")
Back to Journals » Advances in Medical Education and Practice » Volume 10
Clinical vignette-based interactive discussion sessions: feedback from residents
Authors Piryani RM , Piryani S
Received 3 June 2019
Accepted for publication 29 August 2019
Published 24 September 2019 Volume 2019:10 Pages 829—833
DOI https://doi.org/10.2147/AMEP.S218157
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Rano Mal Piryani,1 Suneel Piryani2
1Health Professions Training Committee, Universal College of Medical Sciences, Bhairahawa, Nepal; 2Department of Community Health Sciences, Aga Khan University, Karachi, Pakistan
Correspondence: Rano Mal Piryani
Health Professions Training Committee, Universal College of Medical Sciences, Siddharthanagar, Bhairahawa 32900, Nepal
Tel +977 984 126 9522
Email [email protected]
Introduction: A clinical vignette is a useful tool for teaching both clinical and basic sciences courses. The clinical vignette-based interactive discussion sessions were conducted for residents in the internal medicine department of Universal College of Medical Sciences( Bhairahawa, Nepal) with aim to link the residents to clinical practice setting. The objective of this study was to assess the feedback of participant.
Methods: The sessions were done five days a week between January 16 and February 26, 2019. Each session was between 45 and 60 minutes. The clinical vignettes related to internal medicine were downloaded using Google. Each vignette was divided into sections, related questions with responses were developed and the discussion was updated referring to the latest articles on subject. Eleven residents participated in the session. At the end of last session feedback was taken on a validated semi-structured questionnaire. The data was analyzed using SPSS version 21.
Results: Residents rated the clinical vignette-based interactive discussion sessions on the scale 1 = poor to 10= excellent; usefulness (9.45±1.04), content (9.27±0.90), relevance of session (9.18±1.08), facilitation (9.27±1.10), and overall (9.36±0.81). Participants rated the structure of vignettes discussed (3.73±0.47), the questions related to vignettes discussed (3.82±0.40), and discussion related to vignettes done (3.64±0.50) on a Likert scale 1–4 (4= extremely important, 3= moderately important, 2= slightly important, 1= not important). The two-way interaction, the approach toward differential diagnosis, diagnosis and management, choosing appropriate investigation, clinical relevancy of vignettes, boosts understanding, enhances thinking power and thinking outside the box, improving clinical approach and academic learning were among the strengths of sessions shared by residents. All residents proposed to continue these sessions and develop vignettes of our patients. The majority of the residents recommended conducting session on alternate days.
Conclusion: This method of learning allowing the residents to follow and construct clinical outcome in a logical and systematic sequence that may be applicable in real-life clinical practice settings. This method enhances the thinking power of residents and their problem-solving capacity.
Keywords: clinical practice setting, clinical vignette, feedback, learning teaching method, internal medicine, residents
Introduction
Carolyn Jeffries and Dale W Maeder define vignettes as incomplete short stories that are written to reflect, in a less complex way, real-life situations in order to encourage discussions and potential solutions to problems where multiple solutions are possible.1
A clinical vignette is an abridged report of a patient summarizing any relevant history, physical examination findings, investigations data and treatment.2 This is one of the formats used for teaching problem-solving skills, assessing judgment and decision-making processes, including clinical judgments made by healthcare professionals, as well as assessing professionalism.3–5 The clinical vignette is one of the very useful tools for teaching clinical, as well as basic science subjects, as it provides comprehensive stages where possible etiology, individual patients’ characteristics, symptoms and signs, family history, important investigations and relevant information are revealed and explained.2
Clinical vignettes are patient-related cases and scenarios that have educational value for a wider audience. To link the residents to clinical practice settings and situations, the clinical vignette-based interactive discussion sessions were conducted for the residents in the internal medicine department of Universal College of Medical Sciences (UCMS; Bhairahawa, Nepal). The objective of this study was to take feedback from the participant residents and assess it.
Methodology
To link the residents to clinical practice settings and situations, the clinical vignette-based interactive discussion sessions were conducted for the residents in the internal medicine department of UCMS for post-graduation (MD). These sessions were done for six weeks, five days a week from January 16 to February 26, 2019. Each session was between 45 and 60 minutes, starting at 9.00 am. The sessions were conducted by the principal author.
