Back to Journals » International Journal of General Medicine » Volume 17
Maternal and Neonatal Perinatal Outcomes of Singleton Pregnancies in Advanced-Age Women Undergoing IVF/ICSI-ET Compared with Spontaneous Conception: A Retrospective Propensity Score Matched Cohort Study
Authors Mao J, Yang G ![]() , Su Q
, Su Q ![]() , Zeng Z, Lin J, Kong L, Zhang L, Liu L, Yang Y
, Zeng Z, Lin J, Kong L, Zhang L, Liu L, Yang Y ![]() , Wu H
, Wu H
Received 8 September 2024
Accepted for publication 18 October 2024
Published 13 November 2024 Volume 2024:17 Pages 5249—5259
DOI https://doi.org/10.2147/IJGM.S490959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jingxia Mao,1,2,* Guibo Yang,1,3,* Qin Su,1,4,* Zhonghong Zeng,1 Jueying Lin,2 Lin Kong,3 Lidun Zhang,4 Lidan Liu,1 Yihua Yang,1 Hongbo Wu1
1Guangxi Reproductive Medical Center, The First Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China; 2Department of Obstetrics, The Fifth Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China; 3Department of Obstetrics, The Maternity and Child Health Care of Guangxi Zhuang Autonomous Region, Nanning, People’s Republic of China; 4Department of Obstetrics, The First People’s Hospital of Yulin, Yulin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongbo Wu; Yihua Yang, Guangxi Reproductive Medical Center, The First Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China, Email [email protected]; [email protected]
Objective: To assess the safety and efficiency of in vitro fertilization/ intracytoplasmic sperm injection and embryo transfer (IVF/ICSI-ET) on maternal and neonatal perinatal outcomes in women (≥ 40y) with singleton pregnancies.
Methods: This multi-center retrospective cohort study, carried out from January 2018 to June 2023, enrolled 1762 women (≥ 40y) with singleton pregnancies of at least 28 weeks. Participants were divided into two groups: the IVF/ICSI-ET group (204 cases) and the spontaneous conception (SC) group (1558 cases). After 1:2 propensity score matching (PSM), the two groups were compared for maternal and neonatal outcomes. The SC group (1558 cases) was further divided by age into the < 43 years group (1195 cases) and the ≥ 43 years group (363 cases) for subgroup analysis.
Results: Adverse maternal and neonatal outcomes were comparable between the IVF/ICSI-ET group and the SC group, with a higher cesarean section rate (78% vs 67.5%, P =0.013), an increased maternal ICU admissions rate (5.5% vs 1.3%, P =0.008), and a lower birth defects rate (1.1% vs 4.6%, P =0.037) in the IVF/ICSI-ET group. Subgroup analysis showed that women aged ≥ 43 years had higher incidences of gestational diabetes, gestational hypertension, cesarean section, and neonatal asphyxia compared to women aged < 43 years.
Conclusion: This study indicated IVF/ICSI-ET is relatively safe for women ≥ 40 years with singleton pregnancies. However, advanced maternal age deteriorated maternal and neonatal outcomes, and IVF/ICSI-ET further heightened the risk of cesarean section and maternal ICU admissions. Therefore, enhanced care and vigilance are crucial for women over 40 undergoing IVF/ICSI-ET.
Keywords: in-vitro fertilization, intracytoplasmic sperm injection, advanced maternal age, maternal outcomes, neonatal outcomes
Introduction
As society progresses and attitudes towards fertility evolve, coupled with the widespread adoption of in vitro fertilization/intracytoplasmic sperm injection and embryo transfer (IVF/ICSI-ET) techniques, the global average age of pregnant women has been steadily increasing.1 This trend has greatly increased the proportion of pregnancies in women aged 35 years or older, which was defined as advanced maternal age by the International Federation of Gynecology and Obstetrics (FIGO). Advanced maternal age was not only associated with increased risks of adverse pregnancy outcomes for both the mother and fetus1 but also with increased IVF/ICSI-ET use,2 due to decreased ovarian reserve and poor egg quality.3 Therefore, an accurate assessment of the impact of IVF/ICSI-ET on maternal and neonatal outcomes in women of advanced age is crucial.
Since the birth of the first IVF baby in 1978, IVF/ICSI-ET technology has seen continuous improvements,4 leading to higher pregnancy and live birth rates. However, the use of superovulation simultaneously to mature multiple oocytes, along with the in vitro micromanipulation and culture for fertilization and early embryo development, has sparked controversy regarding their potential to increase adverse maternal-fetal outcomes. Previously, a review paper summarized that fresh embryo transfer was associated with a higher risk of small gestational age, low birth weight, and premature birth, while frozen embryo transfer was linked with large gestational age infants and preeclampsia, and ICSI may lead to a higher risk of premature rupture of membranes,5 birth defects and the transfer of poor semen quality to male offspring.6 But numerous studies suggested that subfertility, whether or not using IVF/ICSI-ET to achieve a pregnancy, may increase the risks of adverse maternal and perinatal outcomes7 independently, and infertility was often accompanied by inflammation, endocrine and metabolic disorders, which might be the reasons for the adverse maternal and perinatal outcomes.8 In addition, many previous studies had limited credibility due to their differences in baseline data, despite the application of logistic regression analyses to adjust for these variables. Finally, few studies focused on perinatal outcomes of older (≥40 years) women with IVF/ICSI-ET.
Therefore, this multicenter retrospective cohort study aimed to evaluate the safety and efficiency of IVF/ICSI-ET concerning maternal and neonatal perinatal outcomes among women aged 40 and older.
Materials and Methods
Study Population and Design
This study was a multi-center retrospective cohort study guided by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.9 The study complied with the Declaration of Helsinki.
