Back to Journals » Clinical Ophthalmology » Volume 19
SCOPING: A Multidisciplinary Treatment Protocol for Neovascular Glaucoma with Completely Open or Partially Open Angles
Authors Mokhashi N ![]() , Kanter J, Komati R, Mackin A, Dao D, Amin P, Skondra D, Qiu M
, Kanter J, Komati R, Mackin A, Dao D, Amin P, Skondra D, Qiu M ![]()
Received 30 July 2025
Accepted for publication 11 November 2025
Published 1 December 2025 Volume 2025:19 Pages 4373—4379
DOI https://doi.org/10.2147/OPTH.S557133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr John Miller
Nikita Mokhashi,1 Jacob Kanter,2 Rahul Komati,3 Anna Mackin,4 David Dao,5 Pathik Amin,1 Dimitra Skondra,1 Mary Qiu6
1Department of Ophthalmology and Visual Science, University of Chicago, Chicago, IL, USA; 2Wilmer Eye Institute, Johns Hopkins University, Baltimore, MD, USA; 3Georgia Retina, Macon, GA, USA; 4Vistar Eye Center, Roanoke, VA, USA; 5Elman Retina Group, Rosedale, MD, USA; 6Cole Eye Institute, Cleveland Clinic, Cleveland, OH, USA
Correspondence: Mary Qiu, Cole Eye Institute, Cleveland Clinic, 2022 E 105 th St, Cleveland, OH, 44106, USA, Email [email protected]
Introduction: A standardized multidisciplinary treatment protocol for NVG was developed in 2020 at the University of Chicago and has been termed Salvaging the Conventional Outflow Pathway in Neovascular Glaucoma (SCOPING). We describe 9 eyes with anterior segment neovascularization and at least partially open angles that underwent the SCOPING protocol to suppress the underlying neovascular drive, control intraocular pressure, and medically or surgically salvage the angle whenever possible.
Methods: Nine eyes from 8 patients with first-time anterior segment neovascularization, at least partially open angles, and normal or elevated IOP were treated with 6 serial monthly intravitreal bevacizumab injections interspersed with pan-retinal photocoagulation.
Results: Five eyes with completely open angles without any peripheral anterior synechiae and each achieved and/or maintained physiologic IOP without requiring surgery. The other 4 eyes presented with partially open angles. Three out of these 4 eyes required subsequent IOP-lowering surgery. None of the 9 eyes developed recurrence of anterior segment neovascularization during the treatment protocol.
Discussion: This protocol may be utilized to salvage the conventional outflow pathway for patients with partially or completely open angles. The etiology and diagnosis of neovascular glaucoma have been established. Current treatment strategies include reduction of neovascular drive including panretinal photocoagulation, intravitreal injections, intraocular pressure lowering medications, and filtration surgery. However, a protocol has not been developed to treat neovascular glaucoma (NVG). Our SCOPING protocol may be helpful for glaucoma specialists in treating patients with neovascular glaucoma.
