Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Clinical Characteristics of COPD Patients According to COPD Assessment Test (CAT) Score Level: Cross-Sectional Study
Authors Gil HI ![]() , Zo S
, Zo S ![]() , Jones PW
, Jones PW ![]() , Kim BG
, Kim BG ![]() , Kang N
, Kang N ![]() , Choi Y
, Choi Y ![]() , Cho HK, Kang D, Cho J, Park HY, Shin SH
, Cho HK, Kang D, Cho J, Park HY, Shin SH
Received 12 December 2020
Accepted for publication 4 May 2021
Published 1 June 2021 Volume 2021:16 Pages 1509—1517
DOI https://doi.org/10.2147/COPD.S297089
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Hyun-Il Gil,1,* Sungmin Zo,2,* Paul W Jones,3,4 Bo-Guen Kim,2 Noeul Kang,2 Yeonseok Choi,5 Hyun Kyu Cho,6 Danbee Kang,7 Juhee Cho,7 Hye Yun Park,2 Sun Hye Shin2
1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea; 2Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea; 3Institute For Infection and Immunity, St George’s University of London, London, UK; 4Value Evidence and Outcomes, Global Medical R&D, GlaxoSmithKline, Uxbridge, UK; 5Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Kyung Hee University School of Medicine, Seoul, Republic of Korea; 6Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Republic of Korea; 7Samsung Advanced Institute for Health Sciences & Technology (SAIHST), Sungkyunkwan University, Seoul, Republic of Korea
*These authors contributed equally to this work
Correspondence: Sun Hye Shin; Hye Yun Park
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
Tel +82-2-3410-3429
Fax +82-2-3410-3849
Email [email protected]; [email protected]
Purpose: The chronic obstructive pulmonary disease (COPD) assessment test (CAT) is widely used to assess the impact of COPD symptoms on health status. Whilst the CAT consists of eight different items, details on the distribution of each item are limited. This study aimed to investigate the distribution and clinical implication of each CAT item, stratified by CAT severity group, in stable COPD patients.
Patients and Methods: This was a cross-sectional study at a single referral hospital in South Korea. Spirometry confirmed COPD patients with CAT measured at the first clinical visit were retrospectively identified. Patients were categorized into three groups: low (0 ≤ CAT < 10), medium (10 ≤ CAT < 20), and high (20 ≤ CAT ≤ 40) impact group. For the purpose of this analysis, the first four items (cough, sputum, chest tightness, and dyspnea) and the remaining four items (activities, confidence, sleep and energy) were also grouped as “pulmonary” and “extra-pulmonary”, respectively.
Results: A total of 815 patients were included, and mean (SD) forced expiratory volume in 1 s (FEV1) was 62.8 (17.4) % pred. Among them, 300 patients (36.8%) were in the high impact group and had a greater exacerbation history and lower lung function. The proportion of “extra-pulmonary” items score was greater in patients with higher total CAT scores, with the activity and confidence items showing higher scores.
Conclusion: In our study, in addition to dyspnea, activity limitation is a particular problem in individual patients with higher CAT total scores, for which physicians need to pay more attention. Our study suggests that whilst CAT total score captures the overall impact of COPD, each item of the CAT contains potentially useful information in understanding the patient’s symptom burden.
Keywords: COPD, COPD assessment test, patient reported outcome, symptom
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent respiratory symptoms and airflow limitation.1 Whilst chronic cough and sputum being the common symptoms,2,3 exertional dyspnea is the most characteristic symptom of COPD that often restricts exercise capacity and activities of daily life of patients.4–6 Accordingly, patients with symptomatic COPD have reduced health-related quality of life, which leads to substantial socioeconomic burden.7 Thus, disease-specific health status questionnaires for comprehensive assessment of symptoms beyond dyspnea are recommended in COPD guidelines, including the St. George’s Respiratory Questionnaire (SGRQ)8 and the Chronic Respiratory Disease Questionnaire (CRQ).9 These tools are well validated and reliable but are too complex to implement in clinical practice.
