Back to Journals » International Journal of Women's Health » Volume 17
Development and Validation of Dynamic Nomograms for Predicting Delivery Mode and Neonatal Intensive Care Unit Admission in Intrapartum Fever: A Retrospective Cohort Study
Authors Ni J ![]() , Zhang D, Ding Y, Ding H
, Zhang D, Ding Y, Ding H ![]() , Munemo ZPR
, Munemo ZPR ![]() , Zhang H
, Zhang H ![]()
Received 4 June 2025
Accepted for publication 20 September 2025
Published 30 September 2025 Volume 2025:17 Pages 3385—3400
DOI https://doi.org/10.2147/IJWH.S544623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jianzhi Ni,1,2 Dan Zhang,3 Yuling Ding,2 Hongmei Ding,4 Zvikomborero Panashe Rejoice Munemo,1 Hongxiu Zhang1 On behalf of the Jiangsu Collaborative Group for Intrapartum Fever & Maternal-Neonatal Outcome Prediction
1Department of Obstetrics and Gynecology, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 2Department of Obstetrics and Gynecology, Huai’an Maternal and Child Health Care Hospital, Huai’an, Jiangsu, People’s Republic of China; 3Department of Obstetrics and Gynecology, Kunshan Maternity and Children’s Health Care Hospital, Kunshan, Jiangsu, People’s Republic of China; 4Department of Obstetrics and Gynecology, Taizhou Fourth People’s Hospital, Taizhou, Jiangsu, People’s Republic of China
Correspondence: Hongxiu Zhang, Department of Obstetrics and Gynecology, the First Affiliated Hospital of Nanjing Medical University, No. 300 Guangzhou Road, Nanjing, Jiangsu, 210029, People’s Republic of China, Email [email protected]
Background: While maternal intrapartum fever is linked to adverse neonatal outcomes, predictive tools for delivery mode and neonatal intensive care unit (NICU) admission in this population remain scarce.
Objective: To develop and validate a dynamic nomogram predicting cesarean delivery and NICU admissions in women with intrapartum fever, facilitating individualized intrapartum decision-making.
Methods: This retrospective cohort study analyzed 24,784 deliveries (2019– 2021) at a tertiary center. After exclusions, 1,047 women with intrapartum fever were included in the study cohort. The dataset was randomly partitioned into training (n=837) and testing (n=210) sets. Backward stepwise multivariable logistic regression models were developed to predict cesarean delivery and neonatal intensive care unit admission. The discriminative capacity of the model was evaluated using receiver operating characteristic (ROC) curve analysis. Calibration performance was assessed via 1000 nonparametric bootstrap resamples to generate calibration curves, with systematic quantification of agreement between predicted probabilities and observed outcomes through the Brier score and Hosmer-Lemeshow goodness-of-fit test.
Results: Predictors of cesarean delivery included advanced maternal age, hypertensive disorders, Intrapartum Antibiotic Prophylaxis (IAP), Meconium-Stained Amniotic Fluid (MSAF), Macrosomia, Postpartum Hemorrhage (PPH), Oligohydramnios, assisted reproductive technology (ART), Hypertensive Disorders of Pregnancy (HDP), Maternal tachycardia, Placental histopathology, intrapartum temperature and Method of inducing labor. Low Birth Weight (LBW), adverse obstetric history (AOH), Fetal tachycardia, Fetal bradycardia, Scarred uterus, Maternal tachycardia and MSAF predicted neonatal intensive care unit admission. The cesarean delivery model achieved AUC of 0.8 (training) and 0.783 (testing); the neonatal intensive care unit admission model showed AUC of 0.681 (training) and 0.748 (testing).
Conclusion: This nomogram provides a clinically useful tool to predict delivery mode and neonatal intensive care unit admission in women with intrapartum fever, aiding risk stratification and improving perinatal outcomes.
Keywords: cesarean delivery, dynamic risk assessment, intrapartum fever, intrapartum decision-making, neonatal outcomes
Graphical Abstract:

Introduction
Intrapartum fever, defined as an axillary temperature≥37.5°C,1,2 is a clinically significant condition associated with adverse maternal and neonatal outcomes, including chorioamnionitis, postpartum hemorrhage, neonatal sepsis, and neonatal brain injury.3–6 Despite variations in diagnostic criteria across studies, this analysis adopts a stringent threshold (≥37.5°C axillary)7–9 to ensure clinical relevance. Intrapartum fever is associated with increased rates of cesarean delivery, fetal distress, intra-amniotic infection, and neonatal intensive care unit admissions.10–12 Although antibiotic prophylaxis and antipyretic therapies are widely used, related complications remain prevalent.13
Globally, the dual challenges of rising cesarean delivery rates and sluggish progress in maternal mortality reduction have fallen short of meeting the 2030 Sustainable Development Goals.14,15 A recent Lancet Global Health analysis,16 highlighted the urgent need for targeted interventions to address preventable causes of maternal death, with intrapartum fever representing a modifiable risk factor. While prediction models exist for preeclampsia and preterm birth,17,18 dynamic risk assessment tools for intrapartum fever are lacking. Current obstetric models (such as the Obstetric Comorbidity Index) focus on general risk stratification rather than fever-specific outcomes.19 Current intrapartum fever models primarily predict either fever occurrence or maternal/neonatal outcomes. Models enabling preventive interventions for its adverse outcomes are currently lacking.20,21 Machine learning advances in perinatal research face challenges, including computational demands and limited interpretability of complex algorithms.22
Unmanaged intrapartum fever may trigger fetal tachycardia, reduce maternal confidence in vaginal delivery, and escalate cesarean rates, antibiotic overuse, and unnecessary interventions. Neonates exposed to fever are often admitted to the NICU for monitoring, risking overtreatment. Notably, most of these adverse consequences (including elevated cesarean rates, unnecessary antibiotic use, and inappropriate neonatal NICU admissions) are modifiable with targeted clinical interventions. However, the lack of dynamic risk assessment tools for women with intrapartum fever undermines such interventions—existing models either only predict the occurrence of intrapartum fever itself or focus on a single maternal/neonatal outcome, failing to provide actionable evidence for preventing key adverse outcomes like cesarean delivery and neonatal NICU admission. This gap leaves clinicians unable to identify high-risk individuals in advance during labor, making it difficult to adjust management plans timely and control adverse outcomes effectively. To address this unmet clinical need, the present study aimed to develop and validate a dynamic nomogram that predicts both cesarean delivery risk in women with intrapartum fever and neonatal NICU admission risk. By enabling precise risk stratification, this tool is intended to assist clinicians in recognizing high-risk cases early, formulating individualized intervention strategies, and ultimately reducing the negative impacts of unmanaged intrapartum fever on maternal and neonatal outcomes. A validated prediction model with targeted interventions is critical to optimizing outcomes. Given the clinical challenges of unmanaged intrapartum fever and the lack of targeted dynamic prediction tools, the primary objective of this retrospective cohort study was to: 1) identify independent predictors of cesarean delivery and neonatal intensive care unit (NICU) admission in women with intrapartum fever; 2) develop dynamic nomograms for predicting these two key maternal and neonatal outcomes; 3) validate the discriminative and calibrate performance of these nomograms, thereby providing an evidence-based tool to support individualized intrapartum decision-making and risk stratification for women with intrapartum fever.
