Back to Journals » Patient Related Outcome Measures » Volume 16
Clinician and Researcher Experiences with Goal Attainment Scaling: A Qualitative Study on Opportunities and Challenges for Personalized Outcome Assessments
Authors Sevinc G ![]() , Escoto-Rivera A, Crespo K
, Escoto-Rivera A, Crespo K ![]() , Nesto S, Chapman CA, Rockwood K
, Nesto S, Chapman CA, Rockwood K ![]()
Received 21 October 2025
Accepted for publication 6 May 2026
Published 27 May 2026 Volume 2025:16 Pages 355—366
DOI https://doi.org/10.2147/PROM.S569608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Mithi Ahmed-Richards
Gunes Sevinc,1 Andrea Escoto-Rivera,1 Katie Crespo,1,2 Sue Nesto,1 Chere AT Chapman,1 Kenneth Rockwood1,3,4
1Ardea Outcomes, Halifax, Nova Scotia, Canada; 2College of Pharmacy, Faculty of Health, Dalhousie University, Halifax, Nova Scotia, Canada; 3Division of Geriatric Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 4Geriatric Medicine Research Unit, Nova Scotia Health Authority, Halifax, Nova Scotia, Canada
Correspondence: Gunes Sevinc, Ardea Outcomes, 200-1741 Lower Water Street, Halifax, NS, B3J 0J2, Canada, Email [email protected]
Purpose: Goal Attainment Scaling (GAS) is a personalized outcome measure that evaluates treatment response based on patient- and caregiver-prioritized goals, offering a structured yet flexible framework for assessing meaningful change. Although GAS is increasingly applied in clinical trials, its implementation remains inconsistent, and the perspectives of clinicians and researchers who use it in practice remain poorly understood. This study explored the experiences of clinicians and researchers with GAS to better understand how it is operationalized, the challenges encountered, and opportunities to improve its consistency and utility in patient-centered care and research.
Participants and Methods: Semi-structured interviews were conducted with 11 clinicians and academics from Canada, the United States, the United Kingdom, and Australia who had experience using GAS in clinical or research settings. Data were analyzed thematically using the Framework Method, with coding conducted inductively and supported by NVivo 12.
Results: Participants valued GAS for capturing outcomes most meaningful to patients and demonstrating treatment responsiveness in heterogeneous conditions. However, clinician resistance, time demands, limited familiarity, and variability in implementation across settings were identified as key challenges. Education, peer advocacy, and digital tools were suggested as strategies to improve feasibility and consistency.
Conclusion: Clinicians and researchers view GAS as a valuable patient-centered outcome measure but highlight variability in implementation as a barrier to broader adoption. Guidelines for GAS implementation, training, and supportive tools may strengthen the use of GAS in both clinical practice and research, ultimately improving the measurement of outcomes that matter most to patients.
Plain Language Summary: Goal Attainment Scaling (GAS) is a personalized way of measuring health outcomes. Instead of relying only on standardized tests, GAS focuses on goals that patients and caregivers identify as most important to them. This approach makes it possible to assess meaningful changes in quality of life, even when people have very different symptoms or needs. GAS has been used in many different contexts, including both research and clinical practice, but it is applied in various ways. We interviewed 11 clinicians/researchers about how they used GAS, the challenges they encountered, and opportunities to improve its consistency and utility in patient-centered care and research. Participants reported that they value GAS because it can capture what matters most to patients and show whether treatments are making a difference. Overall, the findings show that GAS is a promising, patient-centered outcome measure, however clearer guidelines, education, and supportive resources are needed to expand its use.
Keywords: patient-reported outcomes, implementation, patient-centered care, health services research, personalized outcome assessment, goal attainment scaling
Introduction
Personalized outcome assessments, such as Goal Attainment Scaling (GAS), provide a structured yet flexible approach to capturing patients’ lived experiences with treatment, including impacts on quality of life and other personally meaningful outcomes.1 In GAS, patients and/or their caregivers collaborate with clinicians to define and scale a set of individualized goals, targeting symptoms or functional domains that are most relevant to them and also targeted by the intervention.1,2 Goal attainment is then assessed at a prespecified follow-up, and an overall score is calculated using a standardized approach (see Table 1). By combining individualized goal setting with a quantifiable scoring framework, GAS enables the detection of meaningful changes that may be overlooked by standardized, fixed-item measures. As such, it represents a robust method for operationalizing patient-centered outcome assessment in both clinical practice and research settings.
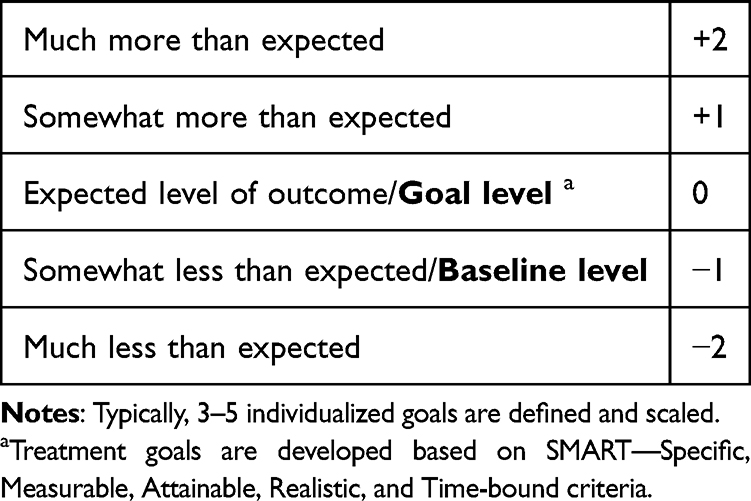 |
Table 1 Goal Attainment Scaling |
Patient-reported outcome measures (PROMs) directly capture patients’ perspectives on their health and care.3–5 Building on this foundation, GAS offers distinct advantages, particularly in conditions with heterogeneous clinical profiles. By focusing on outcomes that are both personally meaningful and targeted by the intervention, GAS avoids the dilution of treatment effects often seen with fixed-item measures. It also avoids the arbitrariness of universal thresholds for clinically meaningful improvement, as it anchors improvement to individualized targets.6,7 Despite its evident strengths, we know little about the perspectives of clinicians and researchers responsible for its implementation. The limited attention paid to the experiences of clinicians and researchers leaves important questions about feasibility, acceptability, and methodological rigor insufficiently addressed.
