Back to Journals » Cancer Management and Research » Volume 14
Clinical Features Analysis and Survival Nomogram of Primary Small Intestinal Diffuse Large B-Cell Lymphoma
Authors Liu X ![]() , Cao D
, Cao D ![]() , Liu H, Ke D, Ke X, Xu X
, Liu H, Ke D, Ke X, Xu X
Received 7 April 2022
Accepted for publication 27 August 2022
Published 5 September 2022 Volume 2022:14 Pages 2639—2648
DOI https://doi.org/10.2147/CMAR.S369086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Sanjeev K. Srivastava
Xiaohong Liu,1 Dedong Cao,1 Hui Liu,2 Dong Ke,3 Xiaokang Ke,4 Ximing Xu1
1Department of Oncology, Renmin Hospital of Wuhan University, Wuhan, 430060, People’s Republic of China; 2Department of Hematology, Renmin Hospital of Wuhan University, Wuhan, 430060, People’s Republic of China; 3Department of Gastrointestinal Surgery, Renmin Hospital of Wuhan University, Wuhan, 430060, People’s Republic of China; 4Department of Pathology; Renmin Hospital of Wuhan University, Wuhan, 430060, People’s Republic of China
Correspondence: Ximing Xu, Department of Oncology, Renmin Hospital of Wuhan University, 99 Ziyang Road, Wuhan, 430060, People’s Republic of China, Tel +8627-88041911, Email [email protected]
Purpose: This study aimed to analyze the clinical features and survival of primary small intestinal diffuse large B-cell lymphoma (PsI-DLBCL), and establish and independently validate a prognostic nomogram for individual risk prediction.
Patients and methods: Data for 24 patients from the Renmin Hospital of Wuhan University were used as an independent validation cohort, data for 1144 patients with PsI-DLBCL from the SEER database were randomly assigned to training (N=817) and internal validation (N=327) sets. The survival nomogram was constructed with the most significant factors associated with OS using Univariate and multivariate analyses on the training set. Decision curve analysis (DCA) was conducted. Internal validation was SEER validation set. Our cancer center cohort was used as an external validation set to further verify the survival nomogram.
Results: Five clinicopathological feature factors associated with OS of the training set yielded (age, marital status, Ann Arbor stage, surgery for primary site and chemotherapy), which were used to create a survival nomogram. Additionally, the calibration curves of the prognostic nomogram revealed good agreement between the predicted survival probabilities and the ground truth values. The stability of our survival nomogram was explained by internal and external validation data.
Conclusion: Our nomogram proposes the clinical and therapeutic factors affecting OS for patients with PsI-DLBCL. It shows that chemotherapy and surgery are beneficial to patients in the choice of treatment options. These results suggest that a survival nomogram may be better at predicting OS for PsI-DLBCL patients.
Keywords: large B-cell lymphoma, non-Hodgkin, small intestine, SEER, nomogram
Introduction
Diffuse large B-cell lymphoma (DLBCL) is an aggressive B-cell lymphoma and the most common pathological type in non-Hodgkin’s lymphoma (NHL).1,2 According to the different primary sites, it can be divided into intranodal diffuse large B-cell lymphoma (N-DLBCL) and extra nodal diffuse large B-cell lymphoma (EN-DLBCL). EN-DLBCL is worse than N-DLBCL because the two subcategories had different biological characteristics and prognosis.3 While primary gastrointestinal diffuse large B-cell lymphoma (PGI-DLBCL) is the most common of EN-DLBCL (34%).4 In China, the main site of PGI-DLBCL is the stomach, followed by the small intestine, with non-specific clinical manifestations, which are prone to misdiagnosis and missed diagnosis.5 Most previous studies5–7 focused on primary gastric DLBCL(PG-DLBCL)/ intestinal DLBCL(PI-DLBCL), or all PGI-DLBCL. Few studies had separately investigated the potential prognostic variables in patients with primary small intestine DLBCL(PsI-DLBCL). Furthermore, patients with primary small intestine DLBCL have been found to have a poor outcome compared with those with lymphoma in other regions of the gastrointestinal tract. The small intestine is located in the middle of the digestive tract different from primary stomach and colorectal DLBCL, which is difficult to reach by gastroscopy or colonoscopy. In addition, clinical complications of perforation and obstruction are more common and critical, severe complications in PGI-DLBCL can lead to delaying and complicating therapy, decreasing the quality of life, and even mortality. At present, there are no standard guidelines for the treatment of primary small intestinal DLBCL at home and abroad. Therefore, we need to improve the understanding of clinical features and prognosis factors of patients with primary small intestinal DLBCL.
At present, evidence-based medicine is lacking due to the low incidence of PsI-DLBCL. Treatment regimen and prognosis of the patients are still controversial in current studies.8,9 Only retrospective studies with small sample sizes are available. There is no prognostic evaluation system for PGI-DLBCL alone. International Prognostic Index (IPI) score does not distinguish between different outcomes in patients with PGI-DLBCL. The Surveillance, Epidemiology, and End Results (SEER) database can provide the largest sample size of patients with PsI-DLBCL. At the same time, our cancer center has also collected cases of this type to provide more evidence-based medical evidence. In our study, we initially used the SEER database to identify clinical features correlating with overall survival (OS) and thus created a survival nomogram. Then, we independently validated the survival nomogram in the cohort from our cancer center. Moreover, a survival nomogram could help clinicians select treatments and determine the prognosis of this disease by predicting 1-year, 3-year or 5-year survival. Therefore, primary small intestinal DLBCL patients may have better treatment options and a relatively low mortality rate.