Keywords: neovascular glaucoma, micro invasive glaucoma surgeries, anti-vascular endothelial growth factor, pan-retinal photocoagulation
Introduction
Neovascular glaucoma (NVG) is a secondary glaucoma that occurs when retinal ischemia leads to the proliferation of fibrovascular tissue anteriorly, leading to neovascularization of the iris (NVI) and/or angle (NVA) with a subsequent increase in intraocular pressure (IOP).1 The management of NVG centers around reducing the vascular endothelial growth factor (VEGF) load and controlling IOP. The two approaches to reduce the VEGF load are intravitreal anti-VEGF therapy such as bevacizumab (IVB) and panretinal photocoagulation (PRP). IVB leads to rapid regression of NVA and NVI which can also contribute to IOP-lowering if the angle is at least partially open and functional.2 While anti-VEGF works immediately, PRP is the gold standard long term solution as it decreases the underlying neovascular drive by inducing tissue coagulation thereby decreasing the production of angiogenic factors by peripheral ischemic retina.3
If the patient presents with NVI or NVA without synechial closure, regression of the anterior neovascularization through anti-VEGF and PRP may be sufficient to achieve physiologic IOP without the need for any glaucoma intervention.4 However, eyes with NVG that have already developed partial or total synechial angle closure often require interventions such as tube shunt implantation or cyclophotocoagulation (CPC) to achieve long-term IOP control.5,6 As a whole, long-term NVG outcomes leave much to be desired,7 and there are many barriers to achieving optimal outcomes in NVG.8 For this reason, a standardized multidisciplinary treatment protocol for NVG was developed in 2020 in collaboration between a glaucoma (MQ) and retina (DS) specialist at the University of Chicago and has been termed Salvaging the Conventional Outflow Pathway in Neovascular Glaucoma (SCOPING). For eyes with anterior segment neovascularization (NVI or NVA) and at least partially open angles, regardless of presenting IOP or presumed visual potential (as long as not already NLP at presentation), we offer an aggressive anti-neovascular treatment protocol in an attempt to medically salvage the conventional outflow pathway and reduce the need for subsequent IOP-lowering surgeries. If IOP becomes uncontrolled on maximum medical therapy, angle-based surgeries may be offered to qualifying patients with the goal of salvaging the conventional outflow pathway whenever possible and delaying or potentially avoiding a tube shunt or CPC.
Materials and Methods
Approval was obtained from the University of Chicago Institutional Review Board (IRB) to perform a retrospective chart review to describe treatment outcomes. Patient consent to review medical records was not required per the University of Chicago IRB given the deidentified nature of the data collected. This work adhered to the 1964 Helsinki declaration and its later amendments. Patients with first-time anterior segment neovascularization (NVI or NVA) and at least partially open angles (defined as no more than 270° of synechial closure) and normal or elevated IOP9 were treated with 6 planned serial monthly IVB injections interspersed with sessions of PRP at the discretion of the retina service with the goal of providing anti-neovascular coverage with the planned monthly injections while sufficient PRP is administered. Given the practice patterns of the retina service, we collaboratively decided to standardize the treatment protocol to 6 scheduled monthly injections, to provide up to 6 months of time for the PRP to be completed. However, depending on the retina specialists’ practice pattern, patients may require greater or fewer than 6 monthly injections to provide an adequate umbrella of anti-neovascular protection while sufficient PRP is completed. Qualifying patients were stratified into 3 stages of disease: patients with NVI or NVA, normal IOP, and absence of PAS; patients with NVI or NVA, elevated IOP, and absence of PAS; and patients with NVI or NVA, elevated IOP, and presence of PAS with partial synechial closure (<75% closure). IVB injections were encouraged to be spaced by 28 days to maintain continuous anti-neovascular protection while the eye undergoes multiple sessions of PRP which has a slower onset of action.3,10,11 If the IOP became elevated despite maximum medical IOP-lowering therapy, and there was no active anterior segment neovascularization, then angle surgery such as gonioscopy assisted transluminal trabeculotomy (GATT) was offered in an attempt to surgically salvage the conventional outflow pathway. Contraindications for GATT included monocular status and inability to hold antiplatelet/anticoagulation. Patients who were considered candidates for GATT first could alternatively elect primary aqueous shunt or CPC instead, depending on the clinical circumstances. Herein, we report pilot results from 9 consecutive NVG eyes that completed the SCOPING protocol, defined as completing 6 scheduled monthly anti-VEGF injections, with as many interspersed PRP sessions as was deemed necessary by the retina service.
Results
In total, 9 eyes from 8 patients qualified for and completed the SCOPING protocol. Presenting clinical characteristics and outcomes are shown in Table 1. Humphrey visual field and OCT testing can be confounded in the setting of NVG due to corneal and retinal findings leading to misinterpretation, thus they were not necessarily performed at baseline in these NVG patients.12,13 The 2 eyes with anterior segment neovascularization and normal IOP were diagnosed despite being asymptomatic because their fellow eye presented symptomatically with NVG and total synechial angle closure.
