Back to Journals » International Journal of Women's Health » Volume 18
Clinical Characteristics, Management, and Perinatal Outcomes of Third-Trimester Preeclampsia at a Tertiary Hospital in Vietnam: A Retrospective Descriptive Study
Authors Nguyen KT ![]() , Bui TTT
, Bui TTT ![]() , To NTH, Phan QN
, To NTH, Phan QN ![]() , Dang NB, Le CTK, Tran NH
, Dang NB, Le CTK, Tran NH ![]()
Received 24 April 2026
Accepted for publication 16 June 2026
Published 18 June 2026 Volume 2026:18 619528
DOI https://doi.org/10.2147/IJWH.S619528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Kien Trung Nguyen,1 Tuyen Thi Thanh Bui,1 Nhung Thi Hong To,2 Quang Ngoc Phan,3 Ngoc Bao Dang,4 Chung Thi Kim Le,5 Nam Hoang Tran6
1Department of Obstetrics and Gynecology, Thai Binh University of Medicine and Pharmacy, Hung Yen, Vietnam; 2Tam Anh General Hospital, Hanoi, Vietnam; 3The Center Service for Technology Science of Medi-Phar, Thai Binh University of Medicine and Pharmacy, Hung Yen, Vietnam; 4General Planning Department, Sun Group International Hospital, Hanoi, Vietnam; 5Institute for Preventive Medicine and Public Health, Hanoi Medical University, Hanoi, Vietnam; 6International Center, Tokushima University, Tokushima, Japan
Correspondence: Nam Hoang Tran, International Center, Tokushima University, Tokushima, Japan, Email [email protected]
Purpose: To describe the clinical and laboratory characteristics of third-trimester preeclampsia, summarize management patterns, and identify factors associated with adverse neonatal outcomes at a single public tertiary referral obstetrics and gynecology hospital in Vietnam.
Patients and Methods: This retrospective descriptive study included 154 pregnant women diagnosed with preeclampsia and delivered at a single public tertiary referral obstetrics and gynecology hospital in Vietnam between August 1, 2022 and July 31, 2023. Clinical, laboratory, treatment, delivery, and neonatal data were analyzed using descriptive statistics and logistic regression. The composite adverse neonatal outcome was defined as the presence of one or more of the following: fetal growth restriction, preterm birth, intrauterine fetal death, low birth weight, neonatal respiratory morbidity, neonatal transfer, or perinatal death.
Results: Severe preeclampsia accounted for 57.1% of cases. Maternal age ≥ 35 years was associated with severe disease (OR 3.00, 95% CI 1.56– 5.85), as were primigravidity (OR 1.98, 95% CI 1.03– 3.78), prior stillbirth (OR 2.94, 95% CI 1.10– 7.80), and assisted conception in the index pregnancy (OR 3.35, 95% CI 1.20– 9.36). Elevated liver enzymes, hypoalbuminemia, hyperuricemia, and elevated urea were more frequent in severe preeclampsia. All women with severe preeclampsia underwent cesarean delivery; the overall cesarean rate was 81.2%. Preterm birth occurred in 35.7% of pregnancies and fetal growth restriction in 10.4%. In multivariable analysis, adverse neonatal outcomes were associated with maternal age > 35 years (adjusted OR 2.24), gestational age < 34 weeks (adjusted OR 8.77), albumin < 35 g/L (adjusted OR 3.24), serum uric acid ≥ 400 umol/L (adjusted OR 3.93), severe hypertension (adjusted OR 2.29), and <=1 day of medical management before delivery (adjusted OR 9.34).
Conclusion: Third-trimester preeclampsia at a public tertiary obstetrics and gynecology hospital in Vietnam was characterized by a high proportion of severe cases and a very high cesarean delivery rate. Older maternal age, primigravidity, assisted conception, severe hypertension, hyperuricemia, and hypoalbuminemia were associated with worse maternal or neonatal profiles. Earlier gestational age at birth remained the strongest predictor of adverse neonatal outcomes.
Plain Language Summary: Preeclampsia is a serious condition in pregnancy that causes high blood pressure and can affect the mother’s organs and the baby’s health. It can lead to problems such as preterm birth, poor fetal growth, and in severe cases, life-threatening complications for both mother and baby. This study looked at 154 pregnant women with preeclampsia in the third trimester who were treated at a major public tertiary obstetrics and gynecology hospital in Vietnam. More than half of the women had severe preeclampsia. Cesarean section was very common, especially in severe cases. Many babies were born too early, and some had growth problems. The study also found that worse neonatal outcomes were more likely when the mother was older than 35 years, the baby was delivered before 34 weeks of pregnancy, the mother had severe high blood pressure, or blood tests showed low albumin or high uric acid levels. A very short time between hospital treatment and delivery was also linked with poorer neonatal outcomes. These findings show that preeclampsia remains a major challenge in maternal care. Early detection, close monitoring, timely referral, and careful delivery planning may help reduce risks for both mothers and babies, especially in referral hospitals and lower-resource settings.
Keywords: hypertensive disorders of pregnancy, maternal outcomes, neonatal outcomes, cesarean delivery, uric acid
Introduction
Preeclampsia remains one of the leading causes of maternal and perinatal morbidity and mortality worldwide.1–4 It is a multisystem pregnancy disorder that typically arises after 20 weeks of gestation and is defined by new-onset hypertension accompanied by maternal organ dysfunction and/or uteroplacental dysfunction.4–7 The disease may progress rapidly to severe maternal complications, including eclampsia, stroke, pulmonary edema, renal impairment, hepatic dysfunction, and death, and is strongly associated with fetal growth restriction, preterm birth, low birth weight, and stillbirth.1,2,4,6 In low- and middle-income settings, these risks are further magnified by delayed recognition and referral, inconsistent antenatal surveillance, and limited maternal and neonatal care capacity, which can increase the probability of preventable maternal and perinatal complications.8–10
The epidemiology and clinical presentation of preeclampsia vary across populations and healthcare settings.3,4,8,11 Previous studies, systematic reviews, and clinical guidelines have consistently identified advanced maternal age, nulliparity, obesity, multifetal gestation, preexisting medical disorders such as chronic hypertension, diabetes, and kidney disease, prior preeclampsia or other adverse obstetric history, family history of chronic illness, smoking exposure, and assisted reproductive technology as important risk factors for preeclampsia.4,6,12–15 Evidence from different regional settings also suggests that risk profiles vary by population structure, ethnicity, body mass index distribution, parity, and health-system context.11,16–19 However, local hospital-based data remain essential, particularly in low- and middle-income settings, because real-world outcomes are shaped not only by biological risk but also by referral pathways, timeliness of diagnosis, institutional management practices, and the availability of maternal and neonatal intensive care support.9,20 In this context, single-center studies can provide clinically meaningful evidence on how preeclampsia presents and is managed within specific health-system constraints, thereby informing more context-appropriate strategies for surveillance, referral, and perinatal care.9
In Vietnam, preeclampsia remains an important obstetric challenge within the broader burden of hypertensive disorders of pregnancy. Vietnam’s national reproductive health guideline recognizes hypertensive disorders in pregnancy as priority conditions requiring standardized antenatal detection, severity assessment, referral, and delivery management.21 Recent Vietnamese data from the National Hospital of Obstetrics and Gynecology have shown that hypertensive disorders of pregnancy continue to be associated with substantial maternal and perinatal complications, including HELLP syndrome, placental abruption, eclampsia, preterm delivery, stillbirth, and perinatal mortality.22 More broadly, hypertensive disorders in pregnancy remain a major contributor to maternal mortality in Southeast Asia, alongside obstetric hemorrhage, underscoring the continuing regional relevance of timely diagnosis and effective management.23 Although Vietnam has made major progress in maternal health over recent decades, the World Health Organization has emphasized that preventable maternal and newborn complications still disproportionately affect women facing delays in access, gaps in quality of care, and resource constraints, particularly outside the highest-level urban centers.10 Against this background, contemporary provincial-level evidence is still relatively limited. A recent Vietnamese hospital-based study noted that published data from Vietnam remain sparse and that many available reports focus mainly on specific subgroups or single manifestations of hypertensive disease in pregnancy rather than providing a detailed picture of severity patterns, delivery management, and maternal–neonatal outcomes across referral settings.22 For this reason, data from a major public tertiary obstetrics and gynecology hospital at the provincial level are especially valuable. Such hospitals do not only provide routine obstetric care; they also receive women transferred for severe hypertension, suspected preeclampsia, fetal compromise, and threatened preterm birth, meaning that their case mix often reflects both the everyday burden of disease and the more complex end of the referral spectrum. Studying preeclampsia in this setting therefore offers a more practice-based understanding of how disease severity, timing of delivery, and available maternal and neonatal support interact to shape outcomes in real-world care, particularly in health systems where referral patterns and treatment capacity may differ from those of national centers or highly resourced urban hospitals.9,22
The study hospital primarily functions as a provincial tertiary referral center, receiving both routine obstetric cases and referrals of women with suspected or confirmed severe preeclampsia, fetal compromise, threatened preterm birth, and other high-risk obstetric conditions from lower-level facilities within the province and surrounding areas. This referral role is important for interpreting the severity distribution, delivery decisions, and intervention rates observed in the cohort. Therefore, this study was conducted to characterize the clinical and laboratory features of third-trimester preeclampsia, describe patterns of medical management and delivery decision-making, and evaluate factors associated with adverse neonatal outcomes in a retrospective hospital-based study.