The study protocol was approved by the Medical Ethics Committees of the First Affiliated Hospital of Guangxi Medical University (approval number:2023-E679-01, approval data:2023.11.30), the Fifth Affiliated Hospital of Guangxi Medical University (approval number: LW2023-011, approval data:2023.12.13), the Maternity and Child Health Care of Guangxi Zhuang Autonomous Region (approval number:[2023]12–5, approval data:2023.12.19), and the First People’s Hospital of Yulin (approval number: YLSY- IRB-SR-2023073, approval data:2023.12.18). Written informed consent was waived by the ethics committees due to the retrospective nature of the study, and the privacy message of patients was highly protected.
The perinatal period is defined in China as the period from the 28th week of pregnancy (or when the baby weighs about 1000 g) to the end of the 1st week after birth. Based on the perinatal definition, maternal and neonatal data spanning January 2018 to June 2023 were extracted through the electronic medical record system of the aforementioned tertiary hospitals. The inclusion criteria were as follows: 1. spontaneous conception or IVF/ICSI-ET assisted conception; 2. women aged ≥40 years; 3. singleton pregnancy delivered in the hospital; 4. gestational age ≥28 weeks or birth weight ≥1000 g. The exclusion criteria were: 1. twin and multiple pregnancies; 2. women using donor oocytes; 3. incomplete maternal and neonatal information.
Definition of Study Groups
A total of 1788 women aged ≥40 years were hospitalized for delivery. Of these, 20 women with incomplete information and 6 women who did not meet perinatal diagnostic criteria were excluded. Finally, 1762 women were successfully enrolled and divided into two groups according to their mode of conception: the IVF/ICSI-ET group (204 cases) and the spontaneous conception group (SC, 1558 cases). Given the statistically significant differences in baseline characteristics between the two groups, we implemented a 1:2 propensity score matching strategy to minimize these disparities. This approach resulted in the successful matching of 182 women from the IVF/ICSI-ET group with 305 women from the SC group, and maternal and neonatal outcomes were subsequently compared.
Subsequently, to study the effect of maternal age on maternal and neonatal outcomes the SC group (1558 cases) was divided into two subgroups: age ≥43 years (363 cases) and age <43 years (1195 cases). This age cut-off was chosen because of the limited number of women over 43 years of age. There were no statistically significant differences in baseline information between the two subgroups, so propensity score matching was not necessary in this analysis. In contrast, no subgroup analyses were performed in the IVF/ICSI-ET group because of the small sample size (Figure 1).
 |
Figure 1 Flow chart of the study. Abbreviations: IVF/ICSI-ET, in vitro fertilization/ intracytoplasmic sperm injection and embryo transfer; PSM, propensity score matching; SC, spontaneous conception. |
Measurement Outcomes
Demographic and clinical data were extracted from electronic medical records, and the data collectors were blinded to the objectives of our study to minimize potential bias.
Maternal outcomes included a range of maternal complications, such as fetal distress, premature birth, postpartum hemorrhage (PPH), premature rupture of membranes (PROM), placental abruption, abnormal thyroid function, placenta previa, gestational diabetes mellitus (GDM), hypertensive disorders of pregnancy (HDP), and hyperbileacidemia. Additionally, pregnancy outcomes such as gestational age at delivery, delivery mode (cesarean section or vaginal delivery), and maternal intensive care unit (ICU) admission were evaluated.
Neonatal outcomes included macrosomia (birth weight≥4000 g), low birth weight (LBW, less than 2500g at birth), mature low birth weight (MLBW, birth weight <2500 g with gestational age >37 weeks), asphyxia neonatorum, birth defects, neonatal pneumonia, pathological neonatal jaundice, perinatal deaths (defined as deaths of infants < 7 days old and fetal deaths at ≥ 28 weeks of gestation or with birth weight≥1000g), and neonatal intensive care unit (NICU) admission.
Statistical Analysis
This study did not include missing data, as women with incomplete information were excluded when enrolled. Continuous variables were presented as mean ± standard deviation (SD) if normally distributed and as median ± interquartile range (IQR) if not normally distributed. Categorical variables are presented mainly as frequency counts and proportions. Statistical analyses were performed using the Student’s t-test or the Mann–Whitney U-test for continuous variables and the chi-square test for categorical variables. To address the unbalanced baseline characteristics between the IVF and SC groups, we used 1:2 nearest neighbor propensity score matching (PSM) with a caliper width of 0.02 and without replacement to reduce selection bias. Patients who were not matched were excluded from the analyses. PSM was performed by R software, version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria), while statistical analyses were carried out using SPSS software, version 26.0 (SPSS Inc, Chicago, IL, USA). Relative risk (RR) was reported with a 95% CI. A 2-tailed P-value of less than 05 was considered statistically significant.
Results
IVF/ICSI-ET Treatment versus Spontaneous Conceptions
Demographics Characteristics
A total of 1762 women were recruited, with 204 in the IVF/ICSI-ET group and 1558 in the SC group. Significant differences were found in age, gravidity, and parity. To reduce differences in demographic characteristics, we used PSM with a ratio of 1:2 to adjust for the 7 variables (age, pre-pregnancy BMI, pre-delivery BMI, gravidity, parity, scarred uterus, and PGDM). After matching, there were 182 women in the IVF/ICSI-ET group and 305 women in the SC group, respectively (Table 1).
