")
Back to Journals » Journal of Pain Research » Volume 15
Clinical Study on the Combination of Transcutaneous Electrical Acupoint Stimulation and Lidocaine for Preventing Propofol Injection Pain
Authors Jin D , Pan Y , Jin W, Yan Y, Huang L , Wang J
Received 28 December 2021
Accepted for publication 2 March 2022
Published 15 March 2022 Volume 2022:15 Pages 745—755
DOI https://doi.org/10.2147/JPR.S356150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Dan Jin,* Yuanyuan pan,* Wenjun Jin, Yixiu Yan, Luping Huang, Junlu Wang
Department of Anesthesiology, The First Affiliated Hospital of Wenzhou Medical University, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junlu Wang, Departments of Anesthesiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China, Tel +86 13806689854, Fax +86 577-55578999-689854, Email [email protected]
Purpose: Propofol is a widely used intravenous anesthetic in clinical practice. Lidocaine pretreatment is currently the most commonly used method to reduce the pain of propofol injection. However, propofol injection pain has not been eliminated and its incidence remains high. Transcutaneous electrical acupoint stimulation is a green therapy that combines transcutaneous electrical nerve stimulation therapy with the traditional acupuncture therapy of our motherland. This study investigated the effectiveness of transcutaneous electrical acupoint stimulation (TEAS) combined with lidocaine in preventing propofol injection pain and determined whether it can reduce postoperative complications and promote rapid postoperative recovery of patients.
Patients and Methods: A total of 220 women scheduled to undergo hysteroscopic surgery were enrolled in the study. The included patients were randomly divided into four groups of 55 patients each: normal saline group (group K), lidocaine group (group L), TEAS group (group T), and lidocaine + TEAS group (group L + T). Patients in group K received 2 mL saline (0.9% NaCl) pre-injection before anesthesia induction. Group L received 40 mg lidocaine pre-injection (2 mL of 2% lidocaine) before anesthesia induction. Group T received 30 min of transcutaneous electrical stimulation at bilateral election Hegu, Neiguan, and 2 mL saline pre-injections before anesthesia induction. Group L + T received TEAS and lidocaine pre-injection.
Results: The VAS scores and the four-point verbal rating scale of propofol injection were significantly different among the four groups. The prevalence of nausea, vomiting, abdominal pain, and abdominal distension after surgery among the four groups were statistically different. The bleeding days after surgery were significantly different among the four groups.
Conclusion: TEAS combined with lidocaine pre-injection reduced the incidence of propofol injection pain and significantly reduced patients’ pain levels compared with single lidocaine pre-injection. TEAS can also reduce the incidence of postoperative nausea and vomiting, abdominal pain, and abdominal distension, shorten postoperative bleeding days, and accelerate the postoperative recovery of patients.
Keywords: transcutaneous electrical acupoint stimulation, propofol, lidocaine, injection pain
Introduction
Propofol is widely used intravenous anesthetics in clinical practice. Nevertheless, pain caused by propofol injection is unbearable for several patients. Propofol Injection Pain Ranked 7th in the most disturbing patient anesthetic experience.1 Furthermore, among the 33 common anesthesia problems associated with outpatient surgeries, the frequency of pain caused by propofol injection was ranked third,2 with an incidence as high as 90%.3 During the induction of general anesthesia and sedation, some patients appear to be shouting, shrinking, and preventing arm action. Simultaneously, it can stimulate the body’s stress response, and the stress response can affect anesthesia induction and produce harm to patients, which is not consistent with the medical goals for anesthesia. The mechanism underlying injection pain associated with propofol has not been established. A study has suggested that it may be related to its composition; the water phase state and that the endothelium interact and stimulate the slow release of peptides, which induces the feel pain.4 Several preliminary studies have investigated approaches to preventing or relieving propofol injection-related pain; these methods include non-drug approaches such as slowing injection speed,5 choosing a thicker vein,6 cooling the propofol,7 dilution,8,9 as well as drug interventions, such as the use of lidocaine,10 opioids,11 and nonsteroidal anti-inflammatory drugs.12,13 Lidocaine pretreatment is the most widely used method for reducing propofol injection pain clinically.3 However, lidocaine has side effects, such as allergy, contraindications, and safety risks related to blood coagulation function, which is a concern for the medical staff. To concurrently reduce the incidence of propofol injection pain and the side effects of lidocaine, we conceived combination therapy.14 Transcutaneous electrical acupoint stimulation (TEAS) is a new therapy that combines Transcutaneous Electrical Nerve Stimulation (TENS) with traditional acupuncture therapy, which applies a specific density wave current to stimulate the human body.15 This yields an effect similar to that of acupuncture and moxibustion, with subsequent analgesic effects.16,17 Several clinical studies have shown that the analgesic effect of TEAS can be effective continuously, and it is not easy to lose the effect, and it has the advantages of being simple to administer, safe, and noninvasive.18–20 It can also shorten the perioperative period in patients with inflammatory reactions, modulate immunity, and promote oxygenation, and it has been widely used in clinical research.21,22
Our previous studies confirmed that TEAS can alleviate propofol injection pain.16 This study investigated the effects of TEAS combined with lidocaine on propofol injection pain. The purpose of this trial is to reduce the incidence of propofol injection pain and the severity of injection pain, observe its analgesic effect and whether it can reduce postoperative complications such as abdominal pain, bloating, nausea and vomiting, and promote faster and better postoperative patients. The rehabilitation of patients can provide a research basis for promoting the application of TEAS in the perioperative period of patients.