Methods
Patient Selection
This study included 1144 cases of PsI-DLBCL from the SEER database and 24 patients from our hospital cohort. Histological diagnosis was confirmed in SEER cases between January 2004 and December 2016. The exclusion criteria were as follows: multiple tumors (first malignant primary indicator), patients younger than 18 years old, deaths that were not tumor-related (SEER “other cause of death” classification). For the validation using our dataset, 24 cases were diagnosed with PsI-DLBCL from January 2014 to February 2021 in our center were enrolled (Supplementary Table 1). The inclusion criteria were defined as follows: histologically proven DLBCL. The primary site is the small intestine.10 The exclusion criteria were defined as follows: a lack of a pathological diagnosis, no treatment, infected with human immunodeficiency virus, younger than 18 years; This retrospective research was approved by the Medical Ethics Committee of Renmin Hospital of Wuhan University and conducted in accordance with the Declaration of Helsinki.
Specific clinical features, therapeutic regimens, and survival outcomes were collected and analyzed, they were randomly assigned to the training set and internal validation set (SEER) according to the ratio 7:3. The patients in our hospital were used as an external validation set. The clinicopathological variables consisted of age at diagnosis, gender, race, insurance, marital status, surgery for primary site, radiation, chemotherapy, and OS time.
Statistical Analysis
Statistical analyses were performed using SPSS software (version 21.0) for Windows (SPSS Inc., Chicago, IL), R software (version 3.3.0) (http://www.r-project.org/). The differences in clinical parameters among the training and validation sets were compared with χ2 test or Fisher’s exact for categorical variables, or one-way ANOVA for continuous variables. P-values< 0.05 