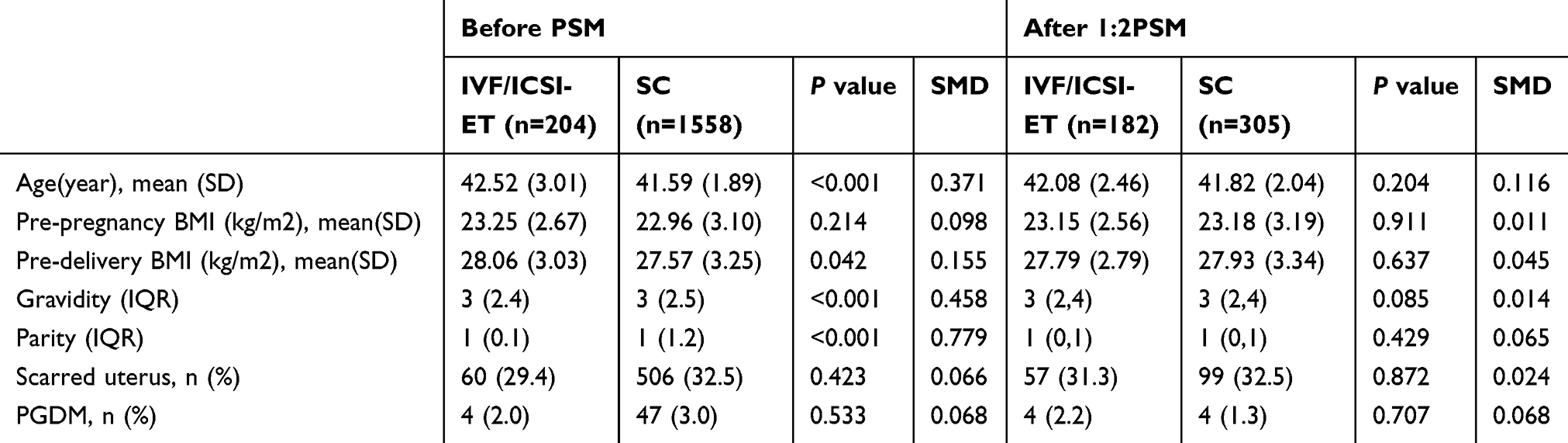 |
Table 1 Demographic Characteristics of the IVF/ICSI-ET Group and the SC Group |
Maternal Outcomes
There were no significant differences in maternal complications between the two groups, nor the gestational weeks of delivery. However, the IVF/ICSI-ET group had higher rates of cesarean section rate (78% vs 67.5%, P =0.013, RR 1.16, 95% CI 1.04–1.29) and maternal ICU admissions (5.5% vs 1.3%, P =0.008, RR 4.19, 95% CI 1.33–13.16) than the SC group (Figure 2).
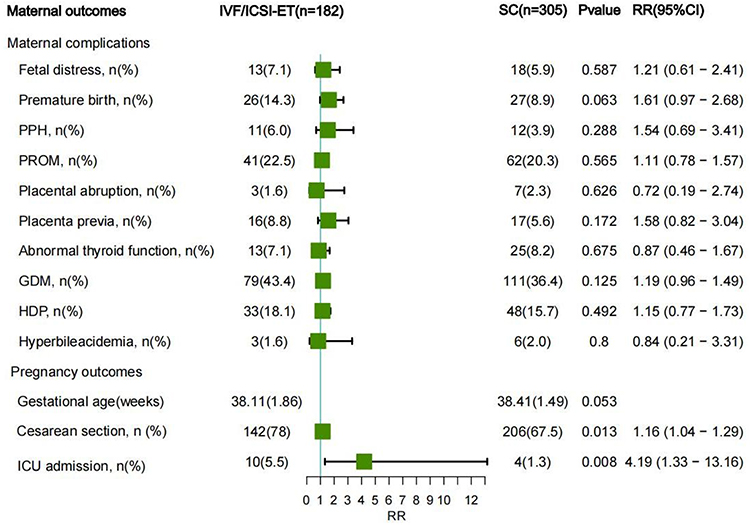 |
Figure 2 Maternal outcomes of the IVF/ICSI-ET group and the SC group. The rates of cesarean section and maternal ICU admission were significantly higher than the SC group. Abbreviations: PPH, Postpartum hemorrhage; PROM, premature rupture of membranes; GDM, gestational diabetes mellitus; HDP, hypertensive disorders of pregnancy; ICU admission, maternal intensive care unit admission. |
Neonatal Outcomes
The rate of birth defects (1.1% vs 4.6%, P =0.037, RR 0.24, 95% CI 0.06–1.04) in the IVF/ICSI-ET group was significantly lower than in the SC group. Although birth weight, rates of macrosomia, LBW, neonatal asphyxia, and NICU admissions were higher in the IVF/ICSI-ET group, and the rates of MLBM and pathological jaundice in the neonates were lower compared to the SC group, these differences were not statistically different (Figure 3).
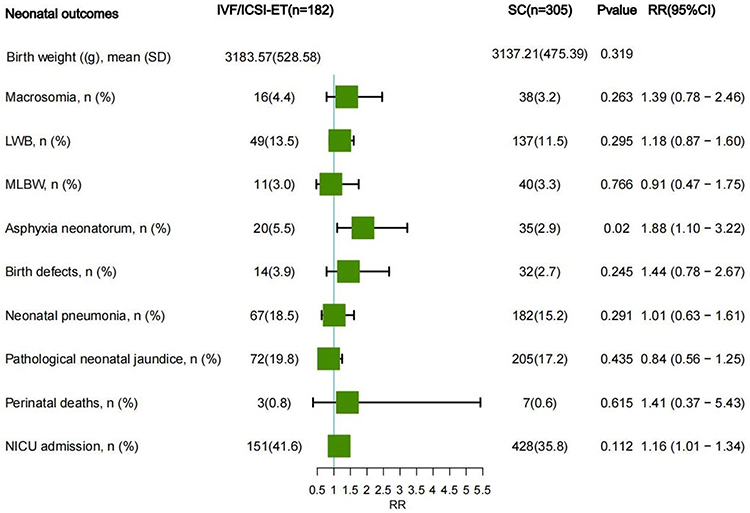 |
Figure 3 Neonatal outcomes of the IVF/ICSI-ET group and the SC group. The rate of birth defects in the IVF/ICSI-ET group was significantly reduced compared to the SC group. Abbreviations: LBW, low birth weight; MLBW, mature low birth weight; NICU admission, neonatal intensive care unit admission. |
Perinatal Deaths
The IVF/ICSI-ET group (204 cases) reported no cases of perinatal deaths, whereas the SC group (1558 cases) experienced 10 cases of perinatal deaths, which included 4 medically induced abortions and 6 fetal deaths. The causes of these perinatal deaths varied: fetal chromosomal abnormalities (1 case), fetal hydrocephalus (1 case), severe preeclampsia (2 cases), fetal cleft lip-palate and limb defects (1 case), umbilical cord factors (3 cases), unexplained stillbirth (1 case), and induced labor due to advanced maternal age (1 case) (Table 2).