Originally developed to evaluate mental health services, GAS has since been adapted for use across diverse patient populations and healthcare settings, resulting in substantial methodological variability.8,9 This includes differences in goal development, rater independence, scale structure, scoring, and training, which can limit comparability and pose challenges to broader adoption. Despite this variability, most studies to date have focused on patient perspectives, with less attention to the experiences of clinicians and researchers.10–12 While patients highlight GAS’s collaborative and person-centered nature, other stakeholders may hold differing views regarding feasibility, burden, and methodological rigor. Moreover, implementation is influenced by contextual factors such as disease characteristics, care settings, and available expertise. Together, these gaps underscore the need to better understand how GAS is applied across contexts and stakeholder groups, a question for which qualitative methods are particularly well suited.
Accordingly, this study qualitatively explores the perspectives of clinicians and researchers on the use of GAS, including their motivations for adoption, approaches to operationalization, and perceived challenges or gaps. As clinical trials increasingly incorporate patient-reported outcomes, such as GAS, as primary, secondary, or exploratory endpoints, these insights may inform strategies to improve GAS implementation and support standardization in research settings, and to enhance broader adoption of this patient-centric method.5,13
Methods
Study Design and Participant Recruitment and Consent
This qualitative study explored the evolving use of GAS in clinical practice and research. Clinicians and academics with current or past experience and a working knowledge of GAS, using it either in clinical care or as an outcome measure in research studies were interviewed to examine their implementation strategies, perceived benefits and challenges, and the features they would consider essential in an electronic tool to support GAS implementation.
The study employed purposive sampling to capture a heterogeneous range of perspectives across roles, regions, and experience levels. Between June and July 2022, 16 individuals with expertise in GAS, identified through the researchers’ existing professional networks were invited to participate via email. Out of those individuals 11 consented and were interviewed, while the remaining individuals did not respond (n=4) or declined (n=1) participation. Prospective participants who expressed interest received a consent form outlining the study’s objectives and procedures and virtual interviews were scheduled.
The study protocol and all associated materials were reviewed and received full ethical approval from the National Research Council of Canada, Research Ethics Board (Approval No. 2022–67). All participants gave written informed consent prior to participation, including consent for the publication of anonymized quotes. The study was conducted in accordance with the ethical standards of the institutional Research Ethics Board and the Declaration of Helsinki.
Data Collection: Qualitative Interviews
One-on-one interviews were conducted virtually using Google Meet by a qualitative researcher, following a semi-structured interview guide (see Supplementary Figure 1). The research team developed the interview guide based on a review of existing GAS literature and consultation with experts, ensuring alignment with the study’s objectives. Interviews were conducted by a researcher with prior training and experience in qualitative methods, ensuring systematic and rigorous data collection. Each interview was conducted with only the participant present, lasted approximately 60 minutes and was both audio and video recorded. At the start of each session, the researcher reviewed the informed consent form, responded to the participant’s questions, and confirmed verbal consent. The researcher then signed the consent form to document the participant’s agreement.
Demographic information, including gender, profession, and years of experience, was collected verbally. Participants were asked open-ended questions about their experiences using GAS in clinical settings or research, including implementation processes, encountered challenges, and perceived requirements for a digital tool to support GAS. Follow-up prompts were used to elicit clarification or elaboration as needed. Field notes were taken to capture contextual information, such as non-verbal cues. Audio recordings were transcribed verbatim by a professional transcriptionist, with all identifying information removed. Transcripts were reviewed and corrected for accuracy by a member of the research team.
Data Analysis
Demographic characteristics (gender, profession, years of experience, and involvement in clinical research or trials) were anonymized and summarized using descriptive statistics. Interview transcripts were analyzed thematically using the Framework Method.14 Two researchers independently coded conducted line-by-line coding of two transcripts, generating inductive codes to capture participants’ perspectives. Coding discrepancies were resolved through discussion, with input from a third researcher when necessary, resulting in a consensus coding framework. This framework was subsequentially applied to the remaining transcripts and iteratively refined as new codes emerged. An audit trail was maintained throughout, documenting coding decisions, codebook development, theme refinement, and summaries of reflexive team discussions, providing transparency and traceability of analytic decisions. All data were managed in NVivo 12. The coded data were then organized within a thematic framework and synthesized into overarching themes, supported by illustrative quotations. The research team’s prior experience with patient-centered care and outcome measurement may have shaped interpretations; reflexive discussions were therefore undertaken throughout the analytic process to enhance rigor.
Results
Participants
Eleven clinicians and academics from Canada (n=4), the United States (n=3), the United Kingdom (n=3), and Australia (n=1) participated in the study. Table 2 summarizes participant demographics. Note that participants often held overlapping roles, with many identifying as both clinicians and researchers; therefore, role categories (clinician vs academic) were not mutually exclusive.
