Back to Journals » Clinical Ophthalmology » Volume 20
Clinical Outcomes of Neovascular Glaucoma in Patients with Prior and Non-Prior Intravitreal Anti-VEGF Treatment: A Retrospective Cohort Study
Authors Thaebanpakul C ![]() , Hongjamrassilp W
, Hongjamrassilp W ![]() , Kooakachai M
, Kooakachai M ![]() , Rojanapongpun P, Tantisevi V
, Rojanapongpun P, Tantisevi V ![]() , Manassakorn A
, Manassakorn A ![]() , Chansangpetch S, Itthipanichpong R, Ratanawongphaibul K
, Chansangpetch S, Itthipanichpong R, Ratanawongphaibul K
Received 29 March 2026
Accepted for publication 29 May 2026
Published 9 June 2026 Volume 2026:20 612268
DOI https://doi.org/10.2147/OPTH.S612268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Chuthaporn Thaebanpakul,1 Watcharapong Hongjamrassilp,2 Monchai Kooakachai,3 Prin Rojanapongpun,1,4 Visanee Tantisevi,1,4 Anita Manassakorn,1,4 Sunee Chansangpetch,1,4 Rath Itthipanichpong,1,4 Kitiya Ratanawongphaibul1,4
1Center of Excellence in Glaucoma, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand; 2Marine Plankton Research Group, Department of Marine Science, Faculty of Science, Chulalongkorn University, Bangkok, Thailand; 3Department of Mathematics and Computer Science, Faculty of Science, Chulalongkorn University, Bangkok, Thailand; 4Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Correspondence: Kitiya Ratanawongphaibul, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, 1873 Rama IV Road, Pathumwan, Bangkok, 10330, Thailand, Email [email protected]
Purpose: To compare 1-year clinical outcomes between patients with neovascular glaucoma (NVG) who received intravitreal anti–vascular endothelial growth factor (anti-VEGF) therapy prior to NVG diagnosis and those who did not.
Patients and Methods: This retrospective cohort study included patients newly diagnosed with NVG at King Chulalongkorn Memorial Hospital, Thailand, who completed a 1-year follow-up. Participants were categorized into a prior anti-VEGF group and a non-prior anti-VEGF group. Ocular characteristics, including intraocular pressure (IOP) and number of anti-glaucoma medications, were recorded at baseline and at 1, 3, 6, and 12 months. Best-corrected visual acuity (BCVA) and pan-retinal photocoagulation (PRP) status were assessed at baseline and 12 months. The number of post-enrollment anti-VEGF injections, requirement for glaucoma surgery, and NVG recurrence were evaluated at 12 months.
Results: Seventy-three eyes from 73 patients were analyzed (18 prior anti-VEGF; 55 non-prior anti-VEGF). Both groups demonstrated significant IOP reduction at all follow-up visits compared with baseline (P< 0.001), with no significant between-group differences at any time point (P=0.205– 0.898). Anti-glaucoma medications use significantly decreased in the non-prior anti-VEGF group starting from 3-month follow-up (P< 0.001), but not in the prior anti-VEGF group (P=0.082), with no significant between-group difference (P=0.586). The prior anti-VEGF group had a higher proportion of no light perception (P=0.047), although BCVA change did not differ significantly between groups (P=0.126). No significant between-group differences were observed in post-enrollment anti-VEGF injections, PRP status, glaucoma surgery, or NVG recurrence (P=0.504– 0.920). Baseline IOP was significantly associated with time to first glaucoma surgery (β= − 0.06, P=0.005).
Conclusion: Although no significant differences in IOP reduction were observed between NVG patients with and without prior anti-VEGF treatment, both groups achieved significant IOP reduction following treatment initiation. Patients without prior anti-VEGF therapy demonstrated a greater reduction in medication burden at 1 year compared with those who had received prior anti-VEGF treatment.
Keywords: neovascular glaucoma, anti-vascular endothelial growth factor, intravitreal injection, intraocular pressure, clinical outcomes
Introduction
Neovascular glaucoma (NVG) is a severe form of secondary glaucoma associated with a poor prognosis and can lead to irreversible blindness. The term was first introduced by Weiss et al in 1963, describing it as a secondary glaucoma characterized by progressive neovascularization of the iris and trabecular meshwork,1 commonly caused by ischemic retinal diseases such as proliferative diabetic retinopathy (PDR), central retinal vein occlusion (CRVO), and ocular ischemic syndrome.2,3 These ischemic conditions trigger the upregulation of vascular endothelial growth factor (VEGF), which promotes neovascularization and subsequent fibrous obstruction of the trabecular meshwork, leading to refractory elevation of intraocular pressure (IOP) and irreversible optic nerve damage.4 The burden of NVG is significant, with global studies reporting its prevalence between 0.2% and 0.55% in the general population, and comprising approximately 3.9% of all glaucoma cases, with retinal vein occlusion as the major cause.5,6 While these global figures provide a broad perspective on the disease burden, local epidemiological data offer critical insights into regional variations. For instance, in Thailand, a study by Kaewkraisorn et al reported a lower prevalence of 0.012%, highlighting a shift in primary etiology, where PDR—rather than retinal vein occlusion—stands as the leading cause, accounting for 60.4% of cases.7 Visual impairment in NVG patients is severe, with 75% to over 90% experiencing significant vision loss. According to Lazcano-Gomez et al, the study also found that 31% were blind in one eye, while 14% of patients were blind in both eyes.8,9
While pan-retinal photocoagulation (PRP) is the standard treatment to address the underlying retinal ischemia, anti-VEGF therapy has become a vital adjunct for inhibiting angiogenesis.3,4,10–12 Although anti-VEGF agents effectively regress neovascularization, their role in long-term IOP control, reduction of medication dependence, and the timing of surgical intervention remains debated.11,13–24 Furthermore, while the therapeutic use of anti-VEGF in established NVG is well-documented, the clinical impact of anti-VEGF injections administered prior to a formal NVG diagnosis, specifically regarding the subsequent stabilization of IOP and long-term surgical requirements, remains poorly characterized. Critically, interpreting the effects of prior anti-VEGF therapy is challenging, as such treatment may be confounded by the baseline severity of the underlying retinal disease—given that these injections were primarily administered to manage advanced neovascular states such as PDR.25
The primary objective of this study is to assess the impact of prior anti-VEGF therapy administered before the diagnosis of NVG on its efficacy in reducing IOP in patients with NVG. The secondary objective is to evaluate additional clinical outcomes, including the number of anti-glaucoma medications required, visual acuity, the proportion of patients undergoing glaucoma surgery, the time to surgical intervention, the recurrence rate of NVG, and the association between baseline characteristics and clinical outcomes in NVG patients.
Materials and Methods
Participants, and Definition of Neovascular Glaucoma with General Inclusion and Exclusion Criteria
This retrospective cohort study was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University (IRB No.131/64) in 2021. The study was conducted in accordance with the Declaration of Helsinki. The requirement for informed consent was waived by the ethics committee due to the retrospective nature of the study. Patients’ names, addresses, and other confidential information were neither collected nor disclosed during the study. Patients newly diagnosed with NVG at King Chulalongkorn Memorial Hospital, Thailand, between 2010 and 2021, with a complete 1-year follow-up, were recruited for this study. NVG was defined as an eye with neovascularization in the angle (NVA) or iris (NVI), accompanied by elevated IOP (IOP >21 mmHg). Exclusion criteria included total blindness (ICD-10 Category 5; no light perception (NLP)) at baseline, as well as the presence of co-existing other types of glaucoma. Eligible patients were divided into two groups: those who had previously received intravitreal anti-VEGF treatment and those who had not. If both eyes were affected in the same patient, the right eye was chosen for analysis.