Materials and Methods
Study Design and Participant Recruitment
In this double-blind randomized control-group clinical trial, we studied the effectiveness of TEAS pre-stimulation combined with lidocaine in preventing propofol injection pain. A total of 220 women aged 18–65 years who were scheduled to undergo hysteroscopic surgery were enrolled in the study. All patients had a body mass index ranging from 18 to 31 kg/m2. Their American Anesthesiologists Society (ASA) grades were I or II. Furthermore, all patients provided written informed consent for elective hysteroscopy or surgical treatment. This study was conducted at The First Affiliated Hospital of Wenzhou Medical University, Zhejiang, China, from August 2020 to December 2020. All patients provided informed consent before participation. This prospective observational cohort study was approved by the Ethics Committee (2020–051) of the Clinical Research of the First Affiliated Hospital of Wenzhou Medical University and conducted in accordance with the Declaration of Helsinki. The Clinical Trial Number is ChiCTR2000036066.
Patients with a history of chronic pain syndrome, thrombophlebitis, neurological disease, forearm or thrombophlebitis syndrome with acute and chronic pain, severe mental illness, communication challenges, or digestive tract ulcers and those allergic to lipid medications, propofol, or general anesthetic drugs were excluded from the study. Patients allergic to lipid propofol, medications, and general anesthetic drugs; those with a history of analgesic or sedative drug use; and those who had a surgical incision, surgical scar, or skin infection at the Hegu and Neiguan acupoints, nerve damage in the upper extremities, or a history of spinal surgery were also excluded.
Types of Outcomes
Visual Analog Scale (VAS)
The visual analogue scale (VAS) is used for pain assessment. The basic method is to use a moving ruler with a length of about 10cm. One side is marked with 10 scales. The two ends are respectively “0” and “10” points. A point of 0 means no pain. A score of 10 represents the most severe pain that is unbearable.
Four-Point Verbal Rating Scale
The verbal rating scale (VRS). It consists of a series of adjectives used to describe pain, also known as the Verbal Evaluation Scale. The descriptive words are arranged in order of pain from the lightest to the strongest. There are 4 grades. VRS scores were categorized as follows: 0, no pain; 1, mild pain; 2, moderate pain; and 3, severe pain. If the score is greater than or equal to 2, the patient has obvious limb response. If the patient has no obvious physical reaction, we can ask the patient if he feels pain, and the score is 0 or 1. The method has been widely used to assess propofol injection-related pain.
Dysmenorrhea Severity
The grade is divided into 0–3 degree. 0 means no dysmenorrhea. 1 means that the pain is mild. 2 is moderate pain, the pain is continuous, which affects rest and daily life, and can be relieved with analgesics. 3 is severe pain, the continuous pain cannot be relieved without medicine.
PADSS (Discharge Scoring System After Anesthesia)
The maximum score is 10 point, and patients can leave the hospital if they reach 9 point.
Index: (a) signs: 2, fluctuations in the preoperative level (20%); 1, fluctuations in the preoperative level (20–40%); 0, fluctuations in the preoperative level (40% or more); (b): 2, can determine the orientation and smooth gait; 1, determine the azimuth or smooth gait; 0, cannot achieve more than anyone; (c): 2, mild; 1, moderate; 0, severe; (d), mild; 1, moderate; 0, severe; (e) Surgical bleeding: 2, mild; 1, moderate; 0, severe.
Observation Indexes
The main observation indexes included the highest severity of propofol injection pain and the VAS score for pain (0–3: mild; 4–6: moderate; 7–10: severe) and pain grade (0: absent; 1: mild; 2: moderate; 3: severe) after propofol injection during anesthesia induction. The secondary outcome measures, hemodynamics (heart rate, blood pressure, and pulse saturation), were recorded before anesthesia induction and 1 min after propofol injection. The total doses of propofol and remifentanil, duration of surgery, and duration from withdrawal to recovery were recorded. Respiratory depression (SpO2 less than 90%) and intraoperative body movements were recorded. The discharge scoring system (PADS) score; postoperative bleeding days; and the types and incidence of postoperative complications after anesthesia were also assessed. Pain, edema, inflammation, and anaphylaxis were observed at the injection site and TEAS-treated acupoints and monitored.
Anesthesia, Surgical Procedures, and Analgesia
The patients had to fast and abstain from drinking, not undergo any other preoperative examination, and take other medications, and four groups of patients use the same equipment.
TThe patients from groups T and L+T were administered TEAS 30 mins before anesthesia induction by an anesthesiologist who was not involved in administering anesthesia or pain efficacy evaluation during anesthesia preparation (groups K and L did not undergo any processing). The anesthesiologist selected acupoints of LI4 (Hegu) and PC6 (Neiguan) on both hands of the patients, stuck the electrodes, and connected Han’s Acupoint Nerve Stimulator (Nanjing Jinan Xinsheng Technology, Jinan, Nanjing, China) capable of producing a dilatational wave with a frequency of 2/100 HZ, which is the maximum tolerable for patients receiving −1 mA of electrical stimulation for 30 mins.