The vignettes related to internal medicine were downloaded from various sources using Google by the principal author. Each vignette was divided into sections such as history, physical examination, investigations, treatment; related questions and responses were developed and the discussion was updated referring to the latest article on the subject. An example of a clinical vignette is given in Figure 1. There are concerns that the learner would usually take a superficial view of vignette activity and work, deduce and interpret vignettes at lower order of thinking or intellectual levels, i.e., remembering and understanding based on the revised Blooms’ Taxonomy of Learning.6,7
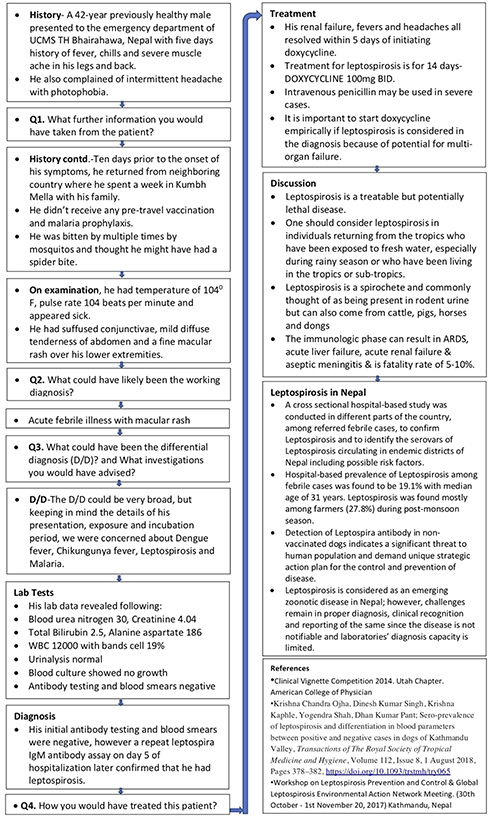 |
Figure 1 Example of a clinical vignette. |
The principal author intended to stimulate the residents at a higher-level of thinking, i.e., applying, analyzing and evaluating (Figure 2).
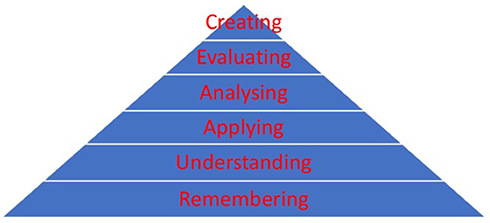 |
Figure 2 Revised Blooms’ Taxonomy of Learning. |
At the end of last session, feedback of the residents was taken on validated semi-structured questionnaire.8 The questionnaire contained four closed ended and three open ended questions. The closed ended questions were: 1) rate the interactive session on the scale 1 = poor to 10 = excellent, for usefulness, content, relevance of session and content, facilitation and overall; 2) rate the structure of clinical vignette discussed on a Likert scale 1–4; 3) rate the questions related to clinical vignettes discussed on a Likert scale 1–4; and 4) rate the discussion related to clinical vignettes done on a Likert scale 1 = not important, 2 = slightly important, 3 = moderately important, 4 = extremely important. The questionnaire is annexed.
Eleven residents participated in these sessions; nine were from internal medicine (three each of first, second, and third year), one each from the emergency department and dermatology, who were posted in the department for their rotational training. Informed consent was taken from the participant residents and Institutional Review Committee of UCMS approved the study vide Letter No: UCMS/IRC/053/19, dated March 20, 2019.
The data collected was checked for completeness, accuracy and consistency. The data was entered into IBMS SPSS version 21 for analysis. The descriptive statistics was calculated for the mean and standard deviation.
Results
The residents rated the interactive clinical vignette-based discussion sessions on a scale of 1 = poor to 10 = excellent; the rating was notable (Table 1).
