Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Evaluation of Polymerase Chain Reaction Coupled with Quantum Dot Fluorescence Analysis for Diagnosis of Candida Infection in Vulvovaginal Candidiasis Practice
Authors Fan W, Li J, Chen L, Wu W, Li X ![]() , Zhong W, Pan H
, Zhong W, Pan H ![]()
Received 9 March 2023
Accepted for publication 29 June 2023
Published 25 July 2023 Volume 2023:16 Pages 4857—4865
DOI https://doi.org/10.2147/IDR.S410128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wenjia Fan,1,2,* Jie Li,1,2,* Lingxia Chen,2 Wenhao Wu,2 Xi Li,3 Weihong Zhong,1 Hongying Pan2
1College of Biotechnology and Bioengineering, Zhejiang University of Technology, Hangzhou, 310014, People’s Republic of China; 2Department of Infectious Disease, Zhejiang Provincial People’s Hospital, Hangzhou, 310014, People’s Republic of China; 3Laboratory Medicine Center, Department of Clinical Laboratory, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, 310014, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongying Pan; Weihong Zhong, Tel/Fax +86-571-8589-3602 ; +86-571-88813378, Email [email protected]; [email protected]
Purpose: Time-consuming culture methods and wet-mount microscopy (WMM) with low sensitivity have difficulties in diagnosing Vulvovaginal candidiasis (VVC). Rapid and highly sensitive polymerase chain reaction coupled with quantum dot fluorescence analysis (PCR-QDFA) for the diagnosis of VVC has not been reported to date. This study was the first to evaluate the performance of PCR-QDFA for diagnosis of Candida strains in the leukorrhea samples from patients with suspected VVC.
Patients and Methods: Leukorrhea samples from all visited patients were taken from the vagina using vaginal swabs by clinicians. We evaluated patients admitted with suspected VVC who completed WMM for diagnosis and reported the diagnostic effectiveness of PCR-QDFA and Candida culture (gold standard) when testing leucorrhea samples.
Results: A total of 720 leukorrhea samples from 387 VVC-positive patients and 333 VVC-negative patients were included in this study. Of the 387 leukorrhea samples from the VVC-positive patients, 391 Candida strains were identified by culture. 99.23% (388/391) Candida strains were included in the PCR-QDFA list. The 388 Candida strains belonged to four different species of Candida, including C. albicans (n = 273, 70.36%), C. glabrata (n = 85, 21.91%), C. tropicalis (n = 16, 4.12%), and C. krusei (n = 14, 3.61%). PCR-QDFA diagnosed Candida strains in 340/384 (88.54%) of the leucorrhea samples with Candida strains infection. The sensitivity of PCR-QDFA for C. albicans, C. glabrata, C. tropicalis, and C. krusei was 89.01%, 85.88%, 81.25% and 92.86%, respectively. The specificity of PCR-QDFA for C. albicans, C. glabrata, C. tropicalis and C. krusei was 93.69%, 99.37%, 99.71%, and 99.57%, respectively.
Conclusion: The highly sensitive and specific PCR-QDFA technique can be exploited as a rapid (approximately 4 h) diagnostic tool for common Candida strains of leucorrhea samples from patients with suspected VVC.
Keywords: PCR-QDFA, VVC, NAC, diagnostic performance, Candida culture
Introduction
VVC is a common mucosal infection of the lower female reproductive tract that afflicts many women.1 Up to 75% women of reproductive age will experience VVC at least once in their lifetime, and up to 9% women experience more than three episodes annually.2 Symptomatic VVC mainly results from the excessive growth of Candida, which is followed by epithelial invasion and the production of virulence effectors. The Candida strain can escape immune responses and resist many antifungal drugs by forming biofilms.3–6 The majority of asymptomatic VVC patients are predominantly colonized by Candida strains.7 When a patient's immunity is weak, colonized Candida strains can release virulence factors to trigger VVC.8 Colonized Candida strains is an important prerequisite of symptomatic VVC.9 The causes of Candida infection in VVC patients are well known and include overuse of glucocorticoids, immune disorders, diabetes, pregnancy, hormone replacement and behavioral risk factors.10–12 Currently, the treatment of Candida infections usually involves azoles such as fluconazole, but Candida species may differ in their drug sensitivities.13,14 Erroneous diagnosis and empirical drug treatment can lead to persistent growth and recurrent infection of resistant strains. Therefore, timely and exact identification of Candida species can facilitate accurate treatment of VVC.