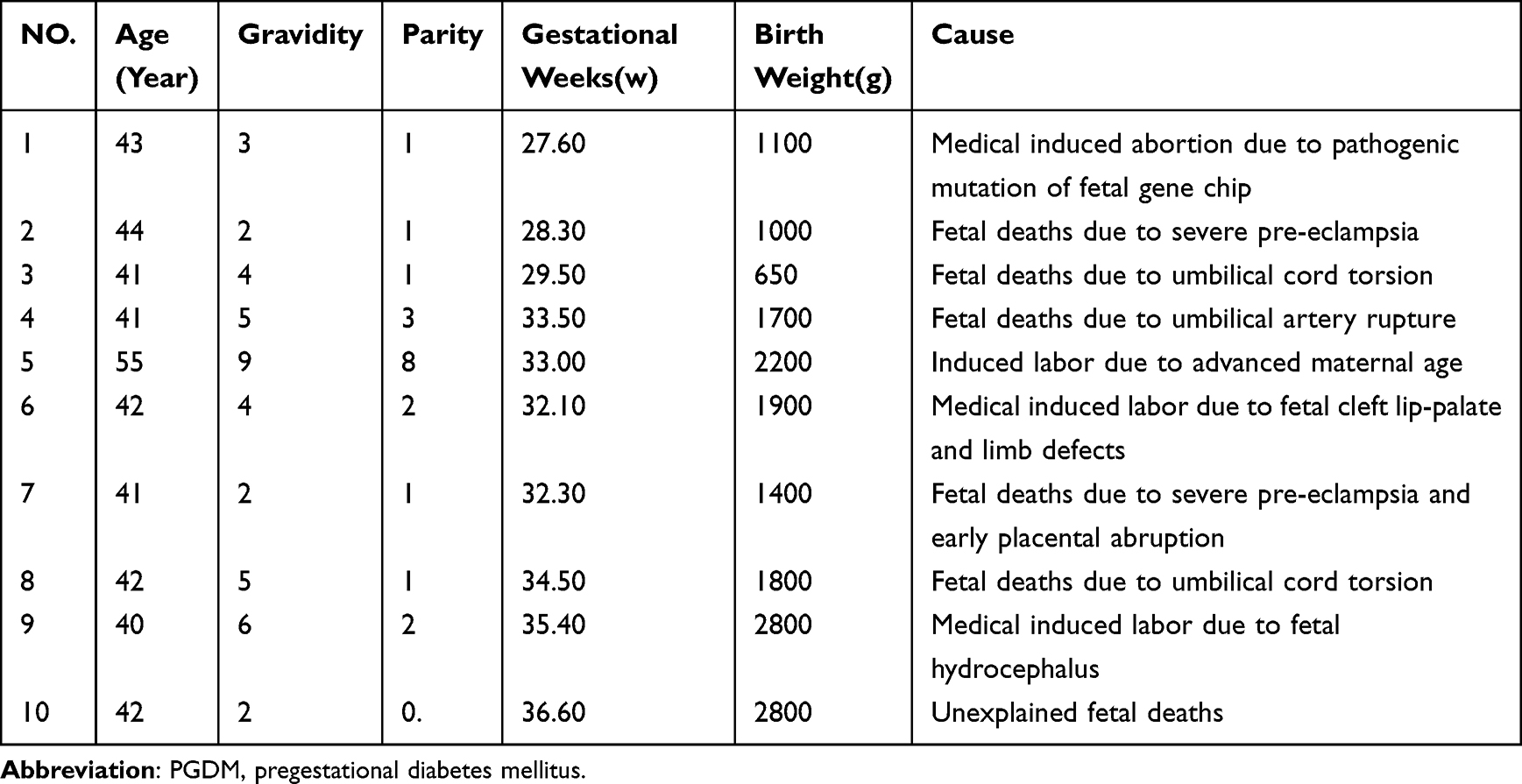 |
Table 2 Clinical Profiles of Perinatal Mortality in the SC Group |
Subgroup Analysis Among the SC Group
Demographics Characteristics
In the SC group, the 1558 cases were subdivided into the <43 years group (1376 cases) and the ≥43 years group (203 cases). There was no significant difference between the two subgroups (Table 3).