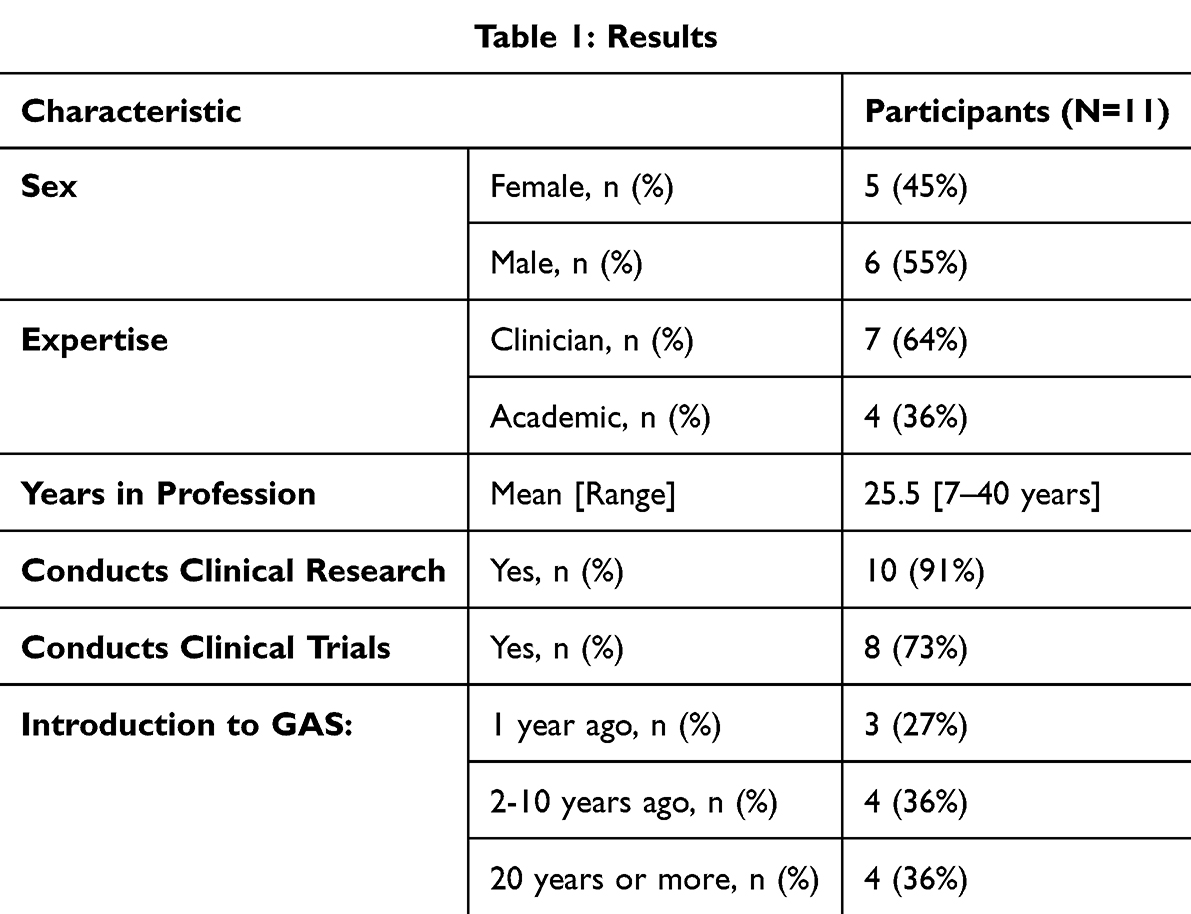 |
Table 2 Clinician and Academic Participant Demographic Information |
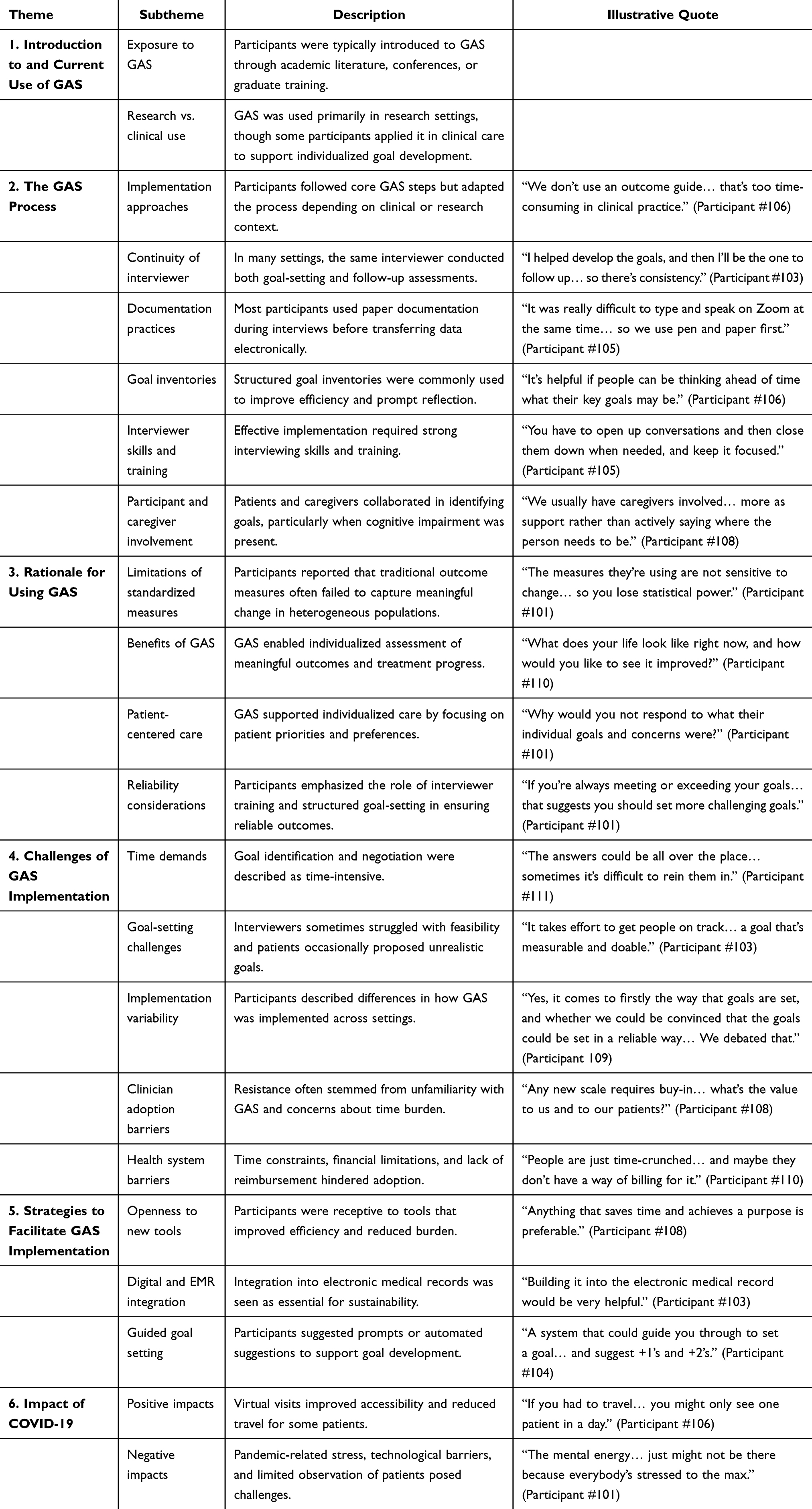 |
Table 3 Themes, Subthemes, and Illustrative Quotations from Participant Interviews |
Qualitative Interviews
Six themes were identified from the analysis: (1) introduction to and current use of GAS, (2) the GAS process, (3) rationale for using GAS, (4) challenges of GAS implementation, (5) strategies to facilitate implementation, and (6) the impact of COVID-19. The coding tree is presented in Supplementary Table 1. Subthemes and illustrative quotations are presented in Table 3 and summarized in Figure 1.
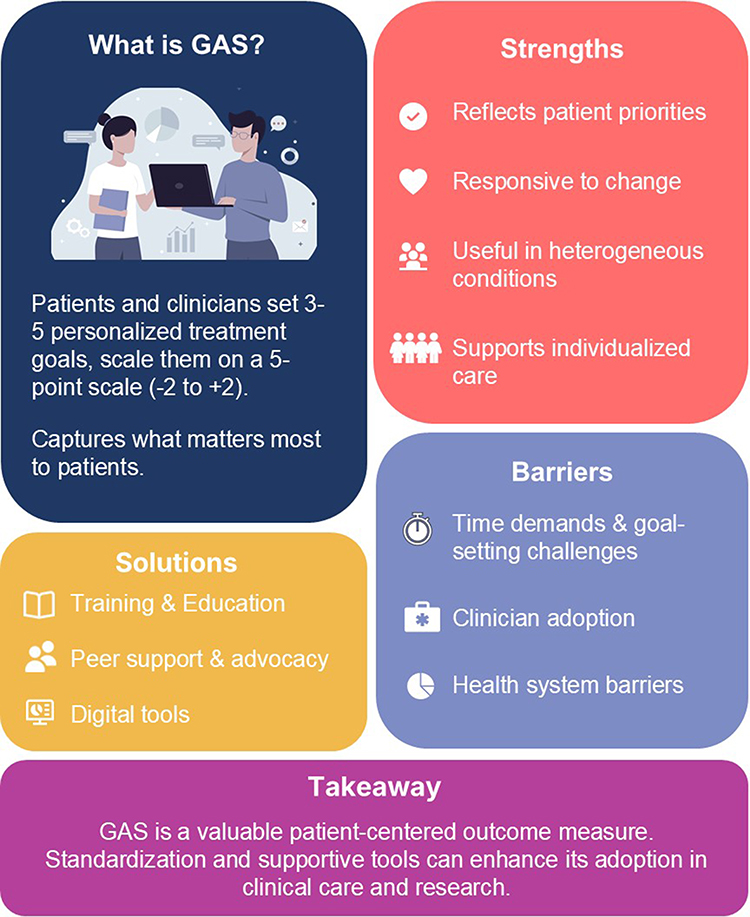 |
Figure 1 Summary of findings. |
Theme 1: Introduction to and Current Usage of GAS
Participants reported varied pathways to learning about GAS most commonly through academic sources such as journal articles, professional conferences (n=5), or graduate training (n=1). Participants reported adopting GAS because it accommodates heterogeneous patient presentations and provides an individualized alternative to standardized outcome measures. Most participants reported using GAS primarily in research contexts (n=7), while a smaller number described using it in clinical care to support personalized goal development and outcome measurement (n=3). One participant highlighted its utility across both domains.
Theme 2: The GAS Process
Participants generally described implementing GAS in ways consistent with the original framework created by Kiresuk & Sherman in 1968—identifying patient priorities, setting personalized goals, developing goal scales, and ranking them by importance—while adapting the process to meet specific clinical or research demands.1 Most participants reported using the standard five-point scale (−2 to +2) (n=6) and emphasized the importance of collaborative goal setting with patients. Implementation approaches varied across settings. In many cases, the same interviewer conducted both goal-setting and follow-up interviews (n=10), although follow-up assessments were sometimes delegated to other clinical or research staff due to time constraints (n=6). Most participants relied on paper documentation during interviews before transferring information electronically, with only two reporting use of electronic clinical outcome assessments (eCOAs). Goal inventories or structured lists of potential goals were widely used to support the process (n=10), as participants reported that these tools improved efficiency and helped prompt patient reflection. However, one participant noted that inventories may introduce clinical terminology that differs from patients’ own language.
Strong interviewing skills were identified as essential for effective GAS implementation (n=9). Participants emphasized the importance of guiding patient discussions, developing measurable goals, and maintaining focus during interviews. Training was highlighted as an important strategy to develop these competencies (n=4). Participants also described GAS as a collaborative process involving both patients and care partners, particularly when individuals had cognitive impairments.