The COPD assessment test (CAT) is an easy and simple measurement with an eight-item questionnaire including severity of cough, sputum, chest tightness, dyspnea, activities, confidence, sleep, and energy.10–12 It is widely used in daily practice to assess and quantify the impacts of COPD symptoms on the health status, and correlates well with the SGRQ score in clinically stable COPD patients.12 It is one of the key determinants in assessing disease severity and guiding treatment in Global Initiative for Chronic Obstructive Lung Disease (GOLD) report.1 Furthermore, a significant increase in CAT total score at a clinic visit is useful to detect worsening or exacerbation of COPD.13,14
Previous studies on CAT mostly focused on total score,10–12 rather than each item of CAT. A few have investigated single CAT items with regard to COPD screening,15 phenotypes,16,17 comorbidities,18,19 emphysema,18 and fatigue.2 However, studies on the distribution and clinical significance of single items in CAT based on CAT total scores are lacking. Therefore, we aimed to evaluate the distribution and clinical implication of each item of CAT according to the total CAT score of stable COPD patients.
Materials and Methods
Study Population
This is a cross-sectional study. Consecutive COPD patients were selected from the CLUE (COPD LUng Evolution) registry, an ongoing cohort at Samsung Medical Center (a 1979-bed referral hospital in Seoul, South Korea) that consists of the patients who have post bronchodilator forced expiratory volume in 1 second (FEV1) over forced vital capacity (FVC) less than 0.7 with age over 40 years. Between January 2016 and April 2019, 875 COPD patients who were enrolled into the registry and measured CAT were retrospectively identified. We excluded 31 patients who experienced acute exacerbation on the day of study visit, 17 patients who had a pulmonary resection or endobronchial valve insertion and 12 patients without matchable spirometry results. The final sample included 815 patients (Figure 1). For this cross-sectional study, data of the first visit were used. The Institutional Review Board of Samsung Medical Center approved this study (No. 2019–09-071-001) and the requirement for informed consent was exempted as this study was a retrospective analysis of the de-identified data that was routinely collected during clinical practice.
 |
Figure 1 Flowchart of study population. |
COPD Assessment Test
The CAT consists of eight items including cough, sputum, chest tightness, dyspnea, activities, confidence, sleep and energy. Item scores range from 0 to 5 points resulting in a total CAT score ranging from 0 to 40 points.11 Based on CAT total scores, patients were categorized into three groups: low (0 ≤ CAT < 10), medium (10 ≤ CAT < 20), and high (20 ≤ CAT ≤ 40) impact group according to CAT users guide (http://www.catestonline.org). In this study, the first four items (cough, sputum, chest tightness, and dyspnea) were grouped pragmatically, based on their content, into “pulmonary items” whilst the remaining four items (activities, confidence, sleep and energy) were grouped as “extra-pulmonary items”.20
Data Collection and Measurements
Data obtained from the CLUE cohort database included age, sex, smoking history, body mass index (BMI), modified medical research council (mMRC) dyspnea scale, COPD assessment test (CAT) score, history of acute exacerbation, and Charlson comorbidity index (CCI).21 Acute exacerbation was defined as an outpatient clinic visit, hospitalization or an emergency room visit owing to one or more of the following: worsening of dyspnea, increased sputum volume and purulent sputum. In this study, we collected the history of moderate to severe exacerbation in the previous year, which was routinely recorded as the structured form during clinic visit.
Spirometry, diffusing capacity of the lung for carbon monoxide (DLco), and lung volumes were performed using a Vmax 22 system (SensorMedics, Yorba Linda, CA, USA) according to American Thoracic Society/European Respiratory Society criteria.22,23 Absolute values of FEV1 and FVC were obtained and the percentages of predicted FEV1 and FVC were calculated using a reference from a representative Korean sample.24 Absolute DLco values (mL/mmHg/min) was obtained using the same apparatus and calculated into the percentage of predicted values using a formula based on a representative Korean sample.25 Moderate to severe decrease in DLco was defined as DLco ≤ 60% pred26 and hyperinflation was defined as residual volume (RV)/total lung capacity (TLC) > 40%.27
Validation Cohort
To validate the findings from the current study, data from a multicenter cohort of COPD patients were used. In brief, the Korean COPD Subgroup Study (KOCOSS) is an ongoing, multicenter observational cohort study, which has recruited COPD patients from referral hospitals in South Korea since December 2011. Patients who were diagnosed with COPD by a pulmonologist, aged ≥ 40 years, had a post-bronchodilator FEV1/FVC < 0.7, and showed respiratory symptoms were included. For this study, we used the data of 2181 patients who were enrolled from January 2012 to December 2019. After excluding those who missed CAT (n = 19), a total of 2162 patients were analyzed.