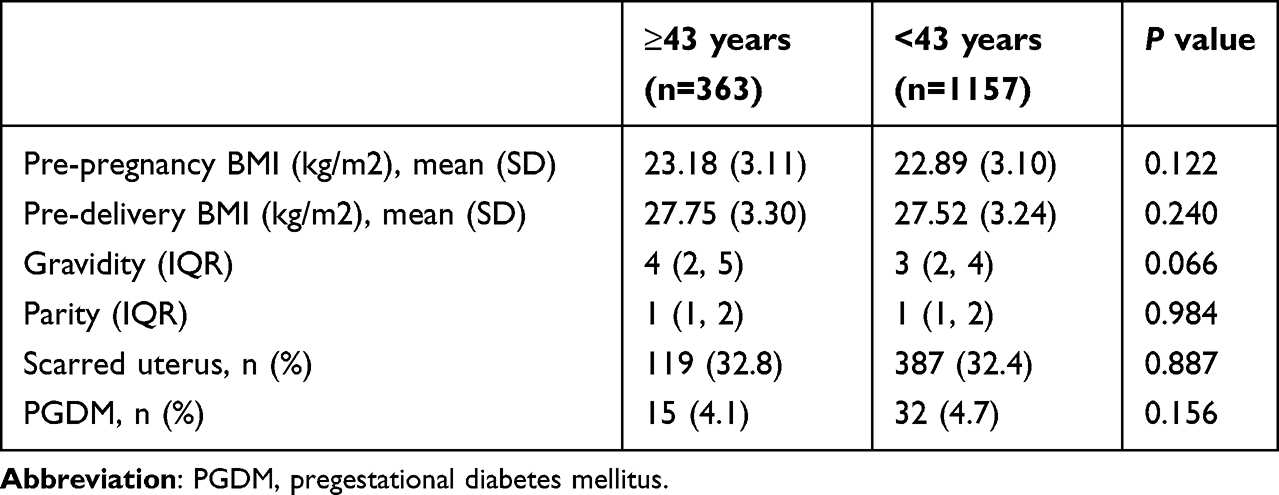 |
Table 3 Demographic Characteristics of the ≥43 Years Group and the <43 Years Group |
Maternal Outcomes
The rates of GDM (39.9% vs 32.15%, P = 0.005, RR 1.25, 95% CI 1.07–1.45) and HDP (23.7% vs 17.1%, RR 1.39, 95% CI 1.11–1.73) were significantly higher in the ≥43 years group than in the <43 years group and there were no significant differences in the rates of other pregnancy complications. The rate of cesarean section was also significantly higher in the ≥43 years group (68.6% vs 62.6%, P = 0.037, RR 1.10, 95% CI 1.01–1.19), while no differences were found in the gestational week of delivery and maternal ICU admissions (Figure 4).
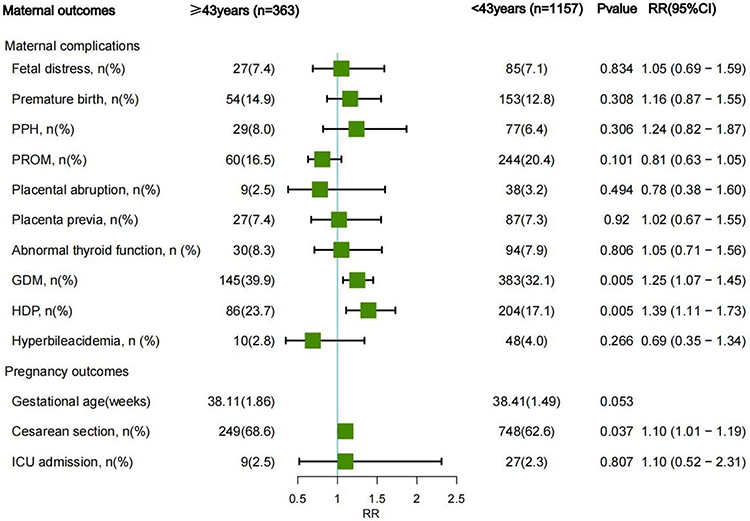 |
Figure 4 Maternal outcomes of the ≥ 43 years group and the <43 years group. The GDM, HDP, and cesarean section rates were significantly higher in the ≥43 years group than in the <43 years group. Abbreviations: PPH, Postpartum hemorrhage; PROM, premature rupture of membranes; GDM, gestational diabetes mellitus; HDP, hypertensive disorders of pregnancy. |
Neonatal Outcomes
The rate of neonatal asphyxia was significantly higher in the ≥43 years group than in the <43 years group (5.5% vs 2.9%, RR 1.88, 95% CI 1.10–3.22). However, there were no significant differences in birth weight or other neonatal outcomes between the two groups (Figure 5).
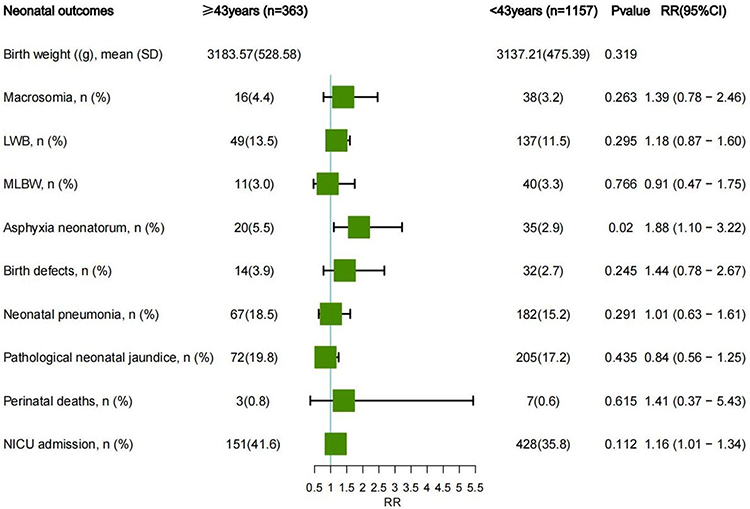 |
Figure 5 Neonatal outcomes of the≥ 43 years group and the <43 years group. The rate of neonatal asphyxia was significantly higher in the ≥43 years group than in the <43 years group. Abbreviations: LBW, low birth weight; MLBW, mature low birth weight; NICU admission, neonatal intensive care unit admission. |
Discussion
The trend of women postponing childbirth and policy changes like China’s three-child policy have indeed led to an increase in the number of older pregnant women, both conceiving naturally and by IVF/ICSI-ET. Although IVF/ICSI-ET has been documented as a relatively safe technology, its impact on maternal and neonatal risks in women aged 40 and above with singleton pregnancies of 28 weeks or more remains less studied. To address this issue, we conducted a retrospective analysis of maternal and perinatal data from women of advanced age across four tertiary hospitals. Our data showed that maternal complications and adverse neonatal outcomes were comparable between the IVF/ICSI-ET group and the SC group, except that the rates of cesarean section and maternal ICU admission were higher in the IVF/ICSI-ET group. Unexpectedly, the IVF/ICSI-ET group had lower rates of birth defects and perinatal deaths compared to the SC group, which reported 10 cases of perinatal deaths. Subgroup analysis of the SC group showed that the rates of GDM, HDP, cesarean section, and neonatal asphyxia were significantly higher in the ≥43 years group than the <43 years group.