Clinical Exams and Study Protocol
Baseline characteristics, including age, gender, systemic diseases, angle types, causes of NVG, best corrected visual acuity (BCVA), and PRP status were collected. BCVA was converted and reported into logMAR units using the European Glaucoma Society Surgical Guide.26 Specifically, hand motion was assigned a logMAR value of 2.3, light perception was assigned 2.8, and NLP was assigned >3.0 (calculated as 3.0 in statistical analysis). Finger count was initially set as logMAR 2.0.27
The IOP was measured using the Goldmann Applanation Tonometer. If measurement was not achievable with this device, an Icare tonometer (Icare Finland OY, Finland) or an Air Puff Tonometer (Nidek CO., LTD., Japan) was used as an alternative. The IOP and number of anti-glaucoma medications were recorded at baseline, 1, 3, 6, and 12 months after enrollment. Data collection allowed for flexibility in the timing of visits, with visits scheduled within 2 weeks for the 1-month visit, within 1 month for the 3-month visit, within 2 months for the 6-month visit, and within 3 months for the 12-month visit.
Other clinical outcomes recorded included BCVA and PRP status at the last follow-up visit (12 months after enrollment), the number of post-enrollment anti-VEGF treatments, the number of glaucoma surgeries, time to first glaucoma surgery, the number of NVG recurrences, and time to first recurrence of NVG. Recurrence of NVG was defined as the reappearance of newly generated NVA or NVI, or the presence of hyphema, along with elevated IOP (>21 mmHg).
Statistical Analysis
Baseline characteristics and clinical outcomes were compared between patients with and without prior intravitreal anti-VEGF treatment. Categorical variables were analyzed using the chi-square test. Data normality for continuous variables was assessed using the Shapiro–Wilk test; normally distributed data were compared using the unpaired t-test, while non-normally distributed data were analyzed using the Mann–Whitney U-test. Within-group changes in BCVA at 12 months relative to baseline were evaluated using the Wilcoxon signed-rank test.
To evaluate longitudinal changes in IOP and the number of anti-glaucoma medications over 1 year, linear mixed-effects models were utilized. These models assessed both within-group changes and between-group differences at each time point, incorporating a group-by-time interaction term and adjusting for clinically relevant covariates, including age, cause of NVG, angle type, lens status, baseline PRP status, and time to first glaucoma surgery.
The probability of NVG recurrence over time was estimated using Kaplan–Meier survival analysis and compared between groups using the Log rank test. The correlation between baseline IOP and time to first glaucoma surgery was assessed using Pearson’s correlation coefficient. To evaluate the association between baseline IOP and time to first glaucoma surgery, a multivariable linear regression analysis was performed using a parsimonious approach. The final model adjusted for clinically relevant confounders, including age, cause of NVG, and prior intravitreal anti-VEGF treatment. Finally, the association of angle type with time to first glaucoma surgery and longitudinal IOP changes was examined using linear regression and linear mixed-effects models (with patient ID as a random effect), respectively. Statistical analysis was calculated using R version 4.5.0., XLSTAT version 2025.1.2 (Addinsoft Inc., France), and STATA version 19.5 SE (StataCorp LLC, the USA). Statistical significance was defined as P < 0.05.
Results
A total of 73 eyes with NVG were analyzed. Of these, 18 eyes (24.7%) had previously received intravitreal anti-VEGF injections, which included 13 (72.2%) of Bevacizumab, 2 (11.1%) of Ranibizumab, 2 (11.1%) of Aflibercept, and 1 (5.6%) of an unknown anti-VEGF agent. The median interval between the last anti-VEGF injection and study enrollment was 122.5 days (interquartile range [IQR], 68.75–264.25 days), based on available data; two values were missing. The remaining 55 eyes (75.3%) had not received such treatment. Baseline characteristics between the two groups were comparable, as shown in Table 1 (P=0.184–1.000), except for PRP status, which was significantly more prevalent in the prior anti-VEGF group compared to the non-prior group (77.8% versus 20.0%, P<0.001, Table 1). Patients with NVG in our study were middle-aged, with approximately 85% having diabetes mellitus as a systemic comorbidity, followed by hypertension and dyslipidemia. The majority of NVG patients presented with closed-angle glaucoma (7 eyes [38.9%] in the prior anti-VEGF group, and 33 eyes [60.0%] in the non-prior anti-VEGF group), primarily due to ischemic retinopathy resulting from PDR (14 eyes [77.8%] in the prior anti-VEGF group, and 31 eyes [56.4%] in the non-prior anti-VEGF group).
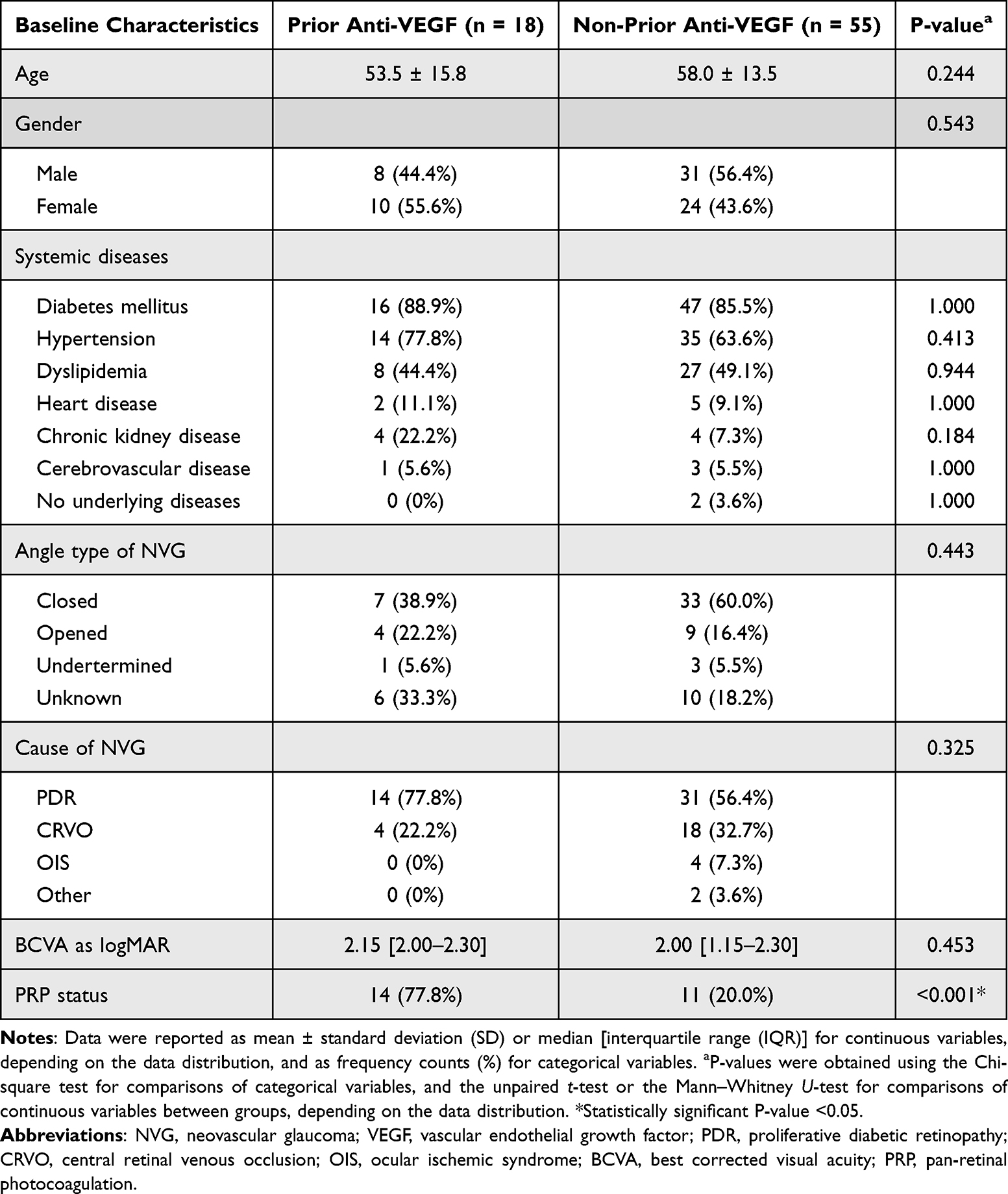 |
Table 1 Baseline Characteristics Comparing NVG Patients with Prior and Non-Prior Intravitreal Anti-VEGF Treatment |
IOP data were analyzed using a linear mixed-effects model, with 80% of measurements obtained via Goldmann applanation tonometry. At baseline, the adjusted mean IOP was 48.3 mmHg (95% confidence interval [CI] 40.6–56.0) in the prior anti-VEGF group and 42.6 mmHg (95% CI 38.7–46.6) in the non-prior anti-VEGF group, with no significant difference between the groups (95% CI −3.1 to 14.5, P=0.205; Table 2 and Figure 1). Both study groups showed a significant reduction in IOP from baseline, starting at 1 month after enrollment, with this reduction continuing at each follow-up visit up to 12 months (P<0.001; Table 2 and Figure 1). However, there was no significant difference in IOP between the groups at any time point (P=0.205–0.898; Table 2 and Figure 1), and no significant overall interaction effect (P=0.854; Table 2). After adjusting for covariates, only lens status showed a marginal association with IOP (P=0.062), while other factors —including age (P=0.157), cause of NVG (P=0.322–0.988), angle type (P=0.326–0.679), baseline PRP status (P=0.404), and time to first glaucoma surgery (P=0.942) —were not significant factors of IOP.