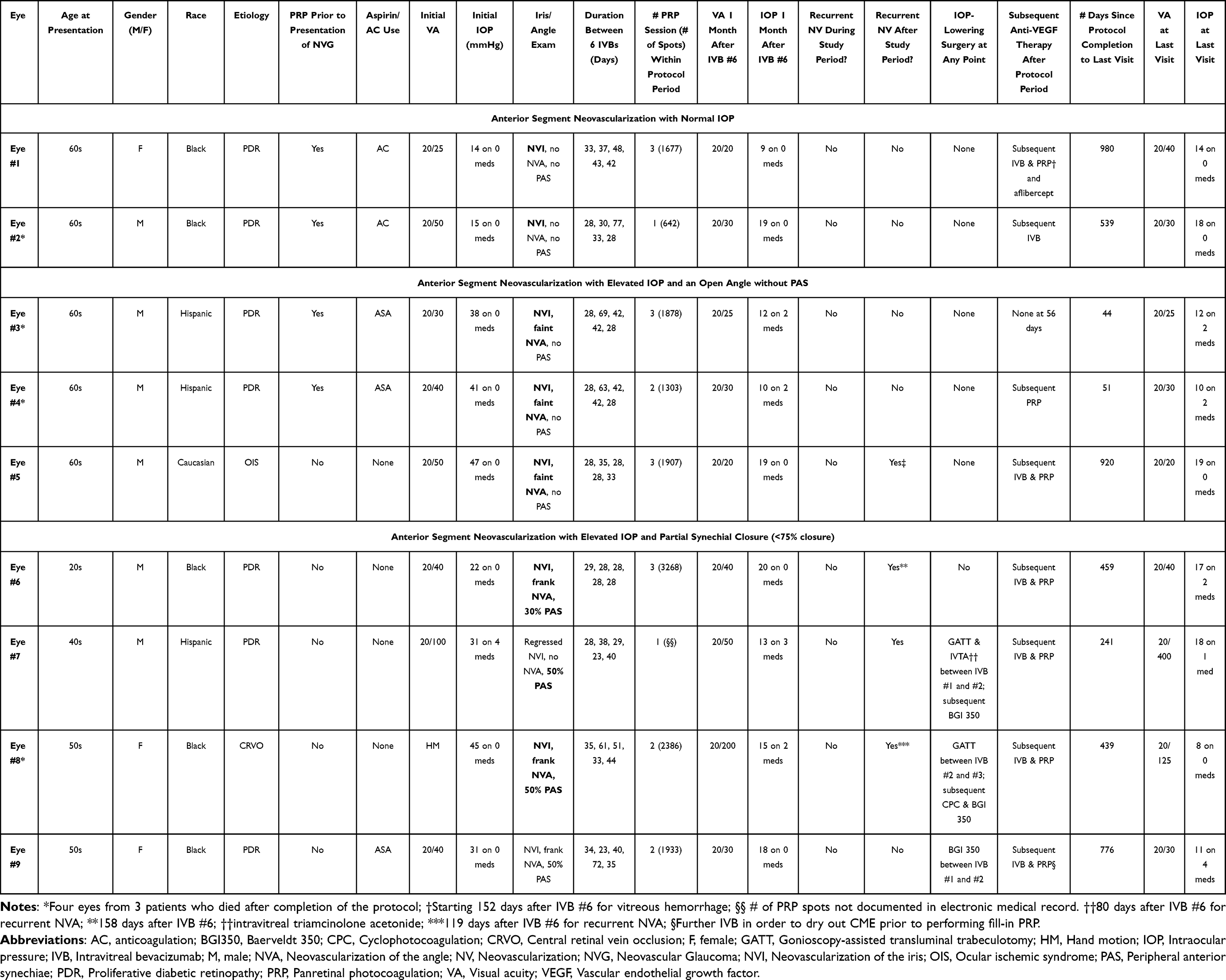 |
Table 1 Demographic Characteristics and Clinical Features of Eyes Presenting with NVI/NVA and Completely or Partially Open Angles Undergoing SCOPING Protocol |
There were 5 male patients, and 5 patients were African American. The median age was 60.5 years (range 25–68). The median presenting VA was 20/40 and the mean presenting IOP was 31 mmHg on 0 medications. IVB was given within 1 day of diagnosis for all but 1 patient who received an injection at a referring doctor’s office 7 days prior to urgent follow up with University of Chicago. Median duration between subsequent IVBs was 35 days (range 23 to 77), median time from IVB #1 to IVB #6 was 203 days (range 152 to 224), and median number of PRP sessions during the protocol period was 2 (range 1–3). One month after IVB #6, median IOP was 15 mmHg (range 9–20) on a median of 2 medications (range 0–2).