Participants described GAS as a collaborative, patient-centered process in which both patients and care partners played an integral role in identifying meaningful goals. The degree of involvement varied according to patient functioning: high-functioning individuals were often actively engaged in goal setting, whereas caregivers’ input predominated for patients with greater cognitive impairments. Goals identified through this process were generally holistic and relevant, though occasionally unrealistic, creating opportunities for discussion and refinement. Participants noted that patients were rarely educated on the full GAS framework; instead, GAS was often presented as a “to-do list” to guide goal tracking. Strategies to enhance engagement included providing goal category handouts and encouraging patients to track progress through journaling, apps, or written notes.
Theme 3: Why Clinicians and Academics Use GAS
Participants described several motivations for using GAS in both research and clinical practice. Many highlighted limitations of traditional outcome measures (n=10), noting that standardized tools may fail to capture meaningful changes in heterogeneous patient populations.
All participants described benefits of GAS (n=11), particularly its ability to capture outcomes that are meaningful to patients and reflect individualized treatment goals. Participants reported that GAS facilitated tracking of progress, supported more holistic understanding of patient needs, and helped translate goals into practical actions, motivated patients and improved multidisciplinary team communication.
Many participants also emphasized the role of GAS in supporting patient-centered care (n=9), noting that individualized goal setting enabled clinicians to address diverse patient priorities and cultural contexts.
Participants also noted that GAS empowered patients through active participation in goal-setting, fostering autonomy and motivation. They reported that the process helped clinicians gain deeper insight into patients’ priorities and motivations, and that many patients expressed satisfaction with the experience.
They felt very listened to. And we got quite a lot of feedback from people saying that they really [stressed the word really] enjoyed that setting of goals. And I don’t think we’d ever get that in a normal standardized [laughing] questionnaire session. People get quite… you know, don’t engage as well as that. (Participant 105)
Several participants also described GAS as a reliable approach to measuring treatment outcomes (n=7), particularly when interviewers received appropriate training and structured goal-setting methods were used. One participant noted the potential for interviewers to set goals that are too easy, which could produce overly favorable results. However, they explained that the GAS scoring system can reveal this issue:
…there’s a perceived difficulty that… you could game the system by setting goals that are not ambitious enough… I don’t think that holds up in reality… there’s some ability for self-correction based on the scoring system… if you’re always meeting or exceeding your goals… that suggests that you should be setting your goals in a more challenging level. (Participant 101)
Theme 4: Challenges of GAS
All participants described GAS as time-consuming (n=11), particularly during the initial goal identification and negotiation process. Participants noted that patients sometimes struggled to articulate goals or required prompting to develop realistic and measurable objectives.
Additional challenges included interviewer difficulty determining goal feasibility, particularly among those without clinical backgrounds, as well as variability in how GAS was implemented across settings. Some participants noted that the individualized nature of GAS could make comparisons between individuals more complex.
Participants also described barriers to clinician adoption, including limited familiarity with GAS and uncertainty regarding its reliability and value in practice. At the system level, several participants identified broader healthcare barriers (n=6), including time constraints, financial limitations, and lack of reimbursement for GAS assessments.
Theme 5: Strategies to Facilitate GAS Implementation
Participants described several strategies to improve the feasibility of GAS implementation. Many expressed openness to learning new tools or methods designed to streamline the process (n=8), particularly if these approaches reduced time burden and demonstrated clear value.
However, some participants emphasized that time and financial constraints may limit adoption of new tools (n=4). Participants frequently highlighted the importance of developing simple and efficient systems to support GAS implementation in clinical settings (n=6).
Integration with electronic medical records was widely viewed as essential for improving accessibility, facilitating longitudinal tracking, and reducing duplication of documentation (n=5). Participants also suggested incorporating guided goal-setting prompts (n=4) or goal inventories (n=2) to improve the efficiency of the tool and support interviewer training.
Theme 6: Effect of COVID-19
Participants reported that the COVID-19 pandemic accelerated the adoption of virtual platforms for GAS interviews and assessments. Many described increased openness to technology (n=9), noting that remote consultations improved accessibility for geographically dispersed patients and reduced clinician travel time. GAS was also perceived as adaptable when external restrictions limited certain activities, allowing goals to focus on achievable outcomes within changing circumstances.
However, participants also described challenges associated with remote implementation. Some goals required modification due to restrictions such as gym closures or reduced social activities. Participants also noted pandemic-related stress and reduced cognitive capacity for goal setting, as well as communication difficulties associated with masks, technical barriers for some patients, and reduced ability to observe patients’ environments and nonverbal cues during virtual visits.