Material and Methods
Study Design and Setting
This retrospective descriptive study used clinical data from pregnant women with preeclampsia who delivered at a major public tertiary obstetrics and gynecology hospital in Vietnam between August 1, 2022 and July 31, 2023.
Participants
Eligible participants were pregnant women diagnosed with preeclampsia who delivered at 28 weeks of gestation or later during the one-year study period. Preeclampsia was diagnosed according to the American College of Obstetricians and Gynecologists (ACOG) 2020 criteria. For severity classification, cases were categorized as preeclampsia with severe features or preeclampsia without severe features. Preeclampsia with severe features was defined by the presence of severe-range blood pressure and/or maternal organ dysfunction, including thrombocytopenia, impaired liver function, renal insufficiency, pulmonary edema, or persistent neurological or visual symptoms. Preeclampsia without severe features referred to cases meeting diagnostic criteria for preeclampsia but without any severe features.5–7 Local clinical management also followed the national reproductive health service guidance used in Vietnam during the study period.21 Women were excluded if they had chronic hypertension, hypertension before 20 weeks of gestation, pre-existing renal disease, chronic liver disease, heart disease, conditions substantially affecting uric acid metabolism, or exposure to medications likely to increase serum uric acid during pregnancy. Consecutive eligible cases were included to reduce selection bias and to reflect the real-world case mix of third-trimester preeclampsia at the study hospital. The minimum required sample size was 113, and the final sample included 154 women, exceeding the minimum sample size required for the primary descriptive objectives. A one-year study period was selected to capture a complete annual cycle of obstetric admissions while maintaining consistency in clinical management, referral patterns, laboratory procedures, and neonatal care practices.
Variables and Assessments
Data were retrospectively extracted from hospital medical records using a structured case report form and included maternal age, gravidity, body mass index, obstetric history, family history of preeclampsia, mode of conception, and multiple gestation. Clinical variables included blood pressure at presentation, edema, headache, visual disturbance, epigastric or right upper quadrant pain, oliguria, and gestational age at diagnosis.
Laboratory assessments included hemoglobin concentration, platelet count, aspartate aminotransferase, alanine aminotransferase, blood urea, serum creatinine, serum uric acid, serum albumin, and urinary protein. Fetal assessment was performed using obstetric ultrasonography and cardiotocography when clinically indicated. Management-related variables included duration of medical treatment before delivery, use of antihypertensive therapy, magnesium sulfate, antenatal corticosteroids for fetal lung maturation, albumin infusion, route of delivery, and indications for cesarean delivery.
The primary neonatal outcome was a composite adverse neonatal outcome, defined as the presence of one or more of the following: fetal growth restriction, preterm birth, intrauterine fetal death, low birth weight, neonatal respiratory morbidity, neonatal transfer, or perinatal death. Multivariable logistic regression was used to examine factors associated with this composite adverse neonatal outcome.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics version 28.0. Continuous variables were summarized as means and standard deviations, while categorical variables were presented as frequencies and percentages. Independent-samples t-tests were used to compare normally distributed continuous variables. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Multivariable logistic regression was performed to identify factors independently associated with the composite adverse neonatal outcome. Variables were selected for inclusion in the multivariable model based on clinical relevance, prior evidence, and significant or near-significant associations in univariable analysis. To avoid overfitting, the number of predictors was limited in relation to the sample size and number of outcome events. Multicollinearity was assessed before model construction, and variables with substantial collinearity were not entered simultaneously in the final model. Adjusted odds ratios with 95% confidence intervals were reported. Statistical significance was defined as a two-sided p value of <0.05. Because the composite adverse neonatal outcome included clinically related but heterogeneous events, the regression findings were interpreted as markers of overall neonatal risk rather than as predictors of any single neonatal complication.
Ethics
The study was approved by the Institutional Review Board of Thai Binh University of Medicine and Pharmacy (Approval No. 002211 on April 18, 2024). The approval covered the retrospective use, anonymization, analysis, and reporting of clinical data collected during routine hospital care between August 1, 2022 and July 31, 2023. No additional intervention or patient contact was conducted for the purpose of this analysis. Personal and clinical data were anonymized before analysis and handled confidentially. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Results
Participant Characteristics and Disease Severity
A total of 154 women with third-trimester preeclampsia were included in the final analysis. Of these, 88 women (57.1%) had severe preeclampsia and 66 women (42.9%) had preeclampsia without severe features. More than half of the participants were aged 35 years or older (53.2%) and were primigravid (56.5%). The most common body mass index category was 25.0–29.9 kg/m2, observed in 59.7% of the cohort. Most cases were diagnosed at 37 weeks of gestation or later (63.0%), while 14.9% were diagnosed before 34 weeks of gestation.
Severe preeclampsia was more frequent among women aged 35 years or older than among younger women (64.8% vs 37.9%). Primigravidity was also more common in the severe preeclampsia group than in the preeclampsia without severe features group (63.6% vs 47.0%). A history of stillbirth and assisted conception were also more frequently observed among women with severe disease. Baseline maternal and obstetric characteristics by preeclampsia severity are summarized in Table 1.