Five eyes presented with anterior segment neovascularization and a completely open angle without any peripheral anterior synechiae (PAS). Among these, 2 eyes had normal IOP and NVA while 3 eyes had elevated IOP and NVA. These 5 eyes all achieved and/or maintained physiologic IOP without IOP-lowering surgery to date. Notably, 3 of the 5 eyes underwent subsequent IVB beyond the 6-month SCOPING protocol period: one for cystoid macular edema secondary to PDR, one for vitreous hemorrhage secondary to PDR, and one for recurrent NVA and elevated IOP in the setting of ocular ischemic syndrome.4 These 3 angles remained completely open with the resumption of serial anti-VEGF therapy.
Among the 4 eyes (eyes #6-9) with partial angle closure at the time of presentation, 1 eye (eye #6) was still partially open after completion of the SCOPING protocol and has not required any further procedures. The other 3 eyes (eye #7-9) underwent further procedures.
Eye #7 underwent a GATT between IVB #1 and #2 for elevated IOP on 4 medications. Although GATT is typically contraindicated in eyes with PAS, it can be completed14 and was successfully performed in eye #8 with NVG and PAS.15 After GATT, eye #7 received anti-VEGF injections with a local retina specialist but there was a lapse in retina follow-up, and this eye did not receive anti-VEGF injections for 82 days. Due to this lapse, this eye subsequently developed recurrent NVI and NVA with total synechial angle closure and elevated IOP and underwent a Baerveldt-350 in the sulcus 5 months after SCOPING protocol completion. This was likely due to incomplete PRP as this patient had only 1 session.
Similarly, eye #8 also underwent GATT 35 days after NVG presentation. Eye #8 subsequently achieved medication-free IOP control for 9 months while undergoing monthly anti-VEGF injections before subsequently becoming lost to follow-up. This eye developed recurrent disease with subsequent total synechial angle closure, requiring Baerveldt-350 in the sulcus 9 months after completing the SCOPING protocol.15 In eyes #7 and #8 with progressive synechial closure, the anti-VEGF had ample time to take effect in regressing anterior segment neovascularization since the angle was partially open on presentation, so GATT could be performed after regression. Eye #9, despite initially being an anatomic candidate for GATT, underwent Baerveldt-350 in the sulcus 8 days after NVG presentation as the patient elected for an aqueous shunt instead.
Discussion
Our results demonstrate the value of prompt and aggressive anti-VEGF treatment for anterior segment neovascularization with completely open or partially open angles. IVB leads to immediate regression of NVI and NVA which is maintained while serial injections keep neovascularization at bay. Under the coverage of monthly IVB, interspersed sessions of PRP exert a long-lasting effect beyond the completion of injections. Once sufficient PRP has been completed, serial monthly injections can be stopped. However, it is important to realize that sufficient PRP is difficult to define. The Early Treatment Diabetic Retinopathy Study (ETDRS) defined sufficient PRP as 1200 to 1600 burns which should extend to the edge of an oval area including the disc and macula, and anteriorly to or beyond the equator.16
Of the eyes that had recurrence after completion of the study protocol (eyes #5-8), eye #7 only had 1 session of PRP which was insufficient according to this definition. The other 3 eyes (eyes #5, #6 and #8) did have greater than 1600 burns documented. It is possible that these 3 eyes also did not have sufficient PRP but it is also possible that despite maximal PRP, they had persistent neovascularization from uveal ischemia which would not be addressed by PRP.16 Indeed, there are some choroidal vascular changes that have been documented in PDR and DME, including decreased combined thickness of the choriocapillaris and medium choroidal vessel layers.17
Once PRP is completed, one could consider obtaining a fluorescein angiogram to assess for areas of persistent leakage, or OCT angiography to assess for choroidal ischemia. With prompt control of neovascular drive, there may be a window of opportunity to salvage the angle medically or surgically, if necessary.