Materials and Methods
Research Design
This was a retrospective cohort study. Trained research staff collected maternal demographic and perinatal data from standardized electronic medical records of 24,784 deliveries at a maternal and child health hospital. The data spanned the period from January 1, 2019, to December 31, 2021.
Inclusion and Exclusion Criteria
Inclusion Criteria
Intrapartum fever (defined as an axillary temperature ≥ 37.5°C); gestational age ≥28 weeks; laboring women; receipt of epidural analgesia.
Exclusion Criteria
Fetal chromosomal or structural anomalies; intrauterine demise; antenatal fever (<37.5°C); maternal allergies; incomplete medical records.
Methods
This study was approved by the Ethics Committee of Huai’an Maternal and Child Health Care Hospital (Approval No. 2023028; Aug 14, 2023). Patient consent for medical record review was waived due to its retrospective design, use of de-identified untraceable routine clinical data, and minimal risk. Patient data confidentiality is ensured by pre-analysis irreversible removal of personal identifiers (names, medical record numbers), encrypted dedicated server storage, and authorized-only access. All procedures comply with the World Medical Association Declaration of Helsinki (2013) and the Committee’s standards.
Methods and Observational Indicators
This retrospective cohort study analyzed clinical data from 24,784 women who delivered at Huai’an Maternal and Child Health Hospital between January 1, 2019 and December 31, 2021. After exclusions, 1,047 women with intrapartum fever were included. The dataset was randomly allocated to a training cohort (n=837) and validation cohort (n=210).
Maternal Baseline Characteristics
Demographic and physical indicators: age, weight, height, body mass index (BMI), gravidity, parity, gestational age at delivery.
Maternal health status: obstetric comorbidities and complications.
Intrapartum-related basic factors: maximum intrapartum temperature, mode of labor induction.
Intrapartum Monitoring and Intervention Factors
Intrapartum physiological indicators: time of membrane rupture, amniotic fluid volume, fetal heart rate during fever.
Laboratory and etiological indicators: white blood cell (WBC) count, neutrophil values, Group B streptococcus (GBS) status, vaginal discharge tests.
Intrapartum interventions: antibiotic use.
Maternal Outcomes
Primary Maternal Outcome: mode of termination of pregnancy (recorded based on clinical delivery methods, such as spontaneous vaginal delivery, cesarean section, assisted vaginal delivery).
Secondary Maternal Outcomes: postpartum blood loss, placental pathology.
Neonatal Outcomes
Primary Neonatal Outcome: neonatal intensive care unit (NICU) admission.
Secondary Neonatal Outcomes: birth weight, 5-minute Apgar score.
Time Points and Frequency
Temperature Monitoring: Record axillary temperature hourly. If the temperature is ≥37.5 C, record every 30 minutes until the end of labor.
Fetal Heart Rate (FHR): Obtain via continuous electronic fetal monitoring (EFM).
Time of Rupture of Membranes: Record precisely to the minute and update dynamically until the end of labor.
Maternal Vital Signs (Heart Rate, Blood Pressure): Record every hour. If abnormalities occur (such as heart rate >100 beats per minute), real-time alerts will be triggered.
Amniotic Fluid Color Changes: For women with ruptured membranes, record the color of amniotic fluid in real time during each vaginal examination.
Variables Extracted
Variable Coding Definitions (Table 1).
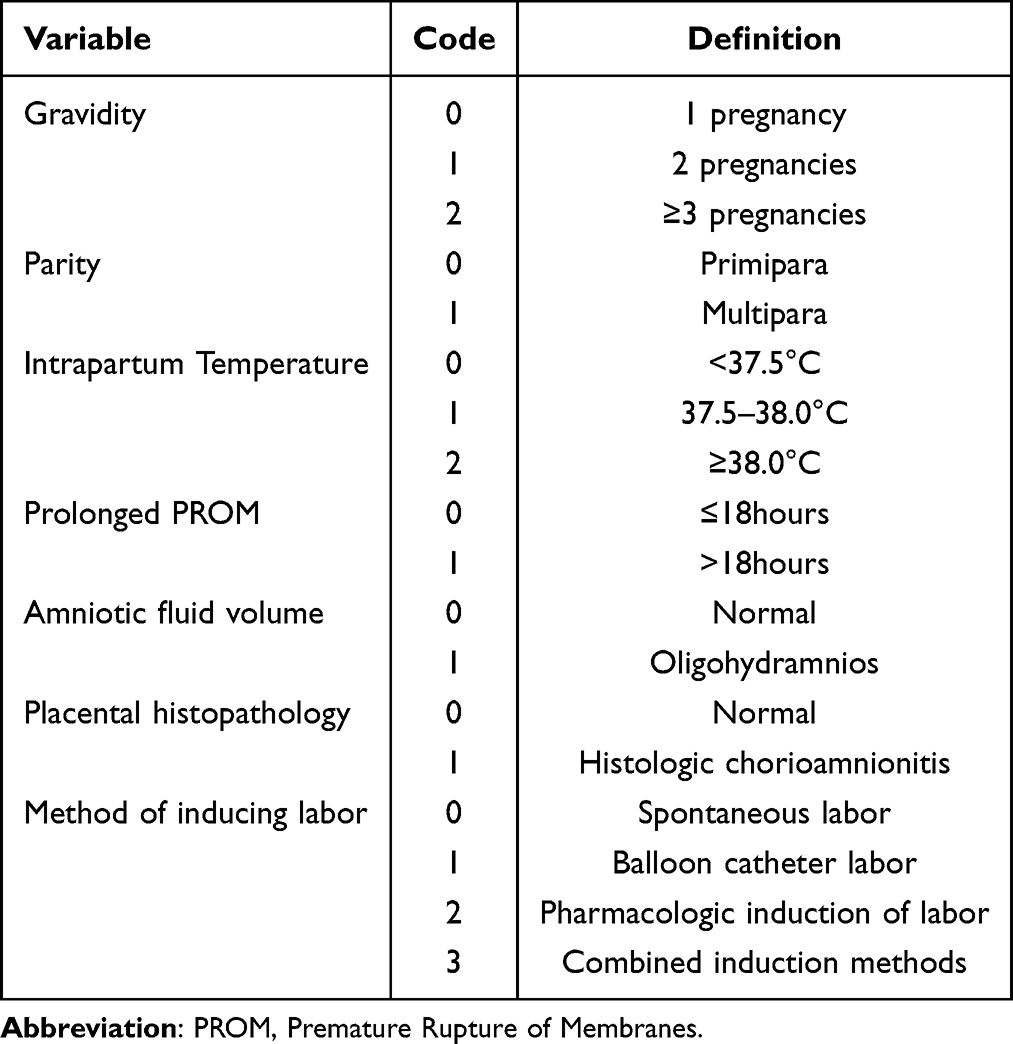 |
Table 1 Variable Coding Definitions |
Statistical Analysis
Continuous Variables: Described as mean±standard deviation (SD) if normally distributed, or median (interquartile range, IQR) if not normally distributed.