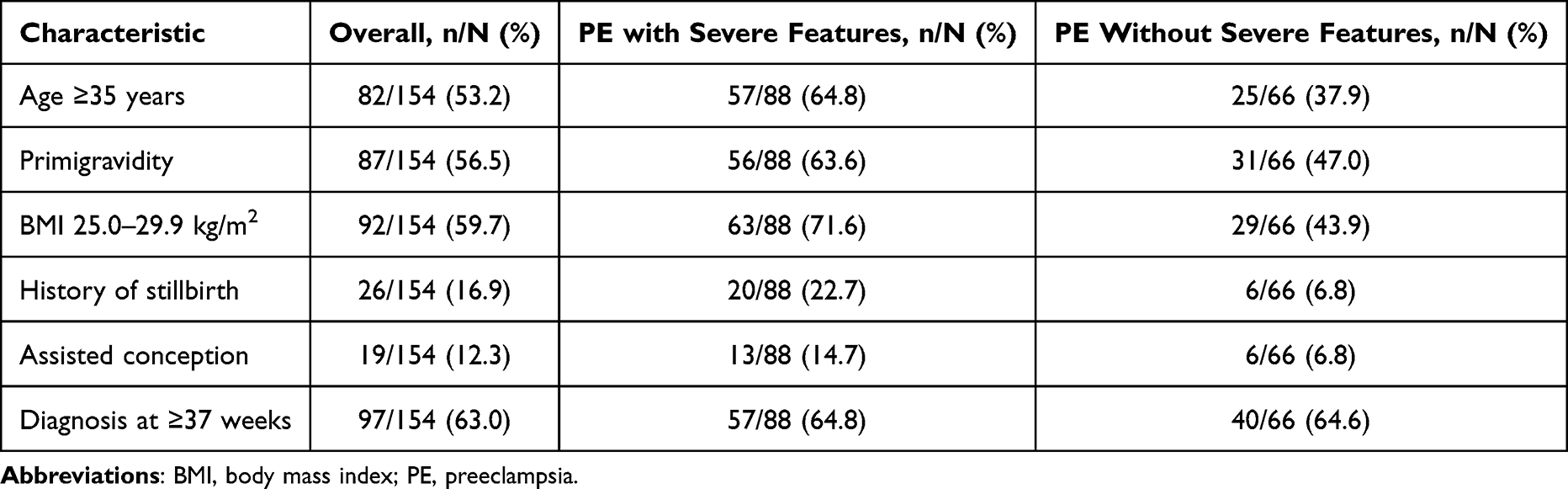 |
Table 1 Baseline Maternal Characteristics by Preeclampsia Severity (N=154) |
Clinical and Laboratory Findings
Among women with severe preeclampsia, headache was the most frequently reported severe symptom, followed by visual disturbance and epigastric pain. Edema was common in the overall cohort, and generalized edema was observed predominantly among women with severe disease.
Laboratory abnormalities were more frequent among women with severe preeclampsia. Elevated aspartate aminotransferase (AST ≥70 U/L) was observed in 35.2% of severe cases compared with 7.6% of cases without severe features. Similarly, elevated alanine aminotransferase (ALT ≥70 U/L) was present in 37.5% of severe cases and 10.6% of cases without severe features. Hyperuricemia, defined as serum uric acid ≥400 µmol/L, was also more common in severe preeclampsia than in preeclampsia without severe features (33.0% vs 15.2%). Hypoalbuminemia, defined as serum albumin <35 g/L, was frequent in both groups but was more common among women with severe disease (81.8% vs 59.1%). Selected laboratory abnormalities associated with severe preeclampsia are presented in Table 2.
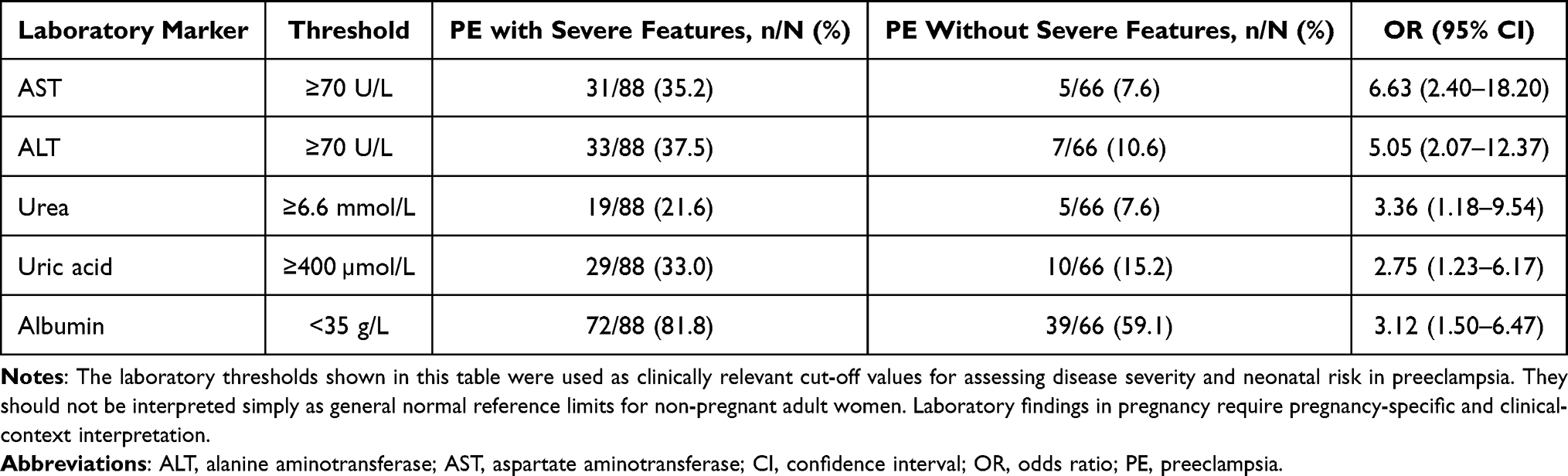 |
Table 2 Selected Clinically Relevant Laboratory Abnormalities by Preeclampsia Severity Category (N=154) |
Management, Delivery Characteristics, and Maternal-Neonatal Outcomes
Medical management before delivery was brief in most cases. Overall, 65.6% of women received one day or less of medical treatment before birth, and this was more common among women with severe preeclampsia. Magnesium sulfate was administered to all women with severe preeclampsia, and a substantial proportion required combination antihypertensive therapy.
Cesarean delivery was the predominant mode of birth, accounting for 125 of 154 deliveries (81.2%). Vaginal delivery occurred in 27 women (17.5%). Preterm birth occurred in 55 pregnancies (35.7%), and fetal growth restriction was documented in 16 pregnancies (10.4%). There were two intrauterine fetal deaths (1.3%). Maternal complications were uncommon but included postpartum hemorrhage, coagulation disorder, and HELLP syndrome. Delivery characteristics and major maternal-neonatal outcomes are shown in Table 3.
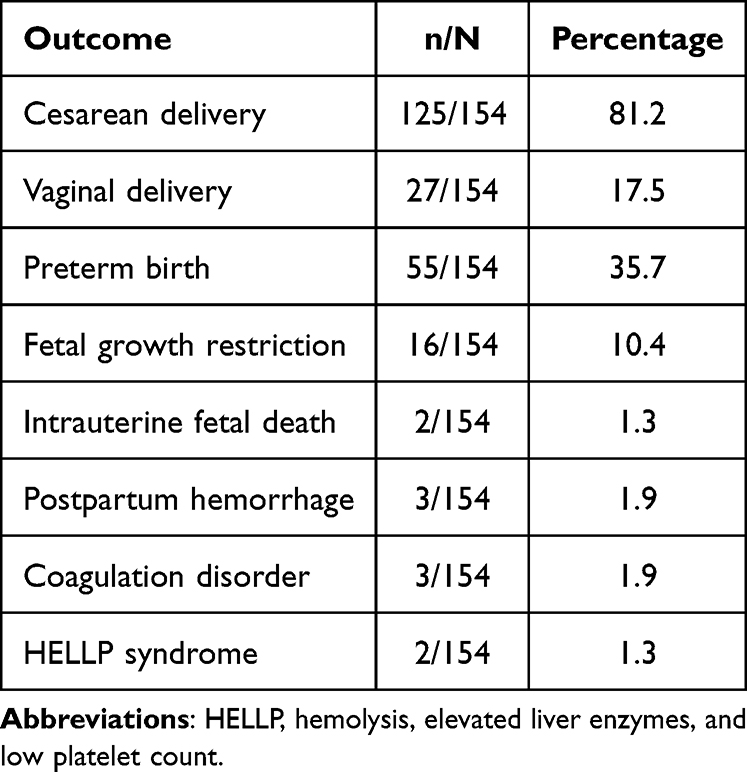 |
Table 3 Delivery Characteristics and Major Maternal-Neonatal Outcomes (N=154) |
Factors Associated with Adverse Neonatal Outcomes
Multivariable logistic regression was performed to identify factors independently associated with adverse neonatal outcomes. Maternal age >35 years, gestational age <34 weeks, serum albumin <35 g/L, serum uric acid ≥400 µmol/L, blood pressure ≥160/90 mmHg, and medical treatment duration of one day or less before delivery were all significantly associated with increased odds of adverse neonatal outcomes. Gestational age <34 weeks showed the strongest association, with an adjusted odds ratio of 8.77. Duration of medical treatment before delivery of one day or less was also strongly associated with adverse neonatal outcomes. The full multivariable model is presented in Table 4.
