement for informed consent was waived by the Institutional Review Board due to the retrospective nature of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Doumouchtsis SK, De Tayrac R, Lee J, et al. An International Continence Society (ICS)/International Urogynecological Association (IUGA) joint report on the terminology for the assessment and management of obstetric pelvic floor disorders. Int Urogynecol J. 2023;34:1–8. doi:10.1007/s00192-022-05397-x
2. Pang H, Zhang L, Han S, et al. A nationwide population-based survey on the prevalence and risk factors of symptomatic pelvic organ prolapse in adult women in China - a pelvic organ prolapse quantification system-based study. BJOG. 2021;128:1313–1323. doi:10.1111/1471-0528.16675
3. Shen L, Yang J, Bai X, Sun Z. Analysis of the current status of pelvic floor dysfunction in urban women in Xi’an City. Ann Palliat Med. 2020;9:979–984. doi:10.21037/apm-20-784
4. Augustina SJ, Suganthirababu P, Rajagopal V, et al. Pelvic floor dysfunction and its impact on quality of life among female health care employees. Work. 2023;74:1055–1059. doi:10.3233/WOR-211125
5. Fontenele MQS, Moreira MA, de Moura ACR, de Figueiredo VB, Driusso P, Nascimento SL. Pelvic floor dysfunction distress is correlated with quality of life, but not with muscle function. Arch Gynecol Obstet. 2021;303:143–149. doi:10.1007/s00404-020-05770-5
6. Giagio S, Innocenti T, Pillastrini P, Gava G, Salvioli S. What is known from the existing literature about the available interventions for pelvic floor dysfunction among female athletes? A scoping review. Neurourol Urodyn. 2022;41:573–584. doi:10.1002/nau.24883
7. Schulten SFM, Claas-Quax MJ, Weemhoff M, et al. Risk factors for primary pelvic organ prolapse and prolapse recurrence: an updated systematic review and meta-analysis. Am J Obstet Gynecol. 2022;227:192–208. doi:10.1016/j.ajog.2022.04.046
8. Woodley SJ, Lawrenson P, Boyle R, et al. Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst Rev. 2020;5:CD007471. doi:10.1002/14651858.CD007471.pub4
9. Jansson MH, Franzén K, Tegerstedt G, Brynhildsen J, Hiyoshi A, Nilsson K. Fecal incontinence and associated pelvic floor dysfunction during and one year after the first pregnancy. Acta Obstet Gynecol Scand. 2023;102:1034–1044. doi:10.1111/aogs.14614
10. DeLancey JOL, Masteling M, Pipitone F, LaCross J, Mastrovito S, Ashton-Miller JA. Pelvic floor injury during vaginal birth is life-altering and preventable: what can we do about it? Am J Obstet Gynecol. 2024;230:279–294.e2. doi:10.1016/j.ajog.2023.11.1253
11. Mejido JAG, Serrano CMS, Palacín AF, Pino AA, Barby MJB, Bueno JAS. Evaluation of levator ani muscle throughout the different stages of labor by transperineal 3D ultrasound. Neurourol Urodyn. 2017;36:1776–1781. doi:10.1002/nau.23175
12. Schütze S, Hohlfeld B, Friedl TWP, et al. Fishing for (in)continence: long-term follow-up of women with OASIS-still a taboo. Arch Gynecol Obstet. 2021;303:987–997. doi:10.1007/s00404-020-05878-8
13. Handa VL, Roem J, Blomquist JL, Dietz HP, Muñoz A. Pelvic organ prolapse as a function of levator ani avulsion, hiatus size, and strength. Am J Obstet Gynecol. 2019;221:
14. Lin C, Huang W, Li X, et al. Diagnostic value of combined pelvic floor ultrasound parameters for pelvic floor dysfunction and risk factors. J Clin Ultrasound. 2023;51:465–471. doi:10.1002/jcu.23397
15. Pipitone F, Miller JM, DeLancey J. Injury-associated levator ani muscle and anal sphincter ooedema following vaginal birth: a secondary analysis of the EMRLD study. BJOG. 2021;128:2046–2053. doi:10.1111/1471-0528.16760
16. Youssef A, Brunelli E, Pilu G, Dietz HP. The maternal pelvic floor and labor outcome. Am J Obstet Gynecol MFM. 2021;3:100452. doi:10.1016/j.ajogmf.2021.100452