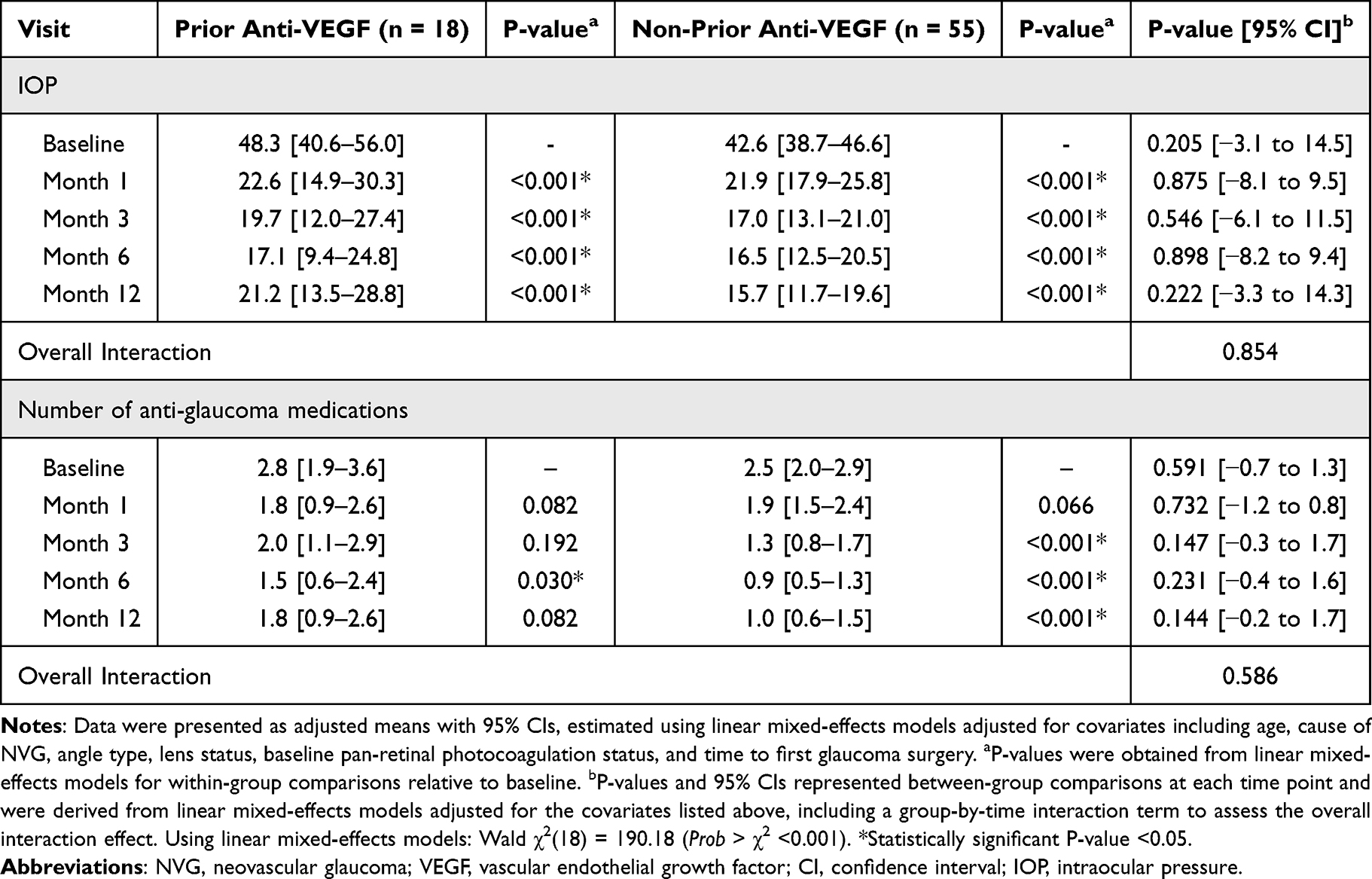 |
Table 2 Comparison of Intraocular Pressure and Number of Anti-Glaucoma Medications Between NVG Patients with Prior and Non-Prior Intravitreal Anti-VEGF Treatment |
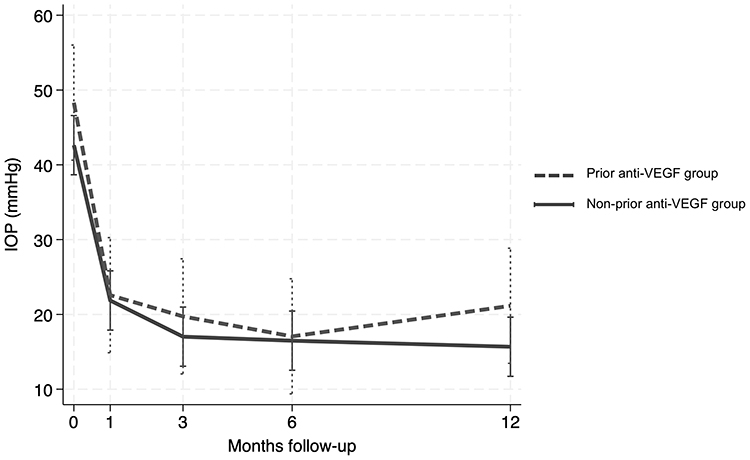 |
Figure 1 Longitudinal trends in adjusted mean intraocular pressure (IOP) over 12 months. The dashed line represents the prior anti-vascular endothelial growth factor (anti-VEGF) group, and the solid line represents the non-prior anti-VEGF group. Vertical error bars represent 95% confidence intervals. A linear mixed-effects model, adjusted for age, cause of neovascular glaucoma, angle type, lens status, baseline pan-retinal photocoagulation status, and time to first glaucoma surgery, was used to compare the longitudinal profiles between groups. Both groups showed statistically significant reductions in IOP from baseline at all follow-up visits (P < 0.001). There was no statistically significant difference in the rate of IOP change between the two groups over the 12-month follow-up (P = 0.854 for group-by-time interaction). |
The prior anti-VEGF group did not exhibit a significant reduction in the number of anti-glaucoma medications compared with baseline at any study visit, except at Month 6 (from 2.8 [95% CI 1.9–3.6] to 1.5 [95% CI 0.6–2.4], P=0.030; Table 2 and Figure 2). In contrast, the number of anti-glaucoma medications in the non-prior anti-VEGF group significantly decreased starting from 3 months after enrollment (from 2.5 [95% CI 2.0–2.9] to 1.3 [95% CI 0.8–1.7], P<0.001; Table 2 and Figure 2), and this reduction persisted through the final visit (1.0 [95% CI 0.6–1.5], P<0.001; Table 2 and Figure 2) compared to baseline. However, comparisons between the groups in each visit showed no significant differences in the number of anti-glaucoma medications used (P=0.144–0.732; Table 2 and Figure 2), or in the overall interaction effect (P=0.586; Table 2). After adjusting for covariates, only the time to first glaucoma surgery showed a significant association with the number of medications (β=0.004, P=0.002). This indicates that for every 100 days surgery is delayed, the patient requires approximately 0.4 additional medications to maintain IOP control. Other factors—including age (P=0.623), cause of NVG (P=0.189–0.743), angle type (P=0.543–0.836), lens status (P=0.560), and baseline PRP status (P=0.871) —were not significant factors.