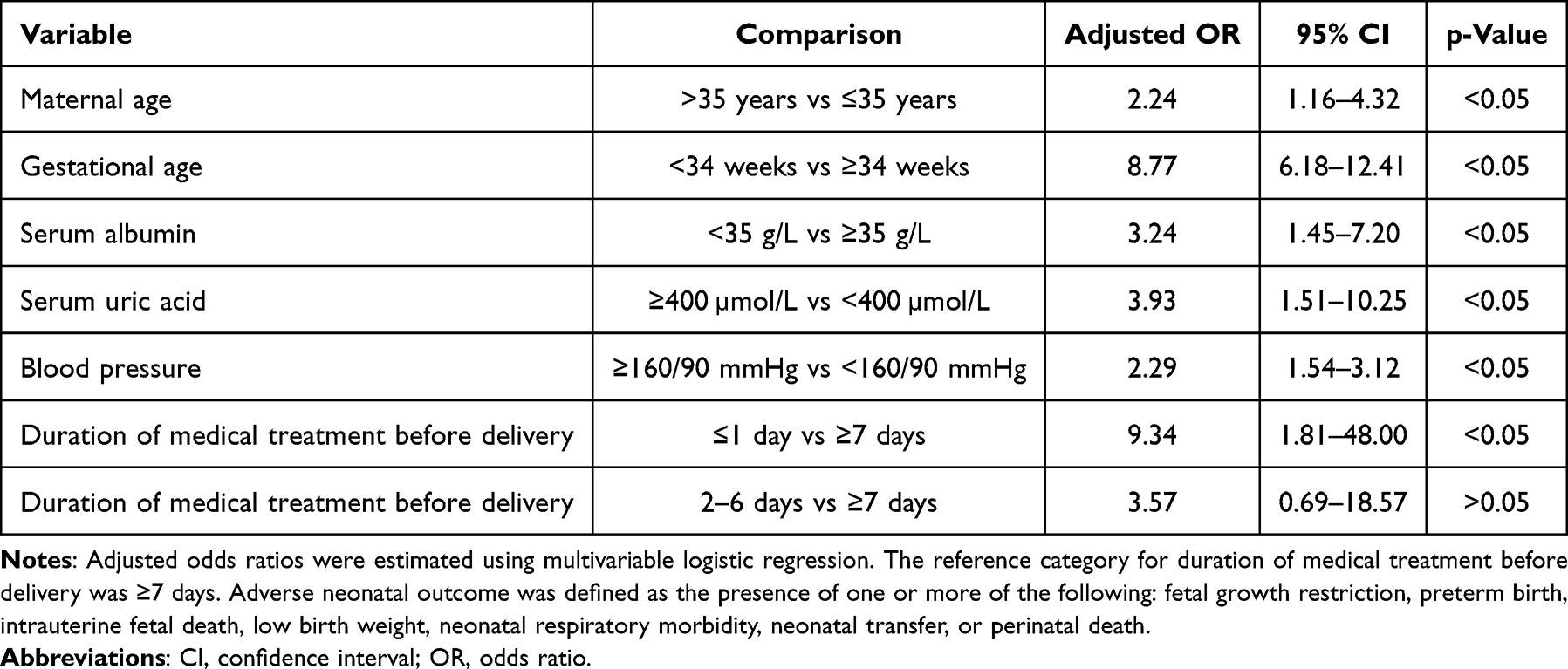 |
Table 4 Multivariable Logistic Regression Analysis of Factors Associated with Adverse Neonatal Outcomes (N=154) |
Discussion
This study identified several clinically important findings regarding third-trimester preeclampsia in a tertiary referral obstetric setting in Vietnam. First, more than half of the women in the cohort had preeclampsia with severe features, indicating a substantial burden of clinically advanced disease in this referral-center population. Second, cesarean delivery was highly frequent, particularly among women with severe features, reflecting the need for timely maternal stabilization and delivery decision-making in a high-risk obstetric setting. Third, older maternal age, primigravidity, prior stillbirth, assisted conception, and several biochemical abnormalities, including elevated liver enzymes, hyperuricemia, hypoalbuminemia, and elevated urea, were more common among women with severe disease. Finally, adverse neonatal outcomes were associated with maternal age above 35 years, gestational age below 34 weeks, hypoalbuminemia, hyperuricemia, severe-range hypertension, and a short duration of medical management before delivery. These findings directly address the study objectives by describing the clinical profile, management patterns, and maternal-neonatal risk factors observed in this cohort.
This study demonstrates a substantial burden of severe preeclampsia in a provincial referral setting, with more than half of the women meeting severe criteria and more than four in five pregnancies ending by cesarean delivery. This pattern is clinically plausible for a tertiary obstetrics and gynecology hospital, where the patient population often includes both women initially diagnosed through routine antenatal care and women referred after disease progression or suspected maternal–fetal compromise. Large international analyses have shown that preeclampsia and eclampsia contribute substantially to maternal mortality and severe perinatal morbidity, particularly in low- and middle-income countries where delays in recognition and referral can worsen outcomes.1,2,8 Similar hospital-based data from Vietnam have shown that hypertensive disorders of pregnancy remain associated with important maternal and perinatal complications, and that adverse outcomes are strongly influenced by disease severity, high blood pressure, severity symptoms, low birth weight, and access to emergency obstetric and newborn care.22 The high proportion of severe cases in the present cohort may therefore reflect not only the underlying clinical burden of preeclampsia but also the referral function of the hospital, where milder cases may be managed locally while more complex or unstable cases are transferred for specialist care.
The high cesarean delivery rate should also be interpreted in this context. In preeclampsia, delivery remains the definitive treatment, and international guidance emphasizes delivery after maternal stabilization when preeclampsia with severe features is diagnosed at or beyond 34 weeks of gestation.6,24,25 Expectant management may be considered in selected preterm cases, but it requires close maternal and fetal monitoring, laboratory surveillance, and immediate capacity for intervention if maternal or fetal status deteriorates.6,26 In low- and middle-income settings, the threshold for prolonged expectant management may reasonably be lower when referral delays, intensive monitoring limitations, blood product availability, and neonatal care capacity are uncertain.9,27 Recent evidence from low- and middle-income settings also suggests that planned delivery for late preterm preeclampsia can reduce severe maternal hypertension and stillbirth without a clear increase in serious neonatal harm, supporting the clinical logic of timely delivery once maternal risk becomes substantial.28 Therefore, the predominance of cesarean delivery in this cohort likely reflects a combination of severe maternal disease, concern for fetal compromise, previous cesarean scar or other obstetric indications, and a low tolerance for delaying birth once severe disease was recognized.