Notably, accurate diagnosis and treatment of vaginitis is challenging due to similarities in clinical symptoms and vaginal discharge with other vaginal conditions. Usually, the diagnosis of VVC is based on the gold standard of Candida culture.15 However, culture methods are reported to have low sensitivity and are time-consuming (approximately 40 h–57 h). Culture methods often require combined time-of-flight analyzer mass spectrometry (MALDI-TOF MS) technique to achieve high sensitivity.16 However, expensive MALDI-TOF MS requires isolates of high purity to be tested. These are the elements that cause the patient’s treatment to be delayed, which raises hospital expenses.17 In addition, wet-mount microscopy (WMM) is often used as a quick, simple, and inexpensive method of VVC diagnosis. However, the observation background in WMM is complex and extremely demanding for the observer, which can easily lead to missed diagnoses.7 WMM was also shown worse sensitivity and specificity.18 Furthermore, Candida species cannot be differentiated by this method.
Several molecular diagnostic approaches for identifying Candida at the species or strain level have been established.17,19 PCR-QDFA to identify Candida species is exactly new technique of a multiplex PCR assay using quantum dot luminescence to transduce a signal. The high sensitivity (86.10%) and specificity (100%) of PCR-QDFA applied to the diagnosis of bloodstream infections have been reported. PCR-QDFA exhibited high sensitivity (100%) and specificity (99.59%) for Candida strains in blood.20 However, the use of PCR-QDFA for the diagnosis of VVC has not been reported. The purpose of the present study was to validate the performance of PCR-QDFA for the identification of Candida strains in leukorrhea samples from patients with suspected VVC.
Materials and Methods
Patients
Between April 2021 and October 2021, this study was carried out at the Zhejiang Provincial People’s Hospital in Zhejiang, China. The leukorrhea samples of all patients enrolled in this study had been removed from the vagina using vaginal swabs by clinicians. All patients enrolled in this study had been diagnosed with WMM. WMM is to directly smear the leucorrhea sample on the glass slide, and then directly observe whether there are spores or hyphae under the microscope without staining agent. The entry criteria of the subjects included (1) being diagnosed with VVC by WMM. VVC was diagnosed when pseudohyphae or budding yeast were found with WMM.21 (2) Being initially diagnosed with vaginitis by the gynecologist. (3) Exhibit clinical symptoms of VVC (eg, abnormal vaginal discharge, vaginal itching, vaginal redness, vaginal mucosal congestion, burning, dysuria).8 Patients who met two of the above entry criteria were recruited for this study. Leukorrhea samples from all enrolled patients were performed for Candida cultures. The diagnosis of VVC was ultimately confirmed by Candida culture method.22 Once one or more Candida strains were isolated from the leukorrhea samples by the Candida culture method, a positive VVC case was confirmed. Otherwise, one negative VVC case would be identified. Notably, leukorrhea samples with negative results of the first culture method and positive results of WMM were required to perform a second Candida culture. The diagnostic result of this leukorrhea samples was defined based on the result of a second Candida culture.
Conventional Microbiological Methods
Vaginal split dilutions were evenly mixed and inoculated into 70 mm Candida chromogenic plates (Autobio Diagnostics CO., Ltd, China) with sterile cotton swabs. The Candida chromogenic plate can be replaced by sabouraud medium plate. The sabouraud medium mainly consists of peptone (10g/l), glucose (40g/l), agar (15g/l), chloramphenicol (125mg/l) and purified water. The 70 mm Candida chromogenic plates placed in an incubator for 48 hours at 37°C.22,23 Three randomly selected Candida colonies with the same morphology were inoculated onto a new Candida chromogenic plate for further culture and finally identified by mass spectrometry (MALDI-TOF, bioMérieux, France).23,24
Description of PCR-QDFA Setup
PCR-QDFA is a fully automated diagnostic technique that can directly diagnose the common Candida strains (C. albicans, C. glabrata, C. tropicalis and C. krusei) of leukorrhea samples from patients with suspected VVC. Biotin labeled PCR primers specifically amplify genes of different Candida strains. The nylon membrane has oligonucleotide capture probes that hybridize to amplified pathogenic targets. When the PCR amplified product was molecularly hybridized with the probe on the Nissl strip, the hybridization product was combined with that of QDs in the detection solution. Under fluorescence excitation at a specific wavelength, the quantum dots emit a fluorescence signal. The presence or absence of this pathogen in a specimen is identified by the finding that the probe hybridizes to this DNA fragment, as judged by the fluorescent signal at a specific position on the membrane strip.