A 22-gauge trocar was used to open the hand dorsal veins of the patients when the patient is in the preoperative preparation room. After the infusion channel was connected to the extension tube, 500 mL Ringer’s solution was infused through the channel, with an infusion speed of 20 mL/min. The surgeons were informed about the patients undergoing routine surveillance, including pulse oxygen saturation, noninvasive blood pressure, and electrocardiogram. Meanwhile, the patients were administered oxygen (4 L/min) via a nasal cannula. Anesthesia was induced by another anesthesiologist. The four groups received 5 μg sufentanil (Yichang Renfu, Yichang, Hubei, China) from the infusion channel. Patients from group K and group T received 2 mL of saline, while those from the L and L+T received 2 mL of 2% lidocaine. After 1 minute, all patients were injected with 10% propofol (AstraZeneca, Shanghai, China) (2 mg/kg) at a rate of 1200 mL/hour by using a micropump (Zhejiang University Medical Equipment Factory, Hangzhou, Zhejiang, China). All patients were asked about the pain score every 5 s until they lost their consciousness (the same questions were used for all of them). We record the pain score at each point. The surgery was commenced, and anesthesia was maintained by continuous infusion of propofol (4 mg/kg·h) and remifentanil (Yichang Renfu, Yichang, Hubei, China) (0.1 μg/kg·min) via a micropump.
During the surgery, an additional single intravenous injection of 10% propofol (0.5 mg/kg) was administered if the patient physically responded to the surgical procedures, and the number of additions was recorded. If patiens’ mean arterial pressure (MAP) dropped below 60 mmHg, the patient received intravenous ephedrine (5–10 mg). And when their heart rate (HR) fell below 60 bpm, intravenous atropine (0.5 mg) was administered. Mask pressure oxygen was provided if their oxygen saturation (SPO2) fell below 90% (Figure 1). All drugs were preserved at room temperature and administered within 30 min of preparation.
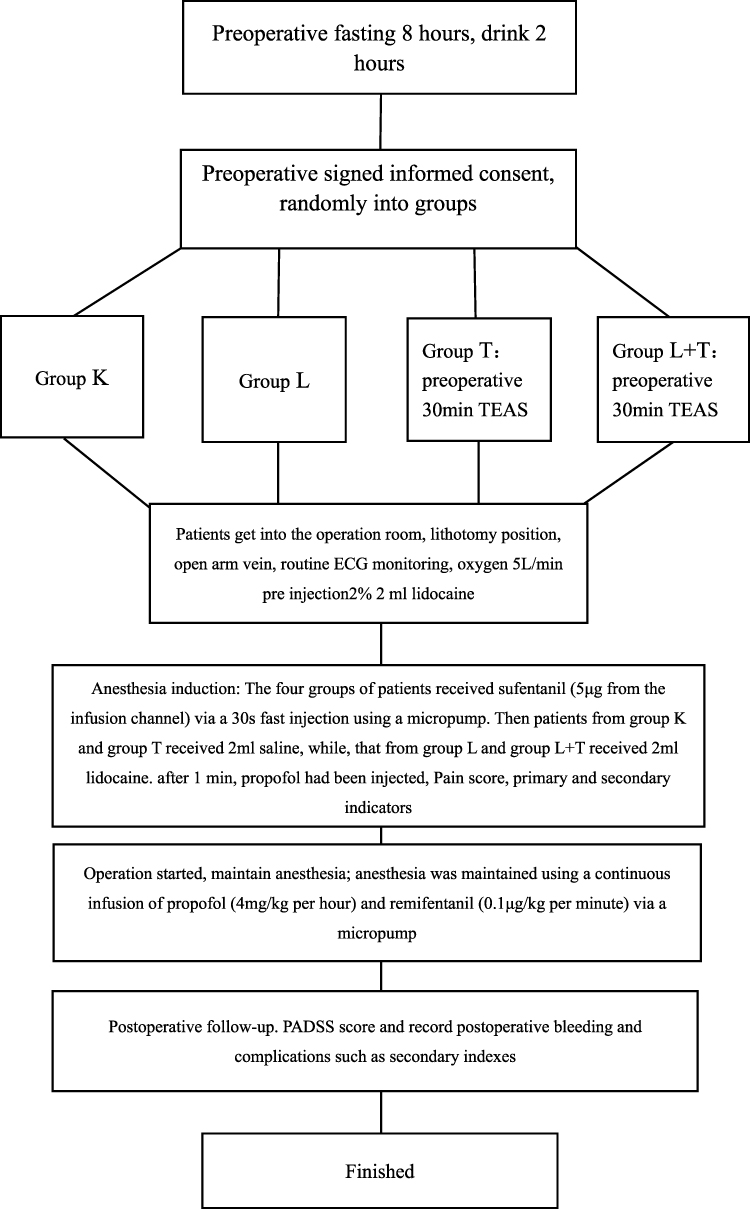 |
Figure 1 Test flowchart. Abbreviations: TEAS, transcutaneous electrical acupoint stimulation; ECG, electrocardiogram; PADSS, discharge scoring system after anesthesia. |
Statistical Analysis
In 42 pilot studies, the incidence of moderate to severe propofol injection-related pain decreased from 95% in the control group to 81% in the saline group (group K). With an α-value of 0.05 and a power of 0.8, the sample size of each group was determined to be 43. Taking into account the possible differences in venous access (hand veins, radial veins and cubital veins) and lack of follow-up, we set the sample size of each group to 55 people.