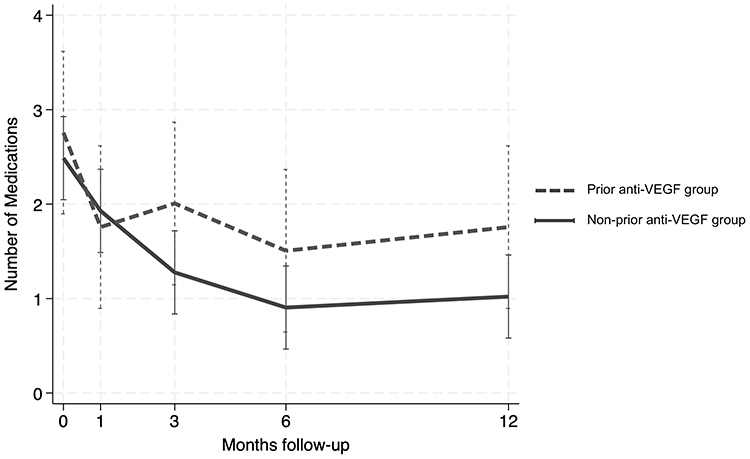 |
Figure 2 Longitudinal trends in adjusted mean number of anti-glaucoma medications over 12 months. The dashed line represents the prior anti-vascular endothelial growth factor (anti-VEGF) group, and the solid line represents the non-prior anti-VEGF group. Vertical error bars indicate 95% confidence intervals. Longitudinal profiles were compared using linear mixed-effects models adjusted for age, cause of neovascular glaucoma, angle type, lens status, baseline pan-retinal photocoagulation, and time to first glaucoma surgery. There was no statistically significant difference in the rate of change between groups over the 12-month follow-up (P = 0.586 for group-by-time interaction). |
Baseline BCVA was similar between the two study groups (P=0.453; Table 1). Regarding within-group changes, the prior anti-VEGF group demonstrated a non-significant trend toward worsening median BCVA (from 2.15 [IQR 2.00–2.30] to 2.55 [IQR 0.90–3.00], P=0.302), whereas the non-prior anti-VEGF group remained stable (from 2.00 [IQR 1.15–2.30] to 2.00 [IQR 0.60–2.30], P=0.107). Although the change in BCVA between groups was not statistically significant (P=0.126; Table 3), the prior anti-VEGF group had a higher proportion of eyes with final BCVA of NLP – 6 eyes (33.3%) – compared with 7 eyes (12.7%) in the non-prior anti-VEGF group (P=0.047; Table 3).
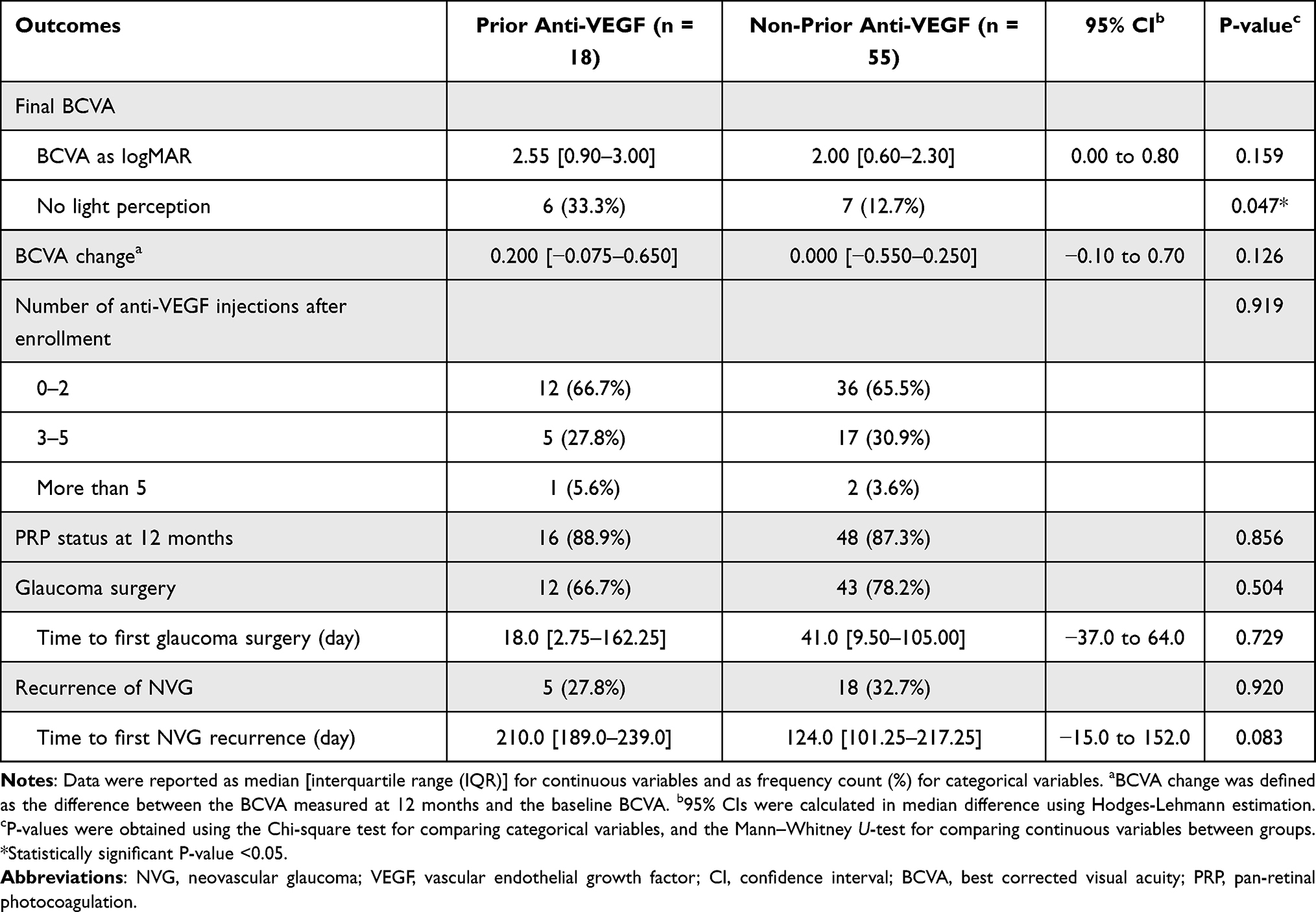 |
Table 3 Clinical Outcomes Comparing NVG Patients with Prior and Non-Prior Intravitreal Anti-VEGF Treatment |
No statistically significant differences were observed between the prior anti-VEGF and non–prior anti-VEGF groups in the number of anti-VEGF injections and PRP status after enrollment, the number of eyes undergoing glaucoma surgery and the time to first surgery, or the number of eyes with NVG recurrence and the time to first recurrence (P=0.083–0.920; Table 3). All glaucoma surgeries performed in this study were trabeculectomy with mitomycin C (MMC). In addition, Kaplan–Meier survival analysis demonstrated no statistically significant difference in time to NVG recurrence between the two groups, as assessed by the Log rank test (P=0.58; Figure 3).