at both sides were considered statistically significant. Cumulative survival rates were estimated using the Kaplan-Meier method and compared using the Log rank test. The survival nomogram was constructed with the most significant factors associated with OS using Univariate and multivariate analyses on the training set. Then, calibration curves were generated for the comparison between the actual outcomes and nomogram-predicted survival outcomes. Finally, decision curve analysis (DCA) was conducted by measuring the net benefits for a group of threshold probabilities to measure clinical utility.11
Results
Baseline Characteristics of Patients
Demographics for patients with PsI-DLBCL in three sets are shown in Table 1. Twenty-four patients who were diagnosed with PsI-DLBCL from January 2014 to February 2021 in our cancer center were enrolled. A total of 10 clinical parameters were included in the SEER data and our hospital. There were differences of race, marital status at diagnosis, Ann Arbor stage and Radiotherapy among the training and validation sets. However, we found no significant statistical difference in OS (median survival: 28.0 vs 26.0 vs 39.5 months, P=0.182) among the three sets. Our cancer center had lower All-cause mortality than SEER (29.2 vs 47.2 vs 44.3%, P=0.165), however, there was no statistical difference. Univariate and multivariate analyses of factors associated with OS in training set showed that (age, marital status, Ann Arbor stage, surgery for primary site, chemotherapy) had statistical significance for prognosis, with P value <0.05 (Table 2).
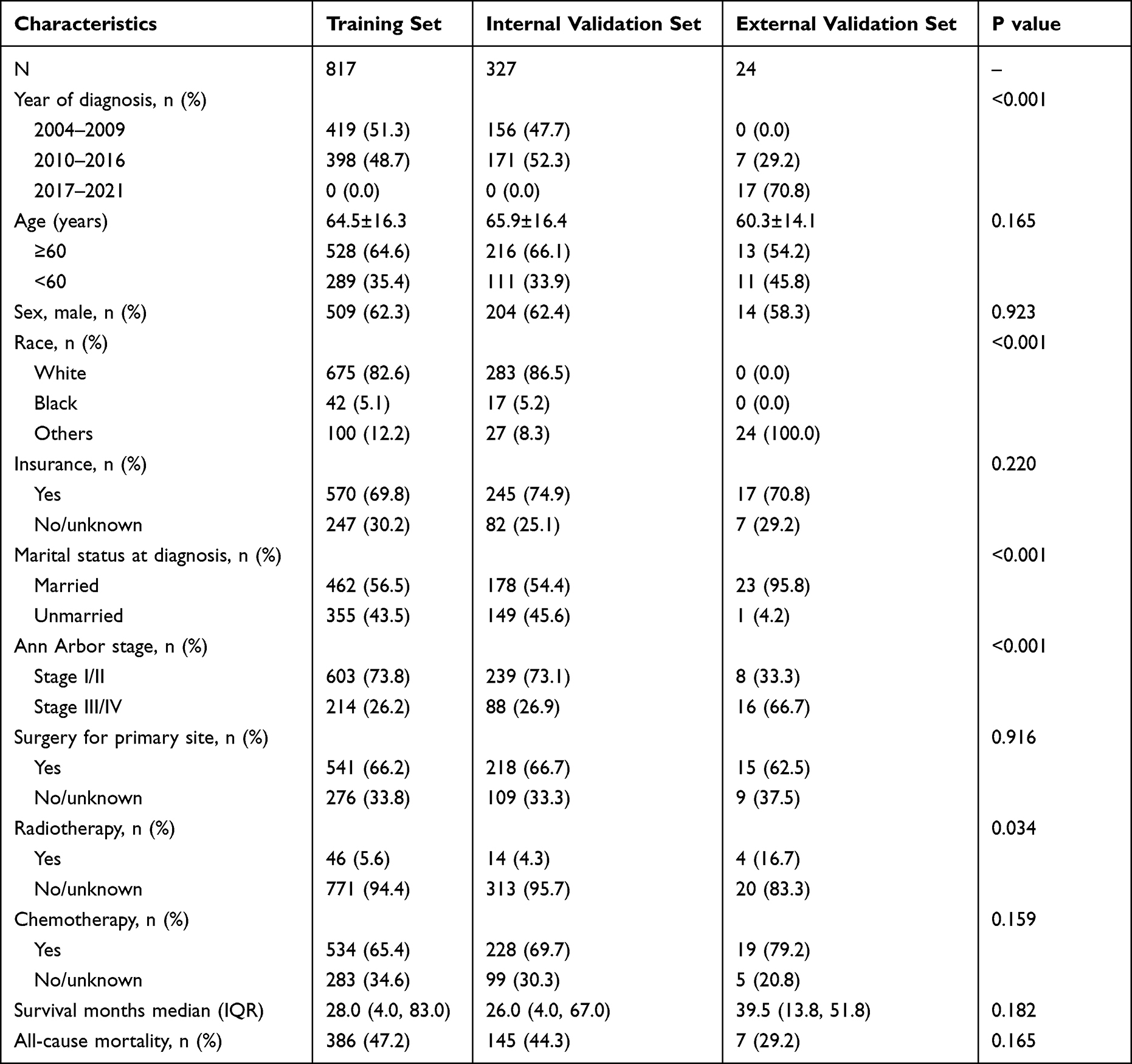 |
Table 1 Clinical Features of All Primary Small Intestinal Diffuse Large B-Cell Lymphoma |
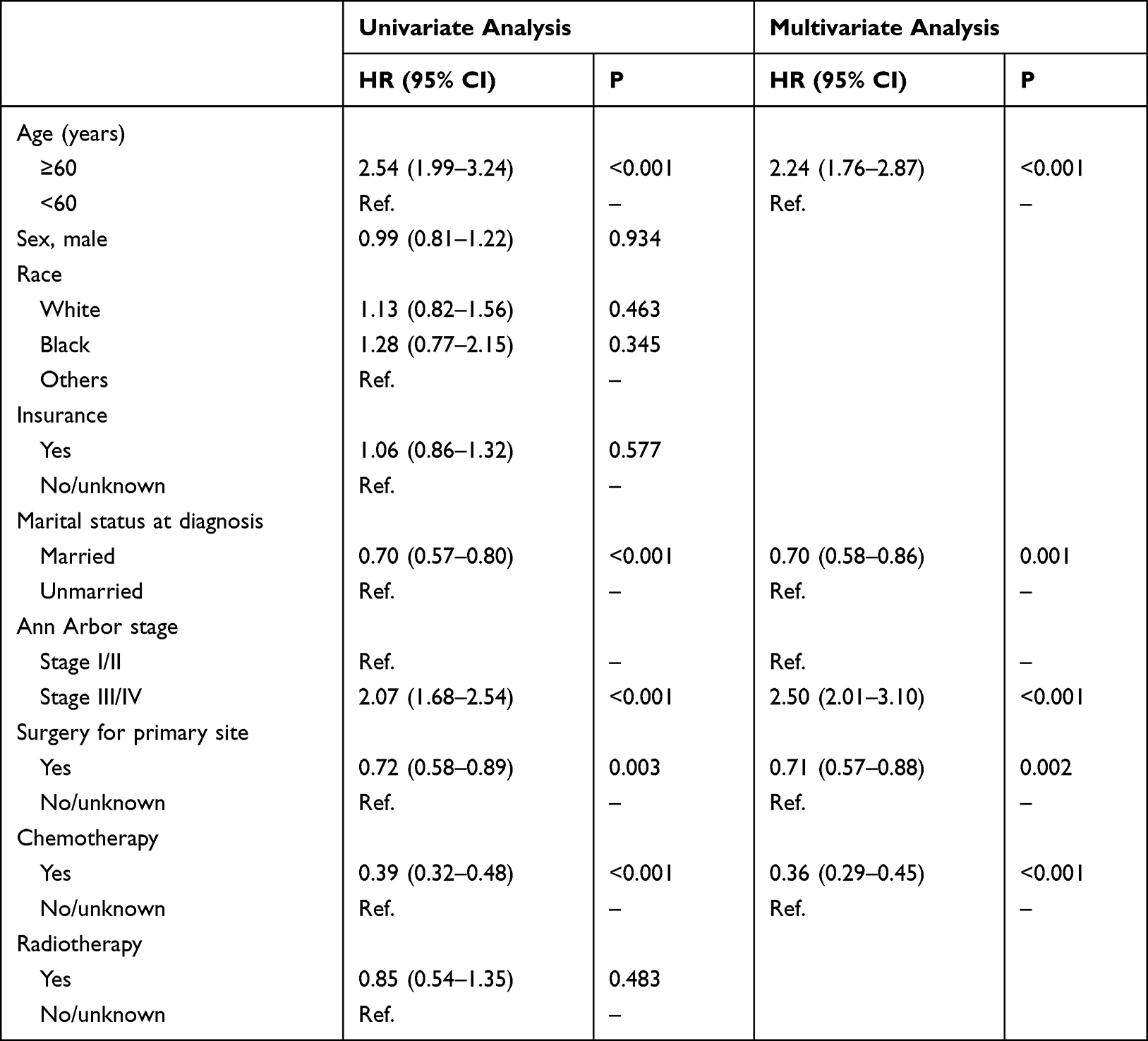 |
Table 2 Univariate and Multivariate Analyses of Factors Associated with OS in Training Set |
The Survival Nomogram