Deoxyribonucleic acid (DNA) was extracted from 400μL vaginal split dilutions using nucleic acid extraction and purification reagents from Hangzhou Kilogene Biotech Co., Ltd, 8μL for following experiments. Ninety-six samples could be detected by each PCR-QDFA test. The 96 samples included 1 positive control (mainly including C. albicans DNA, HPV16 and the house-keeping genes of human), 1 negative control sample (human house-keeping genes) and 94 clinical leucorrhea samples to be tested. The positive control and negative control were from Hangzhou Kilogene Biotech Co., Ltd. The control sample and the extracted gene to be tested were subjected to the same amplification reaction and hybridization reaction as follows. 8μL of the extracted DNA was equally added to configuration tubes No. 1 and configuration tubes No. 2. Configuration tube No. 1 contained 20 μL reaction liquid I (Primer, dN (U) TP, UDG enzyme, buffer) and 1 μL reaction liquid III (Taq DNA polymerase, TAQ-Antibody) from Hangzhou Kilogene Biotech Co., Ltd. Configuration tube No. 2 contained 20 μL reaction liquid II (Primer, dN (U) TP, UDG enzyme, buffer) and 1μL reaction liquid III (Taq DNA polymerase, TAQ-Antibody) from Hangzhou Kilogene Biotech Co., Ltd. PCR-QDFA was mainly employed as a multiplex PCR combined with the hybridization reaction. PCR-QDFA was accomplished as a multiplex PCR reaction in a PCR machine (tc-96; Hangzhou Borge Science and Technology Co., Ltd.) (Figure S1).16 PCR conditions included a uracil-DNA glycosylase reaction at 50°C for 2 min, pre denaturation at 95°C for 10 min, 40 amplification cycles and a further extension at 72°C for 5 min. Each amplification cycle consisted of a denaturation step at 95°C for 30 seconds and an annealing/amplification step at 55°C for 1 minute followed by an extension step at 72°C for 30 seconds. Automated operational hybridization detection was accomplished using an automatic hybridization detector (kj-96; Hangzhou Kilobase Biotechnology Co., Ltd.), as advised by the manufacturer.16 Automated operational hybridization detection was performed using the following conditions: 1 hr hybridization at 48°C; 15 min wash at 48°C; 30 min incubation at room temperature; 5 min wash at room temperature; and final fluorescence detection on a fluorescence imager (js-680e; Shanghai Peiqing Technology Co., Ltd.).
Statistical Analysis
The result of Candida incubation combined with MALDI-TOF MS was employed as a control to evaluate the efficacy of PCR-QDFA.15 Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall percent agreement (OPA) were calculated for each target following comparison to the Candida culture results (which included adjudication of discordant results). The Kappa test was performed in the statistical package (Statistical Package for the Social Sciences) to calculate the statistical significance of sensitivity and specificity.25
Results
Characteristics of Patients Enrolled in This Study
A total of 720 suspected VVC patients were registered in this study. These patients were recruited from gynecological departments, obstetric departments, or reproductive departments. All registered patients were ≥17 years of age, with an average age of 26.5 years (17–69 years). The rate of patients with abnormal leucorrhea (34.11%) and vaginal Itching (47.92%) were relatively higher in the group of patients with VVC while the rate of patients with abnormal cervical secretion (61.56%), hyperemic in vaginal mucosa (9.01%), dysuria (4.20%) and dellyache (3.90%) was higher in the group of patients without VVC. Of the 720 patients with suspected VVC, 272 patients showed positive WMM results. Of the 387 positive VVC patients, 266 patients were diagnosed with WMM (Table 1).
 |
Table 1 Characteristics of Patients with Suspected VVC Enrolled in the Study |
Diagnostic Results of Traditional Laboratory Methods (Conventional)
Of the 720 patients recruited, 387 VVC-positive and 333 VVC-negative samples were confirmed by Candida culture. Of the 387 VVC-positive cases, one case of Saccharomyces cerevisiae infection and two cases of C. parapsilosis infection were excluded from the next performance evaluation of PCR-QDFA for Candida strains within PCR targets. Because S. cerevisiae and C. parapsilosis were not included within the PCR-QDFA diagnostic targets (only 4 species). Therefore, the remaining 717 samples containing 333 VVC-negative cases and 384 VVC-positive cases were included in this study. Of the 384 leukorrhea samples from the VVC-positive patients, 388 Candida strains were identified by culture. The 388 Candida strains belonged to four different species of Candida, including C. albicans (n = 273, 70.36%), C. glabrata (n = 85, 21.91%), C. tropicalis (n = 16, 4.12%), and C. krusei (n = 14, 3.61%) (Figure 1).