IVF/ICSI-ET Did Not Increase the Risk of Maternal Complications
There was no statistical difference in maternal complications between the IVF/ICSI-ET group and the SC group, indicating that IVF/ICSI-ET would not further increase the risk of maternal complications in advanced-age women. However, this result was inconsistent with previous studies, which showed an increased risk of obstetric and perinatal complications,10 GDM,11 and postpartum hemorrhage12 in singleton pregnancies conceived through IVF/ICSI. One possible reason for these discrepancies may come from confounding factors. Notably, the significant difference in GDM between the two groups no longer existed after applying PSM, highlighting that selection bias or baseline imbalances are common limitations in observational studies.13 However, this problem can be partially solved by PSM.14 In addition, advancements in IVF techniques, such as blastocyst culture, vitrification, and single embryo transfer, may have lessened the adverse impacts of IVF/ICSI on pregnancy outcomes, rendering the differences between the two groups undetectable.
Many studies also showed that IVF/ICSI-ET is a safe technology for advanced-age women with singleton pregnancy.15,16 Furthermore, a recent long-term study17 found that IVF/ICSI-ET does not elevate the risk of cardiovascular issues in women. However, as maternal age increases, the prevalence of chronic conditions like pregestational diabetes and hypertension increases, along with a rise in pregnancy-related complications.18,19 This was also confirmed in our subgroup analyses, which showed that the rates of HDP and GDM were significantly higher in the ≥43 years group than in the <43 years group. A study found that the mortality rate in women of advanced maternal age was significantly higher than in young pregnant women, with hemorrhagic shock being the leading cause of maternal mortality in those aged ≥40 years, and over half of these cases are linked to HDP.20 Therefore, to reduce the risk of preeclampsia, aspirin is recommended for women aged ≥40 years with or without IVF/ICSI-ET21 at 12–16 weeks’ gestation. In addition, managing blood glucose levels is crucial since GDM can heighten the risk of maternal mortality later in life.22 Effective blood glucose control before pregnancy can also reduce the risk of metabolic disorders in the offspring.23
IVF/ICSI-ET Increased the Rates of Cesarean Section and Maternal ICU Admission
The cesarean section rate increased to 68.6% with maternal age in subgroup analyses,24–26 and further rose to 78% in the IVF/ICSI-ET group, likely due to the perceived preciousness of the IVF-conceived baby and medical environment.27 However, cesarean sections could elevate the risks of postpartum hemorrhage, infections, deep vein thrombosis, etc,28 further deteriorating maternal health and resulting in a higher rate of maternal ICU admissions in the IVF/ICSI-ET group. Therefore, unnecessary cesarean sections should be avoided to reduce adverse maternal outcomes, as IVF/ICSI-ET itself is not a medical indication for cesarean section, and advanced maternal age is safe for vaginal delivery in the absence of maternal and fetal complications.1
IVF/ICSI-ET Did Not Increase Adverse Neonatal Outcomes
Our results suggested that IVF/ICSI-ET might not affect birth weight or adverse neonatal outcomes during the perinatal period. Conversely, the IVF/ICSI-ET group showed a lower rate of birth defects after PSM. In addition, there were no perinatal deaths in the IVF/ICSI-ET group (204 cases), whereas there were 10 perinatal deaths in the SC group (1558 cases), including 4 medically induced abortions and 6 fetal deaths. While prior studies have suggested that birth defects remain more common in IVF/ICSI-ET infants29 and that the risk of stillbirth is significantly increased compared with natural conception.30 These inconsistencies can be interpreted through several lenses. Firstly, the definition of the perinatal period varies geographically: internationally, it spans from the 22nd week of pregnancy to 7 days post-birth, but in China, it extends from the 28th week of pregnancy to 7 days post-birth. Therefore, we only analyzed data on birth defects and perinatal mortality occurring after 28 weeks of gestation. Secondly, women undergoing IVF/ICSI-ET tend to access more obstetric care, which allows for the early detection of fetal defects and the possibility of inducing labor before 28 weeks if needed. Thirdly, the increase in obstetric care also brings more standardized management of pregnancy complications, such as pre-eclampsia, which in turn reduces the risk of perinatal deaths.
However, an expanding collection of research supports our findings. For instance, a study31 revealed no difference in SGA between IVF and natural pregnancies in the same mother. Another study32 indicated that the overall genetic diagnostic rate and incidence of newborn variations in infants conceived through IVF/CSI are similar to those conceived naturally. In addition, IVF/ICSI-ET had not been shown to influence cognitive and behavioral outcomes at 9 years of age,33 affect school-age developmental and educational outcomes,34 or increase the risk of obstetric or perinatal complications in offspring conceived and delivered by ART at the time of parenthood.35 Therefore, both short- and long-term outcomes in offspring suggest that IVF/ICSI-ET is a relatively safe technology, which offers hope to many parents wishing for a healthy child.36
Finally, subgroup analysis showed a higher rate of neonatal asphyxia with maternal age, verifying that advanced maternal age raises adverse neonatal outcomes, which is in line with previous studies. Studies demonstrated that advanced maternal age increases age-related malformations,37 chromosomal abnormalities, notably trisomy births,38 and discrepancies in birth weight, including both large and small for gestational age babies.39,40 Therefore, with or without IVF/ICSI-ET, health professionals need to be concerned about the risk of adverse neonatal outcomes in advanced maternal age.
Strengths and Limitations
This study has several strengths. Firstly, it was a multicenter cohort study conducted in not only provincial and municipal general hospitals but also general and specialist hospitals, which reduced selection bias. Secondly, all data were obtained from the inpatient system, which reduced recall bias. Lastly, PSM was used to reduce the influence of confounding factors and improve the reliability of the results. However, the study has limitations, including a lack of infertility diagnosis and a small sample size with a short follow-up. Therefore, ongoing longitudinal studies are needed to explore the long-term effects of IVF/ICSI-ET technology on women and children.