Among them, five parameters (age, marital status stage, Ann Arbor stage, surgery for primary site, chemotherapy) were identified as independent prognostic factors by Univariate and multivariate analyses, Hence, based on these five significant variables, a survival nomogram was created to predict 1-year, 3-year and 5-year survival rates of PsI-DLBCL patients (Figure 1). Then, DCA in the training set showed that if the threshold probability is over 0.5, the survival nomogram for prognostic prediction adds more benefit than treating either all or no patients, indicating that our survival nomogram was clinically useful. (Figure 2A)
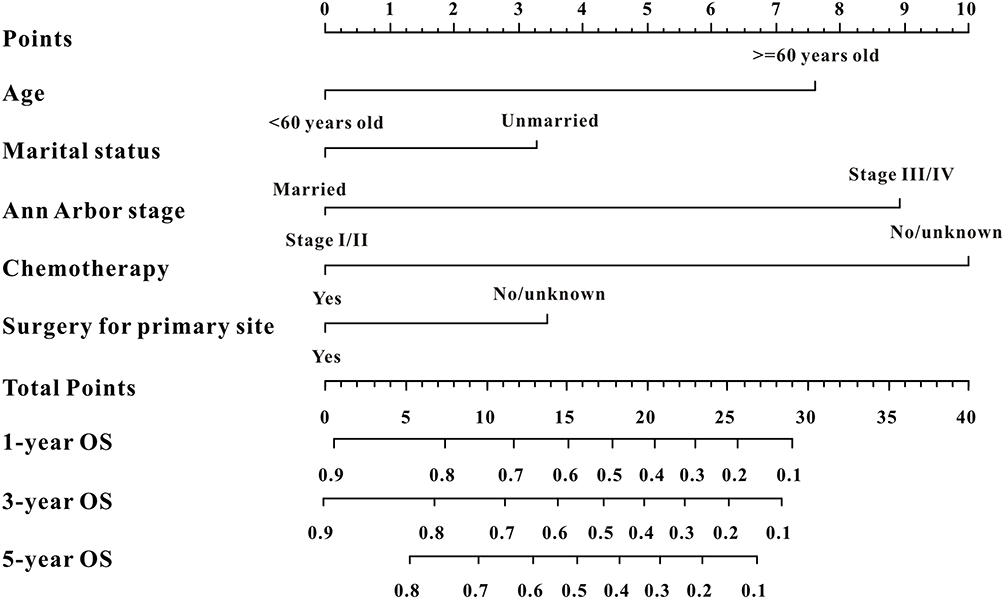 |
Figure 1 A survival nomogram for predicting 1-year, 3-year and 5-year survival rates of primary small intestinal diffuse large B-cell lymphoma patients. |
 |
Figure 2 Decision curves analysis (DCA) for the survival nomogram to predict OS. (A) The DCA of nomogram for OS in training cohort; (B) the DCA of nomogram for OS in internal validation cohort; (C) the DCA of the survival nomogram for OS in external validation cohort. |
Internal and External Validation
Two validation sets were used to verify the resolution and correction ability of the survival nomogram. Internal validation was SEER validation set. Our cancer center cohort was used as an external validation set to further verify the survival nomogram.
Specifically, ROC analysis revealed that the survival nomogram exhibited favorable predictive performance for 1-year, 3-year and 5-year survival. In the training set, td-ROC curves were generated to further evaluate the predictive performance (AUC=0.777, 0.761 and 0.772, respectively) (Figure 3A), the survival nomogram also exhibited good predictive performance in internal validation set (Figure 3B) (AUC=0.735, 0.737 and 0.739, respectively) and external validation set (Figure 3C) (AUC=0.884, 0.870 and 0.865, respectively).