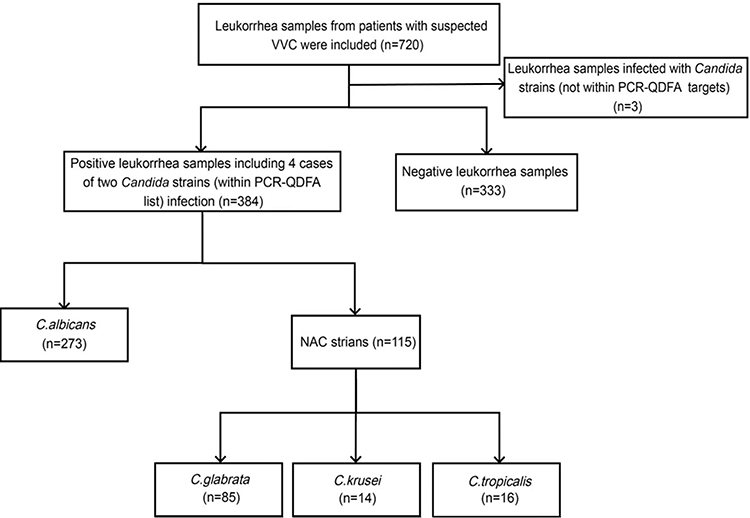 |
Figure 1 Candida diversity analysis in leukorrhea samples from 720 suspected VVC patients. |
Overall Diagnostic Performance of PCR-QDFA for Candida Strains (Within the PCR Targets) in Leukorrhea Samples
Seven hundred and seventeen leucorrhea samples (384 positive VVC samples and 333 negative VVC samples) confirmed by culture method were used to evaluate the diagnostic performance of PCR-QDFA for Candida strains in leucorrhea samples. Three hundred and eighty-four leukorrhea samples of VVC positive cases included 380 leukorrhea samples infected with one Candida strain and 4 leukorrhea samples infected with two Candida strains. Among the 380 leukorrhea samples, which were diagnosed with one Candida strain by culture, 339 (89.21%) Candida strains were successfully identified by PCR-QDFA. Additionally, only 1 (0.25%) leukorrhea sample infected with two Candida strains was successfully detected by PCR-QDFA among 4 leukorrhea samples. Among the 384 positive VVC samples, 44 samples were false-negative samples diagnosed by PCR-QDFA. Of 44/384 (11.46%) leukorrhea samples, 8/44 (18.18%) leukorrhea samples were found with Candida strains by PCR-QDFA that were discordant with the culture method results. PCR-QDFA did not identify any Candida strains in the remaining 36/44 (81.82%) leukorrhea samples (Table S1).
Conversely, among the 333 leukorrhea samples from VVC-negative cases, Candida strains of 28 (8.4%) leukorrhea samples were identified by PCR-QDFA (Table S2). For 305/333 (91.59%) leukorrhea samples without Candida infection, the PCR-QDFA diagnostic results were consistent with the culture results. The sensitivity, specificity, and positive predictive value of PCR-QDFA assay for pathogenic Candida strains in leukorrhea samples from patients suspected VVC were 88.54%, 91.59%, and 89.96%, respectively. The kappa value of PCR-QDFA was 0.80 for pathogenic Candida strains in leukorrhea samples (Table 2).
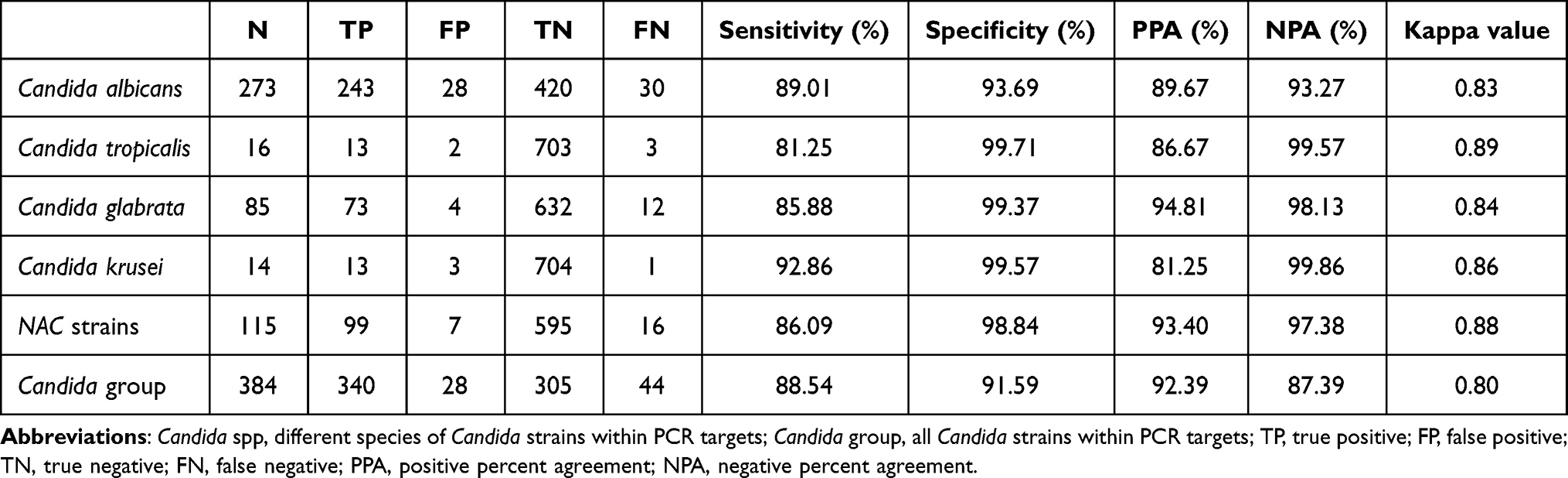 |
Table 2 Performance of PCR-QDFA for Diagnosis of Candida spp |
Diagnostic Performance of PCR-QDFA for C. albicans Strains in Leukorrhea Samples from Patients Suspected of VVC
Performance analysis of PCR-QDFA for different Candida strains was mainly divided into the diagnostic performance of C. albicans and NAC strains. Among the 273/717 (38.07%) leukorrhea samples where C. albicans strains were identified by culture method, the results of 243 samples diagnosed by PCR-QDFA assay were consistent with culture method, while the results of 2 samples were not. The remaining 28/273 (10.26%) C. albicans strains were unidentifiable by PCR-QDFA (Table S1).