More broadly, these findings reinforce the importance of interpreting management patterns through the lens of local health-system capacity rather than assuming that high intervention rates necessarily indicate over-treatment. In a provincial referral hospital, clinicians must balance the maternal risks of disease progression including eclampsia, stroke, pulmonary edema, hepatic injury, renal dysfunction, and coagulopathy, against the neonatal risks of prematurity and the practical availability of neonatal intensive care support.4,6 Where monitoring resources are limited or referral has already occurred late in the disease course, prompt delivery may be favored to prevent catastrophic maternal deterioration, even though this strategy may increase preterm birth and cesarean delivery rates. The present results therefore highlight the need for earlier antenatal detection, timely referral before severe features develop, standardized protocols for severity assessment, and strengthened neonatal preparedness at provincial referral centers.
The observed associations between severe preeclampsia and maternal age of 35 years or older, primigravidity, prior stillbirth, and assisted conception are broadly consistent with established evidence on preeclampsia risk. Advanced maternal age and nulliparity are recognized clinical risk factors in major prospective studies, systematic reviews, and clinical guidelines, likely reflecting a combination of vascular, metabolic, immunological, and placental mechanisms that increase susceptibility to abnormal placentation and maternal endothelial dysfunction.4,6,12–14 Risk-factor studies across Latin America, the Caribbean, South Asia, and sub-Saharan Africa also show that the relative importance of age, parity, obesity, prior disease, family history, and other contextual exposures varies across populations.11,15,16,18,19 Nulliparity has long been linked to preeclampsia risk, partly through maternal immune maladaptation to paternal and placental antigens, while advanced maternal age may increase risk through higher rates of chronic vascular disease, metabolic comorbidity, reduced cardiovascular reserve, and age-related placental dysfunction.4 Although the present study did not directly assess these biological pathways, the higher proportion of severe disease among older and primigravid women supports the need to treat these characteristics as clinically meaningful markers during antenatal risk stratification.
The association with prior stillbirth is also clinically important. Previous adverse pregnancy outcomes, including stillbirth and previous preeclampsia, may indicate an underlying predisposition to placental dysfunction, hypertensive disease, thrombophilia, chronic maternal disease, or other recurring obstetric risks. Prospective evidence has shown that women with previous preeclampsia have increased risks of adverse maternal and perinatal outcomes in subsequent pregnancies, supporting the view that prior complicated pregnancies should trigger heightened antenatal surveillance.29 Preeclampsia itself is a known risk factor for fetal death and other adverse perinatal outcomes, and women with a previous stillbirth require careful evaluation and closer surveillance in subsequent pregnancies.6 In this cohort, the link between prior stillbirth and severe preeclampsia suggests that obstetric history should be given substantial weight during triage, even when women present without severe symptoms at first assessment. A practical implication is that women with a history of stillbirth may benefit from earlier referral, more frequent blood pressure monitoring, assessment of proteinuria, and closer fetal growth surveillance.
Assisted conception was also more common among women with severe preeclampsia in this study. This finding aligns with systematic review evidence showing that pregnancies conceived through assisted reproductive technology have a higher risk of preeclampsia than spontaneous conceptions.30 The relationship is likely multifactorial: women undergoing assisted reproduction are often older, may have underlying infertility-related conditions, and have higher rates of multifetal gestation, all of which can increase placental and vascular risk. In addition, some evidence suggests that assisted reproductive technology itself may influence placentation, although separating the effects of treatment from the effects of parental subfertility remains difficult.4,30 In a referral hospital setting, assisted conception may also lead to heightened surveillance and a lower threshold for intervention, especially when pregnancies are perceived by families and clinicians as high-value or high-risk.
The prominence of older maternal age in this cohort has particular relevance for local screening and triage. Vietnam, like many middle-income countries, is experiencing demographic and fertility transitions, with women increasingly having fewer children and delaying childbirth in some urban and socioeconomically advantaged groups.31 Obesity and overweight are also increasingly relevant in preeclampsia prevention and triage, as meta-analytic evidence demonstrates a positive relationship between body mass index and preeclampsia risk.17 As delayed childbearing, elevated body mass index, and access to fertility treatment become more common, obstetric services may see a growing proportion of pregnancies complicated by advanced maternal age, assisted conception, chronic medical conditions, or combinations of these risks. These trends strengthen the rationale for structured antenatal risk assessment, early identification of high-risk women, timely referral from lower-level facilities, and standardized monitoring protocols for blood pressure, proteinuria, fetal growth, and maternal laboratory markers. In provincial referral settings, such risk-based pathways may be especially useful in preventing late recognition of severe disease and reducing avoidable maternal and neonatal complications.
Biochemical markers were clinically informative in this cohort. Women with severe preeclampsia had substantially higher frequencies of elevated transaminases, hyperuricemia, hypoalbuminemia, and elevated urea, suggesting that severe disease was accompanied by measurable hepatic, renal, endothelial, and protein-loss manifestations. This pattern is consistent with the current understanding of preeclampsia as a multisystem disorder rather than a condition defined by hypertension alone, and with pathophysiological models emphasizing abnormal placentation, endothelial dysfunction, inflammation, vasoconstriction, and coagulation activation.4,32,33 Contemporary diagnostic criteria recognize thrombocytopenia, impaired liver function, renal insufficiency, pulmonary edema, neurological symptoms, and uteroplacental dysfunction as clinically important features of disease severity.6,7 Therefore, routine biochemical testing can provide useful objective evidence of disease progression, particularly when symptoms are subtle, nonspecific, or difficult to interpret.
The higher frequency of elevated AST and ALT among women with severe preeclampsia is clinically meaningful because hepatic involvement reflects systemic endothelial dysfunction, vasospasm, periportal injury, and, in severe cases, progression toward HELLP syndrome. ACOG includes impaired liver function, commonly reflected by elevated transaminases, among the severe features of preeclampsia, especially when accompanied by right upper quadrant or epigastric pain.6 In practice, abnormal liver enzymes may help clinicians distinguish women who require closer monitoring, magnesium sulfate prophylaxis, and timely delivery planning from those with less severe disease. Similarly, elevated urea and other renal markers reflect renal endothelial injury and reduced filtration capacity, which are central to the pathophysiology of preeclampsia and may indicate a higher risk of maternal and fetal compromise.4,6
Among the biochemical variables assessed, serum uric acid and serum albumin were particularly notable because both remained associated with adverse neonatal outcomes in multivariable analysis. Hyperuricemia in preeclampsia has been widely studied and is thought to reflect reduced renal clearance, oxidative stress, endothelial dysfunction, and placental ischemia. Although uric acid is not universally recommended as a standalone diagnostic criterion, multiple studies suggest that higher uric acid levels are associated with more severe disease and adverse perinatal outcomes, including fetal growth restriction, preterm birth, and low birth weight.34,35 In this study, the association between serum uric acid ≥400 µmol/L and adverse neonatal outcomes suggests that uric acid may function as a practical severity marker in settings where more specialized placental biomarkers are unavailable.
Hypoalbuminemia may also carry clinical value. Low serum albumin in preeclampsia can reflect proteinuria, increased vascular permeability, systemic inflammation, hemodilution, and reduced colloid oncotic pressure. These mechanisms are relevant to both maternal complications, such as edema and pulmonary edema risk, and fetal compromise related to placental dysfunction. However, albumin should be interpreted cautiously. Recent evidence suggests that low albumin may be associated with severe proteinuria and disease severity, but it may not independently predict all maternal or fetal complications when used alone.36 In the present cohort, albumin <35 g/L was independently associated with adverse neonatal outcomes, indicating that it may be useful as part of a combined clinical-laboratory risk assessment rather than as an isolated predictor.