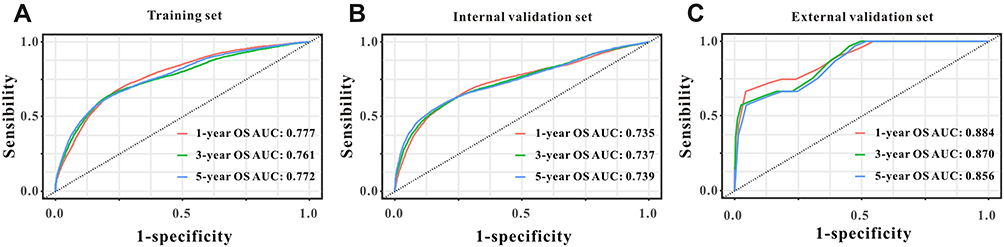 |
Figure 3 The predictive performances of the survival nomogram for predicting 1-year, 3-year and 5-year OS in PsI-DLBCL. ROC curves displayed that this survival nomogram discriminated well in training set (A), internal validation set (B) and external validation set (C). |
Additionally, the calibration curves for the probability of 1-year, 3-year and 5-year survival exhibited an optimal agreement between the predicted outcomes by the survival nomogram and actual values in the SEER training cohort (Figure 4A–C). (Figure 4D–F) calibration plots of 1-year, 3-year and 5-year mortality in internal validation cohort; (Figure 4G–I) calibration plots of 1-year, 3-year and 5-year mortality in external validation cohort.
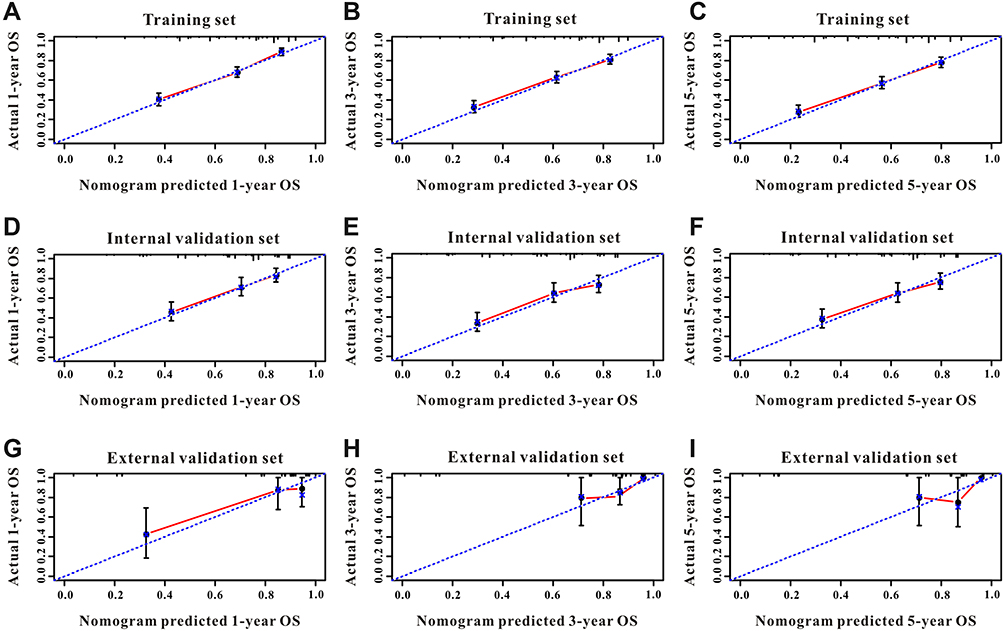 |
Figure 4 The calibration curves for predicting OS in PsI-DLBCL patients. (A–C) Calibration plots of 1-year, 3-year and 5-year mortality in training cohort; (D–F) calibration plots of 1-year, 3-year and 5-year mortality in internal validation cohort; (G–I) calibration plots of 1-year, 3-year and 5-year mortality in external validation cohort. Nomogram-predicted probabilities of OS were plotted on the x-axis, actual observed outcomes were plotted on the y-axis. |
Patients with high risk had a shorter OS period than those with low risk across all subgroups (HR>1) (Figure 5). In internal validation set, patients with high risk exhibited favorable OS (HR=2.75, 95% CI=1.91–3.96, P<0.001) compared to patients with low risk, as reflected by a Kaplan-Meier plot (Figure 5B). As illustrated in Figure 5C, the survival nomogram was also clinically useful in external validation set, the Log rank test indicated that patients with high risk had inferior OS time than those with low risk (HR=8.25, 95% CI=2.05–33.14, P=0.017).