Based on the culture method results, the 444/717 (61.92%) samples that were negative for C. albicans included 333 samples with no Candida infection and 111 samples with NAC strains infection. Furthermore, 25/333 (7.51%) samples were found with C. albicans infection by PCR-QDFA. Meanwhile, 3 (2.70%) leukorrhea samples were diagnosed with C. albicans infection among remaining 111 samples infected with NAC strains (Table S1). In summary, 28 (6.31%) samples with C. albicans infection were found by PCR-QDFA among 444 leukorrhea samples without C. albicans infection according to the culture method results. For 416/444 (93.69%) leukorrhea samples without C. albicans infection, the diagnostic results of PCR-QDFA were consistent with those of culture. The sensitivity, specificity, and kappa value of PCR-QDFA for C. albicans were 89.01%, 93.69%, and 0.83, respectively (Table 2).
Diagnostic Performance of PCR-QDFA for NAC Strains (Within the PCR Targets) in Leukorrhea Samples from Patients Suspected of VVC
Among 115 leukorrhea samples with NAC strain infection, 99/115 (86.09%) NAC strains were identified by PCR-QDFA and consistent with the diagnostic results of the culture method. Among the remaining 16/115 (13.91%) samples where the NAC strains were not identified by PCR-QDFA, 6 samples were identified with C. albicans infection, while the other 10 samples were detected without candida strains. Among the 602 leukorrhea samples without NAC strain infection, 7 NAC strains were identified by PCR-QDFA, including 3 strains diagnosed as C. albicans by culture (Table S2). For the 595/602 (98.84%) leukorrhea samples without NAC strain infection, the PCR-QDFA diagnostic results were consistent with the culture results. The sensitivity, specificity, and kappa value of PCR-QDFA for NAC strains were 86.09%, 98.84% and 0.88, respectively (Table 2).
Of the 717 leukorrhea samples, 85 samples were diagnosed with C. glabrata strains by culture method. A total of 73/85 (85.88%) leukorrhea samples with C. glabrata infection were identified by PCR-QDFA. Of the 12 leukorrhea samples without C. glabrata infection, 5/12 (41.67%) samples were diagnosed with other Candida strains (Table S1). Among the 632 leukorrhea samples without C. glabrata infection, 2 leukorrhea samples with no Candida infection and 2 leukorrhea samples with C. albicans infection were found to have C. glabrata by PCR-QDFA. For the remaining 595/602 (98.84%) leukorrhea samples without NAC strain infection, the diagnostic results of PCR-QDFA were consistent with the culture results. The sensitivity, specificity, and kappa value of PCR-QDFA for C. glabrata were 85.88%, 99.37% and 0.89, respectively (Table 2).
A total of 16/717 (2.23%) leukorrhea samples with C. tropicalis infection were diagnosed by culture. C. tropicalis strains of 13/16 (81.25%) leukorrhea samples were identified by PCR-QDFA. Of the remaining 3 leukorrhea samples with C. tropicalis strains infection, only one C. albicans strain was diagnosed by PCR-QDFA. Among 368 leukorrhea samples with other Candida strains, 1 C. glabrata strain and 1 C. albicans strain were found to be C. tropicalis strains by PCR-QDFA (Table S2). For the remaining 699/701 (99.71%) leukorrhea samples without C. tropicalis strains infection, the diagnostic results of PCR-QDFA were consistent with the culture results. The sensitivity, specificity, and kappa values of PCR-QDFA for C. tropicalis strains were 81.25%, 99.71%, and 0.84, respectively (Table 2).
Among the 717 leukorrhea samples, 14 strains of C. krusei were identified by the Candida chromogenic culture method. Of these, PCR-QDFA diagnostic results were consistent with culture for 13/14 (92.86%) leukorrhea samples. In 703/717 (98.05%) leukorrhea samples without C. krusei infection, 3 strains of C. krusei were identified by PCR-QDFA (Table S2). For the remaining 700/703 (99.57%) of the leukorrhea samples without C. krusei infection, the diagnostic results of PCR-QDFA were consistent with the culture results. The sensitivity, specificity, and kappa values of PCR-QDFA for C. krusei strains were 92.86%, 99.57%, and 0.86, respectively (Table 2).