These findings have practical implications for provincial and resource-constrained obstetric settings. Advanced angiogenic biomarkers, particularly the soluble fms-like tyrosine kinase-1 to placental growth factor ratio, have shown value in the diagnosis and short-term prediction of preeclampsia progression, especially in women with suspected disease.33,37 Nevertheless, such assays may not be routinely accessible or affordable in many low- and middle-income settings. By contrast, liver enzymes, renal function tests, uric acid, serum albumin, platelet count, and urine protein testing are inexpensive, widely available, and already embedded in routine hospital workflows. In this context, the present findings support the use of conventional biochemical markers to assist bedside risk stratification, guide monitoring intensity, and inform delivery planning. However, these markers should not replace clinical assessment, blood pressure monitoring, fetal growth evaluation, or cardiotocography; rather, they should be integrated into a broader severity assessment framework.
The delivery pattern observed in this study deserves particular attention. All women with severe preeclampsia were delivered by cesarean section, and the overall cesarean delivery rate exceeded 80%. This finding should be interpreted within the clinical reality of preeclampsia management, where delivery is the only definitive treatment and where the timing and mode of birth must balance maternal stabilization, fetal condition, gestational age, cervical favorability, and institutional capacity for emergency obstetric and neonatal care.6,24–26 In women with severe features, especially at or beyond 34 weeks of gestation, guidelines generally support delivery after maternal stabilization rather than prolonged expectant management.6 Therefore, the high intervention rate in this cohort likely reflects a safety-oriented approach in a referral setting where many women may have presented with advanced disease, fetal compromise, or limited time for extended observation.
However, the predominance of cesarean delivery also raises important questions about the role of carefully selected induction strategies. Preeclampsia itself is not an automatic indication for cesarean section, and mode of delivery should generally be determined by obstetric indications, disease severity, fetal status, gestational age, and the likelihood of successful vaginal birth.6,25 Evidence on induction for preeclampsia suggests that successful labor induction is possible in selected women at both preterm and term gestational ages, although success depends strongly on gestational age, cervical status, parity, fetal status, and institutional readiness for emergency intervention.38 Vaginal delivery may be appropriate when the maternal condition is stable, fetal status is reassuring, gestational age is suitable, and the cervix is favorable or induction is expected to be feasible. Conversely, cesarean delivery may be clinically appropriate when rapid delivery is required, fetal compromise is suspected, the cervix is unfavorable and vaginal birth is unlikely within a safe timeframe, or additional obstetric indications are present. Thus, while the high cesarean rate in this cohort may be clinically understandable, it should not be interpreted as the only possible management pathway for all severe preeclampsia cases.
Several local and clinical factors probably contributed to the observed pattern. First, the study was conducted in a provincial tertiary referral hospital, where referred cases may be more severe than those seen in routine antenatal settings. Referral bias can increase the proportion of women with severe hypertension, maternal organ dysfunction, fetal growth restriction, non-reassuring fetal status, previous cesarean scar, or advanced gestational age requiring prompt delivery. Second, the presence of previous cesarean scar in a substantial proportion of surgical cases may have reduced the use of induction or trial of labor, particularly if local protocols, staffing, or emergency surgical readiness made vaginal birth after cesarean less feasible. Third, in low- and middle-income settings, clinicians may reasonably have a lower tolerance for prolonged expectant management when continuous maternal-fetal monitoring, blood product availability, and neonatal intensive care capacity are uncertain.9,27 Evidence from low- and middle-income countries also suggests that planned delivery for late preterm preeclampsia can reduce severe maternal hypertension and stillbirth without clearly increasing serious neonatal harm, supporting timely delivery when maternal risk is substantial.28
Nevertheless, the finding that all severe cases were delivered by cesarean section indicates a potential area for protocol review and clinical audit. Such an audit should not simply aim to reduce cesarean delivery rates, since inappropriate delay in severe preeclampsia could increase maternal and perinatal risk. Rather, it should examine whether cesarean delivery was consistently driven by documented obstetric indications, fetal compromise, previous uterine scar, unfavorable cervix with need for urgent delivery, or maternal instability. It would also be useful to identify the subset of women with severe preeclampsia who were clinically stable, at appropriate gestational age, with reassuring fetal status and no contraindication to labor, for whom induction of labor could have been considered. A standardized pathway incorporating severity assessment, Bishop score, fetal status, previous uterine scar, gestational age, and availability of emergency cesarean and neonatal support may help distinguish women who require immediate cesarean delivery from those suitable for carefully monitored induction. In this way, the delivery pattern in the present study should be viewed less as evidence of over-intervention and more as a signal for structured review of decision-making, documentation, and protocol consistency in the management of severe preeclampsia.
Preterm birth was the most frequent adverse neonatal outcome in this cohort, followed by fetal growth restriction. This pattern is consistent with the pathophysiology and clinical management of preeclampsia. Placental dysfunction can directly impair fetal growth, while maternal disease progression often necessitates medically indicated preterm delivery to prevent severe maternal complications or fetal deterioration.4,6 Early-onset and preterm preeclampsia are particularly associated with substantial maternal and neonatal morbidity, and earlier literature has emphasized the high burden of morbidity and mortality when severe disease occurs before term.39 Recent studies of expectant treatment in early-onset preeclampsia also show that fetal growth restriction remains a major clinical concern and that balancing fetal maturity against maternal risk is central to management.40 The strong association between gestational age below 34 weeks and adverse neonatal outcomes is therefore unsurprising and clinically coherent. Birth before 34 weeks is a key threshold in preeclampsia management, as neonatal morbidity is strongly influenced by prematurity, and ACOG recommends antenatal corticosteroids for fetal lung maturation when delivery is indicated before 34 weeks, although maternal or fetal deterioration may preclude delaying delivery to complete corticosteroid exposure.6
However, the multivariable findings suggest that prematurity alone does not fully explain neonatal risk. Maternal age above 35 years, severe-range hypertension, hypoalbuminemia, hyperuricemia, and very short pre-delivery treatment duration were also independently associated with adverse neonatal outcomes. These factors likely represent overlapping dimensions of disease severity. Severe hypertension reflects more advanced maternal vascular dysfunction and is directly linked to urgent delivery decisions, while hyperuricemia may indicate reduced renal clearance, oxidative stress, endothelial dysfunction, and placental ischemia. Although the role of serum uric acid as a standalone predictive test remains debated, systematic reviews and clinical studies have repeatedly reported associations between elevated uric acid and adverse maternal or perinatal outcomes in preeclampsia.35,41,42
The association between hypoalbuminemia and adverse neonatal outcomes may reflect systemic endothelial leakage, proteinuria, reduced oncotic pressure, and more severe maternal disease. Previous studies have linked hypoproteinemia or hypoalbuminemia in preeclampsia with worse maternal and neonatal outcomes, although albumin should be interpreted as a severity marker rather than a disease-specific predictor.36,43 This distinction is important: low albumin is unlikely to replace established clinical criteria, but it may add practical value when combined with blood pressure, symptoms, renal function, liver enzymes, uric acid, platelet count, and fetal assessment. In provincial referral settings where advanced angiogenic biomarkers may not be routinely available, such inexpensive biochemical markers may help clinicians identify women whose pregnancies are at higher risk of fetal compromise or early delivery.
The strong association between one day or less of medical treatment before delivery and adverse neonatal outcomes also deserves careful interpretation. This finding should not be read simply as evidence that short treatment causes poor neonatal outcome. More plausibly, very short pre-delivery management reflects urgent presentation, rapid disease progression, late referral, or the need for immediate delivery due to maternal or fetal instability. In other words, treatment duration may function as a proxy for the clinical window available for stabilization, corticosteroid administration, blood pressure control, fetal assessment, and neonatal preparation. International guidelines support timely delivery when severe preeclampsia is diagnosed and maternal or fetal risk is substantial, but they also emphasize maternal stabilization and careful monitoring where expectant management is feasible.6 In this context, the present findings highlight the importance of earlier detection, faster referral before severe deterioration, and standardized protocols that allow safe stabilization without delaying necessary delivery.