Categorical Variables: Analyzed using the Chi-square test or Fisher’s exact test (for small expected frequencies). Dummy variable encoding was applied to categorical predictors in regression modeling.
Group Comparisons
Two Independent Groups: Independent samples t-test (for normally distributed data) or Mann–Whitney U-test (for non-normally distributed data).
Three or More Independent Groups: One-way ANOVA (for normally distributed data) or Kruskal–Wallis test (for non-normally distributed data); post-hoc tests were conducted if significant differences were found.
Model Development
Variables with potential associations (P<0.05) in univariable analyses were included in multivariable logistic regression modeling. Independent predictors were selected using backward stepwise elimination to minimize Akaike’s Information Criterion (AIC). Clinically relevant variables (such as ART, placental histopathology) that contributed to AIC reduction were retained regardless of their statistical significance (P≥0.05), prioritizing model generalizability through AIC’s parsimony principle.
Model Validation
Predictive performance was assessed in a bootstrap-validated cohort (n=1000 resamples):
Discrimination: ROC analysis with AUC and 95% CI. Calibration: Calibration curves with bias-corrected smoothing; Brier score (scale 0–1, lower values indicate better accuracy). Internal Validation: Calibration accuracy was further evaluated using the Brier score and Hosmer-Lemeshow goodness-of-fit test to assess calibration discrepancy. Calibration curves were used to compare predicted and observed outcomes.
Additionally, to assess model stability and generalization, the data were randomly split into training and test sets at an 8:2 ratio for model development and validation, respectively.
All analyses were conducted using R software (version 4.2.3; R Foundation for Statistical Computing, Vienna, Austria). A P-value<0.05 was considered statistically significant.
Results
General Characteristics
From January 1, 2019 to December 31, 2021, a total of 15,085 pregnant women planned a vaginal birth at a Maternal and Child Health Care Hospital. Following the application of predefined inclusion and exclusion criteria, 1,047parturients were included in the study. Eight hundred thirty-seven participants formed a training set. The remaining women formed a testing set. The Participants recruitment flowchart is shown in Figure 1.
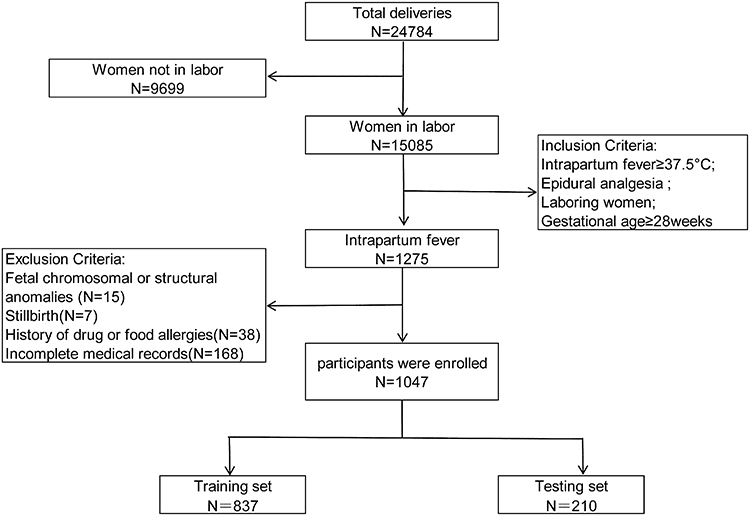 |
Figure 1 Participants recruitment flowchart. |
Table 2 presents the general demographic characteristics and perinatal factors of the training and the testing sets. No statistically significant difference was found between the two groups.