All data were analyzed using SPSS 25.0 (Statistical Product and Service Solutions, SPSS statistics is a statistical analysis software, which provides the core functions required to perform the whole process analysis). Randomization was performed using the random number method. The measurement data conforming to a normal distribution and homogeneity of variance were expressed as mean ± standard deviation. One-way analysis of variance was used for the intergroup comparisons. The LSD (Least—SignificantDifference) method was used for pairwise comparisons of data with statistically significant differences. Data that were not normally distributed were expressed as median (quartile spacing). The Kruskal–Wallis H-test was used. For the data that were significantly different across the groups, the LSD method was used for pairwise comparison of the rank orders. The statistical data were compared according to the sample size, theoretical frequency, and variable classification number and analyzed using the 2 test (or continuous correction 2 test or Fisher’s exact probability method). The rank data were analyzed using the Kruskal–Wallis H-test, and the ranks were compared using the LSD method. The test results were considered statistically significant at P<0.05.
Results
Of the 220 patients, 40 were excluded, including nine who reported abnormal blood pressure as they arrived in the operating room. These patients had no history of hypertension, but their systolic blood pressure (SBP) in the operating room was > 180 mmHg and did not decrease after 5 min. Moreover, 10 patients were excluded because the vein at the back of the hand could not be opened. The remaining 21 excluded patients refused to participate in follow-up trials after hysteroscopy or surgical treatment (Figure 2).