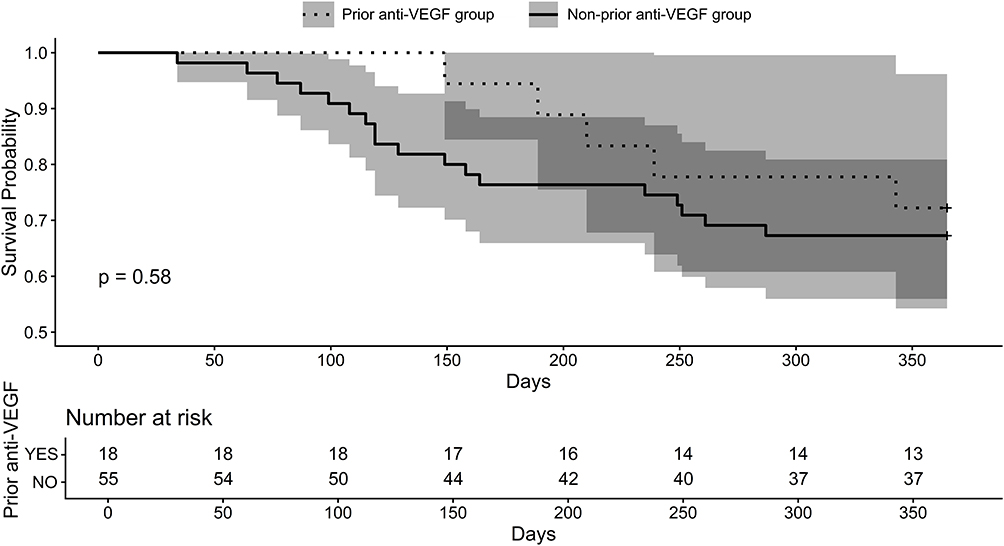 |
Figure 3 Kaplan–Meier survival analysis of time to recurrence of neovascular glaucoma. The survival curves compare eyes with prior anti-vascular endothelial growth factor treatment (dashed line) to those without (solid line). Shaded regions represent 95% confidence intervals. The number of subjects at risk is provided in the table below the plot. The Log rank test revealed no statistically significant difference between the two groups (P = 0.58). |
Figure 4 presents a scatter plot illustrating the relationships between baseline IOP and time to first glaucoma surgery, revealing a significant negative linear correlation (R= −0.402, P=0.003). This finding was further supported by a multivariable linear regression model, which adjusted for age, cause of NVG, and prior intravitreal anti-VEGF treatment. The analysis showed that baseline IOP was an independent factor associated with a shorter time to first glaucoma surgery (β= −0.06, 95% CI [−0.10 to −0.02], P=0.005). Furthermore, the associations between angle status and both IOP change and time to first glaucoma surgery were assessed, revealing no significant associations for either outcome (P=0.931 and P=0.289, respectively).
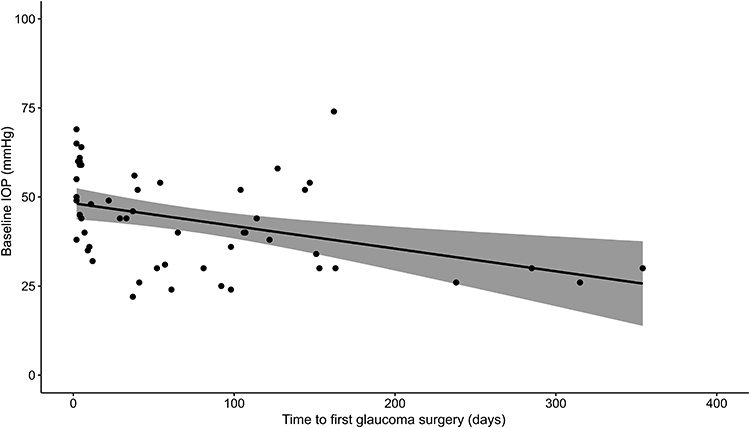 |
Figure 4 Scatter plot showing the linear correlation between baseline intraocular pressure (IOP) and time to first glaucoma surgery. The solid line represents the linear regression fit with the 95% confidence interval indicated by the shaded region. A negative correlation was observed (R = −0.402, P = 0.003), indicating that higher baseline IOP is significantly associated with a shorter time to the first surgical intervention. |
Discussion
Our study revealed that, at the 1-year follow-up, clinical outcomes in patients with NVG were comparable between those who had received intravitreal anti-VEGF treatment prior to NVG diagnosis and those who had not. However, patients without prior anti-VEGF treatment demonstrated a greater reduction in the need for anti-glaucoma medications.