17. Yang Z, Zhou L, Yang L, He H. Restoration of bladder neck activity and levator hiatus dimensions in Asian primipara: a prospective study. J Obstet Gynaecol. 2023;43:2173564. doi:10.1080/01443615.2023.2173564
18. Kreft M, Cai P, Furrer E, Richter A, Zimmermann R, Kimmich N. The evolution of levator ani muscle trauma over the first 9 months after vaginal birth. Int Urogynecol J. 2022;33:2445–2453. doi:10.1007/s00192-021-05034-z
19. Kubotani J, Araujo E, de Queiroz Campos A, Passos J, Do Nascimento Neri C, Diniz Zanetti M. Physiotherapeutic treatment for levator ani avulsion after delivery: a transperineal three-dimensional ultrasound assessment. J Med Ultrasound. 2020;28:245–248. doi:10.4103/JMU.JMU_43_20
20. Dietz HP. Ultrasound imaging of maternal birth trauma. Int Urogynecol J. 2021;32:1953–1962. doi:10.1007/s00192-020-04669-8
21. Cassadó J, Simó M, Rodríguez N, et al. Prevalence of levator ani avulsion in a multicenter study (PAMELA study). Arch Gynecol Obstet. 2020;302:273–280. doi:10.1007/s00404-020-05585-4
22. Rusavy Z, Paymova L, Kozerovsky M, et al. Levator ani avulsion: a systematic evidence review (LASER). BJOG. 2022;129:517–528. doi:10.1111/1471-0528.16837
23. Blomquist JL, Muñoz A, Carroll M, Handa VL. Association of delivery mode with pelvic floor disorders after childbirth. JAMA. 2018;320:2438–2447. doi:10.1001/jama.2018.18315
24. Blomquist JL, Carroll M, Muñoz A, Handa VL. Pelvic floor muscle strength and the incidence of pelvic floor disorders after vaginal and cesarean delivery. Am J Obstet Gynecol. 2020;222:
25. Cheng W, English E, Horner W, et al. Hiatal failure: effects of pregnancy, delivery, and pelvic floor disorders on level III factors. Int Urogynecol J. 2023;34:327–343. doi:10.1007/s00192-022-05354-8
26. Schmidt P, Swenson CW, O DeLancey J, Chen L. Postpartum changes in levator plate shape and genital hiatus size after vaginal delivery. Int Urogynecol J. 2024;35:1413–1420. doi:10.1007/s00192-024-05813-4
27. Zhuang Y, Yao L, Liu Y. Value of transperineal three-dimensional ultrasonography in diagnosis of pelvic floor dysfunction. Br J Radiol. 2024;97:1799–1805. doi:10.1093/bjr/tqae145
28. Abdool Z, Lindeque BG, Dietz HP. The impact of childbirth on pelvic floor morphology in primiparous Black South African women: a prospective longitudinal observational study. Int Urogynecol J. 2018;29:369–375. doi:10.1007/s00192-017-3530-1
29. Friedman T, Eslick GD, Dietz HP. Delivery mode and the risk of levator muscle avulsion: a meta-analysis. Int Urogynecol J. 2019;30:901–907. doi:10.1007/s00192-018-3827-8
30. Liu Y, Liu P, Peng C, et al. Three-dimensional magnetic resonance imaging assessment of levator ani in women progressing from full-term pregnancy to 10 months postpartum. J Obstet Gynaecol Res. 2022;48:2552–2562. doi:10.1111/jog.15370
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Retrospective Analysis of Gut Microbiota and Metabolomic Profiles in Pregnant Women: Association with Cesarean Section Risk
Yuan J, Wang Y, Liu L
International Journal of Women's Health 2025, 17:1763-1770
Published Date: 12 June 2025
Insulin Resistance as a Biomarker for Pelvic Organ Prolapse in Gestational Diabetes Mellitus: Stratification by Delivery Modes
Jiao Y, Dai Y, He L, Fei Z
International Journal of General Medicine 2025, 18:6377-6385
Published Date: 21 October 2025
Clinicians’ Personal Delivery Preference and Decision-Making for Cesarean Delivery: A Survey of Obstetricians and Midwives
Aldardeir NF, Sulaimani MA, Bahowarth SY, Almanasif M, Alghamdi YS, Aseeri SS, Alsulymani B, Heggi R, Hasanain R, Alyazidi A
Risk Management and Healthcare Policy 2026, 19:562709
Published Date: 7 February 2026