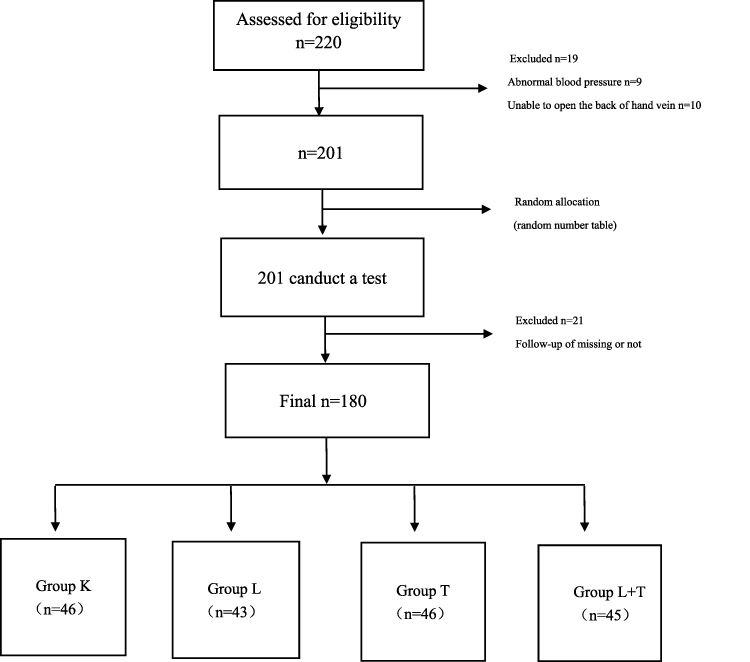 |
Figure 2 Recruitment flowchart numbers of patients recruited, the number of people excluded due to high blood pressure and the number of people missing from follow-up. |
There were no statistically significant differences in the general information, hemodynamics, and basic conditions of anesthesia operation among the four groups (P> 0.05) (Tables 1–3).
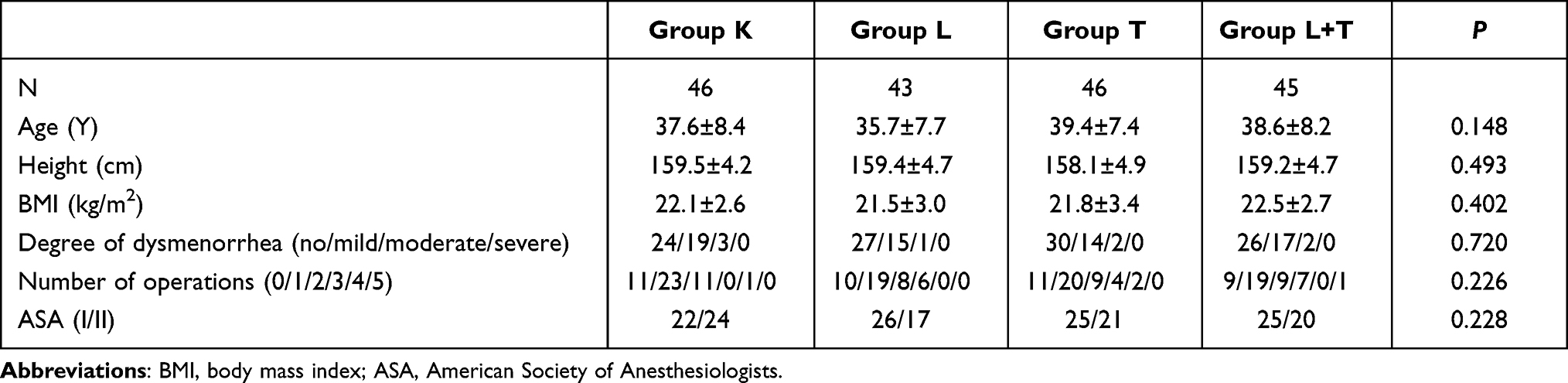 |
Table 1 Four Groups of Patients’ General Information |
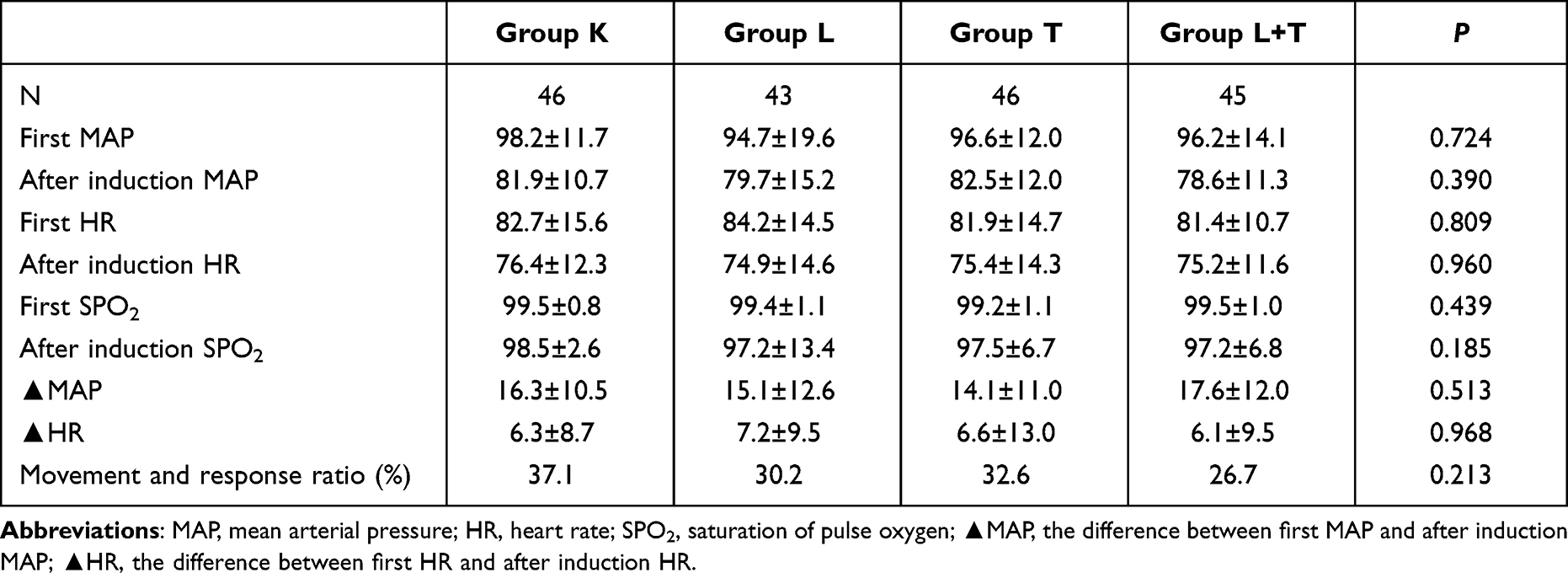 |
Table 2 Four Groups of Patients’ Hemodynamics |
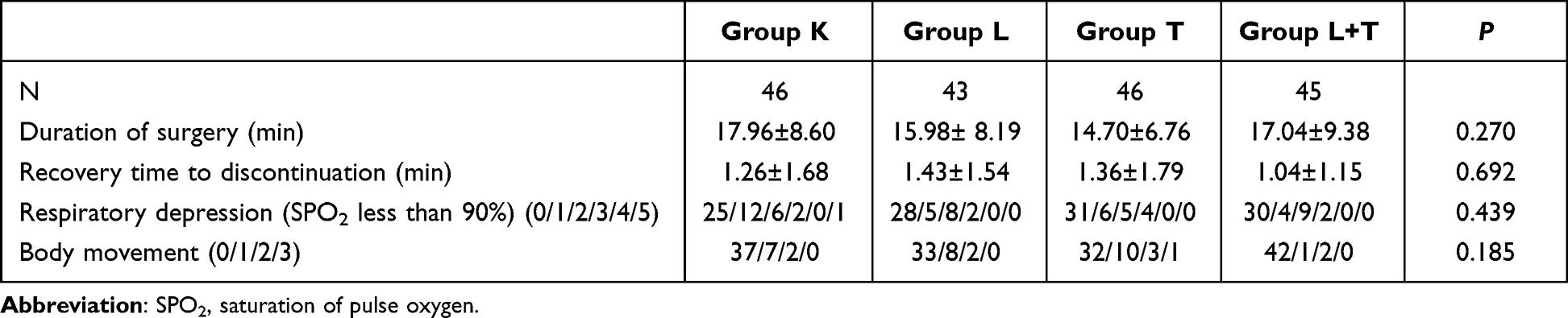 |
Table 3 Four Groups of Patients’ Basic Conditions of Anesthesia Operation |
The four-point verbal rating scale scores for propofol injection pain in the four groups were significantly different (P=0.010). There were statistically significant differences in the incidence of mild, moderate, and severe pain in the groups (P=0.012); the LSD results showed group L+T was significant differences in the incidence of injection pain from group K and group L (P=0.004, P=0.008). There were statistically significant differences in the incidence of mild, moderate, and severe pain among the different groups (P=0.012); the LSD results showed that group L+T was significant differences in the incidence of pain from K and T (P=0.007, P=0.037). The results showed that the combination of TEAS and lidocaine can reduce the incidence of injection pain and is more effective than single-use lidocaine (Table 4).