After NVG treatment, a significant reduction in IOP was observed in both study groups (P<0.001; Table 2 and Figure 1), consistent with previous reports. Wittstrom et al reported significant IOP reductions in NVG patients both with and without Bevacizumab treatment, beginning as early as the first week after treatment initiation (P=0.041 and P=0.011, respectively).13 Similarly, Sun et al demonstrated a marked IOP decrease following NVG treatment using various IOP-lowering strategies, from 42.59 ± 9.44 to 16.68 ± 4.69 (P<0.05).23 Our results are also consistent with those of Yazdani et al, who reported that NVG patients receiving monthly intravitreal Bevacizumab injections for three consecutive months, as adjunctive therapy, achieved significant IOP reductions from Month 1 (P=0.007) that persisted through Month 6 (P=0.047).20 In contrast, patients who received only standard treatments – including medications, PRP, glaucoma shunt or cyclodestructive procedures, or other indicated interventions such as cataract surgery or vitrectomy – experienced a significant IOP increase from 32.3 ± 14.3 to 34.9 ± 15.2 mmHg at Month 1 (P=0.046), which remained unchanged through Month 6 (P=0.29–0.92). These findings suggest that adjunctive intravitreal anti-VEGF therapy, particularly Bevacizumab, may provide additional short-term IOP-lowering benefits when combined with standard NVG management. Although our study primarily investigated the effect of anti-VEGF therapy administered before NVG diagnosis, it is important to note that patients in both groups also received anti-VEGF treatment after enrollment (Table 3), which may have contributed to the overall IOP reduction observed. Moreover, approximately 87.3% of patients in our study received intravitreal anti-VEGF injections before trabeculectomy, which might have improved filtering surgery outcomes, including postoperative IOP control. A meta-analysis by Ramji et al reported that trabeculectomy with adjunctive MMC and anti-VEGF had a higher 12-month success rate (OR=1.90, 95% CI [1.16 to 3.10], P=0.01); however, the magnitude of IOP reduction did not differ significantly between eyes receiving anti-VEGF and those that did not.28 Similarly, Zhou et al found that trabeculectomy combined with intravitreal anti-VEGF improved short term outcomes, demonstrating higher success rates (RR=1.19, 95% CI [1.02 to 1.40], P=0.03) and greater IOP reduction at 6 months (standardized mean difference [SMD]=−0.79, 95% CI [−1.50 to −0.07], P=0.03), but the benefit was not sustained at 12 months (SMD=−0.30, 95% CI [−1.61 to 1.02], P=0.66) among patients with NVG.29 The long-term efficacy of anti-VEGF agents in controlling IOP in NVG remains uncertain. A review by Rodrigues et al highlighted this controversy, noting that favorable IOP control was generally observed only within 1 year of follow-up.10 In our cohort, both the prior and non-prior anti-VEGF groups also demonstrated significant IOP reduction at 1 year, with no difference between groups in the overall interaction effect (P=0.854; Table 2). Meanwhile, Olmos et al found no significant IOP difference between NVG eyes treated with Bevacizumab and those without, at most follow-up visits, except at 1 month (P=0.012).11 Besides the short-term effect of anti-VEGF therapy in controlling IOP, we hypothesize that the IOP reduction observed in our cohort was primarily attributable to glaucoma surgery rather than anti-VEGF treatment, as approximately 70% of eyes in both groups underwent surgical intervention (Table 3). Supporting this interpretation, we observed a multivariable linear regression between baseline IOP and time to first glaucoma surgery (β= −0.06, 95% CI [−0.10 to −0.02], P=0.005), indicating that higher baseline IOP was associated with earlier surgical intervention. This suggests that prompt glaucoma surgery possibly played the predominant role in the sustained IOP reduction among NVG patients. Furthermore, given that the half-lives of anti-VEGF agents such as Bevacizumab, Ranibizumab, and Aflibercept is approximately 4–7 days, with an effective duration of approximately 4–6 weeks,30 it is unlikely that their pharmacologic effect accounted for the IOP reduction observed at 1 year. Moreover, it should be remarked that the median interval between the last anti-VEGF injection and study enrollment was 122.5 days (IQR, 68.75–264.25), and the frequency of prior intravitreal anti-VEGF injections was unavailable. Therefore, any anti-VEGF effect would not be expected to persist at the time of enrollment.
Another observation in our study is a marginal association between lens status and IOP (P=0.062) upon evaluating longitudinal data from our cohort using an adjusted linear mixed-effects model. This finding aligns with the distinction observed in existing literature between acute, transient pressure spikes and sustained, long-term IOP elevation. For instance, Liu et al identified the presence of anative crystalline lens as asignificant predictor of immediate IOP spike at 5 minutes after intravitreal anti-VEGF injection (P<0.001).31 Conversely, Sternfeld et al reported no significant difference in sustained IOP elevation following treatment across phakic, pseudophakic, and pseudophakic eyes with post-capsulotomy (P=0.09).32 Given that our study assessed IOP at scheduled visits—representing long-term stability rather than acute post-injection responses—our results support the conclusion that lens status is not a significant determinant of long-term IOP change. These data suggest that while the physical presence of a lens may influence immediate hydrodynamic changes during an injection, it does not exert a lasting effect on IOP levels in this patient cohort. In addition, all IOP measurements in our study were obtained at scheduled visits prior to any clinical interventions, including intravitreal anti-VEGF injections.
Regarding the number of anti-glaucoma medications, a significant reduction from baseline was observed in the non-prior anti-VEGF group beginning at Month 3 (P<0.001; Table 2 and Figure 2). In contrast, eyes in the prior anti-VEGF group showed no significant reduction at most time points, except at Month 6 (from 2.8 [95% CI 1.9–3.6] to 1.5 [95% CI 0.6–2.4], P=0.030; Table 2 and Figure 2). These findings suggest that IOP control may have been more stable in eyes without prior anti-VEGF treatment, as reflected by their decreased need for anti-glaucoma medications, compared with those that had received anti-VEGF therapy before NVG diagnosis. However, the number of medications did not differ significantly between groups at any follow-up visit (P=0.144–0.732; Table 2 and Figure 2). Our results are consistent with previous reports,11,13 showing no significant difference in the number of anti-glaucoma medications between NVG eyes treated with intravitreal Bevacizumab and those without. However, Wittstrom et al observed that the number of anti-glaucoma medications remained unchanged throughout follow-up in both groups, which differs from our findings.13 Conversely, Yazdani et al demonstrated a borderline significant reduction in medication use among eyes receiving adjunctive intravitreal Bevacizumab at Months 1 and 3 (P=0.1 and P=0.06 respectively), but not at Month 6 (P=0.18); nonetheless, in their comparison group, which received the same standard treatments, except for Bevacizumab, no reduction in medication use was observed at any time point (P=0.32–1.0).20 It should be noted, however, that these results may not be directly comparable to ours, as NVG patients in both of our study groups were allowed to receive intravitreal anti-VEGF treatment after enrollment (Table 3), which could have influenced the longitudinal trend in medication use.
Patients who had not received prior anti-VEGF treatment demonstrated better visual outcomes compared to those who had received anti-VEGF therapy before NVG diagnosis. In the prior anti-VEGF group, median BCVA showed a non-significant worsening from 2.15 [IQR 2.00–2.30] to 2.55 [IQR 0.90–3.00] (P=0.302), whereas in the non-prior anti-VEGF group, BCVA remained stable from 2.00 [IQR 1.15–2.30] to 2.00 [IQR 0.60–2.30] (P=0.107). Although the difference in BCVA change between the two groups was not statistically significant (0.200 [IQR −0.075–0.650] versus 0.000 [IQR −0.550–0.250], P=0.126; Table 3), the proportion of eyes with final NLP vision was significantly higher in the prior anti-VEGF group compared with the non-prior group (33.3% versus 12.7%, P=0.047; Table 3). This finding contrasts with the review by Rittiphairoj et al, which reported a greater proportion of visual acuity improvement among eyes receiving anti-VEGF therapy.19 One possible explanation for our results is that patients in the prior anti-VEGF group may have had more severe or preexisting ocular diseases – specifically advanced retinal pathology– which necessitated early anti-VEGF intervention before the onset of NVG. This baseline clinical disparity is further evidenced by our finding that the prior anti-VEGF group had a significantly higher rate of pre-diagnostic PRP compared to the non-prior group (77.8% vs 20.0%, P<0.001; Table 1). Although the final PRP status did not differ significantly between the groups (P=0.856; Table 3). The greater severity and chronicity of the underlying ischemic retinal disease in the prior anti-VEGF cohort likely contributed to the poorer visual outcomes observed, despite subsequent NVG management. Consequently, prior intravitreal anti-VEGF therapy in our study serves as a clinical marker for more advanced retinal disease, which fundamentally influences the visual prognosis in these patients.