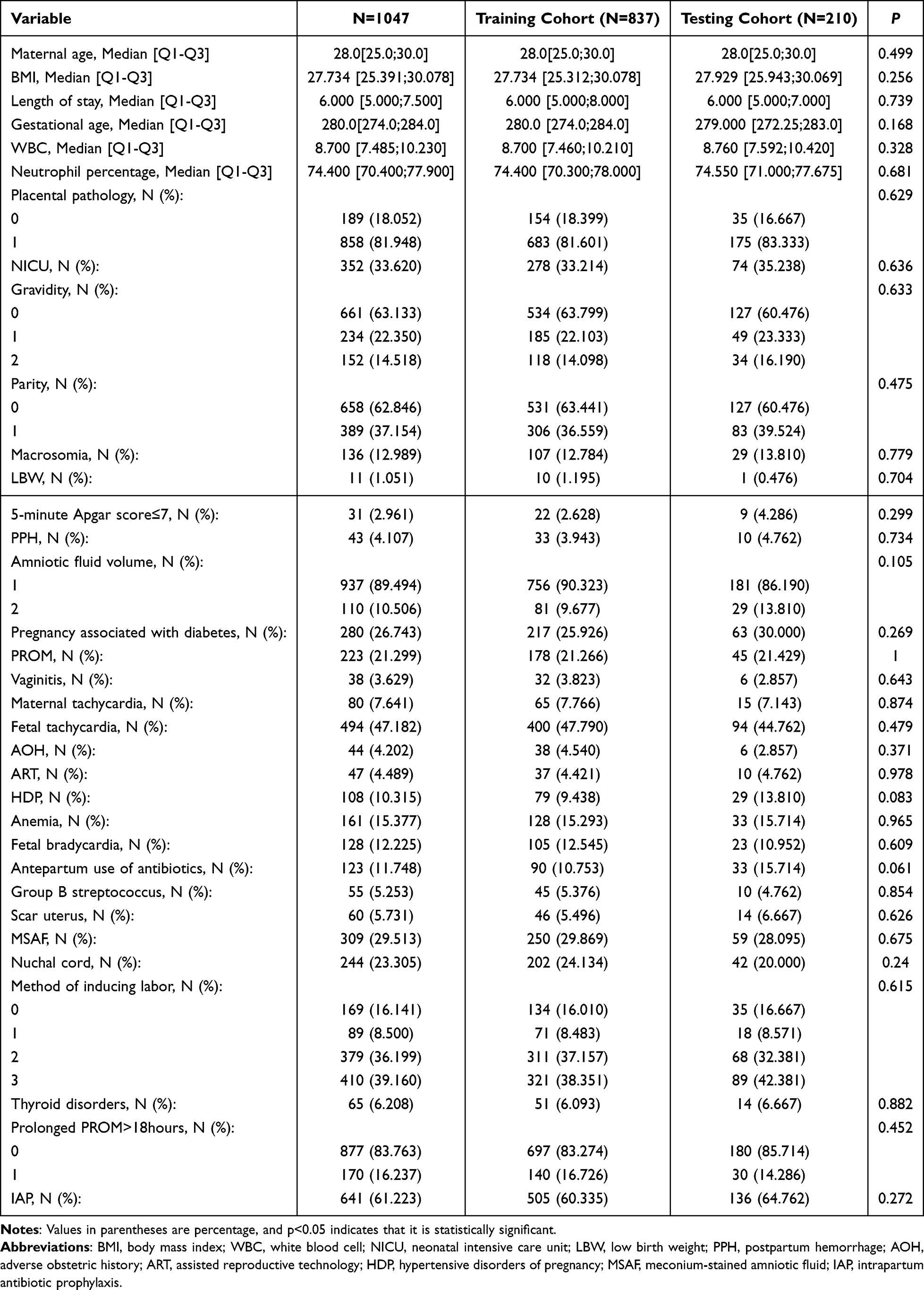 |
Table 2 Comparison of Demographic Characteristics and Perinatal Factors Between the Training and the Testing Sets |
Risk Factor Analysis
Univariate analysis for maternal outcomes (mode of delivery) identified significant differences in maternal age, BMI, gestational age, thyroid disorders, intrapartum antibiotic prophylaxis (IAP), meconium-stained amniotic fluid (MSAF), macrosomia, postpartum hemorrhage (PPH), abnormal amniotic fluid volume, adverse obstetric history, assisted reproductive technology (ART), hypertensive disorders of pregnancy (HDP), maternal tachycardia, intrapartum temperature and method of inducing labor (P < 0.05). Multivariate logistic regression using backward stepwise selection identified maternal age, intrapartum antibiotic prophylaxis, meconium-stained amniotic fluid, macrosomia, postpartum hemorrhage, Oligohydramnios, hypertensive disorders of pregnancy, method of inducing labor, maternal tachycardia, and intrapartum temperature as independent predictors of maternal pregnancy termination methods (P < 0.05, Table 3). These variables were incorporated into the nomogram for predicting the mode of delivery.
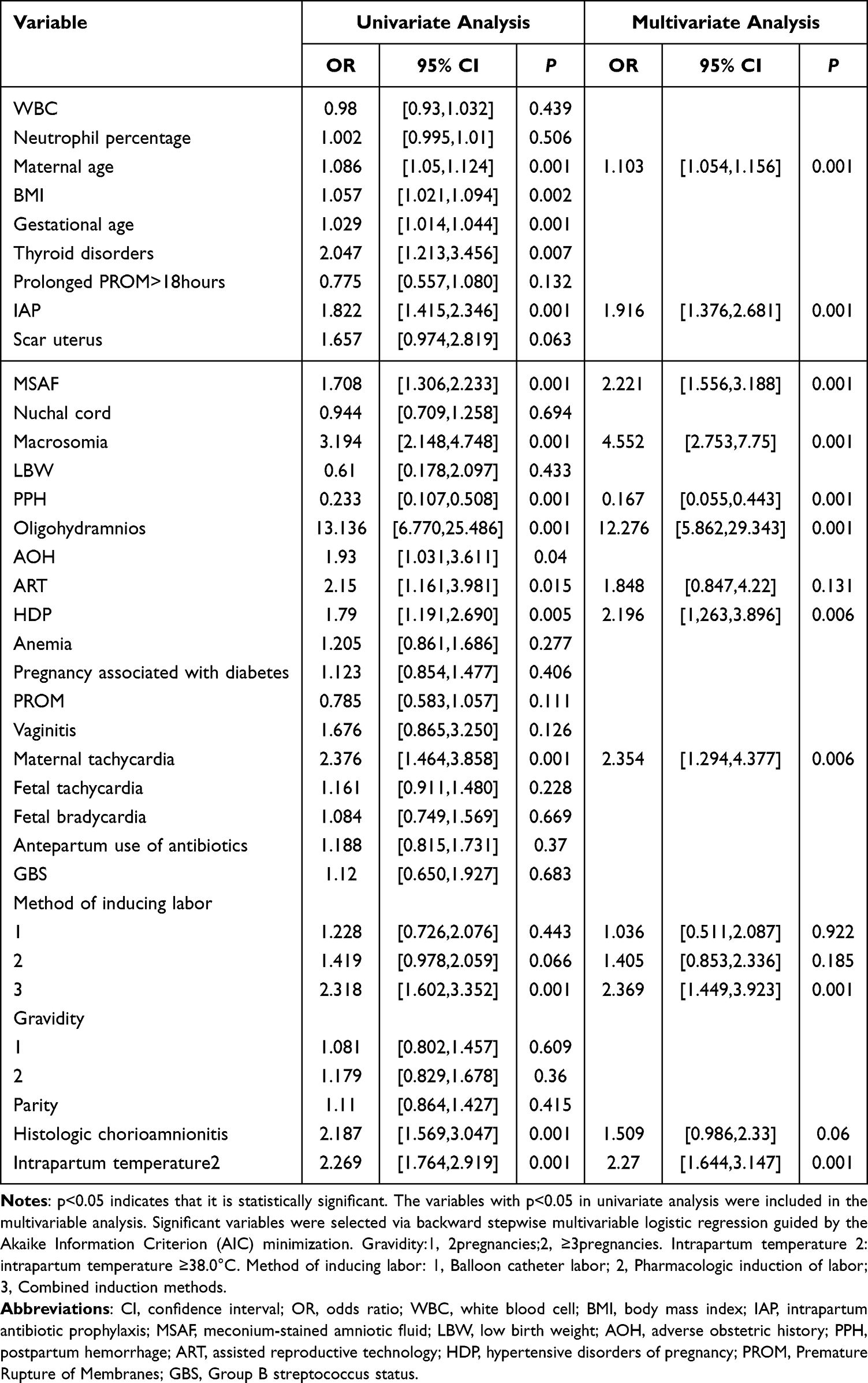 |
Table 3 Univariate and Multivariate Logistic Regression Analysis of Predictors in the Training Set (Mode of Delivery) |
Establishment, Evaluation, and Verification of Prediction Model
The nomogram for predicting the mode of delivery in women with intrapartum fever is shown in Figure 2. Variables demonstrating nonsignificant associations in multivariable analysis (P ≥ 0.05, such as ART and Histologic chorioamnionitis) were retained in the nomogram when contributing to AIC reduction. Each risk factor is assigned points on a variable axis, and the total points are summed to determine the predicted probability of cesarean delivery. The optimal cutoff value was determined using Youden’s index method as 0.475, effectively stratifying patients into high-risk and low-risk groups. The cutoff value for total points was identified as 181.507.