Conclusions
This study showed that IVF/ICSI-ET would not increase the risk of maternal and neonatal complications during the perinatal period in women aged ≥40 years, suggesting that IVF/ICSI is a relatively safe technology for advanced-age women. However, IVF/ICSI-ET heightened the risk of cesarean section and maternal ICU admissions. This study provides new insight for obstetricians and women of advanced maternal age considering IVF/ICSI-ET.
Data Sharing Statement
The data presented in this study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Natural Science Foundation of Guangxi Zhuang Autonomous Region (2019GXNSFFA245013); the National Natural Science Foundation of China (No.82360308); and the Guangxi Medical University Training Program for Distinguished Young Scholars. This research was also supported by the Special Fund of the Female Fertility Preservation Innovation Team of the First Affiliated Hospital of Guangxi Medical University.
Disclosure
The authors report there are no competing interests to declare.
References
1. Gantt A, Metz TD, Kuller JA, et al. Pregnancy at age 35 years or older: acog obstetric care consensus No. 11. Obstet Gynecol. 2022;140:348–366. doi:10.1097/AOG.0000000000004873
2. Levine AD, Boulet SL, Kissin DM. Contribution of assisted reproductive technology to overall births by maternal age in the United States, 2012–2014. JAMA. 2017;317:1272–1273. doi:10.1001/jama.2016.21311
3. Charalambous C, Webster A, Schuh M. Aneuploidy in mammalian oocytes and the impact of maternal ageing. Nat Rev Mol Cell Biol. 2023;24:27–44. doi:10.1038/s41580-022-00517-3
4. Rienzi L, Gracia C, Maggiulli R, et al. Oocyte, embryo and blastocyst cryopreservation in ART: systematic review and meta-analysis comparing slow-freezing versus vitrification to produce evidence for the development of global guidance. Hum Reprod Update. 2017;23:139–155. doi:10.1093/humupd/dmw038
5. Yu J, Ren J, Ren Y, et al. Using metabolomics and proteomics to identify the potential urine biomarkers for prediction and diagnosis of gestational diabetes. EBioMedicine. 2024;101. doi:10.1016/j.ebiom.2024.105008
6. Berntsen S, Söderström-Anttila V, Wennerholm U-B, et al. The health of children conceived by ART: “the chicken or the egg? Hum Reprod Update. 2019;25:137–158. doi:10.1093/humupd/dmz001
7. Luke B. Pregnancy and birth outcomes in couples with infertility with and without assisted reproductive technology: with an emphasis on US population-based studies. Am J Obstet Gynecol. 2017;217:270–281. doi:10.1016/j.ajog.2017.03.012
8. Vannuccini S, Clifton VL, Fraser IS, et al. Infertility and reproductive disorders: impact of hormonal and inflammatory mechanisms on pregnancy outcome. Hum Reprod Update. 2016;22:104–115. doi:10.1093/humupd/dmv044
9. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. STROBE initiative, the strengthening the reporting of observational studies in epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12:1495–1499. doi:10.1016/j.ijsu.2014.07.013
10. Pandey S, Shetty A, Hamilton M, Bhattacharya S, Maheshwari A. Obstetric and perinatal outcomes in singleton pregnancies resulting from IVF/ICSI: a systematic review and meta-analysis. Hum Reprod Update. 2012;18:485–503. doi:10.1093/humupd/dms018
11. Bosdou JK, Anagnostis P, Goulis DG, et al. Risk of gestational diabetes mellitus in women achieving singleton pregnancy spontaneously or after ART: a systematic review and meta-analysis. Hum Reprod Update. 2020;26:514–544. doi:10.1093/humupd/dmaa011
12. Tang D, Cheng Y, Feng X, Li X, Coyte PC. The use of IVF/ICSI and risk of postpartum hemorrhage: a retrospective cohort study of 153,765 women in China. Front Public Health. 2023;11:1016457. doi:10.3389/fpubh.2023.1016457
13. Stürmer T, Joshi M, Glynn RJ, Avorn J, Rothman KJ, Schneeweiss S. A review of the application of propensity score methods yielded increasing use, advantages in specific settings, but not substantially different estimates compared with conventional multivariable methods. J Clin Epidemiol. 2006;59:437–447. doi:10.1016/j.jclinepi.2005.07.004
14. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46:399–424. doi:10.1080/00273171.2011.568786
15. Wang Y, Shi H, Chen L, et al. Absolute risk of adverse obstetric outcomes among twin pregnancies after in vitro fertilization by maternal age. JAMA Network Open. 2021;4:e2123634. doi:10.1001/jamanetworkopen.2021.23634
16. Lang M, Zhou M, Lei R, Li W. Comparison of pregnancy outcomes between IVF-ET pregnancies and spontaneous pregnancies in women of advanced maternal age. J Matern Fetal Neonatal Med. 2023;36. doi:10.1080/14767058.2023.2183761
17. Magnus MC, Fraser A, Håberg SE, et al. Maternal risk of cardiovascular disease after use of assisted reproductive technologies. JAMA Cardiol. 2023;8:837–845. doi:10.1001/jamacardio.2023.2324
18. Badeghiesh A, Hochberg A, Elsherbini N, Baghlaf H, Dahan MH. How does IVF conception affect pregnancy complications in an older cohort of women, at least 38 years of age? Study of a population database. J Assist Reprod Genet. 2023;40:2139–2148. doi:10.1007/s10815-023-02890-0