A more aggressive surgical approach appears to be undertaken in response to higher baseline IOP levels, as evidenced by the significant inverse association between baseline IOP and time to first glaucoma surgery (β= −0.06, 95% CI [−0.10 to −0.02], P=0.005). This observation likely reflects a clinical tendency to address markedly elevated IOP proactively – often in cases of uncontrolled disease or severe ischemic retinal pathology. In our cohort, the rate of glaucoma surgery ranged from 65% to 80% (Table 3) among eyes with baseline IOPs of approximately 40 mmHg (Table 2), with most procedures performed within 1–2 months after NVG diagnosis (Table 3). This association is consistent with the findings of Casselholm de Salles et al, who reported that NVG eyes secondary to CRVO treated with adjuvant anti-VEGF therapy were more likely to require subsequent IOP-lowering procedures when baseline IOP was markedly elevated.33 Another factor potentially influencing outcomes is angle configuration, which reflects NVG severity. In our study, angle closure was present in approximately 40% of the prior anti-VEGF group and up to 60% of the non-prior group (Table 1). Nakano et al also identified angle-closure NVG as the strongest prognostic factor for final IOP outcomes, with a hazard ratio of 3.059, indicating a threefold increase risk of poor IOP control, which may have contributed to the higher rate of filtering surgery.34 Although such cases could partly explain the higher baseline IOP observed, our cohort showed no significant associations between IOP change and angle type (P=0.931), nor between angle type and time to the first glaucoma surgery (P=0.289). However, the presence of undetermined or missing angle-configuration data in 20 eyes (27.4%) may have limited the statistical power of these analyses. Although anti-VEGF agents are recognized as important adjunctive therapies for NVG by suppressing neovascularization,10,15,19 our study demonstrated high NVG recurrence rates within 1 year – approximately 30% in both groups (Table 3) – suggesting renewed neovascular activity. Wang et al reported that intravitreal Ranibizumab significantly reduced intraocular VEGF levels in NVG eyes within 1 week (from 3698 ± 2105 pg/mL to 184 ± 130 pg/mL; P<0.001); however, the effect was transient.35 Similarly, a previous review noted that anti-VEGF agents have half-lives of approximately 4–7 days and therapeutic effects lasting only 4–6 weeks.30 These findings are consistent with recent studies, which emphasized the short-term, adjunctive role of anti-VEGF therapy.10,15,19 Wang et al further found that complete regression of iris neovascularization occurred in only 85% of eyes, with the remaining 15% demonstrating incomplete regression.35 In our study, the number of anti-VEGF injections after enrollment did not differ significantly between groups (P=0.919; Table 3), and NVG recurrence rates and time to recurrence were also comparable between groups (P=0.920 and P=0.083, respectively; Table 3), with no significant difference in time to recurrence observed on Kaplan–Meier analysis (Log rank test, P=0.58; Figure 3). These findings underscore that definitive NVG management continues to depend on the permanent elimination of ischemic stimuli driving VEGF overproduction—most effectively achieved through PRP in eyes with ischemic retinal disease.
The limitations of this study include its small sample size, reflecting the low prevalence of NVG,7 and its retrospective design, which resulted in missing data that may have influenced the findings. Furthermore, our findings are subject to confounding by indication. Patients who received prior anti-VEGF therapy likely had more advanced underlying retinal ischemic disease; this is supported by our observation that significantly more patients in this group underwent prior PRP (77.8% versus 20.0%, P<0.001; Table 1). This baseline imbalance may have influenced functional outcomes—particularly the higher percentage of eyes reaching NLP (P=0.047, Table 3) —and should be considered when interpreting our results, as the underlying disease severity potentially influences functional outcomes. Additionally, our inclusion criterion of a 1-year follow-up introduces a risk of selection bias. According to our institutional database, 14 patients were lost to follow-up, and 2 patients passed away during the study period, representing an attrition rate of 18.0%; their exclusion from the final analysis may have omitted cases with the most severe clinical presentations or poorer prognoses, potentially leading to an underestimation of disease severity or an overestimation of treatment success. Moreover, the disparity in sample size between groups may limit the statistical power and increase the risk of Type II error, warranting cautious interpretation of our findings. Finally, the severity of the underlying retinal disease was not consistently graded prior to study recruitment. Detailed information regarding the number, duration, type, indication, and route of administration of pre-enrollment anti-VEGF injections was unavailable. Bhagat et al reported that the intracameral route is most effective for IOP control in patients with NVG,36 which could have affected the outcomes. Moreover, both groups in our study received similar post-enrollment anti-VEGF regimens, predominantly Bevacizumab (78% in the prior anti-VEGF group and 72.4% in the non-prior group), which may limit the generalizability of our results to other anti-VEGF agents. Future research would benefit from larger, more balanced cohorts, incorporating detailed assessments of underlying retinal conditions and standardized data collection for anti-VEGF treatment regimens.
Conclusion
In conclusion, anti-VEGF therapy administered before NVG diagnosis was not significantly associated with clinical outcomes, including IOP reduction, disease recurrence, or the need for glaucoma surgery. The observed IOP reduction in our cohort was likely attributable to earlier surgical intervention. Although eyes without prior intravitreal anti-VEGF injections tended to show a greater reduction in medication burden than those that had received such treatment, these differences were not statistically significant. Further studies are warranted to explore the potential benefits of anti-VEGF therapy in other aspects of NVG management.
Disclosure
Assoc. Prof. Dr. Prin Rojanapongpun reports Grants or contracts from Program Management Unit for Competitiveness (PMU-C), Chulalongkorn University Quickwin Fund; Honoraria from Alcon, Abbvie, Glaukos, Johnson & Johnson, Kowa, Santen, Transmedic Healthcare; Meeting/travel support from Alcon, Abbvie, Glaukos, Johnson & Johnson, Santen, Transmedic Healthcare; Leadership or fiduciary roles from Asia Pacific Glaucoma Society, Asia Pacific Academy of Ophthalmology; Stock or stock options from Eye Care Box, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Weiss DI, Shaffer RN, Nehrenberg TR. Neovascular glaucoma complicating carotid-cavernous fistula. Archiv Ophthalmol. 1963;69(3):304–12. doi:10.1001/archopht.1963.00960040310007
2. Havens SJ, Gulati V. Neovascular glaucoma. Dev Ophthalmol. 2016;55:196–204 doi:10.1159/000431196
3. Senthil S, Dada T, Das T, et al. Neovascular glaucoma: a review. Indian J Ophthalmol. 2021;69(3):525–534. doi:10.4103/ijo.IJO_1591_20
4. Allingham RR, Damji KF, Rhee DJ, et al. Shields Textbook of Glaucoma.
5. Feibai B, Onua A. Prevalence, causes and management of neovascular glaucoma: a 5-year review. Open J Ophthalmol. 2019;9(1):1–8. doi:10.4236/ojoph.2019.91001
6. Urbonavičiūtė D, Buteikienė D, Janulevičienė I. A review of neovascular glaucoma: etiology, pathogenesis, diagnosis, and treatment. Medicina. 2022;58(12):1870. doi:10.3390/medicina58121870