The main contribution of this study is clinical and regional rather than mechanistic. By providing real-world data from a provincial tertiary referral hospital in Vietnam, the study helps clarify how severe preeclampsia, delivery decisions, and neonatal outcomes present in a low- and middle-income setting. The observed associations of serum uric acid, hypoalbuminemia, and short pre-delivery treatment duration with adverse neonatal outcomes may be particularly useful for risk stratification in settings where advanced biomarkers are not routinely available. These findings should be interpreted as clinically relevant associations, not as evidence of causality or novel biological mechanisms. Overall, these results suggest that neonatal risk in preeclampsia is shaped by the interaction between gestational age, placental disease severity, maternal biochemical derangement, and the amount of time available for clinical optimization before birth. For practice, this supports a risk-stratified approach in which women with severe hypertension, low albumin, elevated uric acid, or early gestational age receive intensified maternal-fetal monitoring and early neonatal team involvement. For health-system planning, the findings reinforce the value of antenatal screening and referral pathways that identify high-risk women before the only safe option becomes urgent delivery.
This study has several limitations. First, it was conducted at a single tertiary obstetrics and gynecology hospital; therefore, the findings may not be generalizable to all obstetric settings in Vietnam, particularly lower-level facilities or private hospitals. Second, although the sample size was adequate for the primary descriptive objectives, it was moderate for multivariable modeling, and some estimates had wide confidence intervals, suggesting limited precision. Third, the analysis was restricted to variables collected in the original study protocol. Potentially relevant factors, including detailed neonatal intensive care course, duration of neonatal hospitalization, long-term neonatal outcomes, socioeconomic status, timing of referral, antenatal care quality, and detailed corticosteroid exposure, were not fully captured. The composite adverse neonatal outcome included clinically heterogeneous endpoints of varying severity; therefore, the regression findings should be interpreted as markers of overall neonatal risk rather than predictors of any single neonatal complication. In addition, some adjusted odds ratios had wide confidence intervals, reflecting moderate statistical imprecision due to the sample size and number of outcome events. Larger multicenter studies are needed to confirm these associations. Finally, some laboratory and proteinuria data required careful interpretation; therefore, key variables should be verified against the original dataset before journal submission to ensure consistency between the analytic dataset, tables, and final manuscript text.
Conclusion
Third-trimester preeclampsia at a major public tertiary obstetrics and gynecology hospital in Vietnam was characterized by a high burden of severe disease, frequent cesarean delivery, and substantial neonatal risk driven mainly by preterm birth. Maternal age above 35 years, primigravidity, assisted conception, severe hypertension, hyperuricemia, and hypoalbuminemia were associated with more severe maternal or neonatal compromise. These findings support vigilant surveillance, timely delivery planning, and risk-stratified management in tertiary obstetric practice. However, the results should be interpreted within the referral-center context and may not be directly generalizable to lower-level obstetric facilities or community settings.
Acknowledgments
The authors thank the staff of the participating hospital for their support in data collection and patient care. The authors are also grateful to the women whose anonymized clinical data were included in this retrospective analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khan KS, Wojdyla D, Say L, Gülmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367(9516):1066–13. doi:10.1016/S0140-6736(06)68397-9
2. Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Heal. 2014;2(6):e323–e333. doi:10.1016/S2214-109X(14)70227-X
3. WHO. Pre-eclampsia. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/pre-eclampsia.
4. Dimitriadis E, Rolnik DL, Zhou W, et al. Pre-eclampsia. Nat Rev Dis Primers. 2023;9(1):8. doi:10.1038/s41572-023-00417-6
5. Tranquilli AL, Brown MA, Zeeman GG, Dekker G, Sibai BM. The definition of severe and early-onset preeclampsia. Statements from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Pregnancy Hypertens. 2013;3(1):44–47. doi:10.1016/j.preghy.2012.11.001
6. ACOG. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet Gynecol. 2020;135(6):1.
7. Tanner MS, Davey M-A, Mol BW, Rolnik DL. The evolution of the diagnostic criteria of preeclampsia-eclampsia. Am J Obstet Gynecol. 2022;226(2, Supplement):S835–S843. doi:10.1016/j.ajog.2021.11.1371
8. Bilano VL, Ota E, Ganchimeg T, Mori R, Souza JP. Risk factors of pre-eclampsia/eclampsia and its adverse outcomes in low- and middle-income countries: a WHO secondary analysis. PLoS One. 2014;9(3):e91198. doi:10.1371/journal.pone.0091198
9. Mayrink J, Reis ZSN. Pre-eclampsia in low and middle-income settings: what are the barriers to improving perinatal outcomes and evidence-based recommendations? Int J Gynaecol Obstet off Organ Int Fed Gynaecol Obstet. 2024;164(1):33–39. doi:10.1002/ijgo.14913
10. WHO. Maternal health in Viet Nam. 2025. Available from: https://www.who.int/vietnam/health-topics/maternal-health.
11. Conde-Agudelo A, Belizán JM. Risk factors for pre-eclampsia in a large cohort of Latin American and Caribbean women. BJOG. 2000;107(1):75–83. doi:10.1111/j.1471-0528.2000.tb11582.x
12. Sibai BM, Gordon T, Thom E, et al. Risk factors for preeclampsia in healthy nulliparous women: a prospective multicenter study. The National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. Am J Obstet Gynecol. 1995;172(2 Pt 1):642–648. doi:10.1016/0002-9378(95)90586-3
13. Knuist M, Bonsel GJ, Zondervan HA, Treffers PE. Risk factors for preeclampsia in nulliparous women in distinct ethnic groups: a prospective cohort study. Obstet Gynecol. 1998;92(2):174–178. doi:10.1016/s0029-7844(98)00143-4
14. Duckitt K, Harrington D. Risk factors for pre-eclampsia at antenatal booking: systematic review of controlled studies. BMJ. 2005;330(7491):565. doi:10.1136/bmj.38380.674340.E0
15. Fikadu K, G/Meskel F, Getahun F, Chufamo N, Misiker D. Family history of chronic illness, preterm gestational age and smoking exposure before pregnancy increases the probability of preeclampsia in Omo district in southern Ethiopia: a case-control study. Clin Hypertens. 2020;26(1):16. doi:10.1186/s40885-020-00149-9
16. Hounkpatin OI, Amidou SA, Houehanou YC, et al. Systematic review of observational studies of the impact of cardiovascular risk factors on preeclampsia in sub-saharan Africa. BMC Pregnancy Childbirth. 2021;21(1):97. doi:10.1186/s12884-021-03566-2
17. Motedayen M, Rafiei M, Rezaei Tavirani M, Sayehmiri K, Dousti M. The relationship between body mass index and preeclampsia: a systematic review and meta-analysis. Int J Reprod Biomed. 2019;17(7):463–472. doi:10.18502/ijrm.v17i7.4857
18. Padhan SC, Pradhan P, Panda B, Pradhan SK, Mishra SK. Risk Factors of Pre-eclampsia: a Hospital-Based Case-Control Study. Cureus. 2023;15(7):e42543. doi:10.7759/cureus.42543
19. Soomro S, Kumar R, Lakhan H, Shaukat F. Risk Factors for Pre-eclampsia and Eclampsia Disorders in Tertiary Care Center in Sukkur, Pakistan. Cureus. 2019;11(11):e6115. doi:10.7759/cureus.6115
20. Ngene NC, Moodley J. Preventing maternal morbidity and mortality from preeclampsia and eclampsia particularly in low- and middle-income countries. Best Pract Res Clin Obstet Gynaecol. 2024;94:102473. doi:10.1016/j.bpobgyn.2024.102473