 |
Table 4 Four Groups of Patients with Different Four-Point Verbal Rating Scale Information |
The VAS scores for propofol injection pain were significantly different among the four groups. There was a statistically significant difference in the pain severity across the groups (p=0.004). The LSD comparison results showed that there were statistically significant differences in pain between groups K and L, groups K and L+T (P=0.019, P=0.000). There were significant differences in the incidence of mild (0–3) or moderate (4–6) pain among the groups (P=0.015). The LSD comparison results showed differences in the incidence between groups K and L+T, groups L and L+T (P=0.003; P=0.011). The comparison showed that the TEAS and lidocaine combination can reduce propofol injection pain and is more effective than single-use lidocaine (Table 5).
 |
Table 5 Four Groups of Patients with Different VAS Information |
The prevalence of nausea, vomiting, abdominal pain, and abdominal distension after surgery among the four groups were statistically different. There were no significant differences in the incidence of nausea and vomiting within 30 min after surgery. The incidence of nausea and vomiting at 24 hours after operation in the four groups was significantly different (P<0.05). The details are as follows. Compared with group L+T, the indexes of group K and L are statistically different (P<0.05). There was a statistically significant difference in the incidence of nausea and vomiting at 24 hours; compared with group T, group K and L had statistical differences (P<0.05). There was no statistically significant difference in the other groups (P>0.05). There was a statistically significant difference in the incidence of abdominal pain and bloating in the four groups at 30 min after operation (P<0.05). The details are as follows. Compared with group L+T, group L has statistically different indicators (P=0.001). There was no statistically significant difference in the other groups (P>0.05). There were statistical differences in the incidence of abdominal pain and abdominal distension at 24 hours after operation in the four groups (P<0.05). The details are as follows. Compared with group L+T, the indexes of group K and L are statistically different (P<0.05); compared with group T, group K and L had statistical differences in indicators (P<0.05), and the differences in the other groups were not statistically significant (P>0.05). TEAS can reduce the incidence of nausea, vomiting, abdominal pain and bloating in patients 24 h after surgery (Table 6).
 |
Table 6 Four Groups of Patients with Different Nausea and Vomiting and Abdominal Pain and Abdominal Distension After Surgical Information |
The bleeding days after surgery were significantly different across the four groups (P<0.05). For groups T and L+T, the number of bleeding days after surgery significantly reduced relative to those for the other two groups. TEAS can shorten the duration of postoperative bleeding (Table 7).
 |
Table 7 Four Groups of Patients with Different the Bleeding Days After Surgical Information |
Discussion
Propofol is among the most widely used intravenous anesthesia drug. However, pain caused by propofol injection is unbearable for several patients. Reducing the incidence and severity of propofol injection pain is an important clinical goal. A safe and effective method for preventing propofol injection pain or reducing its severity has not been established.
TEAS is a new therapy that combines TENS with traditional acupuncture therapy.15 To reduce the incidence and severity of propofol injection pain, as well as the side effects of lidocaine, we adopted combination therapy; therefore, this study combined lidocaine and TEAS for pretreatment to prevent propofol injection pain.
In this study, the incidence of propofol injection pain in group K was 76%, compared to the meta-analysis in 2011 showed that 60% slightly higher incidence of group K.23 A possible reason for this is that the participants were mostly young female patients. Kang et al and Lee et al, in their research results, show that the young women these two factors are high-risk factors of the propofol injection pain occurred.6,24 Group K of VAS score average is the highest among the four groups. The prevalence of nausea, vomiting, abdominal pain, and abdominal distension after surgery were higher in group K than in groups T and T + L.
The incidence and severity of propofol injection pain reduced in group L relative to group K; this shows that lidocaine has a specific preventive effect against propofol injection pain, and it is consistent with the results of previous research. However, the incidence of postoperative nausea, vomiting, and abdominal pain in patients with abdominal distention did not differ significantly. In addition, group L had more bleeding days than group T and L+T. Several studies have reported the inhibition of blood coagulation by lidocaine by mainly inhibiting platelet function.25–27 The underlying mechanism has not been established; however, it has been speculated that lidocaine affects platelet aggregation by altering the platelet membrane stability, and some studies suggest that it can also affect active substances in the plasma.28,29
In this experiment, we selected analgesic acupuncture points from LI4-PC6. LI4 is one of the four groups of essential points of the body, including the acupuncture points in the Yangming hand. Several domestic studies have shown that electrical stimulation in LI4 and PC6 acupunctures can have analgesic effects, promote to activate blood, and calm the nerves, among others. These studies have reported that TEAS stimulation after PC6 acupuncture in patients can reduce the incidence and severity of postoperative nausea and vomiting,30,31 especially among female patients,32 which is also consistent with our experimental results. In group T, the incidence of postoperative nausea, vomiting, and abdominal pain in patients with diarrhea was significantly lower than that in groups K and L, and the difference was statistically significant. The severity of injection pain in groups T and K also decreased, but it was not significantly different from that of group L, compared with the effects of TEAS and lidocaine. However, the number of postoperative bleeding days was reduced after TEAS pretreatment relative to that in groups K and L. The differences were statistically significant. TEAS can shorten the duration of bleeding after hysteroscopy in patients. The present study did not report on the effect of TEAS on postoperative bleeding in patients and the mechanism was not established. Further studies are warranted.