Statistical Analysis
Although the CAT was developed to be unidimensional with no subdomains,11 for the purpose of this descriptive analysis, the items were grouped into two groups based on the face-validity of items that appear to be related. In addition, to provide a continuous estimate of increasing pattern of each CAT item according to the total CAT score, we used locally weighted scatterplot smoothing (Figure 2). We then analyzed the patients grouped by overall CAT impact score using the recommended banding (http://www.catestonline.org).
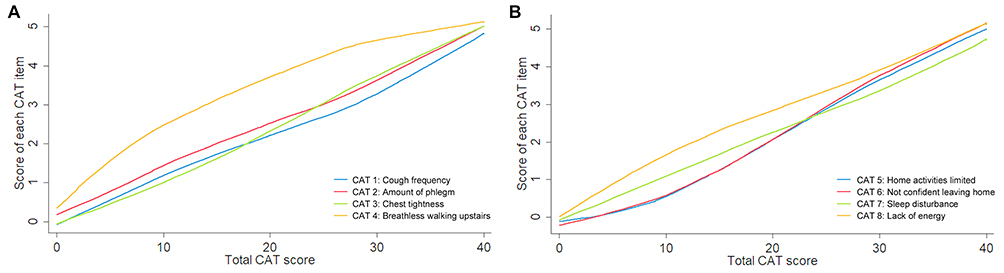 |
Figure 2 Different increasing pattern of each CAT items according to total CAT score. (A) Pulmonary items (cough, sputum, chest tightness and dyspnea) and (B) Extra-pulmonary items (activities, confidence, sleep and energy). |
All data are presented as numbers (%) for categorical variables and means (standard deviation) for continuous variables. Categorical variables were compared using the Pearson chi-square test or Fisher’s exact test, whilst the Student’s t-test was used to compare continuous variables. To test for linear trends, the group category was included as a continuous variable in the regression models. All tests were two-sided, and p-values < 0.05 were considered significant. All analyses were performed using Stata software (ver. 14.0; Stata Corporation, College Station, TX, USA).
Results
The baseline characteristics of 815 patients included in the analysis are summarized in Table 1. The mean age was 72.1 (standard deviation 8.9) years and most patients were male (90.9%). According to the baseline CAT score, 182 (22.3%), 333 (40.9%) and 300 (36.8%) patients were categorized as low, medium and high impact, respectively. The median age and male predominance were similar across the groups, whereas prevalence of current smokers increased from less symptomatic to highly symptomatic group. The high impact group also had a lower BMI, more dyspnea and higher rate of previous exacerbations compared to the other groups. There was no significant trend in comorbidities across three groups. Table 2 shows the baseline pulmonary function of each group; post-bronchodilator FEV1, DLco, and RV/TLC showed worsening trend with higher CAT score.
 |
Table 1 Baseline Characteristics of Patients According to Total CAT Score Groups |
 |
Table 2 Baseline Pulmonary Function Parameters of Patients According to Total CAT Score Groups |
The proportional contribution of the four “pulmonary” items (cough, sputum, chest tightness and dyspnea) and four “extra-pulmonary” items (activities, confidence, sleep and energy) to the total CAT score are presented, split by impact severity group, in Figure 3. The proportion of extra-pulmonary item scores was progressively greater with higher overall CAT total score, whilst that of pulmonary symptoms decreased accordingly.
 |
Figure 3 Proportion contribution of four pulmonary items (cough, sputum, chest tightness and dyspnea) and four extra-pulmonary items (activities, confidence, sleep and energy) to the total CAT score, according to impact severity group. *Four patients had zero score in CAT. |
Figure 4 further demonstrates the distribution of mean score for each CAT item. Dyspnea was the most predominant symptom overall, and the rest of the “pulmonary” items were proportionately higher with total CAT scores. In contrast, the “extra-pulmonary” items, particularly activities and confidence showed sharp increment between moderate impact group and high impact group. The absolute values of each CAT item are available in Supplementary Table E1. In addition, this pattern of deterioration of extra-pulmonary impacts was similar between patients with FEV1 < 50% pred (n = 179) and those with FEV1 ≥ 50% pred (n =636) (Supplementary Figure 1) and between patients with DLco ≤ 60% pred (n =241) and those with DLco > 60% pred (n =350) (Supplementary Figures 2).
 |
Figure 4 Distribution of mean score for each CAT items according to impact severity group (absolute values are available in supplementary table E1). |
Discussion
In this study, we found that patients with high impact CAT scores (≥ 20) were more likely to be current smokers, have more dyspnea and previous exacerbation history and have lower lung function and BMI. In a further analysis on the distribution of each CAT item according to total CAT score categories, the proportion of “pulmonary” items score was much higher than that of “extra-pulmonary” items in patients with mild impact. However, the proportion of “extra-pulmonary” items score was markedly higher in the high impact group. We also found that CAT items about activities and confidence were most severely influenced in the high impact group, and the pattern was similar in subgroups categorized by FEV1 50% pred or DLco 60% pred.