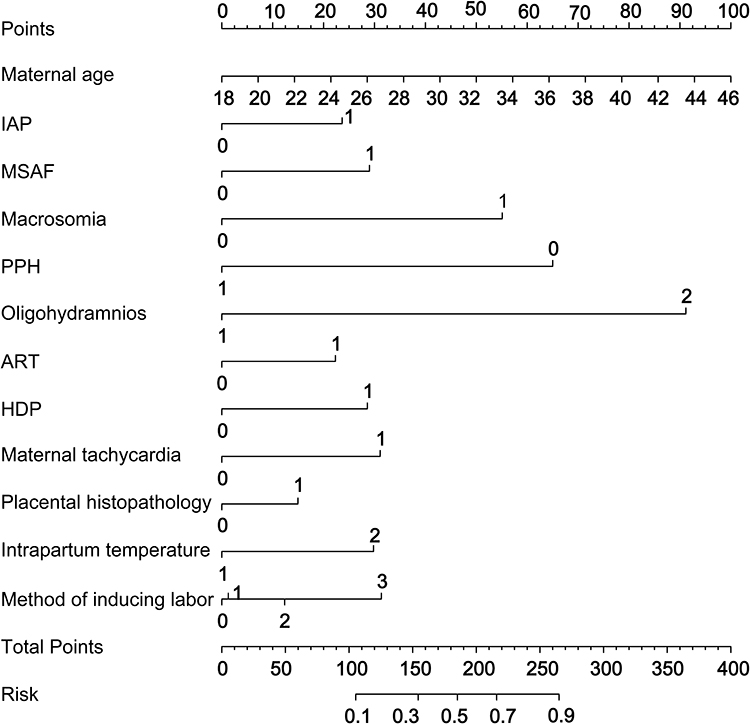 |
Figure 2 Nomogram for Predicting Mode of Delivery Based on Risk Factors for Intrapartum Fever. |
The nomogram demonstrated good accuracy with an AUC of 0.8 (95% CI: 0.77–0.83) in the training set and 0.783 (95% CI:0.722–0.844) in the testing set. (Figure 3) Brier scores were 0.182 and 0.192 for the training and testing sets, respectively. The risk estimate had a good calibration curve of the training set and the testing set. The Hosmer-Lemeshow goodness-of-fit test showed adequate model fit (P = 0.772) (Figure 4).
 |
Figure 3 (A) The receiver operating characteristic (ROC) curves of the nomogram for the training set. (B) The receiver operating characteristic (ROC) curves of the nomogram for the testing set B. |
 |
Figure 4 Calibration curves of the nomogram for predicting Mode of Delivery. (A) Training set. (B) Testing set. Note: The calibration curve was constructed using nonparametric bootstrap resampling with 1,000 iterations. |
For neonatal outcomes (NICU admission), univariate analysis identified significant differences in gestational age, scarred uterus, meconium-stained amniotic fluid, LBW, AOH, maternal tachycardia, fetal tachycardia, and fetal bradycardia (P < 0.05). Multivariate logistic regression identified meconium-stained amniotic fluid, low birth weight, adverse obstetric history, maternal tachycardia, fetal tachycardia, and fetal bradycardia as independent predictors of neonatal intensive care unit (P < 0.05, Table 4). These variables were incorporated into the nomogram for predicting NICU admission.
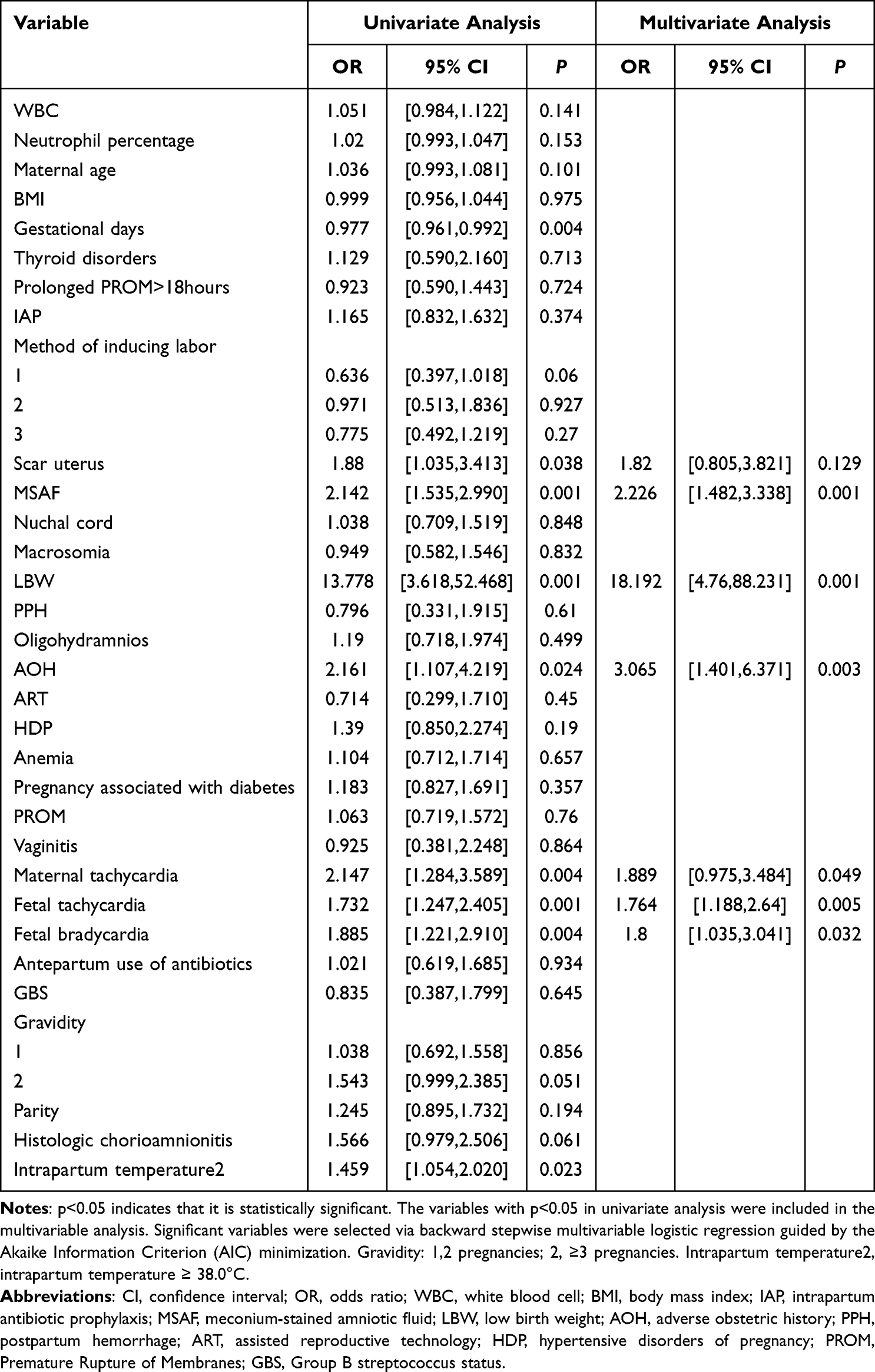 |
Table 4 Univariate and Multivariate Logistic Regression Analysis of Predictors in the Training Set (Neonatal Intensive Care Unit) |
The nomogram for predicting NICU admission in neonates born to women with intrapartum fever is shown in Figure 5. The optimal cutoff value for the model was 0.2. The nomogram demonstrated good accuracy with an AUC of 0.681 (95% CI: 0.630–0.732) in the training set and 0.748 (95% CI: 0.667–0.829) in the testing set. (Figure 6) The Brier scores were 0.120 and 0.161 for the training and testing sets, respectively. The risk prediction model demonstrated well-aligned calibration performance in both the training and validation sets. The Hosmer-Lemeshow goodness-of-fit test showed adequate model fit (P = 0.805) (Figure 7).
 |
Figure 5 Nomogram Predicting Risk Factors for Neonatal Intensive Care Unit Admission. |
 |
Figure 6 (A) The receiver operating characteristic (ROC) curves of the nomogram for the training set. (B) The receiver operating characteristic (ROC) curves of the nomogram for the testing set. |
 |
Figure 7 Calibration curves of the nomogram for predicting NICU. (A) Training set. (B) Testing set. Note: The calibration curve was constructed using nonparametric bootstrap resampling with 1,000 iterations. |
Discussion
Key Findings and Innovation
Presently, existing models for intrapartum fever mainly focus on predicting fever incidence or maternal and neonatal outcomes. However, there is a notable absence of models that can facilitate preventive measures against its adverse effects.20,21 In this large-scale retrospective study, we identified dynamic risk factors for intrapartum fever and developed the first nomogram to predict both delivery mode and NICU admission in this population.