Based on the four-point verbal rating scale and VAS scores, the incidence and severity of propofol injection pain, as well as the incidence of postoperative nausea and vomiting, abdominal pain, and abdominal distension decreased in group L+T, compared with groups K and L. The number of postoperative bleeding days also reduced in group L+T, compared with groups K and L. Thus, for outpatient hysteroscopy or treatment of female patients before surgery, TEAS, which may involve LI4 and PC6 acupuncture on both sides, for 30 min and injection of lidocaine can reduce the incidence and severity of propofol injection pain and the incidence of postoperative nausea, vomiting, and abdominal pain in patients with abdominal distension. In addition, TEAS can shorten the duration of postoperative bleeding and speed up the patients with rapid postoperative recovery.
This study has limitations. We did not further explore the acupoint stimulation mechanism; at the same time, we did not follow patients with postoperative recovery. The study combined TEAS pretreatment with lidocaine to prevent and reduce propofol injection pain. This effectively reduced the incidence and severity of propofol injection pain and significantly reduced the number of women treated with hysteroscopy. The incidence of postoperative nausea, vomiting, and abdominal pain diarrhea were also reduced and the duration of postoperative bleeding was shortened.
The study found that TEAS is effective in preventing propofol injection pain and hope that it will be used more widely given its safety profile. Further research on its mechanisms and other benefits are encouraged. In effect, the analgesic effects of TEAS and its ability to minimize postoperative complications and promote rapid postoperative recovery of patients were assessed to provide insights into its usefulness for perioperative patients and foundations for future research.
Conclusion
TEAS pretreatment combined lidocaine can effectively reduce the incidence and severity of propofol injection pain; the number of women requiring hysteroscopy examination or treatment; incidence of postoperative nausea and vomiting and abdominal pain and distention; and shorten the duration of postoperative bleeding.
Data Sharing Statement
The clinical data used to support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgment
We thank all the individuals who contributed to this study. This work was supported by the National Foundation of Natural Science of China (No.81803937) and the Wenzhou Municipal Science and Technology Bureau (No:2018Y0240).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee HY, Kim SH, So KY. Prevention of microemulsion propofol injection pain: a comparison of a combination of lidocaine and ramosetron with lidocaine or ramosetron alone. Korean J Anesthesiol. 2011;61:30–34. doi:10.4097/kjae.2011.61.1.30
2. Macario A, Weinger M, Truong P, Lee M. Which clinical anesthesia outcomes are both common and important to avoid? The perspective of a panel of expert anesthesiologists. Anesth Analg. 1999;88(5):1085–1091. doi:10.1097/00000539-199905000-00023
3. Picard P, Tramèr MR. Prevention of pain on injection with propofol: a quantitative systematic review. Anesth Analg. 2000;90(4):963–969. doi:10.1213/00000539-200004000-00035
4. Tan CH, Onsiong MK. Pain on injection of propofol. Anaesthesia. 1998;53(5):468–476. doi:10.1046/j.1365-2044.1998.00405.x
5. Huang CL, Wang YP, Cheng YJ, Susetio L, Liu CC. The effect of carrier intravenous fluid speed on the injection pain of propofol. Anesth Analg. 1995;81(5):1087–1088. doi:10.1097/00000539-199511000-00033
6. Kang HJ, Kwon MY, Choi BM, Koo MS, Jang YJ, Lee MA. Clinical factors affecting the pain on injection of propofol. Korean J Anesthesiol. 2010;58(3):239–243. doi:10.4097/kjae.2010.58.3.239
7. Ozturk E, Izdes S, Babacan A, Kaya K. Temperature of propofol does not reduce the incidence of injection pain. Anesthesiology. 1998;89(4):1041. doi:10.1097/00000542-199810000-00039
8. Stokes DN, Robson N, Hutton P. Effect of diluting propofol on the incidence of pain on injection and venous sequelae. Br J Anaesth. 1989;62(2):202–203. doi:10.1093/bja/62.2.202
9. Dewandre J, Van Bos R, Van Hemelrijck J, Van Aken H. A comparison of the 2% and 1% formulations of propofol during anaesthesia for craniotomy. Anaesthesia. 1994;49(1):8–12. doi:10.1111/j.1365-2044.1994.tb03303.x
10. Kim K, Sung kim Y, Lee D-K, et al. Reducing the pain of microemulsion propofol injections: a double-blind, randomized study of three methods of tourniquet and lidocaine. Clin Ther. 2013;35(11):1734–1743. doi:10.1016/j.clinthera.2013.09.018
11. Fletcher JE, Seavell CR, Bowen DJ. Pretreatment with alfentanil reduces pain caused by propofol. Br J Anaesth. 1994;72(3):342–344. doi:10.1093/bja/72.3.342