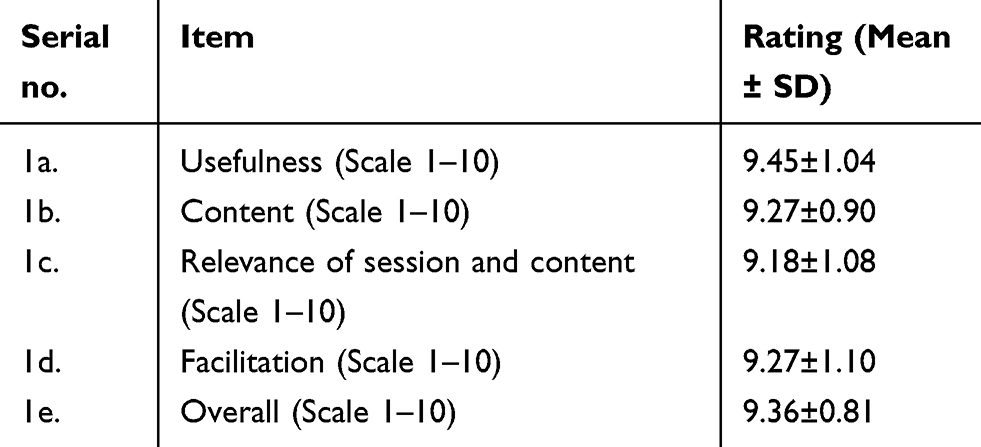 |
Table 1 Rating of residents on the clinical vignette-based discussion sessions |
The residents rated the structure of clinical vignettes discussed in all sessions, the questions related to clinical vignettes discussed and discussion related to clinical vignette done on a Likert scale 1 = not important to 4 = extremely important, the rating was remarkable (Table 2).
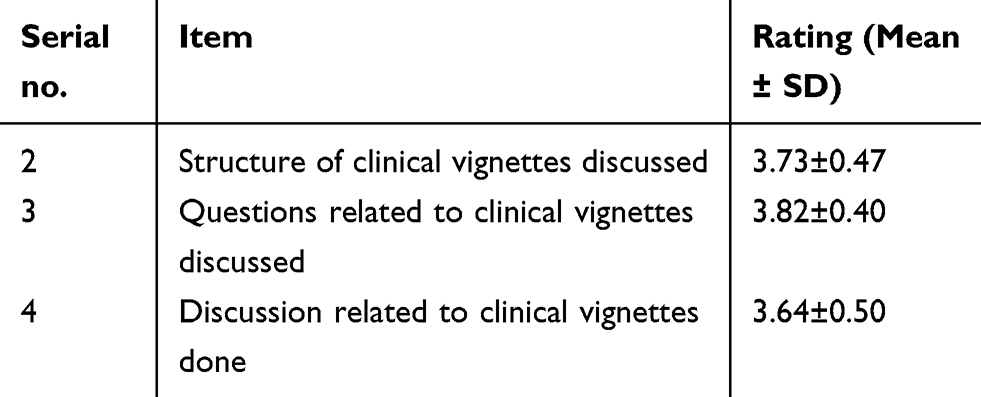 |
Table 2 Rating of residents on the clinical vignette structure, questions and discussion |
Strengths of the interactive clinical vignette-based discussion sessions
The strengths of the interactive clinical vignette-based discussion sessions shared by the residents were two-way interaction, making differential diagnosis, approaches toward diagnosis, differential diagnosis, and management, choosing appropriate or accurate investigation, awareness of different scenarios encountered in daily life, discussion among peers, strengthening knowledge and understanding, clinical relevancy and its application in day to day life, gives clues toward exam questions, vignettes based on common diseases prevalent in our society, brain-storming exercise, enhances thinking power and thinking outside the box, enhances problem-solving capacity, as well as understanding better how to improve clinical approach and academic learning.
Areas for improvement
The majority of the residents recommended that these sessions were conducted on alternate days. Some suggested having a clinical examination session (bedside) the next day, with more interaction and discussion, explanation of differential diagnosis in detail, and more sessions on specific management and protocols of common diseases.
Additional comments
All residents proposed to continue these sessions and also to develop vignettes of patients admitted to our ward, to discuss patients on the ward and treatment specific to them.
Discussion
The clinical vignette-based interactive discussion sessions were conducted for the residents in the internal medicine department of UCMS (Bhairahawa, Nepal) to link and connect the residents to clinical practice settings and situations and to incite and excite them at a higher-level of thinking as per the revised Blooms’ Taxonomy of Learning.6,7
The magnificence of the vignette activity is that when the residents learn, they must be able to transfer this knowledge to other situations and in doing so, incorporate and integrate their knowledge and skills well enough to make predictions and likelihoods about new situations and utilize their knowledge and skills for solving the problem.1
Most of the studies on case vignettes mention the use of hypothetical case studies (patient scenario) designed to achieve a specific learning objective.9 But we selected real cases from recent studies published in last five years and the discussion was focused on the differential diagnosis, investigation and comprehensive management.