21. Ministry of Health of Vietnam. National Guidelines for Reproductive Health Services; 2016.
22. Nguyen THA, Nguyen MT, Truong TH. Maternal and perinatal outcomes of hypertensive disorders in pregnancy: insights from the National Hospital of Obstetrics and Gynecology in Vietnam. PLoS One. 2024;19(1):e0297302. doi:10.1371/journal.pone.0297302
23. Feng J, Huang J, Wu Q, Wei K, Bin Q. Maternal mortality ratios in Southeast Asia (1990–2021): trends, disparities, and projections through 2050 based on the global burden of disease 2021, with reference to SDG 3.1. BMC Pregnancy Childbirth. 2025;25(1):1264. doi:10.1186/s12884-025-08443-w
24. Dhariwal NK, Lynde GC. Update in the Management of Patients with Preeclampsia. Anesthesiol Clin. 2017;35(1):95–106. doi:10.1016/j.anclin.2016.09.009
25. Moussa HN, Arian SE, Sibai BM. Management of hypertensive disorders in pregnancy. Womens Health Lond Engl. 2014;10(4):385–404. doi:10.2217/whe.14.32
26. WHO. WHO Recommendations Policy of Interventionist versus Expectant Management of Severe Pre-Eclampsia before Term.; 2018. Available from: https://iris.who.int/server/api/core/bitstreams/7df8793e-90d8-4b28-a0b4-6a755f6c2d2d/content.
27. von Dadelszen P, Vidler M, Tsigas E, Magee LA. Management of Preeclampsia in Low- and Middle-Income Countries: lessons to Date, and Questions Arising, from the PRE-EMPT and Related Initiatives. Matern Med. 2021;3(2):136–150.
28. Beardmore-Gray A, Vousden N, Seed PT, et al. Planned delivery or expectant management for late preterm pre-eclampsia in low-income and middle-income countries (CRADLE-4): a multicentre, open-label, randomised controlled trial. Lancet. 2023;402(10399):386–396. doi:10.1016/S0140-6736(23)00688-8
29. Bramham K, Briley AL, Seed P, Poston L, Shennan AH, Chappell LC. Adverse maternal and perinatal outcomes in women with previous preeclampsia: a prospective study. Am J Obstet Gynecol. 2011;204(6):512. doi:10.1016/j.ajog.2011.02.014
30. Almasi-Hashiani A, Omani-Samani R, Mohammadi M, et al. Assisted reproductive technology and the risk of preeclampsia: an updated systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019;19(1):149. doi:10.1186/s12884-019-2291-x
31. Doan LP, Nguyen LH, Do HN, et al. Ensuring Population Health in the Era of Aging in Vietnam: policy Review and Factors Associated with Intentions of Childbearing before the Age of 30 among Youths. Healthcare. 2023;11(1):102. doi:10.3390/healthcare11010102
32. El-Sayed AAF. Preeclampsia: a review of the pathogenesis and possible management strategies based on its pathophysiological derangements. Taiwan J Obstet Gynecol. 2017;56(5):593–598. doi:10.1016/j.tjog.2017.08.004
33. Rana S, Lemoine E, Granger JP, Karumanchi SA. Preeclampsia: pathophysiology, Challenges, and Perspectives. Circ Res. 2019;124(7):1094–1112. doi:10.1161/CIRCRESAHA.118.313276
34. Mohamed RA, Ali IA. Role of neutrophil / lymphocyte ratio, uric acid / albumin ratio and uric acid / creatinine ratio as predictors to severity of preeclampsia. BMC Pregnancy Childbirth. 2023;23(1):763. doi:10.1186/s12884-023-06083-6
35. Thangaratinam S, Ismail KMK, Sharp S, Coomarasamy A, Khan KS. Accuracy of serum uric acid in predicting complications of pre-eclampsia: a systematic review. BJOG an Int J Obstet Gynaecol. 2006;113(4):369–378. doi:10.1111/j.1471-0528.2006.00908.x
36. Ciciu E, Alexandru A, Cimpineanu B, et al. Could Low Serum Albumin Level Be an Independent Marker of Severe Preeclampsia? Healthcare. 2025;13(13):1503. doi:10.3390/healthcare13131503
37. Duhig KE, Myers J, Seed PT, et al. Placental growth factor testing to assess women with suspected pre-eclampsia: a multicentre, pragmatic, stepped-wedge cluster-randomised controlled trial. Lancet. 2019;393(10183):1807–1818. doi:10.1016/S0140-6736(18)33212-4
38. Roland C, Warshak CR, DeFranco EA. Success of labor induction for pre-eclampsia at preterm and term gestational ages. J Perinatol off J Calif Perinat Assoc. 2017;37(6):636–640. doi:10.1038/jp.2017.31
39. Murphy DJ, Stirrat GM. Mortality and morbidity associated with early-onset preeclampsia. Hypertens Pregnancy. 2000;19(2):221–231. doi:10.1081/prg-100100138
40. Yi J, Chen L, Meng X, Chen Y. Risk factors and foetal growth restriction associated with expectant treatment of early-onset preeclampsia. Ann Med. 2022;54(1):3250–3257. doi:10.1080/07853890.2022.2144642
41. Corominas AI, Medina Y, Balconi S, et al. Assessing the Role of Uric Acid as a Predictor of Preeclampsia. Front Physiol. 2022;12:785219. doi:10.3389/fphys.2021.785219
42. Ugwuanyi RU, Chiege IM, Agwu FE, Eleje GU, Ifediorah NM. Association between Serum Uric Acid Levels and Perinatal Outcome in Women with Preeclampsia. Obstet Gynecol Int. 2021;2021(1):6611828. doi:10.1155/2021/6611828
43. Chen H, Tao F, Fang X, Wang X. Association of hypoproteinemia in preeclampsia with maternal and perinatal outcomes: a retrospective analysis of high-risk women. J Res Med Sci Off J Isfahan Univ Med Sci. 2016;21:98. doi:10.4103/1735-1995.193170
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Proactive Coping in Early Pregnancy and Adverse Pregnancy Outcomes
Cersonsky TEK, Fain AC, Lewkowitz AK, Werner EF, Miller ES, Clark MA, Ayala NK
International Journal of Women's Health 2024, 16:979-985
Published Date: 30 May 2024
Maternal and Neonatal Perinatal Outcomes of Singleton Pregnancies in Advanced-Age Women Undergoing IVF/ICSI-ET Compared with Spontaneous Conception: A Retrospective Propensity Score Matched Cohort Study
Mao J, Yang G, Su Q, Zeng Z, Lin J, Kong L, Zhang L, Liu L, Yang Y, Wu H
International Journal of General Medicine 2024, 17:5249-5259
Published Date: 13 November 2024
Development and Validation of Dynamic Nomograms for Predicting Delivery Mode and Neonatal Intensive Care Unit Admission in Intrapartum Fever: A Retrospective Cohort Study

Ni J, Zhang D, Ding Y, Ding H, Munemo ZPR, Zhang H
International Journal of Women's Health 2025, 17:3385-3400
Published Date: 30 September 2025
Maternal and Neonatal Outcomes in Pregnant Women Vaccinated Against COVID-19 Compared to an Unvaccinated Group
Nourian T, Sarandili S, Mousavi S, Mirmohammadkhani M, Rahmanian M
International Journal of Women's Health 2025, 17:4131-4142
Published Date: 5 November 2025