Our model uniquely integrates real-time parameters (such as maternal / fetal heart rate trends, meconium-stained amniotic fluid) with static clinical variables. It outperformed traditional tools such as the Obstetric Comorbidity Index (OBCI)19 and single-biomarker models like the Perfusion Index (PI),23 demonstrating significant advantages in predictive accuracy and clinical utility. The OBIC relies on static data from the time of patient admission or early pregnancy and does not incorporate dynamic intrapartum indicators, a limitation that restricts its clinical applicability. Our model, by incorporating dynamic variables, enables real-time decision-making regarding the need for cesarean delivery to terminate pregnancy and the risk of NICU admission after fetal delivery, thereby identifying high-risk patients earlier than traditional methods.
Traditional models such as the Pulse PI and Neutrophil-to-Lymphocyte Ratio (NLR)24 prediction models are limited to predicting the occurrence of intrapartum fever but do not address the risk of cesarean delivery or NICU admission for neonates. The Pulse PI requires measurement of the pulse perfusion in the second toe of the right foot while the woman is in the supine position, which is susceptible to maternal emotions, movements, contractions, and changes in position. The NLR, although non-invasive and low-cost, is limited by physiological fluctuations during pregnancy, dehydration, and stress responses, leading to a higher rate of false positives. Our nomogram, developed from a large sample size with complete case records, is not affected by maternal position, physiological changes during pregnancy, or stress responses during labor. It provides a more accurate assessment of the risks associated with intrapartum fever.
The application of machine learning in pregnancy-related diseases and complications is relatively novel and has increased in recent years.25 Despite significant advancements in pregnancy and perinatal-related research using machine learning, several challenges and limitations remain. Complex algorithms, such as deep learning,26 require substantial computational resources and have poorer interpretability. Moreover, how to fully utilize information from electronic health records (EHRs) while protecting patient privacy remains a contentious issue. Reliance on static features: relying solely on prenatal baseline data, such as BMI and history of chronic diseases,27 leads to lagging predictions.28 Our study model addresses these issues by incorporating dynamic monitoring indicators and updating parameters hourly to achieve real-time risk scoring. Unlike traditional machine learning models that often require customized software or cloud support,29 our nomogram-based model can be directly integrated into existing labor and delivery monitoring systems. It adapts to real-time changes during labor without the need for complex detection equipment, as it relies on routine clinical parameters for risk assessment, making it suitable for widespread adoption in primary hospitals.