Beyond the total CAT score, we elaborated the distribution and clinical significance of each component of CAT. Compared to patients with lower total CAT scores, in patients with high impact (CAT scores ≥ 20), the proportional contribution of “pulmonary” items to the total score was less whilst the contribution of “extra-pulmonary” items increased up to 48.0%. When each of 8 items was analyzed separately, the “pulmonary” item scores were proportionally higher across the impact groups, whilst “extra-pulmonary” items showed a bigger step increase with higher total CAT scores. This was seen particularly with the activities and confidence items. A similar observation was made during the development of the CAT showing that “confidence” better distinguished more severe patients.11 Our finding highlights that limitation in physical activity plays a major role in impaired quality of life in high impact group. Whilst clinicians usually focus more on patients’ respiratory symptoms and pharmacological treatment during routine practice, our results suggest that CAT items can detect patients who suffer from deteriorated physical activities, particularly before they become highly symptomatic in terms of total CAT scores. In this regard, clinicians should pay more attention to “extra-pulmonary” symptoms and seek individualized and comprehensive interventions, such as pulmonary rehabilitation.
Our findings are consistent with previous studies, which reported that CAT score correlates with diverse clinical features of COPD. Several studies have reported that the increased CAT score is associated with dyspnea28,29 and acute exacerbation state or its future risk.11–13,29–31 Whilst it is known that FEV1 has a weak correlation with CAT score,12,28 several studies have shown a correlation between total CAT scores and GOLD grades.12,29 In our study, we also found a correlation between total CAT scores and the degree of airflow limitation and DLco. However, it is of note that one third of patients with FEV1 < 50% pred had CAT score < 20, whereas one third of patients with FEV1 ≥ 50% pred had CAT score ≥ 20. As shown in the Supplementary Figure 1, patients had different degrees of airflow limitation but showed visually similar distribution of each item of CAT when total CAT score was <20. This shows that FEV1 does not fully reflect the impact of COPD, emphasizing that FEV1 does not say it all.28
COPD is a systemic disease not only affecting the lungs but also having non-respiratory manifestations, including skeletal muscle dysfunction with atrophy and weakness, systemic inflammation and nutritional depletion.32,33 Our study showed the association between high CAT scores and a lower BMI, which is a surrogate marker of cachexia.34 GOLD also recommends that nutritional supports should be provided to malnourished COPD patients, which can improve overall quality of life.1,35 Similarly, the higher prevalence of smoking exposure among subjects with high CAT score might partly explain the effect of systemic inflammation on their extra-pulmonary manifestations. These findings suggest that patient reported outcomes are essential component in understanding this complex disease and achieving the goal of reducing symptom burden and improving quality of life, by non-pharmacological and pharmacological therapies.
Our study had several limitations. First, this is a retrospective analysis of data from a single referral center, which limits its generalizability. To address this limitation, we performed the same analysis using the data of 2162 patients from the KOCOSS cohort. As shown in Figure 5 and Supplementary Table E1, the pattern of deterioration of CAT items was very similar in both cohorts (except for sleep). The clinical characteristics of KOCOSS patients were summarized in Supplementary Table E2. Second, our patient cohort showed a marked male predominance (> 90%) which has been consistently reported in multicenter studies from Korea that are based on pulmonology clinics.36,37 This is due to a selection bias, as the male predominance was lesser in national survey.38 In part, this is attributable to a very low female smoking rate (3.4%) in Korea.39 However, there was no gender difference in CAT scores in previous studies.12,40 Third, due to the cross-sectional nature, we could not investigate the impact of each CAT items on clinical outcomes, such as future exacerbation or response to treatments. Further longitudinal studies with serially measured CAT are necessary to better understand the clinical utility of CAT in daily practice. Fourth, as we restricted the study population to stable COPD patients, we carefully reviewed and excluded patients who experienced acute exacerbation on the study visit (who were prescribed systemic steroids or referred to emergency department after clinic visit). However, co-existence of clinical instability caused by other disease could not be completely excluded. Lastly, although there was no significant association between CCI and CAT total scores in our study, we lacked information on patients’ mental health. In the analysis using KOCOSS data (Supplementary Table E2), there were more patients with depressive disorder (defined as a Beck Depression Inventory ≥ 16 or more)41 in high impact group. It is known that depression and anxiety are associated with high CAT scores, especially with the extra-pulmonary items.19 Depression was also correlated with SGRQ score, particularly with impact and activity domain.42 Thus, psychological problem may have contributed to the greater increase of extra-pulmonary items in high impact group, which should also be addressed as part of the integrated patient care.