Discussion
PCR-QDFA, a fully automated VVC diagnostic method with high sensitivity and specificity, takes only approximately 4 h for its diagnosis time. This study was the first to evaluate the diagnostic performance of PCR-QDFA for common Candida strains in the leukorrhea samples from suspected VVC patients.
This retrospective study was designed to evaluate the diagnostic performance of PCR-QDFA for several Candida strains in leukorrhea samples from patients with suspected VVC. Several studies suggest that the clinical diagnosis of VVC should be made mainly based on clinical symptoms combined with WMM results, and only uncertain cases should require further ascertainment by culture.8 Of the 384 VVC positive patients in the study, only 69.27% were diagnosed by WMM. It has been reported that WMM with low sensitivity (48.50%) are prone to underdiagnosis of VVC.26 WMM, a diagnostic method that cannot distinguish strain species is difficult to meet the needs of clinical precision medicine. Interestingly, the diagnostic performance of PCR-QDFA for all Candida strains within the PCR-QDFA targets was comprehensively evaluated. Among the 384 VVC-positive leukorrhea samples diagnosed by Candida culture, 88.54% of the Candida strains could be identified by PCR-QDFA. The sensitivity of other molecular diagnostic techniques was no more than 83.3% for C. krusei strains.10,27 PCR-QDFA had higher sensitivity for C. krusei strains. The sensitivity of PCR-QDFA for C. albicans, C. tropicalis, C. glabrata, and C. krusei were 89.01%, 81.25%, 85.88%, and 92.86%, respectively. The specificity of the PCR-QDFA was above 99.00% for the different Candida species among the NAC strains. The kappa values of PCR-QDFA for C. albicans, C. tropicalis, C. glabrata, and C. krusei were 0.83, 0.84, 0.89, and 0.86, respectively. The kappa values were within the interval of 0.81–0.99 for all strains, indicating that the results of the PCR-QDFA identifications were almost perfectly consistent with the results of Candida strains culture.28 In addition, most of the operationally complex molecular diagnostic kits show lower sensitivity or specificity than PCR-QDFA.10,29 BD MAX™ The vaginal panel (MAX VP) is currently the only reported fully automated molecular diagnostic technique (FAMDT) applied to VVC. The judgment of the diagnostic results of MAX VP requires expensive fluorometric systems. Only 24 samples each time (approximately 3 h) can be diagnosed by MAX VP with high sensitivity (96.2%) and specificity (96.1%).10 PCR-QDFA is a new FAMDT for the identification of Candida species, which combines a multiplex PCR assay with quantum dot luminescence to transduce a signal. PCR-QDFA, a more efficient FAMDT than MAX VP, was able to diagnose 94 leukorrhea samples each time (approximately 4 h). Quantum dots (QDs), low toxicity and inexpensive nanomaterials, which often have strong and stable optical signals coupled with other components.30 The judgment of PCR-QDFA diagnostic results only requires human interpretation of the stable quantum dot fluorescence signal in the UV imager. The QD luminescence signals on the nylon membrane strips in the PCR-QDFA procedure were manually interpreted. Human observations may lead to the occurrence of false-positive results. The high sensitivity of PCR-QDFA was considered as the cause of 8.40% false-positive results. When molecular diagnostic techniques find Candida strains that are not later recoverable, clinical uncertainties may occur.27 Interestingly, all the patients with false-positive PCR-QDFA results were diagnosed with vaginitis by clinicians. 82.14% of these patients had symptoms related to VVC. And 46.43% of these patients showed vaginal itching. According to other literature, some clinical treatments are only able to reduce the expression of virulence factor genes (enzymes proteinase SAP5 and phospholipase PLB2) by 50–60%.31 Therefore, symptoms of patients with false-positive PCR-QDFA results may be caused by toxic factors of inactivated Candida strains or other pathogenic microorganisms.
In addition, the present study also has some limitations. Because the actual number of leucorrhea samples infected by several Candida strains during this study was too small, only a small number of leucorrhea samples infected by a variety of Candida strains were included in this study. For PCR-QDFA, the purity and concentration of the Candida strains DNA in the samples to be tested were strictly required to be 1.4~2.2 and 0.2–100 (ng/μL), respectively. Leukorrhea samples with false-negative results by PCR-QDFA may have been mainly due to insufficient concentration or purity of pathogen-specific genes in the leukorrhea samples to be tested. This prompts clinicians to be advised to increase the volume of leukorrhea samples from different patients as much as possible. The required DNA concentration and purity standards for PCR-QDFA of leukorrhea samples may need to be more precisely determined. Therefore, the correlation between the luminescence intensity of QDs on the nylon membrane strip and positive results should be further investigated. Additionally, the PCR-QDFA targets were insufficient to cover all infectious strains. Therefore, the PCR-QDFA targets need further optimization.