Our results reflect the importance of stratifying eyes with anterior segment neovascularization by angle status as described above. For eyes that present with anterior segment neovascularization with a completely open angle, this protocol may allow them to maintain or achieve physiologic IOP without any subsequent IOP-lowering surgery. For eyes that present with partial synechial angle closure, this protocol allows rapid regression of anterior segment neovascularization and temporary improvement of IOP so that any subsequent IOP-lowering surgery can be considered only after anterior segment neovascularization has fully regressed. Microinvasive glaucoma surgeries such as GATT may be attempted to surgically salvage and/or restore the conventional outflow pathway in select eyes if the patient and team are committed to close follow-up and ongoing treatment.
Of the 4 patients who had NVI/NVA with elevated IOP and PAS with partial synechial closure, 3 required IOP-lowering surgery as described above. The patient who elected to have primary BGI 350 did not have recurrence of neovascularization (eye #9). However, the other 2 patients (eyes #7 and #8) who elected to try GATT first may have had insufficient PRP during the 6-month window of anti-VEGF to completely regress their neovascular drive. Thus, while their IOP was controlled during their monthly anti-VEGF in the protocol period, they developed recurrent NVA with subsequent progressive synechial angle closure requiring additional IOP-lowering surgery with BGI-350 in the sulcus. These 2 patients demonstrate that the angle can be salvaged as long as the neovascular drive is controlled. Crucially, sufficient PRP must be completed while patients are receiving short-term coverage with anti-VEGF in order to allow long term control once the injections are stopped. If they do not get full PRP within this period of coverage, neovascularization may recur if there is a break in regular injections.
Each of the patients in this pilot study had at least a partially open angle. In NVG eyes with total synechial closure (defined as more than 270° of synechial closure) and active anterior segment neovascularization, prompt cyclophotocoagulation with anti-VEGF was recommended as the primary intervention, and we have published our outcomes for those patients separately.5 In such patients, IOP would not be expected to improve with regression of anterior segment neovascularization as the angle is already synechially closed.9
Our study has limitations. First it is a retrospective pilot study with small sample size. Additionally, as it is based on 9 individual patients, there is variability in compliance with treatment and follow up. However, we offer a novel and unique protocol to treat neovascular glaucoma which is valuable given the limited guidelines currently available.
Conclusion
The SCOPING protocol may be utilized to salvage the conventional outflow pathway for patients with any anterior segment neovascularization regardless of IOP when the angle is completely or partially open. Further directions include comparison of outcomes in patients with neovascular glaucoma treated prior to the development of the SCOPING protocol.
Data Sharing Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Patient Consent
Consent to publish personal information and case details was obtained verbally from the patients included in this report. No individual patients are identifiable by their case description.
Acknowledgments
The abstract of this paper was presented at the Women in Ophthalmology Conference in 2023 as a poster presentation with interim findings.
Funding
No funding or grant support was used.
Disclosure
Mary Qiu reports personal fees from Lantrek, personal fees from New World Medical, personal fees from Abbvie, personal fees from Nova, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Khanna S, Chang DS. Epidemiology of neovascular glaucoma. In: Qiu M editor. Neovascular Glaucoma. Springer International Publishing; 2022:5–9. doi:10.1007/978-3-031-11720-6_2.
2. Yazdani S, Hendi K, Pakravan M, Mahdavi M, Yaseri M. Intravitreal bevacizumab for neovascular glaucoma: a randomized controlled trial. J Glaucoma. 2009;18(8):632–637. doi:10.1097/IJG.0b013e3181997211
3. Mackin AG, Massamba N, Skondra D. Panretinal photocoagulation for neovascular glaucoma. In: Qiu M editor. Neovascular Glaucoma. Springer International Publishing; 2022:111–119. doi:10.1007/978-3-031-11720-6_13.