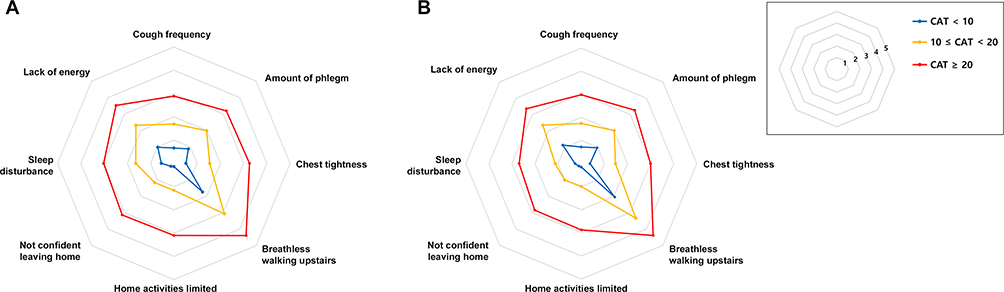 |
Figure 5 Distribution of mean score for each CAT items according to impact severity group in (A) CLUE registry (the present study, N = 815) and (B) KOCOSS cohort (multicenter cohort for validation, N = 2162). |
Conclusion
Using the CAT total scores and distribution of individual items of CAT, we found that dyspnea is the most prominent symptom in all patient groups regardless of total impact categories. Whilst dyspnea increased proportionally with worsening impact of COPD, CAT items regarding activities and confidence showed a sharp deterioration when patients became highly impacted (CAT total score ≥ 20). This novel insight suggests a new look into CAT items such that clinicians need to pay more attention to patients’ activities beyond dyspnea and seek a comprehensive intervention.
Abbreviations
BMI, body mass index; CAT, COPD assessment test; CCI, Charlson comorbidity index; COPD, chronic obstructive pulmonary disease; CRQ, Chronic Respiratory Disease Questionnaire; DLco, diffusing capacity of carbon monoxide of the lung; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, modified medical research council; RV, residual volume; SGRQ, St. George’s Respiratory Questionnaire; TLC, total lung capacity.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding authors (Dr Sun Hye Shin or Hye Yun Park) in response to reasonable requests.
Ethics Approval
This study was approved by the Institutional Review Board of Samsung Medical center and the requirement for informed consent was exempted given the retrospective nature of the study.
Acknowledgments
Hyun-Il Gil and Sungmin Zo are co-first authors of this study. Hye Yun Park and Sun Hye Shin contributed equally as lead authors and supervised the work.
Funding
Development of the COPD Assessment Test (CAT) was funded by GlaxoSmithKline. COPD Assessment Test and its associated CAT logo are trademarks of the GlaxoSmithKline group of companies © 2009 GlaxoSmithKline. All rights are reserved. This work was supported by the Research Program funded Korea National Institute of Health (Fund CODE 2016ER670100, 2016ER670101, 2016ER670102, 2018ER67100, 2018ER67101, 2018ER67102 and 2021ER120500).
Disclosure
Paul W. Jones is an employee and shareholder of GlaxoSmithKline. He received no fees or honorarium for writing this paper. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. Report. 2020. Available from: www.goldcopd.org.