Discussion
This qualitative study explored clinicians’ and researchers’ perspectives on the use of GAS in both clinical and research contexts and identified six major themes highlighting its perceived flexibility, patient-centeredness, and ability to capture meaningful outcomes. Participants also identified challenges, including time constraints, variability in implementation, and barriers to clinician adoption, as well as strategies to enhance feasibility. To our knowledge, this is the first qualitative study to examine GAS from the perspectives of clinicians and researchers, complementing prior work that has primarily focused on patient experiences.11,12
Participants emphasized the sensitivity of GAS to detect meaningful change and its ability to capture outcomes that are salient to patients, particularly in heterogeneous populations where standardized measures may be less responsive. This aligns with prior evidence demonstrating that GAS can identify clinically important changes that may not be captured by conventional outcome measures.6,15–17 Systematic reviews across randomized controlled trials and rehabilitation contexts further indicate that GAS is often more responsive than standardized functional measures and uniquely positioned to capture individualized, patient-centered gains that may not be reflected in other global assessments.8,9,18,19 This finding is particularly important in light of well-documented limitations of existing clinical outcome assessments (COAs), which often prioritize standardization and comparability at the expense of individual relevance and sensitivity to change.20,21
Our results indicated that there is a wide variation in how GAS is applied, reinforcing existing literature.8,9 Differences were seen in adaptations to the original Kiresuk & Sherman (1968) framework, the use of goal inventories, the role and continuity of the interviewer, as well as the use of technology to collect data.1 This variability reflects a lack of standardized protocols, limiting comparability and consistency in implementation. At the same time, such flexibility is a key strength of GAS, enabling adaptation to diverse populations and contexts. Thus, variability may represent necessary contextualization rather than methodological weakness. However, without clear guidance, this flexibility may compromise reliability, validity, and interpretability. In alignment with previous reports, these findings highlight the need to establish core methodological standards (eg., goal setting procedures, scaling rules, and interviewer training) while preserving sufficient adaptability to individual patients.8,19,22–24
In both clinical and research settings, GAS was also valued for its role in enhancing patient engagement and supporting multidisciplinary care. Participants described how the collaborative goal-setting process fosters active patient involvement, promotes shared decision-making, and helps align treatment priorities across stakeholders. This is particularly relevant in complex conditions, where care often spans multiple disciplines and requires coordination around individualized patient needs. These findings also overlap with prior qualitative research on goal setting, which emphasizes patient empowerment, autonomy, and the co-construction of meaningful outcomes.10,13,25,26 Beyond measurement, GAS may therefore function as both an evaluative tool and an intervention in itself, shaping clinical interactions and reinforcing patient-centeredness.27
Despite these strengths, GAS was consistently perceived as time-consuming, particularly during initial goal-setting sessions, which require in-depth discussion to elicit, refine, and scale individualized goals. This upfront investment was often viewed as a barrier in time-constrained clinical and research environments. Yet, previously reported administration times are broadly comparable to commonly used clinical assessments, suggesting that GAS does not impose a substantially greater time burden than established outcome measures.28 As such, the perceived burden may reflect the cognitive and relational demands of individualized goal setting, as opposed to structured questionnaire completion. In this sense, the time required for GAS may represent a shift in effort toward more patient-centered, meaningful assessment. Overall, these findings suggest that perceived inefficiencies may be mitigated through training, experience, and structured supports such as data capture platforms,29 and that the time investment required for GAS should be considered in light of its added value in capturing meaningful, patient-relevant outcomes. Participants also noted that efficiency improved with interviewer experience, as familiarity with the process enabled more focused and structured conversations. The use of goal inventories to prompt ideas and standardized training to guide goal formulation were also identified as key enablers, helping to streamline administration while maintaining quality. This emphasis is well-aligned with increased use of goal inventories, and the proposed benefits of facilitating goal generation, reducing cognitive burden on patients, and improving the specificity and feasibility of selected goals.28,30–34
Participants expressed divergent perspectives on the need for standardization in GAS implementation. Some emphasized that a lack of standardization raises concerns regarding reliability and comparability across studies, while others cautioned that excessive standardization could undermine the patient-centered nature of GAS. These perspectives reflect an inherent tension between standardization and individualization in GAS implementation. Consequently, aligned with earlier views, GAS may be better understood not as a single, uniform scale, but as a flexible family of related methodologies that share common principles while allowing for contextual adaptation.35 Accordingly, efforts to develop methodological guidance should prioritize defining core principles and minimum standards while preserving flexibility in areas essential to individualized, patient-centered goal setting.
Embedding GAS into routine clinical practice was also seen as challenging, particularly in high-volume primary care settings where its use may not be reimbursable. These challenges echo known barriers to implementing patient-centered outcome measures but also highlight distinctive obstacles for GAS, such as the cognitive and conversational demands of goal-setting.16
Participants also proposed specific strategies for improving the efficiency and uptake of GAS. These included embedding GAS into EMRs with automated scoring, guided goal-setting, training and skill development that include structured interviewer training using observation, mock sessions, as well as flexibly used goal inventories to improve efficiency and goal quality. These align with existing efforts to improve promote awareness on reliable use of GAS and encouraging best pracitices.35,36 In addition to actionable pathways for reducing time burden, and improving reliability have been suggested as ways to support adoption, particularly in environments with constrained resources as well as policy and system-level considerations.
At a policy and system level, the inclusion of GAS within clinical guidelines, reimbursement frameworks, and regulatory trial endpoints was proposed as a means to reinforce its legitimacy and promote more consistent use. In line with these developments, the National Committee for Quality Assurance (NCQA) has recently incorporated GAS into its emerging framework for person-centered outcome measures, marking a shift toward more structured yet individualized approaches to quality measurement in health care.37 Similarly, in its draft guidance on patient-focused drug development, the FDA has highlighted key advantages of GAS, including its patient-centeredness, responsiveness, and individual relevance, while also emphasizing the need for greater standardization in its implementation.38 Taken together, these findings underscore that advancing the routine use of GAS will require deliberate alignment across methodological guidance, clinical practice infrastructure, and policy frameworks to balance standardization with flexibility and enable patient-centered implementation of GAS.
Several limitations should be acknowledged. First, the study employed purposive sampling to capture a heterogeneous range of perspectives across roles, regions, and experience levels, rather than aiming for thematic saturation. As a result, the findings reflect the views of this diverse but not necessarily exhaustive group of clinicians and researchers and may not capture all possible experiences with GAS. Second, reliance on professional networks to identify participants, combined with the fact that only those who responded and consented were interviewed, introduces potential selection bias, favoring individuals with established expertise, familiarity, or interest in GAS. Finally, because the sample was relatively small and drawn from select countries, the generalizability of findings to other settings, populations, or healthcare systems may be limited. Future research should examine GAS in more diverse populations and settings, including users with varying levels of experience, and focus on developing standardized guidance, training, and tools to support consistent implementation and broader adoption in clinical practice and research. In addition, future studies should systematically identify and address implementation barriers and facilitators using established implementation science frameworks to better understand contextual factors influencing the uptake and sustainability of GAS.