Conclusions
This study is the first to evaluate the diagnostic performance of PCR-QDFA for Candida strain identification in VVC. This study demonstrates that the diagnosis of suspected VVC patients with significant clinical symptoms needs to be aided by highly sensitive and specific PCR-QDFA techniques. PCR-QDFA, which requires only approximately 4 hours for the diagnosis of VVC, greatly complements the timeliness of the Candida culture diagnostic assay. Therefore, PCR-QDFA is capable of being used in VVC practice as a tool for Candida strain identification with excellent diagnostic performance.
Ethical Approval
We followed the revised Declaration of Helsinki when performing the study. The Zhejiang Provincial People’s Hospital Research Ethics Committee authorized the study. The ethical approval No. was QT2022297. Due to the fact that this was a retrospective study and patient data and medical records were collected anonymously, informed consent for inclusion was waived. Each participant was given a guarantee of privacy protection.
Acknowledgments
We thank Huali Yin and Wenyan Cao for their technical assistance.
Author Contributions
Wen-jia Fan, Jie Li and Lingxia Chen performed the experiments and wrote the manuscript. Wenhao Wu made important contributions to data analysis and interpretation. Hong-ying Pan, Xi Li, and Wei-hong Zhong conceived the idea, designed the study, and revised the manuscript. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Willems HME, Ahmed SS, Liu J, et al. Vulvovaginal candidiasis: a current understanding and burning questions. J Fungi. 2020;6(1):27. doi:10.3390/jof6010027
2. Parsapour H, Masoumi SZ, Shayan A, et al. Comparison of the effects of nika vaginal cream with clotrimazole cream on vaginal candidiasis symptoms: a randomized single-blind clinical trial. Iran J Nurs Midwifery Res. 2021;26(6):521–525. doi:10.4103/ijnmr.IJNMR_82_20
3. Cangui-Panchi SP, Ñacato-Toapanta AL, Enríquez-Martínez LJ, et al. Battle royale: immune response on biofilms - host-pathogen interactions. Curr Res Immunol. 2023;4:100057. doi:10.1016/j.crimmu.2023.100057
4. Cangui-Panchi SP, Ñacato-Toapanta AL, Enríquez-Martínez LJ, et al. Biofilm-forming microorganisms causing hospital-acquired infections from intravenous catheter: a systematic review. Curr Res Microb Sci. 2022;3:100175. doi:10.1016/j.crmicr.2022.100175
5. Atiencia-Carrera MB, Cabezas-Mera FS, Vizuete K, Debut A, Tejera E, Machado A. Evaluation of the biofilm life cycle between Candida albicans and Candida tropicalis. Front Cell Infect Microbiol. 2022;12:953168. doi:10.3389/fcimb.2022.953168
6. Atiencia-Carrera MB, Cabezas-Mera FS, Tejera E, et al. Prevalence of biofilms in Candida spp. bloodstream infections: a meta-analysis. PLoS One. 2022;17(2):e0263522. doi:10.1371/journal.pone.0263522
7. Sobel JD. Vulvovaginal candidosis. Lancet. 2007;369(9577):1961–1971. doi:10.1016/S0140-6736(07)60917-9
8. Farr A, Effendy I, Frey Tirri B, et al. Guideline: vulvovaginal candidosis (AWMF 015/072, level S2k). Mycoses. 2021;64(6):583–602. doi:10.1111/myc.13248
9. Fernandes Â, Azevedo N, Valente A, et al. Vulvovaginal candidiasis and asymptomatic vaginal colonization in Portugal: epidemiology, risk factors and antifungal pattern. Med Mycol. 2022;60(5):myac029. doi:10.1093/mmy/myac029
10. Thompson A, Timm K, Borders N, et al. Diagnostic performance of two molecular assays for the detection of vaginitis in symptomatic women. Eur J Clin Microbiol Infect Dis. 2020;39(1):39–44. doi:10.1007/s10096-019-03694-w
11. Blostein F, Levin-Sparenberg E, Wagner J, Foxman B. Recurrent vulvovaginal candidiasis. Ann Epidemiol. 2017;27(9):575–582.e3. doi:10.1016/j.ajog.2015.06.067
12. Gonçalves B, Ferreira C, Alves CT, et al. Vulvovaginal candidiasis: epidemiology, microbiology and risk factors. Crit Rev Microbiol. 2016;42(6):905–927. doi:10.3109/1040841X.2015.1091805
13. Adjapong G, Hale M, Garrill A. A comparative investigation of azole susceptibility in Candida isolates from vulvovaginal candidiasis and recurrent vulvovaginal candidiasis patients in Ghana. Med Mycol. 2017;55(6):686–689. doi:10.1093/mmy/myw122