2. Stridsman C, Svensson M, Johansson Strandkvist V, Hedman L, Backman H, Lindberg A. The COPD Assessment Test (CAT) can screen for fatigue among patients with COPD. Ther Adv Respir Dis. 2018;12:1753466618787380. doi:10.1177/1753466618787380
3. Waatevik M, Skorge TD, Omenaas E, Bakke PS, Gulsvik A, Johannessen A. Increased prevalence of chronic obstructive pulmonary disease in a general population. Respir Med. 2013;107(7):1037–1045. doi:10.1016/j.rmed.2013.04.008
4. O’Donnell DE, Elbehairy AF, Faisal A, Webb KA, Neder JA, Mahler DA. Exertional dyspnoea in COPD: the clinical utility of cardiopulmonary exercise testing. Eur Respir Rev. 2016;25(141):333–347. doi:10.1183/16000617.0054-2016
5. Hajiro T, Nishimura K, Tsukino M, Ikeda A, Oga T, Izumi T. A comparison of the level of dyspnea vs disease severity in indicating the health-related quality of life of patients with COPD. Chest. 1999;116(6):1632–1637. doi:10.1378/chest.116.6.1632
6. Lahaije AJ, van Helvoort HA, Dekhuijzen PN, Heijdra YF. Physiologic limitations during daily life activities in COPD patients. Respir Med. 2010;104(8):1152–1159. doi:10.1016/j.rmed.2010.02.011
7. Miravitlles M, Ribera A. Understanding the impact of symptoms on the burden of COPD. Respir Res. 2017;18(1):67. doi:10.1186/s12931-017-0548-3
8. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation. The St. George’s Respiratory Questionnaire. Am Rev Respir Dis. 1992;145(6):1321–1327. doi:10.1164/ajrccm/145.6.1321
9. Rutten-van Mölken M, Roos B, Van Noord J. An empirical comparison of the St George’s Respiratory Questionnaire (SGRQ) and the Chronic Respiratory Disease Questionnaire (CRQ) in a clinical trial setting. Thorax. 1999;54(11):995–1003. doi:10.1136/thx.54.11.995
10. Jones P, Harding G, Wiklund I, Berry P, Leidy N. Improving the process and outcome of care in COPD: development of a standardised assessment tool. Prim Care Respir J. 2009;18(3):208–215. doi:10.4104/pcrj.2009.00053
11. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
12. Jones PW, Brusselle G, Dal Negro RW, et al. Properties of the COPD assessment test in a cross-sectional European study. Eur Respir J. 2011;38(1):29–35. doi:10.1183/09031936.00177210
13. Kelly JL, Bamsey O, Smith C, et al. Health status assessment in routine clinical practice: the chronic obstructive pulmonary disease assessment test score in outpatients. Respiration. 2012;84(3):193–199. doi:10.1159/000336549
14. Pothirat C, Chaiwong W, Limsukon A, et al. Detection of acute deterioration in health status visit among COPD patients by monitoring COPD assessment test score. Int J Chron Obstruct Pulmon Dis. 2015;10:277–282. doi:10.2147/COPD.S76128
15. Raghavan N, Lam YM, Webb KA, et al. Components of the COPD Assessment Test (CAT) associated with a diagnosis of COPD in a random population sample. Copd. 2012;9(2):175–183. doi:10.3109/15412555.2011.650802
16. Chai CS, Liam CK, Pang YK, et al. Clinical phenotypes of COPD and health-related quality of life: a cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2019;14:565–573. doi:10.2147/COPD.S196109
17. Yoo SH, Lee JH, Yoo KH, Jung KS, Rhee CK. Different pattern of chronic obstructive pulmonary disease assessment test score between chronic bronchitis and non-chronic bronchitis patients. Tuberc Respir Dis (Seoul). 2018;81(3):228–232. doi:10.4046/trd.2017.0088
18. Marietta von Siemens S, Alter P, Lutter JI, et al. CAT score single item analysis in patients with COPD: results from COSYCONET. Respir Med. 2019;159(105810):105810. doi:10.1016/j.rmed.2019.105810
19. Miyazaki M, Nakamura H, Chubachi S, et al. Analysis of comorbid factors that increase the COPD assessment test scores. Respir Res. 2014;15(1):13. doi:10.1186/1465-9921-15-13
20. Houben-Wilke S, Janssen DJA, Franssen FME, Vanfleteren L, Wouters EFM, Spruit MA. Contribution of individual COPD assessment test (CAT) items to CAT total score and effects of pulmonary rehabilitation on CAT scores. Health Qual Life Outcomes. 2018;16(1):205. doi:10.1186/s12955-018-1034-4
21. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251. doi:10.1016/0895-4356(94)90129-5
22. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
23. American Thoracic Society. Single-breath carbon monoxide diffusing capacity (transfer factor). Recommendations for a standard technique–1995 update. Am J Respir Crit Care Med. 1995;152(6 Pt 1):2185–2198. doi:10.1164/ajrccm.152.6.8520796
24. Choi JK, Paek D, Lee JO. Normal predictive values of spirometry in Korean population. Tuberc Respir Dis. 2005;58(3):230–242. doi:10.4046/trd.2005.58.3.230
25. Park J, Choi I, Park K. Normal predicted standards of single breath carbon monoxide diffusing capacity of lung in healthy nonsmoking adults. Korean J Intern Med. 1985;28:176–183.
26. Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948–968. doi:10.1183/09031936.05.00035205
27. Albuquerque AL, Nery LE, Villaça DS, et al. Inspiratory fraction and exercise impairment in COPD patients GOLD stages II–III. Eur Respir J. 2006;28(5):939–944. doi:10.1183/09031936.06.00040506
28. Kostikas K, Greulich T, Mackay AJ, et al. Treatment response in COPD: does FEV(1) say it all? A post hoc analysis of the CRYSTAL study. ERJ Open Res. 2019;5:1. doi:10.1183/23120541.00243-2018
29. Agustí A, Soler JJ, Molina J, et al. Is the CAT questionnaire sensitive to changes in health status in patients with severe COPD exacerbations? COPD. 2012;9(5):492–498. doi:10.3109/15412555.2012.692409
30. Mackay AJ, Donaldson GC, Patel AR, Jones PW, Hurst JR, Wedzicha JA. Usefulness of the chronic obstructive pulmonary disease assessment test to evaluate severity of COPD exacerbations. Am J Respir Crit Care Med. 2012;185(11):1218–1224. doi:10.1164/rccm.201110-1843OC
31. Mackay AJ, Kostikas K, Roche N, et al. Impact of baseline symptoms and health status on COPD exacerbations in the FLAME study. Respir Res. 2020;21(1):93. doi:10.1186/s12931-020-01354-8
32. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):1165–1185. doi:10.1183/09031936.00128008
33. Celli BR, Locantore N, Tal-Singer R, et al. Emphysema and extrapulmonary tissue loss in COPD: a multi-organ loss of tissue phenotype. Eur Respir J. 2018;51(2). doi:10.1183/13993003.02146-2017
34. McDonald MN, Wouters EFM, Rutten E, et al. It’s more than low BMI: prevalence of cachexia and associated mortality in COPD. Respir Res. 2019;20(1):100. doi:10.1186/s12931-019-1073-3
35. Ferreira IM, Brooks D, White J, Goldstein R. Nutritional supplementation for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:Cd000998. doi:10.1002/14651858.CD000998.pub3
36. Lee JY, Chon GR, Rhee CK, et al. Characteristics of patients with chronic obstructive pulmonary disease at the first visit to a pulmonary medical center in Korea: the KOrea COpd Subgroup Study Team Cohort. J Korean Med Sci. 2016;31(4):553–560. doi:10.3346/jkms.2016.31.4.553
37. Park TS, Lee JS, Seo JB, et al. Study design and outcomes of Korean Obstructive Lung Disease (KOLD) Cohort Study. Tuberc Respir Dis (Seoul). 2014;76(4):169–174. doi:10.4046/trd.2014.76.4.169
38. Hwang YI, Park YB, Yoo KH. Recent trends in the prevalence of chronic obstructive pulmonary disease in Korea. Tuberc Respir Dis (Seoul). 2017;80(3):226–229. doi:10.4046/trd.2017.80.3.226
39. OECD. Daily smokers (indicator). 2021. doi: 10.1787/1ff488c2-en.
40. Varol Y, Anar C, Çimen P, Ünlü M, Halilçolar H, Güçlü SZ. Sex-related differences in COPD assessment test scores of COPD populations with or without significant anxiety and/or depression. Turk J Med Sci. 2017;47(1):61–68. doi:10.3906/sag-1509-60
41. Huffman JC, Doughty CT, Januzzi JL, Pirl WF, Smith FA, Fricchione GL. Screening for major depression in post-myocardial infarction patients: operating characteristics of the Beck Depression Inventory-II. Int J Psychiatry Med. 2010;40(2):187–197. doi:10.2190/PM.40.2.e
42. Hynninen MJ, Pallesen S, Nordhus IH. Factors affecting health status in COPD patients with co-morbid anxiety or depression. Int J Chron Obstruct Pulmon Dis. 2007;2(3):323–328.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.