Conclusion
GAS is valued for its flexibility, patient-centeredness, and ability to capture meaningful outcomes, yet time demands, workflow challenges, and variability in application limit its uptake. Emerging solutions including EMR integration, guided goal-setting features, and structured training, offer promising strategies to enhance efficiency and adoption while preserving the individualized strengths of the method.
Abbreviations
GAS, Goal Attainment Scaling; PROMS, Patient-reported outcome measures; SMART, Specific, Measurable, Attainable, Realistic, and Time-bound; EMR, electronic medical record.
Acknowledgments
The authors thank all participants for their time and contributions to this study and acknowledge the clinicians and research staff who supported participant recruitment and data collection. The authors used ChatGPT (GPT-5, OpenAI) to assist with language refinement, clarity, and adherence to journal formatting guidelines. The authors are solely responsible for the manuscript’s content.
Funding
This research was supported by the National Research Council of Canada Industrial Research Assistance Program (NRC IRAP). Although the funder was not involved directly in this research, our company receives funds for other projects from pharma, non-profits, other contract research organizations, and grants from academic and government groups. The authors affirm that the funder had no influence on the design, conduct, analysis, or reporting of this study.
Disclosure
Two of the authors (CAC, KR) are co-owners of Ardea Outcomes, which received support through NRC IRAP. Additional authors (GS, AER, KC, SN) are employees of Ardea Outcomes. These affiliations are disclosed in the interest of transparency. In addition, CAC has a patent “GoalNav GAS eCOA” pending and reports the copyright material “GAS Rater Training and Certification Program” service to learn about GAS. Later in this project, the authors tested their products and services with some clinicians in a local environment. The authors report no other conflicts of interest in this work.
References
1. Kiresuk TJ, Sherman RE. Goal attainment scaling: a general method for evaluating comprehensive community mental health programs. Commun Mental Health J. 1968;4(6):443–453. doi:10.1007/BF01530764
2. Kiresuk TJ, Smith A, Cardillo JE. Goal Attainment Scaling: Applications, Theory, and Measurement. Psychology Press; 2014.
3. Weldring T, Smith SMS. Article commentary: patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs). Health Services Insights. 2013;6:
4. Field J, Holmes MM, Newell D. PROMs data: can it be used to make decisions for individual patients? A narrative review. Patient Relat Outcome Meas. 2019;10:233–241. doi:10.2147/PROM.S156291
5. Mercieca-Bebber R, King MT, Calvert MJ, Stockler MR, Friedlander M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat Outcome Meas. 2018;9:353–367. doi:10.2147/PROM.S156279
6. Rockwood K, Stolee P, Fox RA. Use of goal attainment scaling in measuring clinically important change in the frail elderly. J Clin Epidemiol. 1993;46(10):1113–1118. doi:10.1016/0895-4356(93)90110-M
7. Rockwood K, Stolee P, Howard K, Mallery L. Use of goal attainment scaling to measure treatment effects in an anti-dementia drug trial. Neuroepidemiology. 1996;15:330–338. doi:10.1159/000109923
8. Logan B, Jegatheesan D, Viecelli A, Pascoe E, Hubbard R. Goal attainment scaling as an outcome measure for randomised controlled trials: a scoping review. BMJ Open. 2022;12(7):e063061. doi:10.1136/bmjopen-2022-063061
9. Cheema K, Dunn T, Chapman C, Rockwood K, Howlett SE, Sevinc G. Asystematic review of goal attainment scaling implementation practices by caregivers in randomized controlled trials. J Patient Rep Outcomes. 2024;8(1):37. doi:10.1186/s41687-024-00716-w
10. Clair CA, Sandberg SF, Scholle SH, Willits J, Jennings LA, Giovannetti ER. Patient and provider perspectives on using goal attainment scaling in care planning for older adults with complex needs. J Patient Rep Outcomes. 2022;6(1):37. doi:10.1186/s41687-022-00445-y
11. McNaughton EC, Curran C, Granskie J, et al. Patient attitudes toward and goals for MDD treatment: a survey study. Patient Prefer Adhere. 2019;13:959–967. doi:10.2147/PPA.S204198
12. Cairns A, Kavanagh D, Dark F, McPhail SM. Setting measurable goals with young people: qualitative feedback from the goal attainment scale in youth mental health. Br J Occup Ther. 2015;78(4):253–259. doi:10.1177/0308022614562584
13. Sevinc G, Nesto S, Chapman C, Rockwood K, Howlett S. P16 standardized implementation of a personalized endpoint: inventory-facilitated goal attainment scaling. Value Health. 2024;27(12):S4. doi:10.1016/j.jval.2024.10.020
14. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117. doi:10.1186/1471-2288-13-117
15. Rockwood K, Howlett S, Stadnyk K, Carver D, Powell C, Stolee P. Responsiveness of goal attainment scaling in a randomized controlled trial of comprehensive geriatric assessment. J Clin Epidemiol. 2003;56(8):736–743. doi:10.1016/S0895-4356(03)00132-X
16. Gordon J. Goal attainment scaling as a measure of clinically important change in nursing-home patients. Age Ageing. 1999;28(3):275–281. doi:10.1093/ageing/28.3.275
17. Fegter O, Santos H, Rademaker AW, Roberts AC, Rogalski E. Suitability of goal attainment scaling in older adult populations with neurodegenerative disease experiencing cognitive impairment: a systematic review and meta-analysis. Gerontology. 2023;69(8):1002–1013. doi:10.1159/000529984