12. Canbay O, Celebi N, Arun O, Karagöz AH, Saricaoğlu F, Ozgen S. Efficacy of intravenous Acetaminophen and lidocaine on propofol injection pain. Br J Anaesth. 2008;100(1):95–98. doi:10.1093/bja/aem301
13. Borazan H, Erdem TB, Kececioglu M, Otelcioglu S. Prevention of pain on injection of propofol: a comparison of lidocaine with different doses of paracetamol. Eur J Anaesthesiol. 2010;27(3):253–257. doi:10.1097/EJA.0b013e328330eca2
14. O′Hara JF, Sprung J, Laseter JT, et al. Effects of topical nitroglycerin and intravenous lidocaine on propofol-induced pain on injection. Anesth Analg. 1997;84(4):865–869. doi:10.1213/00000539-199704000-00030
15. Francis RP, Johnson MI. The characteristics of acupuncture-like transcutaneous electrical nerve stimulation (acupuncture-like TENS): a literature review. Acupunct Electrother Res. 2011;36(3–4):231–258. doi:10.3727/036012911803634139
16. Huang L, Pan Y, Chen S, et al. Prevention of propofol injection-related pain using pretreatment transcutaneous electrical acupoint stimulation. Turk J Med Sci. 2017;47(4):1267–1276. doi:10.3906/sag-1611-35
17. Zhang Q, Gao Z, Wang H, et al. The effect of pre-treatment with transcutaneous electrical acupoint stimulation on the quality of recovery after ambulatory breast surgery: a prospective, randomised controlled trial. Anaesthesia. 2014;69(8):832–839. doi:10.1111/anae.12639
18. Cai H, Zhou Q, Bao G, Kong X, Gong LY. Transcutaneous electrical nerve stimulation of acupuncture points enhances therapeutic effects of oral lactulose solution on opioid-induced constipation. J Int Med Res. 2019;47(12):6337–6348. doi:10.1177/0300060519874539
19. Hsu YC, Liang IT, Huang SY, Wang HS, Soong YK, Chang CL. Transcutaneous electrical acupoint stimulation (TEAS) treatment improves pregnancy rate and implantation rate in patients with implantation failure. Taiwan J Obstet Gynecol. 2017;56(5):672–676. doi:10.1016/j.tjog.2017.08.017
20. Hadadian F, Sohrabi N, Farokhpayam M, et al. The effects of Transcutaneous Electrical Acupoint Stimulation (TEAS) on fatigue in haemodialysis patients. J Clin Diagn Res. 2016;10(9):YC01–YC04. doi:10.7860/JCDR/2016/19516.8532
21. Chae HD, Kwak MA, Kim IH. Effect of acupuncture on reducing duration of postoperative ileus after gastrectomy in patients with gastric cancer: a pilot study using sitz marker. J Altern Complement Med. 2016;22(6):465–472. doi:10.1089/acm.2015.0161
22. Zheng LH, Sun H, Wang GN, Liang J, Wu HX. Effect of transcutaneous electrical acupoint stimulation on nausea and vomiting induced by patient controlled intravenous analgesia with tramadol. Chin J Integr Med. 2008;14(1):61–64. doi:10.1007/s11655-007-9006-2
23. Jalota L, Kalira V, George E, Shi -Y-Y, Hornuss C, Radke O. Prevention of pain on injection of propofol: systematic review and meta-analysis. BMJ. 2011;342:d1110. doi:10.1136/bmj.d1110
24. Lee BW, Kim SH, So KY. The effect of gender on EC(50) of remifentanil to prevent pain during injection of microemulsion propofol. Korean J Anesthesiol. 2012;63(6):504–509. doi:10.4097/kjae.2012.63.6.504
25. Lo B, Hönemann CW, Kohrs R, et al. Local anesthetic actions on thromboxane-induced platelet aggregation. Anesth Analg. 2001;93(5):1240–1245. doi:10.1097/00000539-200111000-00040
26. Chan WP, Levy JV. Effects of antiplatelet agents on platelet aggregation induced by platelet-activating factor (PAF) in human whole blood. Prostaglandins. 1991;42:337–342. doi:10.1016/0090-6980(91)90082-Q
27. Huang GS, Lin TC, Wang JY. Lidocaine priming reduces ADP-induced P-selectin expression and platelet-leukocyte aggregation. Acta Anaesthesiologica Taiwanica. 2009;47:56–61.
28. Seiler SM, Arnold AJ, Stanton HC. Inhibitors of inositol trisphosphate-induced Ca2 + release from isolated platelet membrane vesicles. Biochem Pharmacol. 1987;36:3331–3337. doi:10.1016/0006-2952(87)90307-8
29. Watala C, Golanski J, Boncler MA, Pietrucha T, Gwozdzinski K. Membrane lipid fluidity of blood platelets: a common denominator that underlies the opposing actions of various. Platelets. 1998;9:315–327.
30. Hou L, Xu L, Shi Y, Gu F. Effect of electric acupoint stimulation on gastrointestinal hormones and motility among geriatric postoperative patients with gastrointestinal tumors. J Tradit Chin Med. 2016;36(4):450–455. doi:10.1016/S0254-6272(16)30061-9
31. Shin K-M, Park J-E, Lee S, et al. Effect of siguan acupuncture on gastrointestinal motility: a randomized, sham-controlled, crossover trial. Evid Based Complement Alternat Med. 2013;2013:918392. doi:10.1155/2013/918392
32. Zárate E, Mingus M, White PF, et al. The use of transcutaneous acupoint electrical stimulation for preventing nausea and vomiting after laparoscopic surgery. Anesth Analg. 2001;92(3):629–635. doi:10.1097/00000539-200103000-00014
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.