4. Asif H, Si Z, Quan S, et al. Neovascular glaucoma from ocular ischemic syndrome treated with serial monthly intravitreal bevacizumab and panretinal photocoagulation: a case report. Case Rep Ophthalmolo Med. 2022;2022:1–5. doi:10.1155/2022/4959522
5. Wang J, Chun LY, Qiu M. Cyclophotocoagulation in neovascular glaucoma with near-total synechial angle closure. Case Rep Ophthalmolo Med. 2023;2023:e5719002. doi:10.1155/2023/5719002
6. Shalaby WS, Amarasekera DC, Shukla AG. Aqueous shunt for neovascular glaucoma. In: Qiu M editor. Neovascular Glaucoma. Springer International Publishing; 2022:151–166. doi:10.1007/978-3-031-11720-6_17.
7. Tailor R, Kinsella MT, Clarke JC. Long-term outcome of intravitreal bevacizumab followed by Ahmed valve implantation in the management of neovascular glaucoma. Seminars Ophthalmol. 2018;33(5):606–612. doi:10.1080/08820538.2017.1375123
8. Qiu M, Shukla AG, Sun CQ. Improving outcomes in neovascular glaucoma. Ophthalmol Glaucoma. 2022;5(2):125–127. doi:10.1016/j.ogla.2021.12.001
9. Wakabayashi T, Oshima Y, Sakaguchi H, et al. Intravitreal bevacizumab to treat iris neovascularization and neovascular glaucoma secondary to ischemic retinal diseases in 41 consecutive cases. Ophthalmology. 2008;115(9):1571–1580.e3. doi:10.1016/j.ophtha.2008.02.026
10. Shakarchi FI, Shakarchi AF, Al-Bayati SA. Timing of neovascular regression in eyes with high-risk proliferative diabetic retinopathy without macular edema treated initially with intravitreous bevacizumab. Clin Ophthalmol. 2018;13:27–31. doi:10.2147/OPTH.S182420
11. Viruni N, Cai CX. Anti-vascular endothelial growth factor for neovascular glaucoma. In: Qiu M editor. Neovascular Glaucoma. Springer International Publishing; 2022:121–130. doi:10.1007/978-3-031-11720-6_14.
12. Salazar H, Swaminathan SS. Treatment goals in neovascular glaucoma. In: Qiu M editor. Neovascular Glaucoma. Springer International Publishing; 2022:97–109. doi:10.1007/978-3-031-11720-6_12.
13. Shazly TA, Latina MA. Neovascular glaucoma: etiology, diagnosis and prognosis. Seminars Ophthalmol. 2009;24(2):113–121. doi:10.1080/08820530902800801
14. Fontana L, De Maria M, Iannetta D, Moramarco A. Gonioscopy-assisted transluminal trabeculotomy for chronic angle-closure glaucoma: preliminary results. Graefes Arch Clin Exp Ophthalmol. 2022;260(2):545–551. doi:10.1007/s00417-021-05400-z
15. Kanter JA, Amin P, Komati R, et al. Gonioscopy-assisted transluminal trabeculotomy in neovascular glaucoma: salvaging the conventional outflow pathway. Am J Ophthalmol Case Rep. 2022;28:101668. doi:10.1016/j.ajoc.2022.101668
16. Early Treatment Diabetic Retinopathy Study Research Group. Techniques for scatter and local photocoagulation treatment of diabetic retinopathy: early treatment diabetic retinopathy study Report No. 3. the early treatment diabetic retinopathy study research group. Int Ophthalmol Clin. 1987;27(4):254–264. doi:10.1097/00004397-198702740-00005
17. Adhi M, Brewer E, Waheed NK, Duker JS. Analysis of morphological features and vascular layers of choroid in diabetic retinopathy using spectral-domain optical coherence tomography. JAMA Ophthalmol. 2013;131(10):1267–1274. doi:10.1001/jamaophthalmol.2013.4321
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Outcomes of Neovascular Glaucoma in Patients with Prior and Non-Prior Intravitreal Anti-VEGF Treatment: A Retrospective Cohort Study
Thaebanpakul C, Hongjamrassilp W, Kooakachai M, Rojanapongpun P, Tantisevi V, Manassakorn A, Chansangpetch S, Itthipanichpong R, Ratanawongphaibul K
Clinical Ophthalmology 2026, 20:612268
Published Date: 9 June 2026