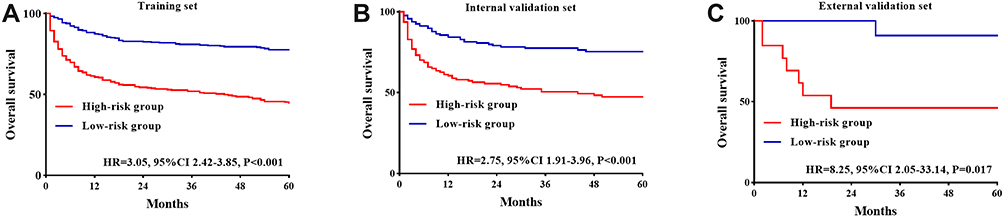 |
Figure 5 Kaplan–Meier curves of the high-risk and low-risk group of PsI-DLBCL patients stratified by the survival nomogram predicted probabilities in training set (A). internal validation set (B) and external validation set (C). |
Discussion
Few clinical studies have been published concerning primary small intestinal DLBCL. In the past 20 years, diagnosis, staging, and treatment of PGI-DLBCL have undergone profound changes. The lack of a uniform staging system has made some historical interstudy comparisons difficult. Of the stage categories defined for each staging system, only the T stage of the Paris classification showed prognostic significance for OS by univariate analysis. However, none of the stage parameters was significantly correlated with patient survival on multivariate analysis.12 Modified Ann Arbor staging criteria as Lugano staging was recommended in our study. Since the addition of rituximab in the DLBCL. The survival rate has been improved.13 However, DLBCL is the most easily perforated gastrointestinal lymphoma the management of severe gastrointestinal complications (GICs) remains a clinical challenge.14 In particular, the PsI-DLBCL is more prone to obstruction and perforation.15 How to identify high-risk and poor prognosis patients, improve the therapeutic effect and overall survival time is still under discussion.
Based on the clinical confusion encountered in patients with PsI-DLBCL, we summarized the clinical and treatment characteristics of 24 cases patients with PsI-DLBCL in our cancer Center in the past 8 years. In view of the relatively rare incidence of the disease, we combined SEER data for systematic comparative analysis. SEER database had recorded detailed clinical parameters such as age, sex, race, insurance, Marital status, Ann Arbor stage, treatment (surgery for primary site, radiotherapy, chemotherapy) between January 2004 and December 2016. In our study, we demonstrated that age, marital status, Ann Arbor stage, surgery for primary site, chemotherapy were independent prognostic factors of OS in patients with PsI-DLBCL. To the best of our knowledge, this is the first survival nomogram based on a series of clinical and treatment features to predict the 1-year, 3-year and 5-year OS in PsI-DLBCL. Indeed, independent validations of survival nomograms are necessary to increase the credibility in their predictive value. Similarly, external validations are also necessary as they can detect the bias of the estimation and evaluate the applicability to different populations.
Among these independent prognostic factors, age and Ann Arbor stage are associated with prognosis in many cases of primary non-Hodgkin’s.2 Our study is consistent with the view. However, there were few studies on the effects of marital status on overall survival, the marital status of patients in our center is significantly different from that in SEER database, which may be related to differences in cultural background. We have relatively more married patients, which suggests that family care in terms of diet, daily living, etc. may helpfully improve the overall survival of patients with gastrointestinal tumors. Marriage was discovered as an independent protective factor for OS in all multiple myeloma adult patients.16 Our study also confirmed that marital status has a statistically significant effect on prognosis. Of course, lymphoma is a systemic disease that requires a combination of treatments. The high heterogeneity of DLBCL leads to different treatment regimens. Our study suggested that chemotherapy and surgery are beneficial to patients with PsI-DLBCL. As we known, surgical treatment was different in gastrointestinal lymphoma, it has been replaced by endoscopic examination, reducing the role of surgery as a means of diagnosis, staging and treatment of PGI-DLBCL. The indications for surgery are relatively narrow. Currently, PGI-DLBCL is mostly treated with chemotherapy combined with surgery or radiotherapy. Surgery is recommended as an urgent treatment for patients with lymphoma presenting with severe perforation, bleeding, or obstruction and as palliative treatment.17,18
At present, many studies have found that chemotherapy combined with radiotherapy can achieve the same survival rate of PG-DLBCL (local stage) and improve the function of gastric preservation.19 A retrospective analysis of 146 patients with primary gastric DLBCL at 8 cancer centers in Turkey suggested that surgical treatment do not improve over survival.20 However, the status of surgical treatment of PsI-DLBCL is controversial, and there are few study evidences. A retrospective analysis of 82 patients with PsI-DLBCL in Taiwan suggested that surgery combined with chemotherapy was the best treatment strategy,21 however pathological types include other types of lymphoma besides DLBCL. We analyzed 15 cases(62.5%) underwent surgical treatments of PsI-DLBCL in our cancer center, five cases underwent surgical procedures for diagnostic purposes, ten cases suffered from emergency surgery due to acute intestinal obstruction, acute gastrointestinal bleeding, and intestinal perforation. Patients with DLBCLs in the small intestine frequently underwent surgery for ileus or perforation and difficult diagnosis,22 surgical resection has little impact on organ function of small intestinal, so we agreed with surgical resection for diagnosis and treatment in PsI-DLBCL. At the same time, treatment of DLBCL relies on systemic chemotherapy. R-CHOP has prevailed as the standard of care for DLBCL, regardless of the immunohistochemical profile or molecular subtype.23 Current studies have confirmed that the presence of Rituximab reduces the surgical rate of PG-DLBCL and do not increase the early mortality.24 However, a SEER-based study of PG-DLBCL suggested that patient age, tumor stage, chemotherapy, and surgery were independent risk factors for long-term survival of PG-DLBCL patients, at the same time, the risk of death was high in the first two years, during which active follow-up should be pursued.6 In our study, Chemotherapy and surgery are beneficial for overall survival of PsI-DLBCL, the internal validation based on SEER is also consistent. The median survival time of our center cases was 39.5 months, which was higher than that of SEER, and the mortality rate was decreased (29.2%).