Mechanistic Insights
The association of intrapartum fever with maternal tachycardia and meconium-stained amniotic fluid (P < 0.01) underscores the likely role of infection and systemic inflammation. Maternal tachycardia (heart rate >100 bpm), a surrogate for systemic inflammatory response syndrome (SIRS),30 correlated with elevated pro-inflammatory cytokines (IL-6, TNF-α; OR = 2.26, P = 0.008).31 Non-infectious contributors, such as epidural analgesia (administered to all participants), may further exacerbate fever via hypothalamic thermoregulatory disruption.9,32 While advanced maternal age was associated with higher risk (OR = 1.106), meta-analyses suggest this may reflect confounding by assisted reproductive technology (ART) induced immune dysregulation (such as Th1/Th2 imbalance)31,33 or surveillance bias. Similarly, antibiotic use reduced GBS risk (RR = 0.29) but correlated with higher maternal risk (OR = 2.05), emphasizing the need for judicious use.34
Strengths and Limitations
This study has limitations, including its retrospective, single-center design. However, the strengths—including placental histopathological examination for all febrile parturients, a large sample size (n=24,784), universal administration of intrapartum obstetric analgesia, TRIPOD-guided validation protocols, and an 8:2 training-test set split—collectively mitigate potential biases. Unlike static models (such as OBCI, PI) or machine learning algorithms with high computational demands, our nomogram offers three key advantages. Dynamic adaptability: Real-time updates (such as adjusting risk weights when amniotic fluid color changes) enable proactive interventions. Clinical practicality: Uses routine monitoring data (such as vital signs, EFM) without requiring specialized equipment or complex software. Comprehensive outcomes: Predicts both cesarean delivery and NICU admission—unlike PI/NLR models limited to fever prediction alone. The PI’s susceptibility to maternal movement and NLR’s false positives from pregnancy-related physiological fluctuations further highlight our model’s robustness.
The nomograms developed in this study not only exhibit good predictive performance but also possess clear clinical application value. By transforming complex models into intuitive tools, this study helps promote the transition of risk prediction from “research” to “bedside”. In the future, exploration can be conducted to embed these nomograms into hospital information systems, enabling automatic scoring and early warning, which will facilitate the construction of smart obstetrics.
Conclusion
In this study, we developed and validated two novel nomograms that dynamically integrate intrapartum parameters with well-established clinical predictors to assess the risks of cesarean delivery and neonatal intensive care unit (NICU) admission in women with intrapartum fever. Unlike conventional static models, our tools enable real-time risk stratification, which addresses a key limitation of existing prediction systems. These nomograms provide clinicians with an evidence-based, actionable framework to enhance obstetric decision-making—with the potential to support more targeted perinatal care—though the specific impact of their clinical application on maternal and neonatal outcomes requires further verification in prospective interventional studies.
Nomograms Offer Several Advantages
- Enhanced accuracy via continuous parameter updates (such as dynamic adjustment of risk weights for continuous electronic fetal monitoring or maternal tachycardia).
- Clinical feasibility, as they rely on routinely collected labor data without requiring specialized equipment.
- Dual-outcome prediction, enabling simultaneous assessment of operative delivery risk and neonatal resuscitation needs, thereby improving preparedness.
Further multicenter prospective studies are needed to validate these models across diverse populations. If widely implemented, this approach may reduce adverse outcomes by facilitating timely interventions in high-risk labors.
Abbreviations
NICU, Neonatal Intensive Care Unit; IAP, Intrapartum Antibiotic Prophylaxis; MSAF, Meconium-Stained Amniotic Fluid; PPH, Postpartum Hemorrhage; HDP, Hypertensive Disorders of Pregnancy; LBW, Low Birth Weight; PI, Perfusion Index; OBCI, Obstetric Comorbidity Index; BMI, body mass index; WBC, white blood cell; PROM, Premature Rupture of Membranes; AOH, adverse obstetric history; ART, assisted reproductive technology; AIC, Akaike Information Criterion.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Huai’an Maternal and Child Health Hospital (Approval No. 2023028). The requirement for written informed consent was waived, as the research involved the analysis of pre-existing de-identified clinical data and posed no more than minimal risk to participants.
Acknowledgments
The authors gratefully acknowledge Professor Liu Jin, MD (Clinical Medicine Research Institution, The First Affiliated Hospital of Nanjing Medical University) and Professor Tang Shaowen, MD (Department of Epidemiology and Biostatistics, School of Public Health, Nanjing Medical University, Nanjing, China.) for their intellectual leadership in study design and rigorous evaluation of statistical methodologies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Ge Y, Zhang C, Cai Y, Huang H. Adverse maternal and neonatal outcomes in women with elevated intrapartum temperature complicated by histological chorioamnionitis at term: a propensity-score matched study. Front Pediatr. 2021;9:654596. doi:10.3389/fped.2021.654596
2. Zhang Z, Deng CM, Ma JH, Li S, Lei B, Ding T. Effects of neuraxial labor analgesia on intrapartum maternal fever in full-term pregnancy and its influence on birth outcomes. Front Med. 2023;10:1208570. doi:10.3389/fmed.2023.1208570
3. Jia L, Cao H, Guo Y, et al. Evaluation of epidural analgesia use during labor and infection in full-term neonates delivered vaginally. JAMA Network Open. 2021;4(9):e2123757. doi:10.1001/jamanetworkopen.2021.23757
4. An H, Zheng W, Zhu Q, Wen H. Retrospective study of intrapartum fever in term pregnancies and adverse obstetric and neonatal outcomes. PeerJ. 2022;10:e14242. doi:10.7717/peerj.14242
5. Abu Shqara R, Glikman D, Jad S, Rechnitzer H, Lowenstein L, Frank Wolf M. Antibiotic treatment of women with isolated intrapartum fever vs clinical chorioamnionitis: maternal and neonatal outcomes. Am J Obstet Gynecol. 2023;229(5):540.e541–540.e549. doi:10.1016/j.ajog.2023.05.013