14. Jafari M, Salari S, Pakshir K, Zomorodian K. Exoenzyme activity and possibility identification of Candida dubliniensis among Candida albicans species isolated from vaginal candidiasis. Microb Pathog. 2017;110:73–77. doi:10.1016/j.micpath.2017.06.024
15. Otašević S, Momčilović S, Stojanović NM, et al. Non-culture based assays for the detection of fungal pathogens. J Mycol Med. 2018;28(2):236–248. doi:10.1016/j.mycmed.2018.03.001
16. Elbehiry A, Aldubaib M, Abalkhail A, et al. How MALDI-TOF mass spectrometry technology contributes to microbial infection control in healthcare settings. Vaccines. 2022;10(11):1881. doi:10.3390/vaccines10111881
17. Mendonça A, Santos H, Franco-Duarte R, Sampaio P. Fungal infections diagnosis-past, present and future. Res Microbiol. 2022;173(3):103915. doi:10.1016/j.resmic.2021.103915
18. Yadav S, Saxena AK, Capoor MR, Ramesh V. Comparison of direct microscopic methods using potassium hydroxide, periodic acid Schiff, and calcofluor white with culture in the diagnosis of onychomycosis. Indian J Dermatol Venereol Leprol. 2013;79(2):242–243. doi:10.4103/0378-6323.107649
19. Arvanitis M, Ziakas PD, Zacharioudakis IM, et al. PCR in diagnosis of invasive aspergillosis: a meta-analysis of diagnostic performance. J Clin Microbiol. 2014;52(10):3731–3742. doi:10.1128/JCM.01365-14
20. Li J, Fan W, Zou X, et al. Clinical evaluation of polymerase chain reaction coupled with quantum dot fluorescence analysis in the identification of bacteria and yeasts in patients with suspected bloodstream infections. Microb Biotechnol. 2023;16(4):827–837. doi:10.1111/1751-7915.14226
21. Schwebke JR, Gaydos CA, Nyirjesy P, et al. Diagnostic performance of a molecular test versus clinician assessment of vaginitis. J Clin Microbiol. 2018;56(6):e00252–18. doi:10.1128/JCM.00252-18
22. Kumar A, Sachu A, Mohan K, et al. Simple low cost differentiation of Candida auris from Candida haemulonii complex using CHROMagar Candida medium supplemented with Pal’s medium. Rev Iberoam Micol. 2017;34(2):109–111. doi:10.1016/j.riam.2016.11.004
23. Mulet Bayona JV, Salvador García C, Tormo Palop N, Gimeno Cardona C. Evaluation of a novel chromogenic medium for Candida spp. identification and comparison with CHROMagar™ Candida for the detection of Candida auris in surveillance samples. Diagn Microbiol Infect Dis. 2020;98(4):115168. doi:10.1016/j.diagmicrobio.2020.115168
24. Mulet Bayona JV, Salvador García C, Tormo Palop N, et al. Novel chromogenic medium CHROMagarTM candida plus for detection of Candida auris and other Candida Species from surveillance and environmental samples: a multicenter study. J Fungi. 2022;8(3):281. doi:10.3390/jof8030281
25. Dhamnetiya D, Jha RP, Shalini S, Bhattacharyya K. How to analyze the diagnostic performance of a new test? Explained with illustrations. J Lab Physicians. 2021;14(1):90–98. doi:10.1055/s-0041-1734019
26. Danby CS, Althouse AD, Hillier SL, et al. Nucleic acid amplification testing compared with cultures, gram stain, and microscopy in the diagnosis of vaginitis. J Low Genit Tract Dis. 2021;25(1):76–80. doi:10.1097/LGT.0000000000000576
27. Aguirre-Quiñonero A, Castillo-Sedano IS, Calvo-Muro F, et al. Accuracy of the BD MAX™ vaginal panel in the diagnosis of infectious vaginitis. Eur J Clin Microbiol Infect Dis. 2019;38(5):877–882. doi:10.1007/s10096-019-03480-8
28. Viera AJ, Garrett JM. Understanding interobserver agreement: the kappa statistic. Fam Med. 2005;37(5):360–363.
29. Trovato L, Domina M, Calvo M, et al. Use of real time multiplex PCR for the diagnosis of dermatophytes onychomycosis in patients with empirical antifungal treatments. J Infect Public Health. 2022;15(5):539–544. doi:10.1016/j.jiph.2022.03.019
30. Svechkarev D, Mohs AM. Organic fluorescent dye-based nanomaterials: advances in the rational design for imaging and sensing applications. Curr Med Chem. 2019;26(21):4042–4064. doi:10.2174/0929867325666180226111716
31. Alves F, de Oliveira Mima EG, Passador RCP, et al. Virulence factors of fluconazole-susceptible and fluconazole-resistant Candida albicans after antimicrobial photodynamic therapy. Lasers Med Sci. 2017;32(4):815–826. doi:10.1007/s10103-017-2177-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.