This study should be considered in the context of a few inevitable limitations. First, the SEER database provides patients with PsI-DLBCL before 2016, There is a time delay in the widespread use of rituximab. Second, the cases in our hospital were in the last 8 years, while the sample size of our cancer center cohort is relatively small. Furthermore, the follow-up time is not long enough, so it is inevitable that there will be statistical bias. But there are still many clinical implications: On one hand, the proportion of stage III–IV patients in our hospital is higher (66.7%), it may be due to the poor awareness and compliance of gastrointestinal physical examination in the Chinese population, in addition, clinical manifestations of PGI-DLBCL are similar to other benign or malignant lesions of gastrointestinal, and the non-specificity is easy to lead to misdiagnosis or delayed diagnosis.25 On the other hand, PsI-DLBCL patients have more advanced disease and a wide range of lesions, so systematic treatment is particularly important, Chemotherapy is the basic treatment, When there is a larger lesions in the gastrointestinal tract, tumors are sensitive to chemotherapy and retreat too quickly, normal tissues cannot be repaired. Therefore, identification of emergency and timely treatment of acute and severe diseases, local surgery can prevent spontaneous perforation and/or bleeding during chemotherapy or radiotherapy, and provide opportunities for subsequent systemic chemotherapy. Under the guidance of clinical experience, radiation therapy can be usually used as an adjunct to surgery, chemotherapy, or both. However, we treat intestinal lymphoma patients with radiotherapy relatively infrequently. It may be because the target area of intestinal radiotherapy is large, especially small intestines have poor tolerance to radiotherapy. Therefore, further clinical studies are needed to explore prognostic factors more comprehensively and validate our survival nomogram for patients with PsI-DLBCL.
Conclusion
Patients with PsI-DLBCL are difficult to diagnose relatively and usually progress with severe gastrointestinal complications. A system that identifies risk stratification is needed. In this study, we analyzed the clinical and therapeutic characteristics of patients with PsI-DLBCL affecting OS from SEER database and our hospital database. Age, marital status, Ann Arbor stage, surgery for primary site and chemotherapy are independent prognostic factors of OS for PsI-DLBCL. Our survival nomogram model provides an applicable tool with good discrimination and calibration abilities to predict the prognosis of PsI-DLBCL. More clinical cases for external validation are expected in future.
Abbreviations
DLBCL, diffuse large B-cell lymphoma; NHL, non-Hodgkin’s lymphoma; N-DLBCL, intranodal diffuse large B-cell lymphoma; EN-DLBCL, extra nodal diffuse large B-cell lymphoma; PGI-DLBCL, primary gastrointestinal diffuse large B-cell lymphoma; PG-DLBCL, primary gastric diffuse large B-cell lymphoma; PsI-DLBCL, primary small intestinal diffuse large B-cell lymphoma; PI-DLBCL, primary intestinal diffuse large B-cell lymphoma; OS, overall survival; GICs, severe gastrointestinal complications; R-CHOP, (Rituximab, cyclophosphamide, doxorubicin/pirarubicin, vincristine, prednisone).
Data Sharing Statement
The Cancer Center of our hospital provided partial data. The Large data regarding patient information were acquired from the SEER database. The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
This study was approved by the Medical Ethics Committee of Renmin Hospital of Wuhan University (number WDRY2021-KS024). The requirement for written informed consent was waived off due to the retrospective nature of the study. The consent waiver was approved via IRB. All data used in this manuscript were anonymized.
Acknowledgments
Great appreciation should be accorded to all the researchers and staff of the SEER Program for their hard work in collecting patient information and maintaining the database.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Li S, Young KH, Medeiros LJ. Diffuse large B-cell lymphoma. Pathology. 2018;50(1):74–87. doi:10.1016/j.pathol.2017.09.006
2. Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390(10091):298–310. doi:10.1016/S0140-6736(16)32407-2
3. Han Y, Yang J, Liu P, et al. Prognostic nomogram for overall survival in patients with diffuse large B-cell lymphoma. Oncologist. 2019;24(11):e1251–e1261. doi:10.1634/theoncologist.2018-0361
4. Castillo JJ, Winer ES, Olszewski AJ. Sites of extranodal involvement are prognostic in patients with diffuse large B-cell lymphoma in the rituximab era: an analysis of the surveillance, epidemiology and end results database. Am J Hematol. 2014;89(3):310–314. doi:10.1002/ajh.23638