6. Goetzl L. Maternal fever in labor: etiologies, consequences, and clinical management. Am J Obstet Gynecol. 2023;228(5s):S1274–s1282. doi:10.1016/j.ajog.2022.11.002
7. Impey L, Greenwood C, MacQuillan K, Reynolds M, Sheil O. Fever in labour and neonatal encephalopathy: a prospective cohort study. Bjog. 2001;108(6):594–597. doi:10.1111/j.1471-0528.2001.00145.x
8. Towers CV, Yates A, Zite N, Smith C, Chernicky L, Howard B. Incidence of fever in labor and risk of neonatal sepsis. Am J Obstet Gynecol. 2017;216(6):596.e591–596.e595. doi:10.1016/j.ajog.2017.02.022
9. Patel S, Ciechanowicz S, Blumenfeld YJ, Sultan P. Epidural-related maternal fever: incidence, pathophysiology, outcomes, and management. Am J Obstet Gynecol. 2023;228(5s):S1283–S1304.e1281. doi:10.1016/j.ajog.2022.06.026
10. Cornet MC, Kuzniewicz MW, Scheffler AW, et al. Epidural analgesia during labor and neonatal hypoxic-ischemic encephalopathy. JAMA Network Open. 2024;7(9):e2433730. doi:10.1001/jamanetworkopen.2024.33730
11. Hensel D, Zhang F, Carter EB, et al. Severity of intrapartum fever and neonatal outcomes. Am J Obstet Gynecol. 2022;227(3):513.e511–513.e518. doi:10.1016/j.ajog.2022.05.031
12. Hu YF. Induction of labor at the 39th week and cesarean delivery: a retrospective study in a Shanghai-based maternity hospital. Eur Rev Med Pharmacol Sci. 2023;27(6):2552–2560. doi:10.26355/eurrev_202303_31789
13. Conde-Agudelo A, Romero R, Jung EJ, Garcia Sánchez ÁJ. Management of clinical chorioamnionitis: an evidence-based approach. Am J Obstet Gynecol. 2020;223(6):848–869. doi:10.26355/eurrev_202303_31789
14. Onoh RC, Eze JN, Ezeonu PO, Lawani LO, Iyoke CA, Nkwo PO. A 10-year appraisal of cesarean delivery and the associated fetal and maternal outcomes at a teaching hospital in southeast Nigeria. Int J Womens Health. 2015;7:531–538. doi:10.2147/ijwh.S81338
15. Cresswell JA, Alexander M, Chong MYC, et al. Global and regional causes of maternal deaths 2009-20: a WHO systematic analysis. Lancet Glob Health. 2025;13(4):e626–e634. doi:10.1016/s2214-109x(24)00560-6
16. Costa ML, Cecatti JG. Urgent and decisive action needed in maternal morbidity and mortality to prevent stagnation in progress. Lancet Glob Health. 2025;13(4):e600–e601. PubMed PMID: 40064190. doi:10.1016/s2214-109x(25)00069-5
17. Chaemsaithong P, Sahota DS, Poon LC. First trimester preeclampsia screening and prediction. Am J Obstet Gynecol. 2022;226(2s):S1071–S1097.e1072. doi:10.1016/j.ajog.2020.07.020
18. Cobo T, Aldecoa V, Figueras F, et al. Development and validation of a multivariable prediction model of spontaneous preterm delivery and microbial invasion of the amniotic cavity in women with preterm labor. Am J Obstet Gynecol. 2020;223(3):421.e421–421.e414. doi:10.1016/j.ajog.2020.02.049
19. Easter SR, Bateman BT, Sweeney VH, et al. A comorbidity-based screening tool to predict severe maternal morbidity at the time of delivery. Am J Obstet Gynecol. 2019;221(3):271.e271–271.e210. doi:10.1016/j.ajog.2019.06.025
20. Wang H, Yang Z, Wei S, et al. Perinatal outcomes and risk factors for epidural analgesia-associated intrapartum maternal fever: a retrospective study. J Matern Fetal Neonatal Med. 2023;36(1):2179383. doi:10.1080/14767058.2023.2179383
21. Liu B, Ling L, Jia F, et al. Development and validation of a machine learning model for predicting intrapartum fever using pre-labor analgesia clinical indicators: a multicenter retrospective study. BMC Pregnancy Childbirth. 2025;25(1):243. doi:10.1186/s12884-025-07203-0
22. Abuelezz I, Hassan A, Jaber BA, et al. Contribution of artificial intelligence in pregnancy: a scoping review. Stud Health Technol Inform. 2022;289:333–336. doi:10.3233/shti210927
23. Sun C, Ren S, Chen C, et al. Pulse perfusion index for predicting intrapartum fever during epidural analgesia. J Clin Anesth. 2022;80:110852. doi:10.1016/j.jclinane.2022.110852
24. Li K, Deng C, Sun D, et al. Predictive value of neutrophil-to-lymphocyte ratio on admission for intrapartum maternal fever in parturients undergoing epidural analgesia: a retrospective cohort study using propensity score-matched analysis. Int J Gynaecol Obstet. 2025;168(1):167–176. doi:10.1002/ijgo.15820
25. Islam MN, Mustafina SN, Mahmud T, Khan NI. Machine learning to predict pregnancy outcomes: a systematic review, synthesizing framework and future research agenda. BMC Pregnancy Childbirth. 2022;22(1):348. doi:10.1186/s12884-022-04594-2
26. Malani SN, Shrivastava D, Raka MS. A comprehensive review of the role of artificial intelligence in obstetrics and gynecology. Cureus. 2023;15(2):e34891. doi:10.7759/cureus.34891
27. Davidson L, Boland MR. Towards deep phenotyping pregnancy: a systematic review on artificial intelligence and machine learning methods to improve pregnancy outcomes. Brief Bioinform. 2021;22(5). doi:10.1093/bib/bbaa369
28. Mennickent D, Rodríguez A, Opazo MC, et al. Machine learning applied in maternal and fetal health: a narrative review focused on pregnancy diseases and complications. Front Endocrinol. 2023;14:1130139. doi:10.3389/fendo.2023.1130139
29. Dhombres F, Bonnard J, Bailly K, Maurice P, Papageorghiou AT, Jouannic JM. Contributions of artificial intelligence reported in obstetrics and gynecology journals: systematic review. J Med Internet Res. 2022;24(4):e35465. doi:10.2196/35465
30. Hrubaru I, Motoc A, Moise ML, et al. The predictive role of maternal biological markers and inflammatory scores NLR, PLR, MLR, SII, and SIRI for the risk of preterm delivery. J Clin Med. 2022;11(23):6982. doi:10.3390/jcm11236982
31. Smulian JC, Bhandari V, Vintzileos AM, et al. Intrapartum fever at term: serum and histologic markers of inflammation. Am J Obstet Gynecol. 2003;188(1):269–274. doi:10.1067/mob.2003.11
32. Mullington CJ, Malhotra S. Hyperthermia after epidural analgesia in obstetrics. BJA Educ. 2021;21(1):26–31. doi:10.1016/j.bjae.2020.08.004
33. Lédée N, Petitbarat M, Prat-Ellenberg L, et al. The next frontier in ART: harnessing the uterine immune profile for improved performance. Int J Mol Sci. 2023;24(14):11322. doi:10.3390/ijms241411322
34. Li S, Huang J, Chen Z, Guo D, Yao Z, Ye X. Antibiotic prevention for maternal group B streptococcal colonization on neonatal GBS-related adverse outcomes: a meta-analysis. Front Microbiol. 2017;8:374. doi:10.3389/fmicb.2017.00374
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics, Management, and Perinatal Outcomes of Third-Trimester Preeclampsia at a Tertiary Hospital in Vietnam: A Retrospective Descriptive Study
Nguyen KT, Bui TTT, To NTH, Phan QN, Dang NB, Le CTK, Tran NH
International Journal of Women's Health 2026, 18:619528
Published Date: 18 June 2026