18. Gaasterland CMW, Jansen-van der Weide MC, Weinreich SS, van der Lee JH. A systematic review to investigate the measurement properties of goal attainment scaling, towards use in drug trials. BMC Med Res Method. 2016;16(1):99. doi:10.1186/s12874-016-0205-4
19. Harpster K, Sheehan A, Foster EA, Leffler E, Schwab SM, Angeli JM. The methodological application of goal attainment scaling in pediatric rehabilitation research: a systematic review. Disability Rehabil. 2019;41(24):2855–2864. doi:10.1080/09638288.2018.1474952
20. Gnanasakthy A, DeMuro CR. The limitations of EQ-5D as a clinical outcome assessment tool. Patient-Centered Outcomes Res. 2024;17(3):215–217. doi:10.1007/s40271-024-00683-w
21. Heneghan C, Goldacre B, Mahtani KR. Why clinical trial outcomes fail to translate into benefits for patients. Trials. 2017;18(1):122. doi:10.1186/s13063-017-1870-2
22. Gaasterland CMW, van der Weide MCJ, Roes KCB, van der Lee JH. Goal attainment scaling as an outcome measure in rare disease trials: a conceptual proposal for validation. BMC Med Res Method. 2019;19(1):227. doi:10.1186/s12874-019-0866-x
23. Krasny-Pacini A, Evans J, Sohlberg MM, Chevignard M. Proposed criteria for appraising goal attainment scales used as outcome measures in rehabilitation research. Arch Phys Med Rehabil. 2016;97(1):157–170. doi:10.1016/j.apmr.2015.08.424
24. Steenbeek D, Ketelaar M, Galama K, Gorter JW. Goal attainment scaling in paediatric rehabilitation: a report on the clinical training of an interdisciplinary team. Child Care Health Dev. 2008;34(4):521–529. doi:10.1111/j.1365-2214.2008.00841.x
25. Stolee P, Zaza C, Pedlar A, Myers AM. Clinical experience with goal attainment scaling in geriatric care. J Aging and Health. 1999;11(1):96–124. doi:10.1177/089826439901100106
26. van Blijswijk SC, Gussekloo J, Heijmans FM, Wind AW, den Elzen WP, Blom JW. Goal attainment scaling with older people in general practice: a feasibility study. Int J Nurs Stud Adv. 2021;3:100015. doi:10.1016/j.ijnsa.2020.100015
27. Cooper C, Vickerstaff V, Barber J, et al. A psychosocial goal-setting and manualised support intervention for Independence in dementia (NIDUS-Family) versus goal setting and routine care: a single-masked, Phase 3, superiority, randomised controlled trial. Lancet Healthy Longevity. 2024;5(2):e141–e151. doi:10.1016/S2666-7568(23)00262-3
28. Sevinc G, Knox K, George M, et al. The feasibility of personalized endpoints in assessing treatment outcomes for rare diseases: a pilot study of goal attainment scaling in SCN2A-associated developmental epileptic encephalopathy. Value Health. 2025;28(3):441–448. doi:10.1016/j.jval.2024.12.004
29. Sevinc G, Shehzad A, Nesto S, et al. PCR67 assessing the feasibility of using an electronic platform for personalized outcome assessment: goalnav for goal attainment scaling. Value Health. 2025;28(6):S322. doi:10.1016/j.jval.2025.04.1388
30. Roberts JC, Richardson S, Miles ME, et al. The GOAL-Hēm journey: shared decision making and patient-centred outcomes. Haemophilia. 2022;28(5):784–795. doi:10.1111/hae.14608
31. Goldstine J, Knox K, Beekman J, et al. A patient-centric tool to facilitate goal attainment scaling in neurogenic bladder and bowel dysfunction: path to individualization. Value Health. 2021;24(3):413–420. doi:10.1016/j.jval.2020.10.023
32. Knox K, Stanley J, Hendrix JA, et al. Development of a symptom menu to facilitate goal attainment scaling in adults with down syndrome-associated Alzheimer’s disease: a qualitative study to identify meaningful symptoms. J Patient Reported Outcomes. 2021;5(1). doi:10.1186/s41687-020-00278-7
33. Knox K, Stanley J, Hendrix JA, et al. Understanding meaningful symptoms and challenges in people with Down syndrome and dementia: a qualitative study of caregivers’ perspectives. Alzheimer’s Dementia. 2020;16(S9):e043046. doi:10.1002/alz.043046
34. Staunton H, McIver T, Tillmann J, et al. Development of a goal attainment scale (GAS) outcome measure for clinical interventional studies in paediatric autism. Autism. 2025;29(12):2975–2990. doi:10.1177/13623613251349904
35. Bard-Pondarré R, Villepinte C, Roumenoff F, et al. Goal attainment scaling in rehabilitation: an educational review providing a comprehensive didactical tool box for implementing goal attainment scaling. J Rehabil Med. 2023;55:6498. doi:10.2340/jrm.v55.6498
36. Turner-Stokes L. Goal attainment scaling (GAS) in rehabilitation: a practical guide. Clin Rehabilitat. 2009;23(4):362–370. doi:10.1177/0269215508101742
37. Person-centered outcome measures. NCQA. Available from: https://www.ncqa.org/hedis/reports-and-research/pco-measures/.
38. FDA patient-focused drug development guidance series for enhancing the incorporation of the patient’s voice in medical product development and regulatory decision making. 2025. Available from: https://www.fda.gov/drugs/development-approval-process-drugs/fda-patient-focused-drug-development-guidance-series-enhancing-incorporation-patients-voice-medical.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Requirements for Brazilian Outpatient Centers of Excellence in Hidradenitis Suppurativa: Consensus Co-Creative Study
Bellei EA, Shirozaki MEM, Puglia ALP, Esteves de Carvalho AV, Riquena B, Vallilo CC, de Barros D, Tamashiro EY, Cintra G, Duarte GV, da Matta Rivitti-Machado MC, Magalhães RF, do Nascimento RF, Tunala R, da Silva R, Cesar WGG, Thies FG
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2029-2044
Published Date: 4 August 2023