5. Chen Y, Chen Y, Chen S, et al. Primary gastrointestinal lymphoma: a retrospective multicenter clinical study of 415 cases in Chinese Province of Guangdong and a systematic review containing 5075 Chinese patients. Medicine. 2015;94(47):e2119. doi:10.1097/MD.0000000000002119
6. Lin JL, Lin JX, Li P, et al. Dynamic prediction of long-term survival in patients with primary gastric diffuse large B-cell lymphoma: a SEER population-based study. BMC Cancer. 2019;19(1):873. doi:10.1186/s12885-019-5993-6
7. Zhang C, Zhang X, Liu Z, et al. The impact of surgery on long-term survival of patients with primary intestinal non-Hodgkin lymphomas based on SEER database. Sci Rep. 2021;11(1):23047. doi:10.1038/s41598-021-02597-1
8. Møller MB, Pedersen NT, Christensen BE. Diffuse large B-cell lymphoma: clinical implications of extranodal versus nodal presentation-a population-based study of 1575 cases. Br J Haematol. 2004;124(2):151–159. doi:10.1046/j.1365-2141.2003.04749.x
9. Wang C, Li W, Liu C, et al. Analysis of clinical and immunophenotypic features along with treatment outcomes of diffuse large B cell lymphoma patients, based on the involvement of nodal or extranodal primary sites[J]. Blood Cells Mol Dis. 2016;57:42–49. doi:10.1016/j.bcmd.2015.12.004
10. Ghimire P, Wu GY, Zhu L. Primary gastrointestinal lymphoma. World J Gastroenterol. 2011;17(6):697–707. doi:10.3748/wjg.v17.i6.697
11. Van Calster B, Wynants L, Verbeek JFM, et al. Reporting and interpreting decision curve analysis: a guide for investigators. Eur Urol. 2018;74(6):796–804. doi:10.1016/j.eururo.2018.08.038
12. Hwang HS, Yoon DH, Suh C, et al. Intestinal diffuse large B-cell lymphoma: an evaluation of different staging systems. J Korean Med Sci. 2014;29(1):53–60. doi:10.3346/jkms.2014.29.1.53
13. Leopardo D, Di Lorenzo G, Federico P, et al. Efficacy of rituximab in gastric diffuse large B cell lymphoma patients. World J Gastroenterol. 2010;16(20):2526–2530. doi:10.3748/wjg.v16.i20.2526
14. Vaidya R, Habermann TM, Donohue JH, et al. Bowel perforation in intestinal lymphoma: incidence and clinical features. Ann Oncol. 2013;24(9):2439–2443. doi:10.1093/annonc/mdt188
15. Maeshima AM, Taniguchi H, Ito Y, et al. Clinicopathological characteristics of diffuse large B-cell lymphoma involving small and large intestines: an analysis of 126 patients. Int J Hematol. 2019;110(3):340–346. doi:10.1007/s12185-019-02687-x
16. Tang L, Pan Z, Zhang X. The effect of marital status on the survival of patients with multiple myeloma. Hematology. 2022;27(1):187–197. doi:10.1080/16078454.2022.2026027
17. Zelenetz AD, Gordon LI, Wierda WG, et al. Diffuse large B-cell lymphoma version 1.2016. J Natl Comprehensive Cancer Netw. 2016;14(2):196–231. doi:10.6004/jnccn.2016.0023
18. Shen Y, Ou J, Wang B, et al. Influence of severe gastrointestinal complications in primary gastrointestinal diffuse large B-cell lymphoma. Cancer Manag Res. 2021;13:1041–1052. doi:10.2147/CMAR.S295671
19. Schmidt W-P, Schmitz N, Sonnen R. Conservative management of gastric lymphoma: the treatment option of choice. Leuk Lymphoma. 2004;45(9):1847–1852. doi:10.1080/1042819042000219476
20. Mehmet K, Sener C, Uyeturk U, et al. Treatment modalities in primary gastric lymphoma: the effect of rituximab and surgical treatment. A study by the Anatolian Society of Medical Oncology. Contemp Oncol. 2014;18(4):273–278.
21. Hong YW, Kuo IM, Liu YY, et al. The role of surgical management in primary small bowel lymphoma: a single-center experience. Eur J Surg Oncol. 2017;43(10):1886–1893. doi:10.1016/j.ejso.2017.06.016
22. Lightner AL, Shannon E, Gibbons MM, et al. Primary gastrointestinal non-Hodgkin’s lymphoma of the small and large intestines: a systematic review. J Gastrointest Surg. 2016;20(4):827–839. doi:10.1007/s11605-015-3052-4
23. Lang R, Gill MJ. Diffuse Large B-Cell Lymphoma. N Engl J Med. 2021;384(23):2261–2262.
24. Prouet P, Giri S, Wiedower E, et al. Addition of rituximab to chemotherapy reduced the rate of surgery for gastric-DLBCL without increasing early mortality. Anticancer Res. 2017;37(2):813–817. doi:10.21873/anticanres.11382
25. Juárez-Salcedo LM, Sokol L, Chavez JC, et al. Primary gastric lymphoma, epidemiology, clinical diagnosis, and treatment. Cancer Control. 2018;25(1):1073274818778256. doi:10.1177/1073274818778256
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Nomogram Based on SEER Database for Predicting Prognosis in Patients with Mucinous Ovarian Cancer: A Real-World Study
Zhang K, Feng S, Ge Y, Ding B, Shen Y
International Journal of Women's Health 2022, 14:931-943
Published Date: 26 July 2022
Analysis of Related Risk Factors and Prognostic Factors of Gastric Cancer with Liver Metastasis: A SEER and External Validation Based Study
An W, Bao L, Wang C, Zheng M, Zhao Y
International Journal of General Medicine 2023, 16:5969-5978
Published Date: 19 December 2023