19. Wu Y, Chen Y, Shen M, et al. Adverse maternal and neonatal outcomes among singleton pregnancies in women of very advanced maternal age: a retrospective cohort study. BMC Pregnancy Childbirth. 2019;19(1):3. doi:10.1186/s12884-018-2147-9
20. Tanaka H, Hasegawa J, Katsuragi S, et al. High maternal mortality rate associated with advanced maternal age in Japan. Sci Rep. 2023;13:12918. doi:10.1038/s41598-023-40150-4
21. Bartsch E, Medcalf KE, Park AL, Ray JG. High Risk of Pre-eclampsia Identification Group, Clinical risk factors for pre-eclampsia determined in early pregnancy: systematic review and meta-analysis of large cohort studies. BMJ. 2016;353:i1753. doi:10.1136/bmj.i1753
22. Wang Y-X, Mitsunami M, Manson JE, et al. Association of gestational diabetes with subsequent long-term risk of mortality. JAMA Intern Med. 2023;e234401. doi:10.1001/jamainternmed.2023.4401
23. Chen B, Du Y-R, Zhu H, et al. Maternal inheritance of glucose intolerance via oocyte TET3 insufficiency. Nature. 2022;605:761–766. doi:10.1038/s41586-022-04756-4
24. Sugai S, Nishijima K, Haino K, Yoshihara K. Pregnancy outcomes at maternal age over 45 years: a systematic review and meta-analysis. Am J Obstet Gynecol MFM. 2023;5:100885. doi:10.1016/j.ajogmf.2023.100885
25. Smithson SD, Greene NH, Esakoff TF. Pregnancy outcomes in very advanced maternal age women. Am J Obstet Gynecol MFM. 2022;4:100491. doi:10.1016/j.ajogmf.2021.100491
26. Osmundson SS, Gould JB, Butwick AJ, Yeaton-Massey A, El-Sayed YY. Labor outcome at extremely advanced maternal age. Am J Obstet Gynecol. 2016;214:362.e1–7. doi:10.1016/j.ajog.2015.09.103
27. Stern JE, Liu C-L, Cabral HJ, et al. Factors associated with increased odds of cesarean delivery in ART pregnancies. Fertil Steril. 2018;110:429–436. doi:10.1016/j.fertnstert.2018.04.032
28. Friedman AM, D’Alton M. Society for Maternal-Fetal Medicine Consult Series #51: thromboembolism prophylaxis for cesarean delivery. Am J Obstet Gynecol. 2021;224:243–244. doi:10.1016/j.ajog.2020.09.033
29. Hansen M, Kurinczuk JJ, Milne E, de Klerk N, Bower C. Assisted reproductive technology and birth defects: a systematic review and meta-analysis. Hum Reprod Update. 2013;19:330–353. doi:10.1093/humupd/dmt006
30. Sarmon KG, Eliasen T, Knudsen UB, Bay B. Assisted reproductive technologies and the risk of stillbirth in singleton pregnancies: a systematic review and meta-analysis. Fertil Steril. 2021;116:784–792. doi:10.1016/j.fertnstert.2021.04.007
31. Ganer Herman H, Mizrachi Y, Shevach Alon A, et al. Obstetric and perinatal outcomes of in vitro fertilization and natural pregnancies in the same mother. Fertil Steril. 2021;115:940–946. doi:10.1016/j.fertnstert.2020.10.060
32. Huang Z, Xiao F, Xiao H, et al. Comparison of genetic profiles of neonates in intensive care units conceived with or without assisted reproductive technology. JAMA Network Open. 2023;6:e236537. doi:10.1001/jamanetworkopen.2023.6537
33. Heineman KR, Kuiper DB, Bastide-van Gemert S, Heineman MJ, Hadders-Algra M. Cognitive and behavioural outcome of children born after IVF at age 9 years. Hum Reprod. 2019;34:2193–2200. doi:10.1093/humrep/dez202
34. Kennedy AL, Vollenhoven BJ, Hiscock RJ, et al. School-age outcomes among IVF-conceived children: a population-wide cohort study. PLoS Med. 2023;20:e1004148. doi:10.1371/journal.pmed.1004148
35. Carlsen EØ, Wilcox AJ, Magnus MC, Hanevik HI, Håberg SE. Reproductive outcomes in women and men conceived by assisted reproductive technologies in Norway: prospective registry based study. BMJ Med. 2023;2:e000318. doi:10.1136/bmjmed-2022-000318
36. Graham ME, Jelin A, Hoon AHJ, Wilms Floet AM, Levey E, Graham EM. Assisted reproductive technology: short- and long-term outcomes. Dev Med Child Neurol. 2023;65:38–49. doi:10.1111/dmcn.15332
37. Zhang X, Chen L, Wang X, et al. Changes in maternal age and prevalence of congenital anomalies during the enactment of China’s universal two-child policy (2013–2017) in Zhejiang Province, China: an observational study. PLoS Med. 2020;17:e1003047. doi:10.1371/journal.pmed.1003047
38. Herbert M, Kalleas D, Cooney D, Lamb M, Lister L. Meiosis and maternal aging: insights from aneuploid oocytes and trisomy births. Cold Spring Harb Perspect Biol. 2015;7:a017970. doi:10.1101/cshperspect.a017970
39. Zapata-Masias Y, Marqueta B, Gómez Roig MD, Gonzalez-Bosquet E. Obstetric and perinatal outcomes in women ≥40 years of age: associations with fetal growth disorders. Early Hum Dev. 2016;100:17–20. doi:10.1016/j.earlhumdev.2016.04.010
40. Palatnik A, De Cicco S, Zhang L, Simpson P, Hibbard J, Egede LE. The association between advanced maternal age and diagnosis of small for gestational age. Am J Perinatol. 2020;37:37–43. doi:10.1055/s-0039-1694775
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Maternal and Neonatal Outcomes in Pregnant Women Vaccinated Against COVID-19 Compared to an Unvaccinated Group
Nourian T, Sarandili S, Mousavi S, Mirmohammadkhani M, Rahmanian M
International Journal of Women's Health 2025, 17:4131-4142
Published Date: 5 November 2025