Feedback from the learners helps to assess innovative teaching–learning methods, and feedback serves as guide for improvement when conducting the same sessions or training in the future. With this aim, feedback of the residents was taken on the clinical vignette-based interactive discussion sessions and assessed.
The participant resident rated the clinical vignette-based interactive discussion sessions on a scale of 1 = poor to 10 = excellent, for usefulness (9.45±1.04), content (9.27±0.90), relevance of session and content (9.18±1.08), facilitation (9.27±1.10) and overall (9.36±0.81); the rating is notable.
The residents rated the structure of clinical vignettes discussed in all sessions (3.73±0.47), the questions related to clinical vignettes discussed (3.82±0.40) and discussion related to clinical vignette done (3.64±0.50) on a Likert scale 1–4; the rating was remarkable.
The two-way interaction; approaches toward differential diagnosis, diagnosis and management, choosing appropriate investigation, clinical relevancy of vignette and its application in day to day life, strengthening knowledge and understanding, discussion among peers, vignettes based on common diseases in our society, brain-storming exercises, enhanceing thinking power and thinking outside the box, as well as how to improve clinical approach and academic learning, were among the strengths of sessions shared by the residents. All residents proposed to continue these sessions and also to develop vignettes of patients admitted to the ward, to discuss patients on the ward and treatment specific to them. The majority of the residents recommended conducting these sessions on alternate days. Some suggested having clinical examination sessions (bedside) the next day, with more interaction and discussion, explanation of differential diagnosis in detail, and more sessions on the specific management and protocols of common diseases.
Kathiresan J, Patro BK (2013) stated that the vignette-based discussion method enables the residents to apply their clinical reasoning skills in real-life contexts and this method motivates them towards self-directed learning and sharing of knowledge. Furthermore, the case vignettes are a promising complement to the existing methods of teaching.10
The clinical vignette-based interactive discussion sessions transform the approach of residents toward patients and their problem-solving and decision-making skills, thereby improving quality of care.
The limitations of the study were the small sample size, conducted in one department of one institution, so the findings cannot be generalized. The study assessed only reaction and perception of the participant residents.
Conclusion
Residents feedback about clinical vignette-based interactive discussion sessions reveals that this method of learning allows them to follow and construct clinical outcomes in a logical, rationale, reasonable, analytical and well-organized sequence, that may be applicable in real-life clinical practice settings and situations. This method enhances their thinking power, thinking outside the box and their problem-solving capacity.
Acknowledgment
We highly appreciate for the residents who participated in training as well as in study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jeffries C, Maeder DW. Using vignettes to build and assess teacher understanding of instructional strategies. Professional Educator. 2005;27(1 & 2):17–28.
2. Cui D, Lynch JC, Daley WP, Yang G, Haines DE. The clinical vignette as a teaching tool for histology and anatomic pathology. FASEB J. 2011;25(1):
3. Nendaz MR, Raetzo MR, Junod AF, Vu NV. Teaching diagnostic skills: clinical vignette or chief complaints? Adv Health Sci Educ. 2000;5:3–10.
4. Evans SC, Roberts MC, Keeley JW, et al. Vignette methodologies for studying clinicians’ decision-making: validity, utility, and application in ICD-11 field studies. Int J Clin Health Psychol. 2015;15:160–170.
5. Khan R, Lee AG, Golink KC, Paranilam J. Residency education professionalism Vignette. Ophthalmology. 2013;120(4):874–875.
6. Emanuel V. using vignettes to teach stroke care. Nurs Times. 2012;108(9):20–22.
7. Krathwohl DR. A revision of Bloom’s Taxonomy: an overview. Theory Pract. 2002;41(4):212–218.
8. Piryani RM. Training workshop on developing Objective Structured Clinical Examination (OSCE) conducted at nursing campus in Nepal: feedback of the nursing faculty participants. Janaki Med Coll J Med Sci. 2018;6(1):49–54. doi:10.3126/jmcjms.v6i1.20576
9. Parekh M, Munjappa H, Shinde S, Vaidya S. Student perceptions on activity-based learning in physiology. Natl J Physiol Pharm Pharmacol. 2018;8(4):590–593.
10. Kathiresan J, Patro BK. Case vignette: a promising complement to clinical case presentations in teaching. Educ Health. 2013;26:21–24.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.