7. Kaewkraisorn C, Sayawat N. Prevalence of neovascular glaucoma in Srinagarind hospital. Srinagarind Med J. 2014;29:97.
8. Lazcano-Gomez G, Soohoo JR, Lynch A, et al. Neovascular glaucoma: a retrospective review from a tertiary eye care center in Mexico. J Curr Glaucoma Pract. 2017;11(2):48–51. doi:10.5005/jp-journals-10028-1222
9. Malgi VS, Gawas L, Lyer AS, Rao A. Clinical profile and outcomes of neovascular glaucoma in the era of anti-vascular endothelial growth factors. Indian J Ophthalmol. 2021;69(10):2728–2733. doi:10.4103/ijo.IJO_528_21
10. Rodrigues GB, Abe RY, Zangalli C, et al. Neovascular glaucoma: a review. Int J Retina Vitr. 2016;2(1):26. doi:10.1186/s40942-016-0051-x
11. Olmos LC, Sayed MS, Moraczewski AL, et al. Long-term outcomes of neovascular glaucoma treated with and without intravitreal bevacizumab. Eye. 2016;30(3):463–472. doi:10.1038/eye.2015.259
12. Olmos LC, Lee RK. Medical and surgical treatment of neovascular glaucoma. Int Ophthalmol Clin. 2011;51(3):27–36. doi:10.1097/IIO.0b013e31821e5960
13. Wittström E, Holmberg H, Hvarfner C, Andréasson S. Clinical and electrophysiologic outcome in patients with neovascular glaucoma treated with and without bevacizumab. Eur J Ophthalmol. 2012;22(4):563–574. doi:10.5301/ejo.5000089
14. Hwang HB, Han JW, Yim HB, Lee NY. Beneficial effects of adjuvant intravitreal Bevacizumab injection on outcomes of Ahmed glaucoma valve implantation in patients with neovascular glaucoma: systematic literature review. J Ocul Pharmacol Ther. 2015;31(4):198–203. doi:10.1089/jop.2014.0108
15. Soohoo JR, Seibold LK, Pantcheva MB, Kahook MY. Aflibercept for treatment of neovascular glaucoma. Clin Exp Ophthalmol. 2015;43(9):803–807. doi:10.1111/ceo.12559
16. Inatani M, Higashide T, Matsushita K, et al. Intravitreal Aflibercept in Japanese patients with neovascular glaucoma: the VEGA randomized clinical trial. Adv Ther. 2021;38(2):1116–1129. doi:10.1007/s12325-020-01579-5
17. Inatani M, Higashide T, Matsushita K, et al. Efficacy and safety of intravitreal Aflibercept injection in Japanese patients with neovascular glaucoma: outcomes from the VENERA study. Adv Ther. 2021;38(2):1106–1115. doi:10.1007/s12325-020-01580-y
18. Horsley MB, Kahook MY. Anti-VEGF therapy for glaucoma. Curr Opinion Ophthalmol. 2010;21(2):112–117. doi:10.1097/ICU.0b013e3283360aad
19. Rittiphairoj T, Roberti G, Michelessi M. Anti-vascular endothelial growth factor for neovascular glaucoma (review). Cochrane Database Syst Rev. 2023;4(4). doi:10.1002/14651858.CD007920.pub4
20. Yazdani S, Hendi K, Pakravan M, Mahdavi M, Yaseri M. Intravitreal Bevacizumab for neovascular glaucoma: a randomized controlled trial. J Glaucoma. 2009;18(8):623–627. doi:10.1097/IJG.0b013e3181997211
21. Ciftci S, Sakalar YB, Unlu K, Keklikci U, Caca I, Dogan E. Intravitreal bevacizumab combined with panretinal photocoagulation in the treatment of open angle neovascular glaucoma. Eur J Ophthalmol. 2009;19(6):1028–1033. doi:10.1177/112067210901900620
22. Wakabayashi T, Oshima Y, Sakaguchi H, et al. Intravitreal Bevacizumab to treat iris neovascularization and neovascular glaucoma secondary to ischemic retinal diseases in 41 consecutive cases. Ophthalmology. 2008;115(9):1571–1580. doi:10.1016/j.ophtha.2008.02.026
23. Sun Y, Liang Y, Zhou P, et al. Anti-VEGF treatment is the key strategy for neovascular glaucoma management in the short term. BMC Ophthalmol. 2016;16(1):150. doi:10.1186/s12886-016-0327-9
24. Sugimoto Y, Mochizuki H, Okumichi H, et al. Effect of intravitreal bevacizumab on iris vessels in neovascular glaucoma patients. Graefes’s Arch Clin Exper Ophthalmol. 2010;248(11):1601–1609. doi:10.1007/s00417-010-1406-x
25. Bahr TA, Bakri SJ. Update on the management of diabetic retinopathy: anti-VEGF agents for the prevention of complications and progression of nonproliferative and proliferative retinopathy. Life. 2023;13(5):1098. doi:10.3390/life13051098
26. European Glaucoma Society. A Guide on Surgical Innovation for Glaucoma. European Glaucoma Society; 2023.
27. Moussa G, Bassilious K, Mathews N. A novel excel sheet conversion tool from Snellen fraction to LogMAR including ‘counting fingers’, ‘hand movement’, ‘light perception’ and ‘no light perception’ and focused review of literature of low visual acuity reference values. Acta Ophthalmol. 2021;99(6):e963–e965. doi:10.1111/aos.14659
28. Ramji S, Tan JCK, Jarrar ZA, Hamid S, Gazzard G, Ansari AS. Trabeculectomy augmented with anti-VEGF improves surgical outcomes in glaucoma: a systematic review and meta-analysis. Am J Ophthalmol. 2025;277:184–202. doi:10.1016/j.ajo.2025.05.005
29. Zhou X, Chen J, Luo W, Du Y. Short-term outcomes of trabeculectomy with or without anti-VEGF in patients with neovascular glaucoma: a systematic review and meta-analysis. Trans Vision Sci Technol. 2023;12(9):12. doi:10.1167/tvst.12.9.12
30. Edington M, Connolly J, Chong NV. Pharmacokinetics of intravitreal anti-VEGF drugs in vitrectomized versus non-vitrectomized eyes. Expert Opin Drug Metab Toxicol. 2017;13(12):1217–1224. doi:10.1080/17425255.2017.1404987
31. Liu Y, Wang T, Zhang X, et al. Contributing factors to short-term intraocular pressure elevation following intravitreal anti-VEGF injections. BMC Ophthalmol. 2025;25(1):281. doi:10.1186/s12886-025-04111-x
32. Sternfeld A, Ehrlich R, Weinberger D, Dotan A. Effect of different lens status on intraocular pressure elevation in patients treated with anti-vascular endothelial growth factor injections. Int J Ophthalmol. 2020;13(1):79–84. doi:10.18240/ijo.2020.01.12
33. Casselholm de Salles M, Lindberg C, Epstein D. Neovascular glaucoma in patients with central retinal vein occlusion: a real-life study in anti-VEGF era. Acta Ophthalmol. 2021;99(1):e7–e12. doi:10.1111/aos.14500
34. Nakano S, Nakamuro T, Yokoyama K, Kiyosaki K, Kubota T. Prognostic factor analysis of intraocular pressure with neovascular glaucoma. J Ophthalmol. 2016;2016:1205895. doi:10.1155/2016/1205895
35. Wang JW, Zhou MW, Zhang X, et al. Short-term effect of intravitreal ranibizumab on intraocular concentrations of vascular endothelial growth factor- A and pigment epithelium-derived factor in neovascular glaucoma. Clin Exp Ophthalmol. 2015;43(5):415–421. doi:10.1111/ceo.12477
36. Bhagat PR, Agrawal KU, Tandel D. Study of the Effect of injection bevacizumab through various routes in neovascular glaucoma. J Curr Glaucoma Pract. 2016;10(2):39–48. doi:10.5005/jp-journals-10008-1200
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Initial Real-World Experience with Faricimab in Treatment-Resistant Neovascular Age-Related Macular Degeneration
Leung EH, Oh DJ, Alderson SE, Bracy J, McLeod M, Perez LI, Bottini A, Chin Yee D, Mukkamala K
Clinical Ophthalmology 2023, 17:1287-1293
Published Date: 5 May 2023
Changes in Aqueous Humor Cytokine Profile Following Intravitreal Brolucizumab Injection
Ruamviboonsuk V, Kongwattananon W, Chuaypen N
Clinical Ophthalmology 2025, 19:427-437
Published Date: 11 February 2025
SCOPING: A Multidisciplinary Treatment Protocol for Neovascular Glaucoma with Completely Open or Partially Open Angles
Mokhashi N, Kanter J, Komati R, Mackin A, Dao D, Amin P, Skondra D, Qiu M
Clinical Ophthalmology 2025, 19:4373-4379
Published Date: 1 December 2025